
Abstract
Purpose:
To demonstrate the technical aspects of the novel Penumbra Indigo Lightning Flash System (Penumbra, Inc.) for mechanical thrombectomy of pulmonary embolism (PE).
Technique:
The novel Penumbra Lightning Flash catheter is a 16 French (F) sheath-compatible device designed for advanced thrombectomy, especially in the pulmonary arteries. This device has large thrombus burden removal capacity; however, technical nuances are necessary to accomplish more with efficacy pulmonary embolism management. Access sites, pulmonary arteries catheterization technique, thrombectomy device navigation and mechanism of action are described thoroughly.
Conclusion:
Penumbra Indigo Lightning Flash system for mechanical thrombectomy as other catheter-directed treatments (CDTs) represents a major advance in contemporary PE management. With favorable safety profile and efficacy, CDTs have become an integral component of the multidisciplinary approach to PE care.
Clinical Impact
The article highlights the Penumbra Indigo Lightning Flash System as a significant advancement in mechanical thrombectomy for pulmonary embolism (PE). By detailing technical aspects and procedural nuances, it supports clinicians for improvement in endovascular PE management. The system’s integration into multidisciplinary care represents a major step forward, providing an effective alternative to traditional therapies, particularly for high-risk PE patients. This innovation promises to enhance patient outcomes in contemporary PE management.
Keywords
Introduction
Venous thromboembolism (VTE), clinically presenting as deep vein thrombosis (DVT) or pulmonary embolism (PE), is globally the third most frequent acute cardiovascular syndrome. 1 Pulmonary embolism poses a significant threat to global health, often necessitating prompt intervention to mitigate potentially fatal outcomes and may cause <300.000 deaths per year in the United States. 2 While systemic anticoagulation remains a cornerstone of treatment across all risk categories, selected patients may benefit from adjunctive endovascular therapies. 3 Among these, the Penumbra Indigo Lightning Flash Mechanical Thrombectomy System (Penumbra, Inc.) has garnered attention for its potential to alleviate thrombus burden in the pulmonary vasculature. This review synthesizes current literature to elucidate the efficacy and technical nuances of employing this device for PE management, encompassing its mechanism of action and procedural intricacies.
Technique
Device Description
The novel Penumbra Lightning Flash catheter is a 16 French (F) sheath-compatible device designed for advanced thrombectomy. Utilizing advanced clot detection capabilities, the Lightning Flash system can achieve near-pure vacuum aspiration when actively engaged with thrombotic material. The Computer Assisted Vacuum Thrombectomy (CAVT) System has dual clot detection algorithms (Pressure differential and flow-based algorithms) and leads to quicker clot detection and quicker patent flow detection to reduce potential blood loss, compared with the traditional Indigo System Lightning 12F (Figure 1). The catheter exhibits trackability and atraumatic properties, facilitating navigation through remote vascular anatomies, including the pulmonary arteries. The device is packed with a 6F Select Bernstein Tip shape (HTORQ) or H1 Tip (XTORQ) and has working lengths of 80 cm (HTORQ Tip), 100 cm (XTORQ and HTORQ Tips), and 115 cm (HTORQ Tip). Those lengths options can be selected based on the access site of the procedure. One of the major advantages of the novel Flash 16F system, aside of the dual clot detection algorithms that reduce blood loss, is a larger size suction catheter that can more effectively suction thrombus out compared with the Indigo System Lightning 12, while maintaining trackability and atraumatic properties. Despite the increase in size, the Lightning Flash catheter is 2 times softer than the Lightning 12.
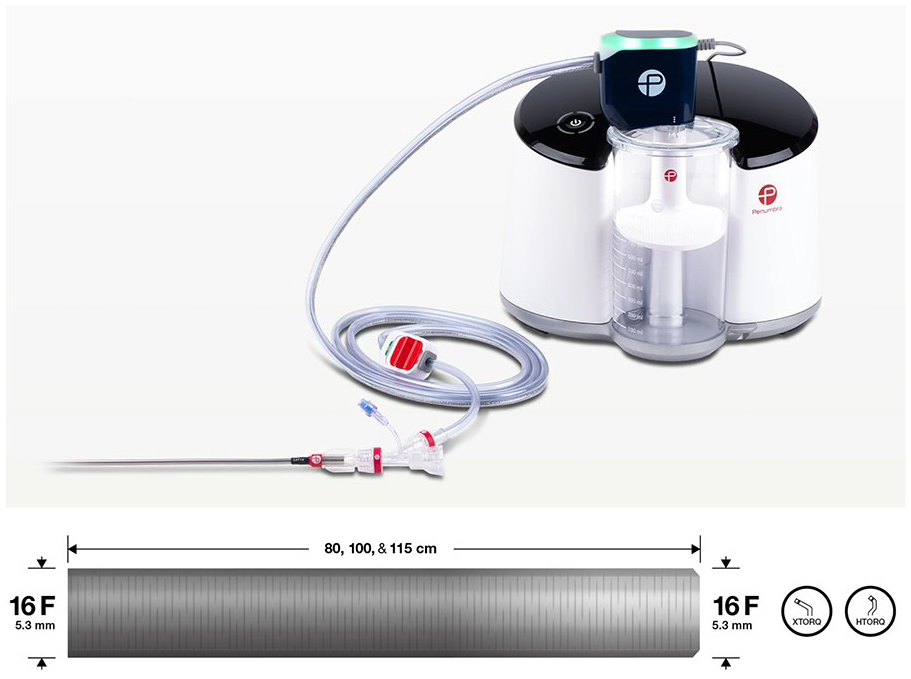
Penumbra Lightning Flash 16F sheath compatible system. The catheter is composed of a singular stainless steel, laser-cut hypotube. The stainless-steel composition enables 1:1 torqueability for the operator, resulting in safe navigation even in tortuous anatomy. The novel Computer Assisted Vacuum Thrombectomy (CAVT) system enables quicker clot detection and quicker patent flow detection to reduce potential blood loss. The system has a variability of working lengths and 6-F Select catheter tips.
Intraoperative Technique
The procedure takes place in a last generation hybrid operating room. Patients presenting with high-risk or severe pulmonary embolism, often accompanied by right ventricular (RV) overload or failure, commonly exhibit hypotension or are at high risk of developing severe hypotension during anesthesia induction, intubation, and positive pressure ventilation. Whenever possible, our standard practice involves non-invasive ventilation via a high-flow nasal cannula as an alternative to intubation, which may induce adverse hemodynamic effects due to positive intrathoracic pressure. Anticoagulation should not be interrupted for the procedure. Access is obtained through the femoral vein using a 7 French femoral sheath. Prior to insertion, a single Proglide (Abbott Vascular, CA, USA) presuture is routinely deployed to accommodate the larger 16-F or 20-F sheaths required for the procedure. However, manual compression following large sheath removal also serves as an effective alternative. It is important to note that when manual compression is anticipated at the end of the procedure, it is preferable to select the femoral access on the contralateral limb to the deep vein thrombosis. This approach helps to prevent additional venous outflow restrictions on the side where compression dressing is applied.
An initial venogram is conducted postaccess to verify thrombus clearance in the iliofemoral segment and the inferior vena cava. If thrombus burden is present, iliocaval thrombectomy should be considered, or an alternative access route, such as the right internal jugular vein, should be established. Subsequently, a 16-F 33cm or 20-F 33 cm Gore DrySeal sheath (Gore & Associates, AZ, USA) is introduced. The decision to initially utilize a 20-F sheath is to allow bilateral PA thrombectomy or for potential implementation of a buddy-wire technique in the pulmonary arteries, if needed, to stabilize and facilitates navigation of the Indigo device in tortuous anatomical configurations. Accurate identification of the thrombus location based on preoperative computed tomographic pulmonary angiography (CTPA) is crucial to optimal target pulmonary artery catheterization. Inaccurate target vessel catheterization can lead to ineffective thrombectomy.
Pulmonary artery catheterization is typically a straightforward step of the procedure. However, it is not our standard practice to employ a hydrophilic 0.035 wire and a catheter for this step. This approach involves extensive manipulation of the guidewire within the right atrium and ventricle, which can potentially lead to arrhythmias and perforation, posing challenges for intraoperative diagnosis of this complication. Instead, we opt to perform pulmonary artery catheterization using only a Torcon NB AP2 Shaped Catheter (Cook Medical, Bloomington, IN, USA). This catheter offers sufficient pushability and torqueability to navigate to the right ventricle, and with rotation and push maneuvers, it facilitates navigation to the main pulmonary artery (Figure 2).
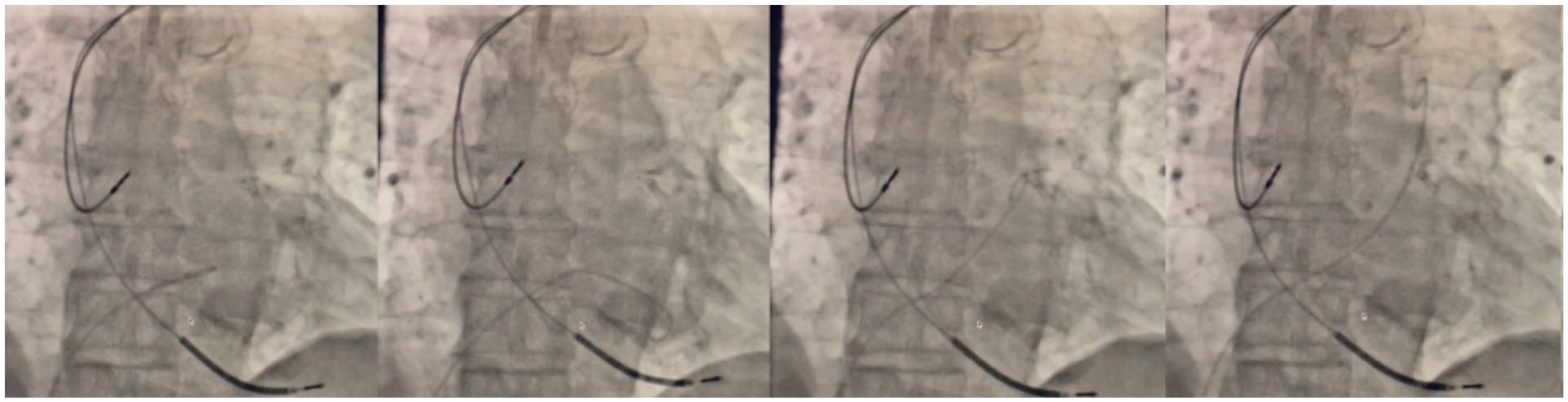
Pulmonary artery catheterization. (A) Placement of the Torcon NB AP2 Shaped Catheter (Cook Medical) in the right atrium. (B) Successful catheterization of the right ventricle. (C and D) Rotational and pushing maneuvers facilitate main pulmonary artery catheterization.
The left pulmonary artery typically presents a more straightforward catheterization due to its relatively straight anatomy. Following target pulmonary artery catheterization, the AP2 catheter is pushed as far as possible and a 0.035x260 cm 1 cm J-shaped tip Amplatz guidewire is securely positioned, followed by the insertion of the Lightning Flash 16F catheter over the wire. Angiography can be conducted through the thrombectomy catheter after dilatator removal, and the Amplatz guidewire is then retrieved prior to commencing thrombectomy to optimize space within the device and enhance aspiration efficiency.
Thrombus aspiration is initiated, with the catheter’s reservoir displaying a yellow light to indicate active engagement with the clot. Upon completion of thrombectomy, the system signals with a green light, indicating disengagement from the clot, prompting the immediate cessation of the system to minimize blood loss. Subsequently, final angiograms are obtained, and in the event of residual clot within the pulmonary artery or segmental arteries, targeted vessel catheterization can be performed over the 6F Select Catheter inside the Indigo catheter, followed by exchange for an Amplatz wire and device advancement over the wire with the dilatator tip. After adequate positioned near the thrombus, the wire can be again retrieved and new thrombectomy performed. Care must be taken with extensive hydrofilic guidewire manipulation into the pulmonary arteries due to the increased perforation risk.
In a minority of cases, device navigability can be more challenging due to a tortuous pulmonary anatomy. In these circumstances a lateral puncture into the 20-F sheath is performed, followed by catheterization of the contra lateral PA and an Amplatz guidewire secured to allow to perform a buddy wire technique (Figure 3). This maneuver provides more system stability to navigates the Indigo catheter into the target PA.
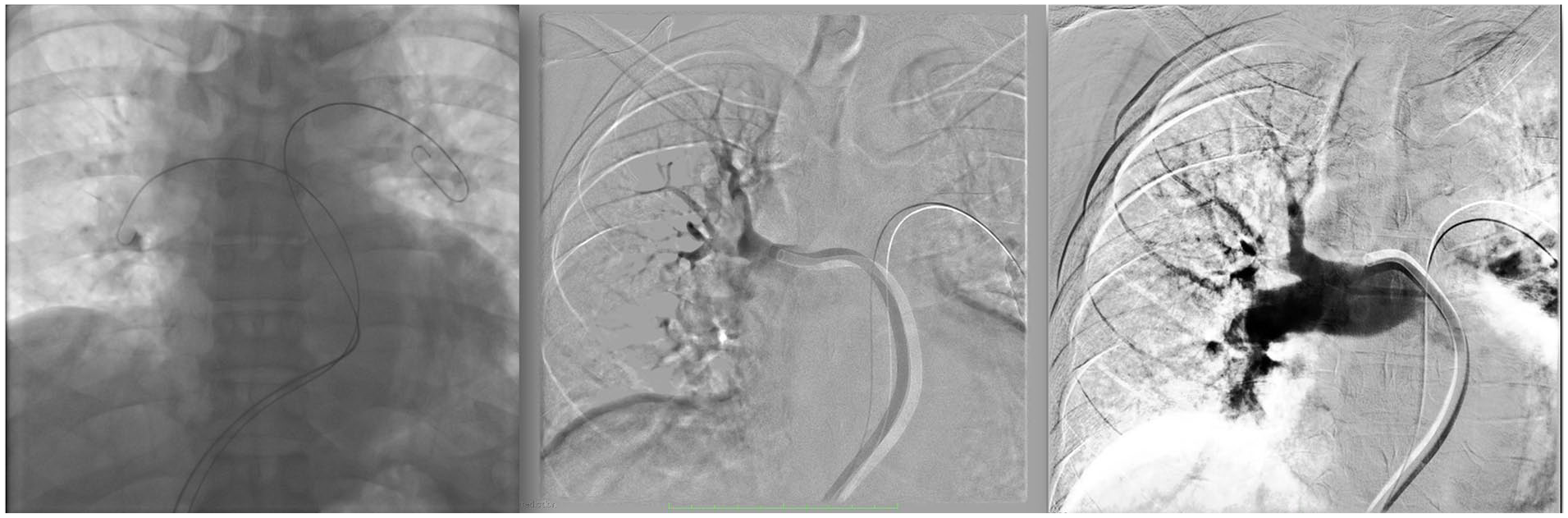
(A) Intraoperative angiography showing bilateral pulmonary arteries (PA) catheterization and the Amplatz guidewire securely positioned for a “buddy-wire” technique, enhancing systemic support for right PA mechanical thrombectomy. (B) Initial angiography using the Penumbra Indigo 16-F Catheter reveals a significant thrombus burden in the superior trunk of the right pulmonary artery. (C) Final angiography postmechanical thrombectomy demonstrates complete clot removal in the right PA.
If bilateral pulmonary artery thrombectomy is planned, our protocol involves securing an Amplatz guidewire in each PA at the start of the procedure, followed by sequential thrombectomy.
In cases involving extensive thrombus burden in bilateral iliac veins or the vena cava, or when the presence of a previous infrarenal vena cava filter with thrombus burden complicates femoral access, our preferred approach is via the right jugular vein. In such scenarios, our initial choice is the Lightning 12F catheter. Following jugular vein access, the target pulmonary artery (PA) is catheterized as outlined previously, and a 12F × 45 cm HFAN Sheath (Cook Medical) is securely positioned within the target vessel and the 12F thrombectomy device advanced (Figure 4). If residual thrombus is detected after thrombectomy with the 12F device, an Amplatz wire is secured within the target PA and the 16F Flash device advanced over the wire for more extensive thrombectomies. It is our choice to start with the lower profile device to mitigate the possibility of any cardiac injury due to the sharp angulation needed for thrombectomy from a superior approach. Nevertheless, in our experience performing the procedure from a jugular access with the 16F device is both feasible and safe. It is crucial, however, to ensure that the Amplatz wire is positioned as distally as possible within the target PA and that the system is advanced carefully while continuously monitoring hemodynamics and the cardiac monitor.
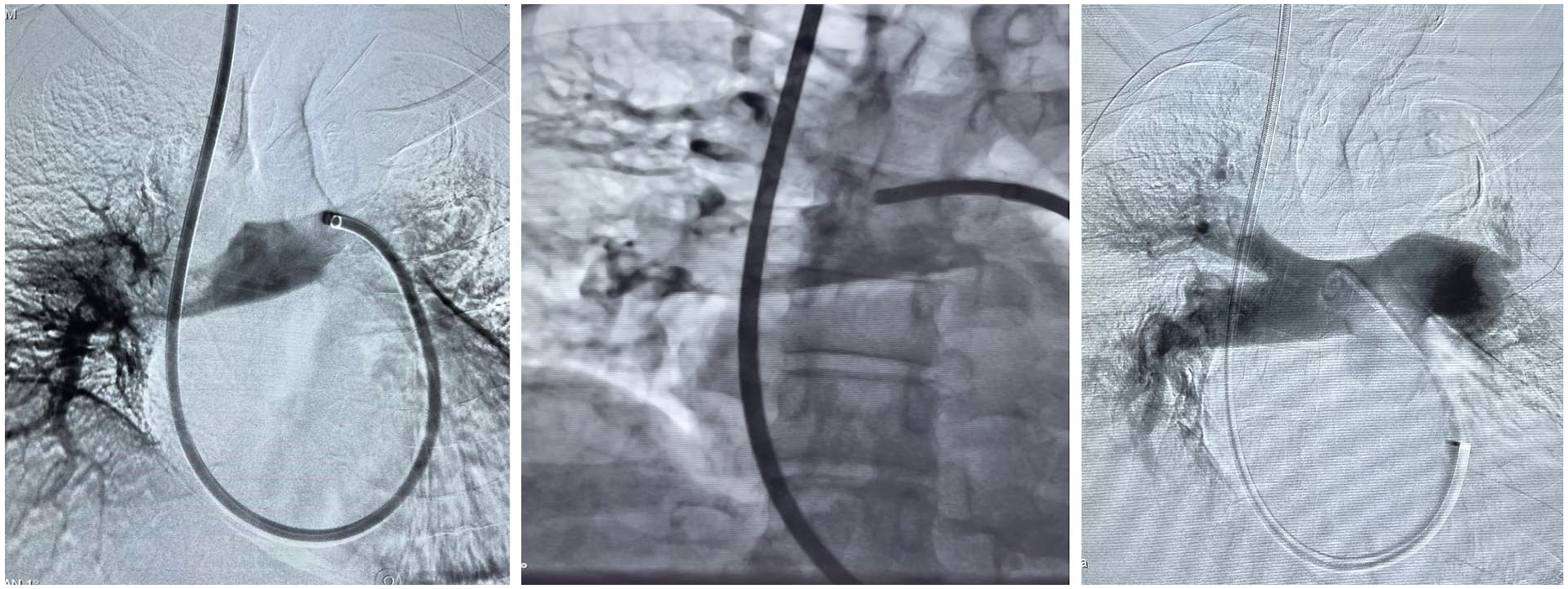
Right pulmonary artery mechanical thrombectomy with the Lightning Flash 12-F catheter from a right jugular approach.
Cardiac computed tomography images with measurements of right ventricular-to-left ventricular ratio (RV/LV) prethrombectomy and postthrombectomy should be employed in all cases, as RV/LV ≥ 0.9 was an independent predictor of an adverse intrahospital outcome both in overall population with PE and in hemodynamically stable patients.4,5 Postoperative difference between the baseline and the 48-hour RV/LV ratio and thrombus burden may serve as an efficacy marker aside of clinical evaluation (Figure 5).
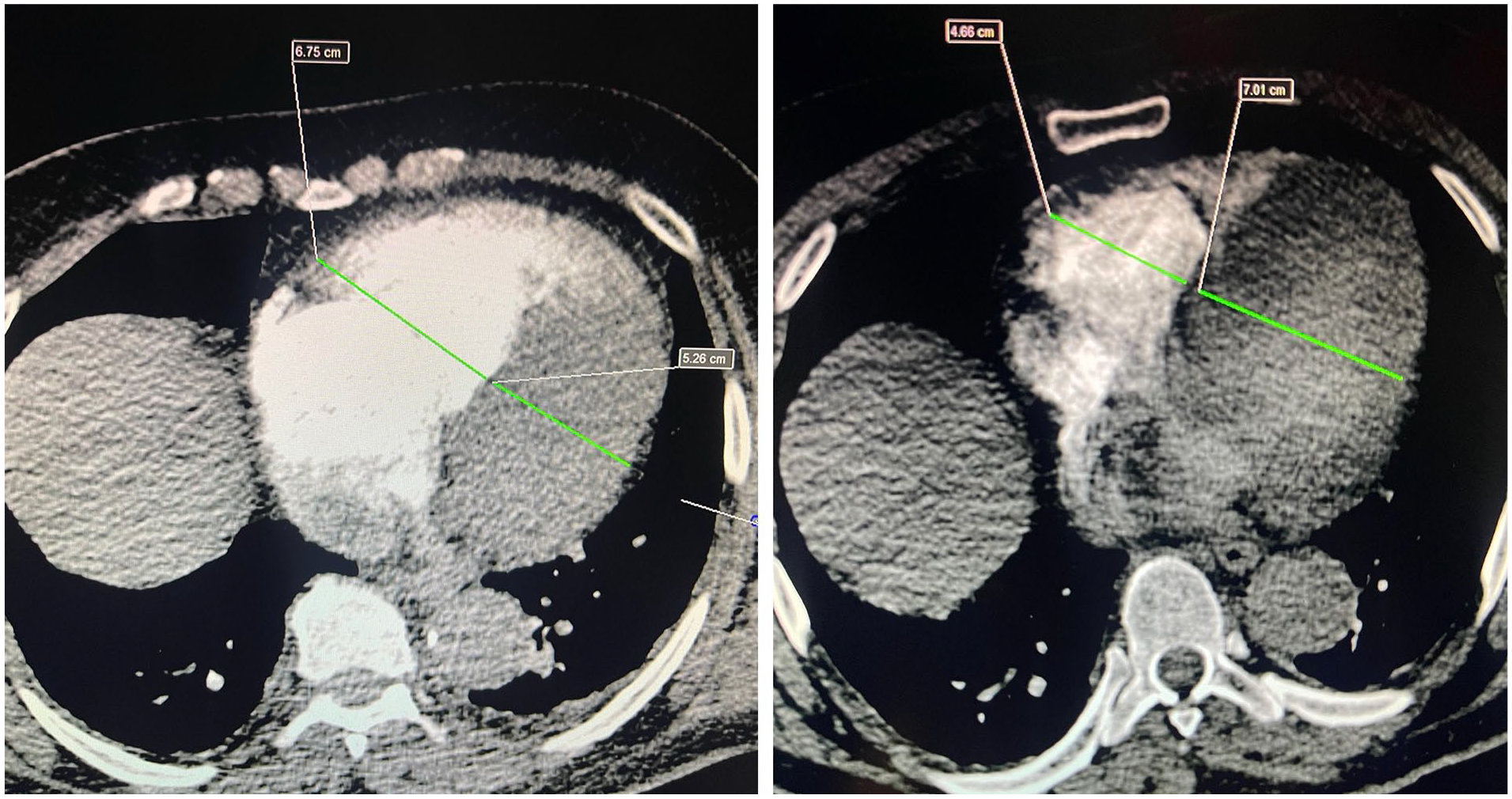
(A) Preoperative cardiac computed tomography of a high-risk patient with pulmonary embolism, illustrating an RV/LV ratio of 1.27. (B) Cardiac computed tomography 48 hours postthrombectomy, showing a reduced RV/LV ratio of 0.68.
Discussion
Although anticoagulation remains the cornerstone of treatment of pulmonary embolism across all risk categories, catheter-directed treatments (CDTs) has gained space in the last years as an important adjunctive therapy in many centers. First, intermediate, and high-risk PE must result in prompt activation of the PE response team (PERT). Previous report shows the impact of implementation of a multidisciplinary PE response team, with decreasing 30-day mortality, lower rater of major or clinically relevant non major bleeding and decrease use of inferior vena cava filters. 6
Rapid diagnostic should be employed with rigorous clinical evaluation, use of transthoracic echocardiography, computed tomographic pulmonary angiography (CTPA), low extremity ultrasound, laboratory biomarkers (troponin and brain natriuretic peptide) and risk stratification employed through prognostic clinical scores such as the low Pulmonary Embolism Severity Index (PESI) classes, that can reliable address the low-risk PE that requires anticoagulation alone. Patients with hemodynamic instability are classified as high-risk PE and must be evaluated for prompt reperfusion treatment. Furthermore, normotensive patients with evidence of RV dysfunction and elevated cardiac biomarkers are classified as intermediate-high risk patients. 3
Recommendations for acute-phase treatment of high-risk PE include anticoagulation and systemic thrombolytic therapy, as percutaneous CDT or surgical embolectomy should be considered for patients in whom thrombolysis is contra indicated or has failed. However, as thrombolytic therapy was associated with significant reduction in the combined endpoint of death or treatment escalation, PE-related mortality and PE recurrence, complications as major hemorrhage and fatal or intracranial bleeding were significantly more frequent among these patients. 3 Overall, in the setting of high-risk PE, the benefits of immediate reperfusion of systemic thrombolysis mostly outweighs the hemorrhage risks. Nevertheless, its widespread use is limited due to several contraindications.
For most normotensive patients of acute PE anticoagulation alone is adequate treatment. However, patients with at least one indicator of elevated PE-related risk, such as PESI class III-IV or serious comorbidity, should be hospitalized. In this group, patients with RV dysfunction accompanied by a positive troponin test, classified as intermediate high-risk PE, should be monitored due to the risk of hemodynamic collapse. Routine primary reperfusion treatment, notably full-dose systemic thrombolytic, is not recommended, as the risk of potentially life-treating bleeding outweighs the benefits. 3 The PEITHO 7 randomized controlled trial investigated the role of systemic thrombolysis in normotensive patients with intermediate-risk PE and demonstrated that the decreased risk of hemodynamic decompensation associated with systemic thrombolysis was not accompanied by a reduction in 7-day mortality and was associated increased risk of severe bleeding. In this context, rescue thrombolytic therapy, surgical embolectomy or CDTs should be reserved for patients who develop signs of hemodynamic deterioration.
In response to the limitations of systemic thrombolysis, CDTs represent a pivotal advancement in the management of pulmonary embolism (PE) and has emerged as an alternative treatment option that address thrombus burden while minimizing systemic effects. Techniques such as mechanical thrombectomy and catheter-directed thrombolysis enable direct removal or dissolution of thrombi, thereby restoring pulmonary blood flow and alleviating RV strain. Overall, several interventional options are currently available and include in situ thrombolysis, ultrasound-assisted thrombolysis (USAT), fragmentation techniques, mechanical aspiration devices and rheolytic therapies. 8
Local thrombolytic therapies, consists in positioning a dedicated multiperforated catheter into the thrombotic pulmonary arteries to deliver low-dose thrombolytic drug, which aims to maximize thrombolytic efficacy while reducing bleeding complications. Dosing regimens vary among centers, but overall, 0.5 to 1 mg/h alteplase per catheter, with total dose not exceeding 30 mg for about 12 to 24 hours under monitoring. The infusion should be stopped in case of major bleeding or evidence of hemodynamic improvement.8,9
The EkoSonic Endovascular System (Boston Scientific, Marlborough, MA) is an USAT device that achieves increased thrombolytic drug penetration into the thrombus at a lower dose over a short duration and it’s an evolution of the standard in situ thrombolysis. The SEATTLE II study enrolled 150 acute massive or submassive PE patients treated with ultrasound-assisted catheter-directed thrombolysis and reported an associated reduction in the RL/LV ratio at 48 hours, but also a 10% major bleeding rate, with no intracranial hemorrhage, within 72 hours of treatment. 10
Mechanical thrombectomy interventions include catheter-directed thrombus fragmentation, rheolytic therapy and the novel aspiration devices. Pigtail thrombus rotational thrombectomy is easily available; however, effectiveness is poorly described and carries a risk of distal embolization. The AngioJet device (Boston Scientific, Marlborough, MA) is a rheolytic system that uses pressurized fluid to disrupt thrombus and a vacuum to actively remove debris and can result in shorter treatment time and flow restoration.8,11,12 However, is associated with a higher incidence of serious adverse effects in massive PE treatment, such as asystole and atrioventricular blocks and should be used with extreme caution.8,13
Mechanical aspiration devices, such as the Indigo System herein described, aims to restore hemodynamic by removing thrombus burden and preventing distal embolization. Results of the EXTRACT-PE trial regarding mechanical aspiration with Indigo Aspiration 12-F System, demonstrates significant reduction in RV/LV ratio and lower major adverse event rate in submassive PE patients. Intraprocedural thrombolytic drugs were avoided in 98.3% of patients. Rates of cardiac injury, pulmonary vascular injury, clinical deterioration, major bleeding, and device-related death at 48 hours were 0%, 1.7%, 1.7%, 1.7%, and 0.8%, respectively. 14 Follow-up was 30 days and all-cause mortality was 1.1%.
The novel Indigo Lightning Flash 16-F System herein described was design to address with more efficacy thrombus burden in PE compared with the 12-F device, however further studies are necessary to demonstrates clinical improvement and major adverse event rates. Important limitations of this device are that is possibly only effective in fresh thrombi and have no possibility to reinfuse aspirated blood, leading to mild blood loss that usually does not exceed 400 mL, rarely leading to the need for transfusions.8,14
Approximately half the patients who receive a diagnosis of pulmonary embolism have functional and exercise limitations 1 year later (known as post–pulmonary-embolism syndrome), and the health-related quality of life for patients with a history of pulmonary embolism is diminished as compared with that of matched controls. 15 Further evidence with mid- and long-term results is necessary to place CDTs as the main therapy for pulmonary embolism, especially in intermediate and high-risk patients. Nevertheless, while CDTs hold promise as an alternative to systemic thrombolytic treatment, current guidelines do not recommend them as a first choice for any PE category.3,8
Conclusion
The novel Penumbra Indigo Lightning Flash system for mechanical thrombectomy as other CDTs represents a major advance in contemporary PE management. With favorable safety profile and efficacy, CDTs have become an integral component of the multidisciplinary approach to PE care, particularly in high-risk and intermediate-high risk PE patients with contraindications to systemic thrombolysis. The technical aspects and pitfalls of mechanical aspiration with the novel 16-F Indigo Flash system were highlighted in this paper. Continued research is essential to further refine techniques, optimize patient selection, and enhance PE management.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: TC is a speaker for Penumbra, Inc. The other authors have no conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.