
Abstract
Objectives:
Type I and III endoleaks following endovascular aneurysm repair (EVAR) can lead to catastrophic events that require major re-interventions. We reviewed our experience with aortic endograft re-interventions for type I and III endoleaks and other serious failures among different devices.
Methods:
We retrospectively reviewed patients with a prior EVAR who underwent open conversion (OC) or major endovascular intervention (MEI) (re-lining, cuff/limb extension, parallel graft) for type I/III endoleaks at our institution from 2002 to 2019. Baseline characteristics, procedural details, re-interventions, and outcomes were collected.
Results:
A total of 229 patients (194 men) underwent re-interventions for type I and III endoleaks after EVAR (90 OC, 139 MEI) for devices implanted between 1997 and 2019. Average age at re-intervention was 78±8.5 years. A total of 135 (59%) were implanted at our institution, whereas 93 (41%) were referred. Median time to re-intervention was 4 years with 25% to 75% interquartile range (IQR) of 2.2–6.6 years. There was no significant difference in baseline demographics or type of re-interventions (OC/MEI) between device types. 42/229 (18%) presented with ruptured aneurysms, 20/229 (9%) were symptomatic, whereas the rest presented with asymptomatic radiographic findings. Type 1A endoleak was present in 146/229 (63.8%—72 with proximal migration), type IB in 46/229 (20.1%), type IIIA in 37/229 (16.6%), type IIIB in 15/229 (6.5%), and persistent aneurysm sac growth with no radiographic evidence of an endoleak in 6/229 (2.6%). Devices included most commercial products: AFX, Excluder, AneuRx, Ancure, Endurant, and Zenith. A smaller number of investigational devices accounted for the rest. Type 1A endoleak was the most common indication for re-intervention among all devices except for AFX and ancure devices, proximal migration was a frequent presentation with AneuRx. AFX devices more frequently presented with a type III and ancure devices more frequently presented with a type IB endoleak.
Conclusions:
Serious failure modes after EVAR differ between endografts and occur throughout the follow-up period. This is important to guide targeted interrogation of surveillance studies and follow-up schedules, even for discontinued devices, as well as comparisons between various series and estimation of EVAR failure rates.
Clinical Impact
Surveillance after EVAR is critical for long term success of the repair, understanding of the differential modes of failure of every graft available is important in the longitudinal evaluation of these endografts. Equally important is the understanding of the modes of failure of legacy endografts that are no longer on the market but still being followed, in order to be able to tailor a surveillance regiemn and the evntual repair if needed.
Introduction
Endovascular aneurysm repair (EVAR) has revolutionized the care of abdominal aortic aneurysms (AAAs) since its introduction in the 1990s. The prevalence of EVAR use continues to increase from about 35% of AAA repairs in 2003 to about 70% of repairs in 2013 in a study of Medicare beneficiaries. 1 Although EVAR and open repair have similar short term outcomes, long-term follow-up from the EVAR-1 trial has shown an increased risk of re-intervention with EVAR compared with open repair, in addition to higher 8–14 year mortality with EVAR compared with open repair, both in terms of total and aneurysm-related mortality. 2 In long-term follow-up of the OVER trial, 30.5% of patients developed one or more endoleak; 12% type I, 76% type II, 3% type III, 3% type IV, and 6% indeterminate. Most of the type II endoleaks resolved with no intervention, whereas 70% of type I endoleaks and 100% of the type III endoleaks in this cohort required an intervention. 3 Other retrospective series have also demonstrated that endoleaks are common after EVAR, with type II endoleaks being the most common; however, up to 80% of type II endoleaks are likely to resolve spontaneously. 4 Analyses of data from the EUROSTAR registry and from the Vascular Quality initiative database have shown that while type II endoleaks contribute to the majority of the re-interventions they are not significantly associated with aneurysm rupture compared with patients with no identifiable endoleak.5,6 Conversely, type I and III endoleaks are less common but more likely to require a secondary intervention have a delayed presentation and to be associated with subsequent aneurysm rupture and mortality. 4 In several series between 15% and 26% of patients with type I or type III endoleaks present with delayed aneurysm rupture.7,8 Although the majority of re-interventions for type I and III endoleaks after EVAR are endovascular such as proximal or distal extension or endograft re-lining, open surgical conversion either with graft explantation or other graft preserving techniques occurs in up to 6% of patients as reported in multiple series.9,10 Moreover, open conversion (OC) with graft replacement or graft preservation techniques have increased over time as the prevalence of EVAR for more complex AAA repair continues to increase. 11 Given the delayed and often catastrophic consequences of types 1 and III endoleaks, we sought to describe our institutional experience with re-interventions for types I and III endoleaks and to examine the variable outcomes and modes of failure among the commercially available and discontinued endografts.
Methods
We retrospectively reviewed the electronic health record at our institution for consecutive patients who underwent OC or major endovascular intervention (MEI) for type I and type III endoleaks following EVAR from 1997 to 2019. Major endovascular intervention was defined as endograft re-lining, proximal and/or distal endograft extension, or insertion of parallel grafts (ie, chimney or periscope grafts). We included patients who underwent the index EVAR at our institution and those who had their initial procedure at an outside institution provided the re-intervention was performed at our institution. Patients who underwent re-interventions for type II endoleaks, para-visceral aneurysms (para-visceral aneurysmal degeneration without type 1 endoleak or development of thoracoabdominal aneurysms), or endograft infection were excluded. The type of intervention (OC or MEI) was dictated by the failure mode and residual landing zones. An endovascular first approach was generally adopted if anatomically feasible and parallel grafting was reserved for patients at high risk for OC. Patient records were reviewed for demographics, procedural details, peri-procedural complications, and follow-up data. The study protocol was approved and exempted from informed consent by the Institutional Review Board.
Data were collected on baseline demographics, medical comorbidities, and prior surgical history. When available details of prior AAA treatment was collected such as EVAR procedure date, endograft device type, aneurysm size at initial EVAR, and prior interventions when available. Time to re-intervention was captured from the date of the index EVAR in order to understand early and late failure modes of different devices. Pre-operative computed tomography angiograms (CTAs), conventional angiography, and operative notes were reviewed to determine the type of endoleak, mode of failure, and technical details of the procedure. Post-operative outcomes were ascertained at 30 days and included mortality, cardiovascular events (myocardial infraction, atrial fibrillation, congestive heart failure), respiratory failure (prolonged mechanical ventilation, re-intubation, need for tracheostomy), renal failure (transient with no dialysis need, temporary dialysis need, permanent dialysis need), limb complications, and hospital re-admissions. Mid-term outcomes were ascertained at 1 year and included mortality, aortic-related mortality where available, and delayed rupture. Data were collected in Excel (Microsoft, Redmond, Washington) and analyzed using Stata SE 17 (StataCorp LLC, College Station, Texas) and Statistical Package for the Social Sciences, version 26 (IBM Corp, Armonk, New York). The Student t-test (for continuous variables) and χ
Results
Population Characteristics
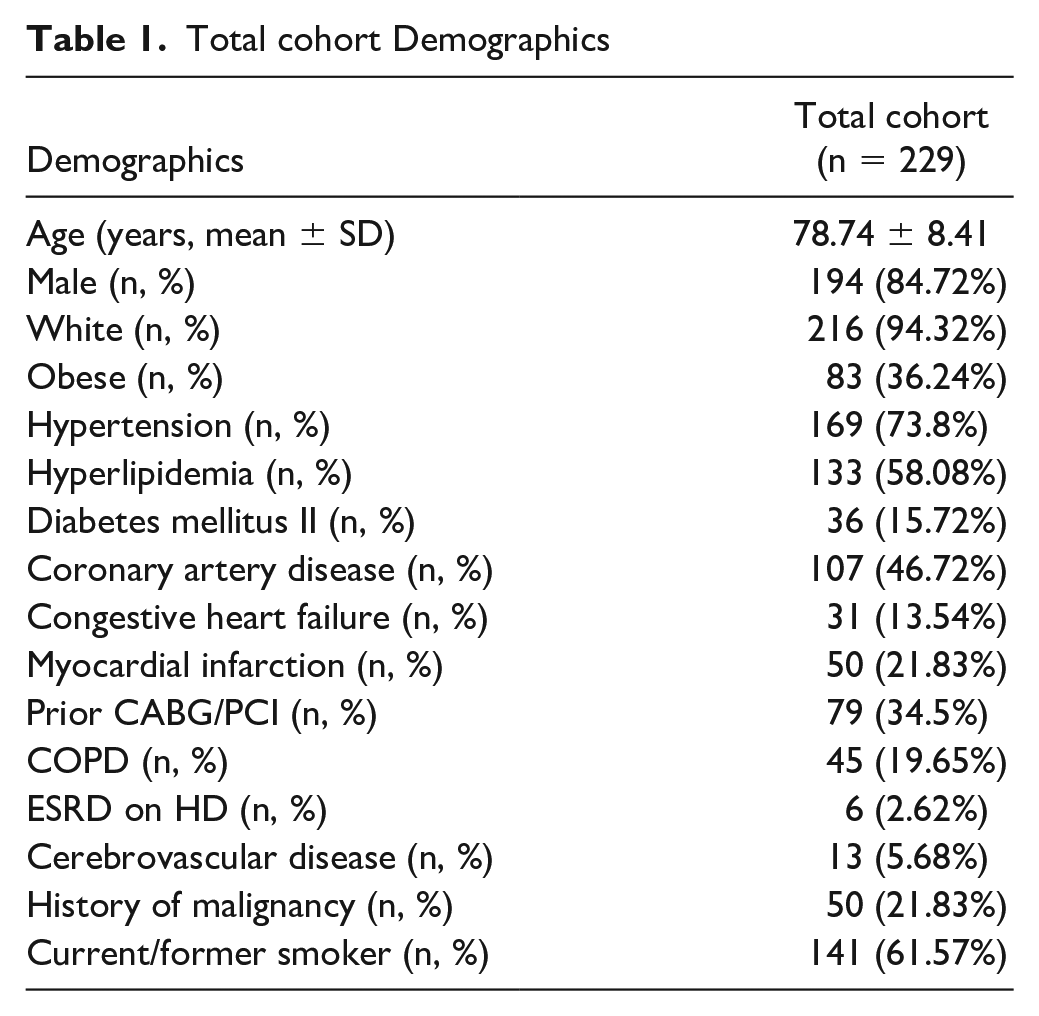
We identified 229 patients who underwent re-interventions for type I or type III endoleak. The average age was 78 years, the majority were male (194/229, 85%) and white (216/229, 94%). Common comorbidities included hypertension (169/229, 74%), hyperlipidemia (133/229, 58%), coronary artery disease (107/229, 47%), and positive active/former smoking status (141/229, 62%) (Table 1).
Total cohort Demographics
Procedural Data
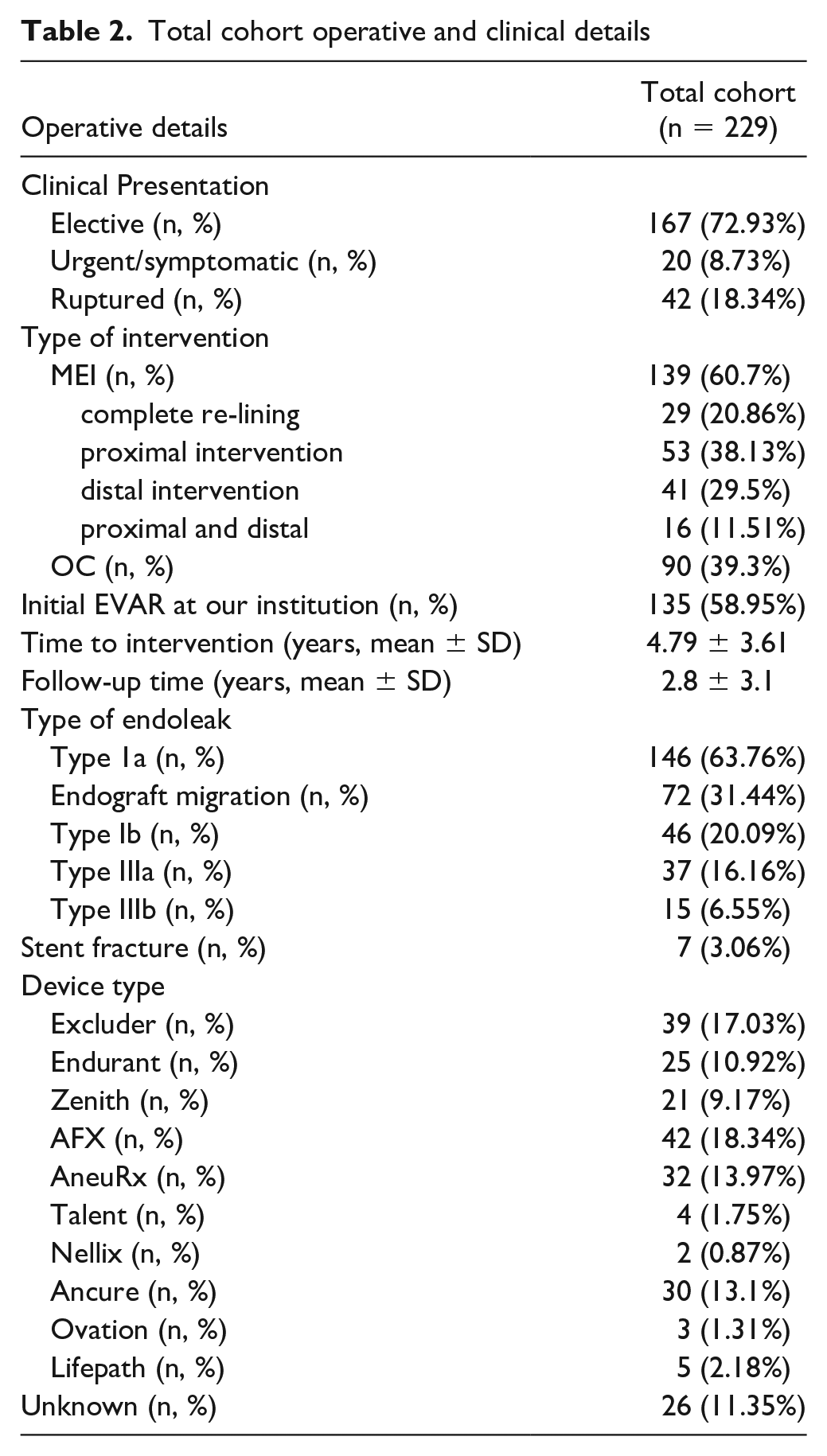
Of the 229 patients, 61% (139/229) underwent MEI and 39% underwent OC. Twenty nine of 139 patients with MEI (21%) underwent complete re-lining of their existing endograft with a new endograft system for type Ia endoleak with proximal migration, type III endoleak, or type I and type III endoleak. A total of 53 (38%) underwent a proximal extension/re-lining for type Ia endoleak, type III endoleak, and unexplained AAA growth, 41 (29%) underwent distal extension/re-lining for type Ib or type III endoleak, and 16 underwent both proximal and distal extensions for type Ia and Ib endoleaks, type Ia and III endoleaks, and unexplained AAA growth. The majority of patients presented with asymptomatic radiographic findings of endoleak (167/229, 73%), whereas 9% of patients (20/229) presented with a symptomatic endoleak (abdominal pain, hemodynamic changes without radiographic evidence of rupture), and 18% of patients (42/229) presented with a ruptured aneurysm, patients who underwent an open repair were more likely to present with a symptomatic or ruptured aneurysm (p=0.013). 59% of patients had undergone the index EVAR at our institution and the remainder were referred for re-intervention. The median time to re-intervention was 4 years with 25% to 75% interquartile range (IQR) of 2.2 to 6.6 years. The most common indication for re-intervention after EVAR in this study cohort was type IA endoleak (146/229, 63.8%) associated with proximal migration of the endograft in 72 instances. Type IB endoleaks were present in 46/229 (20.1%), type IIIA in 37/229 (16.6%), type IIIB in 15/229 (6.5%), and persistent aneurysm sac growth without radiographic endoleak in 6/229 (2.6%). Devices in the cohort included most commercial products: AFX, Excluder, AneuRx, Ancure, Endurant, and Zenith. A smaller number of investigational devices accounted for the rest, and the remainder of devices were unknown (26/229, 11%) due to either lack of imaging for review and/or no clarification in the operative report (Table 2).
Total cohort operative and clinical details
Procedural Outcomes
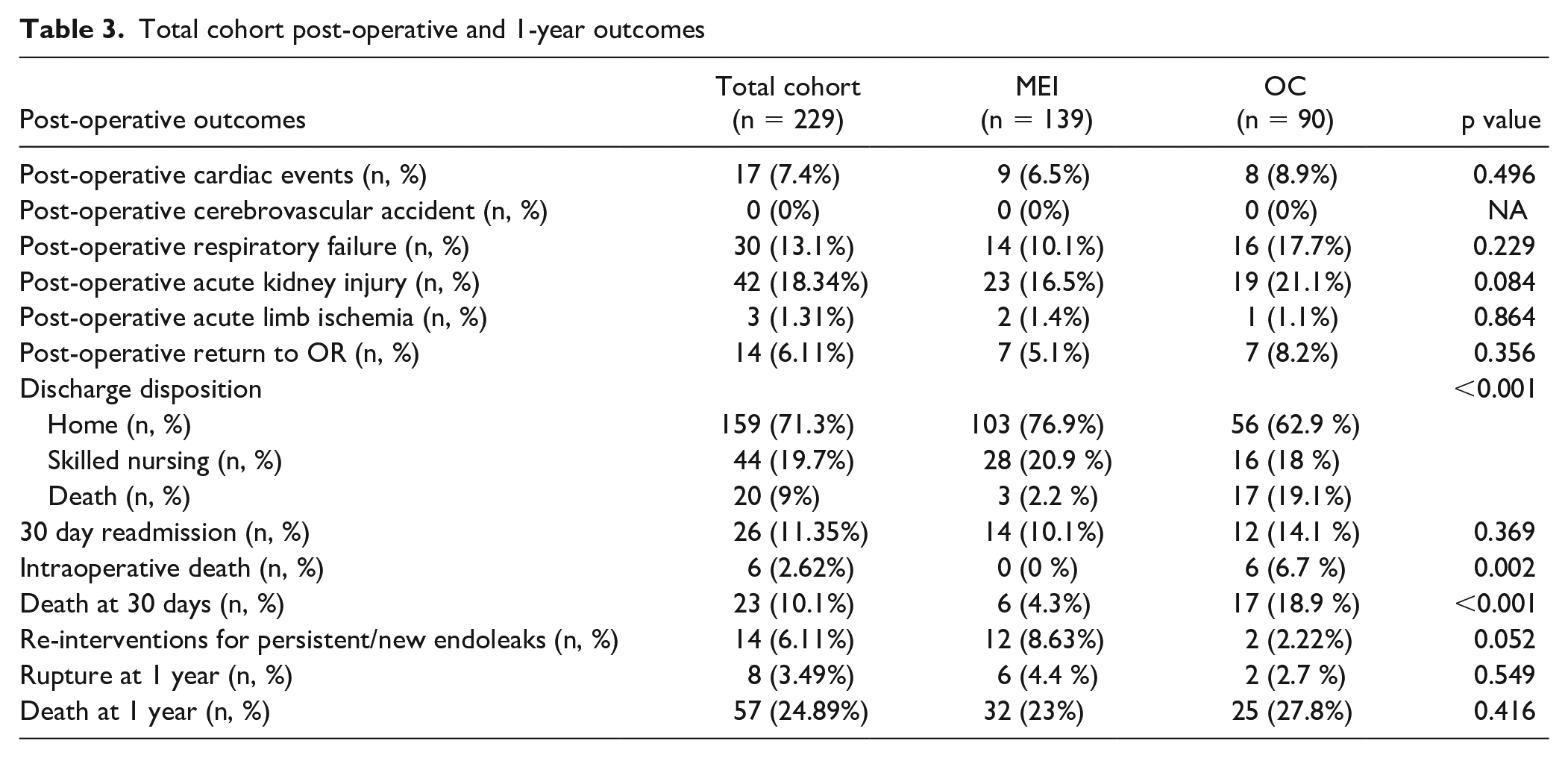
Common post-operative morbidities included, cardiac events (17/229 7.4%), respiratory failure (30/229, 13%), acute kidney injury (42/229, 18%), and 30 day hospital readmission (26/229, 11%). 159/229 (71.3%) of patients were discharged home following the re-intervention, 44/229 (19.3%) were discharged to skilled nursing facilities, and 20/229 (9%) were in-hospital deaths. There were 6 intraoperative deaths (2.6%), and mortality at 30 days was 10% (23/229). At 1 year follow-up, delayed rupture after re-intervention occurred in 8/229 patients (3.5%) and mortality was 25% (57/229) (Table 3). When comparing MEI and OC cohorts, patients in the OC cohort were less likely to be discharged home (62.9% 56/90 OC vs 76.9% 103/139 MEI, p<0.001). Intraoperative death (6.7% 6/90 OC vs 0% 0/139 MEI, p=0.002) and 30 mortality (19% 17/90 OC vs 4% 6/139 MEI, p<0.001) were higher in the OC cohort compared with the MEI cohort. There was no difference in other immediate post-operative outcomes or 1 year delayed rupture/mortality between OC and MEI cohorts (Table 3).
Total cohort post-operative and 1-year outcomes
Endoleak Outcomes
There were 14 re-interventions for persistent or new endoleaks in 229 patients in the total cohort, with a median time to re-intervention of 21 months (IQR=4-48 months). In the MEI cohort, 12/139 (8.63%) patients underwent additional re-interventions for persistent/new endoleaks, 3 for type Ia, 5 for type 1b, and 4 for type III. Although 2/90 (3.33%) patients in the OC underwent re-interventions, both were for type Ib endoleaks in cases of partial graft explantation.
Outcomes and Modes of Failure by Device
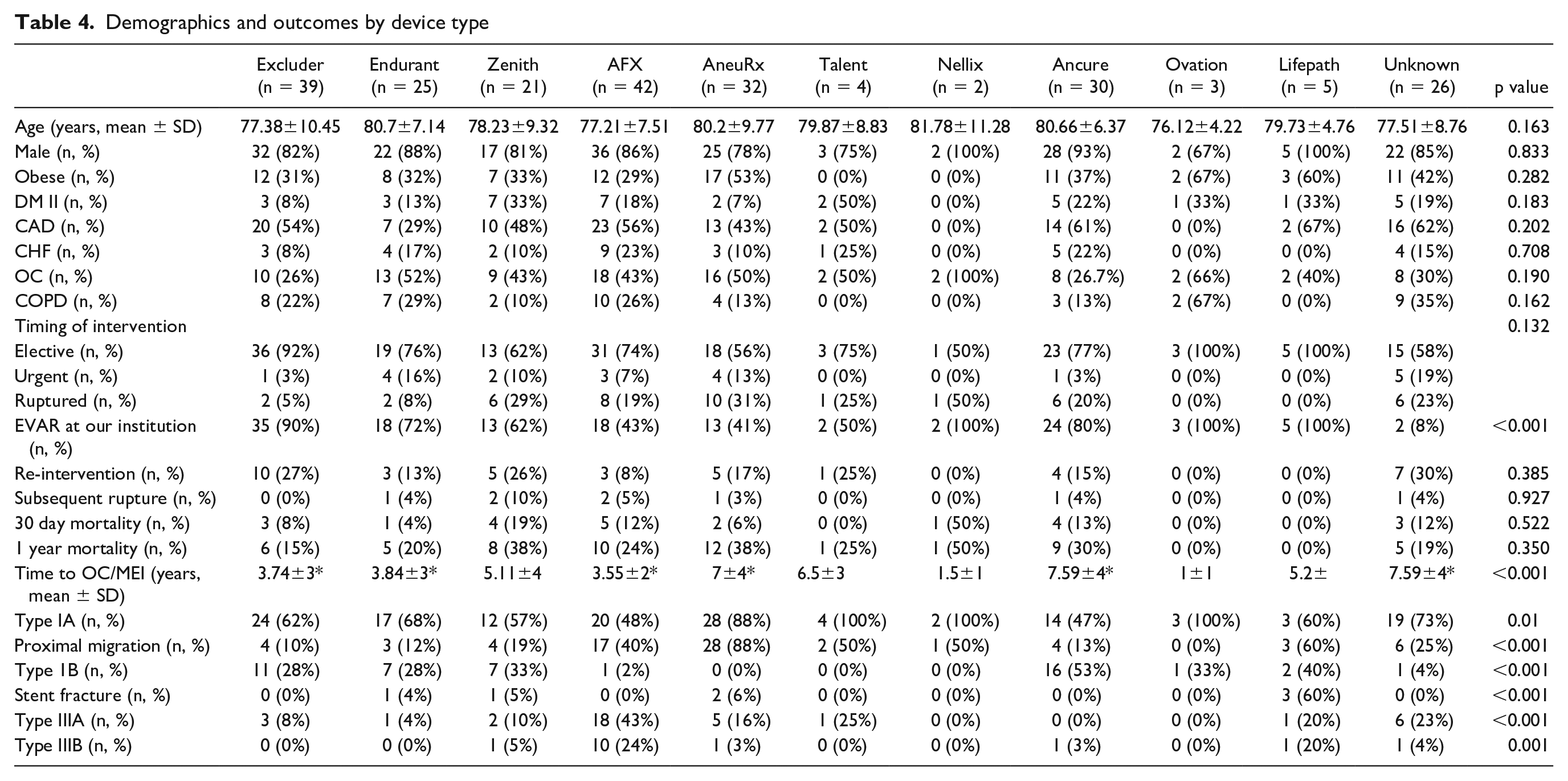
There were no significant differences in demographics, comorbidities, type of re-intervention (MEI vs OC), clinical presentation (rupture vs non-ruptured,) or post-operative outcomes among different devices (Table 4). However, we did note differential presentations with regard to the mode of failure of difference endografts. Type 1A endoleak was the most common presentation overall in most device types, except for AFX which was more likely to present with a type III and ancure which was more likely to present with a type IB endoleak. Proximal migration was most frequently noted with AneuRx and AFX, 17/20 AFX devices with a type IA endoleak had proximal migration, and all 28 AneuRx devices with a type IA endoleak had evidence of proximal migration. Type IB endoleak was a common presentation of the Ancure device, comprising 16/30 of endoleaks in the Ancure group. Type III endoleaks were a prominent presentation of AFX devices, accounting for 28/52 of type III endoleaks in the cohort. Of the type III endoleaks in AFX devices, 18/28 were type IIIA secondary to component uncoupling, and 10/28 were type IIIB secondary to fabric tears. Furthermore, type III endoleaks continued to be a prominent presentation even in AFX devices implanted after 2014, which marked the transition from the first-generation Strata fabric to the upgraded Duraply stent graft material, 7/16 AFX devices implanted after 2014 presented with type III endoleaks (3 IIIA and 4 IIIB). Time to re-intervention was significantly longer for AneuRx and Ancure devices compared with Excluder, Endurant, and AFX (p<0.05) but not different compared with Zenith devices (Table 4).
Demographics and outcomes by device type
Discussion
In this retrospective analysis of 229 patients who underwent repair MEI/OC for type I and III endoleaks, we showed that re-interventions for type I and III endoleaks are common among a wide range of commercial and discontinued EVAR devices. Re-interventions are associated with significant post-operative morbidities such as renal failure and respiratory failure and mortality. Re-interventions for type I and III endoleaks were associated with 25% mortality (57/229) [23% 32/139 in MEI and 28% 25/90 in OC] at 1 year. Type IA endoleaks are the most common mode of major failure among most devices; however, different devices appear to be associated with differential modes of failure, such as type III endoleak in AFX devices and proximal migration in AneuRx and AFX devices.
Type I and III endoleaks, while not necessarily common after EVAR, can be catastrophic failures with significant risk of morbidity and mortality following re-interventions. Scali et al compared open surgical conversion after EVAR to primary open juxta-renal AAA repair and found that the surgical conversion after EVAR group had a 16% mortality at 1 year follow-up and a 28% rate of AAA-related intervention or death at 1 year. 12 Similarly, Turney et al reported on a series of 100 consecutive patients requiring explant after EVAR; the most common indications for explant in their cohort was type I and III endoleaks, and the 30 day mortality was 10% for patients undergoing elective explant secondary to an endoleak (excluding infection). 13 These findings are similar to the mortality rates observed in our series especially for patients undergoing OC. Even with endovascular treatment, re-interventions for type I and III endoleaks remains a source of substantial morbidity and mortality. In a series by Naughton et al of 22 patients with type I and III endoleaks treated by endovascular means, they observed an 18% mortality rate during their follow-up period (median=14 months). 14 Similar results were seen in a systematic review and meta-analysis of type III endoleaks by Kwon et al; they identified 46 type III endoleaks the majority of which were treated with endovascular techniques (29/46 endovascular, 8/46 hybrid, 9/46 open), with an overall perioperative mortality of 15.2% (7/46). 15 The risk of morbidity and mortality persists in long-term follow-up; Maleux et al report a series of 20 patients with 25 type III endoleaks with 25% AAA-related re-interventions and 40% mortality throughout their 10 year follow-up period. 16
Although morbidity and mortality do not necessarily differ between devices, certain types of endoleaks have a predilection to occur with certain device types. The US Food and Drug Administration (FDA) in 2018 issued a class I recall of Endologix AFX devices due to a higher tendency of type III endoleaks associated with fabric tears; this is demonstrated in our cohort where type III A and B endoleaks were most frequent with AFX (Table 4). A more recent warning by the FDA indicated that it is uncertain whether the newer generation AFX devices mitigate the risk of endoleak and urged providers and patients to consider alternatives options in the endovascular treatment of AAA. 17 This was a response to the findings published in several series. Skibba et al in 2015 reported on a series of 701 patients who underwent primary EVAR with Endologix Powerlink and AFX devices, 32/701 required re-intervention for endoleaks, and 19 for type III endoleaks (17 type IIIA and 2 IIIB). 18 Similarly, Lemmon et al in 2015 reported on a series of 151 consecutive EVARs at a single institution (83 Endologix endografts and 68 other grafts), when comparing Endologix endografts (AFX and Powerlink) to all others they noted 14 type III endoleaks (6/14 IIIA and 8/14 IIIB) in the Endologix cohort compared with none in the non-Endologix cohort, and this was associated with an increased risk of re-intervention compared with non-Endologix devices. 19 Although we were not able to report incidence rates given our study design, we did note that AFX devices were more likely to present with type III endoleaks compared with other devices, accounting for 28/52 type III endoleaks in our cohort. Interestingly, we found that this held true even for AFX devices implanted after 2014 after which changes were made to both the AFX endograft fabric (first-generation Strata fabric was replaced by the Duraply fabric) and to the AFX IFU criteria to mitigate the risk of type III endoleak.
Another specific mode of failure observed in our study was proximal migration, which was common with AneuRx and AFX devices. AFX devices have not been associated with proximal migration in prior published series; however, those series like our own have limited data on IFU criteria, making it difficult to ascertain whether the cause of migration was non-compliance with IFU criteria, device migration, or neck degeneration. However, multiple published series have reported on the failure mode of the AneuRx device, with the propensity of the device to present with type IA endoleaks and specifically with endograft migration or loss of proximal fixation. van Lammeren et al described secondary interventions following AneuRx devices, in 212 AneuRx patients. Of total, 59/212 (28%) required secondary interventions for endoleaks, with type IA being the most common (28/59), the 30-day mortality after re-intervention was 5% (3/62).20,21 Sampaio et al described a series of 109 patients undergoing primary EVAR with AneuRx device, with 15 patients developing endograft migration within 1 year of implantation, which was associated with a 3.39 fold increase in type IA endoleaks in those patients. 22
The median time to re-intervention after the initial EVAR in our cohort was about 4 years, and longer for devices that were removed from the market (7 years AneuRx, 7.48 Ancure). This highlights the necessity of diligent surveillance and follow-up imaging, even for discontinued devices. Furthermore, the utilization of EVAR for off label use has also increased over time. 23 This off label utilization has been associated with worse outcomes with regard to in-hospital mortality, endoleak, migration, and re-intervention in multiple series.24 –26 As the role of EVAR, and specifically off label EVAR in the treatment of AAA continues to increase, careful and perhaps more frequent imaging surveillance targeting known modes of failure of particular endografts is necessary to prevent catastrophic failures of these devices.
Our study has several limitations, as a single-center study and a retrospective analysis both of which can introduce bias and affect the generalizability of our results to larger cohorts. In addition, because a substantial proportion of devices were implanted at outside institutions, no estimates could be made of failure rates based on IFU, or differential rates between devices; therefore, this study does not serve as a comparison of incidence of stent graft failure, rather as a description of differential modes of failure across stent grafts. Furthermore, there was no standardized follow-up protocol seeing as a large proportion of patients were referred into our system. Despite these limitations we feel this study sheds light on specific modes of failure of different commercial devices reflecting a real-world experience of endograft re-interventions while updating and expanding on the existing literature.
Conclusions
Modes of failure differ following EVAR across commercially available and discontinued endografts, suggesting that specifically targeted surveillance protocol or modalities to identify these types of endoleaks to prevent significant morbidity and mortality is essential. Type I and III endoleaks can have a delayed presentation, highlighting the importance of long-term follow-up and careful device specific interrogation of the endovascular repair, even in discontinued devices.
Footnotes
Author’s Note
This manuscript was presented as an oral presentation at the 2021 meeting of the Eastern Vascular society in Charleston, SC.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr M.M. is a member of the advisory boards of Gore and Medtronic.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Othman Abdul Malak was funded through NIH grant T32 HL 098036-11 for dedicated research time.