
Abstract
Purpose:
Endovascular aortic aneurysm repair (EVAR) is the dominant treatment modality over open repair for abdominal aortic aneurysms. However, a higher rate of reinterventions remains the Achilles heel of EVAR. Although type 1A endoleak from proximal seal zone failure of EVAR remains one of the leading causes for reintervention, fenestrated branched devices suitable for proximal extension of failed EVAR are not widely available in the United States. Gore Thoracoabdominal Multibranch Endoprosthesis (TAMBE) is an off-the-shelf investigational device that provides supraceliac seal by incorporating 4 visceral and renal arteries via preloaded inner branches.
Case Report:
In this article, we describe 2 cases of type 1A endoleak from previous EVAR devices repaired using TAMBE. Both cases were performed under the Food and Drug Administration (FDA) compassionate use exemption. Considerations on the case planning and implantation techniques of TAMBE specific to previous EVAR devices are reviewed.
Conclusions:
Gore TAMBE can be utilized to repair a type 1A endoleak of a previous infrarenal EVAR device. Greater supraceliac coverage necessary for TAMBE relative to the minimal seal zone should be considered when applying this device for a type 1A endoleak.
Clinical Impact
This report demonstrates the feasibility of applying off-the-shelf TAMBE device to treat one of the most common failure modes of EVAR, type1A endoleak.
Keywords
Introduction
Endovascular aortic aneurysm repair (EVAR) has replaced open repair as the dominant treatment modality for abdominal aortic aneurysms. However, compared with open repair, EVAR is associated with higher reintervention and rupture risks at long-term follow-up.1,2 Type 1A endoleak, resulting from dilatation of the proximal aorta, loss of the infrarenal neck, or a combination of both, remains a frequent indication for reintervention. Fenestrated-branched endovascular aortic repair (FBEVAR) custom-manufactured devices (CMD) have shown excellent results for type 1A endoleak; however, they are not widely available in the United States.3–5 Gore Thoracoabdominal Multibranch Endoprosthesis (TAMBE) (W.L. Gore & Associates, Flagstaff, Arizona) is an off-the-shelf stent graft containing 4 portals or inner branches, designed to incorporate 2 visceral and 2 renal arteries (Figure 1).
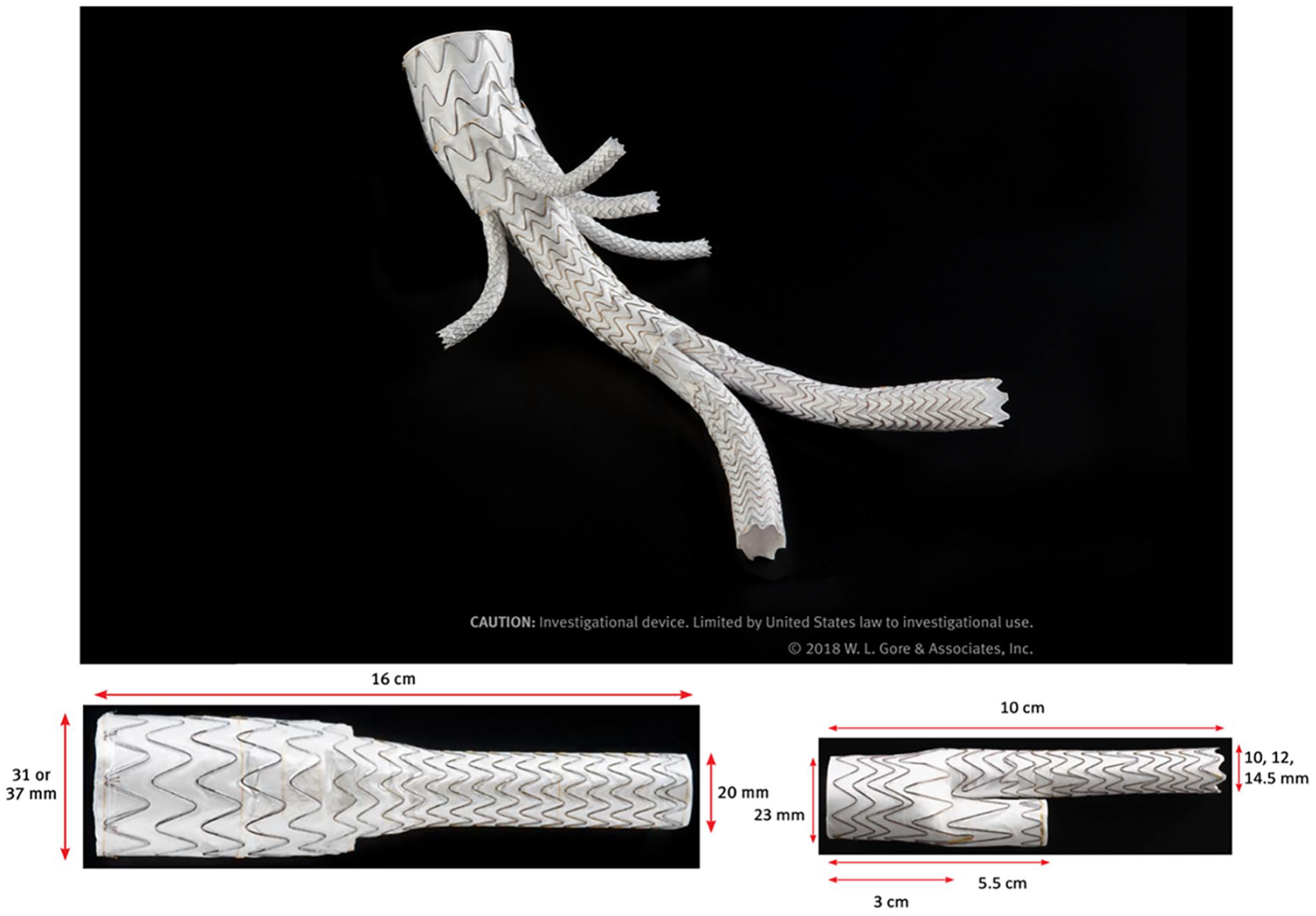
Gore TAMBE device and components with measurements of the main body and distal bifurcated component.
In this article, we describe the first 2 cases where TAMBE was used for repair of type 1A endoleaks from previous Excluder (W.L. Gore & Associates) EVAR devices. In addition to the planning and implantation considerations, we discuss the limitations of the TAMBE device when applied to type 1A endoleak repairs. This compassionate use of TAMBE device was approved by the US Food and Drug Administration for each case. Patients provided their consent for publication.
Case Report
Case 1
A 77-year-old man with a history of infrarenal EVAR 18 years prior and right internal iliac embolization with limb extension for type 1B endoleak 1 year prior presented with type 1A endoleak due to juxtarenal aortic dilatation causing aneurysm expansion (Figure 2A). The patient’s medical history included stroke, stage 3 chronic kidney disease (CKD), and hypertension. Given his age, comorbidities, and strong preference to avoid open explanation, endovascular options were explored. Centerline imaging analysis showed the supraceliac aortic seal zone and the target vessels to be of adequate diameter. Given the distance from the renal arteries to the flow divider of the previous EVAR device, 85 mm supraceliac coverage was planned to accommodate the branched and bifurcated components of TAMBE (Figure 2B). Prophylactic lumbar drain was not placed. Under general anesthesia, bilateral percutaneous femoral access and left brachial cut down were performed. With 3D fusion guidance, the preloaded branched TAMBE component was delivered with sequential branch stent placement. Celiac, superior mesenteric artery (SMA), and right and left renal arteries were bridged with appropriately sized Viabahn VBX stents (W.L. Gore & Associates). Following the full deployment of the branched main body and the visceral and renal bridging stents, the bifurcated component was deployed down to the contralateral gate, 1 cm above the flow divider of the previous EVAR device. Distal seal of the TAMBE device was achieved in the iliac limbs of the previous EVAR. Total operative time was 241 minutes, fluoroscopy time was 43 minutes, and 80 mL of contrast were required. The patient had an uneventful postoperative recovery and was discharged home on postoperative day 4. Surveillance computed tomography angiography (CTA) at 8 months showed resolution of the type 1A endoleak, patent branch stents, and stable aneurysm sac (Figure 2C).
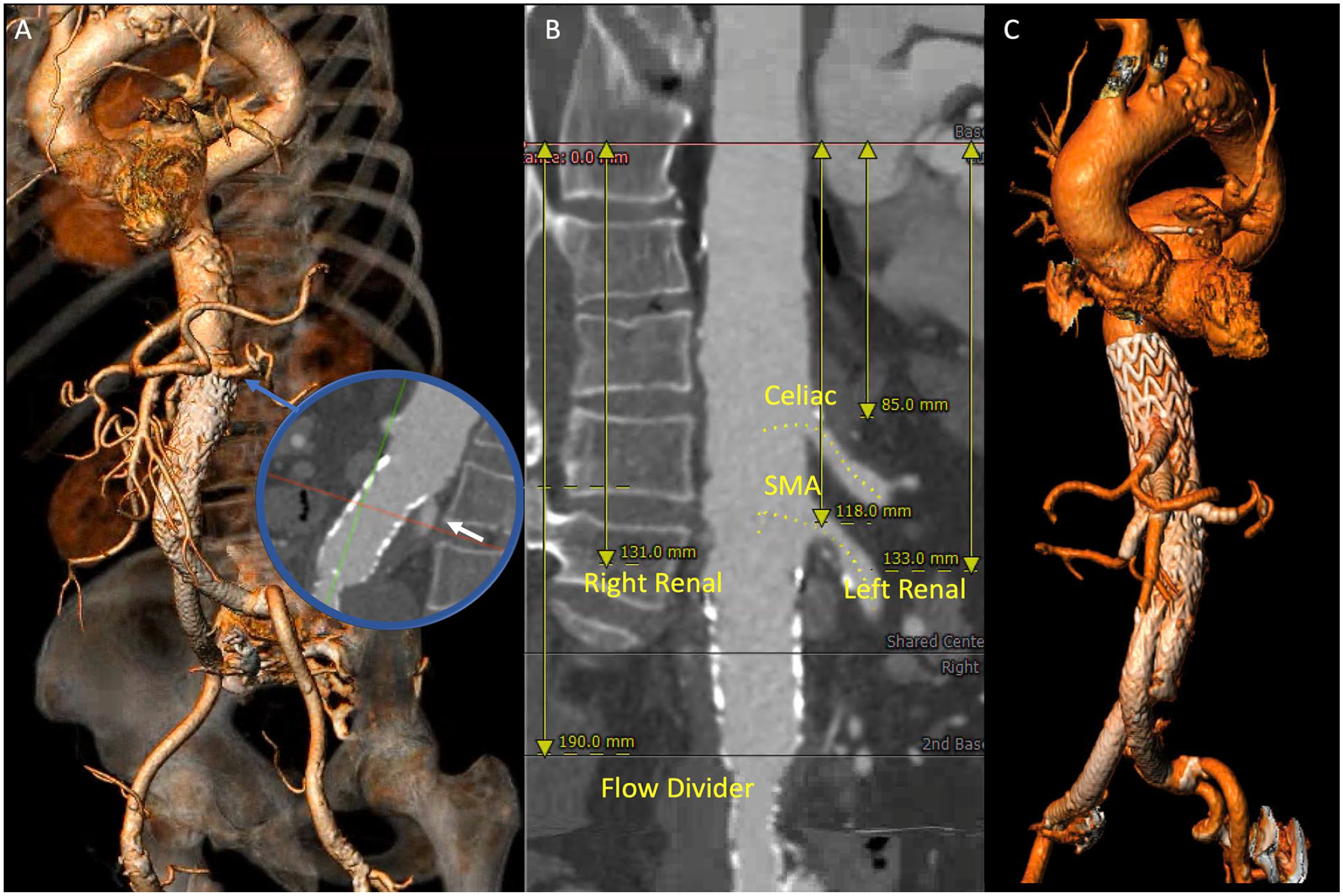
Case 1 operative planning showing (A) 3D reconstruction and type 1A endoleak 18 years after infrarenal EVAR. (B) Measurements relevant to TAMBE sizing include spacing of target arteries and flow divider of the EVAR device. (C) 3D reconstruction of the follow-up computed tomography angiography. EVAR, endovascular aortic aneurysm repair; TAMBE, thoracoabdominal multibranch endoprosthesis; SMA: superior mesenteric artery.
Case 2
A 72-year-old man underwent EVAR for infrarenal abdominal aortic aneurysm 12 years prior. Surveillance imaging revealed poor apposition of the proximal seal zone resulting in a type 1A endoleak with expansion of the aneurysm sac (4-5.5 cm in less than 2 years). He was also noted to have a 5.3 cm thoracic aortic aneurysm (TAA) at that time. His medical history was significant for coronary artery disease, hypertension, hyperlipidemia, and a 50 pack per year smoking history. The patient failed screening for enrollment in the TAMBE trial due to inadequate distal seal length in native iliac vessels. Subsequent approval for compassionate use of the TAMBE graft was obtained from W.L. Gore & Associates and the US Food and Drug Administration. A lumbar drain was placed preoperatively. Operative steps were similar to those described in case 1. The TAMBE device was implanted without any issues, and 3D fusion guidance was used to identify the location of target vessels and facilitate cannulation and stenting. Total operative time was 226 minutes, fluoroscopy time was 64 minutes, and 106 mL of contrast was used. A total of 8 cm of supraceliac aortic coverage was necessary. The lumbar drain was removed postoperative day 1, and the patient was discharged on postoperative day 3 with no issues.
Surveillance CTA at 1 month showed patent visceral stents and no evidence of a type 1A endoleak. Repeat CTA at 8 months showed sac regression to 4.4 cm, no evidence of endoleak, and patent branch stents. However, the TAA had grown to 61 mm. He subsequently underwent endovascular repair of the TAA utilizing a 36 mm × 113 mm Cook Zenith Alpha endoprosthesis (Cook Medical, Bloomington, Indiana) with preoperative lumbar drain placement. The drain was uneventfully removed on postoperative day 1, and he was discharged on postoperative day 2 with no complaints or issues. On postoperative day 18, the patient presented with acute onset bilateral lower extremity paraparesis. Magnetic resonance imaging showed signal alteration at T11/T12 concerning for spinal cord infarct. He was treated with the “COPS protocol” for delayed spinal cord ischemia including lumbar drain placement, mean arterial pressure > 90 mm Hg, and hemoglobin > 12 g/dL. 1 The patient regained full function of his lower extremities and was discharged on hospital day 5 with no residual neurologic deficits. He underwent follow-up CTA 1 month after the event that showed the TAA was excluded with no evidence of endoleak throughout 210 cm of total aortic coverage.
Discussion
The concept of open conversion as the “gold standard” for proximal failure of EVAR has been challenged with recent data showing that open conversion with partial or full stent-graft explant after failed EVAR can carry high morbidity and mortality. 6 The literature on FBEVAR for failed EVAR has demonstrated that endovascular repair is feasible and reproducible at multiple institutions with excellent outcomes.3–5,7 To this extent, the most recent European Society of Vascular Surgery guidelines recommend endovascular repair of type 1A endoleak over open repair. 8 Despite these advancements, access to CMD FBEVAR devices continues to be restricted to only a handful of centers in the United States, prompting other aortic surgeons to utilize physician-modified endografts (PMEGs) or deploy other totally endovascular or hybrid techniques for these complex cases. 9 Gore TAMBE device is the first dedicated thoracoabdominal aortic endograft that has completed the feasibility clinical trial and is now actively enrolling in the pivotal clinical trial.10,11 Type 1A endoleak from previous EVAR device resulting in insufficient distal seal zones in the native common iliac arteries is excluded from enrollment for these trials. Nevertheless, it is an important area of unmet need in the United States, where TAMBE can provide a valuable solution. Given relative prevalence of infrarenal abdominal aortic aneurysms and thoracoabdominal aortic aneurysms, and the established rates of late proximal failure after EVAR, it is conceivable that the need for endovascular solutions for failed EVAR exceeds that of de novo true thoracoabdominal aortic aneurysms.
Although we did not find the implantation of TAMBE to be significantly more challenging in these 2 cases compared with de novo aneurysms, the presence of a previous EVAR device requires additional considerations. First, the distance from the lowest renal to the flow divider of the pre-existing EVAR device must be considered to assess how high the bifurcated TAMBE aortic component will be deployed (Figure 3A). The bifurcated TAMBE component should be deployed high enough so the contralateral gate is approximately 1 cm above the flow divider to facilitate gate cannulation (Figure 3B). This, in turn, determines the placement of the branched TAMBE aortic component, which needs to be deployed high enough to preserve the distal overlap with the bifurcated aortic component (Figure 3C). This results in more supraceliac aortic coverage that may be necessary for TAMBE relative to the minimal seal zones required to repair a type 1A endoleak with other means, specifically with fenestrated CMD or PMEG devices. The associated increased risk of spinal cord ischemia, which was experienced in the second patient, should be considered. This consideration prompted a staged approach to the second patient with a concomitant TAA, who nonetheless experienced an unusual, delayed spinal cord infarct several weeks after surgery. Second, the higher deployment of the branched TAMBE aortic component may result in renal bridging stents entering the native vessels at the level of the distal aortic component overlap zone. Balloon molding of the aortic components must be done while protecting the renal branches in these situations (Figure 4). Leaving wires in the renal arteries following branch stent deployment may be a useful practice to correct any branch compression that may occur.
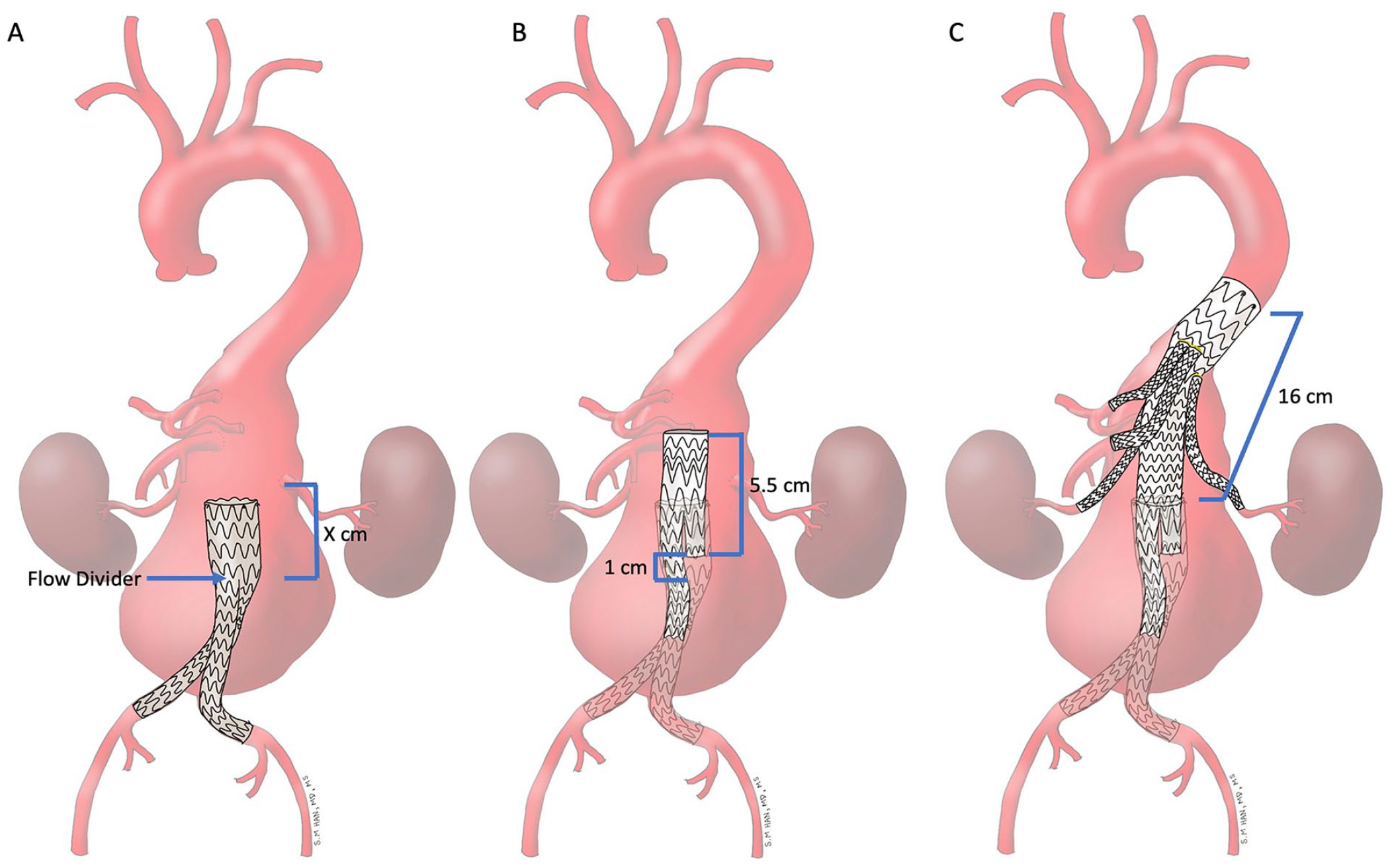
Deployment planning for TAMBE into a previous EVAR showing (A) the distance from the lowest renal to the flow divider of the pre-existing EVAR, (B) deployment of the bifurcated TAMBE component so that the contralateral gave is 1 cm above the flow divider, and (C) the branched TAMBE component deployed high enough to preserve overlap with the bifurcated component. EVAR, endovascular aortic aneurysm repair; TAMBE, thoracoabdominal multibranch endoprosthesis.
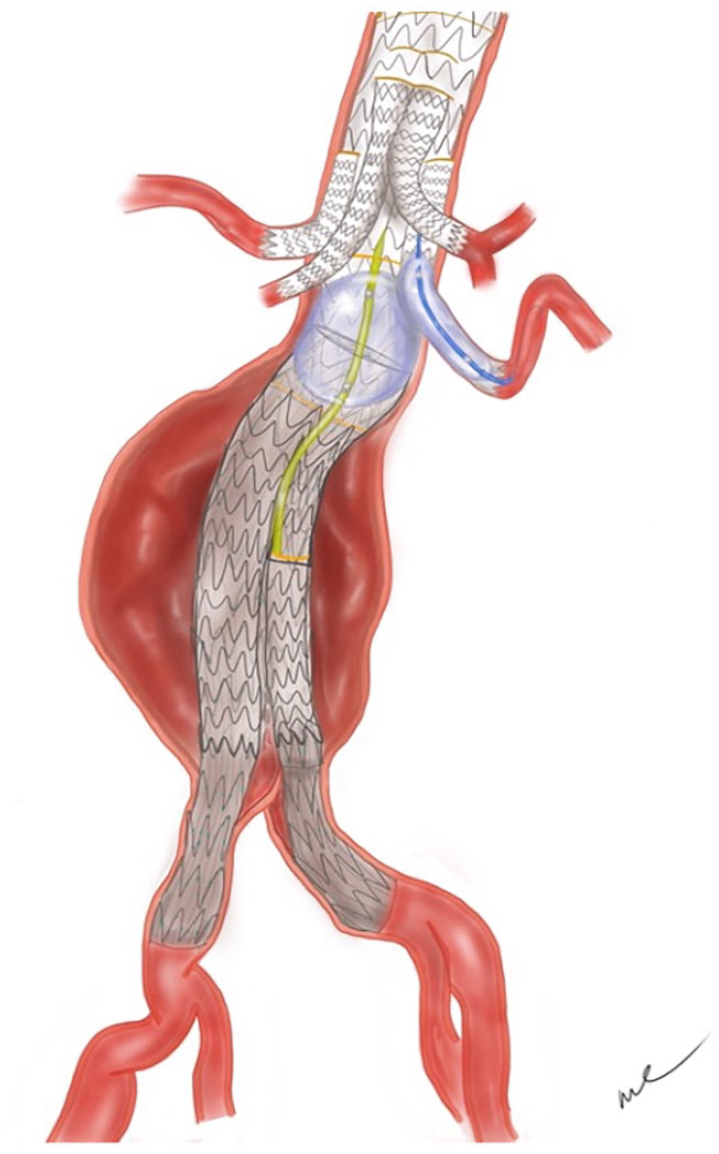
Presence of infrarenal EVAR results in higher deployment of TAMBE main body component and longer renal branches. Kissing balloon of the lower renal branch and aortic component overlap may be required. EVAR, endovascular aortic aneurysm repair; TAMBE, thoracoabdominal multibranch endoprosthesis.
Previous reports have utilized fenestrated branched cuffs with successful outcomes. 4 However, this approach is not suitable for TAMBE because of the tapered design of the branched TAMBE aortic component, which makes it difficult to utilize as an isolated cuff unless aorto-uni-iliac configuration is chosen. In addition, we felt that implantation of the entire TAMBE including its iliac limbs achieves more secure proximal and distal seal than a cuff alone. Although our cases demonstrate feasibility of TAMBE to repair a type 1A endoleak, technical success may be more difficult to reproduce in other EVAR devices that have robust suprarenal fixation systems, a short main trunk with smaller diameters, and other complex endovascular repairs including chimneys and endoanchors.
Conclusions
Gore TAMBE can be utilized to repair a type 1A endoleak of a previous infrarenal EVAR device. Greater supraceliac coverage necessary for TAMBE relative to the minimal seal zone should be considered when applying this device for a type 1A endoleak. Future iterations of the TAMBE design should take this into account.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.M.H. is a consultant for W. L. Gore & Associates, Cook Medical, Terumo Aortic, and Vestek. S.M.H. is on the scientific advisory board for W. L. Gore & Associates and Vestek. A.J.M. is a consultant for W. L. Gore & Associates.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Presentation
This work has not been presented at a scientific meeting.