
Abstract
Aim:
This study aimed to evaluate the effect of ultrasound-assessed lesion morphology on the outcomes of drug-coated balloon (DCB) versus plain old balloon angioplasty (POBA) treatment for de novo dysfunctional arteriovenous fistulas (AVF) lesions.
Methods:
This single-center retrospective study enrolled 114 consecutive patients (mean age, 73 ± 10 years; male, 69%) with de novo dysfunctional AVF lesions who underwent percutaneous transluminal angioplasty (PTA) using DCB (n = 48) and POBA (n = 66). The morphology of the stenotic lesions, evaluated using ultrasonography, was classified into intimal hyperplasia and shrinking types. The outcome measure was 12-month primary patency. Factors associated with loss of primary patency were evaluated using Cox proportional hazards models.
Results:
The baseline characteristics were not significantly different between the 2 treatment groups. The 12-month primary patency rate was significantly higher in the DCB group than in the POBA group (66.8 ± 7.1% versus 35.9 ± 6.3%, P = .006). The 12-month primary patency rate in the lesions with intimal hyperplasia type was not significantly different (DCB: 70.3 ± 9.5% versus POBA: 45.9 ± 8.0%; P = .310), whereas that in the shrinking type was significantly higher in the DCB group than in the POBA group (61.9 ± 10.6% versus 15.2 ± 8.1%; P < .001). The interaction analysis demonstrated that lesion morphology had a significantly different hazard ratio (HR) for restenosis between the POBA and DCB groups (P for interaction = .031). The multivariate analysis revealed that DCB usage (adjusted hazard ratio [aHR], 0.49; 95% confidence interval [CI]: [0.28, 0.87]; P = .015), ultrasound-assessed lesion morphology (shrinking type: aHR, 1.77; 95% CI: [1.07, 2.93]; P = .026), and location of stenosis (aHR, 2.26; 95% CI: 1.15, 4.46; P = .018) were significantly associated with AVF patency after PTA.
Conclusion:
This study revealed that lesion morphology evaluated using ultrasonography had a differential impact on DCB and POBA outcomes. The therapeutic effect of DCB was unexpectedly confirmed in the shrinking type.
Clinical Impact
The effectiveness of DCB in inhibiting smooth muscle cell proliferation in intimal hyperplasia lesions was expected based on the known mechanism of action of paclitaxel. However the therapeutic effect of DCB was unexpectedly confirmed in the shrinking type too. We may not need to hesitate usage of DCB for shrinking type.
Introduction
Although arteriovenous fistulas (AVFs) are the first-line vascular access for hemodialysis patients, AVFs are frequently associated with dysfunctions such as stenosis, occlusion, and inadequate maturation. 1 Percutaneous transluminal angioplasty (PTA) is the standard treatment for dysfunctional AVF. 2 We have previously reported that the ultrasound-assessed lesion morphology, such as intimal hyperplasia or shrinking type, was associated with patency after plane old balloon angioplasty (POBA). 3 Recently, drug-coated balloons (DCBs) are more effective than noncoated angioplasty for the treatment of dysfunctional AVF.4,5 The effectiveness of DCB in inhibiting smooth muscle cell proliferation in intimal hyperplasia lesions was expected based on the mechanism of paclitaxel. We hypothesized that DCB treatment would affect especially, intimal hyperplasia-type lesions. This study aimed to evaluate the effect of ultrasound-assessed lesion morphology on the outcomes of DCB versus POBA treatment for de novo dysfunctional AVF lesions.
Methods
Study Design
This study retrospectively reviewed a prospectively maintained database of hemodialysis patients who underwent PTA for de novo dysfunctional AVF defined as inadequate (blood removal failure, increased venous pressure, recirculation, and puncture difficulty) or at risk of inadequate hemodialysis treatment (decreased flow volume < 400 mL/min with physical findings suggesting underlying clinically significant lesions) due to stenosis. Thrombosed AVF, central vein lesion, and arterial inflow lesion were excluded. The study population was divided into DCB (between IN.PACT AV DCB clinical trial in 2017 and June 2022; the DCB group of the clinical trial was included in this group) and POBA (between July 2014 and before IN.PACT AV DCB clinical trial in 2017; the control group of the trial was included in the POBA group) groups. The local ethics committee approved the study, which was conducted in accordance with the principles of the Declaration of Helsinki.
Ultrasound Assessment Before PTA
Ultrasound assessments of stenosis lesions have been previously reported. 3 In short, the arteries, anastomotic sites, and veins were observed to identify clinical abnormality-associated stenosis, measure the size of the stenosis (inner and outer diameters at the stenotic site), and determine the morphological pattern of the stenosis. Valve-type lesions (Supplemental Figure 1) were excluded from this study. The inner and outer diameters at the stenotic site were measured, and the intimal hyperplasia rate was calculated using the following formula: Intimal hyperplasia rate (%) = (outer diameter − inner diameter)/outer diameter. Stenosis with an intimal hyperplasia rate ≥50% was referred to as intimal hyperplasia-type stenosis and that with an intimal hyperplasia rate <50% as shrinking-type stenosis (Figure 1). The technician-assessed AVF patency, stenosis diameter, flow volume, and morphological patterns were measured using a LOGIQ S8 (ML6-15-D and L8-l8-D probes; GE Healthcare, Little Chalfont, UK) and an Applio i700 (PLI-2002BT and PLI1205BX probes; Canon Medical Systems Corporation, Tochigi, Japan) ultrasound scanner before PTA. Juxta anastomosis stenosis was defined as stenosis located in the first 5 cm of the vein distal to the anastomosis site. Duplex testing was conducted while the patient was in a supine position with the arm resting on a bed. Flow volume was measured twice at a location along the brachial artery where blood flow was less turbulent, and the average value of these measurements was calculated.
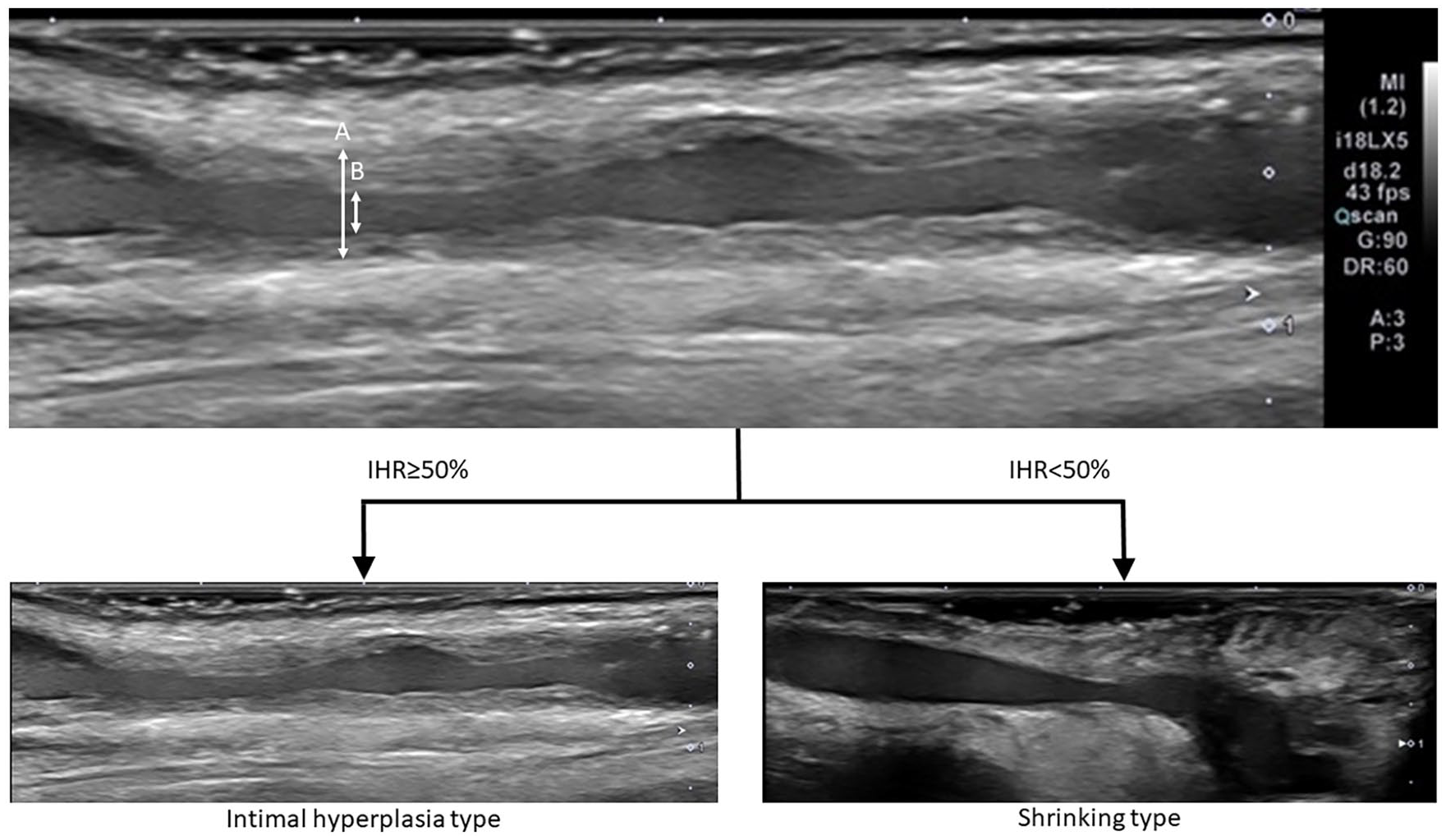
The morphological assessment of stenotic lesion in dysfunctional AVF using ultrasound. Morphological assessment of stenotic lesion at the minimum lumen area site was conducted using ultrasound imaging to determine the stenotic patterns (intimal hyperplasia and shrinking). The inner and outer diameters at the stenotic site were measured, and the intimal hyperplasia rate was calculated using the following formula: Intimal hyperplasia rate (%) = (outer diameter − inner diameter)/outer diameter. Stenosis with an intimal hyperplasia rate ≥50% was referred to as intimal hyperplasia-type stenosis and that with an intimal hyperplasia rate <50% as shrinking-type stenosis. (A: outer diameter; B: inner diameter). AVF, arteriovenous fistulas.
Endovascular Treatment
The patients in both groups underwent balloon angioplasty (MUSTANG and ATHLETIS: Boston Scientific, Massachusetts, US, OHICHO3, YOROI and SHIRANUI: Kaneka Medix Corporation, Osaka, Japan, CONQUEST and DORADO: Becton, Dickinson and Company, New Jersey, US) without cutting balloons, scoring balloons, or stent grafts. Patients in the DCB group underwent dilation with an IN.PACT AV DCB (Medtronic, Dublin, Ireland) at nominal pressure for 3 minute after balloon angioplasty. The method of POBA treatment was physician discrimination.
Outcome Measurement
The primary outcome measure was the duration of primary patency after PTA. Primary patency was defined as the duration from PTA until any first intervention (endovascular or surgical) to maintain or restore blood flow, the first occurrence of thrombosis, or reaching a censored event (death, transfer to peritoneal dialysis, or transplantation). The patients who died were counted as cases in which the AVF remained functional, with the date of death as the cutoff date. Additional nonsurgical/surgical interventions were recorded if hemodialysis could not be performed correctly because of low flow volume, occlusion, blood removal failure, elevated venous pressure, or recirculation.
Statistical Analysis
Continuous variables were analyzed using the Student’s t-test, and binary variables were compared using the chi-squared test. The Kaplan-Meier method was used to estimate the patency rate, and intergroup comparisons were performed using the log-rank test. A Cox proportional hazards model was used to identify independent factors associated with primary patency. These parameters in Cox multivariate analysis were selected based on their significance in our previous study 3 and factors that exhibited differences between the POBA and DCB groups in this study. Specifically, we considered lesion morphology, DCB usage, location of stenosis, lesion length, balloon size/reference vessel size, and flow volume. The selection of these parameters was not predefined but rather based on their potential impact on the primary patency outcomes.
Results
Patient Characteristics
A total of 114 patients (mean age, 73 ± 10 years; 69% men) underwent PTA, with no significant differences in baseline characteristics between the DCB (n = 44) and POBA (n = 66) groups (Table 1). The median observation period was 8.3 months (interquartile range: 4.1-12.6 months) after PTA. There were no significant intergroup differences in the intimal hyperplasia (n = 71) or shrinking (n = 43) types (Supplemental Table 1).
Patient Characteristics.
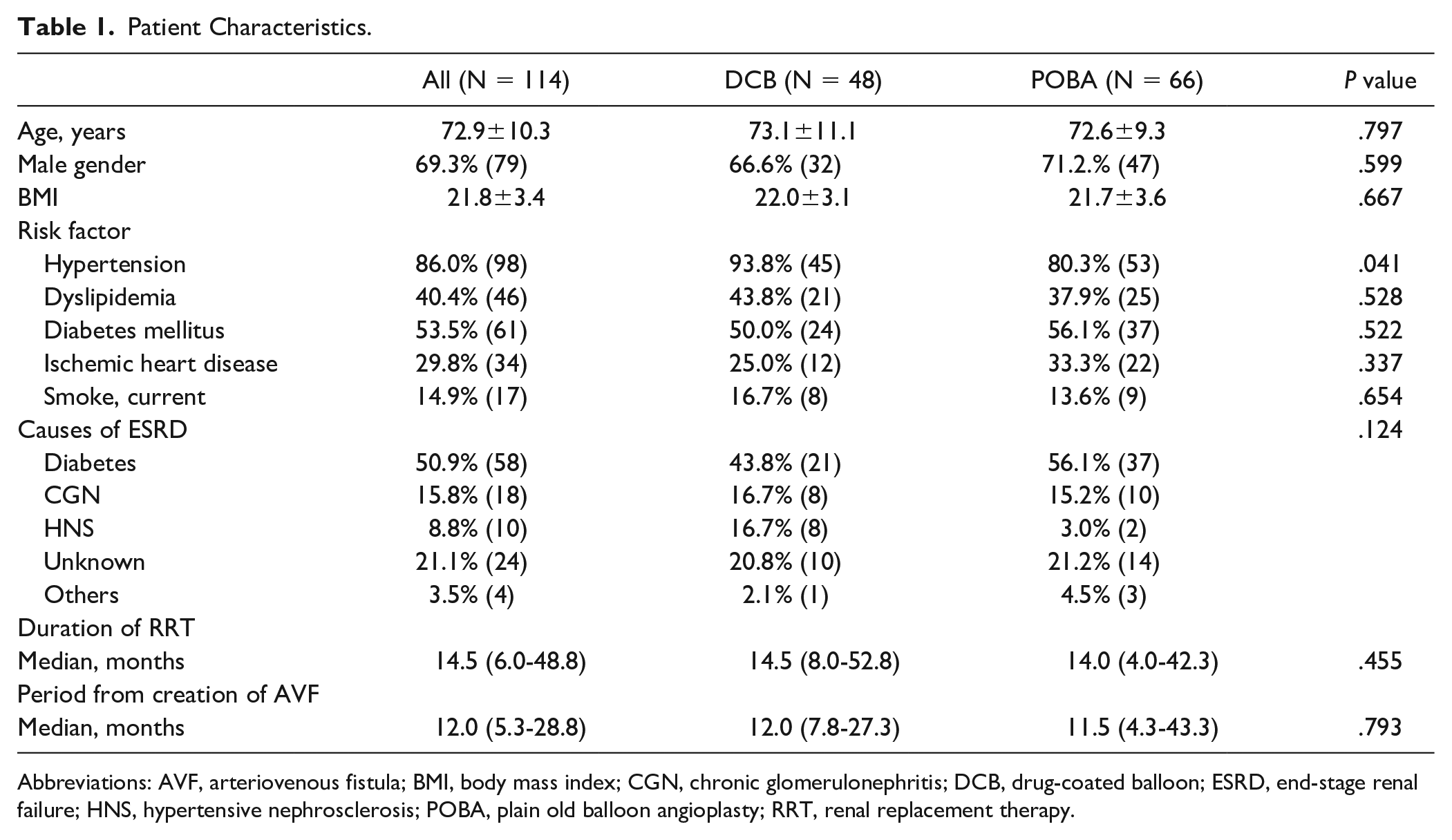
Abbreviations: AVF, arteriovenous fistula; BMI, body mass index; CGN, chronic glomerulonephritis; DCB, drug-coated balloon; ESRD, end-stage renal failure; HNS, hypertensive nephrosclerosis; POBA, plain old balloon angioplasty; RRT, renal replacement therapy.
Procedural Characteristics
The stenosis lesion location, length, and balloon size/reference vessel size differed significantly between the POBA and DCB groups (Table 2). Lesion size and stenosis rate were similar between the 2 groups. An ultrasound-guided lesion morphological assessment revealed that intimal hyperplasia was present in 54.2% (26/48) of patients in the DCB group and 68.2% (45/66) of patients in the POBA group. In comparison, the shrinking type was present in 45.8% (22/48) and 31.8% (21/66) of patients in the DCB and POBA groups, respectively (Table 2). The lesion length differed significantly between the POBA and DCB groups for the intimal hyperplasia type. The balloon size and balloon size/reference vessel size differed significantly between the groups for the shrinking type (Supplemental Table 2).
Lesion and Procedural Characteristics.
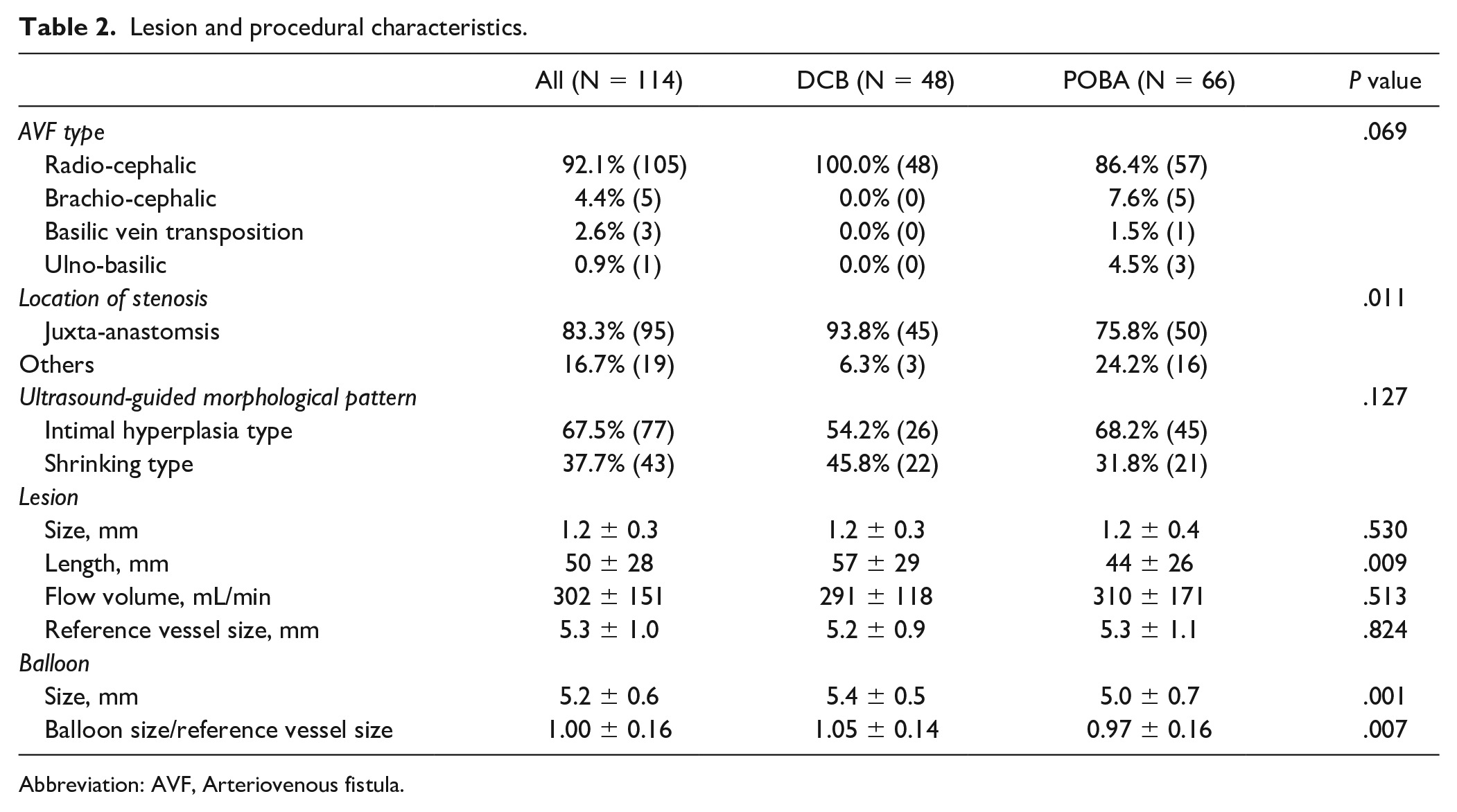
Abbreviation: AVF, Arteriovenous fistula.
Predictors of Primary Patency
The 12-month primary patency rates were 66.8% ± 7.1% in the DCB group and 35.9% ± 6.4% in the POBA group (P = .006, Figure 2). The multivariate analysis revealed that DCB use (adjusted hazard ratio [aHR], 0.49; 95% confidence interval [CI]: [0.28, 0.87]; P = .015), ultrasound-assessed lesion morphology (aHR, 1.77; 95% CI: [1.07, 2.93]; P = .026), and location of stenosis (aHR, 2.26; 95% CI: [1.15, 4.46]; P = .018) were independently associated with AVF patency after PTA (Table 3).
Predictors of Primary Patency After Endovascular Therapy.
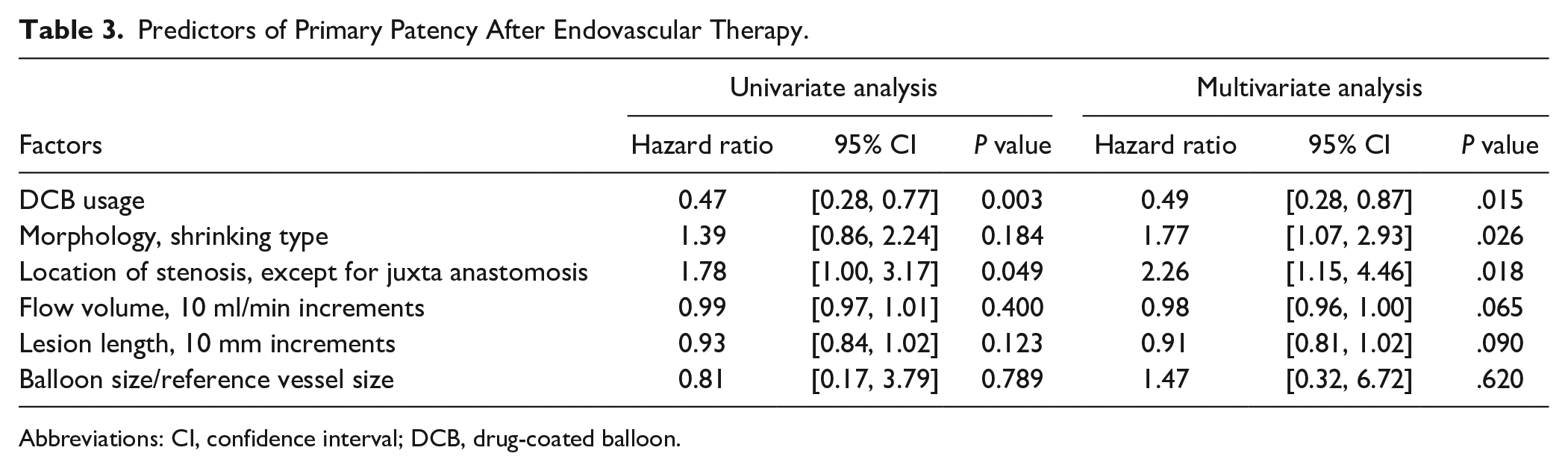
Abbreviations: CI, confidence interval; DCB, drug-coated balloon.
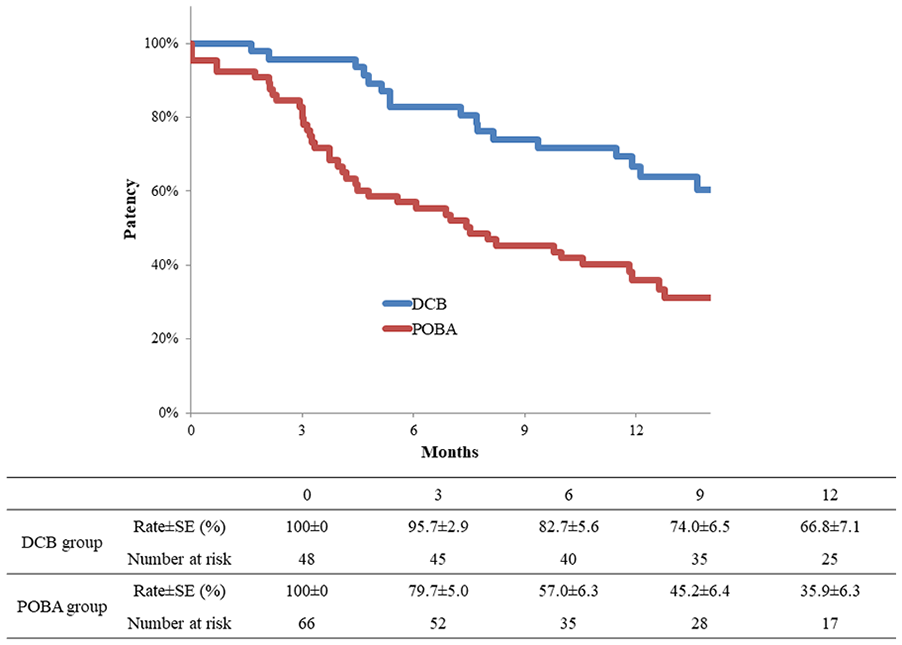
Kaplan-Meier estimates of primary patency. The 12-month primary patency rate was 66.8% ± 7.1% in the DCB group and 35.9% ± 6.3% in the POBA group (P = .006). DCB, drug-coated balloon; POBA, plain old balloon angioplasty.
Impact of Ultrasound-Guided Lesion Morphology on Primary Patency
The 12-month primary patency rate was higher in the DCB group than that in the POBA group for both intimal hyperplasia (70.3% ± 9.5% vs. 45.9% ± 8.0%, P = .310) and shrinking type lesions (61.9% ± 10.6% vs. 15.2% ± 8.1%, P < .001; Figure 3). The interaction analysis demonstrated that lesion morphology had a significantly different HR for restenosis between the POBA and DCB groups (P for interaction = .031).
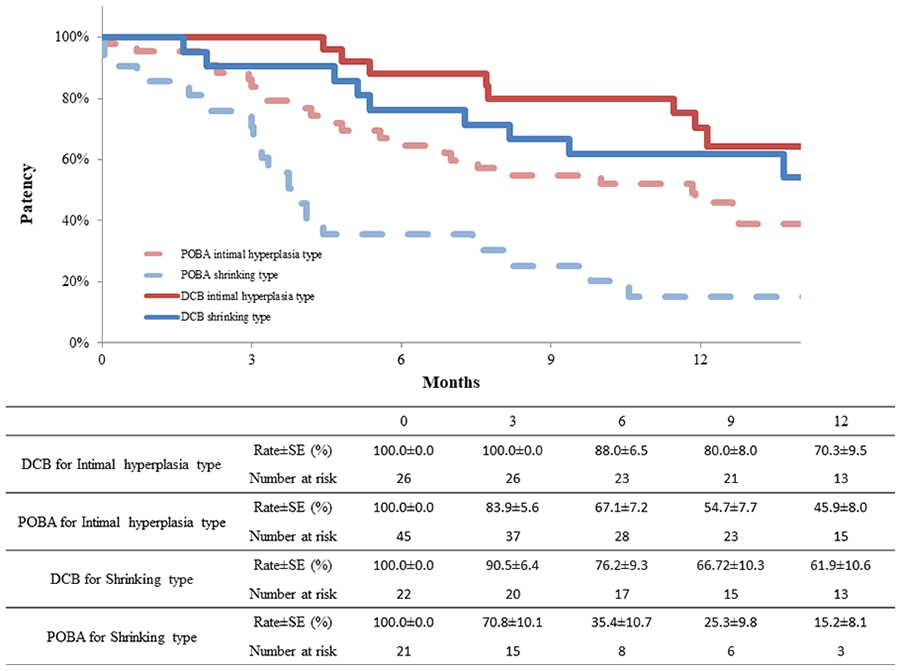
Primary patency after DCB versus POBA for failed arteriovenous fistulas according to lesion morphology. The 12-month primary patency rate of the intimal hyperplasia type was 70.3% ± 9.5% in the DCB group and 45.9% ± 8.0% in the POBA group (P = .310). The 12-month primary patency rate of shrinking type was 61.9% ± 10.6% in the DCB group and 15.2% ± 8.1% in the POBA group (P ≤ .001). DCB, drug-coated balloon; POBA, plain old balloon angioplasty.
Discussion
This study aimed to evaluate the effect of ultrasound-assessed stenotic lesion morphology divided into intimal hyperplasia and shrinking types on the patency of de novo dysfunctional AVF lesions after PTA with DCB versus POBA. We hypothesized that DCB treatment especially affects intimal hyperplasia type by suppressing intimal proliferation. Here, we revealed an unexpected but important effect of DCB on shrinking type of dysfunctional AVF lesions.
The effectiveness of DCB in inhibiting smooth muscle cell proliferation in intimal hyperplasia lesions was expected based on the known mechanism of action of paclitaxel. However, the mechanism underlying the efficacy of DCB in shrinking type lesions needs to be explored through further pathological investigations. Animal experiments have revealed that the effects of paclitaxel extend beyond the vascular endothelium, reaching even the outer layers of the vessel wall. 6 Reports suggest that the use of paclitaxel devices in coronary and lower limb arteries can induce aneurysmal changes associated with lumen enlargement.7 –9 In our previous study, POBA maintained patency for valve types in dysfunctional AVF. 3 These results highlight the importance of considering ultrasound-assessed lesion morphology in the treatment decision-making process for dysfunctional AVF and the potential for DCB as a valuable therapeutic option for all lesions other than the valve type. The usefulness of ultrasound in evaluating AVG outflow lesion morphology during stent placement has been previously reported. 10 However, a key difference between their classification of lesion types and ours is that we did not use the normal vessel diameter in our classification. Unlike coronary or lower-extremity arteries, AVF vessel diameters vary and lack uniformity. In addition, their study highlighted that a classification solely based on neointimal hyperplasia rate had an impact on the outcomes after stent placement.
Considering these findings, in our study, we opted to use a classification based on neointimal hyperplasia rate. Our previous study 3 revealed poor outcomes for shrinking type lesions with POBA alone. However, we observed surprisingly favorable results with DCB for “Shrinking type,” though not reaching the outcomes shown in their stent results.
In addition, the stenosis location significantly impacts patency after PTA, with stenosis at the juxta-anastomosis being the most common; 11 however, other difficult-to-treat stenosis also occurs, such as the cephalic arch 12 and swing segment of basilic vein transposition. 13 Further investigation is required to examine the effects of different stenosis sites.
This study had limitations, such as its single-center design and the small sample size of only Japanese patients. In addition, the disparity in treatment timing between the POBA and DCB groups was one of its limitations. Moreover, the comparison of the DCB group, derived from a randomized controlled trial to the POBA group in real-world clinical practice could potentially introduce selection bias. The exclusion of calcified, restenotic, and occlusive lesions may have limited the generalizability of our results. Although propensity score matching is a valuable approach for mitigating selection bias in observational studies, the sample size in our study was relatively small, which limited our ability to employ propensity score matching. Further studies with larger sample sizes performed at multiple centers are required to confirm our findings. There are several DCBs, each DCBs has different paclitaxel doses, and excipients. It is unclear whether DCBs except IN.PACT DCB have a similar effect, as this difference affects the delivery of paclitaxel to the lesion.
Conclusion
This study revealed that lesion morphology evaluated using ultrasonography had a differential impact on DCB and POBA outcomes. The therapeutic effect of DCB was unexpectedly confirmed in the shrinking type lesions.
Supplemental Material
sj-pptx-1-jet-10.1177_15266028231215225 – Supplemental material for Ultrasound-Assessed Lesion Morphology and Drug-Coated Balloon Treatment for de novo Dysfunctional Arteriovenous Fistula in Hemodialysis Patients
Supplemental material, sj-pptx-1-jet-10.1177_15266028231215225 for Ultrasound-Assessed Lesion Morphology and Drug-Coated Balloon Treatment for de novo Dysfunctional Arteriovenous Fistula in Hemodialysis Patients by Kotaro Suemitsu, Tatsuya Shiraki, Osamu Iida, Kanako Oka, Naomi Ota and Masaaki Izumi in Journal of Endovascular Therapy
Supplemental Material
sj-tif-2-jet-10.1177_15266028231215225 – Supplemental material for Ultrasound-Assessed Lesion Morphology and Drug-Coated Balloon Treatment for de novo Dysfunctional Arteriovenous Fistula in Hemodialysis Patients
Supplemental material, sj-tif-2-jet-10.1177_15266028231215225 for Ultrasound-Assessed Lesion Morphology and Drug-Coated Balloon Treatment for de novo Dysfunctional Arteriovenous Fistula in Hemodialysis Patients by Kotaro Suemitsu, Tatsuya Shiraki, Osamu Iida, Kanako Oka, Naomi Ota and Masaaki Izumi in Journal of Endovascular Therapy
Footnotes
Acknowledgements
The authors gratefully acknowledge the work of past and present members of their team.
Correction (February 2024):
Article updated to correct Table 2 in the article. Previously, Table 1 was incorrectly added twice as Table 2. Please see https://doi.org/10.1177/15266028241236599 for more details.
Prior Presentation
This study has never been presented at any meeting.
Authors’ Contributions
KS and TS made a substantial contribution to the concept and design of the work; acquisition, analysis, and interpretation of data; drafted the article and revised it critically for important intellectual content; approved the version to be published; and participated sufficiently in the work to take public responsibility for appropriate portions of the content. OI and MI made a substantial contribution to the concept and design of the work and analysis and interpretation of data; revised the article critically for important intellectual content; approved the version to be published; and participated sufficiently in the work to take public responsibility for appropriate portions of the content. KO and NO made a substantial contribution to the concept and design of the work; acquisition of data; revised the article critically for important intellectual content; approved the version to be published; and participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KS received honoraria from Medtronic Japan and Boston scientific Japan. OI received honoraria from Medtronic Japan. TS, KO, NO, and MI have no competing interests.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.