
Abstract
Objective:
To conduct a meta-analysis to assess the safety and efficacy of t-Branch off-the-shelf multibranched endograft for the treatment of thoracoabdominal aortic aneurysm (TAAA).
Data Sources:
PubMed, Embase, and Web of Science.
Review Methods:
Online databases were searched from June 2012 to March 2023. The data were pooled together using a random-effects model of proportions. The outcomes overall included technical success, spinal cord ischemia, target vessel occlusion, type I or III endoleak, reintervention, early mortality (30-day), and mid-term outcomes. Subgroup meta-analyses and meta-regression were performed to explore variation among studies.
Results:
A total of 15 studies containing 1238 patients were included in the meta-analysis. The overall study quality assessment was found to be moderate to good. The pooled technical success was 97.0% (95% confidence interval [CI]=95.5–98.6, I2=53.01%, 1185/1238 cases, 15 studies). Overall, early mortality was 7.3% (95% CI=4.4–10.1, I2=74.48%, 124/1238 cases, 15 studies). Early spinal cord ischemia was 13.4% (95% CI=9.6–17.2, I2=67.24%, 160/1238 cases, 15 studies), and early type I or III endoleak was 6.0% (95% CI=3.4–8.5, I2=53.71%, 68/1032 cases, 9 studies). Mid-term outcomes showed target vessel occlusion was 4% (95% CI=1.4–6.5, I2=65.18%, 28/528 cases, 10 studies, 5–21.2 months), type I or III endoleak was 4.7% (95% CI=2–7.5, I2=49.74%, 38/512 cases, 10 studies, 5-21.2 months), reintervention was 11.2% (95% CI=8.1–14.3, I2=31.06%, 85/650 cases, 10 studies, 5–21.2 months), and pooled mortality was 13.9% (95% CI=7.2–20.7, I2=76.32%, 84/550 cases, 11 studies, 5–21.2 months). Meta-regression found a significant linear association between higher technical success and earlier publication year (p=0.014) and studies with anatomic inclusion criteria (p=0.037). Urgent patients (p=0.021) and later publication year (p=0.048) were significantly associated with higher early mortality.
Conclusion:
The use of the off-the-shelf t-Branch multibranched endograft for elective or urgent endovascular TAAA repair is associated with high technical success rates and proved to be safe and effective at early and mid-term follow-up. However, the heterogeneity between the included studies is high, and prospective, randomized studies along with future larger studies with long-term follow-up are needed.
Clinical Impact
The Zenith t-Branch (Cook Medical, Bloomington, Ind) was approved as a commercially available device in Europe in June 2012. Although a decade has past, the outcomes of t-Branch have rarely been synthesized at the global level. This meta-analysis included 15 studies containing 1238 patients. The meta-analyses included technical success, major adverse events, reintervention, early mortality, and mid-term outcomes. The outcome was very meaningful and representative for the use of t-Branch. It is helpful for endovascular surgeons to make decisions on the treatment of TAAA patients.
Keywords
Introduction
Endovascular aortic repair (EVAR) is preferred because it could reduce early morbidity and mortality for high-risk surgical candidates.1,2 In patients presenting with complex abdominal aortic aneurysm (AAA), who demonstrate anatomic features that are not in accordance with the instructions for use (IFU) of available commercial devices (which are designed for implantation below the renal arteries), advanced endovascular techniques are nowadays available that permit minimally invasive treatment of such extensive pathologies. The use of fenestrated endografts has increased rapidly, with high technical success and low mortality and morbidity at centers of excellence.3–5 2019 European Society for Vascular Surgery (ESVS) AAA guidelines recommend fenestrated endografts as the preferred option for complex AAA repair, when feasible. 6 However, thoracoabdominal aortic aneurysm (TAAA) patients have anatomic limitations to fenestrated endografts: first, a wider gap between endografts and aortic wall may decrease the sealing and support force and increase the risk of type III endoleak. Second, a healthy proximal landing zone, such as infra or suprarenal angulation <45°, 7 is necessary. Third, the impact of fenestrations on the stability and sealing of the stent graft system is unknown. 8
The availability of custom-made devices (CMD) could fit most aortic anomalies. Substantial manufacturing delay is an important limitation for CMD, which exposes urgent patients to risk of interval aneurysm rupture. The shortcomings of physician-modified endografts (PMEGs) and in situ fenestration (ISF) include a lack of quality control, learning curve, variability in size, potential contamination risks, and violations of device integrity, as well as legal, regulatory, and reimbursement issues. And the worldwide experience on ISF for TAAA is few published in the available literature, with ultra-brief follow-up. 9 Parallel devices carry high risk of type IA endoleak due to the gaps among parallel grafts, aorta, and main stent graft; moreover, increasing parallel graft number could increase chimney occlusion, type IA endoleak, and mortality risk. 10 This has led to the development of branched-EVAR (B-EVAR) as the technical option of choice for such patients.
Alternative off-the-shelf (OTS) B-EVAR devices have also been reported, such as inner-branched devices. The E-nside Multibranch stent-graft system (Artivion, Kennesaw, Georgia), with 4 antegrade oriented inner branches, is a new OTS device commercially available in Europe in 2020; only preliminary experiences are reported at present.11–13 The Gore Excluder Thoracoabdominal Branch Endoprosthesis (TAMBE; W.L. Gore & Associates, Flagstaff, Arizona) is currently restricted to investigational trials.
In 2009, the first results assessing TAAA patient eligibility for the use of standardized OTS multibranched endografts were reported. 14 In addition to no manufacturing delay, the complexity of the procedure, the branch morphology, and the perioperative outcome were similar to those of CMD. 15 The Zenith t-Branch (Cook Medical, Bloomington, Indiana), specifically developed for the treatment of TAAA, was approved as a commercially available device in Europe in June 2012. It has a standard tapered configuration with 4 downward cuffed branches for the celiac artery, superior mesenteric artery, and 2 renal arteries, which are matched according to the clock position of the target vessel take-off from the aorta. The device characteristics and deployment technique have been described in detail in many studies.16,17 Although a decade has past, the outcomes of t-Branch have rarely been synthesized at the global level, the meta-analysis aims to assess the safety and efficacy of t-Branch for the treatment of TAAA on early and mid-term outcomes.
Materials and Methods
Search Strategy
This meta-analysis was registered in PROSPERO (CRD42023412830). The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 18 statement and Meta-analyses Of Observational Studies in Epidemiology (MOOSE) 19 guidelines were followed in the review. Two researchers searched PubMed, Embase, and Web of Science using various combinations of key words, including “t-Branch,” “multibranch,” “off the shelf,” “endovascular,” “endograft,” and “aneurysm.” For PubMed and Embase, we used both controlled vocabulary and text words for synonymous terminology within titles and abstracts in the development of search strategies. Web of Science was searched using only text word searches of titles and abstracts. The search strategy contained 2 concepts that were linked together with the AND operator. Detailed search strategies are shown in Supplementary Table 1. In addition, a reference search was carried out to identify additional publications by screening reference lists.
Eligibility Criteria
Studies reporting on patients submitted to TAAA repair with t-Branch were included. Patients with previous aortic surgery or left common carotid artery-left subclavian artery (LCCA-LSA) bypass in different stages were accepted. Only studies reporting the use of the t-Branch to reconstruct visceral arteries (renal artery, superior mesenteric artery, celiac artery) were included, and the number of target vessel was not restricted. All study designs were included if they provided baseline details and follow-up outcomes. Only studies published after June 2012 were included when the CE mark approved the t-Branch. For studies that were conducted for both t-Branch and other techniques, the data of t-Branch had to be disaggregated and extractable. This meta-analysis included only published studies that were written in the English language.
Conference abstracts, case series with 10 or fewer cases, and animal studies were excluded. Studies reporting on the same population and period were excluded. In addition, the studies were excluded if specific and independent information was not given regarding t-Branch. For multiple articles that used data from the same investigation (duplicates), the one with the most comprehensive results or the largest sample size was kept. Studies that met none of the inclusion criteria or any of the exclusion criteria were excluded.
Study Selection, Data Collection Process, and Synthesis
After removing duplicates from different online databases, 2 reviewers independently screened the titles and abstracts of all retrieved records from the literature search, and the third reviewer intervened in case of dispute arising and served as final arbitrator. Three reviewers assessed the eligibility of potentially relevant articles in full text against the selection criteria, with disagreements being resolved by a fourth reviewer served as the final arbitrator. For studies reporting on aortic repair using other techniques, such as fenestration or chimney endografts, only the data reporting the patients treated with a t-Branch were collected; otherwise, the study was excluded. If needed, additional information was sought from the corresponding author by e-mail to resolve questions about eligibility. The motives were recorded for exclusion only at the full-text screening stage. None of the reviewers were blinded to the journal titles, study authors, or institutions.
Data were independently extracted from the included articles by 2 reviewers. The collected information included authors, publication year, countries, study design, study period, number of participants, number of t-Branch, inclusion and exclusion criteria, definitions, participant demographics, and baseline characteristics, including age, gender, smokers, hypertension, hyperlipidemia, diabetes mellitus, coronary artery disease (CAD), chronic kidney disease (CKD) with glomerular filtration rate (GFR) or creatinine (Cr), chronic cerebrovascular disease (CVD), chronic obstructive pulmonary disease (COPD), previous aortic surgery, American Society of Anesthesiologists (ASA) score, and body mass index (BMI); anatomic characteristics and perioperative outcomes, including aneurysm location and type, aneurysm size, proportion of dissection, urgency (elective, urgent, rupture), staged approach, additional devices (iliofemoral conduit, proximal thoracic grafts, distal aortic-iliac components), additional procedures (cerebrospinal fluid drainage), aortic length of coverage, number of target vessel, operation time, fluoroscopy time, contrast use, blood loss, technical success, intensive care unit (ICU) stay, and hospital stay; major adverse events, reintervention (aortic, target vessel, or graft related), early mortality (≤30 days), and mid-term (from 30 days to 5 years) outcomes.
Technical success was defined as successful access, endograft, and bridging stent implantation, with exclusion of the aneurysm and patency of all target vessels, without type I or III endoleak. 20 Aneurysm-related mortality was defined as death owing to a primary or secondary procedure related to the t-Branch, or death owing to surgical conversion. Major adverse events included myocardial infarction, respiratory failure requiring prolonged (>24 hours from anticipated) mechanical ventilation or reintubation, renal function decline resulting in >50% reduction in baseline eGFR or new-onset dialysis, spinal cord ischemia (SCI), stroke, occlusion of target vessel, type I or III endoleak, and conversion to open repair. Thoracoabdominal aortic aneurysms were classified according to the Crawford classification as extent I-V. 21 Elective patients defined as asymptomatic patients with a maximum TAAA diameter of <80 mm; urgent patients defined as symptomatic TAAAs (pain, peripheral embolization) or asymptomatic TAAAs with a maximum diameter of >80 mm; and emergent patients defined as ruptured TAAA.22,23
The outcome rates in TAAA patients using t-Branch were estimated for each study and reported as the proportion of patients with the corresponding outcome. The meta-analyses included technical success, major adverse events, reintervention, early mortality, and mid-term outcomes.
Study Quality and Publication Bias
Study quality assessment was performed following the IHE (Institute of Health Economics) quality appraisal checklist, 24 assessing the following domains: study objective; study design; study population; intervention and cointervention; outcome measure; statistical analysis; results and conclusions; and competing interests and sources of support. Funnel plot and Egger’s test were used to evaluate publication bias in analyses with 10 or more included articles.
Meta-regression and Subgroup Analyses
When 10 or more studies were included, meta-regression and subgroup analyses were used to investigate potential sources of heterogeneity between the studies. Crude meta-regression analysis was performed by including the study characteristics one at a time as variates in the meta-regression model. Characteristics considered included publication year, demographics, comorbidities, urgency, anatomic characteristics such as mean aneurysm diameter and target vessels, perioperative characteristics such as the use of cerebrospinal fluid drainage or not, mean operation time, and hospital stay. For each subgroup, at least 3 studies should be available.
Statistical Analysis
Data were analyzed using Stata version 16.0 (Stata Corp) and R version 4.2.3 (R Foundation for Statistical Computing) using the “meta” package 6.2-1. Heterogeneity was estimated using the I2 test. Because of high heterogeneity as expected and observed, a random-effects (Der Simonian and Laird method) meta-analysis was used for t-Branch with 95% CIs throughout this study. 25 To examine whether single studies had a disproportionally excessive influence, a leave-one-out sensitivity analysis was applied for each meta-analysis. 26
Results
Included Studies
A total of 1307 studies were identified from various online databases, including 369 records in PubMed, 614 records in Embase, and 321 records in Web of Science. Three records were identified in references. After removal of duplicate publications and publications before June 2012, 315 potentially eligible studies were identified in the literature search by reviewing titles and abstracts. A total of 40 relevant articles were further evaluated by reviewing full-text articles. Then, 22 articles were deemed relevant to be included in the systematic review. Among them, Bosiers et al, 16 Fernandez et al, 27 Gallitto et al, 28 and Spanos et al,29–31 were excluded for duplication. Reilly et al 32 and Walker et al 33 were from the same center, and only the former was included for more useful data. Eleshra et al studied t-Branch in 202034 and 202222; the former focused on multicenter patients with previous EVAR, while the latter was a single-center study, and both were included due to few duplication. Finally, 15 articles22,23,32–45 were included in the meta-analysis. Flow diagram for the literature search for the outcomes of the t-Branch off-the-shelf multibranched endograft for TAAA is shown in Figure 1.
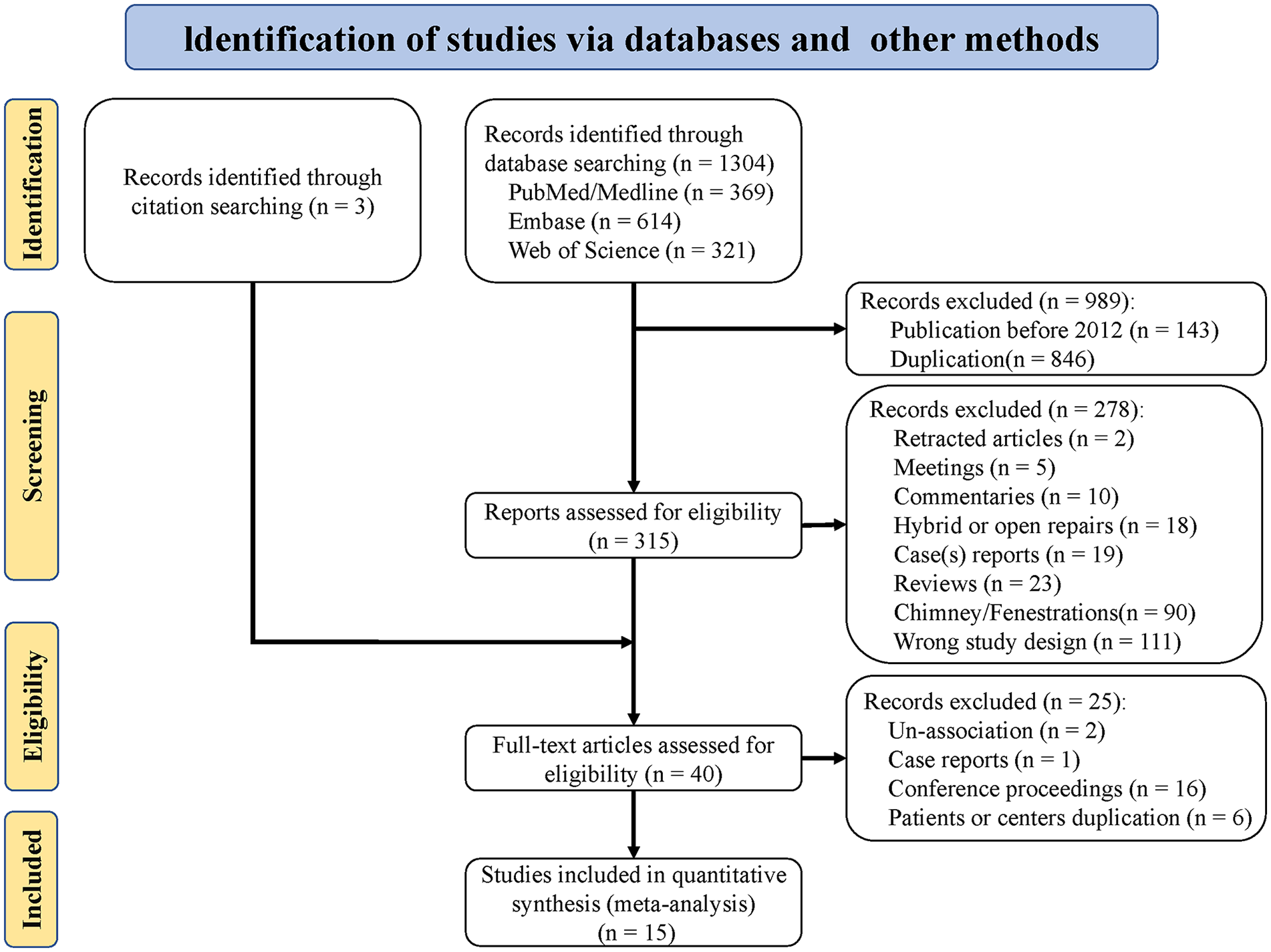
Flow diagram for the literature search for the outcomes of the t-Branch off-the-shelf multibranched endograft for thoracoabdominal aortic aneurysm.
Study Characteristics and Demographic Data
The baseline, anatomy, and intraoperative characteristics of the 15 eligible studies are shown in Table 1. Overall, the sample sizes of the included studies ranged from 11 to 542 patients. A total of 1238 patients underwent t-Branch implantation in the thoracoabdominal aorta. In a total of 15 included studies, 5 studies34,41–44 reported the use of t-branch in a small number of J/PAAA (juxtarenal/paravisceral AAA) patients. A proportion of J/PAAA patients were 8.3% (103/1238) in all included patients. The mean aneurysm diameter ranged from 60.4 to 79 mm, except for one not mentioned. 37 Among all eligible studies, 10 studies32,35–37,39–43,45 definitely emphasized anatomic inclusion criteria for t-Branch. Seven studies32,35,38–40,43,45 reported that 118 patients underwent a staged approach. Twelve studies22,23,32,34,35,39,41–45 reported that the patients were treated in either an elective or urgent setting, 2 studies only reported elective patients,36,37 1 study only reported urgent patients, 38 and 1 study did not mention urgency. 40 The overall mean target vessel per patient ranged from 3 to 4. The mean follow-up ranged from 5 to 21.2 months. The greater baseline, anatomy, and intraoperative characteristics are detailed in Supplementary Tables 2 and 3.
The Baseline, Anatomy, and Intraoperative Characteristics of the 15 Included Studies.
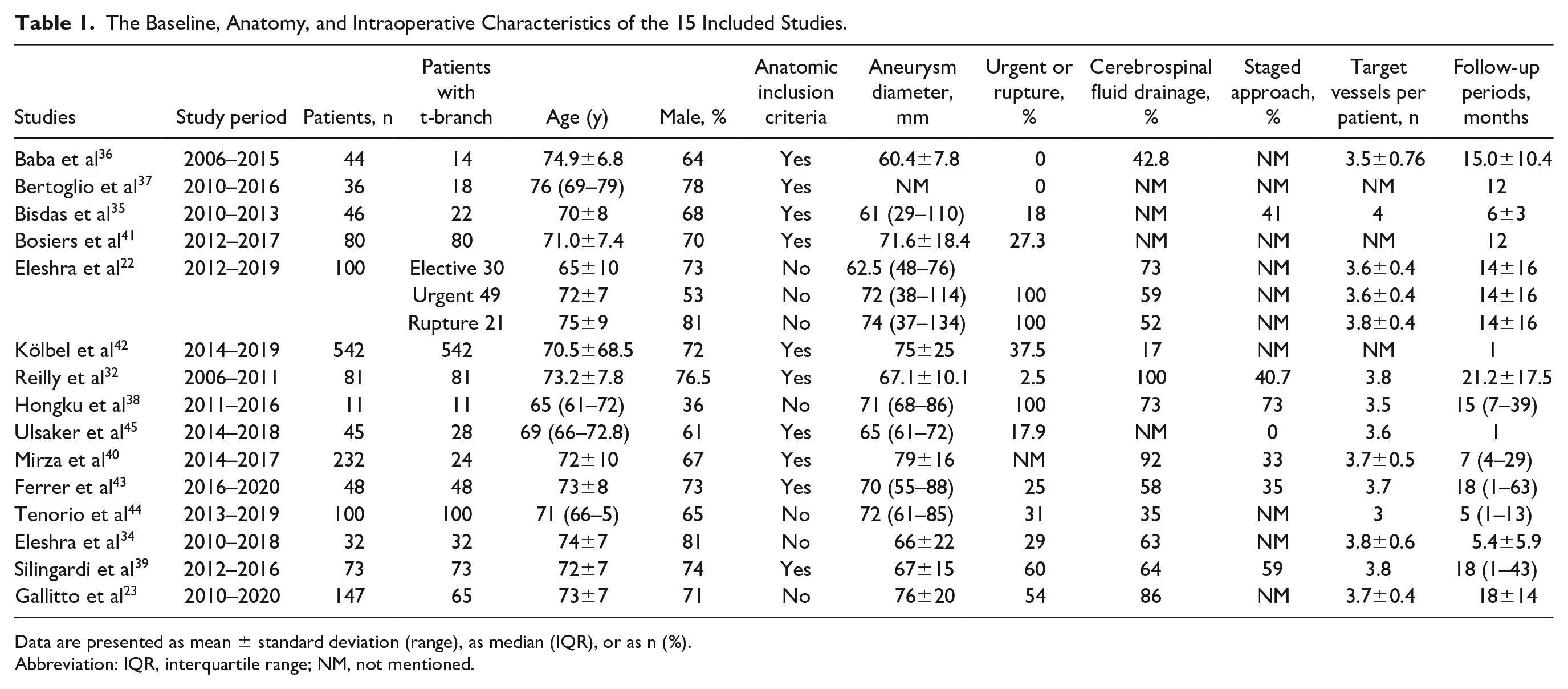
Data are presented as mean ± standard deviation (range), as median (IQR), or as n (%).
Abbreviation: IQR, interquartile range; NM, not mentioned.
Study Quality Assessment
The quality of the included studies assessed through the IHE checklist is shown in Supplementary Figure 1. The obtained scores ranged between 14 and 17 points out of 20, indicating that the general quality of the included studies was moderate to good.
Meta-analysis
Technical success
The pooled technical success was 97.0% (95% CI=95.5–98.6, I2=53.01%, 1185/1238 cases, 15 studies). Subgroup meta-analyses showed technical success of studies with anatomic inclusion criteria was 98.2% (95% CI=96.7–99.6, I2=40.91%, 902/930 cases, 10 studies), and studies without anatomic inclusion criteria were 94.4% (95% CI=91.0–97.7, I2=53.63%, 283/308 cases, 5 studies) (Figure 2).
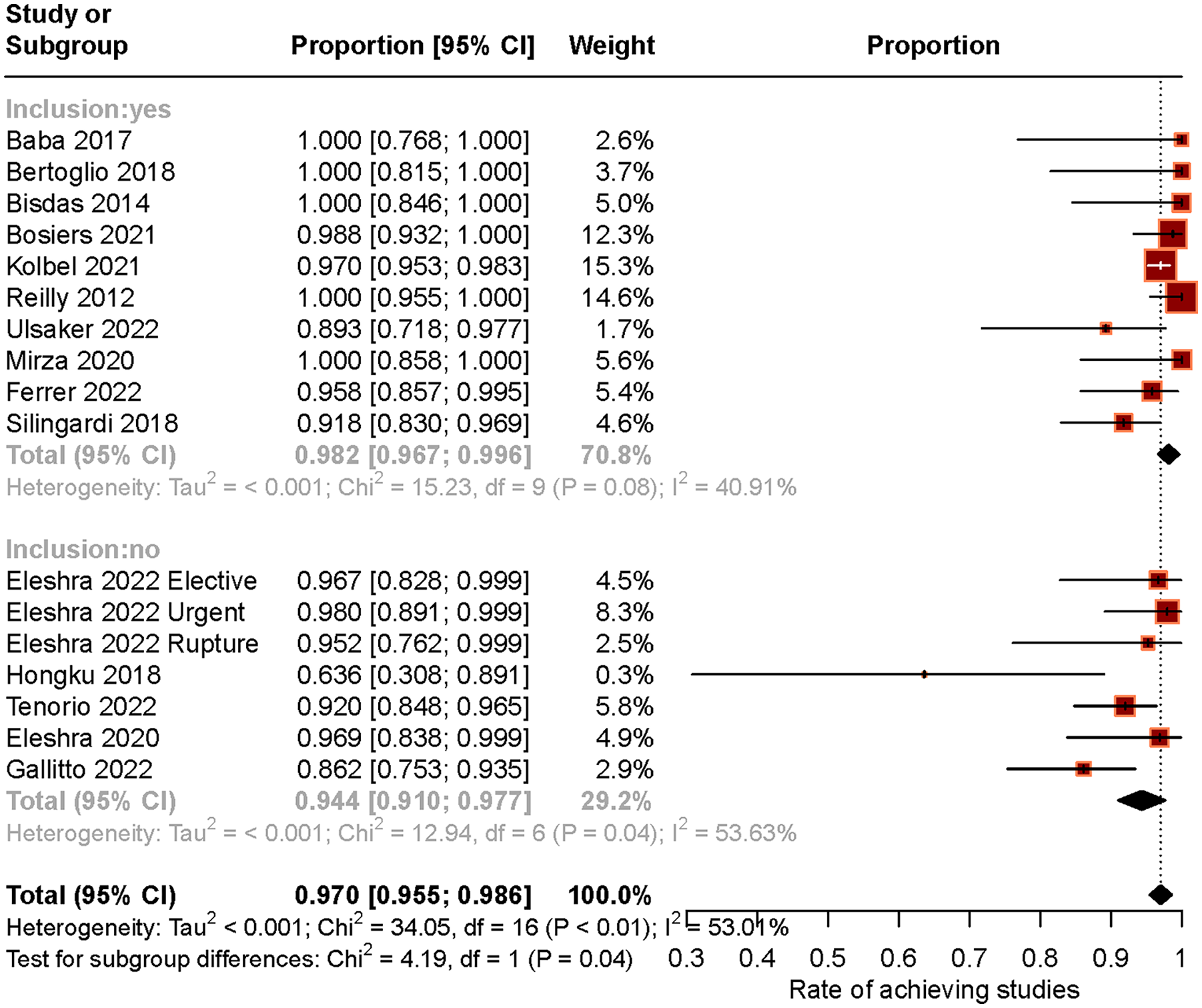
Technical success and subgroups with (out) anatomic inclusion criteria. CI, confidence interval.
Early (30-day) mortality
Overall, early mortality was 7.3% (95% CI=4.4–10.1, I2=74.48%, 124/1238 cases, 15 studies) (Figure 3), with aneurysm-related mortality of 0.7% (95% CI=0–1.7, I2=0%, 17/564 cases, 12 studies) (Supplementary Figure 2). Elective subgroup meta-analyses showed that mortality was 4.8% (95% CI=1.6–8.1, I2=0%, 9/171 cases, 5 studies). Urgent subgroup meta-analyses showed that mortality was 19.1% (95% CI=10.6–27.6, I2=0%, 16/81 cases, 2 studies).
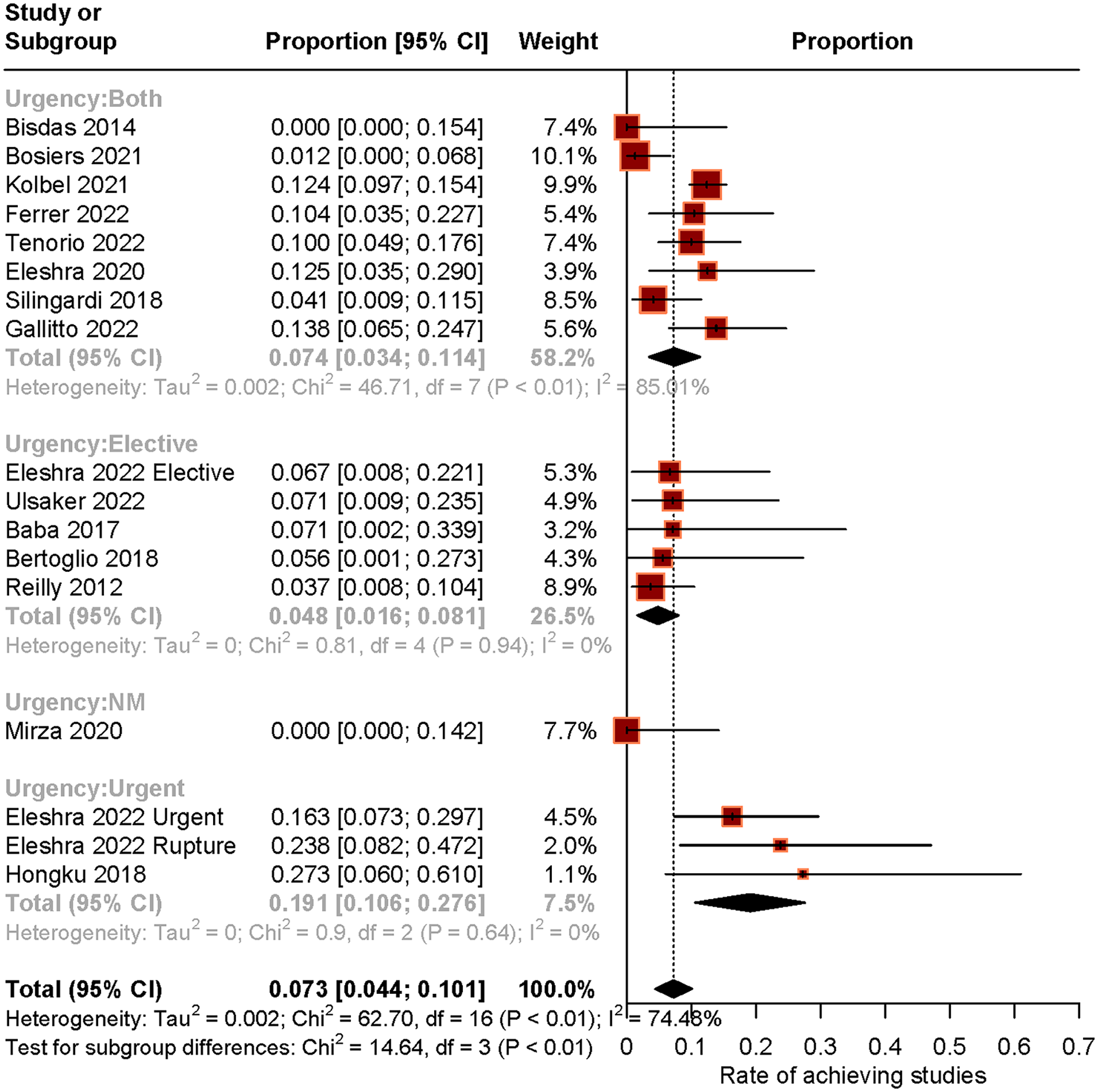
Early mortality and subgroups of urgency. CI, confidence interval.
Mid-term mortality
Eleven studies described the number of deaths from 30 days to 5 years after EVAR/thoracic endovascular aortic repair (TEVAR). The pooled mortality was 13.9% (95% CI=7.2–20.7, I2=76.32%, 84/550 cases, 11 studies, 5–21.2 months) (Figure 4). Aneurysm-related mortality was 0.9% (95% CI=0–1.9, I2=0%, 6/442 cases, 5–21.2 months) (Supplementary Figure 3).
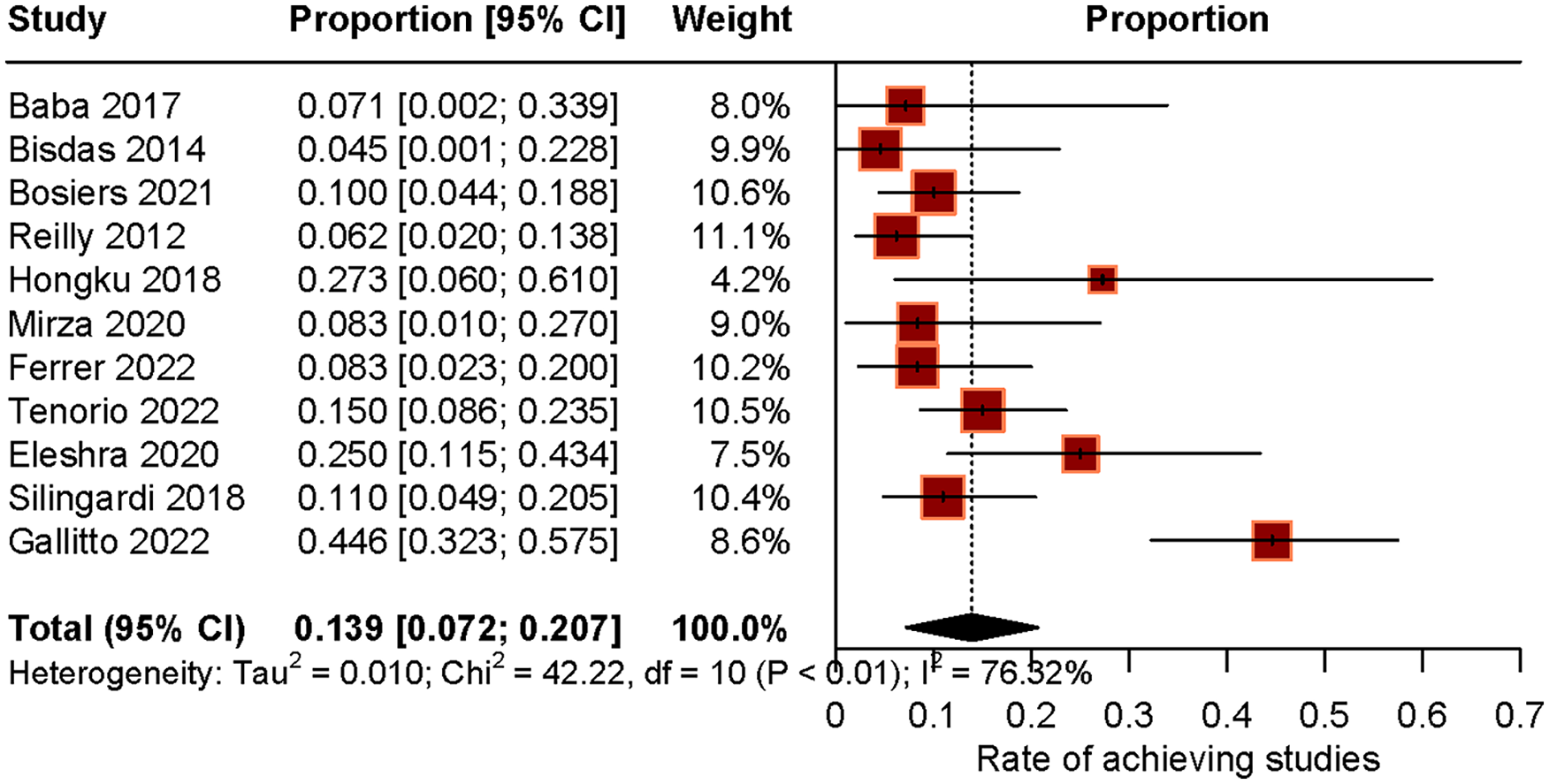
Mid-term all-cause mortality. CI, confidence interval.
Spinal cord ischemia
The early SCI was 13.4% (95% CI=9.6–17.2, I2=67.24%, 160/1238 cases, 15 studies) (Supplementary Figure 4). The pooled prevalence of permanent paraplegia was 1.5% (95% CI=0.2–2.7, I2=55.27%, 38/1200 cases, 13 studies, 5–21.2 months) (Supplementary Figure 5).
Target vessel occlusion
The early target vessel occlusion was 1.6% (95% CI=0.9–2.4, I2=33.26%, 32/1092 cases, 12 studies) (Supplementary Figure 6). Among them, the proportion of occlusion of SMA (n=3) or celiac arteries (n=5) was 0.5% (95% CI=0–1.1, I2=0%, 8/992 cases, 11 studies) (Supplementary Figure 7). All 3 patients with occlusion of SMA showed evidence of ischemic events.
The mid-term results of target vessel occlusion are shown in Supplementary Figure 8. The pooled target vessel occlusion was 4% (95% CI=1.4–6.5, I2=65.18%, 28/528 cases, 10 studies, 5–21.2 months). Among them, 0.4% (95% CI=0–1.3, I2=0%, 7/480 cases, 9 studies) of occluded arteries are SMA (n=2) and 5 of celiac arteries (n=5) (Supplementary Figure 9).
Type I or III endoleak
The early type I or III endoleak was 6.0% (95% CI=3.4–8.5, I2=53.71%, 68/1032 cases, 9 studies; Supplementary Figure 10).
Mid-term results of type I or III endoleak are shown in Supplementary Figure 11. The pooled type I or III endoleak was 4.7% (95% CI=2–7.5, I2=49.74%, 38/512 cases, 10 studies, 5–21.2 months).
Other major adverse events
The meta-analyses and subgroup meta-analyses of stroke, myocardial infarction, respiratory failure, and renal dialysis early outcomes are shown in Supplementary Figures 12–15. Overall, early stroke was 2.6% (95% CI=1.6–3.6, I2=0%, 36/1112 cases, 11 studies), early myocardial infarction was 2.0% (95% CI=1.1–2.8, I2=0%, 30/1163 cases, 11 studies), early respiratory failure was 6.4% (95% CI=3.6–9.2, I2=66.17%, 66/1163 cases, 11 studies), and renal dialysis was 4.1% (95% CI=3.0–5.3, I2=0%, 59/1188 cases, 13 studies). In addition, open conversion during follow-up was reported in 10 studies, but only 1 patient experienced conversion. 22
Reintervention
The pooled early reintervention was 11.5% (95% CI=4.6–18.3, I2=80.65%, 87/928 cases, 8 studies) (Supplementary Figure 16). The mid-term reintervention was 11.2% (95% CI=8.1–14.3, I2=31.06%, 85/650 cases, 10 studies, 5–21.2 months) (Supplementary Figure 17).
Sensitivity Analysis and Publication Bias
Sensitivity analysis and publication bias for each meta-analysis are shown in Table 2. The range of sensitivity analysis after removing a single study at one time showed that no single study had an excessive influence on the pooled results. Funnel plot (Supplemental Figure 18A–D) and Egger’s test showed publication bias in technical success (t=−2.25, p=0.04), early SCI (t=3.04, p=0.008), early target vessel occlusion (t=2.95, p=0.012), and mid-term target vessel occlusion (t=5.34, p<0.001).
Sensitivity Analysis and Publication Bias for Each Meta-analysis.
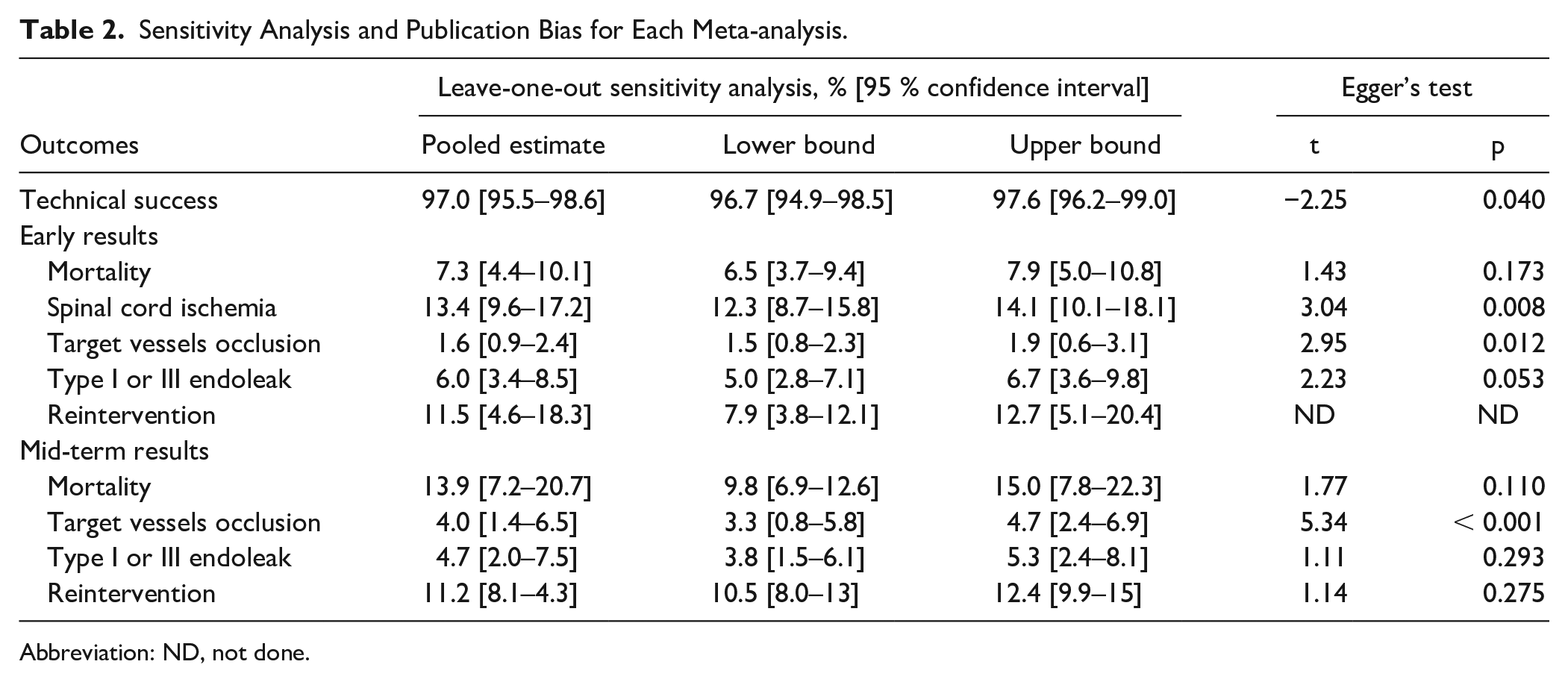
Abbreviation: ND, not done.
Meta-regression
Meta-regression was performed to explore variation in technical success, early mortality (Figure 5A–D), and mid-term mortality. In technical success outcome, earlier publication year (coefficient=−0.004, 95% CI=−0.0068 to −0.0008, p=0.014, R2=73.92%) and studies with anatomic inclusion criteria (coefficient=0.034, 95% CI=0.002–0.065, p=0.037, R2=40.66%) were significantly associated with higher technical success. In early mortality outcomes, urgent patients (coefficient=0.12, 95% CI=0.19–0.23, p=0.021, R2=20.18%) and later publication year (coefficient=0.008, 95% CI=0.001–0.017, p=0.048, R2=18.52%) were significantly associated with higher early mortality. For mid-term mortality, no significant association was observed in follow-up time (coefficient=0.0014, 95% CI=−0.011 to 0.014, p=0.825, R2=0%).
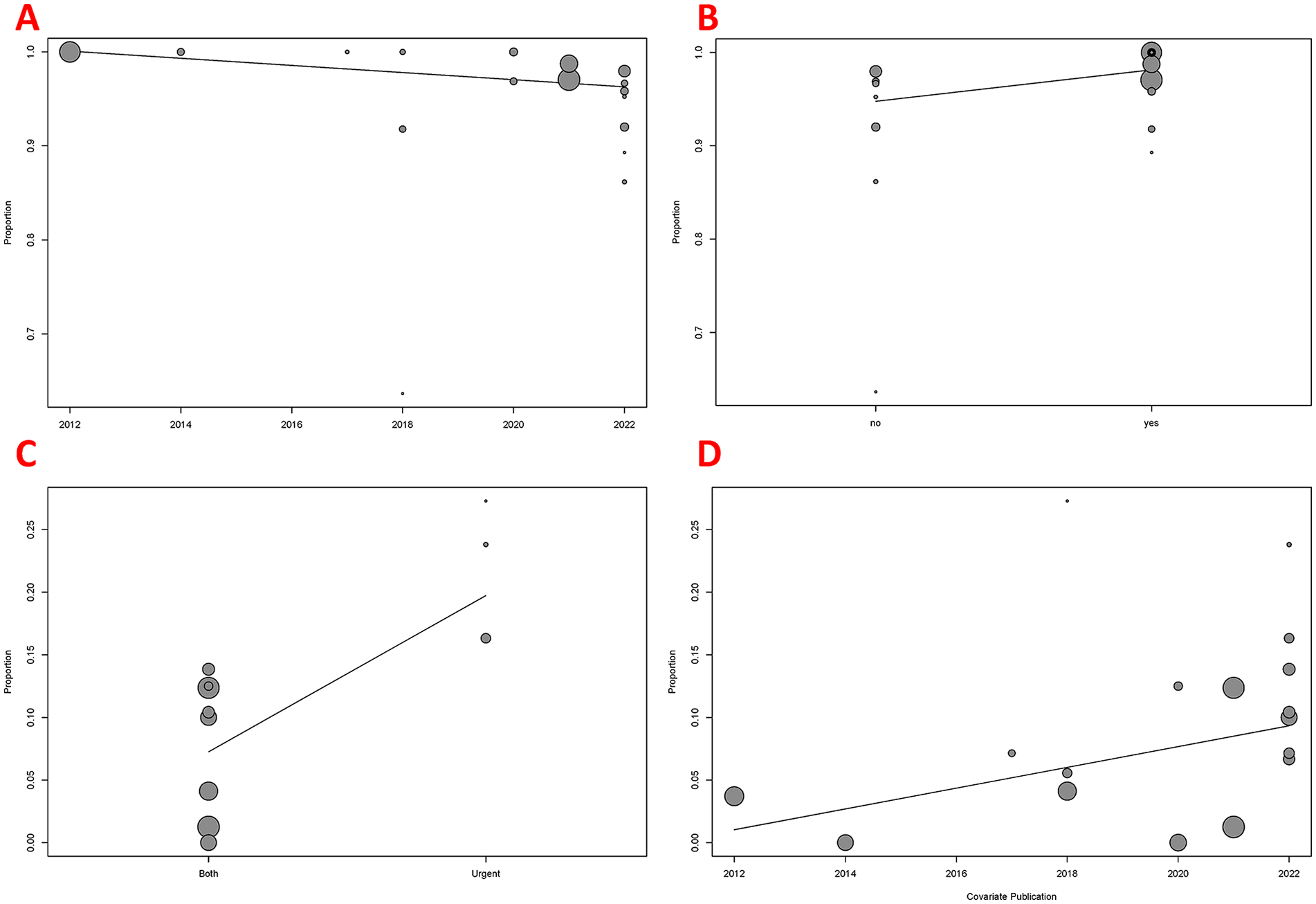
Meta-regression results in technical success and early mortality outcomes: (A) technical success outcome among different publication year; (B) technical success outcome between studies with and without anatomic inclusion criteria; (C) early mortality outcome between studies only including urgent (and/or ruptured) patients and studies including elective urgent (and urgent/ruptured) patients; and (D) early mortality outcome among different publication year.
Discussion
This pooled systematic review and meta-analysis of available online data on t-Branch showed high technical success and acceptable outcomes regarding major adverse events, reintervention, and mortality in early and mid-term follow-up.
The pooled technical success was 97%, which was similar with PMEG and CMD reported technical success as 97.2% 46 and 98% 47 for TAAA or J/PAAA patients. In the meta-regression, interestingly, earlier publication had a higher technical success. Maybe previous researchers screened candidates more conservatively to this new stent graft. Meta-regression also showed anatomic inclusion criteria for t-Branch was another factor improving technical success. Patients treated outside the instructions for use were more technically demanding. 22 It was reported that the anatomical suitability of the t-Branch ranged from 47% to 88%.14,48–50 These values could be increased by some adjunctive maneuvers, such as using low-profile endografts, iliac conduits, iliac bypass for device insertion, target vessel stenting treating stenosis, carotid-subclavian bypass for a proximal landing zone, and distal sealing with a straight aortic cuff in healthy infrarenal aorta for deployment distal body endograft.48,49,51 Hongku et al 38 performed 11 ruptured TAAAs using the t-Branch, and only 2 patients complied with the anatomical instructions for use of the device, which might cause its technical success as low as 64%.
It seemed feasible to use t-Branch for urgent or ruptured patients who could not wait for a CMD for up to 8 weeks. 52 Not surprisingly, early mortality was higher in the urgent subgroup (19.1% vs 4.8% for the elective subgroup). Stable patients were more capable of tolerating a time-consuming complex operation. However, pooled aneurysm-related mortality was rare, with 0.7% and 0.9% subgroups in early and mid-term results. The results were consistent with the recent 2022 ACC/AHA (American Heart Association/American College of Cardiology Joint Committee) guideline which recommended an off-the-shelf or modified device was considered for higher-risk patients who presented with symptomatic or contained ruptured aneurysms, were hemodynamically stable, and had suitable anatomy. 53 Later publication year was another factor associated with higher early mortality. This might be because later studies recruited more urgent and rupture patients (Supplementary Figure 19).
In this meta-analysis, the most frequent pooled major adverse event was SCI, with a mean of 13.4% of patients. Long sacrifice of healthy aorta and intercostal arteries for adequate deployment were important drawback of the t-Branch compared with open repair, 37 and CMD. 54 Bertoglio et al 37 found the length of sacrificed healthy aorta was 49 mm in t-Branch and 14 mm in open repair (p<0.001), and intercostal arteries lost was also higher in t-Branch group (4 pairs), comparing with open repair group (2 pairs; p=0.004). Spath et al 54 found that compared with CMD, OTS devices required a mean of 74±19 mm of additional proximal healthy aortic coverage (CMD: 33±19 mm vs OTS: 108±6 mm; p<0.001), as well as an average sacrifice of 2.5 additional segmental arteries (CMD: 1.3±0.8 vs OTS: 3.8±0.9; p<0.001). Long sacrifice of healthy aorta was the important risk for SCI, with a mean length of 180 to 435 mm reported in included studies.35,36,39,45 And there was general consensus that patients with shorter (≤150 mm) stent graft lengths were at lower risk for SCI.55,56 Moreover, patients with previous thoracic aorta repair, left common carotid, and subclavian repair were accepted in the meta-analysis, which might increase the risk of SCI. Spinal cord ischemia usually occurred within the first few days, 57 and luckily, most of them were transient and resolved spontaneously. The pooled permanent paraplegia was 1.5%. The use of preoperative cerebrospinal fluid drainage was reported in all included studies though based on different applicable standards. The largest randomized controlled trial containing 145 TAAA patients proved that cerebrospinal fluid drainage was significantly lower than the control (2.6% vs 13.0%, p=0.03). 58 However, the main controversy with cerebrospinal fluid drainage was that it was not a safe procedure and could be associated with a high incidence of drain-related complications.59,60 And the SVS (Society for Vascular Surgery) guidelines assigned prophylactic cerebrospinal fluid drainage a I B recommendation for SCI protection in TEVAR cases that were deemed high risk. 20 Additional measures reducing SCI included preservation of antegrade perfusion of the left subclavian artery and at least one hypogastric artery, staging the coverage of large segments of the aorta, minimization of lower limb ischemia reperfusion injury, or even purposeful spinal artery embolization.61,62 Eleshra et al 22 tried to prevent SCI by using a 2-in-1 stent graft, and it included outer and inner stent grafts of different diameters. The outer stent graft was designed to cover as many intercostal arteries as possible in the first stage of TAAA repair to effectively precondition the spinal cord.
The worsening of renal function was also frequent and reported in a mean of 3.3% to 30% of cases.23,34,36,41 Possible reasons included preoperative renal insufficiency, contrast use, technical complexity, and embolization/infarct during the procedure. Although we could not conduct a corresponding meta-analysis due to the various definitions of renal function deterioration among the included studies, overall renal dialysis was found in 4.1% of patients. Renal vessel occlusion was another factor worsening renal function during follow-up. And renal vessel occlusion was 4 times as many as visceral vessel occlusion in our meta-analysis. A previous study found renal occlusion following branched devices was significantly higher than that following fenestrated devices. 63 The mid-term target vessel occlusion rates were 4%, comparable with the CMD of target vessel occlusion, approximately 3%. 64 Two meta-analyses have reported a pooled primary target vessel patency rate of 98.9% for PMEG 46 and 98% 65 for fenestrated stent grafts. In the setting of TAAA, there was not any other option than use of branches, as fenestrations need to be closely aligned with the target vessels. Urgent-emergent settings were another likely that many non-elective cases had challenging anatomies, 38 and this could have influenced the target vessel occlusion. The loss of visceral vessels may be devastating, resulting in ischemic bowel and/or patient mortality. Fortunately, the occlusion of visceral vessels was rare, with 0.5% of early outcome and 0.4% of mid-term outcome. The use of a balloon-expandable endoprosthesis 66 or combination with a distal self-expandable endoprosthesis 67 could improve the patency of target vessel. But the meta-regression or subgroup meta-analysis regarding the type of bridging stents was not conducted because of rarely reported in included studies.
Endoleak was a sign that the aortic aneurysm failed to be isolated from the systemic circulation. Type I or III endoleak even represented technical failure. The early and mid-term type I or III endoleak rate was 6.0% and 4.7%, which seemed better than PMEGs reporting type I or III endoleak was 9.0%. 46
A high reintervention was observed, with overall rates of 11.2% and 11.5% in early and mid-term follow-up periods. It was comparable with 12.3% of PMEGs 46 and 13% of fenestrated/branched endografts. 65 A previous meta-analysis showed that urgent PMEGs were associated with higher reinterventions (19.1% vs 8.7%). 46 We did not conduct a subgroup meta-analysis or meta-regression for shortage in number of available groups. Surveillance was critical to identify major adverse event after initial placement and to evaluate whether long-term complications appeared. 2021 SVS (Society for Vascular Surgery) guidelines recommended clinical examination and computed tomography (CT) scans at 1 month, 6 months, and yearly thereafter for aneurysm surveillance after EVAR/TEVAR. For emergent indications, earlier evaluation either during hospitalization or within 1 week of placement may be warranted. 20
There was a prior meta-analysis of t-Branch on endovascular repair of TAAA. 68 It identified 7 retrospective studies published before 2018, with only 197 patients. Our meta-analysis, however, included 15 studies and 1238 patients undergoing t-Branch implantation. And our meta-analysis included more later studies (12 studies were published after 2018) and prospective studies (5). Moreover, Meta-regression and subgroup meta-analysis were performed to explore heterogeneities of outcomes of studies.
Limitations
There were many limitations of the pooled analyses. First, there are methodologic limitations of observational studies. Second, many heterogeneities were not extensively considered in the meta-analysis, such as study period, patient selection, outcome definitions, aneurysm type, operator learning curve, and clinical setting. These terms presented bias and limited the applicability of our findings to individual settings. Third, not all included studies reported all outcomes, and some subgroup analyses might have limited power.
Conclusions
The use of the off-the-shelf T-Branch multibranched endograft for elective or urgent endovascular TAAA repair is associated with high technical success rates and proved to be safe and effective at early and mid-term follow-up. Overall, there is increasing use of t-Branch for urgent patients; although these subjects might experience higher odds for early mortality, pooled aneurysm-related mortality is low. However, the heterogeneity between the included studies is high, and prospective, randomized studies along with future larger studies with long-term follow-up are needed.
Supplemental Material
sj-docx-1-jet-10.1177_15266028231220322 – Supplemental material for Systematic Review and Meta-analysis of Short-term and Mid-term Outcomes After Use of t-Branch Off-the-shelf Multibranched Endograft for Elective and Urgent Treatment of Thoracoabdominal Aortic Aneurysms
Supplemental material, sj-docx-1-jet-10.1177_15266028231220322 for Systematic Review and Meta-analysis of Short-term and Mid-term Outcomes After Use of t-Branch Off-the-shelf Multibranched Endograft for Elective and Urgent Treatment of Thoracoabdominal Aortic Aneurysms by Yonghui Chen, Zongwei Liu, Shuaishuai Wang, Mario D’Oria, Xiaoxing Zhang, Jiaxue Bi, Dongsheng Cui and Xiangchen Dai in Journal of Endovascular Therapy
Supplemental Material
sj-docx-2-jet-10.1177_15266028231220322 – Supplemental material for Systematic Review and Meta-analysis of Short-term and Mid-term Outcomes After Use of t-Branch Off-the-shelf Multibranched Endograft for Elective and Urgent Treatment of Thoracoabdominal Aortic Aneurysms
Supplemental material, sj-docx-2-jet-10.1177_15266028231220322 for Systematic Review and Meta-analysis of Short-term and Mid-term Outcomes After Use of t-Branch Off-the-shelf Multibranched Endograft for Elective and Urgent Treatment of Thoracoabdominal Aortic Aneurysms by Yonghui Chen, Zongwei Liu, Shuaishuai Wang, Mario D’Oria, Xiaoxing Zhang, Jiaxue Bi, Dongsheng Cui and Xiangchen Dai in Journal of Endovascular Therapy
Supplemental Material
sj-docx-3-jet-10.1177_15266028231220322 – Supplemental material for Systematic Review and Meta-analysis of Short-term and Mid-term Outcomes After Use of t-Branch Off-the-shelf Multibranched Endograft for Elective and Urgent Treatment of Thoracoabdominal Aortic Aneurysms
Supplemental material, sj-docx-3-jet-10.1177_15266028231220322 for Systematic Review and Meta-analysis of Short-term and Mid-term Outcomes After Use of t-Branch Off-the-shelf Multibranched Endograft for Elective and Urgent Treatment of Thoracoabdominal Aortic Aneurysms by Yonghui Chen, Zongwei Liu, Shuaishuai Wang, Mario D’Oria, Xiaoxing Zhang, Jiaxue Bi, Dongsheng Cui and Xiangchen Dai in Journal of Endovascular Therapy
Supplemental Material
sj-docx-4-jet-10.1177_15266028231220322 – Supplemental material for Systematic Review and Meta-analysis of Short-term and Mid-term Outcomes After Use of t-Branch Off-the-shelf Multibranched Endograft for Elective and Urgent Treatment of Thoracoabdominal Aortic Aneurysms
Supplemental material, sj-docx-4-jet-10.1177_15266028231220322 for Systematic Review and Meta-analysis of Short-term and Mid-term Outcomes After Use of t-Branch Off-the-shelf Multibranched Endograft for Elective and Urgent Treatment of Thoracoabdominal Aortic Aneurysms by Yonghui Chen, Zongwei Liu, Shuaishuai Wang, Mario D’Oria, Xiaoxing Zhang, Jiaxue Bi, Dongsheng Cui and Xiangchen Dai in Journal of Endovascular Therapy
Footnotes
Author Contributions
Yonghui Chen: Study design, Data analysis, Writing.
Zongwei Liu: Study selection, Data collection, Data analysis.
Shuaishuai Wang: Study selection, Data collection, Data analysis.
Mario D’Oria: Review.
Xiaoxing Zhang: Study selection.
Jiaxue Bi: Study search.
Dongsheng Cui: Data analysis.
Xiangchen Dai: Final arbitrator, Review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Natural Science Foundation of China projects (No. 82241207 and No. 82070489); Tianjin Health Science and Technology Project (ZC20189); Youth Project of Tianjin Natural Science Foundation (19JCQNJC099000); and Science and Technology Project of Binhai New Area Health Commission (2019BWKQ037).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.