
Abstract
Objective:
To report on the recommendations of an expert-based consensus on the indications, timing, and techniques of aortic balloon occlusion (ABO) in the management of ruptured abdominal aortic aneurysms (rAAA).
Methods:
Eleven facilitators created appropriate statements regarding the study issues that were voted on using a 4-point Likert scale with open-comment fields, by a selected panel of international experts (vascular surgeons and interventional radiologists) using a 3-round modified Delphi consensus procedure (study period: January-April 2023). Based on the experts’ responses, only the statements reaching grade A (full agreement ≥75%) or B (overall agreement ≥80% and full disagreement <5%) were included in the final study report. The consistency of each round’s answers was also graded using Cohen’s kappa, the intraclass correlation coefficient, and, in case of double resubmission, Fleiss kappa.
Results:
Sixty-three experts were included in the final analysis and voted on 25 statements related to indication and timing (n=6), and techniques (n=19) of ABO in the setting of rAAA. Femoral sheath or ABO should be preferably placed in the operating room, via a percutaneous transfemoral access, on a stiff wire (grade B, consistency I), ABO placement should be suprarenal and last less than 30 minutes (grade B, consistency II), postoperative peripheral vascular status (grade A, consistency II) and laboratory testing every 6 to 12 hours (grade B, consistency) should be assessed to detect complications. Formal training for ABO should be implemented (grade B, consistency I). Most of the statements in this international expert-based Delphi consensus study might guide current choices for indications, timing, and techniques of ABO in the management of rAAA. Clinical practice guidelines should incorporate dedicated statements that can guide clinicians in decision-making.
Conclusions:
At arrival and during both open or endovascular procedures for rAAA, selective use of intra-aortic balloon occlusion is recommended, and it should be performed preferably by the treating physician in aortic pathology.
Clinical Impact
This is the first consensus study of international vascular experts aimed at defining the indications, timing, and techniques of optimal use of ABO in the clinical setting of rAAA. Aortic occlusion by endovascular means (or ABO) is a quick procedure in properly trained hands that may play an important role as a temporizing measure until the definitive aortic repair is achieved, whether by endovascular or open means. Since data on its use in hemodynamically unstable patients are limited in the literature, owing to practical challenges in the performance of well-conducted prospective studies, understanding real-world use by experts is of importance in addressing critical issues and identifying main gaps in knowledge.
Introduction
The use of endovascular techniques for the treatment of ruptured abdominal aortic aneurysm (rAAA) with endovascular aortic repair (EVAR) has been steadily increasing and has become the dominant method of repair over the last few decades.1,2 It can be achieved using adjunctive techniques, one of which is aortic balloon occlusion (ABO), the conceptual basis of which is similar to Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) in the trauma setting. The use of ABO is supported by several major vascular guidelines, although these do not provide detailed guidance on its practical implementation; in fact, ABO is also conceptually integrated into the standard workflow in endovascular resuscitation and trauma management (EVTM).3–13
Indeed, ABO is a temporary supportive tool to treat hemodynamic instability and can be used for both EVAR and open aortic repair (OAR) of rAAA, although its use has been associated with increased complication rates, particularly abdominal compartment syndrome after EVAR, probably due to the highly unstable hemodynamic status of the patient and different logistical problems in its implementation in routine practice.14–17 Abdominal compartment syndrome is notably related to prolonged suprarenal clamping, so clearer indications on timing and modality of ABO could play a role in preventing such a dreadful event.
To date, there are no prospective data on this topic, while randomized controlled studies are difficult to design and conduct because of recruiting issues and ethical reasons. Due to the fact that ABO is in clinical use worldwide and that the indications, timing, and techniques of its optimal use are not well defined, we performed a Delphi study of the major issues regarding the implementation of ABO for rAAA. The aim of the study was to find a consensus among clinically active experts that may be useful in guiding both clinical practice and further research in this controversial area.
Materials and Methods
Study Design
An expert consensus on the indications, timing, and techniques of endovascular balloon occlusion of the aorta in the setting of rAAA was obtained using a modified Delphi consensus process. The study (acronym CONTROL-RAAA) was designed by study teams at 2 Italian universities. All surveys were submitted online and recorded through SurveyMonkey (https://www.surveymonkey.com). Invited experts were unaware of the identity of any other members of the international panel. Institutional review board approval was not required for this type of study.
Core Team and International Experts’ Panel Selection
The Core Team members comprise the study’s principal investigators (L.B., M.D., S.B., S.L.), and 7 adjunctive external facilitators (T.M.H., T.R., G.P., G.F.V., K.M., A.M.I., A.M.), selected according to their expertise and clinical experience in the field of the consensus. All Core Team members are vascular surgeons (VSs). To ensure proper statistical analysis, a professional biostatistician with prior experience in Delphi-based research was also invited to join the Core Team (R.L.). Potential international experts to be included as panel members were selected among active physicians with a specialization in vascular surgery or interventional radiology, practicing in Europe, America, Asia, and Oceania. Physicians were identified based on prior publications in high-ranking vascular scientific journals and/or from international-conference presentations on aortic endovascular procedures, and/or serving on editorial boards for peer-reviewed journals relevant to the study practice. To be included in the consensus, they had to meet all the following pre-specified entry criteria: at least 5 years in independent practice, at least 20 EVAR/year as first operators, and at least 100 EVAR as first operator from beginning of independent practice. To investigate the endorsed practices at each aortic center or vascular division just once, and avoid the potential bias derived from duplicate responses, only one physician per institution was allowed to participate in the Delphi process. The Core Team members were not allowed to vote in any of the questionnaire, but an expert colleague from their own center was invited to fill out the survey responses. The study was performed on a voluntary basis and external funding was not provided for participation.
Delphi Methodology Generalities
A modified Delphi method was used to construct the expert consensus. 18 To develop the initial lists of statements for expert evaluation, a preliminary exploratory questionnaire (with multiple-choice questions and the option of open-ended suggestions) was administered by the Core Team to the invited experts to investigate the daily practice at each center or division (Supplementary Table 1). The answers given in the questionnaire were analyzed by the Core Team, and statements were designed and approved by all Core Team members. A compressed 4-point Likert-type scale was used to grade statements based on the level of agreement: fully agree (score 3), agree (score 2), disagree (score 1), and completely disagree (score 0). The central fifth grade of the Likert scale (ie, “no opinion”) was omitted in view of the panel’s expertise and based on the assumption that the invited experts would be able to offer their opinion on each statement. The statements were submitted to 3 rounds of evaluation and eventually modified by the Core Team to increase consensus according to the experts’ open comments during the first 2 rounds. The first round was intended to submit the first formulation of the statements and obtain a broad indication of the strength of the consensus. The second round was intended to obtain a detailed estimate of the consensus change from the original formulations to the modified formulations after they had been implemented as per the process above. The third round was intended to confirm the strength of consensus from the second to the third formulation and to confirm the statements that had failed to reach sufficient consistency of agreement at all previous steps.
Statistical Analysis, Evaluation of Consensus Strength, and Consistency of Scoring
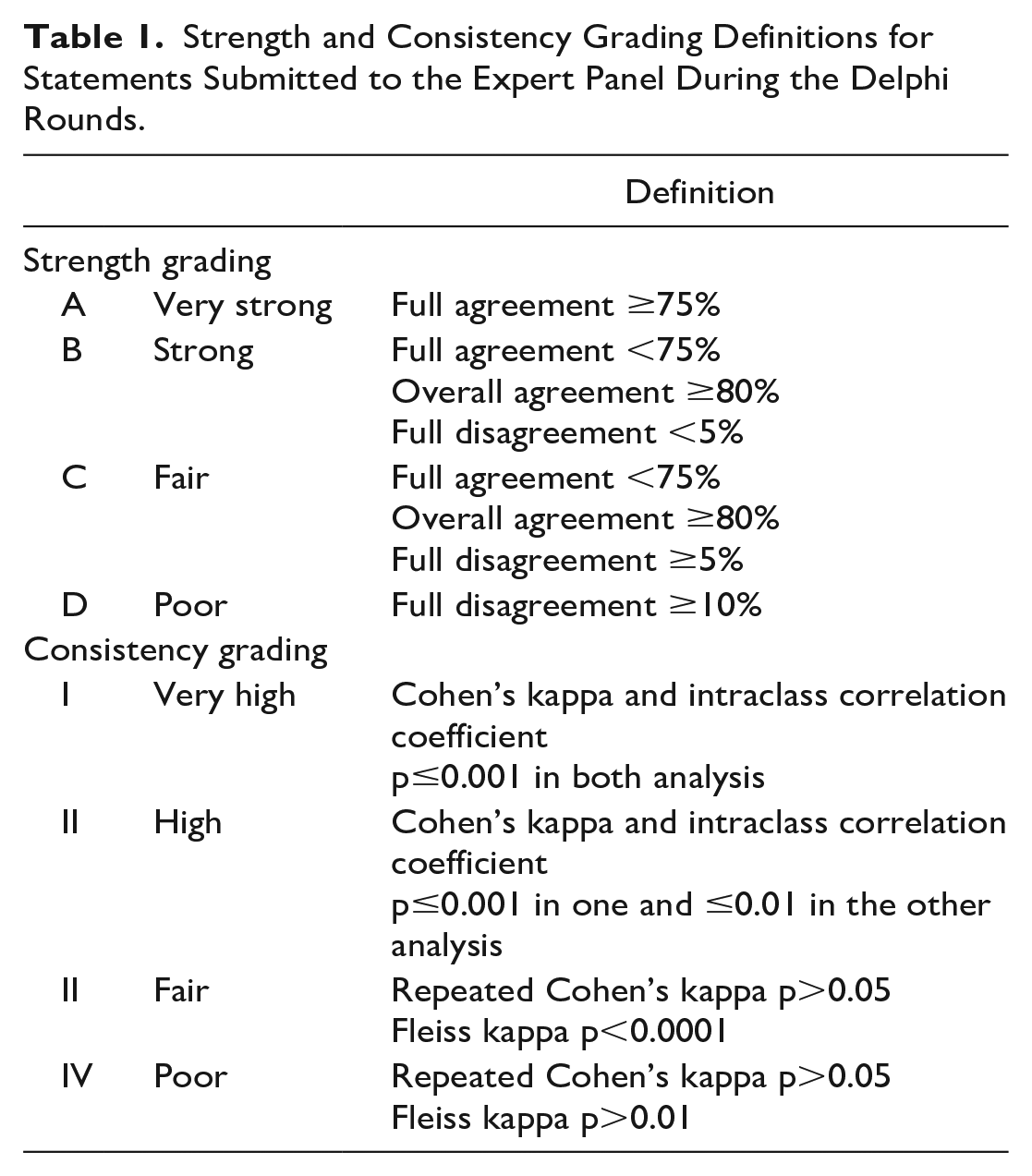
The data were analyzed by a professional biostatistician as described above; all statistical analyses were carried out using R software.19–22 The strength of consensus was classified based on the experts’ responses into 4 categories (Table 1). In addition, the corrected mean score (range, 0–3) assigned to each statement with its 95% confidence interval (95% CI), the significance of the change from the previous round according to the Wilcoxon test, and the significance of the correlation with the previous rating were all evaluated. These items were used to confirm the strength of the consensus in light of the lower bound of the 95% CI (>2.00 to confirm a strong consensus). Only a p value of ≤0.025 was regarded as a significant variation given that a degree of multiplicity was expected. The consistency of scoring (Table 1) between rounds with the proportion of agreement was estimated using p values from Cohen’s kappa and from the intraclass correlation coefficient (ICC), which were set for consistency using a 2-way model (separately between the first and second and between the second and third rounds). Consistency was defined as grade I or very high if both had a p value of ≤0.001, or as grade II or high if the p value was ≤0.001 in one analysis and ≤0.01 in the other. The proportion of ratings exceeding the critical difference was estimated to monitor test-retest reliability according to Bland and Altman23,24 and was considered as a modifier of consistency; a proportion of outliers greater than 10% was deemed to be indicative of significant heterogeneity across experts. Fleiss kappa was complemented by the estimate of the category-wise k in the case of a double resubmission of a statement. Statements with a consistency grade of III or IV according to the repeated Cohen’s kappa analysis, but which otherwise resulted in being highly consistent according to Fleiss kappa, were eventually classified as grade III.
Strength and Consistency Grading Definitions for Statements Submitted to the Expert Panel During the Delphi Rounds.
Statement Selection and Change Criteria
Several different statistical criteria were used to decide whether to reject a statement or let the person make changes and resubmit it. The predefined criteria for submission/resubmission after the first round were set as follows: statements with a proportion of full disagreement ≥10% and/or a mean score of <2.0 were not to be resubmitted; all other statements were to be resubmitted after textual adaptation and/or merging of statements, as appropriate. The predefined criteria for submission/resubmission after the second round were set as follows: (1) statements with a proportion of overall agreement <80% and a proportion of full disagreement >5% (grades C and D) were to be removed from the consensus; (2) statements with at least 5 of the following—a proportion of “fully agree” >75% or a proportion of overall agreement >80%, a proportion of full disagreement <5%, a mean score change from the first to the second round not statistically significant (Wilcoxon test, see above), a significant score correlation between the first and second round, a significant measure of agreement (Cohen’s kappa, see above), a significant ICC set for consistency, and a good test-retest reliability—were to be accepted in their current form, unless the Core Team suggested resubmission. At the third and last round, only statements with grades of strength A and B were considered of sufficient quality to be included in the final set of recommendations.
Results
One hundred and thirty-seven experts were initially contacted and invited to participate in the survey (VSs and interventional radiologists [IRs]). Of those, 70 answered the preliminary questions. Sixty-five participants (64 VSs, 1 IR), all meeting the pre-specified inclusion criteria, actively responded to the survey rounds and were included in the final analysis, thereby yielding an overall inclusion rate of 47%. The experts were mainly practicing in European (N=38; 58%) or North American (N=14; 22%) hospitals. Fifty-five experts (85%) participated in all 3 Delphi rounds; overall, 62 experts completed round 1, 62 experts completed round 2, and 63 experts completed round 3.
The Core Team designed the first round with 25 initial statements. The complete texts of the 25 statements (as in the formulation of the final round) are listed in Table 2. Table 3 summarizes the degrees of consensus obtained by each statement in the third round. At the end of the process, no statements were rejected; 24 statements (96%) received a grade B consensus strength, and 1 statement (4%) reached a grade A consensus strength. Table 4 summarizes the estimates of consistency across rounds. Most statements (22/25) were classified as grade I or II, while 3 of 25 were classified as grade III or IV.
List of the 25 Statements Related to Indications, Timing, and Technique of Endovascular Balloon Occlusion of the Aorta in the Setting of Ruptured Abdominal Aortic Aneurysms That Received a Grade A and B Strength Consensus During the 3 Rounds of the Delphi Consensus Voted on by the 64 Members of the International Expert Panel.
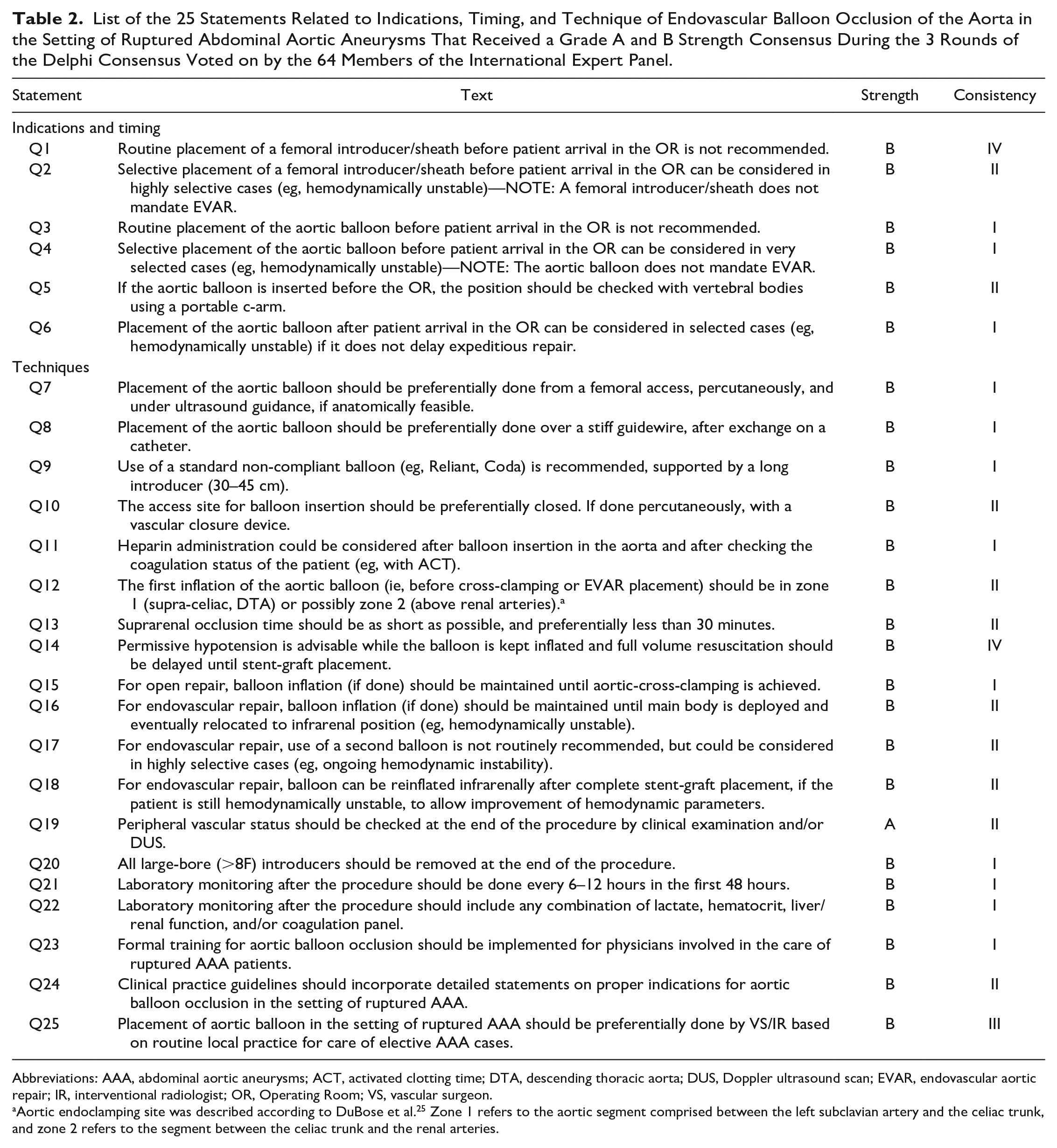
Abbreviations: AAA, abdominal aortic aneurysms; ACT, activated clotting time; DTA, descending thoracic aorta; DUS, Doppler ultrasound scan; EVAR, endovascular aortic repair; IR, interventional radiologist; OR, Operating Room; VS, vascular surgeon.
Aortic endoclamping site was described according to DuBose et al. 25 Zone 1 refers to the aortic segment comprised between the left subclavian artery and the celiac trunk, and zone 2 refers to the segment between the celiac trunk and the renal arteries.
Strength of Each Statement in the Delphi Consensus for the Recommendation of Balloon Occlusion of the Aorta in the Setting of Ruptured Abdominal Aortic Aneurysms.
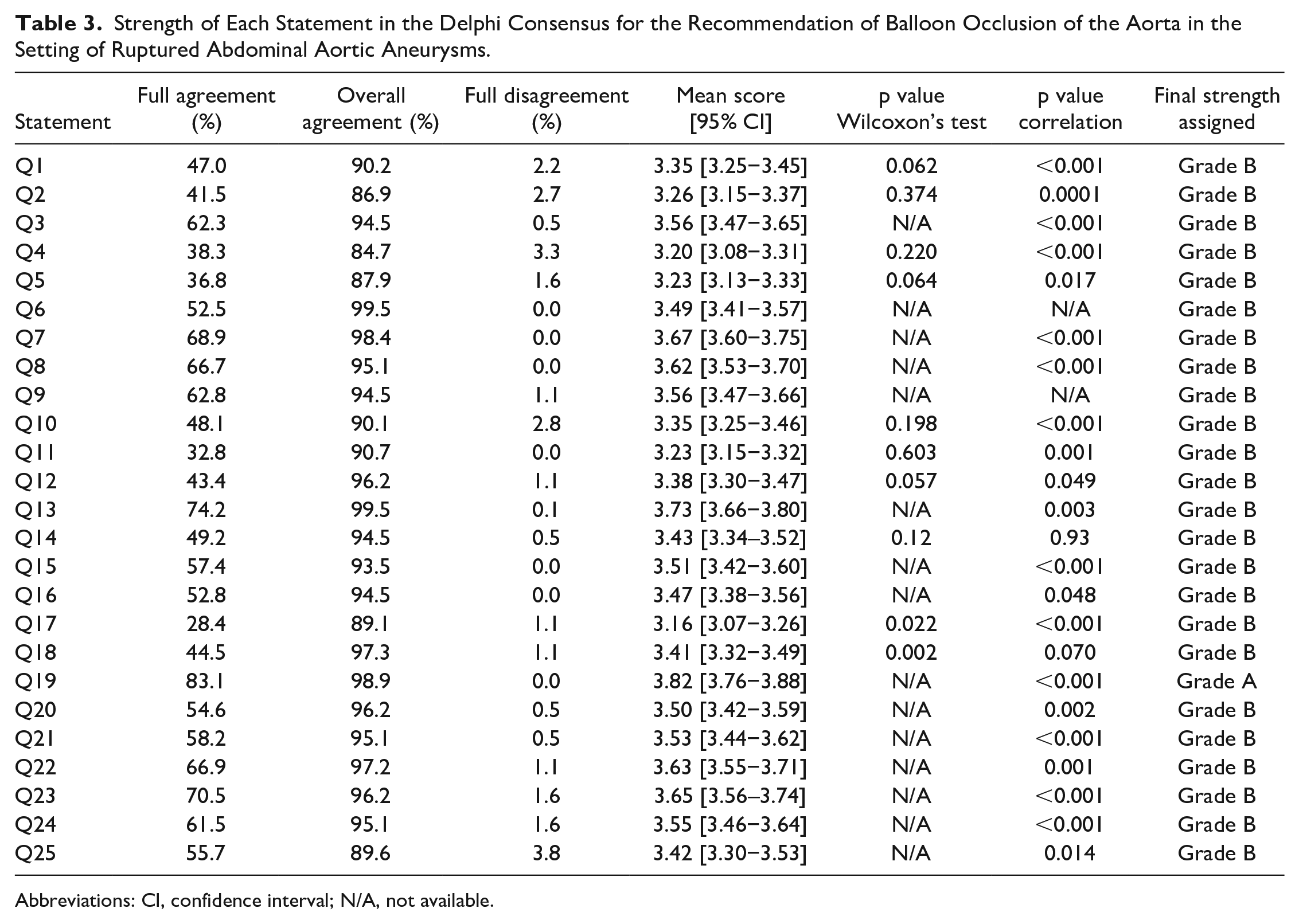
Abbreviations: CI, confidence interval; N/A, not available.
Estimates of Consistency Based on Cohen’s Kappa Evaluation After 3 Rounds in the Delphi Consensus on Balloon Occlusion of the Aorta in the Setting of Ruptured Abdominal Aortic Aneurysms.
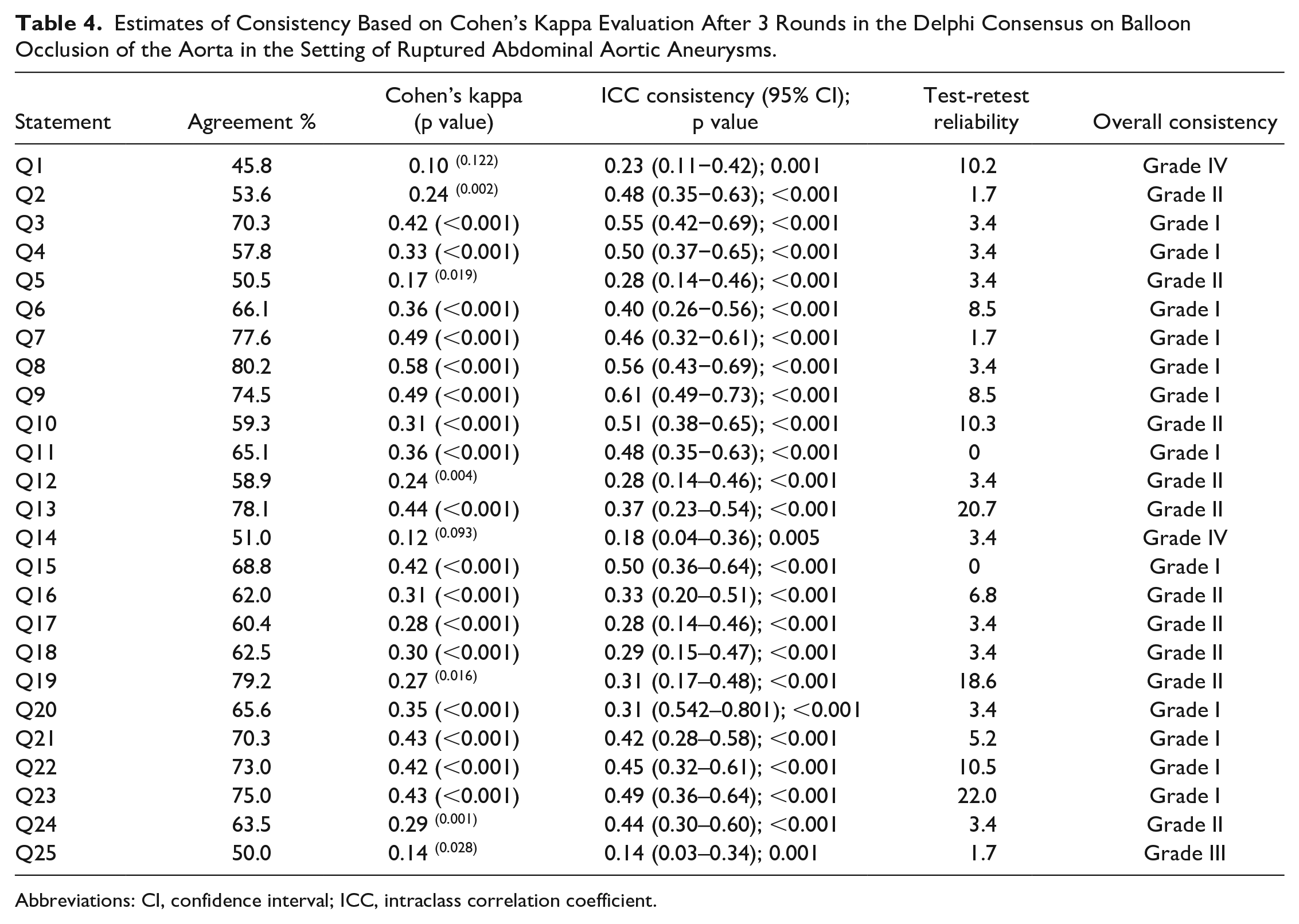
Abbreviations: CI, confidence interval; ICC, intraclass correlation coefficient.
For instance, the panel suggested that routine placement of a femoral introducer/sheath (grade B, consistency IV) as well as of the aortic balloon (grade B, consistency I) before patient arrival in the operating room is not recommended. Also, the experts suggested that placement of the aortic balloon should be done preferentially from a femoral access, percutaneously, and under ultrasound guidance, done over a stiff guidewire, using a non-compliant balloon supported by a long introducer (grade B, consistency I). Furthermore, it was the panelists’ opinion that placement of aortic balloon in the setting of ruptured AAA should be preferentially done by VS/IR based on routine local practice for care of elective AAA cases (grade B, consistency III). The only grade A statement (consistency II) is the need for peripheral vascular status assessment at the end of the procedure by clinical examination or duplex ultrasonography.
Discussion
This is the first consensus study of international vascular experts aimed at defining the indications, timing, and techniques of optimal use of ABO in the clinical setting of rAAA. Aortic occlusion by endovascular means (or ABO) is a quick procedure in properly trained hands that may play an important role as a temporizing measure until the definitive aortic repair is achieved, whether by endovascular or open means.16,26 Since data on its use in hemodynamically unstable patients are limited in the literature, owing to practical challenges in the performance of well-conducted prospective studies, understanding real-world use by experts is of importance in addressing critical issues and identifying main gaps in knowledge.
In general, the experts’ panel supported the use of ABO for rAAA in hemodynamically unstable patients, using femoral vascular access, preferably in the operating room or a hybrid suite with percutaneous ultrasound-guided access and fluoroscopy guidance. This is reasonably supported by the specific aspects of rAAA that must be considered when the implementation of ABO is sought. 27 In fact, rAAA is fundamentally different from any other major exsanguination scenario, such as polytrauma, and the use of ABO, therefore, differs from REBOA in these scenarios. Current data suggest a positive effect of using ABO, as mortality rates are lower in studies with higher rates of ABO, and intraoperative mortality may be lower using ABO than conventional aortic cross-clamping.28,29 However, ABO does not reduce in-hospital mortality, which is likely to reflect the severity of the clinical presentation rather than any direct effects of the techniques used to achieve aortic control.
The panel did not recommend initiating femoral access or ABO routinely in the emergency room, mainly due to the technical difficulties that can be encountered when trying to get the balloon quickly into the descending thoracic aorta in a controlled and safe manner. Placing a femoral sheath is, however, easier, faster, and less invasive than introducing an ABO and on this specific item the consistency of the panel’s response is consequently weaker (grade IV vs grade II for ABO). The balloon should be preferably placed, according to experts’ recommendations, once the patient has already arrived in the operating room and with imaging assistance to check its position, which should be above the renal arteries or celiac trunk. However, strong and more consistent agreement indicate the possibility in selected unstable patients could benefit from preoperative femoral sheath and ABO positioning (Statements Q2 and Q4). In special settings in which interhospital transfer is necessary for logistic reason, the delay in aortic repair is counterbalanced by improved patients’ outcomes. 30 In-hospital and pre-transfer ABO positioning should be further evaluated in such situations. The ABO should be inflated, when the patient is hemodynamically unstable, in both open and endovascular procedures, until definitive aortic control is achieved. More specifically, the panel recommended maintaining inflation until aortic cross-clamping or until delivery of the main body of the stent-graft; in the latter case, the balloon can be slowly removed, or its location changed to an infrarenal position to allow further inflation if needed. Balloon initial positioning in the operating room should be tailored according to the employed aortic repair technique (open repair, EVAR with or without suprarenal stent). The panel also recommended the preferential use of percutaneous access with closure devices and removal of the sheaths at the end of the procedure, with clinical and ultrasound control of blood flow to the lower extremities. In general, it was recommended that ABO balloons should be placed using a stiff guidewire and long sheath, using locally available standard aortic compliant balloons.
A growing body of evidence has shown that procedural volume is correlated with improved outcomes after the repair of intact as well as ruptured AAA.31–33 Furthermore, the implementation of training protocols proved to be effective in streamlining the process of care for rAAA patients, improving the process in real life, and potentially enhancing outcomes. 26 Accordingly, the Delphi panel recommended that formal training in ABO should be implemented for physicians involved in the care of rAAA patients, and balloon placement should be preferentially done by providers with proven skills and experience, based on routine local practice for the care of elective AAA cases. Based on the findings of the study, further research on this topic should focus on preoperative parameters indicating/contraindicating selective/routine aortic balloon positioning, the most efficient location and timing for endoclamping, and best resuscitative policies (delayed resuscitation until balloon occlusion vs until complete aortic repair). While conducting high-quality research in the field of emergency vascular surgery, well-conducted prospective studies might be needed to transition from “consensus” to “evidence” for some of the topics that have been highlighted in the present study.
Study Limitations
This study must be interpreted within the context of its limitations. First, the Delphi methodology has accepted inherent shortcomings. Delphi studies have been criticized because the included items are chosen by the researcher(s), thereby potentially introducing bias. To counteract this, our experts had the opportunity to modify and comment on the statements or suggest additional ones. In this study, all statements were eventually approved after only minor modification through the poll rounds, and no statement was added or removed. Second, since random selection was not feasible, because of the experts’ inclusion criteria, a large pre-selected group of international experts proposed by the Core Team was invited, potentially introducing selection bias since they might not fully the real worldwide expertise; however, it is recognized that the pool did not include other acute care non-surgical physicians such as anesthetists or a higher proportion of IRs, and results might also be partly influenced by local regulations and hospital policies. Therefore, generalization especially outside Europe and the United States requires caution as Asia was underrepresented in the panel. Third, the strength of consensus among experts is often considered to represent the same level of evidence as literature-based guidelines, although this might not necessarily hold true because guidelines, which are graded with a definition of strength recommendations, are based on literature analysis, whereas consensuses derived from the Delphi process can only be indicative of hints at good practice. Therefore, consensus statements should only be considered as evidence in progress to be further investigated and confirmed by clinical studies, if possible, and need to be implemented in daily practice with proper clinical judgment. Nonetheless, for clinical scenarios in which high-quality evidence may be difficult to obtain, the recommendations derived from a large body of experts may be seen as an important adjunct to support decision-making. 34 To mitigate this limitation, whenever present, clinical practice guidelines from recognized scientific societies were consulted to ensure that the proposed statements would not be discordant.
Conclusions
At arrival and during both open or endovascular procedures for ruptured AAA, selective use of intra-aortic balloon occlusion is recommended by study panelists, and it should be performed preferably by the treating physician in aortic pathology. Most of the statements in this international expert-based Delphi consensus study might guide current choices for indications, timing, and techniques of ABO in the management of rAAA. Clinical practice guidelines should incorporate dedicated statements that can guide clinicians in decision-making.
Supplemental Material
sj-docx-1-jet-10.1177_15266028231217233 – Supplemental material for An International Expert-Based CONsensus on Indications and Techniques for aoRtic balloOn occLusion in the Management of Ruptured Abdominal Aortic Aneurysms (CONTROL-RAAA)
Supplemental material, sj-docx-1-jet-10.1177_15266028231217233 for An International Expert-Based CONsensus on Indications and Techniques for aoRtic balloOn occLusion in the Management of Ruptured Abdominal Aortic Aneurysms (CONTROL-RAAA) by Mario D’Oria, Rosalba Lembo, Tal M. Hörer, Todd Rasmussen, Kevin Mani, Gianbattista Parlani, Anna Maria Ierardi, Gian Franco Veraldi, Andrea Melloni, Stefano Bonardelli, Sandro Lepidi, Luca Bertoglio, Michele Antonello, Barend Mees, Jonathan Bath, Frederico Bastos Goncalves, Adam W Beck, Sergi Bellmunt, Xavier Berard, Joseph Du Bose, Jacob Budtz-Lilly, Cristiano Calvagna, Martin Czerny, David Dawson, David T McGreevy, George Greenberg, Ajay Savlania, Mark G Davies, Nuno Dias, Mark A Farber, Simone Fajer, Marcelo Ferreira, Marco Franchin, Enrico Gallitto, Ilya Goldin, Tomasz Jakimowicz, Isabelle van Herzeele, Joseph A Hockley, Andrew Holden, Andrea Kahlberg, Kristofer M Charlton-Ouw, Manar Khashram, Drosos Kotelis, Isernia Giacomo, Thomas S Maldonado, Gregory Magee, Blandine Maurel, Luca Mezzetto, Ross Milner, Giuseppe Panuccio, Paivi Helmio, Giovanni Pratesi, Michel M P J Reijnen, Timothy Resch, Vincente Riambau, Benjamin Starnes, Nicla Settembre, Matthew R. Smeds, Salvatore Scali, Anastasios Psyllas, Jonathan Sobocinski, Sundeep Guliani, Glenn Wei Leong Tan, Giovanni Tinelli, Nikolaos Tsilimparis, Santi Trimarchi, Patrick Vriens, Carl Wahlgren, Wouter Van den Eynde, Thodur Vasudevan, Hence JM Verhagen, Sergio Zacà, Nicola Troisi, Anders Wanhainen, Miranda Witheford and Alexander Zimmermann in Journal of Endovascular Therapy
Footnotes
Collaborative Study Group (PubMed indexed list—in alphabetical order)
1. Michele Antonello (
2. Barend Mees (
3. Jonathan Bath (
4. Frederico Bastos Goncalves (
5. Adam W Beck (
6. Sergi Bellmunt (
7. Xavier Berard (
8. Joseph Du Bose (
9. Jacob Budtz-Lilly (
10. Cristiano Calvagna (
11. Martin Czerny (
12. David Dawson (
13. David T McGreevy (
14. George Greenberg (
15. Ajay Savlania (
16. Mark G Davies (
17. Nuno Dias (
18. Mark A Farber (
19. Simone Fajer (
20. Marcelo Ferreira (
21. Marco Franchin (
22. Enrico Gallitto (
23. Ilya Goldin (
24. Tomasz Jakimowicz (
25.
26. Isabelle van Herzeele (
27. Joseph A Hockley (
28. Andrew Holden (
29. Andrea Kahlberg (
30. Kristofer M Charlton-Ouw (
31. Manar Khashram (
32. Drosos Kotelis (
33. Isernia Giacomo (
34. Thomas S Maldonado (
35. Gregory Magee (
36. Blandine Maurel (
37. Luca Mezzetto (
38. Ross Milner (
39. Giuseppe Panuccio (
40. Paivi Helmio (
41. Giovanni Pratesi (
42. Michel M P J Reijnen (
43. Timothy Resch (
44. Vincente Riambau (
45. Benjamin Starnes (
46. Nicla Settembre (
47. Matthew R. Smeds (
48. Salvatore Scali (
49. Anastasios Psyllas (
50. Jonathan Sobocinski (
51. Sundeep Guliani (
52. Glenn Wei Leong Tan (
53. Giovanni Tinelli (
54. Nikolaos Tsilimparis (
55. Santi Trimarchi (
56. Patrick Vriens (
57. Carl Wahlgren (
58. Wouter Van den Eynde (
59. Thodur Vasudevan (
60. Hence JM Verhagen (
61. Sergio Zacà (
62. Nicola Troisi (
63. Anders Wanhainen (
64. Miranda Witheford (
65. Alexander Zimmermann (
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.