
Abstract
Objective:
To provide a descriptive overview on the contemporary outcomes of thoracic endovascular arch repair with inner branched endoprosthesis (bTEVAR) for the treatment of aortic arch pathologies.
Methods:
A comprehensive literature search was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement. Pre-defined search terms were used to interrogate PubMed and OVID Medline databases from January 1999 to July 2022. Patient characteristics, indication for treatment, procedural data, mortality rates, postoperative complications, and reintervention rate during follow-up were evaluated.
Results:
Nineteen articles were included, encompassing a total of 618 patients who received bTEVAR, most of which were double-branched (63.9%, n=395). The main indication for treatment was aneurysm secondary to chronic aortic dissection (38.8%, n=240/618) with a mean maximum diameter of 58.3±11.4 mm. Pooled mean technical success rate was 97.4±4.4% (95% confidence interval [CI]=95.1%–99.5%); 2 and 3 patients required conversion to chimney technique and open repair, respectively. Among the pooled rates of early complications, postoperative stroke was the highest (10.5%; 95% CI=6.8%–14.3%). Thirty-day and in-hospital mortality rate was 5.5% (95% CI=2.6%–9.7%). Forty patients (6.5%; 95% CI=2.5%–9.5%) required early reintervention. During a mean follow-up of 20.7±13.5 months, the mortality rate was 18.2% (n=108/593; 95% CI=8.6%–20.6%) where 12 (11.1%) were aortic-related. Pooled late reintervention rate was 9.6% (95% CI=4.8%–14.3%). Comparison of demographics and outcomes found no significant difference between single and double bTEVAR.
Conclusion:
Branched thoracic endovascular aortic repair is a promising approach for aortic arch pathologies with a high technical success rate despite a steep learning curve. However, contemporary outcomes reflect that postoperative stroke remains the predominant concern. Further experience and long-term follow-up are required to sufficiently elucidate the safety and durability of bTEVAR in the management of aortic pathologies for high-risk patients.
Clinical Impact
This systematic review summarized the contemporary outcomes of thoracic endovascular aortic repair with different inner branched stent-grafts for the management of aortic arch pathologies. Pooled results from nineteen studies with 618 patients demonstrated a high technical success rate and an acceptable mortality rate. However, postoperative stroke remains the major concern. Long-term follow-up is needed to evaluate its durability.
Introduction
Open surgical repair (OSR) is the gold standard for managing proximal aortic arch diseases. 1 However, OSR is associated with high stroke incidence and mortality rates ranging 2%–18% and 2%–16.5%, respectively. 2 During the past 2 decades, there has been a paradigm shift toward thoracic endovascular aortic repair (TEVAR) for different aortic pathologies. 3 Contemporary endovascular options include scallop or fenestrated endografts, chimney or parallel techniques, which serve as an alternative for high-risk patients unfit for OSR. Thoracic endovascular aortic repair of aortic arch diseases remains clinically and technically challenging. 4 The proximal arch is an anatomically complex segment due to multiple vital arterial branches and a variable 3-dimensional curvature.
Inoue et al 5 reported the first experience of unimodular custom-designed branched stent-grafts (BSG) that demonstrated good technical feasibility, but failures arose from endoleaks and strokes. The experience pioneered the design of BSGs that improved over time. Recent joint guidelines published by the European Association for Cardio-thoracic Surgery and the European Society for Vascular Surgery regarding aortic arch diseases recommend total endovascular repair of the arch in patients unfit for OSR with a favorable anatomy, 6 defined as follows: >30 mm proximal sealing zone (measured on the inner curvature); maximum diameter of the ascending aorta <38 mm; and free of excess calcification or thrombus.
Inner BSGs have been manufactured to allow for endovascular branch vessel reconstruction, which may be a preferred solution to address arch pathologies. The initial experience was documented by Haulon et al 7 for degenerative aneurysms and the results were encouraging despite an initial learning curve. Branched (b-)TEVAR may serve as an alternative for high-risk patients. However, only a few off-the-shelf and customized devices are currently available. 8
The aim of this study was to provide a descriptive overview by summarizing the current outcomes of BSG in TEVAR in the management of aortic arch pathologies.
Materials and Methods
Search Strategy
This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. 9
The PubMed and OVID Medline databases were searched from January 1999 to July 2022 to identify all publications on total endovascular aortic arch repair with BSGs in the English language. The following keywords were used: “branched endograft,” “branched stent-graft,” “aortic arch,” “aortic arch aneurysm,” “endovascular,” “aortic dissection,” and “thoracic endovascular arch repair.” The Medical Subject Heading (MeSH) terms are available in Supplementary Table 1. In addition, full texts and references of the retrieved articles were searched to identify further relevant studies fulfilling the inclusion criteria. References were managed with Endnote X9.3.3 (Clarivate Analytics, 2018).
Eligibility Criteria, Outcome Measures, and Definition
Studies were included according to the following inclusion criteria: (1) Clinical trials or case series that evaluated total endovascular aortic repair of any aortic pathologies with BSGs; (2) Studies reporting the clinical characteristics of patients (gender, age, co-morbidities, and underlying arch disease indicated for treatment), safety endpoints of BSGs (death, endoleak, stroke, spinal cord ischemia [SCI], myocardial ischemia, renal failure requiring dialysis, and retrograde aortic dissection within 30 postoperative days), and changes to the arch pathology during follow-up; (3) comparison studies between BSGs, chimney grafts, and fenestrated grafts in which the reported data of interest could be extracted separately for analysis; and (4) studies published in English. Exclusion criteria were studies focusing only on the anatomical feasibility of BSGs, hemodynamic analysis of BSGs configurations, delivery techniques, hybrid procedures or OSR with BSGs, and BSGs with customized or physician-modified fenestrations, animal, and cadaver studies. Cohorts or clinical trials with less than 5 patients and those without reporting of at least 6-month follow-up were excluded.
The efficacy of BSGs was determined by evaluating both technical and clinical success upon follow-up of each study per the reporting standards for TEVAR by the Society of Vascular Surgery and the American Association for Vascular Surgery. 10 Technical success was defined on an intent-to-treat basis that requires successful introduction and deployment of the endograft with secure proximal and distal fixation, and no evidence of type I or type III endoleak as evidenced by procedural angiography. Clinical success required continuous exclusion of the aneurysm, survival without rupture, freedom from type I or type III endoleak, no permanent paralysis, and no long-term dialysis.
Study Selection and Data Collection
Retrieved references were independently assessed for eligibility according to the selection criteria. Papers published from the same institute were individually judged to prevent overlapping and duplication of patient data from previous reports. Data for the outcome measures described above were extracted from the selected studies and entered into standardized data forms. Other data extracted include authors, year of publication, enrollment period, study design, arch pathology characteristics, BSG design and manufacturer, procedural data (operative time, landing zones, left subclavian artery [LSA] revascularization and occlusion methods, access conduit, and blood flow reduction), and emergency cases were collected where available. Data not clearly expressed were regarded as unavailable.
The primary data search and extraction was performed by one author (KJSK) and crosschecked by another author (LHL). Final results were scrutinized by the other co-authors. Disagreements were resolved by consensus by all authors.
Statistical Analyses
Standard descriptive statistics (mean and 95% confidence interval [CI]) were used to summarize baseline demographics. Outcome data were pooled, weighted, and compared using SPSS software (Version 26.0; IBM Corporation, Armonk, NY, USA). Data for the pooled analyses are given as the proportion and 95% CI. All p values are 2-sided; differences were significant at the level of p<0.05.
Results
Study Selection
Figure 1 shows the flowchart for the selection of eligible studies. The search strategy identified a total of 1368 references. There were 76 duplicates. Non-English publications, case reports, commentaries, reviews, and animal-/cadaveric-studies were filtered by automation tools. After screening 109 articles by titles and abstracts, 24 publications remained potentially relevant. After full text review, 9 further publications were excluded for reasons stated in Figure 1. Four additional studies were identified after evaluating the full texts and references of the included studies.11,12 Thus, 19 articles were included and analyzed.7,13–30
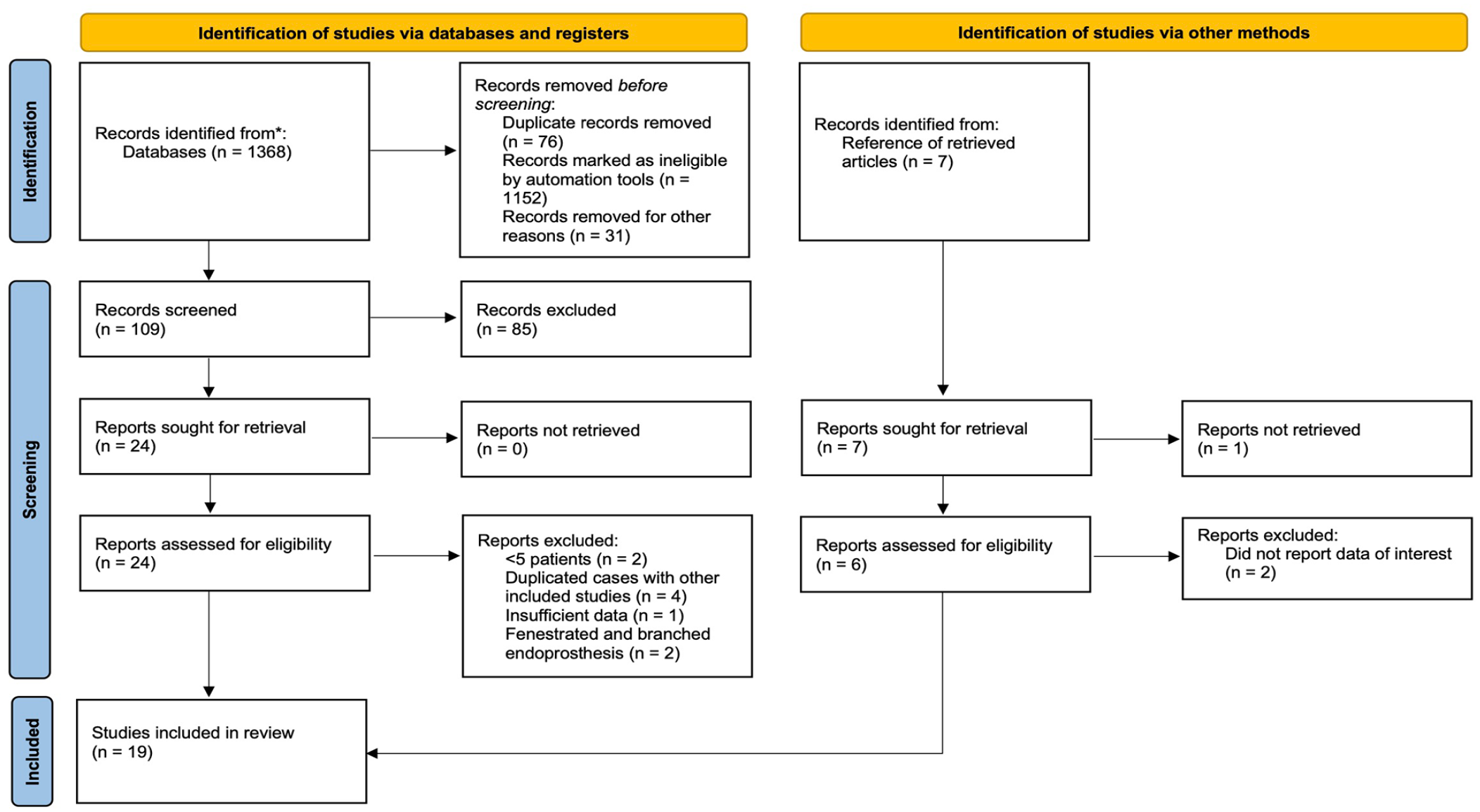
Preferred reporting items for systematic reviews and meta-analysis (PRISMA) flow diagram for studies on branched stent-graft endovascular repair for aortic arch pathologies.
Study Characteristics
The 19 included studies involved 618 patients who underwent endovascular repair of the aortic arch with BSGs. The study design, device, and manufacturer details are summarized in Table 1. The single-center series by Tsilimparis et al 23 included patients with prior open repair of the ascending aorta previously described in their sub cohort. All studies were included since the duplicate data were minimum (n=14).7,15,21
Summary of Characteristics of the Nineteen Included Studies.
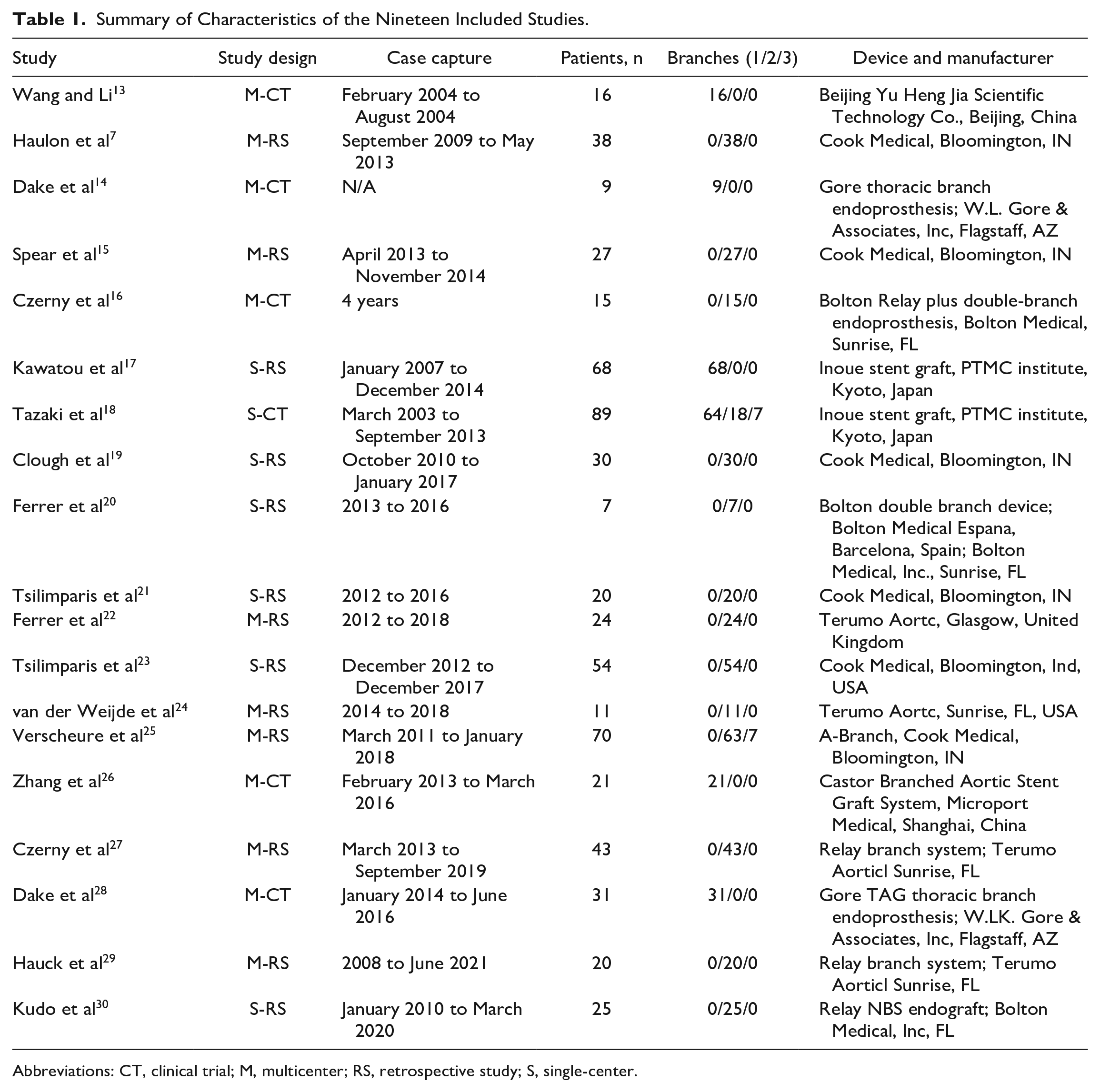
Abbreviations: CT, clinical trial; M, multicenter; RS, retrospective study; S, single-center.
Baseline patient demographics and co-morbidities are shown in Table 2. The mean age was 71.8±8.9 years and 74.4% were male (n=460/618). All articles reported information on patient co-morbidities, producing a pooled proportion of 89.2% (95% CI=85.2%–93.3%) with hypertension, 13.3% (95% CI=7.6%–19.1%) with diabetes, 53.0% (95% CI=43.1%–62.9%) with dyslipidemia, 38.7% (95% CI=31.5%–46.0%) with coronary artery disease, 14.3% (95% CI=10.9%–17.7%) with peripheral artery disease, 16.1% (95% CI=10.5%–21.8%) with previous cerebrovascular accident, 23.3% (95% CI=16.6%–29.9%) with renal insufficiency, 35.0% (95% CI=27.6%–42.4%) with chronic pulmonary obstructive disease, and 47.9% (95% CI=37.9%–57.9%) with smoking history.
Summary of Demographics and Pooled Outcomes of the 19 Included Studies and Comparison Between Single- Versus Double-Branched Endografts.
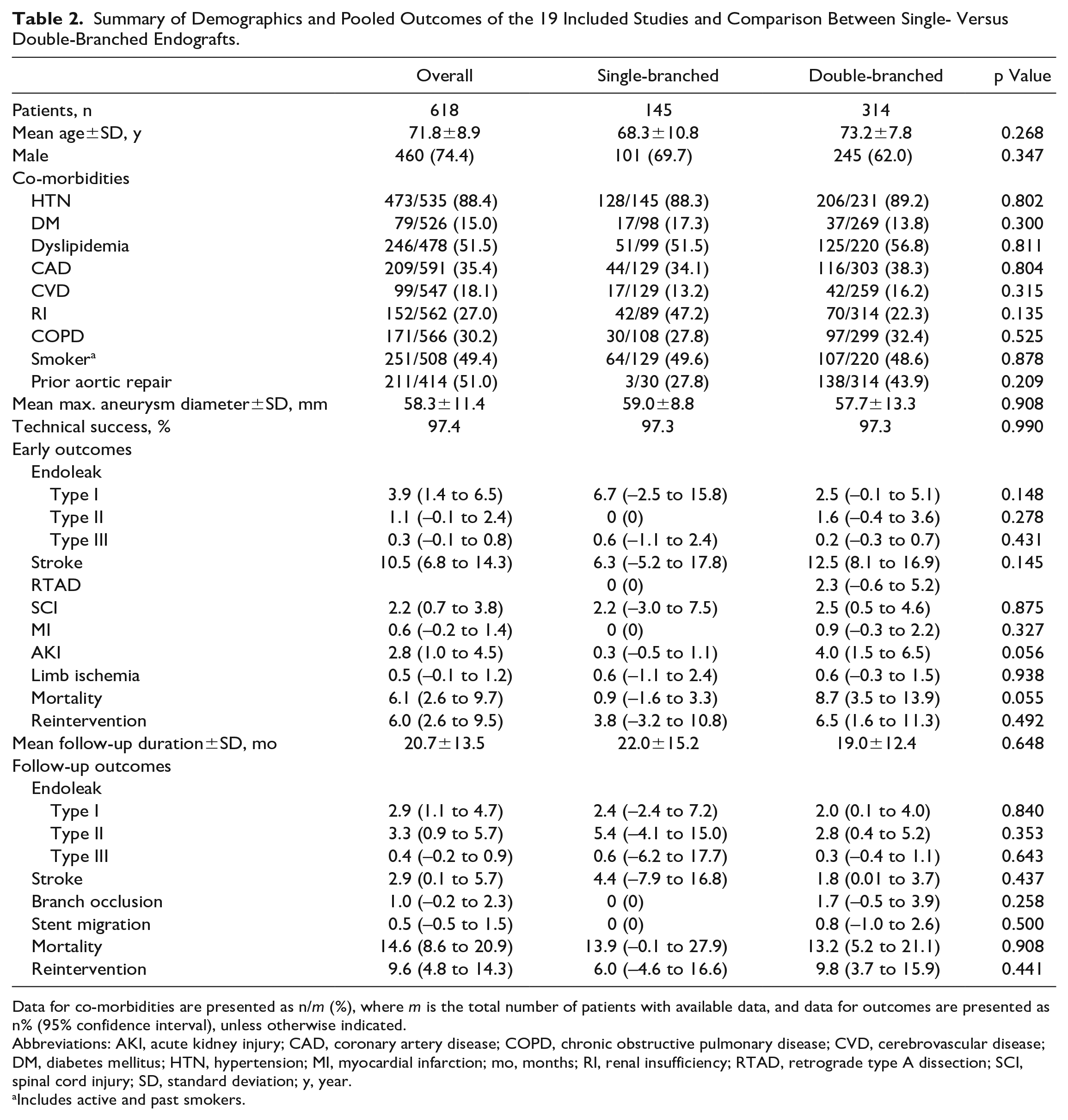
Data for co-morbidities are presented as n/m (%), where m is the total number of patients with available data, and data for outcomes are presented as n% (95% confidence interval), unless otherwise indicated.
Abbreviations: AKI, acute kidney injury; CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; CVD, cerebrovascular disease; DM, diabetes mellitus; HTN, hypertension; MI, myocardial infarction; mo, months; RI, renal insufficiency; RTAD, retrograde type A dissection; SCI, spinal cord injury; SD, standard deviation; y, year.
Includes active and past smokers.
Fifteen articles reported on patients with prior aortic surgery. Overall, 51.0% (n=211/414) had previous aortic repair but only 7 studies specified the type of repair. Majority were OSR (69.9%, n=58/83).
High-risk patients with aortic arch aneurysm were the main indication for TEVAR with BSGs. The mean maximum diameter of the aortic arch was 58.3±11.4 mm. The types of aneurysms were 38.8% (n=240/618) from chronic dissection, 16.7% (n=103/618) degenerative, 4.6% (n=29/618) from penetrating ulcers, and the remainder unspecified. The study by Czerny et al 27 included 4 patients with bicarotid trunk that underwent bTEVAR. Four studies reported the location of entry tears, most begun at zone 2 (40.0%).
Device and Procedural Characteristics
There were 17 customized or off-the-shelf BSG studies and the remaining 2 were handmade Inoue stent grafts. Single-, double-, and triple-inner BSGs were deployed in 33.8% (n=209), 63.9% (n=395), and 2.3% (n=14) of the included 618 patients, respectively.
Table 3 provides an overview of available procedural data. The mean procedural time was 235.3±56.2 minutes. Mean fluoroscopy time was 44.0±28.0 minutes. The duration varied depending on whether LSA revascularization was conducted in the same procedure or via staged approach. Ten articles documented the type of LSA revascularization, which was conducted in 89.5% (n=274/306) patients with 45.3% (n=124/274) bypasses and 10.6% (n=29/274) transposition. The remaining was not clearly distinguished. Seven articles documented their methods of achieving blood flow reduction via rapid cardiac pacing (75.0%, n=189/252), followed by inferior vena cava occlusion (27.4%, n=69/252). Graft oversizing rate ranged from 5% to 31%. Proximal landing zone was mainly in zone 0 (57.7%, n=97/168), followed by zone 2 (41.7%, n=70/168). Only 1 case had a proximal landing zone at zone 1. 14
Procedural Details of Inner Branched Total Endovascular Repair of the Included Studies.
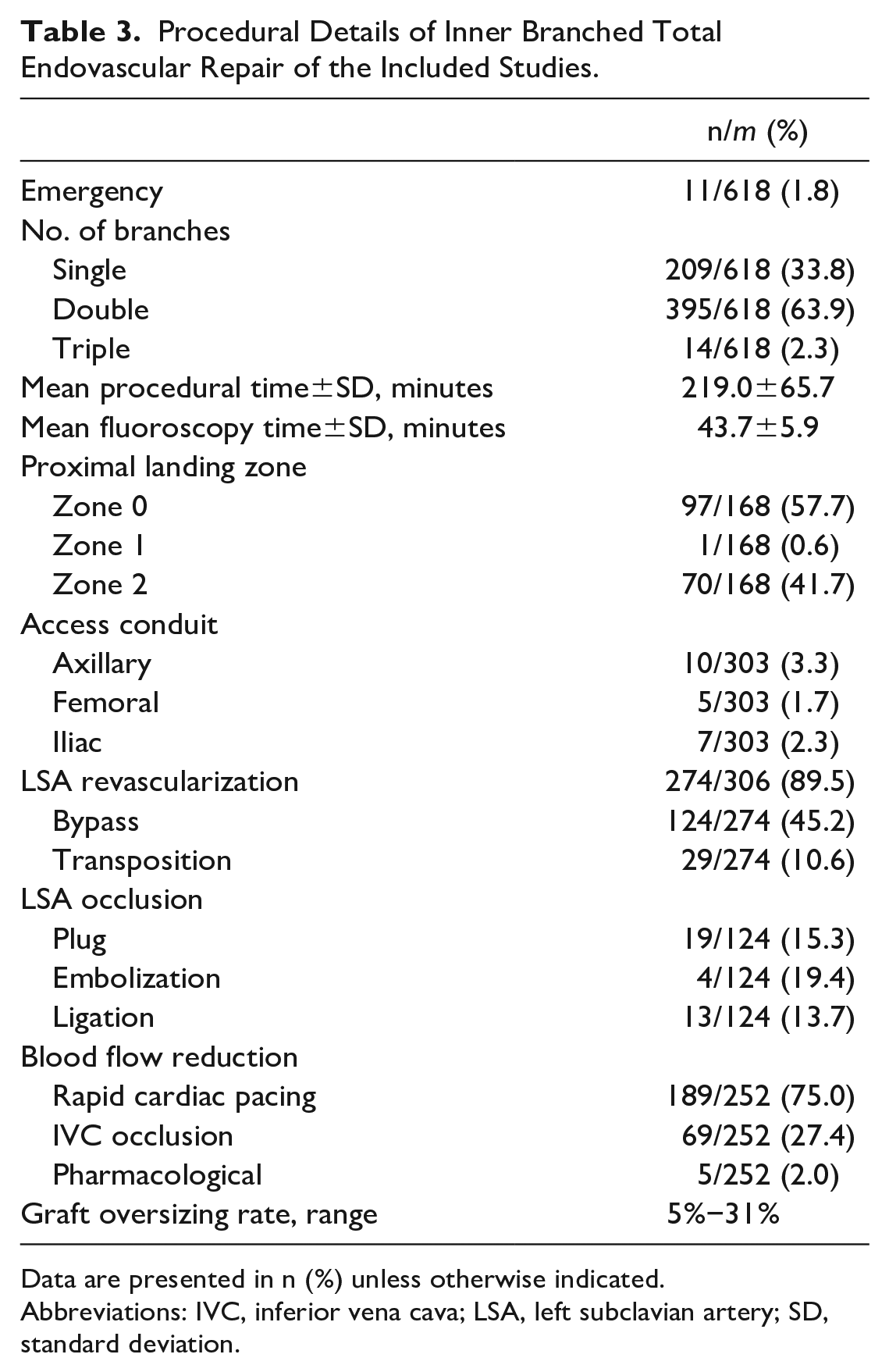
Data are presented in n (%) unless otherwise indicated.
Abbreviations: IVC, inferior vena cava; LSA, left subclavian artery; SD, standard deviation.
Early (≤30 Days) and In-Hospital Outcomes
Pooled mean technical success rate was 97.4±4.4% (95% CI=95.1%–99.5%). Three procedures required conversion to OSR for the following reasons: (1) branch entrapment in the LSA at the left thoracic outlet; (2) intraoperative aortic coarctation secondary to a severe kink of the graft; and (3) type 1A endoleak secondary to endograft oversizing and proximal infolding. There were 2 conversions to chimney due to misplacement of the endograft that made cannulation of the supra-aortic vessels impossible.
The pooled rates of perioperative complications include 3.9% (95% CI=1.4%–6.5%) type I endoleak, 1.1% (95% CI=–0.1% to 2.4%) type II endoleak, 0.3% (95% CI=–0.1% to 0.8%) type III endoleak, 10.5% (95% CI=6.8% to 14.3%) stroke, 1.6% (95% CI=–0.2% to 3.4%) retrograde type A aortic dissection, 2.2% (95% CI=0.7%–3.8%) SCI, 0.6% (95% CI=–0.2% to 1.4%) myocardial infarction, 2.8% (95% CI=1.0%–4.5%) renal injury, and 0.5% (95% CI=–0.1% to 1.2%) limb ischemia. No patient with postoperative renal injury required permanent dialysis. No patient with SCI developed permanent paraplegia and their transient paraplegia either resolved spontaneously or through cerebral spinal fluid drainage.
Early and in-hospital mortality rate was 5.5% (n=34/618; 95% CI=2.6%–9.7%). Forty patients (6.5%; 95% CI=2.5%–9.5%) required early reintervention.
Follow-Up Outcomes
The mean follow-up duration of the cohorts was 20.7±13.5 months. The pooled rates of persistent or new endoleaks was 2.9% (95% CI=1.1%–4.7%) for type I, 3.2% (95% CI=0.9%–5.7%) for type II, 0.4% (95% CI=–0.2% to 0.9%) for type III, and 1.9% (95% CI=–0.6% to 4.4%) for indeterminate types. Late stroke rates were 2.9% (95% CI=0.1%–5.7%) and late cardiac complication rate was 2.2% (95% CI=0.5%–4.0%). The reported rate of branch occlusion was 0.8% (n=4/521; 95% CI=–0.2% to 2.3%). Stent migration rate was 0.6% (n=3/521; 95% CI=–0.5% to 1.5%).
The mean maximum aneurysm diameter has decreased to 48.3 mm. Four papers reported the remodeling of the false lumen, where partial thrombosis was observed in 9.4% (n=5/53) patients and complete thrombosis in 84.9% (n=45/53) patients.
During the follow-up period, the mortality rate was 18.2% (n=108/593; 95% CI=8.6%–20.6%), where 12 (11.1%) were aortic-related. Pooled late reintervention rate was 9.6% (95% CI=4.8%–14.3%).
Single Versus Double Inner-Branched Endoprosthesis
Five studies utilized single BSGs and 12 studies on double BSGs. Comparison between the patient demographics and outcomes of single and double BSGs can be found in Table 2. No statistically significant differences were found between the single and double BSGs.
Discussion
This study provides a descriptive overview of published literature on the outcomes of TEVAR with BSGs for the management of aortic arch pathologies. Several important findings were made: (1) pooled outcomes of this study reflect a high technical success rate and low rate of perioperative mortality; (2) postoperative stroke rate is high when compared with other complications; (3) heterogeneity of patients and aortic arch pathologies, different types of BSGs used, and means of reporting preclude any attempts of meta-analyses; (4) concurrent procedures, such as LSA revascularization, blood flow reduction, use of bridging stents, may improve patient outcomes; (5) there remains a paucity of evidence to determine the feasibility of BSGs in emergent settings and a specific type of aortic arch pathology; and (6) long-term follow-up and multicenter collaboration is necessary to obtain sufficient evidence for meaningful analyses.
The main impetus for using BSGs has been to achieve anatomical reconstruction of the aortic arch with complete exclusion of the involved lesion when there is inadequate landing zone distal to the LSA. 31 However, risk of complications, such as neurological injuries, type I endoleak, and retrograde dissection remains a concern for TEVAR procedures. During graft and wire manipulation, detachment of atherosclerotic plaques in the arch can lead to consecutive embolization into carotid arteries. 32 Tsilimparis et al 23 stressed on the potentiality of air embolism-induced stroke, thereby switching to carbon dioxide preflushing of all thoracic endografts before saline flushing 33 to reduce the amount of air captured within. 34 Recent studies on selective antegrade cerebral perfusion in total arch replacement have demonstrated possible benefits in cerebral protection by regulating cerebral flow, 35 which may be implemented in TEVAR but requires further validation.
Theoretically, the risk of endoleaks is reduced in BSGs as it allows sealing within the supra-aortic trunks. In the review by Scurto et al, 12 pooled total of type I endoleaks in BSGs were lower than chimney and fenestrated techniques, yet linked to other complications, such as retrograde dissection. 36 Rapid cardiac pacing was to induce hypotension thereby permitting accurate stent-graft deployment and was found to decrease the risk of retrograde type A dissection after zone 0 hybrid aortic arch repair. 37
Studies have shown a direct correlation between the length of aorta covered and the risk of SCI or even potential paralysis. 38 Prevention is majorly achieved by cerebrospinal fluid (CSF) drainage to reduce the occurrence to a minimum by permitting swelling of the spinal cord during an ischemic insult. 39 Verscheure et al 25 performed staged procedures to promote spinal cord preconditioning and reduce the risk of SCI, which explained the higher rate of secondary procedures but was intended as part of the treatment plan. Although CSF drainage is a method to decrease paraplegia without being systematic, it carries non-negligible complications. A systematic review found that preoperative CSF drainage placement was not related to favorable outcome regarding SCI rate in endovascular thoracoabdominal aortic aneurysm repair. 40 Preoperative control of hypertension and prevention of anemia have to be considered so as to decrease the possibility of SCI.
Almost all of the included studies belonged exclusively to highly specialized centers. Despite so, many experienced surgeons emphasized a steep learning curve. In the early global experience, Haulon et al 7 found that intraoperative complications and secondary procedures were significantly higher in their first 10 patients compared with the subsequent 28. Patients in the early experience group and with an ascending aortic diameter ≥38 mm were associated with higher rates of combined early mortality and neurologic complications. Spear et al 15 observed significant decrease in overall mortality in the latter group. Ferrer et al 20 noted statistical difference with operative technique.
Several anatomical and hemodynamic studies have been conducted but conclusions differ. Milne et al 41 found that approximately 70% of patients with arch aneurysm formation after open ascending aortic replacement for type A aortic dissection anatomically suitable for double inner-branched device by Cook Medical. Benfor et al 42 found that only 47% were anatomically suitable for either the Zenith double or triple inner-branched device also manufactured by Cook Medical. A comprehensive hemodynamic analysis with the double-branched RelayPlus device was reconstructed in 2 patients by Sengupta et al, 43 which was found to have normal aortic flow patterns restored with no major risk of thrombus formation within the branches. Tricarico et al 44 compared different BSG configurations and noted that shorter an LSA BSG protrusion into the aortic lumen up to 5 mm carries a smaller risk of thrombus generation.
Certain BSG options were not included in this study but are noteworthy. For example, the Nexus system from Endospan (Herzlia, Israel), 45 SEAL stent graft (S&G Biotech Inc, Seongnam, Korea), 46 and the Valiant Mona LSA Thoracic Stent Graft system (Medtronic, Santa Rosa, Calif). 47 The first 2 were case reports, whereas the latter case series lacked follow-up data. All studies have demonstrated initial technical and treatment success with relative safety and durability. Two papers on RELAY Branched (Terumo Aortic, Inchinnan, UK) were excluded, as it did not contain enough data for analyses. However, both raised important points. First, prolonged procedural duration is unlikely to have any major effect over neurological outcomes for arch TEVAR. 48 Second, significant differences in reintervention between single-, double-, and triple-branched devices were noted during the first 30 days, 6, 12, and 24 months of the procedure. 49 Third, target vessel patency at 12 months was statistically different between branching number groups
From the interpretations above, it is certain that TEVAR with BSGs is a promising solution for aortic arch pathologies with an anticipated steep learning curve. Preoperative planning, with thorough assessment and accurate measurement of the luminal diameter, arch angulation, and proximal and distal landing lengths, is vital for a successful TEVAR. Appropriate staged procedures (eg, LSA revascularization) and prophylactic strategies toward preventing complications (eg, stroke, SCI, retrograde dissection, and endoleak) and reducing reintervention should be tailored to each patient, which is just as important as customizing a BSG. Based on anatomical studies, it may seem that a BSG with variable proximal diameter and extended distal landing zone would make it more adaptable for the general population. Utilization of patient-specific computational fluid dynamics analysis may help predict the hemodynamic outcomes of different treatment scenarios and aid endograft selection. 50
Nonetheless, this review has several limitations. This study comprises outcomes of BSGs with different number of branches, custom-made, and off-the-shelf models for different types of aortic arch pathologies. An effective comparison of outcomes regarding the number of branches, endoprosthesis design, and feasibility for a specific type of aortic arch pathology could not be conducted. Similarly, evidence supporting bTEVAR over OSR, fenestrated, chimney, or parallel TEVAR was low. Triple-branched BSGs have only been introduced recently, 51 thereby lacking sufficient evidence and may overestimate its benefits. The literature consists of a few ongoing clinical trials and results can inevitably change according to the duration of follow-up. The necessity of LSA revascularization in almost all papers makes the TEVAR procedure arguably a hybrid procedure. An assessment of selection bias would have been particularly informative, as there is an obvious heterogeneity in patient selection, emergent versus elective bTEVAR, and indication of arch repair (dissection vs. aneurysm). Surgeon factors play an important role in the efficacy of TEVAR with BSGs. It is evident from the learning curve that preliminary studies or those from small single centers may have underestimated the effectiveness of TEVAR with BSGs. This study can only serve as a descriptive overview.
Conclusion
Thoracic endovascular aortic repair with BSGs is a promising approach for aortic arch pathologies. Its use achieved satisfactory aortic remodeling with low early mortality. Stroke and endoleak remain the predominant concern. To date, the quality of evidence is limited by the clinical heterogeneity of early publications, steep learning curve, and lack of long-term follow-up data. Further studies are needed to accurately elucidate the efficacy of BSGs with regard to different design, patient, lesion, and interventional characteristics.
Supplemental Material
sj-docx-1-jet-10.1177_15266028231197395 – Supplemental material for Safety and Efficacy of Inner Branched Stent-Graft in the Treatment of Aortic Arch Disease: A Systematic Review
Supplemental material, sj-docx-1-jet-10.1177_15266028231197395 for Safety and Efficacy of Inner Branched Stent-Graft in the Treatment of Aortic Arch Disease: A Systematic Review by Kristine J. S. Kwan, Hai-Lei Li, Yiu Che Chan and Stephen W. K. Cheng in Journal of Endovascular Therapy
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.