
Abstract
Clinical Impact
We developed a novel Endovascular aortic repair technique for internal iliac artery preservation using a physician modified Endurant contralateral limb. This procedure was safe and reliable for preserving internal iliac artery flow in 24 patients with common and internal iliac artery aneurysms. We believe that our technique has the potential to expand the anatomic indications for internal iliac artery preserving procedures.
Keywords
Introduction
The incidence of buttock claudication associated with the embolization of the internal iliac artery (IIA) is relatively high (26%-41%), while rectal ischemia (1%-3%), and gonadal dysfunction (3.3%-10.2%) are also associated problems; however, these incidences are low.1,2 Hence, when endovascular aortic repair (EVAR) became a more popular technique performed for abdominal aortic aneurysms (AAAs) with common iliac artery aneurysms (CIAAs) and/or internal iliac artery aneurysms (IIAAs), methods of internal artery preservation was highlighted as an important focus area. To preserve the IIA flow, the Gore Excluder Iliac Branch Endoprosthesis ([IBE]; W.L. Gore & Associates, Flagstaff, Arizona),1,3 –5 the Zenith Branch Endovascular Iliac Bifurcation Graft, 6 or E-liac™ STENT GRAFT SYSTEM 7 are usually used for AAA cases with CIAAs, and there have been several reports on its safety, efficacy, and durability. However, the Excluder IBE has anatomic constraints. Many Japanese patients do not fit within the recommended instructions for use, particularly in terms of arterial length. Moreover, the Zenith Branch Endovascular Iliac Bifurcation Graft and the E-liac™ STENT GRAFT SYSTEM cannot be used in Japan. Therefore, in August 2019, we developed a novel technique using a physician-made fenestrated Endurant contralateral limb (Medtronic, Minneapolis, MN, USA) for IIA preservation. Herein, we describe the details on how to create and use a physician-modified fenestrated Endurant contralateral limb.
Technique
Fenestration for IIA preservation was performed using the Endurant contralateral iliac limb (Medtronic, Minneapolis, MN, USA). Typically, an 82-mm length of Endurant contralateral limb is used for physician-modified fenestrated limbs. An appropriately sized distal limb was selected considering the diameter of the patient’s external iliac artery (EIA). The central 3-stent portion of the limb was used as a junction, and a fenestration was created at the distal portion of the taper and distal to the first stent from the central 3-stent segment. The position of fenestration should be in the taper area to ensure a working space outside the limb. At the end of the limb, at least two stents were reserved for the landing zone in the EIA (Figure 1A). A small battery-powered scalpel (Accu-Temp® Cautery Variable Low Temperature Cautery—Dial Controlled; Beaver Visitec, Massachusetts, USA), commonly used to achieve hemostasis in ophthalmic surgery, was used to melt the polyester between the stents and to create a hole of approximately 4 to 5 mm (Figure 1B). An AZUR detachable 18 HydroCoil, 6 mm/20 cm (Terumo Co., Tokyo, Japan) was triple rolled onto a 5-mm neraton catheter, and it was sutured with 12 single stitches of 5-0 monofilament at the previously created hole. It was used to reinforce the fenestration, while hydrogel was used as the sealing material for the bridging device using the method illustrated by Azuma et al 8 (Figure 1C). The coil itself is an adequate marker of the fenestration position. Hence, we did not add any other markers.
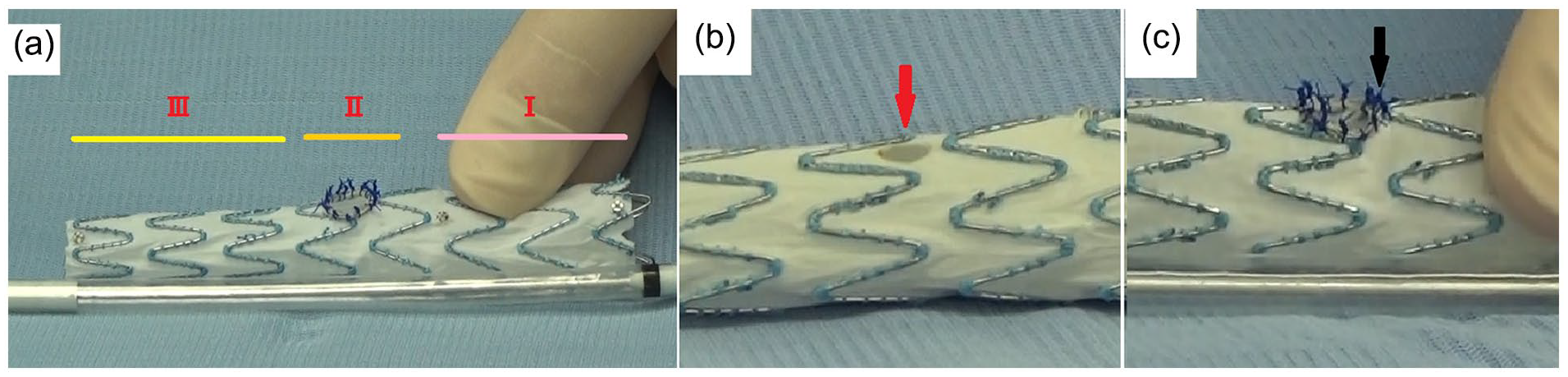
Details of the modified Endurant contralateral limb. (A) Location of the central junction (I), fenestration site (graft tapered position) (II), and distal landing zone (III). (B) Fenestration (red arrow). (C) Reinforced fenestration using an AZUR detachable 18 HydroCoil.
A wire preload system was also developed to deliver the sheath from the contralateral side to the fenestration site. First, the modified limb fully unsheathed to pass the preloaded wire, and a small battery-powered scalpel was used to create a small hole in the sheath of the delivery system through which the wire could pass. Next, a Radifocus guidewire (diameter: 0.025-in, length: 260 cm; Terumo Co., Tokyo, Japan) was threaded through the hole in the sheath. The guidewire was then passed through the fenestration portion of the modified limb (Figure 2A). The modified limb and preloaded wire were re-sheathed into the delivery system (Figure 2B). The modified graft can be re-sheathed by wrapping the graft with silk thread to reduce the diameter. The preloaded wire was snared from the contralateral side to deliver a bridging graft in the IIA. We believe that this detail is better understood by watching Supplemental Video 1. We prepared the modified graft either during the induction of anesthesia or while performing embolization of side branches, such as the inferior mesenteric artery and/or lumbar artery. The average time required to prepare one modified graft typically ranges from 15 to 20 minutes.
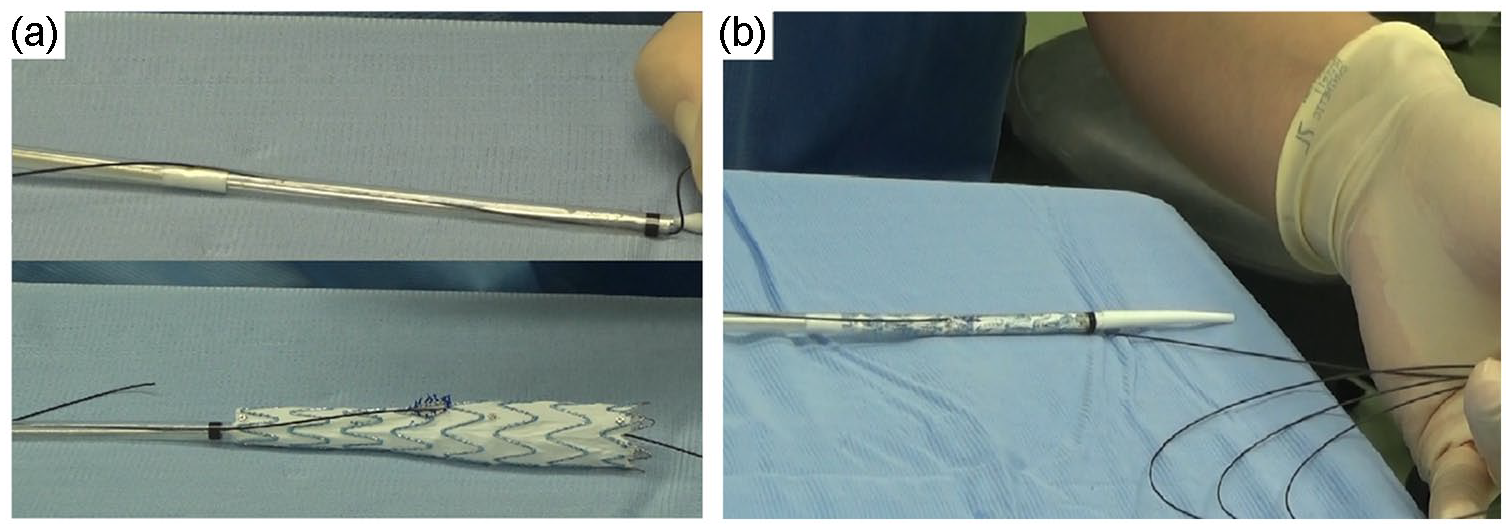
The pull-through system for contralateral sheath delivery. (A) A pull-through wire passes through the sheath of the delivery system and limb fenestration. (B) Overall image of the modified Endurant contralateral limb.
A DrySeal sheath (W.L. Gore & Associates, Flagstaff, Arizona) was inserted through the femoral artery at the site of the modified limb insertion. This technique was chosen because the hemostatic valve of the DrySeal sheath performs extremely well when the delivery system and 0.025-in Radifocus guidewire are inserted simultaneously, and the tip of the Endurant delivery sheath may become frayed during resheathing. Next, a 0.025-in Radifocus guidewire was inserted and snared from the contralateral side, and the fenestration portion of the modified limb was delivered in the direction of the IIA bifurcation. The 0.025-in Radifocus guidewire was inserted using an inserter that could be peeled away. The rationale for using 0.025-inch diameter wire is to allow the space needed for the catheter to perform IIA cannulation within the delivery sheath. In addition, if the wire is thinner than 0.025-in, snare manipulation becomes more difficult. The Endurant contralateral limb device was adjusted to align the fenestration with the IIA bifurcation, and the limb was opened to the fenestration. A destination sheath (Terumo Co., Tokyo, Japan) matching the requirement of the Viabahn VBX endoprosthesis (W.L. Gore & Associates, Flagstaff, Arizona) was delivered from the contralateral side to the limb using an above-mentioned 0.025-in Radifocus guidewire. Tugging the 0.025-in Radifocus guidewire, which facilitates the delivery of the destination sheath into the limb. A 5-Fr catheter with 0.035-in Radifocus guidewire was inserted through the side of the 0.025-in wire, into the destination sheath and cannulated into the IIA through the fenestration. The 5-Fr catheter was delivered as deep as possible into the IIA branch, and the 0.035-in Radifocus guidewire was changed to an Amplatz Super Stiff™ Guidewire (Boston Scientific, Natick, MA, USA). The preloaded 0.025-in Radifocus guidewire was removed, the destination sheath was delivered to the IIA, and the Viabahn VBX endoprosthesis was implanted in the IIA or IIA branch. In cases involving an IIAA, the branches of the IIA were embolized to pre-emptively prevent a type II endoleak before implanting the Viabahn VBX. This step was facilitated by the robust and dependable support provided by the catheter during the embolization of the IIA branches. The Viabahn VBX is left inside the modified Endurant contralateral limb about 1.5 stents’ length (approximately 7-9 mm). The aim of this is to avoid pulling out the reinforced fenestration of the Viabahn VBX and to avoid impeding the passage of the devices. When the diameter of the common iliac artery (CIA) at the IIA bifurcation was <16 mm, the kissing balloon technique was performed at the Viabahn VBX endoprosthesis and Endurant contralateral limb. Considering that the proximal diameter of the Endurant contralateral limb is 16 mm, if the IIA bifurcation is <16 mm, the limb does not fully expand, and it reduces the space in the limb. Consequently, it impedes the passage of the devices. Finally, EVAR was completed by connecting the central main device and modified limb using the contralateral legs. These procedures are demonstrated in Figure 3 and Supplemental Video 2.
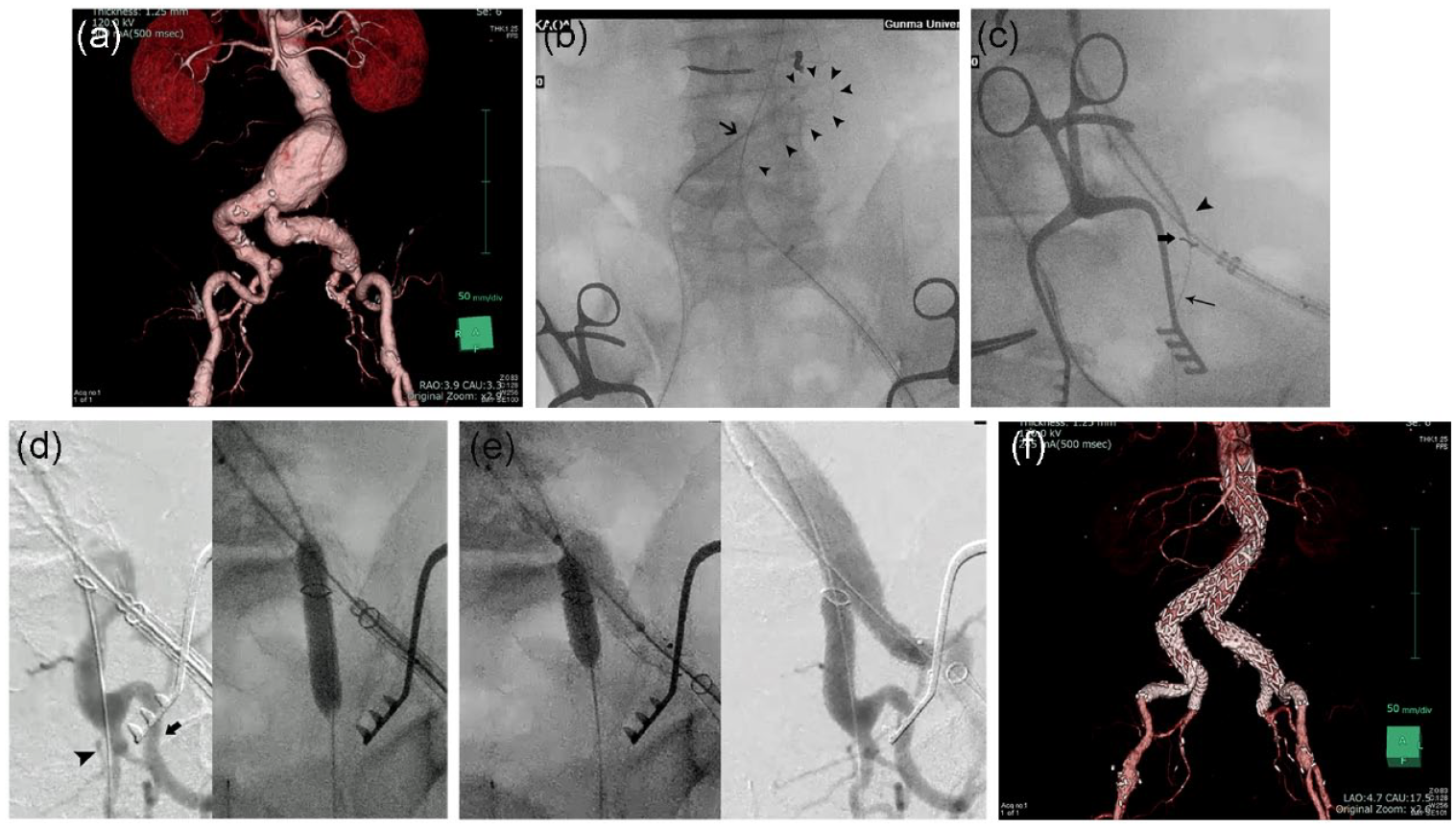
Intraoperative fluoroscopy images of the procedure and preoperative and postoperative 3D image of computed tomography (CT). (A) 3D image of preoperative CT. (B) Catch the preloaded 0.025-in Radifocus guidewire by snare catheter from contralateral side; arrow: snare catheter; arrowhead: 0.025-in Radifocus guidewire. (C) After tugging of 0.025-in Radifocus guidewire, destination sheath was delivered into the limb and 5-Fr catheter with 0.035-in Radifocus guidewire cannulate into internal iliac artery aneurysm IIA; thin arrow: 0.035-in Radifocus guidewire in internal iliac artery; thick arrow: the tip of 5-Fr catheter; arrowhead: the tip of destination sheath. (D) contrast images of internal iliac artery and its branches (left) and Viabahn VBX deployment (right); Arrowhead: inferior gluteal artery; Arrow: superior gluteal artery. (E) Kissing balloon technique (left) and final contrast image of internal iliac artery preservation. (F) 3D image of preoperative CT.
Results
We used this new technique in 24 patients from August 2019 to December 2020 in our institution. The follow-up time was 1 year in all cases in this study. This study was approved by the appropriate Institutional Review Board, and informed consent was obtained from all patients for our procedure and surgery. All patients were diagnosed using computed tomography (CT). Patients with prior EVAR, aneurysm rupture, and infectious aneurysm were excluded. We checked the technical success rates, patency rates of the bridging branch and Endurant contralateral limb, IIA ischemic events, and endoleaks. The technical success rate in this study was defined as successful deployment of the endoluminal graft with secure proximal and distal fixation, absence of either type I or III endoleak, a patent endoluminal graft without significant twist, kinks, or obstruction by intraoperative measurements, 9 and patency of preserved branches. Complications were checked using CT performed at 1 week, 6 months, and 1 year after surgery in all patients.
Table 1 shows the patient and aneurysm characteristics. Among them, the number of patients with AAA + CIAA, patients with AAA + CIAA + IIAA and with AAA + IIAA was 10, 7, and 2, respectively. Table 2 shows the details of the surgical procedures. In 24 patients, 31 branch preservations were performed (7 cases were bilateral preservations). Table 3 shows the details of the outcomes during follow-up. The technical success rate was 100%. The patency rates of both the IIA branch and Endurant contralateral limb were 100% at 1 year. There were no IIA ischemic events or type Ib or type III endoleaks or occlusions associated with the fenestrated limb and branched graft.
Clinical Characteristics of the Patients and Characteristics of Aneurysms.
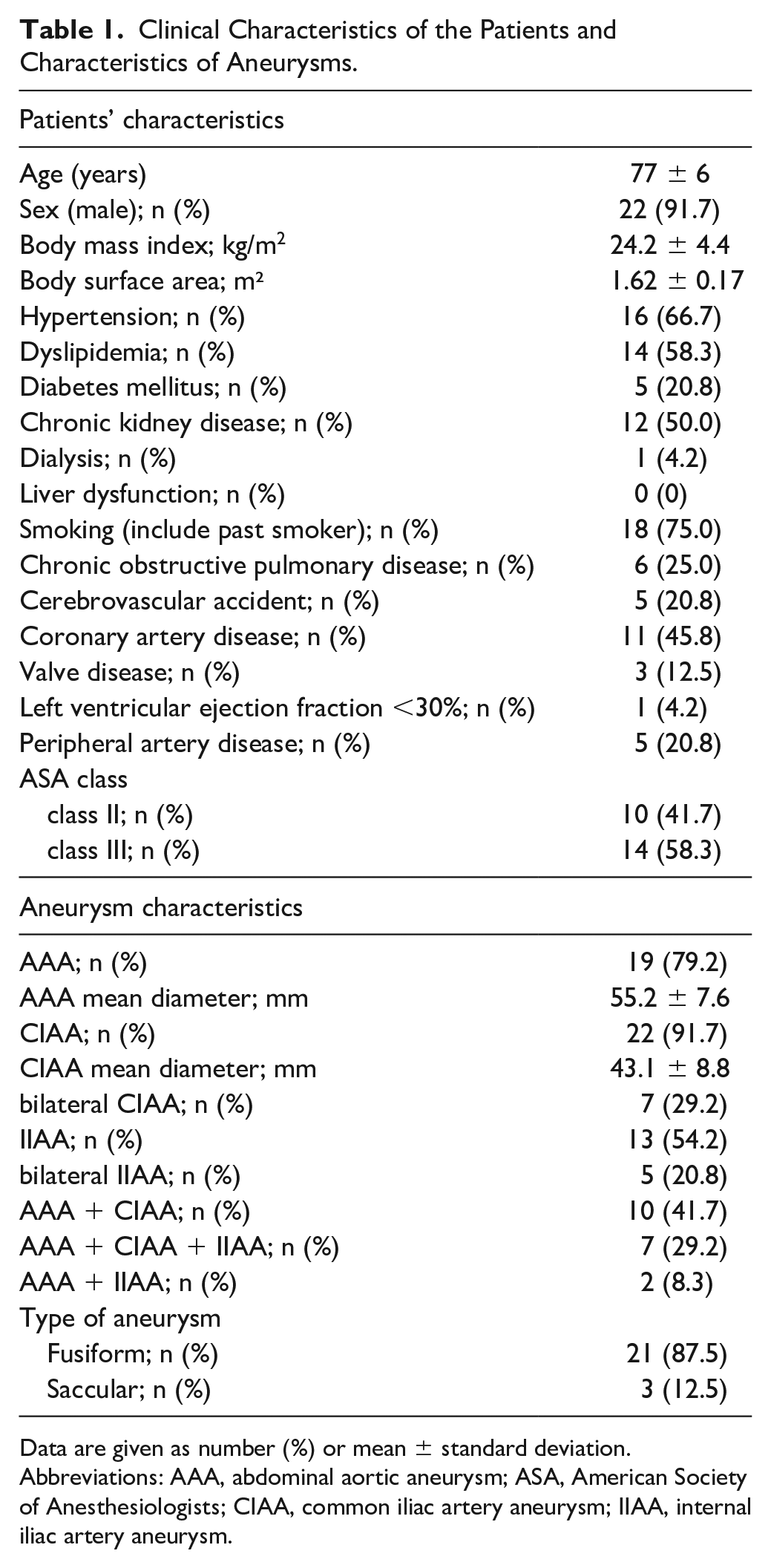
Data are given as number (%) or mean ± standard deviation.
Abbreviations: AAA, abdominal aortic aneurysm; ASA, American Society of Anesthesiologists; CIAA, common iliac artery aneurysm; IIAA, internal iliac artery aneurysm.
Details of the Surgical Procedure.
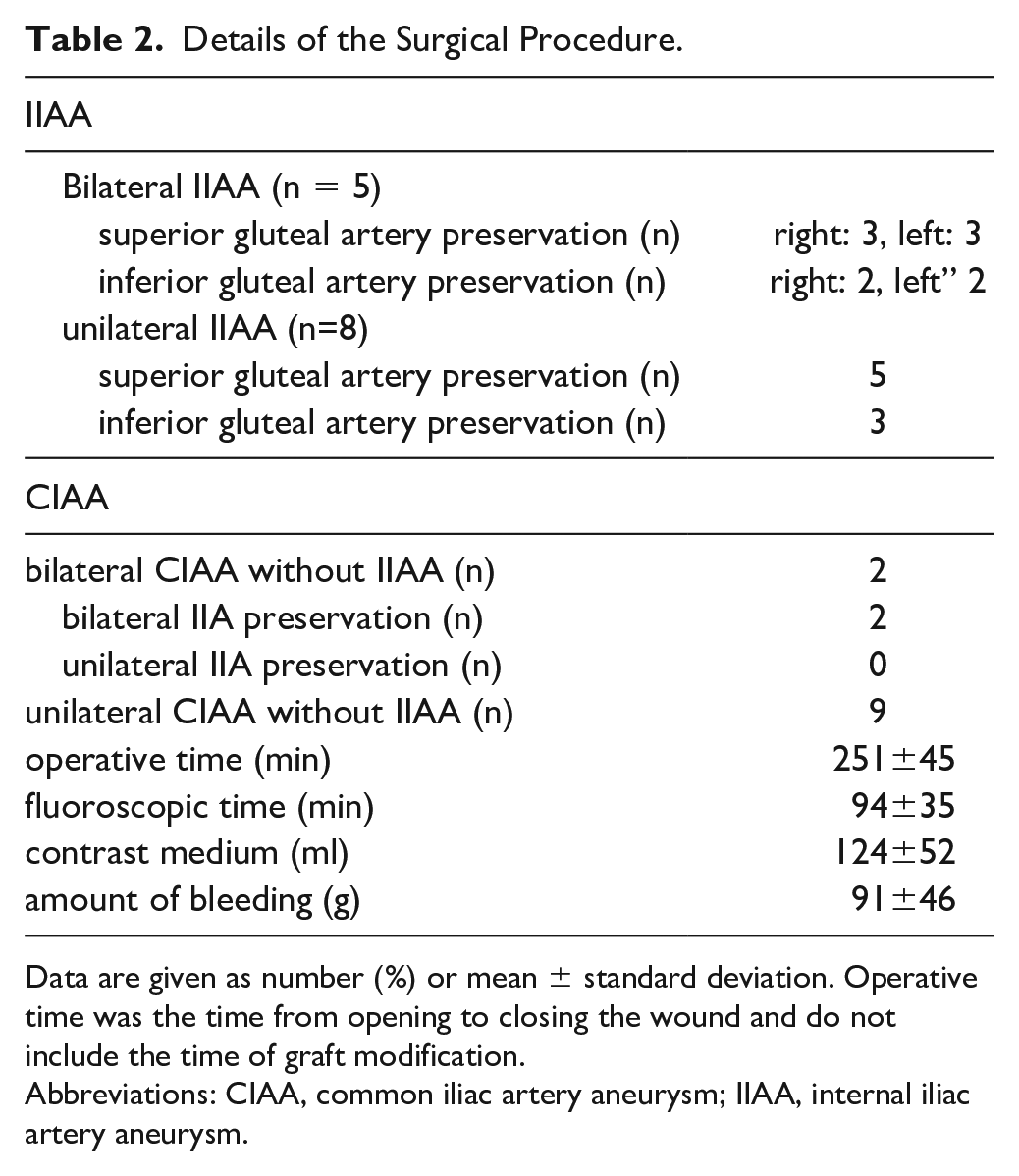
Data are given as number (%) or mean ± standard deviation. Operative time was the time from opening to closing the wound and do not include the time of graft modification.
Abbreviations: CIAA, common iliac artery aneurysm; IIAA, internal iliac artery aneurysm.
The Details of Postoperative Outcomes During Follow-up.
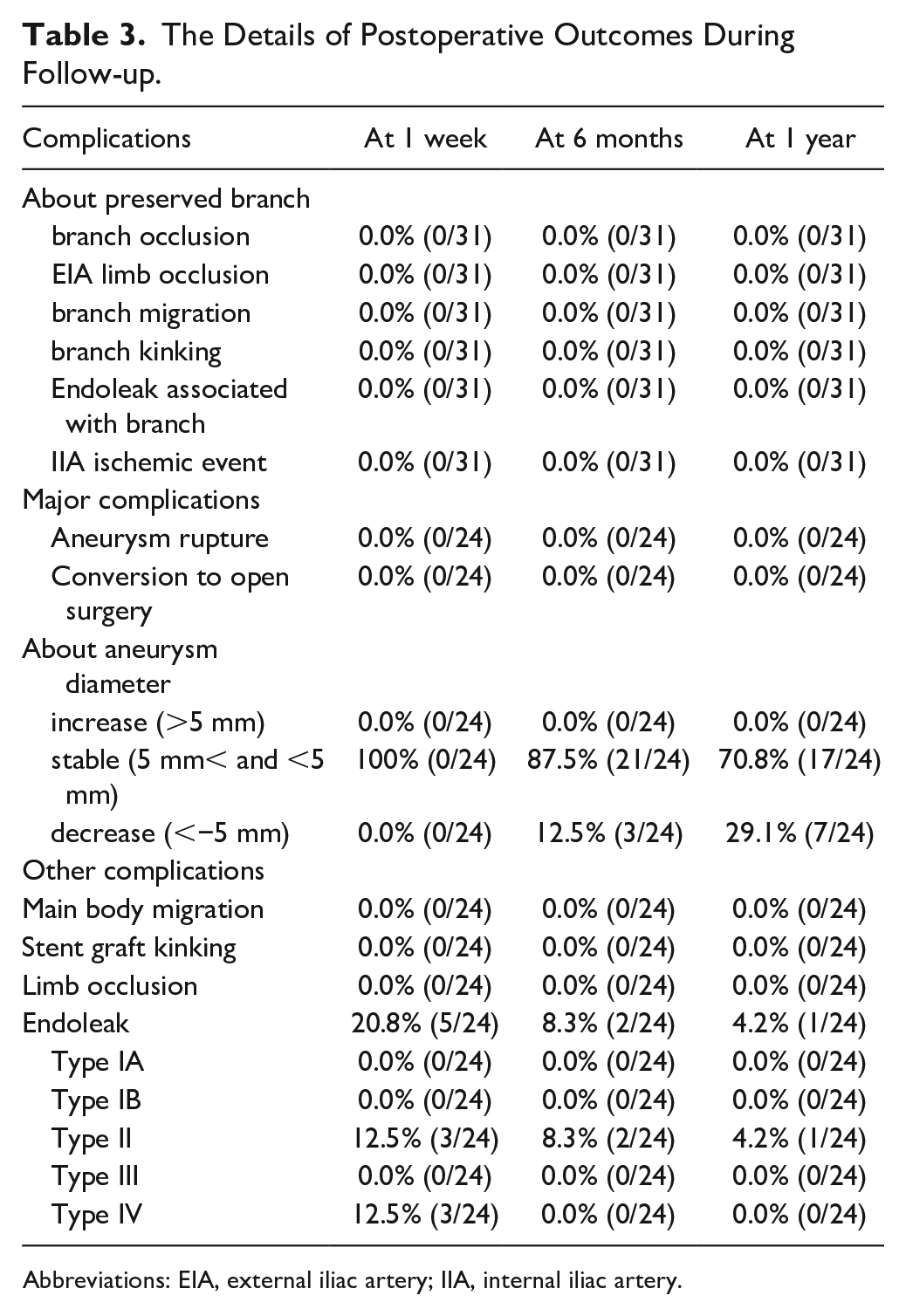
Abbreviations: EIA, external iliac artery; IIA, internal iliac artery.
Discussion
The features of a new technique of a physician-modified fenestrated Endurant contralateral limb are as follows. First, our technique is characterized by very few anatomical constraints. The Excluder IBE has a main trunk diameter limitation of 17 mm for the CIA. In contrast, unless the diameter of the CIA is extremely small, the physician-modified graft can be used for this procedure, and the anatomical indications are much wider than those for the Excluder IBE. Regarding the anatomical length requirement, our technique is applicable as long as the length of the contralateral gate of the main device is more than 84 mm from the renal artery bifurcation to the terminal aorta when using Endurant 2s stent graft system, that is, the length of the main device’s contralateral gate that is deployed within the abdominal aorta. The use of the Viabahn VBX for IIA grafts has also expanded its indications. This is because the Viabahn VBX stent graft is available in a wide variety of lengths, and its diameter can be controlled by postdilation to fit a variety of IIA forms. The Viabahn VBX endoprosthesis with a diameter of <6 mm was not used because of the high possibility of occlusion. After surgery, we used only 100 mg aspirin daily as the antiplatelet medication to avoid increasing the risk of endoleaks. The pull-through system we developed is based on the report by Lounes et al. 10 This procedure allows the delivery of the sheath close to the fenestration site and greatly facilitates the technique of cannulation to the IIA, which is considered as a highly reliable procedure. We conducted the identical procedure without employing a guidewire preloaded system. Nevertheless, it is important to note that the contralateral approach can be exceptionally challenging in situations where the terminal aorta exhibits a large diameter, the angle between the bilateral CIA is acute, or the length of the CIA measures less than 30 mm. Although the technique may be feasible if an upper extremity approach is added to these cases, the long distance from the upper extremity to the fenestration makes the catheter difficult to control and limits the types of catheters that can be used. Our guidewire preloaded system can be adapted to these cases without an additional approach.
Compared with the results of other iliac branch devices such as Excluder IBE,4 –6,11 Zenith Branch Endovascular Iliac Bifurcation Graft6,12 and E-liac™ STENT GRAFT SYSTEM7,13 in past literature, our new technique caused less occlusion and had a lower incidence of endoleak associated with bridging branch and less incidence of re-intervention at 1 year. It is difficult to mention the difference between our technique and Zenith Branch Endovascular Graft- Iliac Bifurcation or E-liac™ STENT GRAFT SYSTEM, as we have no experience with these other systems. There is also concern regarding blood flow obstruction by the bridging device in the modified limb. Although, as shown in Figure 4, there is sufficient space for the EIA in the limb, and we believe that flow reduction of the EIA is unlikely to occur.
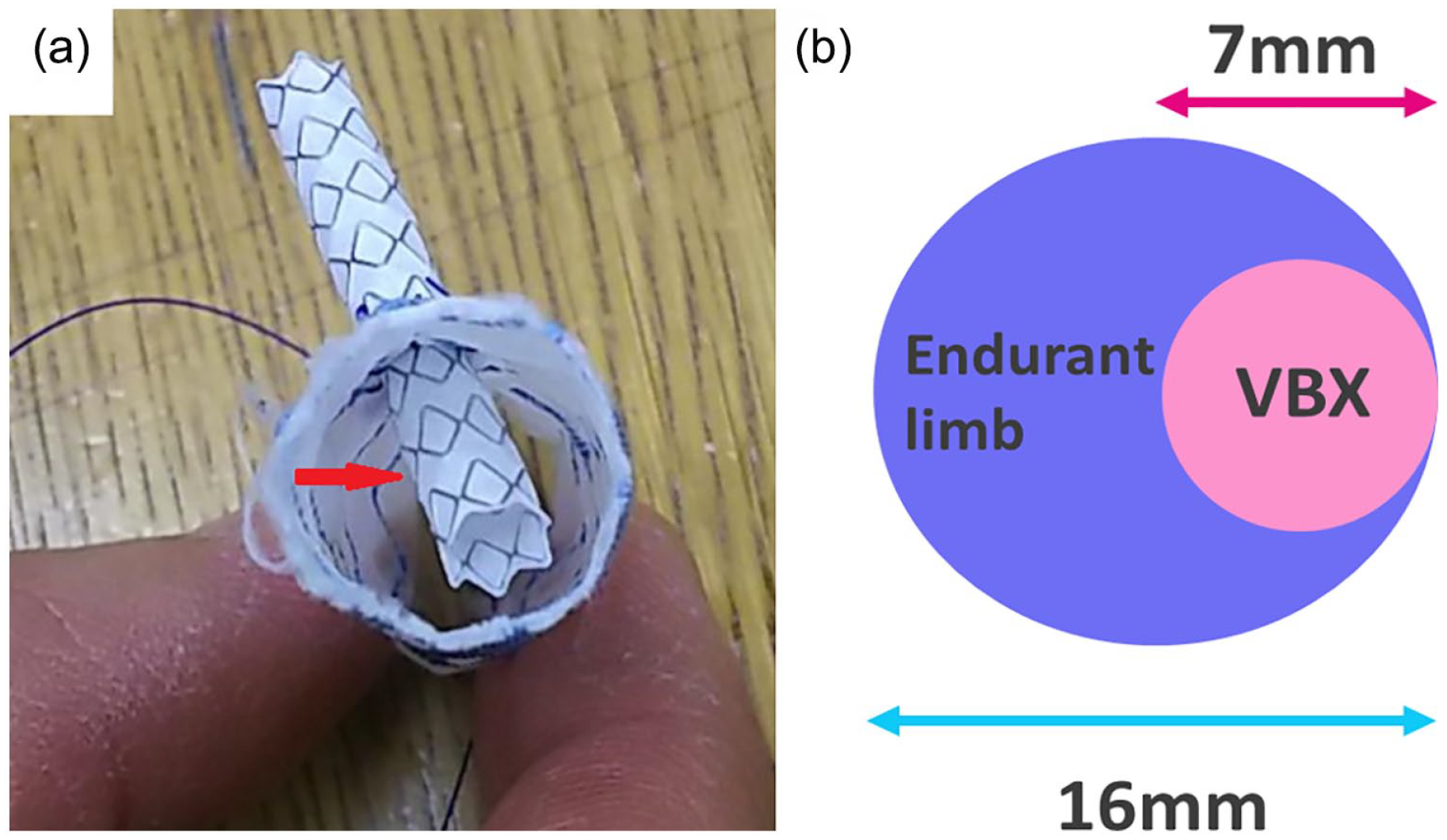
Inside image of the Endurant contralateral limb with a Viabahn VBX endoprosthesis branch. (A) The Viabahn VBX endoprosthesis deployed at the 3-stent position in vitro. In this state, it was positioned such that it nearly reached the opposite sidewall of the fenestration. In practice, a length of approximately 1.5 stents of the Viabahn VBX was inserted into the limb, such that there was no obstruction of the blood flow within the limb or the passage of additional delivery systems. (B) Image of a space in the Endurant contralateral limb and the Viabahn VBX endoprosthesis.
The pitfalls of this technique are the Endurant contralateral limb twisting when the CIA is <16 mm and limb occlusion. About the former, if the limb is twisted during resheathing, fenestration misalignment can be avoided by rotating the delivery system when the CIA is large; however, if the CIA is <16 mm, the CIA may fix the limb in a twisted position, making it difficult to correct the fenestration position, especially in cases with severe tortuosity. Moreover, when the internal iliac bifurcation cannot be separated on fluoroscopic contrast, the fenestration is difficult to align for IIA bifurcation. In such cases, we did not perform the technique as the success rate of the procedure might be considerably lower. About the latter, based on previous reports, there is a risk of occlusion at the Endurant contralateral limb. 14 Given that the position of the EIA landing site cannot be controlled during this procedure, there is an elevated risk of limb occlusion if the EIA at the landing site is curved or stenotic. Additional bare stent implantation should be considered in such cases.
The favorable clinical outcomes found in the 24 patients are promising, although future studies should examine long-term outcomes among larger populations. We are currently continuing this treatment in many cases and would like to present the long-term results in the future.
Conclusion
The new technique of a physician-made fenestrated Endurant contralateral limb is a highly versatile and reliable technique for preserving IIA flow. We believe it has a wide range of anatomical indications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.