
Abstract
Purpose:
Our objective was to investigate whether patients who receive anticoagulation therapy have different outcomes after endovascular aneurysm repair (EVAR) from those who do not.
Materials and Methods:
We conducted a systematic review of studies that compared outcomes of EVAR in patients who were on therapeutic anticoagulation vs those who were not. We developed and reported the review in accordance with the PRISMA guidelines with a registered protocol (CRD42022375894). The Ovid interface was used to search Medical Literature Analysis and Retrieval System Online (MEDLINE), Excerpta Medica Database (EMBASE), and Cochrane Central Register of Controlled Trials (CENTRAL) up to November 2022. The quality of studies was assessed with the Newcastle-Ottawa Scale (NOS) (maximum score=9), and the evidence was appraised with the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) framework. The hazard ratio (HR) and 95% confidence interval (CI) was the effect estimate in time-to-event meta-analyses, calculated using the inverse-variance statistical method and random-effects models.
Results:
Sixteen studies qualified for inclusion reporting a total of 35 739 individuals. Anticoagulated patients had a statistically significantly higher hazard of death (HR=1.93, 95% CI=1.03-3.63), endoleak (HR=2.13, 95% CI=1.55-2.93), reintervention (HR=1.79, 95% CI=1.27-2.52), and aneurysm sac expansion (HR=2.72, 95% CI=1.57-4.72) than patients not receiving anticoagulation therapy. The median score on the NOS was 7 (range=4-9). The certainty of evidence was very low for mortality and reintervention and low for endoleak and sac expansion.
Conclusions:
Anticoagulation is a poor prognostic factor after standard EVAR and should be considered in decision-making, consent processes, and surveillance strategies.
Clinical Impact
The number of individuals who take anticoagulation treatment has been rapidly increasing over the recent years. We aimed to investigate the effect of such treatment on outcomes after endovascular aneurysm repair (EVAR). Anticoagulated patients were found to have increased mortality, endoleak, and reintervention rates after EVAR compared to their non-anticoagulated counterparts. Anticoagulation therapy has a prognostic role in EVAR and should be considered in decision making and EVAR surveillance. Anticoagulated patients need to be informed of the higher failure rates of EVAR, and intensified surveillance strategies may need to be implemented in this patient cohort.
Introduction
Endovascular aneurysm repair (EVAR) is currently the preferred treatment method for patients with abdominal aortic aneurysm (AAA) and the standard of care according to clinical practice guidelines, with open repair being reserved for patients with specific clinical characteristics and aortic anatomies. 1 Abdominal aortic aneurysm is predominantly a disease of the elderly; thus, EVAR, being a less invasive operative procedure, confers incremental benefits in this patient cohort, which are particularly important in elderly and frail patients with an increased prevalence of cardiovascular comorbidities.2,3 Commonly, individuals with AAA take anticoagulation treatment for other clinical conditions, such as cardiac arrhythmia or thromboembolic events, which, in theory, can affect the results of EVAR. The number of individuals who take anticoagulation treatment has been rapidly increasing over the recent years, and there appears to be a shift from traditional anticoagulation agents, such as warfarin, to newer direct oral anticoagulants.4,5 The effect of such treatment on clinical outcomes after EVAR has not yet been established. Increased rates of reintervention, rupture, and aneurysm-related mortality after EVAR have cast a shadow over its long-term effectiveness and durability compared with open repair, and the increasing use of anticoagulation treatment may account for such adverse events. Confirming an association between anticoagulation use and adverse events after EVAR has important implications in clinical decision-making and surveillance strategies, eg, enhanced follow-up may be needed for this cohort of patients. We aimed to investigate whether individuals who take anticoagulation treatment at the time of or after EVAR have worse clinical outcomes than those who are not on such treatment.
Materials and Methods
Review Registration and Reporting
The objectives and methodology of the review were prespecified in a protocol, which was registered in PROSPERO (CRD42022375894). The review was developed according to principles described in the Cochrane Handbook for Systematic Reviews of Interventions. 6 Reporting of the review complied with the updated PRISMA 2020 guidelines. 7 The PRISMA 2020 checklist was generated using a Shiny App available at https://prisma.shinyapps.io/checklist/ (available upon request) and the study flow diagram using a Shiny App available at https://www.eshackathon.org/software/PRISMA2020.html.
Eligibility Criteria
Types of studies
Eligible studies reported comparative outcomes of standard EVAR in patients taking therapeutic anticoagulation vs those not on such treatment. Studies of any design were eligible, eg, retrospective or prospective cohort studies, case-control studies, cross-sectional studies, and randomized clinical trials. There was no limit in the duration of follow-up post-EVAR that studies should report to be included in the review. Owing to funding constraints, only articles published in the English language were considered. No time constraints were applied, and the entire literature was searched from the date of the first publication on EVAR. Studies published in an abstract format, ie, no full text available is available, and those with an unpublished manuscript were excluded.
Types of participants
Eligible participants had an intact or ruptured infra-renal AAA treated with standard EVAR. Endovascular aneurysm repair could be performed with any commercially available bifurcated or aorto-uni-iliac device and any type of anesthesia, ie, local, regional, or general, using percutaneous access or surgical exposure of the femoral arteries. Patients treated with complex endovascular procedures—eg, fenestrated or branched EVAR—were excluded.
Types of prognostic factor
The prognostic factor of interest is therapeutic anticoagulation at the time of EVAR or at any time during the post-EVAR follow-up. From here on, therapeutic anticoagulation is referred to as anticoagulation. Any type of anticoagulant agent or anticoagulation regime was considered including unfractionated heparin, low molecular weight heparin, pentasaccharide, vitamin K antagonist, direct thrombin inhibitor, or factor Xa inhibitor. Any indication for therapeutic dose anticoagulation was considered including, but not limited to, atrial fibrillation, mechanical cardiac valve, or venous thromboembolic disease. Comparator to therapeutic dose anticoagulation was no antithrombotic treatment, any antiplatelet regime, a combination of antiplatelet and nontherapeutic dose anticoagulation, or nontherapeutic dose anticoagulation alone.
Types of outcomes
Studies should report at least 1 primary or secondary outcome to be eligible for inclusion. Primary outcomes are all-cause mortality, AAA-related mortality, and AAA rupture. Secondary outcomes are endoleak, reintervention, and sac expansion.
Information Sources and Search Strategy
The literature search strategy was developed by the senior review author, who has experience in outreach, knowledge, and evidence search, with support from library services at our institution. Access to health care databases was via online sources of institutional library services.
MEDLINE (Medical Literature Analysis and Retrieval System Online) and EMBASE (Excerpta Medica Database) were searched using the Ovid interface. CENTRAL (Cochrane Central Register of Controlled Trials) was also searched for eligible studies. The PICO (patient, intervention, comparison, outcome) framework was used to develop the search strategies. A combination of controlled vocabulary (subject headings) and free-text terms was used to search electronic bibliographic databases. Subject headings/thesaurus trees, search operators, and search limits in each of the above databases were adapted accordingly. Search syntaxes in each of the databases are presented in Appendix 1. Electronic searches were last run on November 30, 2022. A second-level search was conducted by manually interrogating the bibliographic list of articles that qualified for inclusion in this review and previous systematic review reports on the same or a similar topic.
Study Selection and Data Collection Process
Two review authors screened each record and each report retrieved. The reviewers worked independently at each stage of the screening process. Disagreements between screeners were resolved by discussions, with the senior review author acting as an arbitrator, if necessary.
Collected data from individual studies were prespecified during the development of the review protocol. Additional relevant data identified during the data collection process were extracted and entered into a Microsoft Excel spreadsheet. Data were extracted from the main text, figures, and tables of the original publications. Data extracted from published Kaplan-Meier curves were digitalized using an open-source software (http://plotdigitizer.sourceforge.net). Two review authors extracted data from selected studies independently. Once checked for accuracy and consistency, data were subsequently transferred to the statistical computer program. Only published material was considered, and no study investigators were contacted to obtain or confirm relevant information.
Data items were grouped as follows: (1) study level data: first author, journal, year of publication, study period, country where the study was conducted, type of anticoagulant agent, and length of follow-up; (2) individual study population data: age, sex, maximum AAA diameter, number of patent lumbar arteries, and inferior mesenteric artery patency; (3) data pertaining to risk of bias assessment; and (4) outcome data, as outlined in section “Eligibility criteria.”
Study Risk of Bias Assessment and Evidence Appraisal
The quality of nonrandomized studies was assessed with the Newcastle-Ottawa Scale (NOS). 8 The tool uses a star system, with a maximum score of 9, by which studies are judged on 3 broad methodological areas: selection of the study groups, comparability of the groups, and ascertainment of the exposure or outcome of interest for case-control and cohort studies, respectively. Studies achieving less than 7 stars were arbitrarily deemed of lower methodological quality for the purposes of sensitivity analyses. The assessment was done by 2 review authors independently, and the results were then cross-checked for consistency.
The Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) framework was used to assess the certainty of the body of evidence. The GRADE approach specifies 4 levels of evidence for a given outcome, namely, high, moderate, low, and very low. A summary of findings table was generated using an online platform (https://gdt.gradepro.org/app/). 9 The GRADE assessment was performed for the primary (time-to-event) analyses.
Effect Measures and Synthesis Methods
Primary analyses were time-to-event data meta-analyses for primary and secondary outcomes using the hazard ratio (HR) and 95% confidence interval (CI) as the effect estimate. A mixture of direct (eg, from reported HR with CI) and indirect methods (eg. from survival curves incorporating numbers at risk) was used to calculate individual study log HR and its standard error (SE). An open-source software/spreadsheet was used to facilitate the estimation of HR from published summary statistics or data extracted from Kaplan-Meier curves.10,11
Secondary analyses used dichotomous data for the primary and secondary outcomes. Data synthesis of binary data was performed using the odds ratio (OR) and 95% CI as the summary statistic. Numbers of events and total numbers of patients in each group were extracted from individual studies.
Data were then inputted into the Review Manager (RevMan) computer program (Version 5.4, Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2020). Effect estimates for binary outcomes were calculated using the Mantel-Haenszel statistical method. Time-to-event data meta-analyses were conducted using the inverse-variance method. A forest plot was generated for graphical presentation of meta-analysis for each outcome.
Important between-study heterogeneity was anticipated, eg, due to different anticoagulant agents, and therefore, the random-effects method for meta-analysis was used. 12 The extent and impact of between-study heterogeneity were assessed by inspecting the forest plots and by calculating the τ 2 and the I2 statistics, respectively. Inconsistency was quantified and interpreted as previously described. 13 To explain potential sources of heterogeneity, subgroup analyses for type of anticoagulation treatment—eg, vitamin K and newer direct oral anticoagulants—were planned but not performed due to insufficient data.
Sensitivity analyses were conducted to explore the robustness of meta-analyses by excluding studies that were deemed to be of high risk of bias (score on NOS <7). Furthermore, the analyses were repeated after removing 1 study at a time to examine the impact of each study on the overall meta-analysis.
To assess risk of bias due to missing results in a synthesis arising from reporting biases, the effect by the inverse of its SE was plotted for each study. The possibility of publication bias was assessed visually evaluating the symmetry of the funnel plot. Such reporting bias assessments would be conducted for outcomes reported by at least 10 studies.
Results
Literature Search Results and Study Characteristics
Database searches retrieved 1769 reports. Sixteen studies14 –29 qualified for inclusion in quantitative syntheses. All reported comparative data on patients who were on anticoagulation therapy at the time of EVAR or during the post-EVAR follow-up vs a control group of patients who were not taking anticoagulation treatment at the time of or after the EVAR. The PRISMA flow diagram is presented in Figure 1.
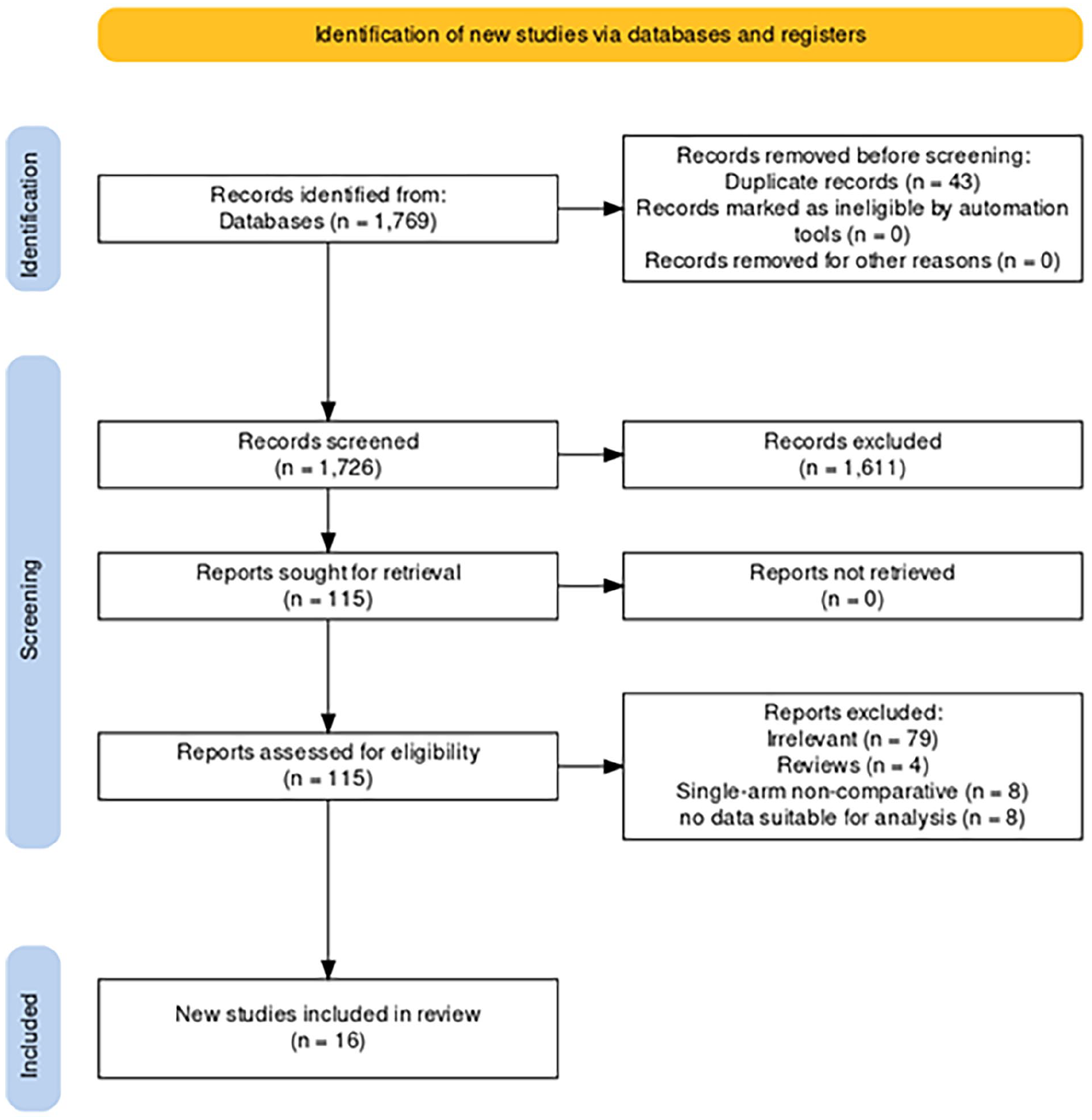
Literature flow diagram generated using a Shiny App available at https://www.eshackathon.org/software/PRISMA2020.html.
Fourteen studies14 –24,26,28,29 were observational (11 retrospective and 3 prospective) and another 2 25 , 27 reported administrative databases (from the Society for Vascular Surgery Vascular Quality Initiative). The 2 studies that used the Vascular Quality Initiative databases had overlapping populations with study periods from 2003 to 2017 and 2003 and 2019 but reported different outcomes and therefore were considered as reports of the same study for the purposes of the analysis. The studies were published between 2002 and 2022, and their recruitment period spanned from 1997 to 2019.
The studies reported a total of 35 739 patients, of whom 3180 were on anticoagulation therapy and the remaining 32 559 were not. Most studies reported use of warfarin. One study also included patients receiving low molecular weight heparin and another 2 included patients receiving direct oral anticoagulants. The mean/median follow-up ranged across the studies from 1.1 to 6.2 years. The individual study characteristics are summarized in Table 1. Most patients included in the analysis were male in their seventies. Baseline characteristics of patients are summarized in Table 2.
Characteristics of Studies Reporting Comparisons of Patients With Versus Without Anticoagulation Treatment at the Time of or After Endovascular Aneurysm Repair.
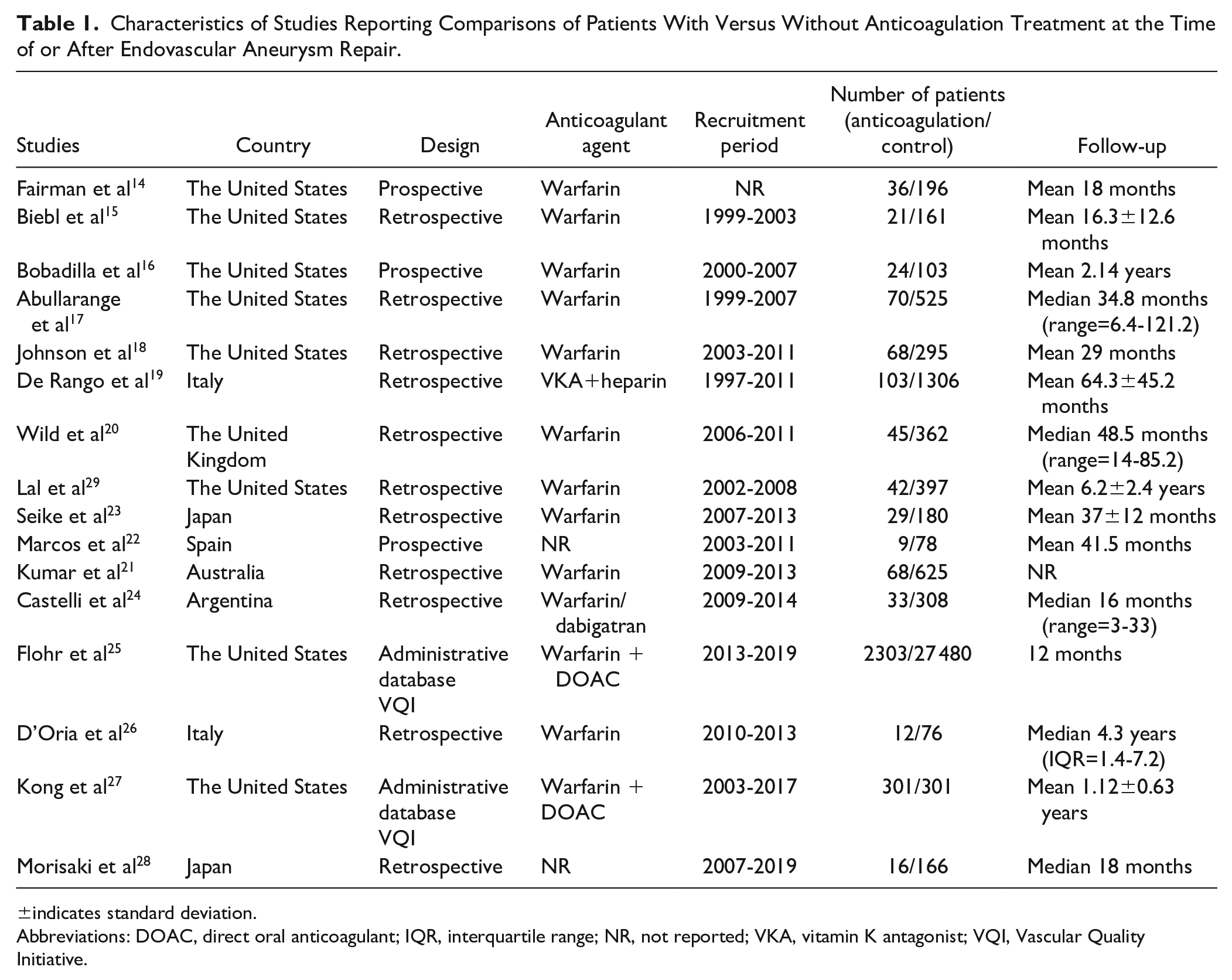
±indicates standard deviation.
Abbreviations: DOAC, direct oral anticoagulant; IQR, interquartile range; NR, not reported; VKA, vitamin K antagonist; VQI, Vascular Quality Initiative.
Patient Characteristics of Studies Reporting Comparisons of Patients With Versus Without Anticoagulation Treatment at the Time of or After Endovascular Aneurysm Repair.
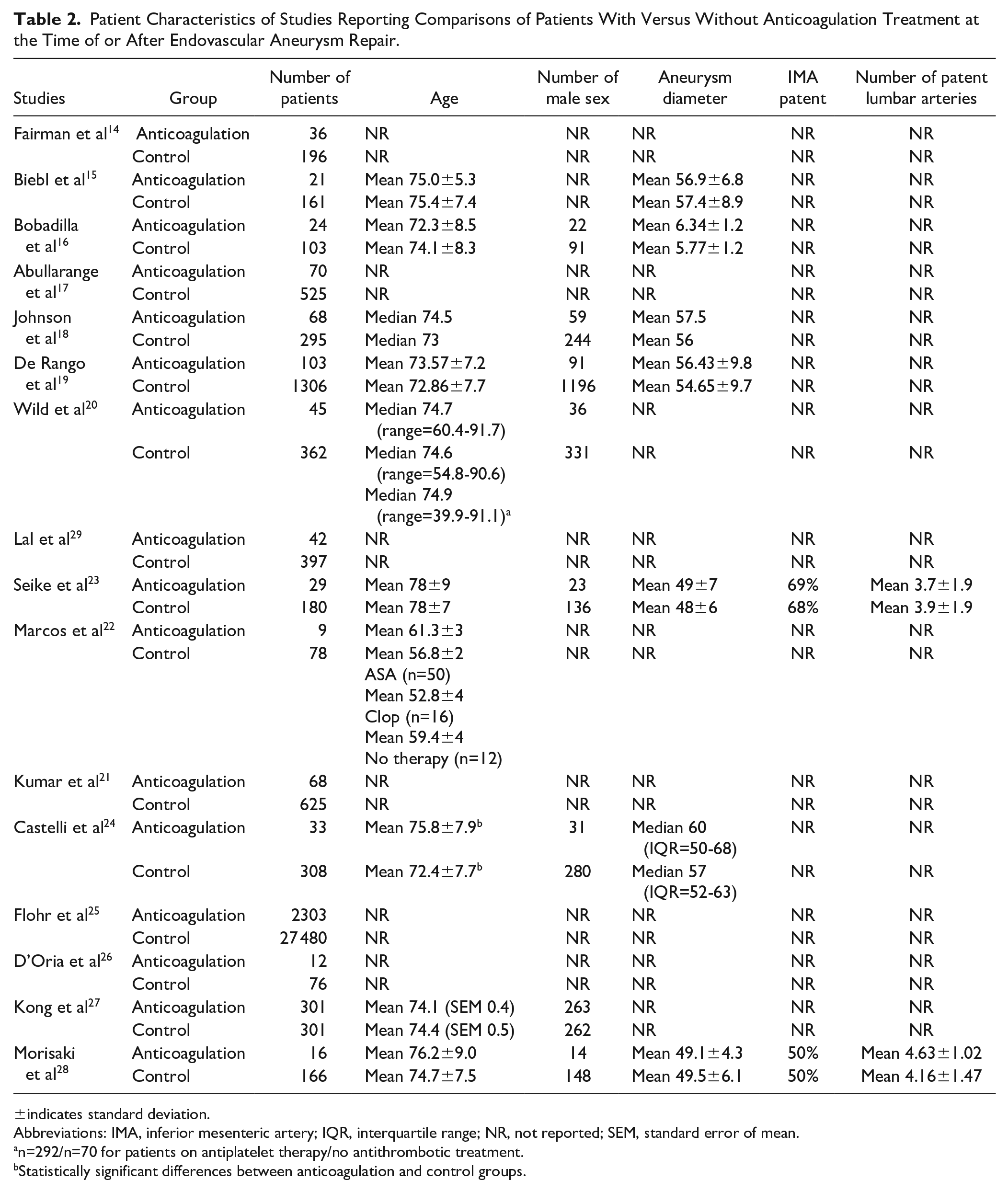
±indicates standard deviation.
Abbreviations: IMA, inferior mesenteric artery; IQR, interquartile range; NR, not reported; SEM, standard error of mean.
n=292/n=70 for patients on antiplatelet therapy/no antithrombotic treatment.
Statistically significant differences between anticoagulation and control groups.
Results of the Risk of Bias Assessment and Evidence Appraisal
The median score on the NOS was 7 (range=4-9). In general, issues were identified with comparability on the basis of the design and/or analysis and with ascertainment of exposure and assessment of outcome for case-control and cohort studies, respectively. The results of the NOS assessment are presented in Supplementary Tables 1 and 2.
The results of the GRADE assessment are presented in a summary of evidence table (Table 3). The level of evidence was very low for most time-to-event outcomes, with the exception of freedom from endoleak and freedom from sac expansion, for which the certainty of evidence was judged to be low. Downgrading of the evidence was mainly due to high risk of bias of studies, inconsistency resulting from between-study heterogeneity, and imprecision.
Summary of Findings Presenting the Certainty of Evidence Assessed With the Grading of Recommendations, Assessment, Development, and Evaluation Method.
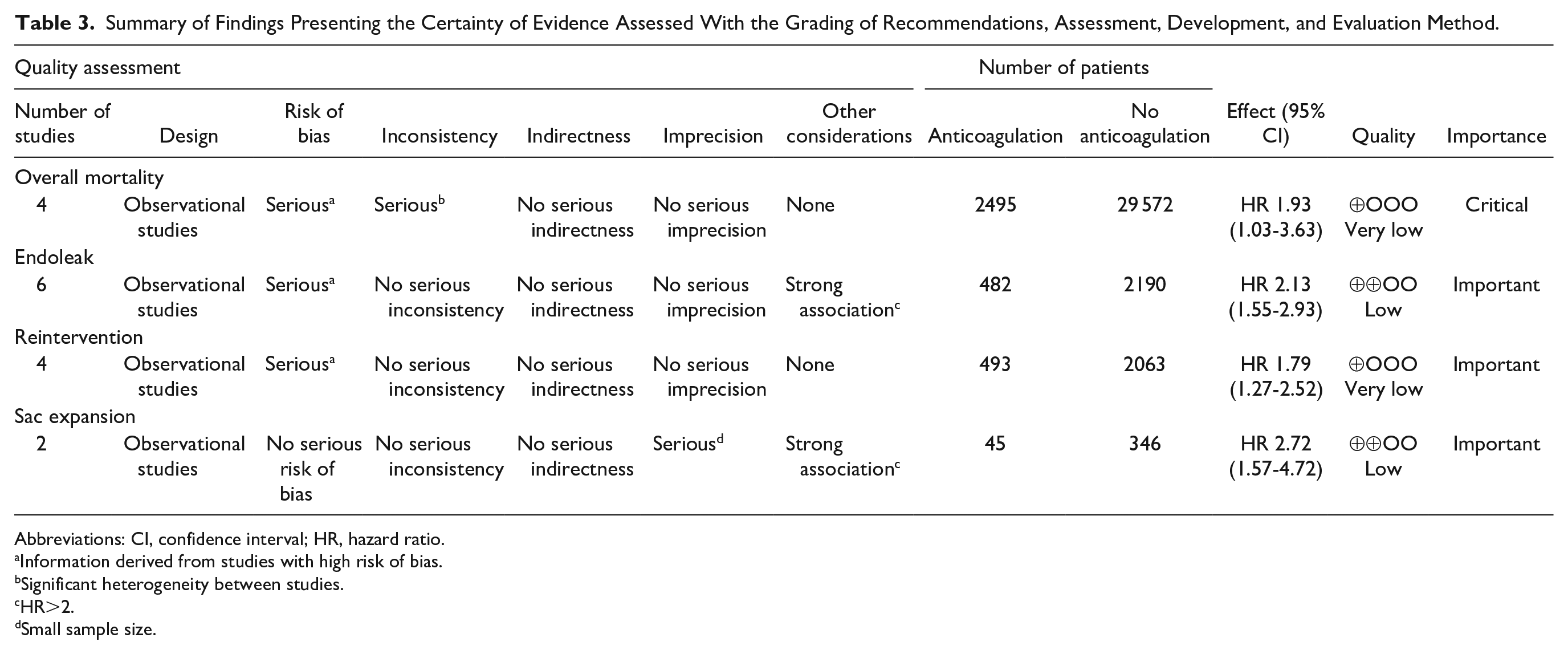
Abbreviations: CI, confidence interval; HR, hazard ratio.
Information derived from studies with high risk of bias.
Significant heterogeneity between studies.
HR>2.
Small sample size.
Results of Synthesis
Forest plots for time-to-event (primary analyses) and binary data (secondary analyses) meta-analyses are presented in Figure 2 and Supplementary Figure 1, respectively. The methods of calculation of HR and information on time-to-event outcome data are presented in Supplementary Table 3.
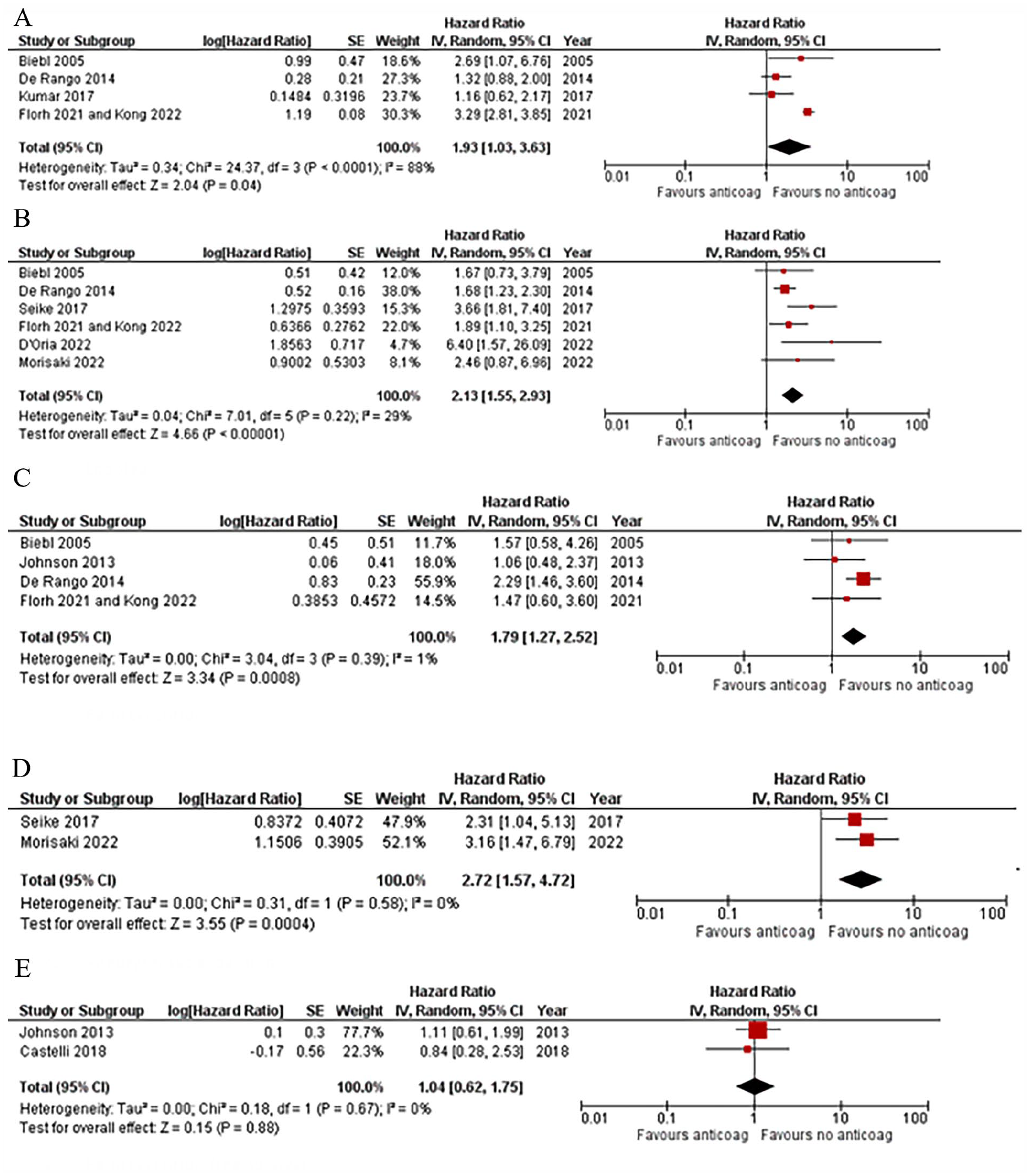
Forest plots for primary and secondary post-endovascular aneurysm repair outcomes for the comparison of anticoagulation versus no anticoagulation. The solid squares denote the hazard ratios, the horizontal lines represent the 95% confidence intervals, and the diamonds denote the pooled hazard ratios. (A) Overall mortality. (B) Endoleak. (C) Reintervention. (D) Aneurysm sac expansion. (E) Reintervention-free survival. SE, standard error; IV, inverse variance; CI, confidence interval.
Primary outcomes
Overall mortality
Time-to-event data on overall mortality were reported in 4 studies15,19,21,25,27 that included a total of 32 067 patients (2495 on anticoagulation and 29 572 controls). Patients on anticoagulation had a statistically significantly higher hazard of death at any time after the EVAR than patients not receiving anticoagulation therapy (HR=1.93, 95% CI=1.03-3.63, p=0.04). The between-study heterogeneity was considerable (p=0.0001, I2=88%). Similarly, meta-analysis of 3 studies20,22,23 reporting binary data on 1705 patients (141 on anticoagulation and 1564 controls) found statistically significantly higher odds of mortality in patients receiving anticoagulation treatment (OR=2.64, 95% CI=1.41-4.69, p=0.002; heterogeneity: p=0.92, I2=0%).
Aneurysm-related mortality
One study 24 reported comparative data on aneurysm-related mortality with no statistically significant difference between patients with and without anticoagulation (3.03% in anticoagulated patients and 2.59% in controls, p=0.44). No data suitable for meta-analysis were available.
Aneurysm rupture
No time-to-event data on aneurysm rupture were available for meta-analysis. Dichotomous data on AAA rupture could be extracted from 3 studies16,18,23 reporting a total of 699 patients (121 on anticoagulation and 578 controls). No statistically significant difference was found between patients who received anticoagulation therapy and those who did not (OR=2.25, 95% CI=0.37-13.53, p=0.38; heterogeneity: p=0.43, I2=0%).
Secondary outcomes
Endoleak
Time-to-event data on freedom from endoleak were reported by 7 studies15,19,23,25,27,28 with a total of 2672 patients (482 on anticoagulation and 2190 controls). Patients on anticoagulation had a statistically significantly higher hazard of developing endoleak than patients not receiving anticoagulation therapy (HR=2.13, 95% CI=1.55-2.93, p<0.00001) with an unimportant between-study statistical heterogeneity (p=0.22, I2=29%). Similarly, meta-analysis of 6 studies16,18,20,25 –27,29 reporting binary data on 2026 patients (492 on anticoagulation and 1534 controls) found statistically significantly higher odds of endoleak at any time in patients receiving anticoagulation treatment (OR=2.64, 95% CI=1.41-4.69, p=0.002; heterogeneity: p=0.92, I2=0%).
Binary data on early (detected within 30 days after the procedure) or perioperative endoleak were reported by 5 studies14,15,19,20,23 with a total of 2439 patients (234 on anticoagulation and 2205 controls). Patients on anticoagulation treatment had statistically significantly higher odds of early/perioperative endoleak (OR=1.55, 95% CI=1.10-2.19, p=0.01; heterogeneity: p=0.86, I2=0%).
Reintervention
Time-to-event data on freedom from reintervention were reported by 4 studies15,18,20,25,27 that included a total of 2556 patients (493 on anticoagulation and 2063 controls). Patients receiving anticoagulation therapy had a statistically significantly higher hazard of secondary intervention than patients not on anticoagulation therapy (HR=1.79, 95% CI=1.27-2.52, p=0.0008) with an unimportant between-study statistical heterogeneity (p=0.39, I2=1%).
Similarly, meta-analysis of 6 studies15,16,18,20,23,25,27 reporting binary data on 31 071 patients (2490 on anticoagulation and 28 581 controls) found statistically significantly higher odds of reintervention in patients receiving anticoagulation treatment (OR=2.06, 95% CI=1.08-3.93, p=0.03; heterogeneity: p=0.004, I2=72%). The type of reintervention was reported in 4 studies15 –17,24 with the primary cause being endoleak followed by limb-related complications, such as stenosis or occlusion. The vast majority of secondary procedures were performed by endovascular means.
Sac expansion
Time-to-event data on sac expansion were reported by 2 studies23,28 that included a total of 391 patients (45 on anticoagulation and 346 controls). Patients on anticoagulation had a statistically significantly higher hazard of developing sac expansion than those not receiving anticoagulation (HR=2.72, 95% CI=1.57-4.72, p=0.0004) with no statistical evidence of between-study heterogeneity (p=0.58, I2=0%).
Similarly, meta-analysis of 8 studies15,16,18,20,22,23,25,27 reporting binary data on 31 158 patients (2499 on anticoagulation and 28 659 controls) found statistically significantly higher odds of sac expansion in patients receiving anticoagulation treatment (OR=2.20, 95% CI=1.11-4.33, p=0.02; heterogeneity: p=0.03, I2=57%).
Additional outcomes
Persistent type II endoleak
Binary data on persistent type II endoleak were reported by 7 studies14 –17,23,25,28 including a total of 31 310 patients (2499 on anticoagulation and 28 811 controls). Definitions of “persistent” are presented in Supplementary Table 4. Patients on anticoagulation had statistically significantly higher odds of persistent endoleak (OR=2.63, 95% CI=2.35-2.95, p=0.00001; heterogeneity: p=0.46, I2=0%).
Spontaneous resolution of type II endoleak
Binary data on spontaneous resolution of type II endoleak were reported by 5 studies14 –16,19,25,27 including a total of 306 patients with type II endoleak (104 receiving anticoagulation and 202 controls). Patients on anticoagulation had lower odds of spontaneous resolution of type II endoleak without statistical significance (OR=0.50, 95% CI=0.23-1.09, p=0.08; heterogeneity: p=0.28, I2=22%).
Reintervention-free survival
Data on reintervention-free survival were reported by 2 studies18,24 with a total of 704 patients (101 on anticoagulation and 603 controls). No statistically significant difference was found between the groups (HR=1.04, 95% CI=0.62-1.75, p=0.88; heterogeneity: p=0.67, I2=0%).
Sensitivity and subgroup analyses
Sensitivity analyses excluding studies of low methodological quality (<7 stars on the NOS scale) did not affect the direction of effect for any of the outcomes, but the statistical significance was lost for overall survival (HR=2.13, 95% CI=0.87-5.19, p=0.10; heterogeneity: I2=94%, p<0.0001). Exclusion of 1 study at a time did not affect the direction of effect estimate for any of the outcomes, but the statistical significance was lost for overall survival, when the study of Biebl et al 15 was excluded (HR=1.78, 95% CI=0.83-3.78, p=0.14, heterogeneity: I2=92%, p<0.00001), and freedom from reintervention, when the study De Rango et al 19 was excluded (HR=1.31, 95% CI=0.78-2.19, p=0.30; heterogeneity: I2=0%, p=0.80). Two studies included patients with ruptured AAA (5.6% of the total cohort in the study of Flohr et al 25 and 12% in the study of Johnson et al 18 ). Exclusion of these studies in a posthoc sensitivity analysis found no change in the significance or direction of effect estimate. We were not able to do subgroup analysis for the type of anticoagulation treatment due to paucity of data.
Discussion
Meta-analysis of observational data showed that anticoagulation therapy has an important effect on clinical outcomes after standard EVAR. Primary outcomes were overall and aneurysm-related mortality and aneurysm rupture. Individuals receiving anticoagulation treatment at the time of EVAR or during the post-EVAR follow-up were found to have higher overall mortality than those not receiving such treatment. There is a paucity of data on aneurysm-related mortality, most probably due to difficulties with data capture in retrospective study designs, with only 1 study reporting pertinent information with no significant difference between groups. Similarly, limited data were identified for aneurysm rupture, the rate of which was not significantly different between groups, but the 3 studies included in this meta-analysis had a very low event rate, and therefore, the absence of difference may merely be the result of a type II error. Secondary outcomes were endoleak, reintervention, and aneurysm sac expansion. Endoleak was more common in anticoagulated patients, as was persistent type II endoleak, and patients on anticoagulation therapy were less likely to have spontaneous resolution of a type II endoleak, albeit without statistical significance. Patients receiving anticoagulation therapy were more likely to undergo secondary intervention and develop aneurysm sac expansion after the index EVAR.
The reduced survival of anticoagulated patients cannot be fully explained without considering confounding factors. Hazard estimates were calculated from survival curve data, and the exposed and nonexposed individuals were not matched in the design nor confounders were adjusted for in the analysis. Individual patient data would give further insight into potential causal associations of anticoagulation therapy and mortality. It may well be that patients receiving anticoagulation therapy may have more cardiac comorbidities putting them at higher risk of cardiovascular complications and mortality during the post-EVAR follow-up.
Although most studies failed to report detailed information on the type of endoleak, the higher rate of endoleak in anticoagulated patients is likely due to aortic side branches failing to thrombose, resulting in type II endoleak, often persisting despite secondary interventions. Of note, persistent type II endoleaks have been reported to correlate with sac expansion, secondary interventions, surgical conversion, and aneurysm rupture.30,31 As opposed to early type II endoleaks, which resolve in up to 75% of cases, late endoleaks often persist, with only a third resolving spontaneously and more than half requiring reintervention in case of sac expansion or rupture. 32
Individuals receiving anticoagulation therapy were twice as likely to require secondary intervention. Although lack of data granularity does not allow making inferences about indications and types of reinterventions, we know that such interventions are commonly performed to treat type II endoleaks which cause the aneurysm sac to expand. Such procedures are technically complex, often with suboptimal results, and require a high level of expertise and experience. A systematic review found little evidence demonstrating the efficacy of secondary interventions for such endoleaks. 33 Another systematic review found a technical failure rate as high as 28.5%. 34 The reduced overall survival in anticoagulated patients might be due to higher rates of persistent type II endoleak and reintervention, as previously shown.30,31 Unfortunately, the lack of data on aneurysm-related mortality does not allow reaching conclusions on potential causal associations between anticoagulation therapy and mortality. Similarly, a potential causal association of anticoagulation treatment and AAA rupture post-EVAR has to be investigated. The role of anticoagulation in patients with unrepaired AAA also remains controversial with some reports indicating a positive effect and some others demonstrating no effect.35,36
With the considerably larger number of studies (16 vs 5) and patients (35 739 vs 1499) than the previous meta-analysis on this topic published in 2014, our work adds to the evidence base with additional important information and implications for clinical practice. 35 We conducted additional analyses to those of the previous report, including time-to-event meta-analyses for overall survival, freedom from endoleak, freedom from reintervention, freedom from sac expansion, and endoleak-free survival. We investigated additional outcomes, such as perioperative/early endoleak, persistent type II endoleak, and spontaneous resolution of type II endoleak.
Based on our findings, anticoagulation treatment needs to be considered in decision-making processes. Furthermore, patients need to be informed of the higher failure rates of EVAR compared with their nonanticoagulated counterparts, and intensified surveillance strategies may need to be implemented in this patient cohort. Identifying anticoagulation as a prognostic factor after EVAR has additional clinical and research implications. Risk prediction modeling in EVAR should be based on clinical as well as anatomical and procedural parameters, and anticoagulation therapy should be factored into such models. 36 Risk stratification based on a multifactorial approach will inform decision-making, optimize consenting processes, and help develop risk-informed surveillance strategies.37,38 Anticoagulation should be considered alongside other parameters that have been described as risk factors for developing type II endoleak, such as number and size of patent lumbar arteries, patency, and size of the inferior mesenteric artery. In the presence of such factors, concomitant use of anticoagulants may have an additive effect, putting patients at risk for developing adverse events. 39
Our findings should be viewed and interpreted in the context of limitations. Meta-analyses are limited by the retrospective observational study design. The low event rate for several of the investigated outcomes suggests that such events may be under-reported and not representative of real-world practice. Most studies were judged to be of low methodological quality. As a result, the level of evidence was downgraded, increasing the uncertainty about the findings and not allowing safe clinical translation and transfer to clinical practices. The level of evidence was also downgraded due to heterogeneity in patient characteristics and anticoagulation regimes, as well as due to inconsistency in outcome reporting and definition, and was judged to be very low or low for all outcomes. Critical and important outcomes, such as aneurysm-related mortality and aneurysm rupture, were not reported or reported by a limited number of studies, resulting in imprecision and limiting the power of statistical analyses. Paucity of data did not allow subgroup analyses for type of anticoagulation agent; thus, effects of different anticoagulation agents or regimes on post-EVAR outcomes were not investigated. Most studies examined patients on warfarin. With the increasing use of the newer direct oral anticoagulant agents, the study cohorts included in our meta-analysis may not be representative of the overall anticoagulated population, resulting in diminished external validity of our findings. Furthermore, lack of data did not allow subgroup analyses of patients receiving a combination of antiplatelet and anticoagulation therapy vs those on anticoagulation therapy alone.
Conclusions
Anticoagulation may be a poor prognostic factor after standard EVAR. Patients receiving anticoagulation treatment may have worse clinical outcomes than those not receiving such treatment, as indicated by the increased mortality, endoleak, and reintervention rates. Our results have important clinical implications in decision-making and patient consenting. Intensified post-EVAR follow-up should be considered in this patient cohort. Anticoagulation should be included in research on risk prediction building and modeling. The effects of direct oral anticoagulants compared with other anticoagulant agents should also be the focus of future research.
Supplemental Material
sj-docx-1-jet-10.1177_15266028231214761 – Supplemental material for Systematic Review and Meta-Analysis of the Effect of Anticoagulation on Outcomes After Endovascular Aneurysm Repair
Supplemental material, sj-docx-1-jet-10.1177_15266028231214761 for Systematic Review and Meta-Analysis of the Effect of Anticoagulation on Outcomes After Endovascular Aneurysm Repair by Nikolaos Kontopodis, Nikolaos Galanakis, Christos V. Ioannou and George A. Antoniou in Journal of Endovascular Therapy
Supplemental Material
sj-docx-2-jet-10.1177_15266028231214761 – Supplemental material for Systematic Review and Meta-Analysis of the Effect of Anticoagulation on Outcomes After Endovascular Aneurysm Repair
Supplemental material, sj-docx-2-jet-10.1177_15266028231214761 for Systematic Review and Meta-Analysis of the Effect of Anticoagulation on Outcomes After Endovascular Aneurysm Repair by Nikolaos Kontopodis, Nikolaos Galanakis, Christos V. Ioannou and George A. Antoniou in Journal of Endovascular Therapy
Supplemental Material
sj-docx-3-jet-10.1177_15266028231214761 – Supplemental material for Systematic Review and Meta-Analysis of the Effect of Anticoagulation on Outcomes After Endovascular Aneurysm Repair
Supplemental material, sj-docx-3-jet-10.1177_15266028231214761 for Systematic Review and Meta-Analysis of the Effect of Anticoagulation on Outcomes After Endovascular Aneurysm Repair by Nikolaos Kontopodis, Nikolaos Galanakis, Christos V. Ioannou and George A. Antoniou in Journal of Endovascular Therapy
Supplemental Material
sj-docx-4-jet-10.1177_15266028231214761 – Supplemental material for Systematic Review and Meta-Analysis of the Effect of Anticoagulation on Outcomes After Endovascular Aneurysm Repair
Supplemental material, sj-docx-4-jet-10.1177_15266028231214761 for Systematic Review and Meta-Analysis of the Effect of Anticoagulation on Outcomes After Endovascular Aneurysm Repair by Nikolaos Kontopodis, Nikolaos Galanakis, Christos V. Ioannou and George A. Antoniou in Journal of Endovascular Therapy
Supplemental Material
sj-docx-5-jet-10.1177_15266028231214761 – Supplemental material for Systematic Review and Meta-Analysis of the Effect of Anticoagulation on Outcomes After Endovascular Aneurysm Repair
Supplemental material, sj-docx-5-jet-10.1177_15266028231214761 for Systematic Review and Meta-Analysis of the Effect of Anticoagulation on Outcomes After Endovascular Aneurysm Repair by Nikolaos Kontopodis, Nikolaos Galanakis, Christos V. Ioannou and George A. Antoniou in Journal of Endovascular Therapy
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: G.A.A. has received fees from GE Healthcare for providing educational support. The rest of the review authors have no competing interests to disclose or any relationships that could be perceived as conflict of interest for the conduct of this review.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of Data,Code,and Other Material
A list of studies that were excluded from this review with reasons, template data collection forms, data extracted from included studies, data used for all analyses, analytical code, and the PRISMA 2020 checklist can be obtained by the corresponding author upon request. Such data are not publicly available.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.