
Abstract
Purpose:
Traumatic popliteal pseudoaneurysms may occur in accidents or as an iatrogenic complication of a total knee arthroplasty. Complications often arise in open repair because of distorted anatomy. Up to 22% of the patients may suffer above-knee amputation. Endovascular treatment has proven to be an effective solution. However, the long-term performance of stents at the hinge point of the popliteal artery is questionable. We present a hybrid technique that was used successfully in 2 cases.
Technique:
Our approach takes advantage of both open and endovascular techniques. At first, we apply a stent graft at the side of the injury to cover the arterial trauma and stop blood leakage to the aneurysm sac. This allows for a safer dissection and open repair. We clamp the artery proximally and distally, open the sac, extract the stent graft, and extend to a longitudinal arteriotomy. We then reconstruct the entire area with a standard in lay end-to-end anastomosis using a vein graft. This hybrid technique may reduce the risk of uncontrollable bleeding and allow for a safer nerve decompression.
Conclusions:
Repair of such injuries is technically demanding. A hybrid approach may reduce the risk of complications and offer excellent long-term outcomes.
Clinical Impact
The hybrid approach to the treatment of traumatic popliteal pseudoaneurysms combines the advantages of both open and endovascular approaches. It may be possible to make an acute operation just as safe as an elective operation by implementing the proposed strategy. The procedure can be performed by surgeons of all levels, and patients may benefit from a safer surgical dissection with fewer complications and blood loss. This smart combination of standard techniques may prove invaluable in a hostile surgical environment where limb loss is likely.
Keywords
Introduction
Traumatic popliteal pseudoaneurysms occur as a result of penetrating trauma rather than blunt trauma. 1 Changes in bone structure, such as exostosis and osteochondroma, 2 as well as iatrogenic procedures, such as arthroplasty 3 and acupuncture, 4 can result in popliteal pseudoaneurysms.
Injury to the neurovascular structures is a well-recognized complication in total knee arthroplasty (TKA). Many studies have reported pseudoaneurysms of the popliteal artery in TKA at an incidence of 0.03% to 0.17%.5,6 On the contrary, there are very few case reports of popliteal pseudoaneurysms following blunt trauma without dislocation or significant fracture. Specifically, popliteal artery pseudoaneurysms have been reported in connection with minor falls, traction injuries in automobile accidents, and occupational accidents. 1
Regardless of the cause, it is difficult to diagnose a popliteal artery pseudoaneurysm early. Symptoms can be subtle, nonspecific, or mimic other conditions, resulting in delayed diagnosis and serious complications. Early diagnostic imaging modalities, including computed tomography (CT) scans, that can provide an accurate diagnosis, are not always used. It is common for pseudoaneurysms to go undetected until they are too large and exert pressure on the adjacent neurovascular structures, leading to progressive foot drop due to peroneal neuropathy. 7
A delayed diagnosis and an expanding pseudoaneurysm can create a hostile surgical field. An open repair has excellent long-term results, but it is technically demanding and has a high rate of complications. As a result, most popliteal artery pseudoaneurysms nowadays are treated endovascularly. The damaged part of the popliteal artery is covered with a stent graft. Although endovascular therapy may be easy and effective in the short term, the technique’s durability is questionable, particularly for the P2 segment which is located from the proximal part of the patella to the knee joint space.
We sought to develop a hybrid approach that may combine the advantages of open and endovascular techniques and report 2 cases of popliteal artery pseudoaneurysms that have been successfully treated.
Case Reports
Case 1
A 50-year-old woman gymnast with post-traumatic arthritis underwent a redo TKA. Bleeding following the osteotomy was documented in the operation notes. It was effectively controlled with tourniquet inflation and suturing of a bleeding point originating posteriorly from the popliteal fossa. Post-operatively, the patient complained for knee pain. She managed, however, to mobilize and was discharged home on pain killers and rivaroxaban for 2 weeks. At follow-up, she reported increasing knee pain and was noticed to suffer from peroneal nerve palsy with decreased foot sensation and reduced dorsiflexion motor power. On examination, there was a pulsating popliteal mass and duplex scan revealed a large pseudoaneurysm occupying the entire popliteal fossa. Computed tomography angiography (CTA) of the lower extremity demonstrated a gigantic pseudoaneurysm of the right popliteal artery occupying the entire popliteal fossa and pushing away the artery both proximally and distally (Image 1). The anatomic relations had been altered by this large pseudoaneurysm making this field extremely hostile for an open repair. The pseudoaneurysm sac extended distally almost to the trifurcation. The point of rupture was not clear in the CTA because of the artifacts caused by the orthopedic prosthesis.
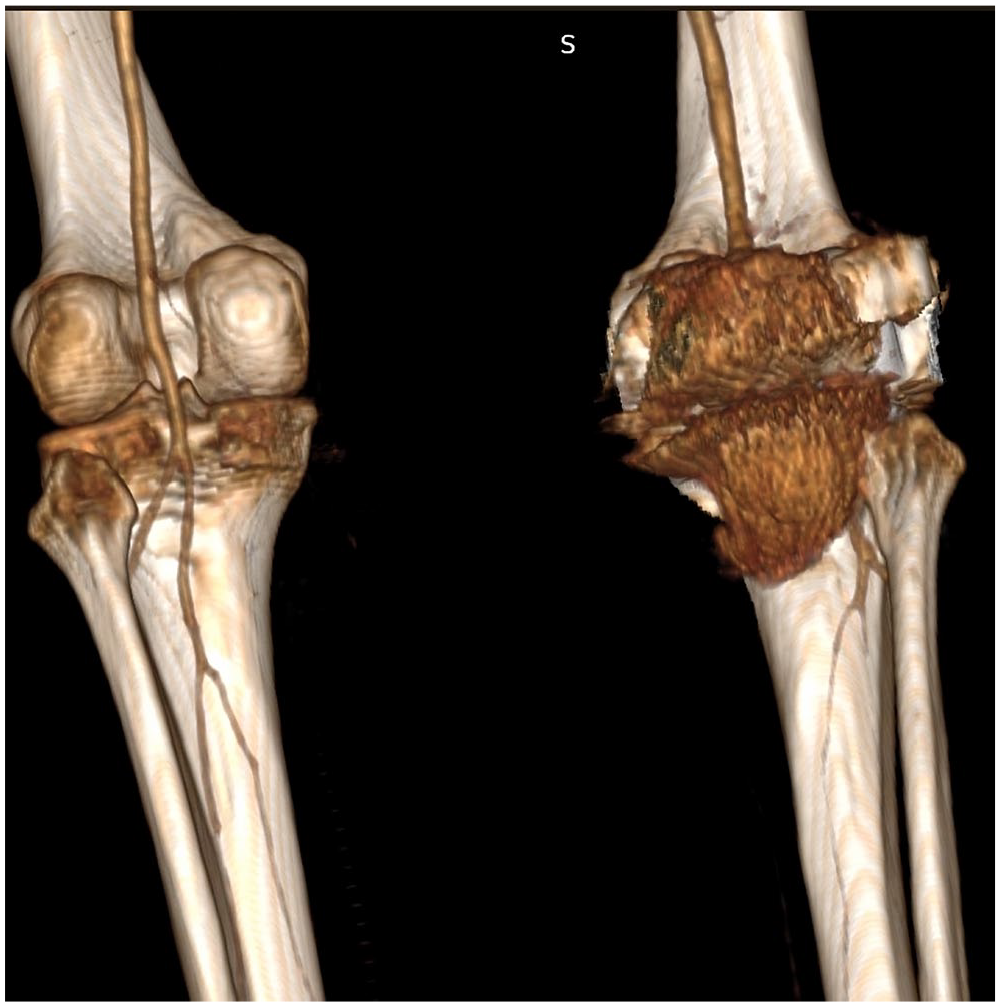
Pseudoaneurysm after TKR at the P2 segment causing palsy of the tibial and peroneal nerves.
Due to the size of the rupture and the distortion of the anatomy of the area, we opted for a hybrid technique to reduce the risk of uncontrollable bleeding, reconstruct the artery, and also safely decompress of the peroneal nerve. Through a small longitudinal femoral incision, the superficial femoral artery was accessed and an antegrade vascular access sheath was put in place. The intraoperative angiogram showed 2 points of injury with 2 distinct jets of blood filling the popliteal fossa. A 5 to 37 mm balloon-expandable Bentley Begraft (Bentley InnoMed, Hechingen, Germany) was applied to seal the ruptured artery (Image 2). Then, the proximal part of the saphenous vein was harvested through the same incision. The time between the endovascular and the open repair was about 20 minutes. The femoral wound was closed, and the patient was pronated to proceed with an open repair using a posterior approach. The sealed sac was easily evacuated, and the popliteal artery was safely controlled. A small arteriotomy was done to pull out the stent and then extended to a longitudinal arteriotomy. The injured area was bypassed with a short 4 cm saphenous vein graft with end-to-end anastomoses (Image 3). The patient made an excellent recovery and has been followed up for 1.5 years.
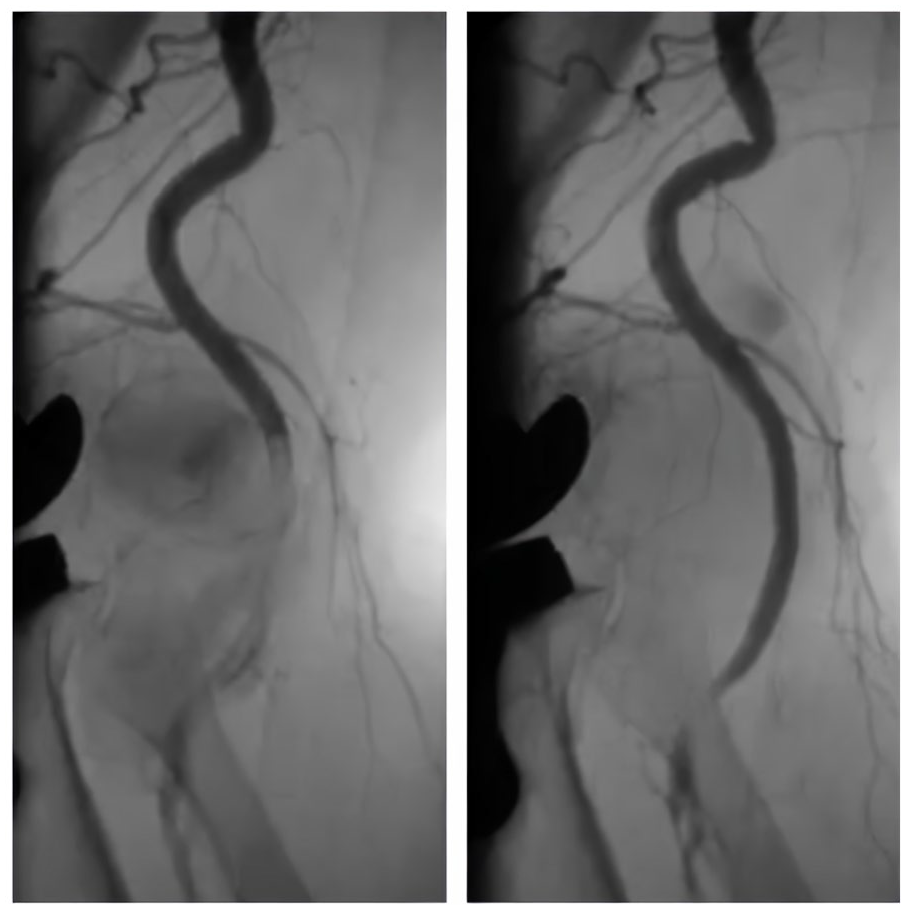
Intraoperative angiogram showing the leakage from the popliteal artery to the pseudoaneurysmal sack before and after the placement of the stent graft.
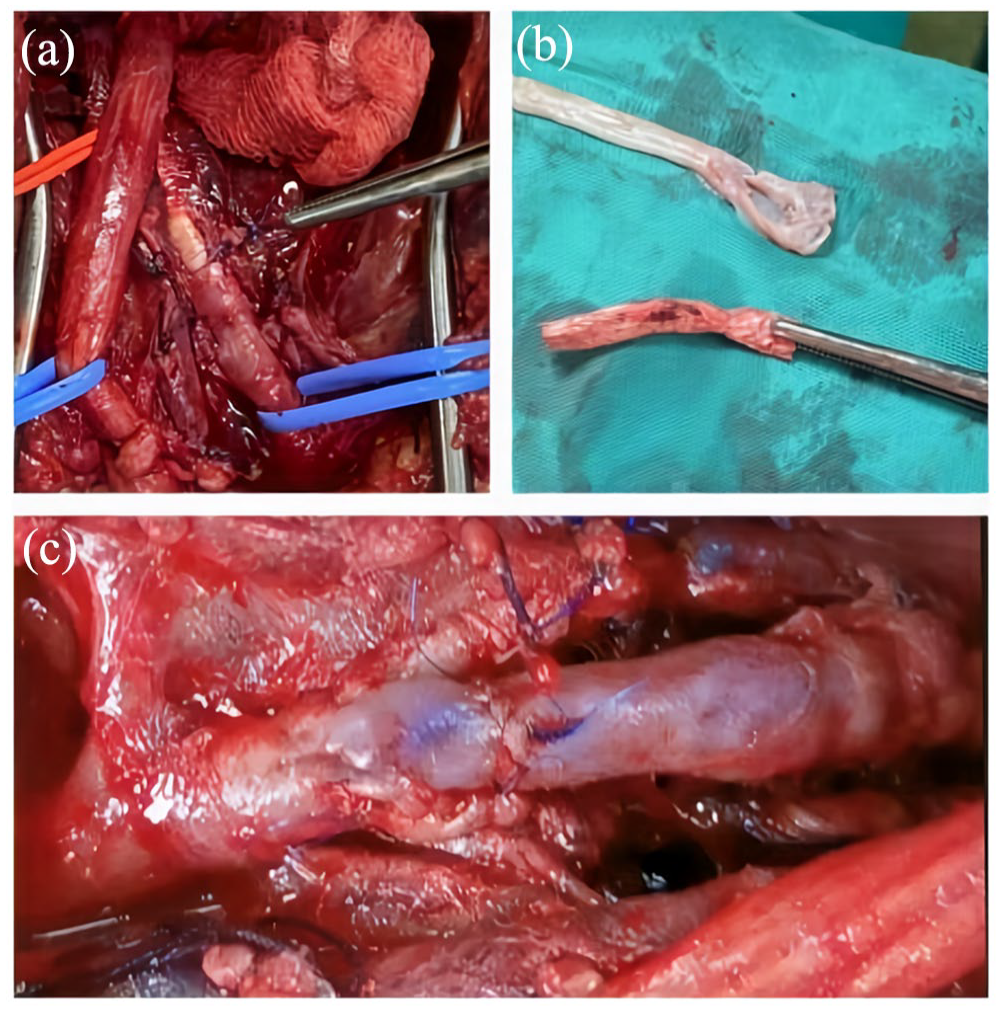
(A) The stent graft inside the popliteal artery and the hole the saw blade made. (B) The saphenous vein and the stent graft after the removal from the artery. (C) The reconstruction of the popliteal artery.
Case 2
In this case, a 60-year-old woman suffered knee hyperextension and traction of the right popliteal artery as a result of a fall. Initially, she was asymptomatic. A few weeks later, she referred to the emergency department with a pulsatile mass and pain at the right thigh. She underwent a CTA and a gigantic pseudoaneurysm at the P1 segment, which is located from the intercondylar fossa to the proximal edge of the patella, measuring 8 by 10 cm was revealed (Image 4). Similarly to the first case, we proceeded with a hybrid repair. First, a 5 to 37 mm balloon-expandable Bentley Begraft (Bentley InnoMed) was applied to seal the ruptured area (Image 5) allowing for a safer dissection of the field, and then we converted to open repair. We clamped the artery proximally and distally, opened the aneurysm sac, extracted the stent graft, and then extended to a longitudinal arteriotomy of the popliteal artery. We then reconstructed the entire area with a standard in lay end-to-end anastomosis using a vein graft and a side approach, bypassing the stent’s proximal and distal landing zones. The time between endovascular and open repair was estimated to be about 15 minutes. The patient made an excellent recovery and has been followed up for 6 months.

Pseudoaneurysm of the P1 segment measuring 7 by 8 cm.
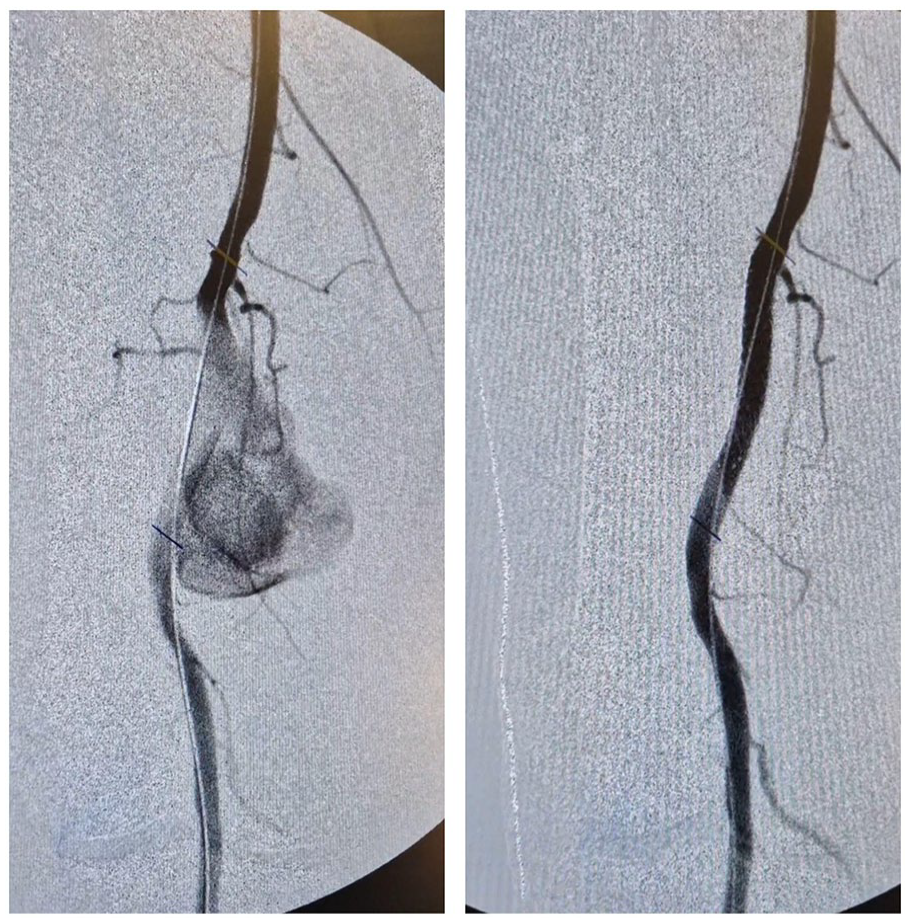
Intraoperative angiogram showing the leakage from the popliteal artery to the pseudoaneurysmal sack before and after the placement of the stent graft.
A written informed consent has been obtained from both of the above patients to publish their data.
Discussion
Open repair of popliteal artery pseudoaneurysms is technically demanding because of the hostile anatomy of the traumatic area. The distorting effect of pseudoaneurysms can make it difficult to identify and visualize anatomical landmarks. The popliteal fossa encloses the 2 terminal branches of sciatic nerve and the small saphenous vein. These neurovascular structures may become compressed and displaced. In turn, hemostasis and surgical dissection are more difficult due to altered tissue plans, adhesions, and increased bleeding. Moreover, the pseudoaneurysm may be affixed to nearby tissues, complicating surgical access and increasing the risk of inadvertent damage to nearby tissues.
Endovascular management of popliteal artery pseudoaneurysms has been reported to be successful in several cases. 8 However, there are concerns due to the relatively mobile popliteal artery and the risk of device migration or stent fracture. Especially in young patients, the long-term patency of a stent in the popliteal artery is also concerning. Finally, the endovascular approach cannot offer immediate evacuation of pressure exerted on neurovascular structures.
There are numerous benefits to the hybrid approach we suggest. The first benefit is a significant reduction in blood loss, as the veins and arterial branches of the area can be safely dissected. Essentially, this strategy can transform a subacute operation into an elective one, making it easier for surgeons of all levels to perform the procedure. This strategy also offers reduced clamping time as the entire dissection can be completed with distal blood flow.
It may be argued that a balloon can be inserted at the orifice of the pseudoaneurysm intraoperatively to obstruct the blood flow instead of a stent graft. Nevertheless, this technique increases ischemia time, risk of reperfusion injury, and need of fasciotomy. Furthermore, the balloon may rupture or move during dissection. It should also be mentioned that with a vascular sheath and an inflated balloon in place, a posterior approach to the popliteal artery is difficult, if not impossible.
One may also argue that, regarding the second case, the placement of a Viabahn graft at the P1 segment followed by decompression is an excellent option. Minimal invasiveness and no need for an open reconstruction are its main advantages. Nevertheless, we have to decide the best course of treatment for a young energetic patient with a long life expectancy. It has been shown that saphenous grafts have a longer patency rate than stent grafts. 8 A hybrid repair, which makes dissection safer, gives us the option to offer a proper reconstruction, even in the acute phase, to a young patient without comorbidities. In addition, a reconstruction with a vein graft may require less frequent surveillance and fewer additional interventions. 8
A major limitation of this technique is the controversial application of an expensive stent graft that will be removed afterwards. In most cases, this is much cheaper than a full endovascular repair that requires a larger sealing zone that typically requires 2 overlapping stent grafts. Finally, in the cost-effectiveness equation and comparison with the standard open technique, additional factors need to be considered, namely reduced blood loss, reduced injury of nerves, and other significant structures in the area, which may lead to complications that require costly rehabilitation and a longer hospital stay.
In conclusion, repair of traumatic popliteal artery pseudoaneurysms is technically demanding. The field is hostile, and the risk of limb loss is high. A hybrid approach may reduce the risk of complications and offer excellent long-term outcomes.
Supplemental Material
sj-docx-1-jet-10.1177_15266028241237674 – Supplemental material for A Hybrid Approach That May Facilitate the Repair of Traumatic Popliteal Artery Pseudoaneurysms
Supplemental material, sj-docx-1-jet-10.1177_15266028241237674 for A Hybrid Approach That May Facilitate the Repair of Traumatic Popliteal Artery Pseudoaneurysms by Areti Vassiliou, Michail Peroulis, Vassilios Tatsis and Vangelis G. Alexiou in Journal of Endovascular Therapy
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.