
Abstract
Purpose:
The purpose of this study was to identify the independent predictors of higher patency rates and investigate the selection of specifications of stent graft in the treatment of central venous disease.
Materials and Methods:
This retrospective study included 54 patients who underwent stent–grafts’ placement for the treatment of central venous disease between March 2017 and September 2022 at a tertiary hospital. The demographic data for the patients and the clinical data of the treated lesions were collected and analyzed. The patency rates of the treated lesions with different oversizing range were calculated via the Kaplan-Meier and log-rank analyses. The multivariate Cox proportional hazard models were constructed to identify the independent predictor of the target site primary patency.
Results:
The median follow-up period was 21.5 months. The primary patency rates of the target sites were 90.7%, 72.2%, and 55.1% at 6, 12, and 24 months, respectively. The assisted primary patency rates of the lesions were 96.3%, 92.5%, and 80.3% at 6, 12, and 24 months, respectively. The log-rank analysis showed that the stent–grafts’ placement with small oversizing had significantly higher primary patency rates than those with large oversizing (p=0.022). The multivariate analysis revealed that concomitant stenosis and large oversizing stent graft were the independent predictors of target site primary patency.
Conclusions:
Stent grafts showed reasonable primary patency for the treatment of central venous disease in hemodialysis patients. A stent graft with small oversizing is associated with better target site primary patency rates than those with large oversizing.
Clinical Impact
Stent grafts showed reasonable primary patency for the treatment of central venous disease in hemodialysis patients. Few studies, however, have explored the efficiency of stent grafts to treat CVD by considering different factors such as sizing considerations, the rate of oversizing percentage, etc. A stent graft with small oversizing is associated with better target site primary patency rates than those with large oversizing. Excessive oversizing should be avoided to prevent infolding or stent collapse.
Introduction
Central venous disease (CVD) is a prevalent and significant problem with an incidence of 25% to 40% in patients receiving long-term hemodialysis. 1 Central venous disease disrupts the hemodialysis access circuit, leading to venous hypertension, edema of an ipsilateral extremity, and access flow dysfunction. 1 Central venous disease can lead to loss of limited vascular resources, resulting in increased mortality in patients on dialysis.2,3
The Kidney Disease Outcomes Quality Initiative (KDOQI) guidelines recommend percutaneous transluminal angioplasty (PTA), with or without stent placement, as the preferred approach for the treatment of CVD. 4 However, multiple repeated reinterventions are required for the high recurrence rate, with the 12-month primary patency of PTA ranging from 12% to 50%.2,5–7 A previous meta-analysis also reported that bare metal stents (BMSs) did not improve patency rates compared with PTA for CVD in hemodialysis patients. 7 The KDOQI guidelines 2019 update also indicate that stent grafts may show improved patency for CVD; however, they are based on several small retrospective studies. 4 Recently, several studies have reported outstanding performances of stent grafts in the treatment of CVD.4,8 Stent grafts provide mechanical support and a physical barrier to intimal hyperplasia. The covered segment of the stent graft is unlikely to develop intimal hyperplasia, and restenosis always develops at the proximal and distal ends of the stent.2,4 Few studies, however, have explored the efficiency of stent grafts to treat CVD by considering different factors such as sizing considerations and the rate of oversizing percentage.
Therefore, in this study, we retrospectively reviewed a single institution’s data regarding the use of stent grafts for the treatment of CVD in hemodialysis patients to identify the independent predictors of higher patency rates and provide a single center’s experience for further clinical use of stent grafts.
Materials and Methods
Study Design and Patients
The study was approved by the Institutional Research Board of the hospital, and informed consent was taken from all the patients included in the study. This study retrospectively enrolled the patients on hemodialysis with symptomatic CVD who underwent stent-graft placement between March 2017 and September 2022 at Suzhou Municipal Hospital. The patients with symptomatic central vein occlusion and treated successfully using stent grafts and who have detailed follow-up data were included in this study. The patients with definite venous thoracic outlet syndrome, infection due to dialysis access or systemic infection, severe cardiac insufficiency, or who were treated without stent-graft implantation were excluded from the study. The patients who were lost to follow-up or if the primary patency could not be evaluated for reasons such as stent graft combined with open surgery or unexplained death or kidney transplantation were also excluded from the study. The indications of stent placement were chronic total occlusion, acute elastic recoil of >50%, or symptomatic recurrence within 3 months of a previous successful PTA. The demographic and clinical data as well as the information regarding the treatment of occluded lesions and the stent grafts employed were collected and analyzed.
Stent-Graft Placement Procedure
Preoperative computed tomography angiography was performed to diagnose and preliminarily evaluate the condition of the lesions. The procedures were performed by a well-trained senior vascular surgeon after applying local anesthesia. An ipsilateral basilic vein or cephalic venous approach was used to perform the preliminary digital subtraction angiography, attempting to cross the lesions after the occluded lesion was evaluated. When the lesion was difficult to pass through, the femoral vein approach was used for reverse crossing, and the through-and-through technique or even sharp recanalization technique was used when necessary. Once the occluded segment was crossed, pre-dilation of the target lesion was performed using balloons with slightly smaller or equal diameters to the normal vessels at the distal end (peripheral end) of the lesion segment. The size of the stent graft was chosen based on the diameter of the normal vessels at the distal end of the lesion segment measured through angiography images after pre-dilation. Next, a stent graft was placed to restore the central venous blood flow when the indications for stent implantation were met. If the stent delivery system exceeded the 8F sheath, we preferred to use the femoral vein approach for stent implantation. When the diameter of the target site does not exceed 13 mm, Viabahn endoprosthesis (W. L. Gore & Associates, Flagstaff, Arizona) is placed, otherwise Fluency Plus (CR Bard Angiomed, Karlsruhe, Germany) or Endurant (Medtronic, Minneapolis, Minnesota) abdominal aortic aneurysm (AAA) leg or iliac extender is used. Post-dilatation was not routinely performed after placement of stent graft, and if there is residual stenosis or in-folding, post-dilatation is performed with the same balloon used for pre-dilatation. However, when stent graft was placed with a diameter larger than 13 mm, post-dilatation was always performed using a 14 mm angioplasty balloon. Antithrombotic drugs were not routinely used after the procedures. However, for some patients with comorbidities such as coronary heart disease or arteriosclerosis, or with high-risk factors for thrombosis, oral aspirin treatment was given. Patients were closely followed up via ultrasound examination every 3 months and the monitoring indicators during the regular hemodialysis procedures. The imaging evaluation such as chest CT angiography or venographic surveillance was performed for patients with suspected restenosis, symptom recurrence, or abnormal dialysis monitoring indicators. Endovascular treatment was performed for recurrent symptomatic CVD, if necessary.
Definitions
Technical success is defined as the exclusion of the lesion without significant residual stenosis (≥30%). Primary patency is defined as the interval from the stent-graft implantation until the first reintervention of the treated segment. Assisted primary patency is defined as the stent-graft patency, regardless of the number of further interventions needed. Secondary patency is defined as the permanent loss of flow in the treated segment, irrespective of any interval therapies.4,9 The procedure-related complications were recorded according to the Society of Interventional Radiology (SIR) classification. 10 The percentage of stent-graft oversizing to angiographic reference vessel diameter (RVD) was calculated using the formula: oversize percentage=(nominal stent-graft diameter−RVD)/RVD×100 (%). 11
Statistical Analysis
Statistical analyses were performed via SPSS software (version 17; SPSS, Chicago, Illinois). The Kolmogorov-Smirnov test was used to identify the normality of data. Continuous data were reported as mean±standard deviation if they were normally distributed; otherwise, they were reported as the median and interquartile range (IQR). The post intervention patency rate was plotted as the Kaplan-Meier survival curves using the Graph Pad Prism software (Graph Pad Software, San Diego, California), which was analyzed using the log-rank test. The univariate and multivariate Cox proportional hazard models were performed to detect the independent predictors of stent-graft restenosis and target lesion primary patency. Results were expressed as hazard rate (HR) with 95% confidence intervals (CIs). A p-value of ≤0.05 was considered statistically significant.
Results
A total of 54 patients, including 29 females (53.7%) and 25 males (46.3%), who underwent the placement of stent grafts for the treatment of CVD were included in this study. The demographic and clinical data of the patients are presented in Table 1. The mean age of the patients was 65.02±10.43 years (range=42–87 years). Technical success was achieved in all the patients. The range of target diameters of the treated lesions was 10.71±2.49 mm. The distribution of stent-graft diameters is presented in Table 2. Five patients had their internal jugular veins covered with stent grafts because of the need for treatment, and no complications such as facial edema were observed during the follow-up. The symptoms of all the patients ameliorated within 48 hours after the procedure, and no perioperative mortality was observed. According to the SIR classification, 2 minor complications (SIR classification B) were observed. Minor complications occurred in 2 patients involving hemorrhage of the brachial artery in the process of establishing basilic vein approach and chest pain after the procedure.
Baseline Characteristics of Study Population Receiving Endovascular Treatments With Stent Grafts (N=54).
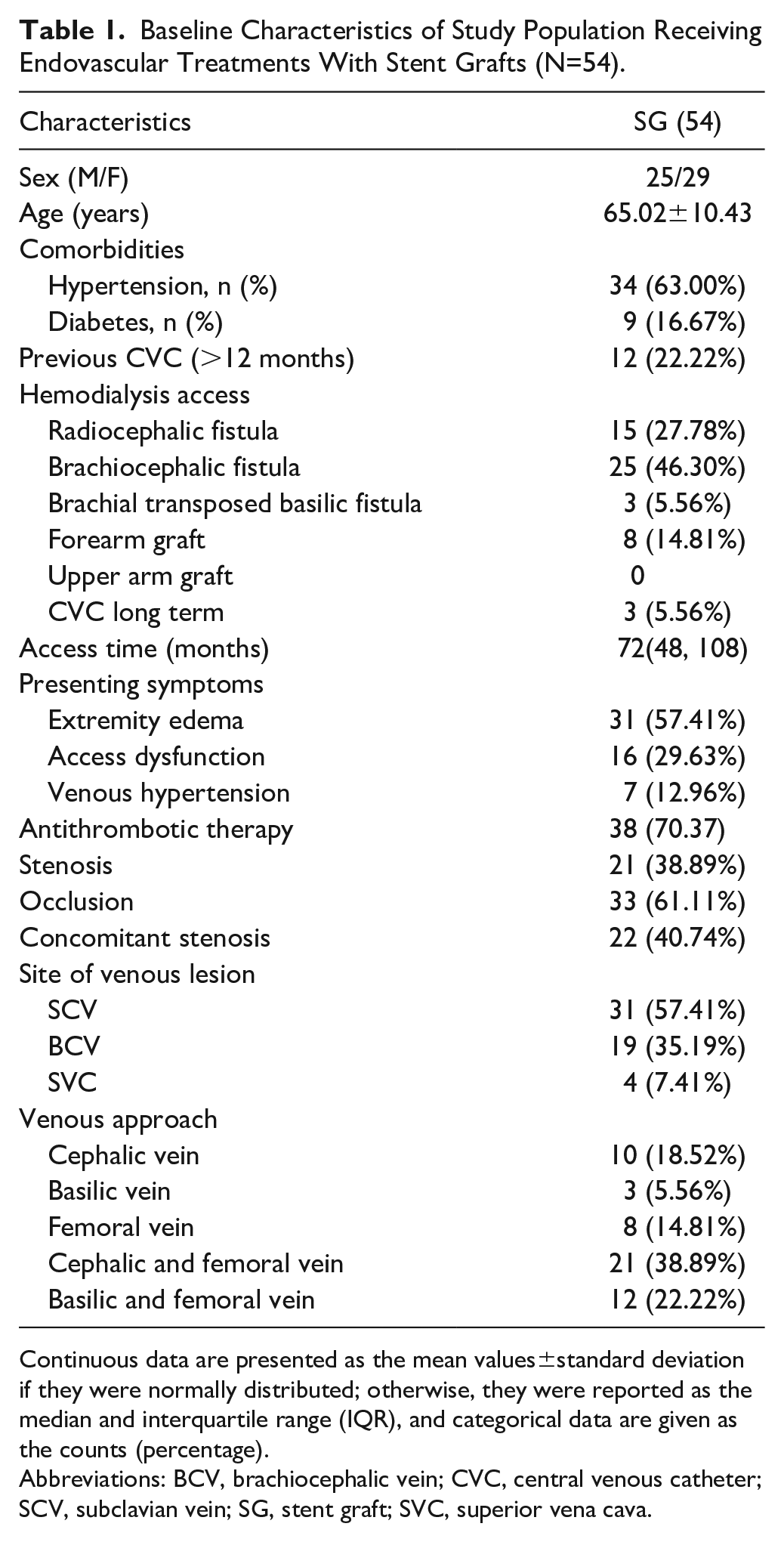
Continuous data are presented as the mean values±standard deviation if they were normally distributed; otherwise, they were reported as the median and interquartile range (IQR), and categorical data are given as the counts (percentage).
Abbreviations: BCV, brachiocephalic vein; CVC, central venous catheter; SCV, subclavian vein; SG, stent graft; SVC, superior vena cava.
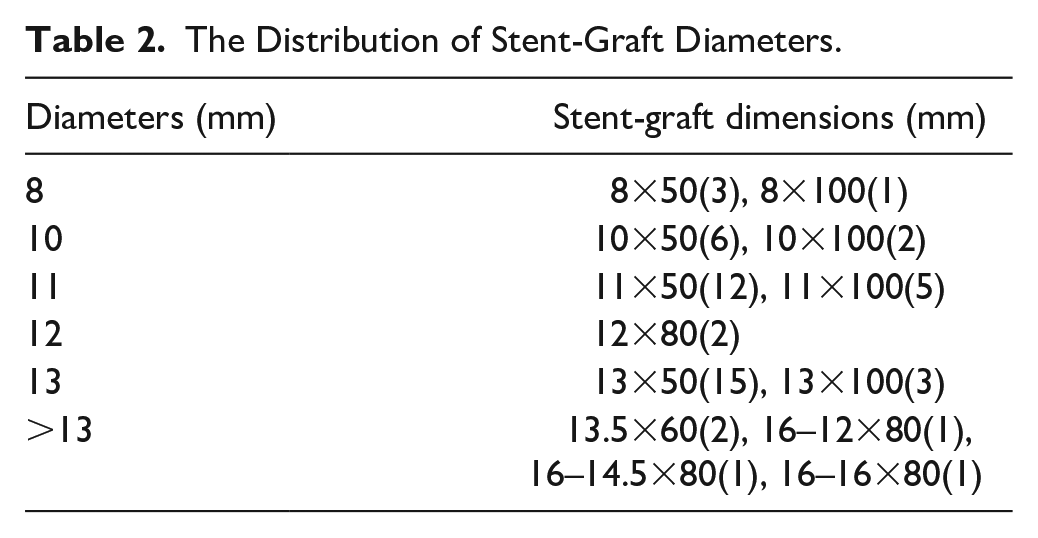
The Distribution of Stent-Graft Diameters.
The median follow-up period was 21.5 months (IQR=14.0-27.0 months). The primary patency rates of the target sites with the placement of stent grafts were 90.7%, 72.2%, and 55.1% at 6, 12, and 24 months, respectively. The assisted primary patency rates of the lesions were 96.3%, 92.5%, and 80.3% at 6, 12, and 24 months, respectively. There were no instances of stent-graft fracture, migration, or stent-related infection during the follow-up period. Most of the stent-graft restenoses (81.5%) observed during the follow-up were stent edge restenosis at the distal end of the stent grafts, as shown in Figures 1 and 2. Considering the small sample size of this study, the median of the oversizing range is used for grouping. The median of the oversizing range was found to be 3.65 (IQR=0.0-21.5). The Kaplan-Meier survival curve of the primary patency of the 2 sets of data grouped by median is shown in Figure 3. The log-rank analysis showed that the stent-graft placement with small oversizing had significantly higher primary patency rates than those with large oversizing (p=0.022). Similarly, the stent-graft placement with small oversizing had significantly higher assisted primary patency rates than those with large oversizing (p<0.05).
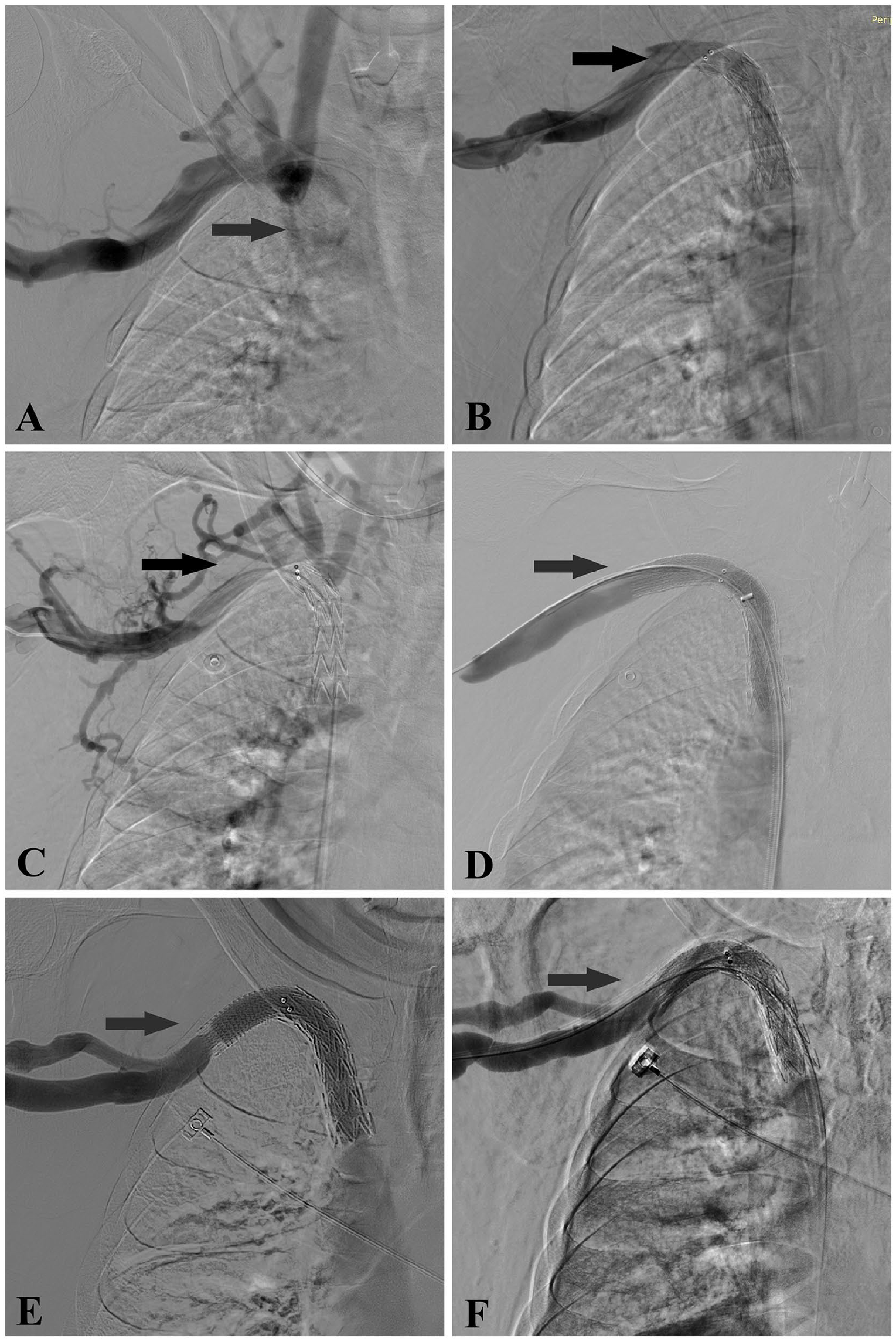
A 72-year-old man with a right forearm radiocephalic fistula constructed for 13 years. Representative angiograms of the stent edge restenosis after the placement of the stent graft. (A) An angiogram showing the brachiocephalic vein occlusion accompanied by an obvious collateral vein formation (arrowhead). (B) The collateral pathways disappeared after the occluded segment was recanalized and stent graft was placed successfully. (C) The target site lesion was found occluded after a 7-month follow-up. (D) The occluded segment was recanalized with a small oversizing Viabahn stent graft (arrowhead). (E) Upper limb edema recurred after 22 months, and stent edge restenosis was observed at the distal end of the stent graft (arrowhead). (F) Balloon dilation was performed for the stent edge restenosis to restore the blood flow (arrowhead).
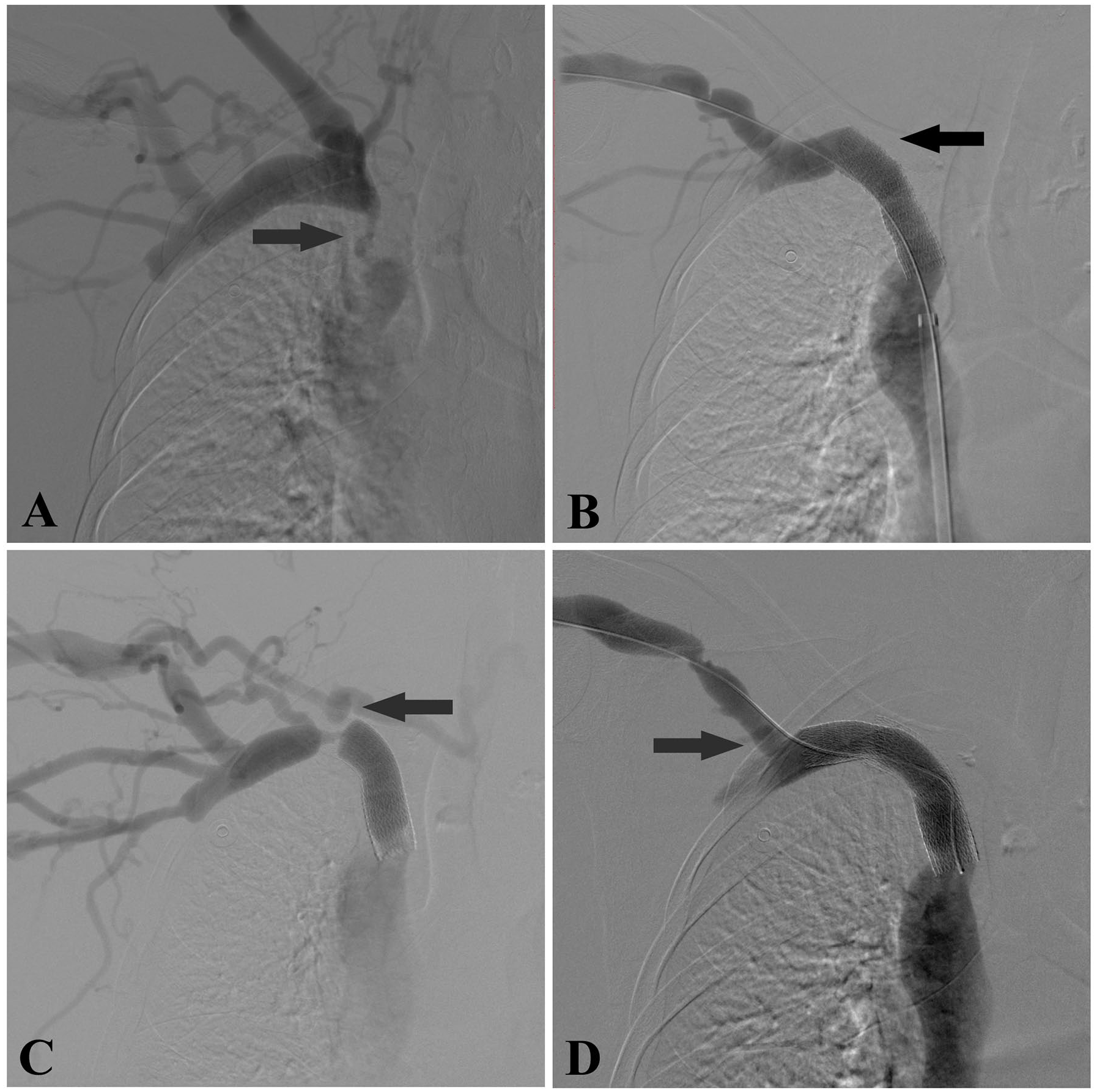
A 65-year-old woman with a right brachiocephalic fistula constructed for 5 years. (A) An angiogram showed that the patient had severe stenosis in the right brachiocephalic vein (arrowhead) with an obvious collateral vein formation. (B) The collateral veins disappeared after the brachiocephalic vein stenosis was recanalized and the stent graft was placed, a 5 cm Viabahn stent graft was placed in the subclavian veins, where the clavicle overlies the first rib, presented a poor stent morphology. (C) Upper limb edema recurred after 20 months, and stent edge restenosis was observed at the distal end of the stent graft (arrowhead). (D) The blood flow was restored by placing a small oversized Viabahn with stent-graft extension across the thoracic outlet (arrowhead) and achieved long-term patency.
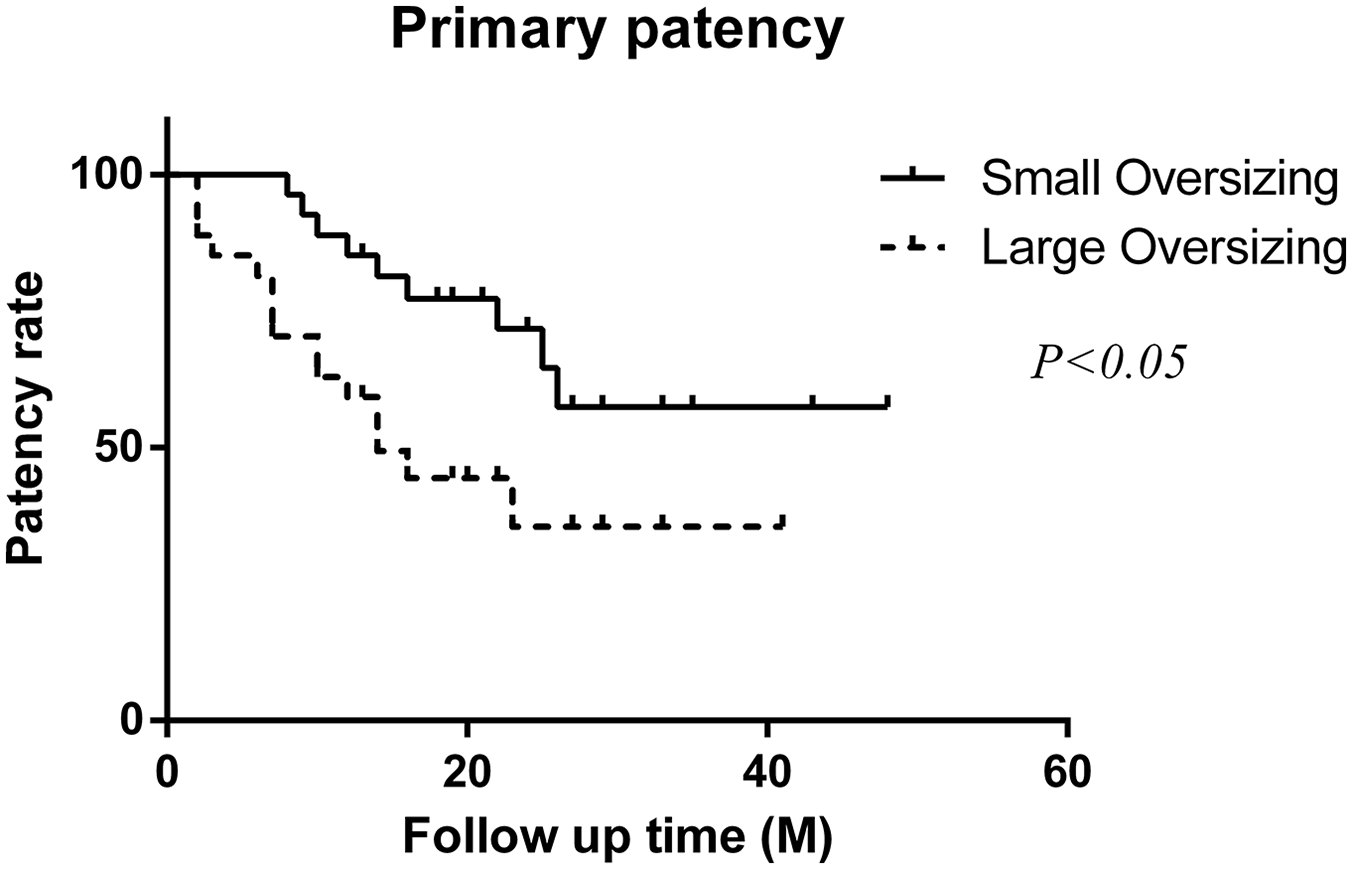
The Kaplan-Meier survival curves indicated that the patients with small oversizing of the stent graft had significantly higher primary patency rates than those with large oversizing of the stent graft (p=0.022).
The univariate analysis was used to investigate the potential factors related to the outcomes of primary patency. At univariate analysis (Table 3), 13 baseline variables and imaging characteristics were included in the univariate analysis, large stent-graft oversizing (hazard ratio [HR]=1.025; 95% CI=1.008-1.042; p=0.004), concomitant stenosis (HR=3.057; 95% CI=1.392-6.714; p=0.005) were independent predictors of target site primary patency dysfunction. Multivariate analysis using Cox proportional hazard models of target site primary patency revealed that concomitant stenosis and large oversizing stent graft were the independent predictors of target site primary patency (Table 4).
Overall Survival: Univariate Analysis.
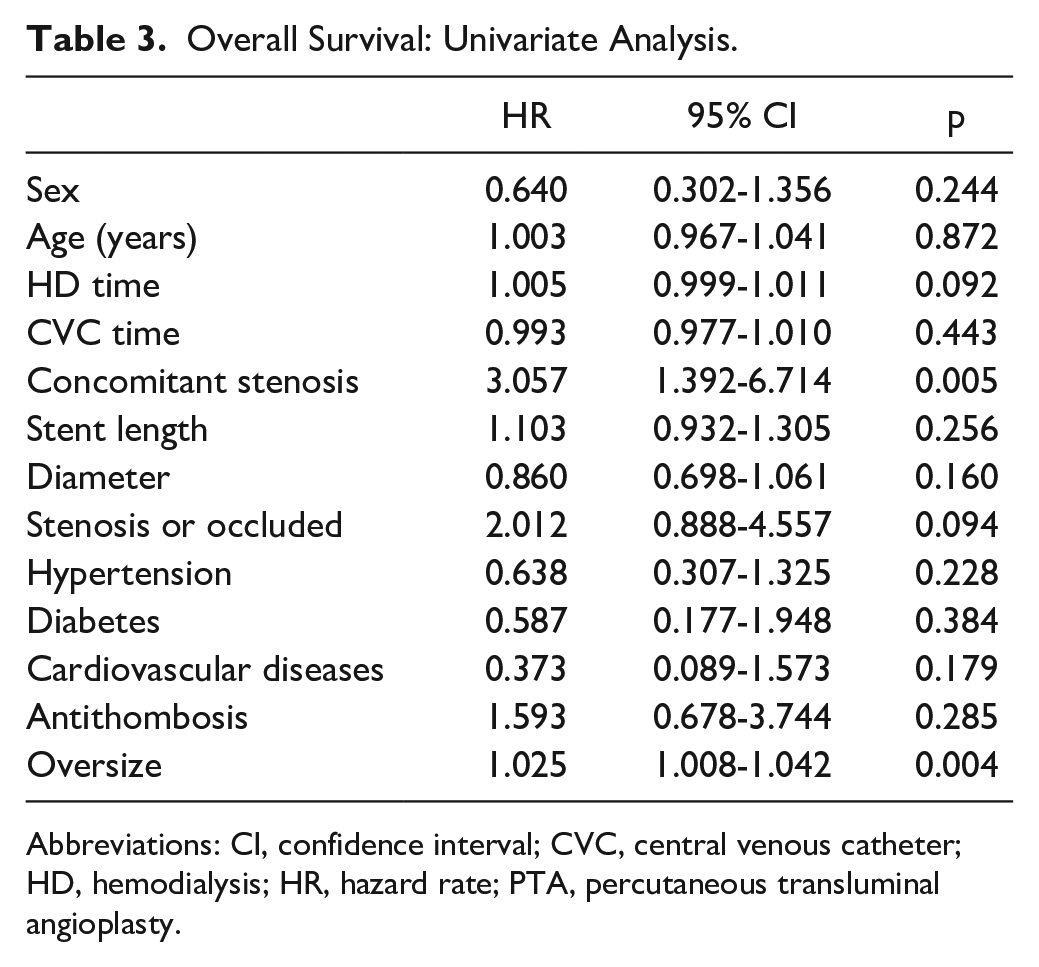
Abbreviations: CI, confidence interval; CVC, central venous catheter; HD, hemodialysis; HR, hazard rate; PTA, percutaneous transluminal angioplasty.
Overall Survival: Multivariate Analysis.
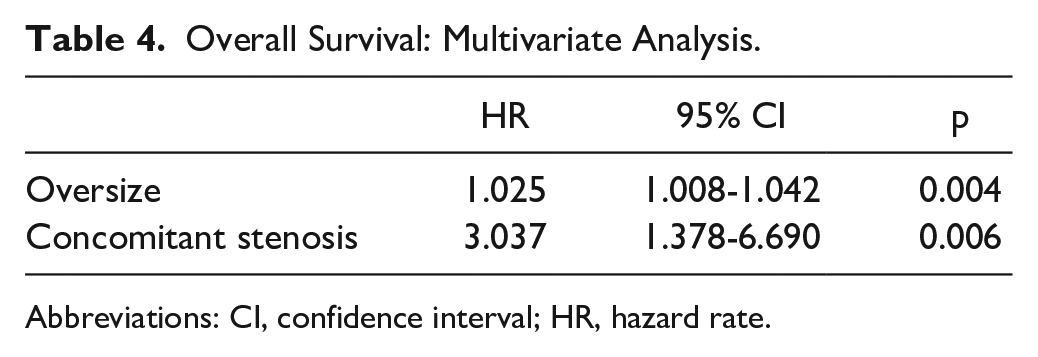
Abbreviations: CI, confidence interval; HR, hazard rate.
Discussion
The KDOQI clinical practice guidelines recommend PTA, with or without stent placement, as the preferred treatment approach for CVD. 4 Stent placement is recommended by the current KDOQI guidelines for stenosis recurrence within 3 months or acute elastic recoil of >50%. 4 However, a recent meta-analysis concluded that BMS could not improve the patency rate compared with PTA. 7 Without additional intervention, at least 75% of the BMS will lose patency due to endothelial hyperplasia inside and around the BMS. 12 Multiple repeat interventions are essential for PTA or BMS to maintain patency.12–15 Several studies showed significantly improved patency with stent grafts than with BMS or PTA.5,16–19 These studies reported that stent grafts achieved a very significant patency rate in the treatment of CVD, with a reported 6-month patency rate of 90% to 100%.5,16–19 However, stent grafts also have some limitations in the treatment of CVD, such as stent migration, stent restenosis, and the coverage of important branches.8,20,21
Stent grafts provide mechanical support and a physical barrier to intimal hyperplasia, and the covered segment of the stent graft is unlikely to develop intimal hyperplasia. 2 Different from that of the in-stent restenosis with BMS, the type of restenosis with covered stents is always stent edge restenosis, occurring within 0.5 cm of the distal edge of the stent graft. 19 Most of the restenosis may occur at the junction between the stent graft and the vessel wall, especially at the distal end. 19 However, few studies have examined the association between stent selection and the patency rate of stent-graft placement. Thus, it is important to identify the factors associated with stent edge restenosis to improve the patency rate after stent-graft placement.
The multivariate analysis in this study revealed that large oversizing is an independent predictor of the patency rates of stent grafts. The survival analysis curve, based on the oversizing range grouping, also confirmed that the small oversizing of a stent graft has a higher patency rate (p<0.05) than those with large oversizing. Some studies reported that a large stent diameter may stimulate intimal hyperplasia.8,22 The higher patency rates of stent grafts with small oversizing may be because a small oversizing stent may produce a small radial force, reduce the stimulation on the vein wall, and reduce the intimal hyperplasia. 22
When a stent graft is placed to treat an aneurysm or arterial dissection, a 10% to 20% oversizing covered stent is recommended to provide an effective seal and fixation, thereby avoiding stent-graft migration, collapse, or endoleak formation and providing a more reliable endovascular exclusion effect. 23 However, when a stent graft is placed to treat central venous occlusive disease, the placement of the stent graft is mainly to provide mechanical support for elastic retraction that is unresponsive to PTA and to provide a physical barrier for intimal hyperplasia and to maintain the patency of the central venous lesions. Therefore, in theory, there is no higher requirement for a degree of oversizing when stent grafts are placed to treat CVD. Excessive oversizing can lead to stent in-folding or stent collapse. A large oversizing may cause changes in the biomechanical properties of the adjacent vessel wall, stimulating the hyperplasia of the distal vein intima, and resulting in stent edge restenosis and loss of patency in a short time. Therefore, in this study, we preferred to choose a stent with 1:1 sizing or small oversizing at the distal end. Stent-graft size either equal in diameter to the distal normal vessels or slightly larger size closest to the measured diameter was considered ideal among limited stent-graft diameter options.
Chen et al 2 reported the use of Gore Excluder iliac stent grafts in a series of 60 hemodialysis patients to treat symptomatic CVD. They deployed the stent graft with 1:1 sizing at the distal vein and achieved remarkable technical success and target site patency rates. In their research methodology, although they proposed to use the stent graft with 1:1 sizing at the distal vein, they did not explain the reasons and factors to be considered. They also reported a case of intimal hyperplasia caused by an oversized distal end of the stent graft, resulting in repeated edge stenosis and stent-graft occlusion. However, this study did not provide further analysis on the selection of a stent diameter. 2 Chen et al 8 reported that stents with large sizes may provide better patency than those with small sizes; the larger the diameter of the vein and the larger the size of the stent, the better the patency rate. However, the patients included in this study were placed with 22 stent grafts and 49 BMSs, and the mechanisms of restenosis of BMS and stent grafts are different.
The central vein usually has a large diameter and tapered configuration, and its diameter gradually increases as it gets closer to the heart.2,24 Because of this anatomical feature, the risk of stent migration such as migration to the pulmonary artery or cardiac chambers must be paid significant attention to prevent serious consequences. 8 These risks can be avoided through some surgical details. First, an obvious residual stenosis or elastic retraction can produce radial force to avoid migration of the stent. Second, it is recommended to select a balloon diameter smaller than the stent diameter during the prior pre-dilation of the target lesion. Third, post-dilation after successful placement of the stent graft is performed using a balloon that is slightly smaller in size than the stent graft, while satisfying the stent-graft’s expansion and reducing the risk of stent-graft detachment. In this study, no small oversizing related stent migration was observed during the follow-up. However, “0” oversizing stent graft must be used with caution due to an increased risk of stent migration. Some experts recommend using an oversized stent graft with a diameter between 18 and 22 mm to treat CVD. 22 However, to date, no relevant study which deployed such an oversized stent graft is reported in the literature. It may be due to the concern that such an oversized stent graft is more likely to stimulate intimal hyperplasia, resulting in stent-graft occlusion.
Stent grafts are deployed conditionally and are not used routinely because of the risks, including stent-graft migration, infection, thoracic inlet compression, and obstruction of important branches. To preserve the internal jugular vein, short stents are usually placed in some jugular angle lesions, thereby increasing the probability of poor stent morphology. Therefore, it is necessary to develop stent grafts with more suitable geometric configurations for the treatment of central venous lesions. The stent-graft oversizing has often been mentioned in endovascular treatment of arterial diseases, but it has not been presented in stent-graft placement of central venous occlusion. Initially, the stent-graft oversizing percentage was quantified and divided into groups of 0-5, 5-10, 10-15, 15-20, and >20 for analysis. However, some groups had a small number of patient cases, leading to less reliable statistical analysis. The analysis showed that stent grafts with 0%-5% oversizing achieved better patency. However, due to the limited number of cases, as well as the relatively small median value of stent-graft oversizing (3.5%), we found a statistically significant difference when using this median value for the analysis. Therefore, the median of the oversizing range is roughly used for grouping to determine the small or large oversizing. The limitations of this study are its small sample size and retrospective nature. Prospective, multi-center and large studies are needed to further validate the results.
Conclusions
In conclusion, stent grafts show reasonable primary patency rates for the treatment of CVD in hemodialysis patients. Stent grafts with small oversizing are associated with better primary patency rates of the target sites.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the “Suzhou Science and Education Revitalize Health” Youth Science and Technology Project (KJXW2022032).