
Abstract
Purpose:
To report the use of modified ex vivo renal artery (RA) reconstruction in a patient with 2 small right RAs (RRAs) in anticipation of planned fenestrated-branched endovascular aortic repair (FB-EVAR) of thoracoabdominal aortic aneurysm (TAAA).
Case Report:
A staged hybrid repair was utilized in a patient with Extent II TAAA involving celiac axis (CA), superior mesenteric artery (SMA), single left RA (LRA), and 2 small (<3 mm) RRAs. The first-stage operation consisted of hepato-renal bypass using modified ex vivo renal reconstruction with single end-to-end anastomosis to both RAs using a saphenous vein graft. A second stage FB-EVAR was performed using patient-specific manufactured stent-graft with 3 fenestrations for the CA, SMA, and LRA 6 weeks later. The patient recovered with no complications. At 4 years, the patient had widely patent hepato-renal bypass and target vessels with normal renal function.
Conclusion:
The use of adjunctive hybrid procedures may optimize or facilitate FB-EVAR. In this patient, salvage of 2 small RAs was not ideally suited for branch stenting but was possible using modified ex vivo RA reconstruction with preservation of kidney parenchyma and function.
Clinical Impact
This case report illustrates a hybrid approach to overcome one of the most frequent limitations to total endovascular incorporation of renal arteries, eg small diameter, early bifurcation and multiple vessels. The modified ex vivo technique allows meticulous renal artery reconstruction without the deleterious effect of warm ischemia and without the cumbersome reconstruction of ureter and vein that is needed with traditional on table ex vivo auto transplantation. The technique is used in a minority of cases and adds the morbidity of open approach. Case selection is of paramount importance.
Keywords
Introduction
Thoracoabdominal aortic aneurysms (TAAA) make up roughly 3% of annually identified aortic aneurysms in the United States. 1 Open surgical repair (OSR) has been the gold standard treatment modality for TAAA repair. 2 In the last decade, fenestrated-branched endovascular aortic repair (FB-EVAR) has been increasingly used in the treatment of TAAAs, with several single and multicenter experiences showing lower morbidity and mortality as compared with OSR. One of the most frequent anatomical limitations to FB-EVAR is the presence of small renal arteries (RAs) or accessory RAs (ARAs) not suitable for branch stenting. 3
Double RAs originating from the aorta are the most common renal morphological variations with reported prevalence ranging from 14% to 30%. In a study of 272 kidneys, double RAs were present in 20% of samples; unilateral double RAs on the left side were predominant, accounting for 9.2%, which was 6.3% on the right.
4
In anatomically constraining patients, OSR may still be the best treatment option to maximize RA patency and preserve renal function. 7 However, a hybrid approach consisting of a staged open surgical reconstruction of a visceral artery followed by FB-EVAR in TAAA patients may reduce the risk of target vessel loss, minimize morbidity, and preserve end-organ function. 8 Herein, we report a patient treated by FB-EVAR for TAAA using a staged open surgical modified ex vivo RA reconstruction to preserve flow into 2 small right RAs (RRAs) with high-grade ostial stenosis prior to the FB-EVAR procedure.
Case Report
A 70-year-old female patient presented with an asymptomatic enlarging 6-cm Extent II TAAA on computed tomography angiography (CTA). The aneurysm involved the celiac axis (CA), superior mesenteric artery (SMA), a single left RA (LRA), and 2 small RRAs measuring < 3 mm with high-grade ostial stenosis each; the right kidney was not atrophic (Figure 1). Her past surgical history included prior thoracic endovascular aortic repair (TEVAR) of a descending thoracic aortic aneurysm 2 years prior to presentation. The patient’s history was notable for hypertension, hyperlipidemia, stage II chronic kidney disease, and past cigarette smoking. There was no evidence of hepatic or cholecystic disease. Pre-operative estimated Glomerular Filtration Rate (eGFR) was measured to be 72 mL/min. Because of the surgical risk and small caliber of the 2 RRAs, a staged open surgical RA reconstruction was planned, followed by a second-stage FB-EVAR.

CTA 3D reconstruction showing TAAA with involvement of the renal and mesenteric arteries and a thoracic stent-graft in the proximal descending aorta (A). Two small RRAs are present, each with high-grade ostial stenosis (B). Axial view of the image revealed the maximum aortic diameter of 5.8 cm and mural thrombi (C).
The first stage was performed using right subcostal incision. The 2 small RRAs were identified and dissected freely posterior to the inferior vena cava (IVC), along with the right renal vein (RRV), IVC, and the ureter. A segment of left great saphenous vein (GSV) was harvested. The RRV was clamped along with the 2 small RRAs, which were ligated and transected close to the aortic origin. A small venotomy was performed in the confluence of the RRV and IVC. The ureter was controlled with elastic vessel loops. The RAs were flushed copiously with cold renal perfusate the kidney became white (Figure 2A). The 2 small RRAs were anastomosed into the GSV graft using a single end-to-end spatulated anastomosis, followed by completion of the proximal end-to-side anastomosis into the common hepatic artery (CHA; Figure 2B–D). Once the anastomoses were completed, the venotomy was closed and flow was restored to the right kidney. Intraoperative duplex ultrasound revealed a widely patent hepato-renal bypass with no evidence of technical defects.
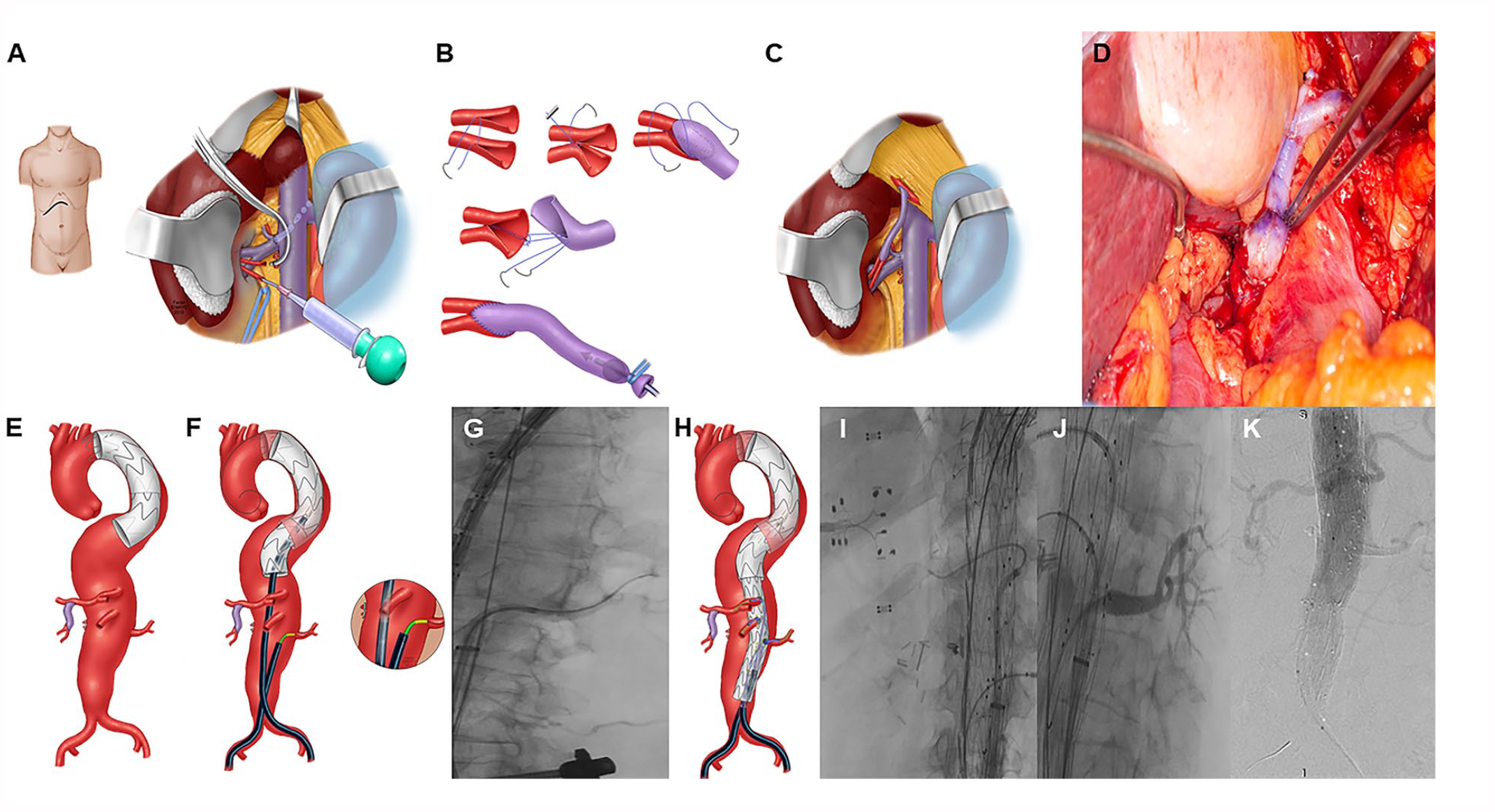
Summary of the staged procedures. Staged open surgical RA reconstruction was performed via right subcostal incision (A). Illustrations of reconstruction of 2 small ERA using end-to-end spatulated anastomosis into the GSV graft (B) and the proximal GSV anastomosed end-to-side into the CHA (C). Operative photo showing hepato-renal graft and the distal anastomosis (D). Illustrations of aortic anatomy and renal-mesenteric arteries at the time of FB-EVAR (E) and 20-French Sheath with guide catheters and wires in the thoracic and abdominal aorta, with a preloaded guidewire to the LRA (F). Using right femoral access, the LRA was catheterized to assist with calibration of onlay infusion with CTA (G). Illustration of selective catheterization of the celiac, SMA, and LRA fenestrations (H). Selective catheterization of the celiac and LRAs on fluoroscopic image (I) and patent LRA and distal branches after stent placement (J). Completion cone beam CTA demonstrating adequate aortic, visceral, and renal vessel perfusion (K).
The second-stage FB-EVAR was performed using proximal thoracic stent-graft (Zenith Alpha, Cook Medical Europe, Bjaeverskov, Denmark) and a manufactured patient-specific fenestrated aortic stent-graft (Cook Medical, Brisbane, Australia) with 3 fenestrations for the CA, SMA, and LRA 6 weeks after the first-stage operation. The procedure was done via total percutaneous transfemoral approach. A 20-French sheath was advanced via the left femoral approach into the abdominal aorta and accessed with 6-7 Fr sheaths and guide catheters for selective catheterization of the renal-mesenteric arteries (Figure 2E and F). Lunderquist wires were advanced to the thoracic aorta under the protection of Kumpe catheters. The proximal thoracic stent-graft was placed into Zone 3, and a second distal component was introduced and deployed in Zone 5. The fenestrated device was deployed with perfect apposition between the 3 fenestrations and target vessels. Using a preloaded femoral guidewire, a 6 Fr sheath was advanced through the LRA fenestration and used for catheterization of the LRA (Figure 2F and G). The SMA and CA fenestrations were performed via the contra-lateral femoral approach using 7 Fr sheaths over Rosen guidewires (Figure 2H and I). The diameter-reducing ties were released followed by the removal of the delivery. Each fenestration was sequentially stented using iCAST-covered stent-grafts (Figure 2J; Atrium Medical Corporation, Merrimack, New Hampshire), with reinforcement of the SMA fenestration using VBX stent-graft (W.L. Gore & Associates, Inc., Flagstaff, Arizona). The repair extended distally with a tubular stent-graft into the infrarenal aorta. Completion digital subtraction angiography showed evidence of a type Ic endoleak from the LRA. This was revised with angioplasty. A cone beam CT was analyzed and revealed no further technical defects and no evidence of type I or III endoleaks (Figure 2K).
The patient’s course was uncomplicated except for an incidental asymptomatic sub-segmental pulmonary embolism (PE) on pre-dismissal CTA. Lower extremity ultrasound also demonstrated focal acute deep venous thrombosis within the bilateral gastrocnemius and left soleal veins. The patient was treated with anticoagulation for 3 months. At hospital dismissal, the patient eGFR was 85 mL/min. The patient required a secondary intervention for type IIIc endoleak involving the SMA stent at 6 months after the FB-EVAR. The patient was doing well without evidence of hepatic or cholecystic disease during the follow-up. At 4 years, eGFR was measured to be 46 mL/min; follow-up CTA revealed no evidence of Type I or III endoleak, and widely patent fenestrated stents and right renal bypass with stable aneurysm sac diameter (Figure 3).
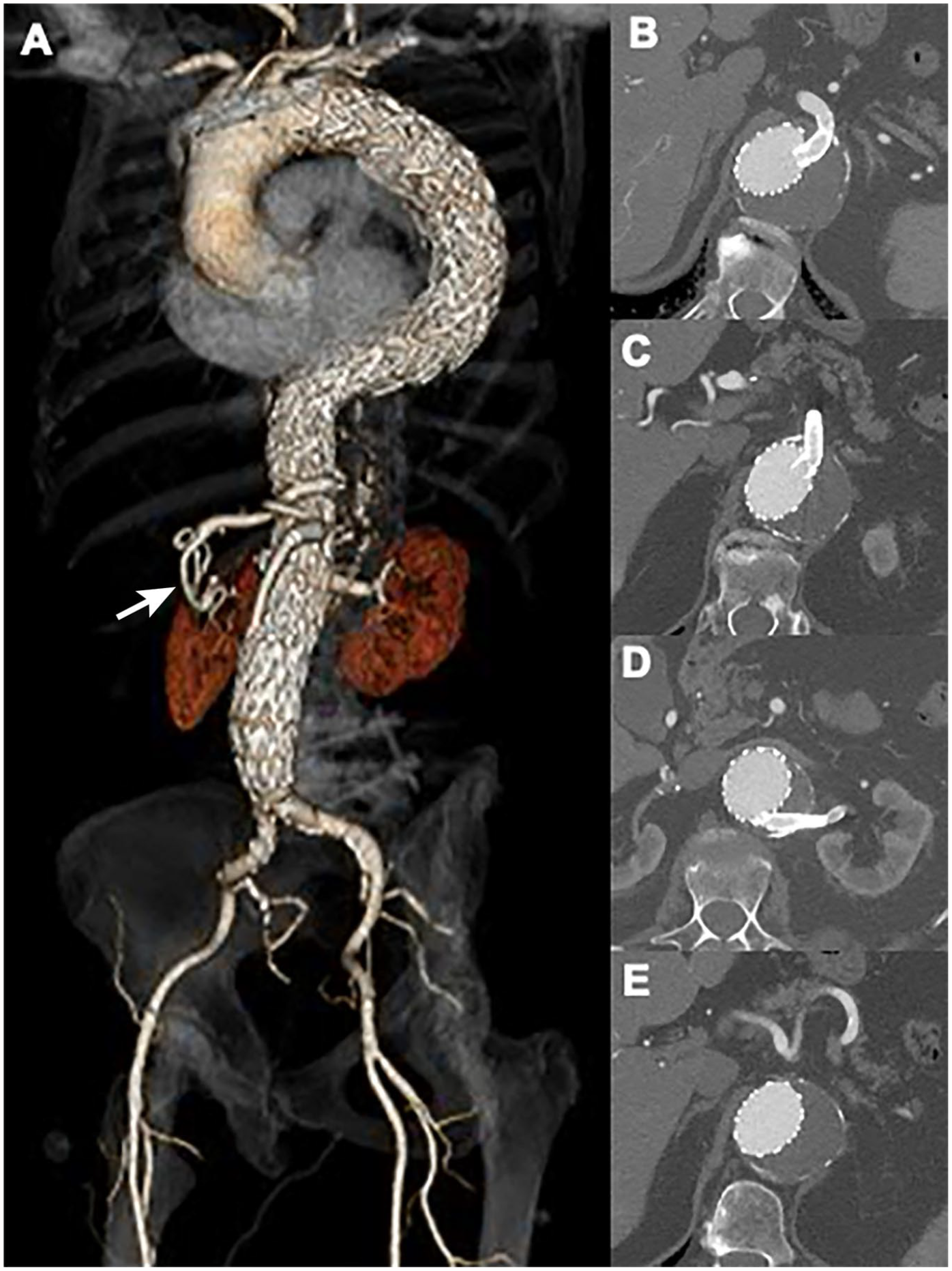
Four-year follow-up CTA demonstrated well-positioned aortic devices without migration or type I or type III endoleaks (A), and widely patent celiac (B), SMA (C), left renal fenestrated stents (D), and hepato-renal bypass graft (E) on axial view.
Discussion
Endovascular TAAA repair has rapidly evolved in the modern era with increasing utilization of FB-EVAR. 9 Although several single and multicenter studies have shown favorable early and mid-term outcomes, 10 anatomical constraints often limited the ability to incorporate side branches using stents. The presence of small RAs or RAs with early branch bifurcation is one of the most frequent limitations.
Sacrificing renal parenchyma may have significant clinical implications if there is deterioration of renal function. In these cases, a hybrid approach using extra-anatomical surgical reconstruction of the RAs may help optimize the endovascular procedure and minimize the risk of renal function deterioration. 11 Hybrid procedures were popularized by Quiñones-Baldrich, as a means to reduce the physiologic stress of open TAAA repair. 12 However, this approach fell in disfavor over FB-EVAR because of significant risks of mortality and complications. 13 With the advent of contemporary endovascular approaches as well as improved fenestrated and branched stent-graft designs, hybrid repair is infrequently utilized in most centers with access to these devices.
In the case herein presented the modified ex vivo technique allowed to meticulous reconstruction of the 2 small RRAs while minimizing the effect of prolonged renal ischemia. Several aspects of perioperative care have evolved since the procedure. We no longer advocated the use of prophylactic drains nor obtained pre-dismissal CTAs, although, in this case, this depicted an asymptomatic PE that could have resulted in significant clinical sequela if left untreated.
When considering treatment options, preservation of renal function is an imperative tenet of aortic repair. A prior investigation from the US Aortic Research Consortium demonstrated that AKI is associated with increased early major adverse events and decreased survival after FB-EVAR. 14 Maintaining renal function is further constrained anatomically when small RA and ARA are present, particularly when the RA diameter is 4 mm or smaller, as was present in our case, which measured <3 mm in diameter with high-grade ostial stenosis each, respectively. Branches or fenestrations were not considered for RRA incorporation due to concerns about long-term durability for small vessels even if technical success could be achieved. In addition, incorporation of <4.0 mm RAs during F-BEVAR has been reported to be associated with lower technical success and higher risk of arterial disruption during FB-EVAR procedure and increased risks of loss of kidney function and primary and secondary patency at 1 year. 15 This creates a formidable challenge for vascular surgeons and consideration of various options to preserve renal function should be explored. Staging multiple procedures, initially to preserve adequate renal function, followed by extensive endovascular treatment for TAAA can optimize long-term outcomes for select patients.
Furthermore, in cases where the aorta cannot serve as an inflow site, for example, due to landing zone coverage during the FB-EVAR procedure as we planned in our case, it leads to alternative strategies to achieve adequate renal perfusion. Hepato-renal bypass, consisting of autologous vein graft originating from the CHA in an end-to-side manner and anastomosing in the RRA offers such an alternative. This facilitated the endovascular procedure by eliminating the challenges imposed by the small-sized RAs. The CHA served as an adequate inflow site for renal perfusion for multiple reasons. Its proximity to the renal anastomosis site was beneficial as well as the liver itself being a dual blood supply organ. Given our patient’s baseline hepatic function was optimal and the majority of perfusion to the liver itself comes from the portal system, and there was no evidence of hepatic or cholecystic disease, we felt it was appropriate to take flow of the hepatic artery. Hepato-renal bypass has also been reported by Haulon and colleagues to be implemented in a 2-staged hybrid fenestrated EVAR of juxtarenal abdominal aortic aneurysm when the orifices of RRA and SMA were too close to hindering the utilization of fenestrations. 16
Device design was left at the discretion of the senior author. In our case, we selected 3 fenestrations at that time, which was 4 years ago, taken consideration of the anatomy of the CA, SMA, LRA, and the upgoing of the vessels. With more mid-term outcomes obtained, nowadays, we use branches rather than fenestrations when the aortic lumen at the level of the origin of the target vessels is very large. In general, branches are selected for target vessels that originated from wider aortic segments with a preferential caudal orientation, whereas fenestrations are selected when the target vessel originates from a minimally enlarged aorta. Indeed, for vessels originating in proximity the combination of 2 branches or 1 branch and 1 fenestration is a reasonable option and has been widely used by our group. In this case, we opted for bypass given the exceedingly small diameter of the RAs of less than 3 mm each. The senior author wants to emphasize the importance of surgeons utilizing open surgical approaches in suboptimal cases, rather than the endovascular approach in all cases even when anatomical conditions are poor.
Additionally, the decision to a hybrid approach of TAAA repair should be individualized according to patient surgical risk, aneurysm size, aortic anatomy, and life expectancy. In general, our approach has been to preserve renal function whenever possible and to avoid inadvertent or intentional sacrifice of renal parenchyma. We recommend considering the use of staged adjunctive hybrid reconstructions for target vessels that are not suitable for standard methods of endovascular incorporation.
Conclusion
This case illustrates a scenario in which small double RRAs were present in a patient with Extent II TAAA. A hybrid modality combining staged open surgical modified ex vivo RA reconstruction using hepato-renal autogenous GSV bypass graft, followed by endovascular repair of TAAA using aortic and fenestrated aortic stent-grafts was done successfully, and achieved favorable 4-year outcomes. This allows us to expand indications for FB-EVAR for previously unfit patients when a hybrid technique to reconstruct the visceral arteries is feasible to troubleshoot difficult anatomical constraints. The long-term durability of the technique is warranted, and ongoing multicenter collaboration will be needed to further advance the hybrid approach and continue to innovate the treatment modalities for TAAA patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Gustavo S. Oderich has received consulting fees and grants from Cook Medical, W. L. Gore, Centerline Biomedical, and GE Healthcare (all paid to Mayo Clinic and The University of Texas Health Science at Houston with no personal income).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.