
Abstract
Objective:
Type B aortic dissection (TBAD) is a life-threatening condition, and it takes heavy burden to family and society. Return to work (RTW) not only means patients’ physical health but also demonstrates their mental well-being. Thoracic endovascular aortic repair (TEVAR) has been successful in treatment of TBAD patients. However, less studies have addressed on the social functional recovery of TBAD after TEVAR, especially for RTW.
Methods:
From January 1, 2017 to January 1, 2021, TBAD patients who underwent TEVAR and completed a 12-month follow-up were retrospectively enrolled. Primary outcome was RTW. Patients’ demographic, sociological, and clinical characteristics, and so on were recorded to analyze and demonstrate independent risk factors for RTW.
Results:
Four hundred thirty-two TBAD patients (388 males) were enrolled with a mean age of 48.3±8.9 years (ranged from 19 to 60 years). The 12-month cumulative RTW rate was 62.7% (95% confidence interval [CI]: 57.2%–67.8%). Age <50 years (odds ratio [OR]=3.675, 95% CI: 1.436–9.405) was identified as independent protective factors for RTW, while preoperative job as manual workers (OR=0.101, 95% CI: 0.029–0.353), average annual income, <30 000 Chinese Yuan (CNY) [<4400 US dollar], (OR=0.186, 95% CI: 0.054–0.637), complicated TBAD (malperfusion) (OR=0.246, 95% CI: 0.092–0.659), and distal stent graft-induced new entry (SINE) (OR=0.218, 95% CI: 0.083–0.575, p=0.002) were identified as independent risk factors.
Conclusion:
Approximately 64% of our patients were able to RTW in the 12 months post-TEVAR for TBAD. Younger patients, patients with less physically demanding jobs, and patients with less complex surgeries were more likely to RTW. Based on these results, more can be done to facilitate the patient’s ability and willingness to RTW after TEVAR.
Clinical Impact
Type B aortic dissection (TBAD) is a life-threatening condition that poses significant burden on both individuals and society. The ability to return to work (RTW) not only reflects the patient’s physical health but also indicates their mental well-being. Therefore, identifying risk factors for RTW and promoting the reintegration of TBAD patients into the workforce is crucial in clinical practice.To our knowledge, this study is the first to elucidate and predict the RTW outcomes of TBAD patients who underwent thoracic endovascular aortic repair (TEVAR).
Introduction
Thoracic endovascular aortic repair (TEVAR) is increasingly being used for the treatment of type B aortic dissection (TBAD) due to low perioperative morbidity and mortality.1,2 However, the mid- to long-term outcomes have been a source of concern.2–4 The ability to return to work (RTW) has been used as an important recovery indicator in cardiovascular disease,5,6 as it is a surrogate marker for a meaningful recovery. Conversely, unemployment can result in significant direct, indirect, and intangible costs for patients. Direct costs of unemployment are the economic costs, such as medical expenses, transportation costs, and any other out-of-pocket expenses incurred by the patient. Indirect costs are the costs that are associated with the impact of returning to work on the patient’s family, such as the need for caregivers, lost income due to time off work, and any other related expenses. Intangible costs are the non-economic costs that are difficult to quantify, such as the impact on the patient’s quality of life included physical well-being7,8 (a healthy body weight, good nutrition, and regular physical activity.) and emotional well-being5,9–11 (feelings of sadness or hopelessness, difficulty concentrating, loss of interest in activities, changes in appetite and sleep patterns, etc)
In our population, the average age of patients presenting with TBAD is 52.7±11.1 years, about 10 years younger than that in Western countries. 12 Hence, their loss of employment often negatively impacts the patients, and in turn the country’s economic burden. This is compounded by the high medical bills related to the TEVAR and TBAD, often adding to the patient’s financial woes. 13
To date, there have been few studies focusing on RTW in patients with aortic dissection. Lin et al found that less than 25% type A aortic dissection (TAAD) patients returned to the same occupations at 12 months after open triple-branched stent graft placement. 14 However, compared with open surgery, TEVAR is less invasive and hence associated with a shorter recovery period and lower perioperative morbidity, possibly facilitating RTW. To our best knowledge, there has been no prior published research on returning to work after TEVAR for TBAD patients. The aim of this study is to evaluate the rate of patients returning to work within 12 months after TEVAR for TBAD, and assess the predictors affecting RTW in TBAD patients who underwent TEVAR.
Materials and Methods
Patients and Data Collection
All patients who underwent TEVAR for TBAD in our center from January 1, 2017 to January 1, 2021 were enrolled. Patients were included if they met the following inclusion criteria: (1) age 18- to 60-year old at time of diagnosis, (2) had a full-time or part-time job at time of diagnosis, and (3) underwent successful TEVAR for the TBAD. Patients were excluded if they: (1) were unemployed at time of diagnosis of TBAD, (2) did not give consent for their participation in the study, and (3) were lost to follow-up or died within 12 months after discharge.
Management and TEVAR
All patients with TBAD were admitted and managed according to our department protocol.3,4 On admission, the computed tomographic angiography (CTA) was performed to confirm the diagnosis and for preoperative planning. All TEVAR procedures were performed under general anesthesia in our hybrid operating theater, and the endovascular procedure has been detailed elsewhere.3,4,15 Briefly, an oversizing ratio of 5% to 10% is recommended in the choice of stent graft; a ≥15 mm proximal landing zone was necessary and the deployment of proximal portion of stent graft was decided on the anatomical characteristics of the lesion; additional branch reconstruction was performed when necessary.3,4,15,16 The success of TEVAR was defined as successful deployment of stent graft with primary tear covered as intended.
Data Collection
All eligible patients were identified from the hospital electronic medical records. Details on the patient biodata, pre-existing comorbidities, as well as employment status and annual income on admission were collected as part of our standard admission screening. We divided patients’ occupations into 3 categories: (1) professional and clerical, (2) semi-skilled occupations (eg, police/military, chefs, skill labor), and (3) manual labor (general labor, farmers). The perioperative characteristics of the TBAD and TEVAR were also recorded, including operating time, TEVAR procedural details, length of hospital, and intensive care unit (ICU) stay.
Outcomes and Follow-up
All patients were followed up by CTA at 3, 6, 12 months, and then annually after TEVAR. In particular, detailed information regarding the patient’s employment after TEVAR was obtained via in in-person interview during the patient’s follow-up visits. If patients who were unable to attend clinic visits, telephone interview was used as an alternative. These tasks were completed by the attending physicians in the outpatient department.
The primary endpoint was RTW, defined as full-time employment at any time point from post-TEVAR to 12 months after discharge (RTW group). Patients who returned to work immediately after TEVAR but were lost to follow-up before the 12-month endpoint assessment, or those who returned to work but subsequently lost their job before the 12-month endpoint assessment, will also be included in the analysis. The RTW group was further classified into 3 groups based on whether they returned to the same job, switched to another job due to health concerns resulting from the TBAD, or switched to another job for other reasons. The timepoint at which the patient returned to work was also recorded. For patients who did not RTW at 12 months after TEVAR (non-RTW group), their reasons were divided as follows: (1) unable to work owing to TBAD, (2) preferred not to work due to TEVAR, (3) lost their jobs due to the TBAD, and (4) other reasons.
This study was approved by the Ethics Committee of our center. All patients provided written informed consent for inclusion in the study, which was performed in agreement with the ethical principles of the Declaration of Helsinki. In addition, all data were anonymized to ensure patient confidentiality.
Statistical Analysis
Categorical variables (presented as frequencies and percentages) were compared using the χ2 test or Fisher exact test. For quantitative data, which were compared using the Student t-test, Mann-Whitney U test or nonparametric test are shown as mean ± standard deviation (SD) or as the median with the interquartile range (IQR), depending on their distribution. Binary logistic regression was performed to identify the independent risk factors for RTW by stepwise selection of variables. Factors in univariate analyses were introduced into the multivariate model if the p value was less than 0.05. Kaplan-Meier was applied to analyze cumulative incidence of RTW rate. All statistical tests were performed using a 2-sided α of 0.05. All tests were performed utilizing STATA software version 15.1. (StataCorp, College Station, Tex), or GraphPad Prism, version 8.0.0 (San Diego, California, USA).
Results
Baseline Characteristics
From January 1, 2017 to January 1, 2021, 432 TBAD patients were included in our study (Figure 1). The mean age of the patients was 48.3±8.9 years (range: 19–60 years), and 89.8% were males (n=388). Among the 432 patients, 402 (93.1%) were married, 408 (94.4%) had children, 281 (65.0%) lived in urban areas, and 140 (32.4%) received college education. At time of diagnosis of TBAD, 55.3% (n=239) of patients were professional workers, and 19.7% (n=85) were manual workers. Among the study population, a total of 75 patients (17.4%) had an annual income of less than 30 000 Chinese Yuan (CNY) (corresponding to less than 4400 US dollars), while 167 patients (38.7%) reported an annual income exceeding 70 000 CNY (equivalent to more than 10 105 US dollars]. More details of the baseline characteristics are shown in Table 1.
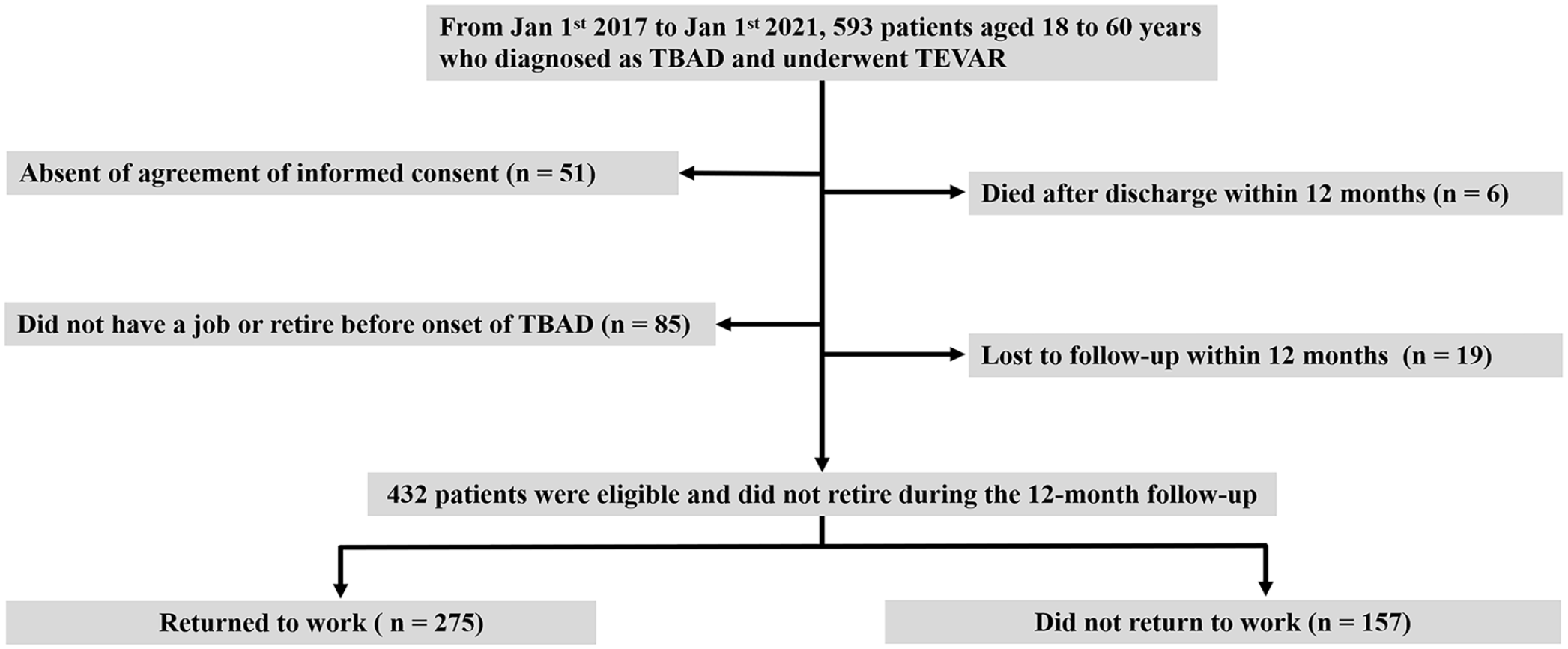
Protocol of current study. TBAD, type B aortic dissection; TEVAR, thoracic endovascular aortic repair.
Baseline Characteristics Between 2 Groups of Patients.
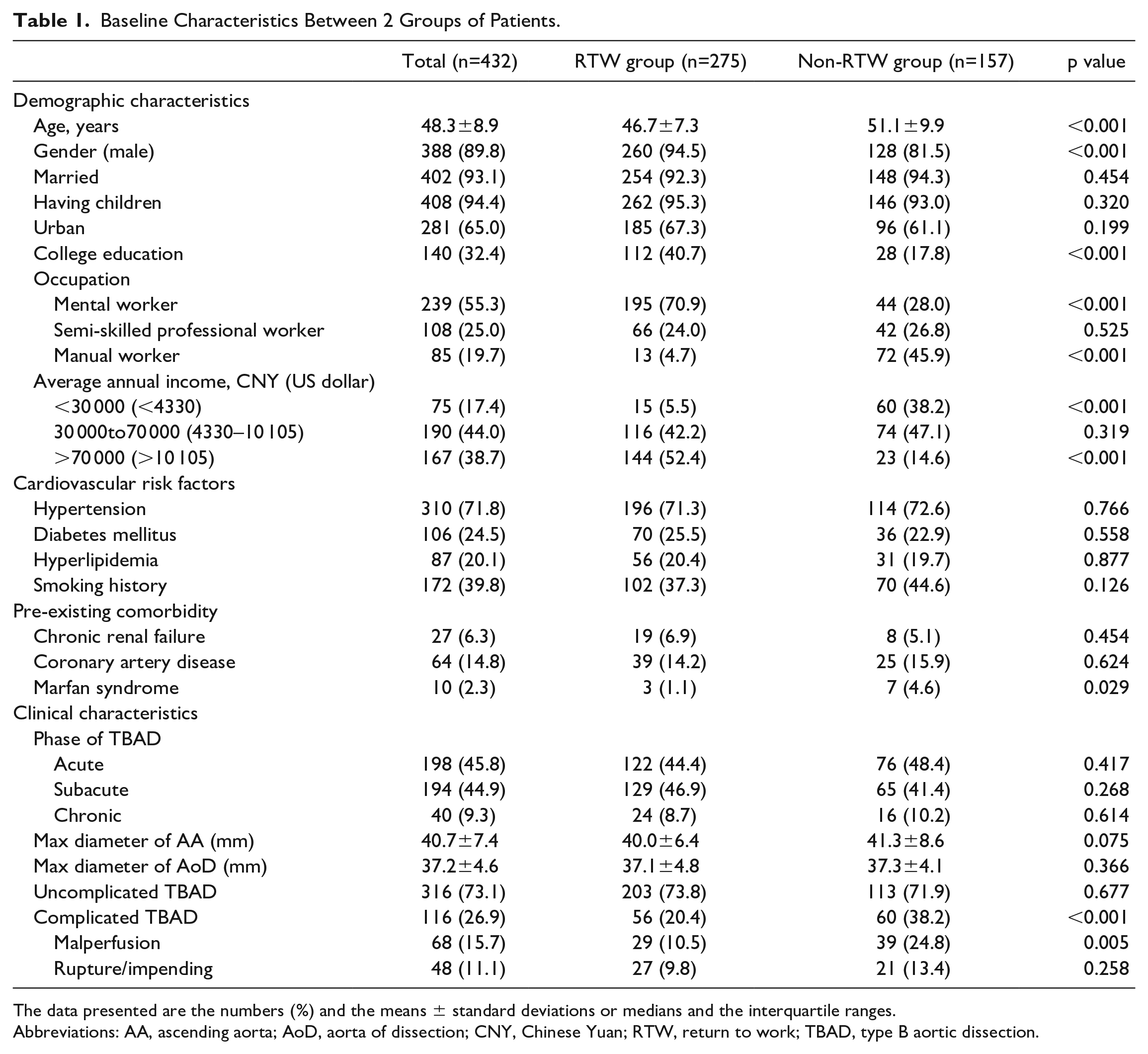
The data presented are the numbers (%) and the means ± standard deviations or medians and the interquartile ranges.
Abbreviations: AA, ascending aorta; AoD, aorta of dissection; CNY, Chinese Yuan; RTW, return to work; TBAD, type B aortic dissection.
RTW and Related Reasons
In this study, only 10 patients (2.3%) were followed up by telephone due to long distance from our center, and we obtained their CTA data by email. Two hundred seventy-five (62.7%, 95% confidence interval [CI]: 57.2%–67.8%) patients returned to work within 12 months after TEVAR (RTW group) (Figure 2). Among the 275 RTW patients, 171 patients (62.2%) returned to the same occupation, 81 patients (29.5%) had changed jobs due to health concerns from the TBAD, and 23 patients (8.4%) changed their jobs for other reasons (Supplemental Table 1). One hundred fifty-seven patients failed to RTW within 12 months after TEVAR, among whom 70 patients (44.6%) were unable to work due to TBAD, 57 patients (36.3%) preferred not to work, and 21 patients (13.4%) lost their jobs owing to the TBAD. The remaining 9 patients (5.7%) were unable or preferred not to work owing to other reasons (1 due to family affairs, 7 due to the COVID-19 pandemic, and 1 for no specific reason) (Supplemental Table 1).
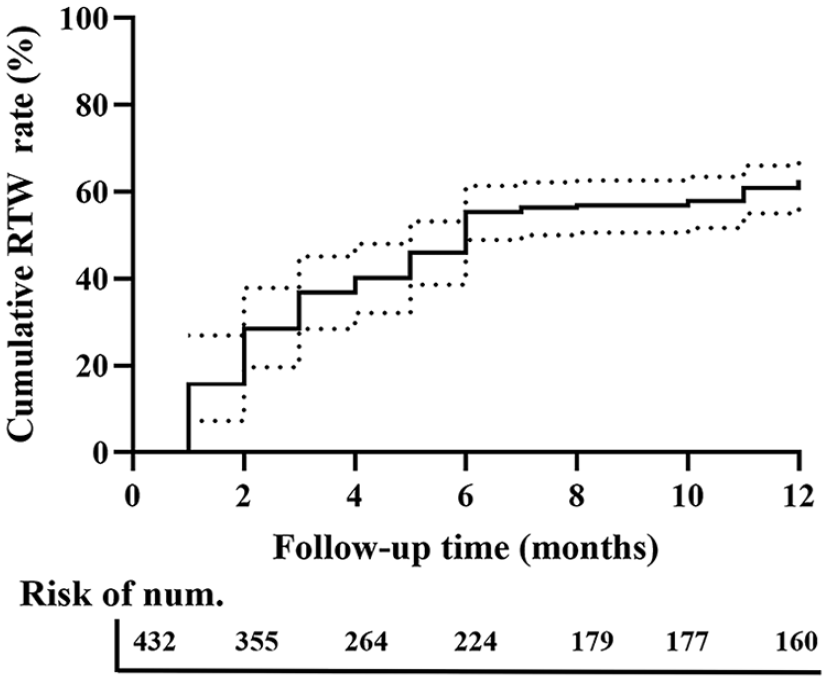
Kaplan-Meier curves showing the probabilities of cumulative return to work (RTW) rate of type B aortic dissection (TBAD) patients after thoracic endovascular aortic repair (TEVAR).
Characteristics of RTW Group and Non-RTW Group
No significant differences were observed between RTW group and non-RTW group in terms of family status, cardiovascular risk factors, acuity of TBAD, and maximum aorta diameter (Table 1).
However, univariate analysis showed that the mean age of patients in the RTW group tended to be younger than that of the non-RTW group (46.7±7.3 vs. 51.1±9.9 years, p<00.001) and that males were more likely to RTW (94.5% vs. 81.5%, p<0.001). Patients with college education (40.7% vs. 17.8%, p<0.001), mental workers (70.9% vs. 28.0%, p<0.001), and patients with higher annual income (52.4% vs. 14.6%, p<0.001) were also more likely to RTW.
Perioperative characteristics and follow-up outcomes were compared in Table 2. Operating time, complexity of TEVAR, and length of hospital stay did not significantly affect a patient’s ability to RTW. However, a longer ICU stay was a risk factor (2.0 [1.0–6.0] vs. 4.5 [2.0–8.5], p=0.048) for not returning to work. Of note, the occurrence of in-hospital complications did not impact ability to RTW.
Perioperative Characteristics and Follow-Up Outcomes Between 2 Groups.
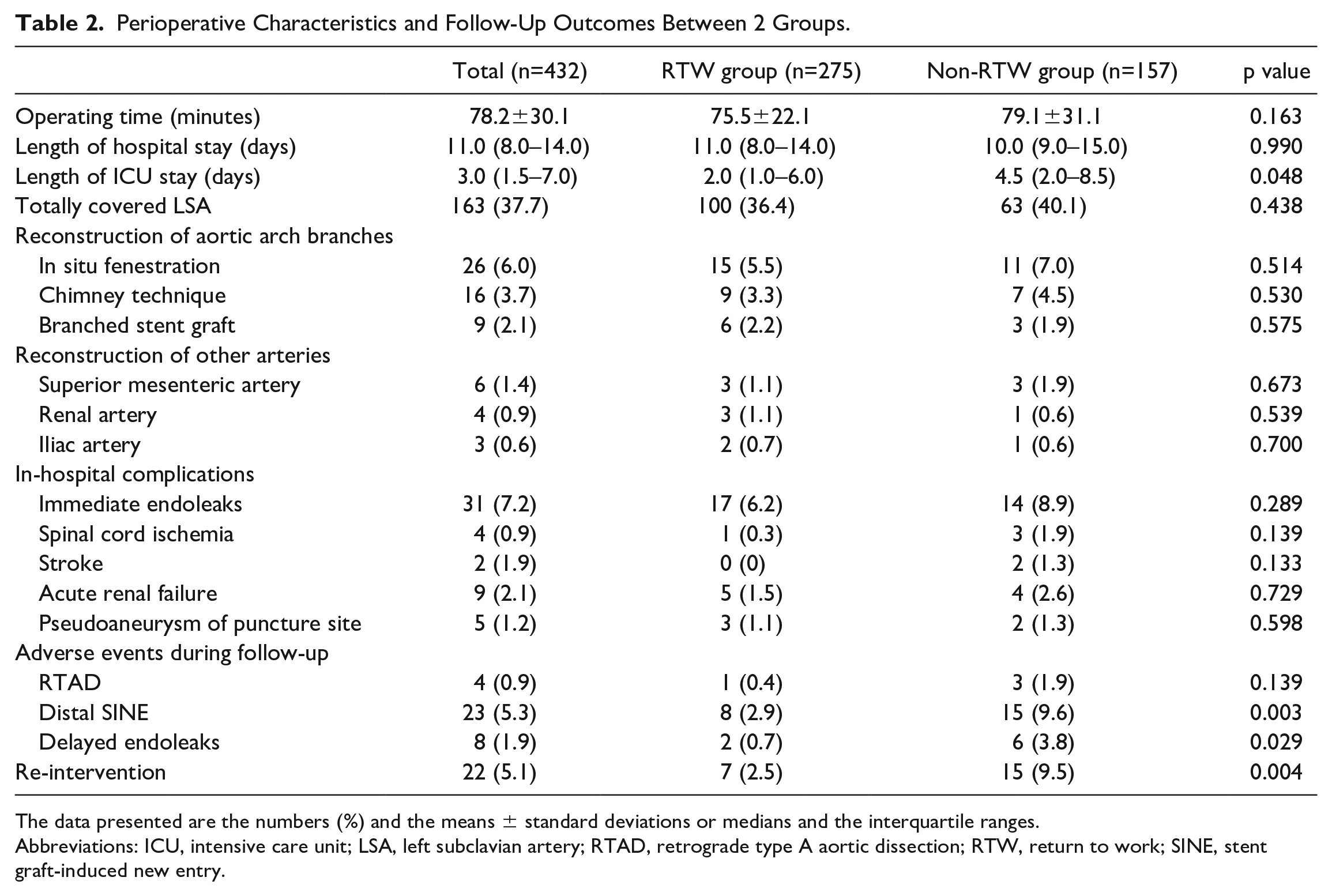
The data presented are the numbers (%) and the means ± standard deviations or medians and the interquartile ranges.
Abbreviations: ICU, intensive care unit; LSA, left subclavian artery; RTAD, retrograde type A aortic dissection; RTW, return to work; SINE, stent graft-induced new entry.
There were 23 patients who developed distal stent graft-induced new entry (SINE) during the follow-up period. Eight of these patients (2.9%) returned to work and 15 patients (9.6%) did not (p=0.003). Patients with delayed endoleaks were less likely to RTW (0.7% vs. 3.8%, p=0.029). And patients who underwent re-intervention of RTW group were also less than non-RTW group (2.5% vs. 9.5%, p=0.029) (Table 2). In the cohort of patients requiring re-intervention, 3 underwent graft replacement of the ascending thoracic aorta, with or without partial or total aortic arch replacement, as a result of retrograde type A dissection (RTAD). Fifteen patients underwent secondary TEVAR due to distal SINE, and 4 patients underwent secondary TEVAR with adjunctive reconstruction of aortic arch branches due to type Ia endoleak.
Multivariate Analysis
Based on the results of the univariate logistic regression, several variables were identified: age <50 years, gender (male), received college education, preoperative occupation (mental and manual worker), average annual income (<30 000 CNY [4400 US dollars] and >70 000 CNY [10 105 US dollars]), Marfan syndrome, complicated TBAD (malperfusion), distal SINE, delayed endoleaks, and re-intervention. After multivariate logistic analysis, age <50 years (OR=3.675, 95% CI: 1.436–9.405, p=0.007) was identified as independent protective factors, while preoperative job as manual workers (OR=0.101, 95% CI: 0.029–0.353, p<0.001), average annual income (<30 000 CNY [4400 US dollars]) (OR=0.186, 95% CI: 0.054–0.637, p=0.007), complicated TBAD (malperfusion) (OR=0.246, 95% CI: 0.092–0.659, p=0.005), and distal SINE (OR=0.218, 95% CI: 0.083–0.575, p=0.002) were identified as independent risk factors for RTW (Table 3). We established a multiple logistic regression model of RTW at 12 months for TBAD patients after TEVAR and the area under receiver operating characteristic curve (ROC)=0.9055 (Figure 3).
Univariate and Multivariate Logistic Regression Analyses of Independent Risk Factors.
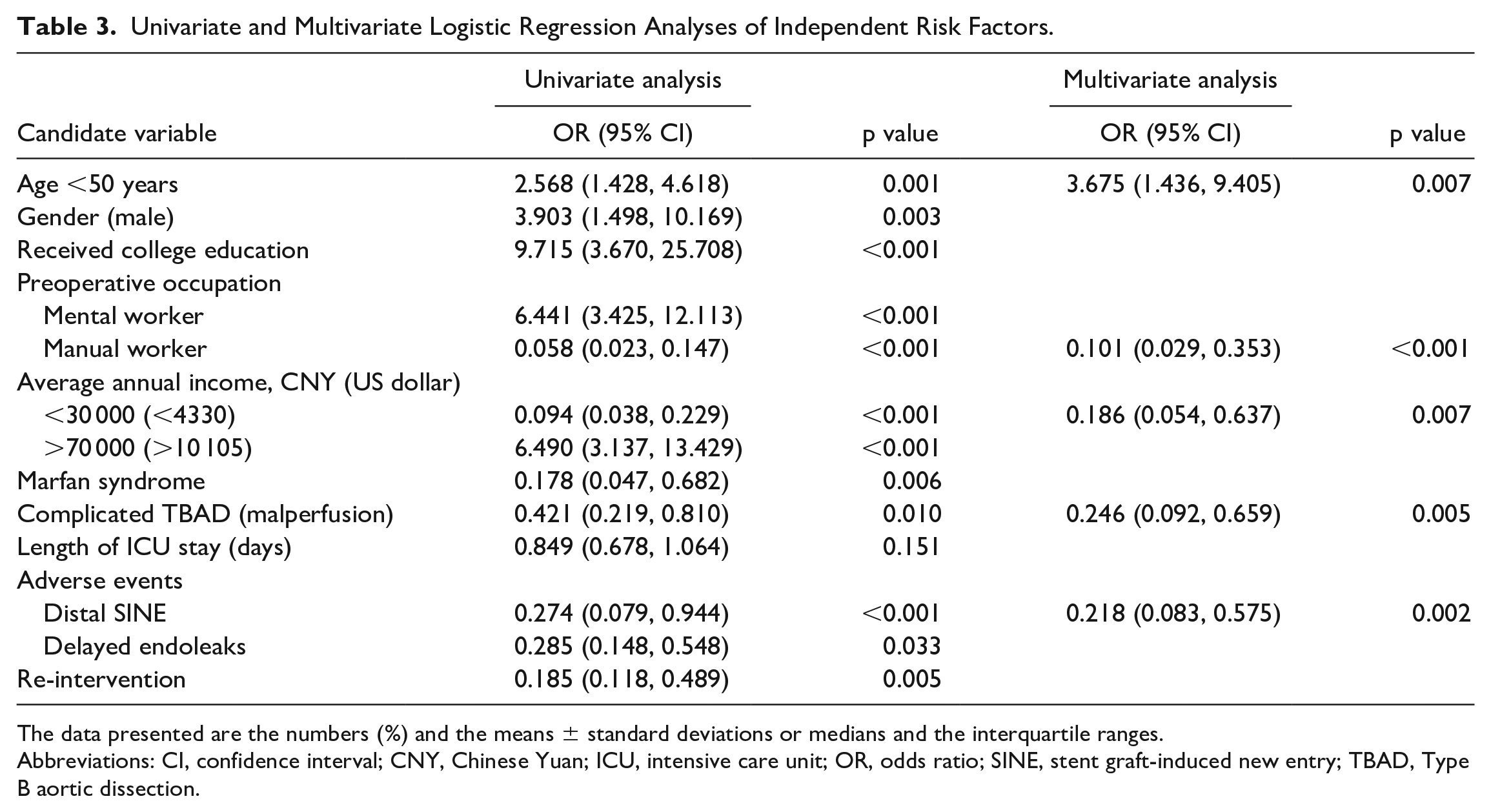
The data presented are the numbers (%) and the means ± standard deviations or medians and the interquartile ranges.
Abbreviations: CI, confidence interval; CNY, Chinese Yuan; ICU, intensive care unit; OR, odds ratio; SINE, stent graft-induced new entry; TBAD, Type B aortic dissection.
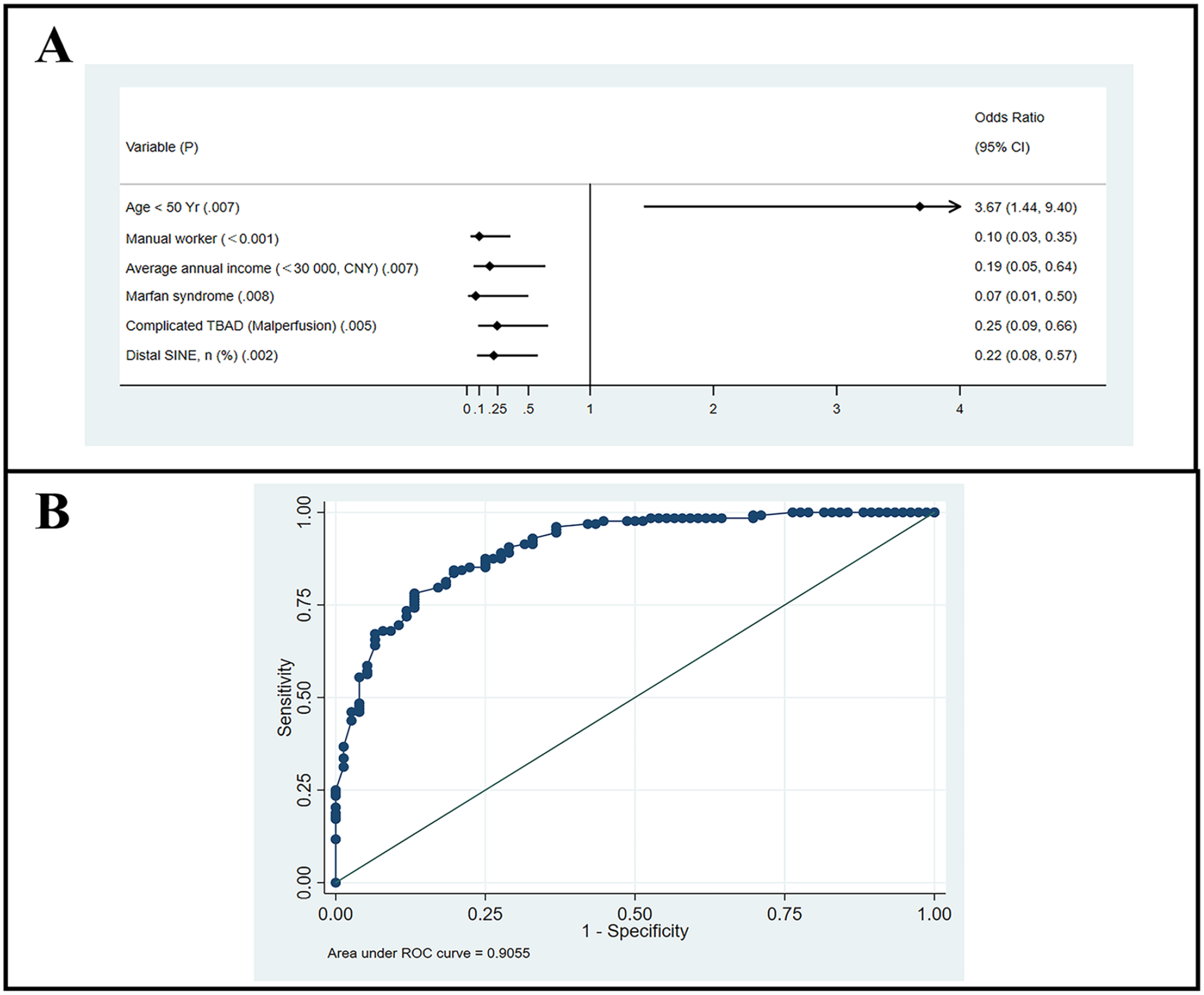
Adjusted odds ratio (OR) of returning to work within 12 months after thoracic endovascular aortic repair (TEVAR) for TBAD patients. (A) Forest plot; (B) receiver operating character curve of the binary logistic regression model. CI, confidence interval; TBAD, type B aortic dissection; SINE, stent graft-induced new entry; CNY, Chinese Yuan; ROC, receiver operating characteristic.
Discussion
This is a retrospective cohort study of TBAD patients who underwent TEVAR in a tertiary hospital in China. In the present study, the 12-month cumulative rate of RTW following hospitalization for patients with TBAD was 62.7%, which is comparable with the RTW rates reported in patients with myocardial infarction and heart failure (55.9%–72.2%) according to previous publications.5,6,17,18 These findings suggest that a less invasive surgical approach for TBAD may confer notable benefits. We also identified several independent factors, including age younger than 50 years, preoperative job as manual workers, lower average annual income, complicated TBAD (malperfusion), and distal SINE, which affected patients’ ability to RTW after TEVAR. To our best knowledge, it is the first study to illustrate RTW after TEVAR in TBAD patients.
We observed that the patient cohort with TBAD in our study was comparatively younger than those reported in other countries, and notably below the Chinese retirement age of 65 years. 12 These patients belong to the age group that forms the backbone of the nation’s workforce, and often they are often the main breadwinners of their families. Therefore, successful RTW post-TEVAR is vital from both a social and economic point of view. Interestingly, most patients (75.6%, 208/275) were able to RTW within 6 months (Figure 2). We hypothesize 2 potential explanations: (1) patients experience a physical and mental recovery within the first 6 months, leading to a decrease in their fear of the disease and (2) economic needs or company requirements prompt patients to RTW within 6 months.
Our study showed that younger patients (age <50 years old) were more likely to RTW. This is consistent with other studies published indicating the RTW rates for patients with cardiovascular after treatment.5,19,20 Several aspects may explain that age played an important role in the ability of patients to RTW. First, the clinical presentations and postoperative outcomes in older AD patients are much worse than those in younger AD patients1,21; therefore, younger AD patients are likely to have a better physiological recovery after surgery and are more likely to regain social function and working ability. Second, younger patients are likely to have less comorbidities, thus reducing the risk of adverse events after TEVAR, which might be not conducive to the RTW. Finally, we speculate that TBAD patients in their 30s to 50s are more likely to work after TEVAR because of financial pressures, especially in our population where young males often bear the entire family financial burden.
Our study also revealed that patients of a lower annual income (<30 000 CNY [4400 US dollars]) and who were previously working in manual occupations trend toward status quo post recovery, that is, they do not return to their previously physically demanding jobs. As a cross-sectional survey of aortic dissection patients showed that, only 3% patients who worked as a manual worker came back to the jobs requiring the same physical intensity. 22 And these results are also consistent with RTW studies involving patients who underwent surgery.23–25 This can be attributed to a deep-seated cultural belief that one is better off avoiding physically strenuous work after a major surgery. However, such an outcome does not bode well for these possibly lower-educated patients economically, as they face limited employment options if their only viable alternative is to seek out non-manual-labor jobs. The proportion of people who changed their jobs in this group was also relatively high, as many likely opted for jobs with shorter working hours after their TBAD.
The above observation vis-à-vis the manual workers can be contrasted with the professional and clerical workers. We noted that this group is more likely to RTW after their surgery. Some studies showed that the preoperative occupation types and education levels are influential indicators of socioeconomic status, and it may reveal the conditions of income and health status.26,27 We hypothesize this to be the case because, with the benefit of higher education, these workers are not shackled by scientifically unproven cultural beliefs that one is unable to work after major surgery. Finally, the physical demands of their jobs are likely lower and they have many more options when it comes to choosing or changing jobs.
In our study, we have demonstrated that complicated TBADs, specifically malperfusion, are an independent negative factor for RTW. Suzuki et al reported that 28% mortality in acute TBAD with malperfusion compared with 9.6% in those whom without malperfusion indicating that the patients’ health conditions were terribly affected by malperfusion. 20 In addition to the increased physiological impact associated with a more complex surgery and hospital stay, the emotional toll that illness has on patients cannot be overlooked. Ashish et al first demonstrated that physical and sexual activity will decrease after AD, especially in complicated AD, and reported that 32% of patients with AD self-reported anxiety due to the disease. 22 Thus, for these selected patients, we should make greater efforts to develop approaches to facilitate their RTW, such as providing targeted rehabilitation exercises and health education by the nursing team, and advocating for more favorable policies from the government. 26
Distal SINE is a known adverse complication post-TEVAR that often necessitates re-intervention.2,4,28 While it is mostly detected on imaging, some patients can present with symptoms, such as chest pain or abdominal pain. The physical discomfort and need for re-intervention certainly impact a patient’s ability to RTW.2,4 From mental standpoint, distal SINE brings with more attention from doctors during follow-up after TEVAR, then might make patients feel much more mental stress. In addition, re-intervention can cause a secondary injury or harm to the patient, potentially resulting in increased physical and physiological susceptibility, longer recovery time, and higher risk of complications. 22 Thus, the occurrence of distal SINE and subsequent re-intervention may significantly impact patients’ ability to RTW.
The limitation of our study is that it is a single-center retrospective study, and this might have led to some selection bias. In addition, the outcomes were self-reported by patients, we did not have any means of verifying if the patients had accurately reported their employment status or occupations. Given that employment patterns are something intrinsically tied to the culture and healthcare insurance policies within a society, some results of our study might not be applicable in other countries. However, we believe that RTW is an important indicator that needs to be studied especially in an aging population where healthcare burden continues to increase yearly.
Conclusion
Approximately, 64% of our patients were able to RTW in the 12 months post-TEVAR for TBAD. Younger patients, patients with less physically demanding jobs, and patients with less complex surgeries were more likely to RTW. Based on these results, more can be done to facilitate the patient’s ability and willingness to RTW after TEVAR.
Supplemental Material
sj-docx-1-jet-10.1177_15266028231197133 – Supplemental material for Predictors of Return to Work After Thoracic Endovascular Aortic Repair in Patients With Type B Aortic Dissection
Supplemental material, sj-docx-1-jet-10.1177_15266028231197133 for Predictors of Return to Work After Thoracic Endovascular Aortic Repair in Patients With Type B Aortic Dissection by Lingwei Zou, Xiaolang Jiang, Hao Liu, Bin Chen, Junhao Jiang, Tao Ma, Gang Fang, Daqiao Guo, Xin Xu, Weiguo Fu and Zhihui Dong in Journal of Endovascular Therapy
Footnotes
Acknowledgements
The authors thank Dr. Haoyun Yap from Department of Vascular Surgery, Singapore General Hospital, Singapore for her support in language editing.
Author Contributions
LZ: Conception and design, collection and assembly of data, data analysis and interpretation, and manuscript writing; XJ: Conception and design, collection and assembly of data, data analysis and interpretation; HL: Conception and design, collection and assembly of data, data analysis and interpretation, and manuscript writing; BC: Collection and assembly of data, data analysis and interpretation; JJ: Collection and assembly of data, data analysis and interpretation; TM: Collection and assembly of data, data analysis and interpretation; GF: Collection and assembly of data, data analysis and interpretation; DG: Administrative support and manuscript writing; XX: Collection and assembly of data, data analysis and interpretation; WF: Conception and design, administrative support, final approval of the manuscript, manuscript writing and financial support; ZD: Conception and design, administrative support, final approval of the manuscript, manuscript writing and financial support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by China National Natural Science Funds (Grant No. 82270507, 81970395), pre-study of major projects in 2022 (Grant No. IDF152075), and the excellent physician training program at Fudan University, China (Grant No. 2021MYPY002).
Ethics Approval
The study design was approved by the Ethics Committee of Zhongshan Hospital, Fudan University, Shanghai, China.
Informed Consent
All included patients were informed about the nature of the study and gave their written informed consent.
Consent for Publication
All patients signed a consent form for their data to be used for research or publication.
Availability of Data and Materials
Due to the confidential and identifiable nature of this data set, data sharing will not be available. All authors have accessed the database and verified its accuracy.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.