
Abstract
Purpose:
To develop a strategy for the iliac vein stenting in patients with a combination of the left common iliac vein (LCIV) compression stenosis and pelvic venous insufficiency (PVI).
Methods:
This prospective comparative cohort study included 55 patients with hemodynamically significant LCIV stenosis out of 285 females with PVI screened in 2014–2022. All 55 patients underwent duplex ultrasound, multi-detector computed venography, ovarian venography, and multiplanar pelvic venography. Patients underwent LCIV stenting or the left gonadal vein (LGV) embolization as the primary intervention. The endpoints (chronic pelvic pain [CPP] relief, patency of stents, and reduction in pelvic venous reflux [PVR]) were evaluated 1 and 10 days, as well as 1, 6, and 12 months after the procedure. All patients received antithrombotic therapy after the interventions.
Results:
The primary LCIV stenting was performed in 49 patients and resulted in the CPP relief in 69.4%, pain reduction from 7.9±1.3 to 1.7±1.1 visual analog scale (VAS) scores (p=0.005), and substantial reduction of PVR in LGV (from 4.3±0.6 seconds to 1.9±0.3 seconds, p=0.003). The LGV embolization as the second stage of treatment was performed in 30.6% of patients with the LGV reflux greater than 5 seconds as a possible cause for the CPP persistence. The primary LGV embolization failed in 100% of patients (no changes in CPP and PVR). The LCIV stenting at the second stage resulted in the CPP relief within 10 days and the pelvic venous reflux (PVR) reduction. There were no complications of stenting, and the patency of stents in the follow-up period was 100%. Postembolization syndrome occurred in 9.5% of patients. No thromboses of the veins of the pelvis and lower extremities were identified.
Conclusion:
Treatment of patients with a combination of LCIV compression and PVI involves staged endovascular interventions: the LCIV stenting should be considered the first-line treatment, while the LGV embolization is performed when the PVI symptoms persist for more than 6 months and is not acceptable as the first-line treatment.
Clinical Impact
The developed strategy of endovascular treatment for the combination of left common iliac vein (LCIV) and pelvic venous insufficiency (PVI) provides an effective elimination of chronic pelvic pain (CPP) and reflux in the pelvic veins and avoids unnecessary embolizations of the gonadal veins, thereby eliminating possible risks related to complications of embolization. The use of antithrombotic therapy is an effective and safe approach for preventing venous thromboembolic events after endovascular interventions.
Keywords
Introduction
Pelvic venous disorders (PeVDs) are a group of several conditions characterized by abnormalities of the pelvic veins (gonadal, parametrial, uterine veins, and tributaries of the internal iliac veins) and their main outflow routes (left renal and iliac veins, pelvic communicating veins).1,2 This term encompasses the nutcracker, May-Thurner and pelvic venous congestion syndromes. The pathologic compression of the left common iliac vein (LCIV) by the right common iliac artery, also known as the May-Thurner syndrome, can have at least 4 presentations: asymptomatic, with the chronic venous disease (CVD) symptoms, with formation of pelvic varicose veins with reflux in them and development of pelvic venous insufficiency (PVI), or as a combination of CVD and PVI. 3 According to various authors, the combination of LCIV compression and PVI can be present in 23% to 80% of patients with PeVD. 4 – 6 Blood flow abnormalities in LCIV can lead to the collateral venous outflow through the pelvic veins, an increase in hemodynamic load on the pelvic veins, and, eventually, the venous dilation and reflux with the occurrence of PVI symptoms. Intervention strategy for patients with a combination of LCIV compression and PVI has not been clearly defined, and the reported outcomes are contradictory. 7 Senechal et al 8 recommend first to embolize gonadal veins and then to perform LCIV stenting, while Daugherty and Gillespie 9 and Lakhanpal et al 10 give priority to the iliac vein stenting.
This study was aimed at developing a strategy of the iliac vein stenting in patients with a combination of LCIV compression and PVI and clarifying the rational sequence of endovascular interventions in this type of patients.
Materials and Methods
This prospective comparative cohort study included 55 consecutive female patients (aged 29–44 years; interquartile range 11.3 years), who underwent treatment at our clinic in 2014 to 2022. The study protocol was approved by the local ethics committee of the University. All patients signed an informed consent on recruitment to the study. The study is registered on ClinicalTrials.gov (Protocol ID: NCT05076448).
Inclusion criteria were as follows: the presence of PVI symptoms (chronic pelvic pain [CPP], dyspareunia, feeling of heaviness in hypogastrium, vulvar varicosities); the pelvic vein dilation with a diameter >5 mm and reflux >1 second 7 by transabdominal and transvaginal duplex ultrasound (DUS); the LCIV stenosis >50% by multi-detector computed venography (MDCV); and the hemodynamically significant LCIV compression by multiplanar pelvic venography (MPPV). Exclusion criteria were as follows: PVI with pelvic vein reflux by DUS and without the LCIV stenosis; nutcracker syndrome; the absence of a hemodynamically significant LCIV compression by MPPV; comorbidities of non-venous origin accompanied by CPP; the LCIV compression with CEAP (Clinical-Etiology-Anatomy-Pathophysiology) class 3 to 6 CVD without PVI; or refusal of pelvic venography.
Patients
A total of 285 women with symptoms of PVI verified by ultrasound and radiographic contrast studies were evaluated over 9 years. The LCIV stenosis was diagnosed in 97 (34%) patients, of which 55 (56.7%) had venographic signs of a hemodynamically significant compression stenosis. All patients had non-thrombotic iliac vein disease, and none of them had deep vein thrombosis secondary to the LCIV stenosis. Chronic pelvic pain was assessed using a visual analog scale (VAS). 11 Patients underwent clinical examination with DUS and were consulted by a gynecologist, urologist, and neurologist. Patients with verified PVI underwent MDCV with the assessment of the iliac veins, and those with the diagnosed LCIV stenosis were evaluated using MPPV for determination of hemodynamic significance of LCIV stenosis and deciding on the need for the LCIV stenting.
The primary intervention was LCIV stenting in 49 and left gonadal vein (LGV) coil embolization in 6 patients. The choice of intervention was random and did not depend on the degree of stenosis, the LGV diameter, and severity of reflux in it. Then, patients were assessed for the clinical effect of interventions and the need for additional LGV embolization or LCIV stenting. The study design is presented in Figure 1. Intravascular ultrasound (IVUS) was not performed in this study as the required equipment was not available.
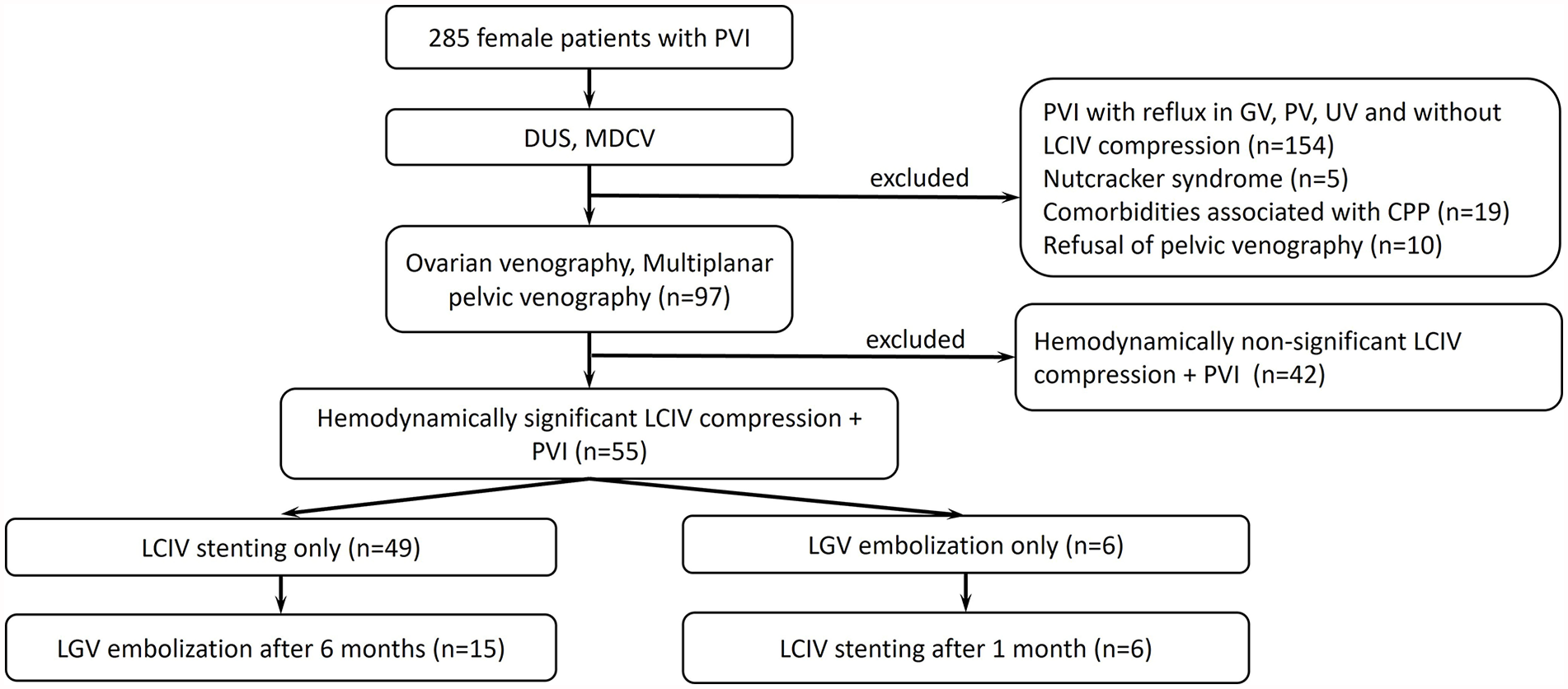
Study design. PVI, pelvic venous insufficiency; DUS, duplex ultrasound; MDCV, multidetector computed venography; GV, gonadal veins; PV, parametrial veins; UV, uterine veins; LCIV, left common iliac vein; CPP, chronic pelvic pain; LGV, left gonadal vein.
Duplex Ultrasound
Duplex ultrasound (DUS) of the pelvic and lower limb veins was carried out using the Philips HD11, Philips EPIQ 5 (Philips, Amsterdam, The Netherlands) and Esaote MyLab Class C (Esaote, Genoa, Italy) systems equipped with linear (3–18 MHz) and convex (3–5 MHz) probes, and endovaginal microconvex probes (3–9 and 3.5–10 MHz). All patients underwent transabdominal and transvaginal DUS, as well as ultrasound study of the veins of lower extremities, according to the protocol published elsewhere. 12 These studies were aimed at verification of pelvic varicosities with reflux duration >1 second and at evaluation of the left renal and iliac veins, perineal veins, and veins of the lower extremities.
The pelvic venous reflux (PVR) duration was graded as follows: 1 to 2 seconds = type I (mild), 2.1 to 5 seconds = type II (moderate), and >5 seconds or spontaneous reflux in the absence of a loading test = type III (severe). 12 Assessment of the iliac veins included measurements of the blood flow velocity in LCIV before its intersection with the right common iliac artery (Vpre-stenosis) and cranial to this intersection (Vpost-stenosis). The ratio Vpost-stenosis/Vpre-stenosis greater than 2.5 was considered an ultrasound sign of the hemodynamically significant compression stenosis of LCIV. 13
Multi-Detector Computed Venography
The study was performed using the Canon Aquilion Prime SP 160 (Toshiba, Japan) tomographs in all patients in order to clarify anatomy of the gonadal veins, location of the renal-ovarian and renal-caval junctions, as well as to diagnose LCIV compression. The study was performed according to the technique described elsewhere.14,15 The LCIV compression >50% was considered a significant stenosis requiring a more accurate assessment using MPPV.
Venography
The study was performed using the Siemens Axiom Artis (Siemens AG, Germany) system in patients with the LCIV stenosis >50% by MDCV. The inferior vena cava (IVC), left and right renal veins (LRV and RRV), gonadal veins (GVs), and common, external, and internal iliac veins (IIVs) were successively catheterized and visualized under local anesthesia with intravenous sedation through the femoral (n=19) or brachial (basilic or cephalic veins) (n=36) access.5,16 The patency and diameter of these vessels were determined, the presence and duration of reflux in the GVs, IIV and their tributaries were recorded, and the presence and severity of LCIV stenosis were evaluated. The status of the iliac veins was assessed in antero-posterior, lateral, and oblique-lateral projections. Venographic signs of hemodynamically significant LCIV stenosis were as follows: the LCIV prestenotic dilation; the left IIV dilation with reflux of the contrast media; collateralization of blood flow with visible dilated pelvic veins and its “overflow” to the contralateral side; visible left ascending lumbar vein and left gonadal vein (LGV); the LCIV narrowing in lateral and oblique-lateral projections of greater than 50%. A prerequisite for the recognition of hemodynamic significance of the LCIV compression stenosis was the presence of PVI clinical manifestations, which were observed in all patients included in the study.
Endovascular Interventions
The LCIV stenting was performed under local anesthesia with ultrasound guidance through the femoral approach according to the standard technique described elsewhere. 5 In all cases, pre- and post-dilation were performed. In 46 patients, the self-expanding stent systems Wallstent Uni (Boston Scientific, Marlborough, Massachusetts) with sizes of 16x90 mm (n=41), 16x60 mm (n=2), and 18x90 mm (n=3), and Abre Venous (Medtronic, Minneapolis, Minnesota) with size of 16x90 mm (n=9) were used. The LGV embolization was performed in patients with its dilation and reflux according to the standard technique described previously. 17 For the LGV occlusion, the 0.035″ coils made of Inconel with interwoven long collagen fibrils (MReye; Cook Medical Inc., Bloomington, Indiana) were used. The diameter of coils was 8 to 12 mm, and the length was 10 to 20 cm. No embolization of the IIV tributaries was performed in any patient.
Antithrombotic Therapy After Endovascular Interventions
Anticoagulant therapy was prescribed to all patients after stenting and included enoxaparin sodium or nadroparin calcium subcutaneous injections into the abdominal wall in a dose of 1 mg per 1 kg of body weight once daily for 10 days and then apixaban 5 mg/d or rivaroxaban 20 mg/d for 3 months. In addition, the patients received an antiplatelet agent clopidogrel 75 mg per day for 6 months. In patients who underwent primary or secondary (after stenting) LGV embolization, the prophylactic doses of low-molecular-weight heparin (LMWH) at the doses indicated above were administered for 10 days after the procedure to prevent thrombosis of the pelvic veins and the stented segment of the iliac vein.
Primary Outcome
Primary outcome was the change in pelvic pain intensity by the visual analog scale (VAS) at 1 and 10 days, 1, 6, and 12 months after the isolated LCIV stenting or LGV embolization. The needs and time frame for the LGV embolization after LCIV stenting or, conversely, the LCIV stenting after LGV embolization were also determined.
Secondary Outcomes
The patency of stents, the presence and severity of reflux in the pelvic veins after LCIV stenting, or LGV embolization at 1 and 10 days, 1, 6, and 12 months after the procedure were assessed.
Statistical Methods
Statistical analysis was performed using Microsoft Excel (Microsoft Corp, Redmond, USA), Statistica 10 software (StatSoft, TIBCO, Palo Alto, USA) and VassarStats online calculator (open-source online project). Descriptive statistics included the mean and standard deviation (M ± SD) for quantitative variables with normal distribution, median and interquartile range for quantitative variables with nonnormal distribution, and absolute number and frequency (in percentages) for qualitative variables. For comparisons between the groups by quantitative and categorical variables, the Mann-Whitney and chi-square tests were used, respectively. The differences were considered statistically significant when the p-value was equal to or less than 0.05.
Results
The primary intervention was LCIV stenting in 49 (89%) and LGV embolization in 6 (11%) out of 55 patients. The baseline characteristics of the 2 groups of patients are presented in Table 1.
Baseline Demographic, Clinical, and Morpho-Functional Characteristics of Patients With a Combination of the Left Common Iliac Vein (LCIV) Compression Stenosis and Pelvic Venous Insufficiency (PVI).
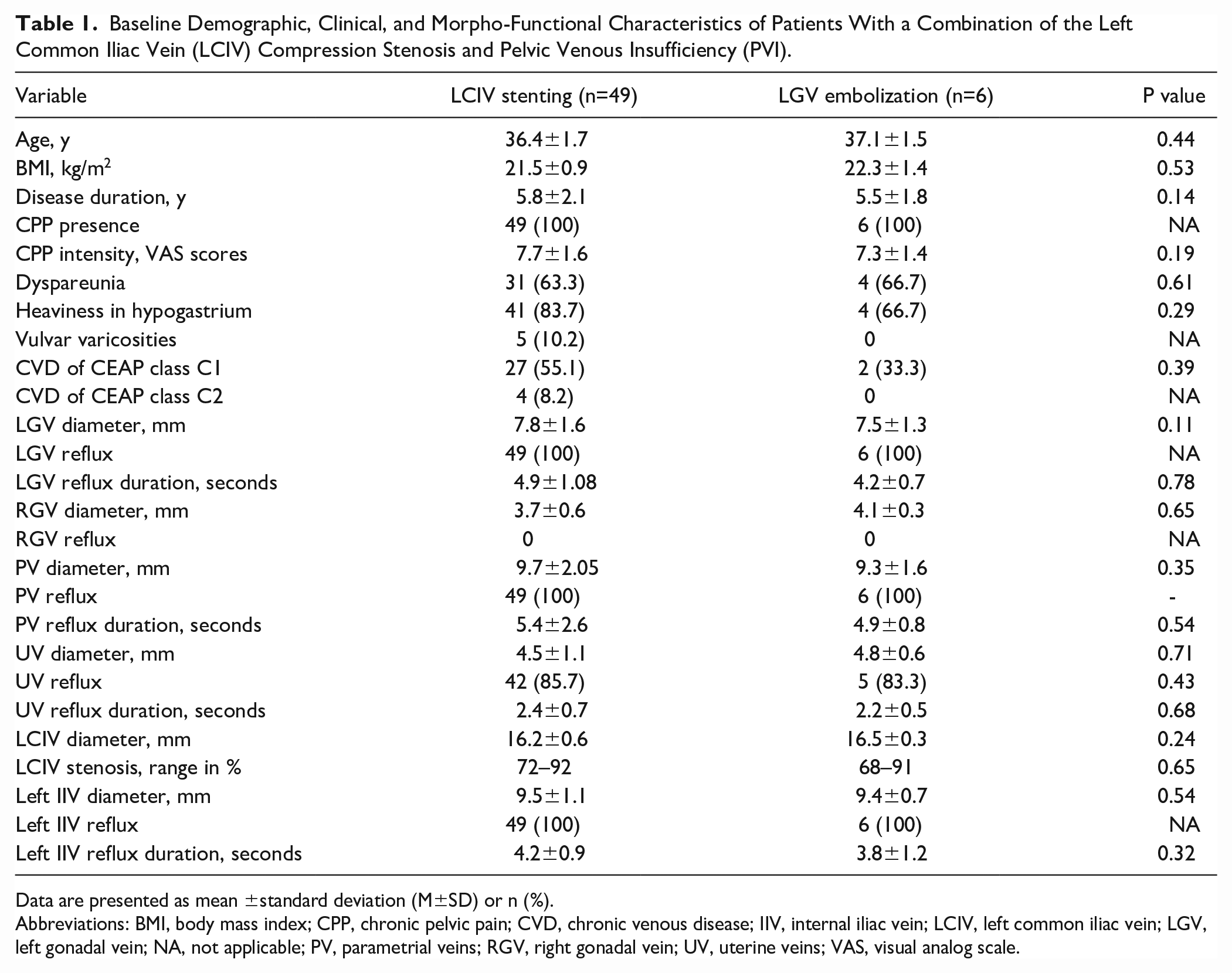
Data are presented as mean ±standard deviation (M±SD) or n (%).
Abbreviations: BMI, body mass index; CPP, chronic pelvic pain; CVD, chronic venous disease; IIV, internal iliac vein; LCIV, left common iliac vein; LGV, left gonadal vein; NA, not applicable; PV, parametrial veins; RGV, right gonadal vein; UV, uterine veins; VAS, visual analog scale.
Isolated LCIV Stenting
The LCIV narrowing was eliminated in all patients (technical success rate 100%). The stents used were Wallstent Uni 16x90 mm (n=36), 16x60 mm (n=2), or 18x90 mm (n=3), and Abre venous 16x90 mm (n=8). When using Wallstent 16x60 mm stents, 2 patients were implanted with 2 stents each, as the 60 mm length was not enough to eliminate compression while ensuring reliable stent fixation in the vessel lumen. If one stent is used, its length must be at least 90 mm. An obvious advantage of the Abre Venous stents was their precise deployment immediately at the confluence, which made it possible to avoid jailing in 100% of cases (Figure 2).
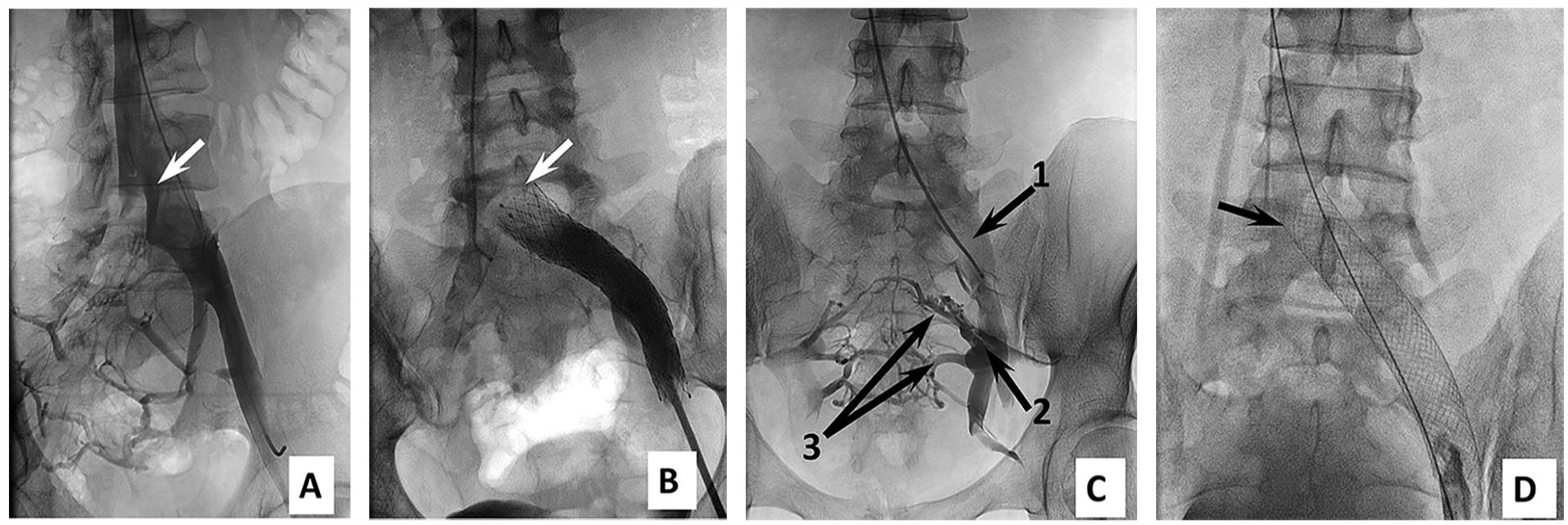
Pelvic venograms. (A) Lateral projection. The LCIV compression stenosis. (B) Frontal projection. The cranial segment of the Abre stent is located immediately in the area of confluence. (C) Frontal projection. The LCIV compression stenosis. (1) Prestenotic LCIV dilation; (2) Reflux of contrast media into LIIV and its tributaries; (3) Intrapelvic veins. (D) Frontal projection. The cranial segment of Wallstent is located in IVC and crosses RCIV (indicated by arrows). LCIV, left common iliac vein; RCIV, right common iliac vein; LIIV, left internal iliac vein; IVC, inferior vena cava.
In addition, no tapering was observed when using these stents. As for the Wallstent stents, jailing occurred in 85.4% (35 out of 41) of patients, which is explained by technical features of this stent implantation. Tapering was found in 65.9% (27 of 41) of patients, as the repeated balloon post-dilation of the cranial and caudal sections of Wallstents did not always allow its elimination.
With the primary LCIV stenting, CPP was eliminated in 34 out of 49 patients (clinical success rate 69.4%), and its severity decreased within 10 to 30 days from 7.9±1.3 to 1.7±1.1 VAS scores (p=0.005). The follow-up DUS after 10 days, 1, 6, and 12 months showed a reduction in the pelvic vein diameters and reflux duration (Table 2). In the rest 15 patients (30.6%), the CPP intensity did not change significantly (from 7.3±0.9 to 5.8±0.6 VAS scores; p=0.17) in 6 months after stenting. In these 15 patients without clinical effect, the reflux in LGV and PV of more than 5 seconds (type III) prevailed (in 14 out of 15 patients), and DUS showed no positive trend in the reduction of the pelvic vein diameters and reflux (Table 2).
Efficacy of Isolated LCIV Stenting in the CPP Relief and Reduction of Pelvic Venous Reflux 6 Months After the Intervention.
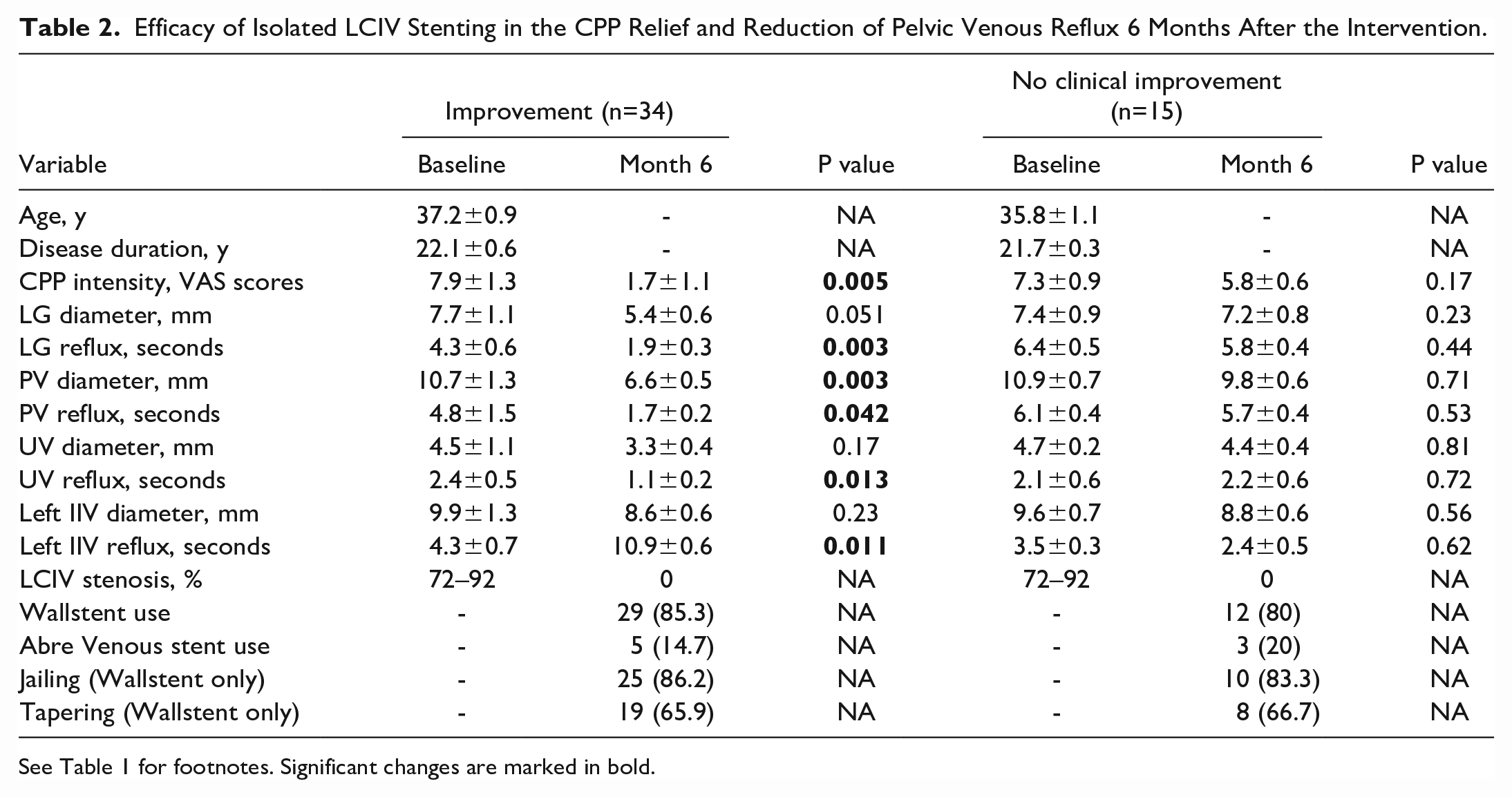
See Table 1 for footnotes. Significant changes are marked in bold.
During the follow-up ovarian venography in 15 patients without a significant clinical effect of stenting, the injection of a contrast media in the area of the ovarian-renal junction on the top of Valsalva maneuver was accompanied by its reflux into the distal parts of LGV and the left pampiniform plexus with contrasting parametrial veins (Figure 3).
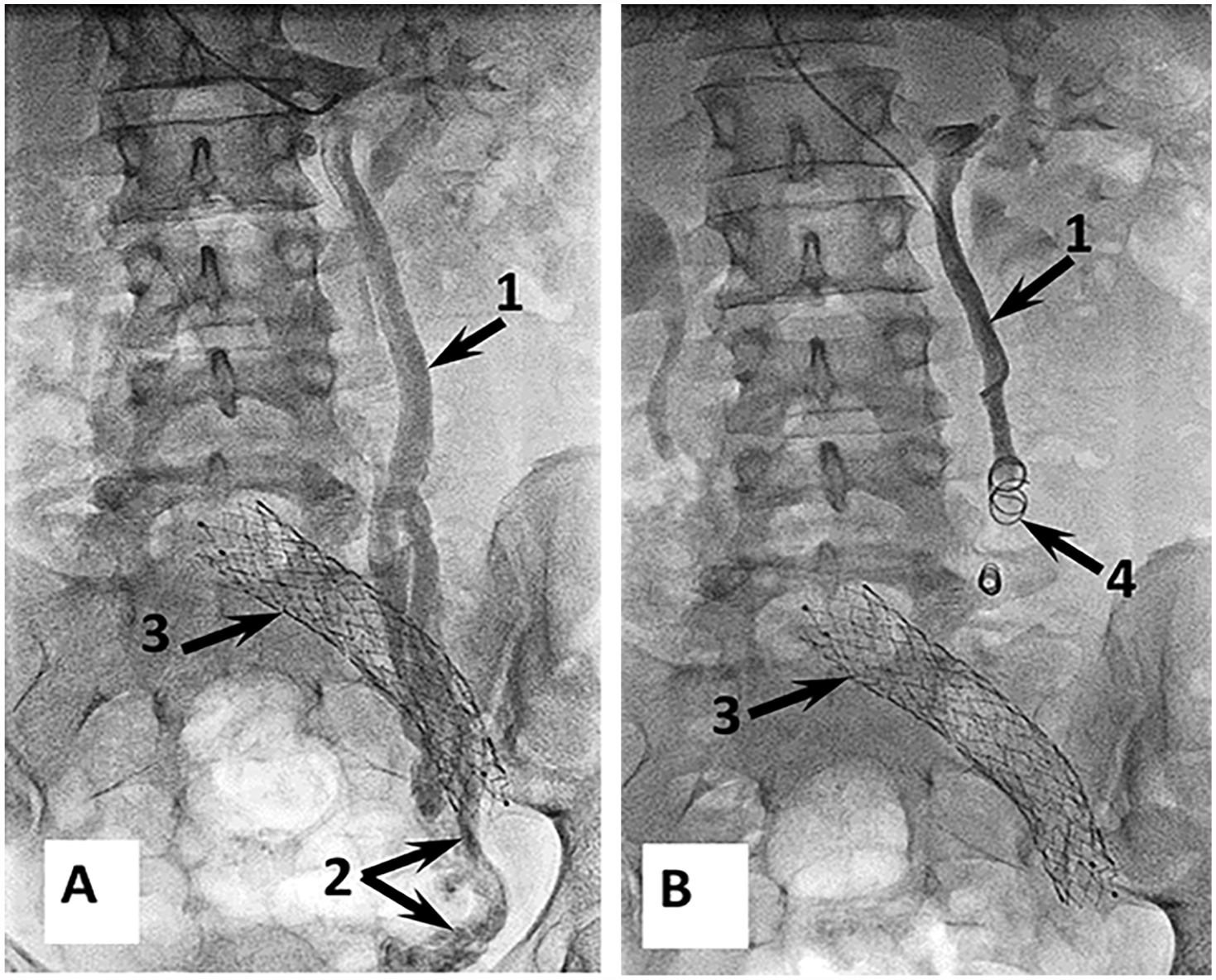
Ovarian venograms of a patient after LCIV stenting. Frontal projections. (A) Reflux in LGV. (B) The LGV is embolized, and there is no reflux below the coils. (1) LGV; (2) left pampiniform venous plexus; (3) stent in LCIV; (4) coils in LGV. LCIV, left common iliac vein; PVI, pelvic venous insufficiency; IIV, internal iliac vein; LGV, left gonadal vein.
All these 15 patients underwent LGV coil embolization 6 months after stenting. As a result, CPP was relieved within 10 to 30 days after the intervention, and its intensity was reduced from 5.8±0.6 to 1.4±0.5 VAS scores (p=0.006). The follow-up DUS revealed a decrease in the PV and UV diameters and reflux duration in these veins 6 months after embolization (Table 3).
Results of LGV Embolization 6 Months After LCIV Stenting.
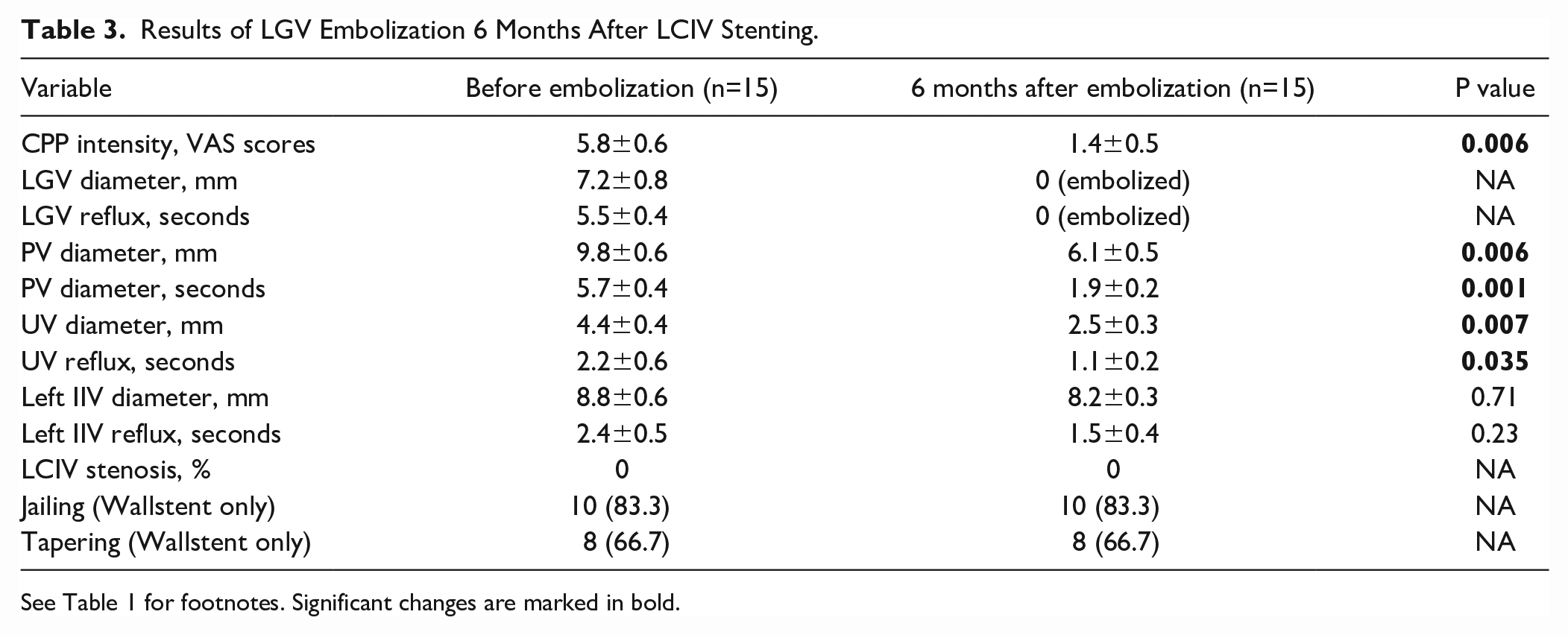
See Table 1 for footnotes. Significant changes are marked in bold.
In the follow-up periods from 1 to 9 years, no cases of stent thrombosis or migration, pelvic vein thrombosis (PVT), or thrombosis of the right iliac veins were observed. Nine (18.4%) patients had lower back pain on the first day after stenting, which was relieved with nonsteroidal anti-inflammatory drugs (NSAIDs). In 2 (13.3%) patients, post-embolization syndrome (PES) occurred after LGV embolization, which was relieved with NSAIDs and venoactive drugs (VADs) within 7 days. Jailing and tapering persisted over the entire follow-up period. Stent patency was 100% in the follow-up period.
This group of patients was also followed up for longer periods; in total, 41, 39, and 7 patients were examined after 3, 5, and 9 years, respectively. In these patients, clinical examination with additional DUS revealed no or short PVR, complete patency of the stents, and no signs of disease relapse, previous stent thrombosis, or deep vein thrombosis (DVT) of the lower limbs.
Isolated LGV Coil Embolization
This procedure was the first intervention in 6 patients with a combination of LCIV compression and PVI. These patients did not differ significantly in demographic, clinical data, and anatomical features of the pelvic and iliac veins as compared with patients who initially underwent LCIV stenting (see Table 1). The LGV embolization failed in all 6 patients (clinical success rate 0%): the CPP intensity did not change in 2 or even increased in 4 patients (in 2 of them the left-sided vulvar varicosities also occurred) within 1 month after embolization. Therefore, it was decided to abandon this procedure at the first stage of treatment in patients with a combination of LCIV compression and PVI. Duplex ultrasound revealed the blood flow reduction in LGV; however, there were no positive changes in the PV and UV diameters or reflux duration within 10 and 30 days after the procedure. No cases of PES or PVT were observed in these patients (Table 4).
Efficacy of Isolated LGV Embolization in the CPP Relief and Reduction of Pelvic Venous Reflux 1 Month After the Intervention.
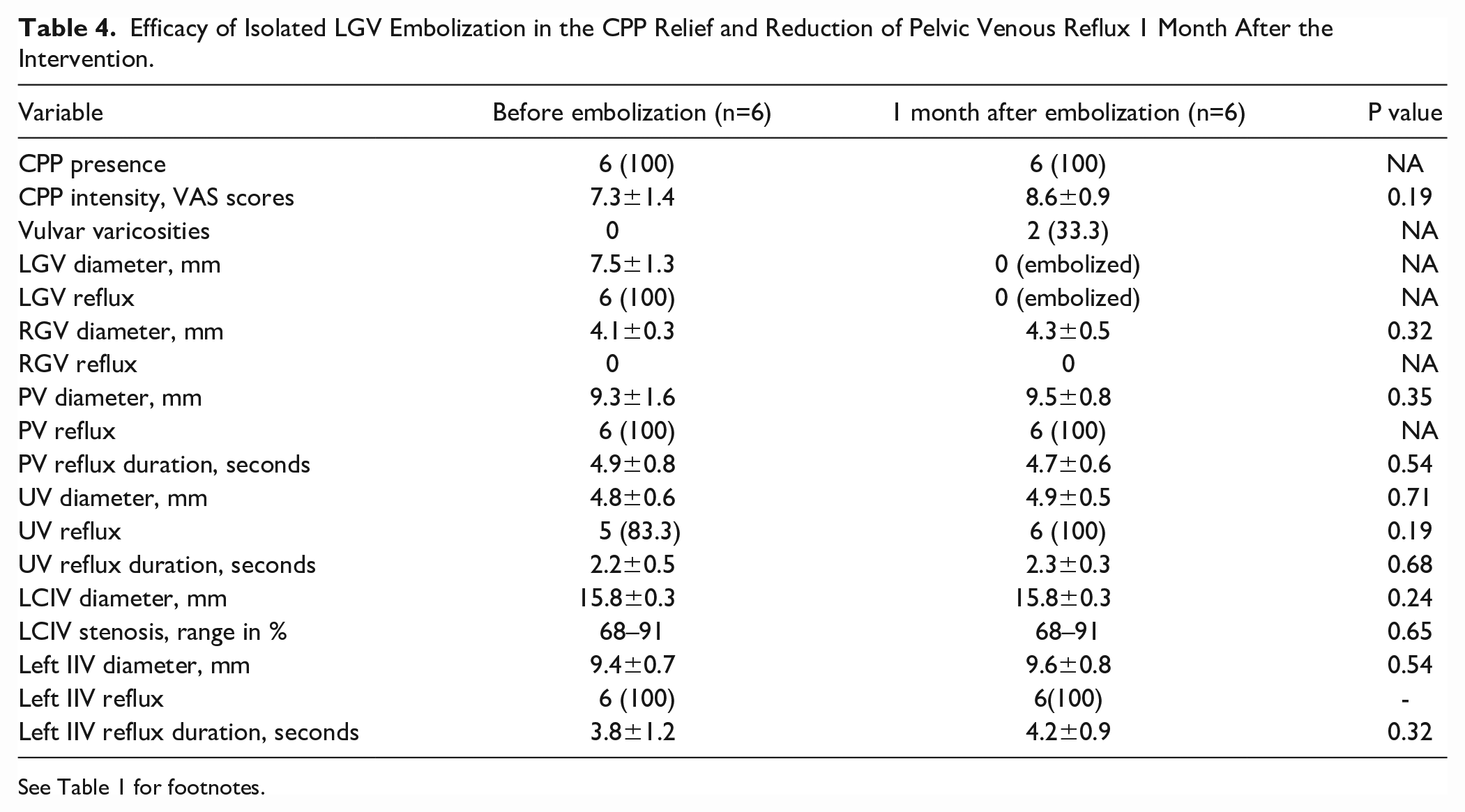
See Table 1 for footnotes.
In 1 month after embolization, these patients underwent LCIV stenting with Wallstent Uni 16x90 mm (n=5) or Abre Venous 16x90 mm (n=1) stents (Figure 4), which resulted in the CPP reduction from 8.6±0.9 to 1.1±0.5 VAS scores and even its complete elimination by day 30 after the procedure.
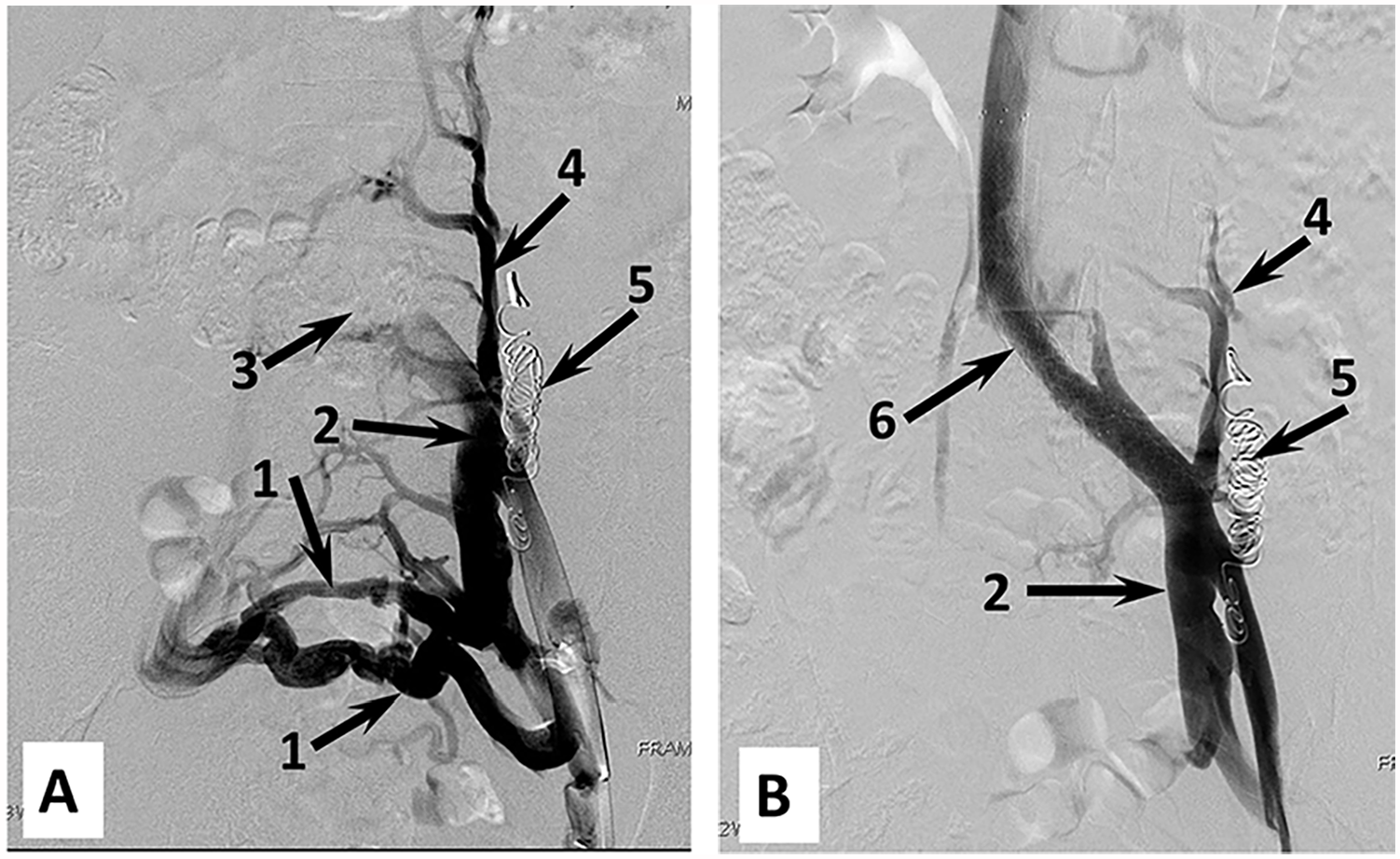
Pelvic venograms of a patient with combination of LCIV compression and PVI. (A) After LGV embolization. Frontal projection. (B) After LCIV stenting. Frontal projection. (1) Pelvic collaterals; (2) dilated left IIV; (3) LCIV stenosis; (4) dilated left ascending lumbar vein; (5) coils in the LGV; (6) stent in the LCIV. For abbreviations, see Figure 2.
The PVR grade improved from type II and III to type I (<2 seconds). No complications of stenting were observed. With the Wallstent use, jailing and tapering were identified in 80% and 60% of patients and persisted over the entire follow-up period. One patient (16.7%) had lower back pain, which was relieved by NSAIDs within 8 days. Stent patency was 100% in the follow-up period.
From this group of patients, 4 women were examined after 3 years, 3 after 5 years, and 1 after 9 years. Examination additionally included DUS and revealed no symptoms or signs of the disease relapse, no PVR, as well as complete patency of stents without previous stent thrombosis. Stent patency in the total group of patients in the various follow-up periods was 100% and is presented in Figure 5.
Kaplan-Meier curve showing stent patency of 100% during the entire follow-up period.
Discussion
The choice of treatment method for patients with a combination of LCIV compression and PVI represents a difficult task. 18 – 21 Previous studies showed that the grade of LCIV narrowing is not a major criterion determining the need for its stenting. 22 – 24 Moreover, venographic signs of a hemodynamically significant LCIV stenosis can also be found in healthy volunteers.25,26 In this regard, when determining the hemodynamic significance of stenosis, one should take into account not only the results of radiological studies but also the presence and severity of symptoms indicating a disturbance of the outflow from the pelvic veins. The clinical situation becomes more confusing when the pelvic vein dilation with reflux in them and symptoms of PVI are associated with signs of LCIV compression by MDCV, pelvic venography, and IVUS. The reasonable question arises whether CPP is primarily caused by the pelvic vein reflux or the LCIV stenosis. A number of authors argue that LCIV compression is an obvious cause for the PVI development, and elimination of blood flow disturbances in the iliac veins is the primary task in the treatment of patients with a combination of LCIV compression and PVI.4,9,10
In this single-center prospective comparative cohort study, the LCIV compression was diagnosed in 34% of patients with PVI, and 56.7% of them required endovascular treatment due to hemodynamically significant stenosis. The primary intervention was LCIV stenting in 49 patients and LGV embolization in 6 patients. We initially planned to create groups of stenting and embolization with equal number of patients, but as the study progressed, it became obvious that in a patient with hemodynamically significant LCIV compression the LGV embolization is absolutely ineffective. Acting in the interests of the patient and in order to prevent possible conflicts and legal claims from patients, it was decided to abandon LGV embolization at the first stage, which limited this group to 6 patients only.
The LCIV stenting was eventually performed in all 55 patients and resulted in the CPP relief in 72.7% of them (34 and 6 patients after primary and secondary stenting, respectively). Obviously, in these patients, the PVI was caused by LCIV compression, the elimination of which restored venous outflow not only in the iliac but also in the pelvic veins. Follow-up DUS showed a reduction in the pelvic vein diameters and reflux. According to the protocol, patients underwent several clinical examinations and DUS during the first year. In addition, most of the patients were followed up for 3 to 5 years (81.8% and 76.4%, respectively), and no cases of the CPP recurrence and increase in the pelvic vein diameter or reflux duration were observed. The findings suggest that in patients with a combination of LCIV compression and PVI, the LCIV stenting is the optimal first-line treatment for restoring venous outflow from the pelvis. These data are consistent with findings from the Lakhanpal et al 10 study, in which the LCIV stenting resulted in the relief of PVI symptoms in 76% of patients with a combination of LCIV compression and PVI.
In 15 patients, the primary LCIV stenting was not associated with significant clinical or hemodynamic effects. Most likely, this is due to the presence of reflux >5 seconds in LGV and PV. The LGV reflux duration was 4.3±0.6 seconds and 6.4±0.5 seconds in patients with and without a positive effect of stenting, respectively (p=0.01). No other differences were found between these groups (by age, disease duration, CPP severity, pelvic vein diameters, and degree of LCIV stenosis).
Although the clinical effect was non-significant (the CPP intensity decreased from 7.3±0.9 to 5.8±0.6 VAS scores, p=0.17), patients reported an improvement in their well-being. In this regard, we did not perform LGV embolization after 1 or 3 months but waited for 6 months expecting the stenting effect to become greater, which, unfortunately, was not a case in these 15 patients. Secondary embolization after 6 months was accompanied by complete CPP relief and reflux reduction within 1 month.
Therefore, the staged approach to endovascular interventions on LCIV and LGV made it possible not only to effectively eliminate CPP and reflux in the pelvic veins but also to significantly reduce the number of LGV embolizations, in addition to reducing the risks of complications of the procedure.
The primary LGV embolization was not effective in the CPP relief and even associated with the CPP increase in 66.7% of patients (from 7.3±1.4 at baseline to 8.6±0.9 VAS scores at 1 month; p=0.19) despite the elimination of LGV reflux. It was clear that this intervention was unacceptable as the primary and single treatment option for patients with a combination of LCIV compression and PVI.
All patients received antithrombotic therapy after stenting or embolization, which included LMWH or oral anticoagulants as monotherapy or in combination with clopidogrel. Despite the lack of a unified protocol for antithrombotic therapy after endovascular venous interventions,27,28 we followed exactly this approach, considering that any endovenous intervention is a risk factor for the development of venous thromboembolism. This treatment prevented stent thrombosis and thrombosis of pelvic and deep veins of the lower extremities in 100% of patients, and the complete patency of stents was maintained in 100% of cases. In addition, PES occurred after LGV embolization rarely (in 9.5%; 2 out of 21 embolizations) and was rapidly relieved in the first 7 days after the intervention. No cases of complications of antithrombotic therapy were observed. These findings confirm the efficacy and safety of antithrombotic therapy after endovascular interventions on the iliac and gonadal veins.
Limitations
This study had several limitations. First, this is not a randomized study, as it was not possible to form equal groups of patients for randomization. Second, the work included a small number of patients despite the long period of the study, which was due to strict inclusion/exclusion criteria for determining hemodynamic significance of LCIV stenosis. In this study, we did not use IVUS, which is recognized as the standard for assessing the degree of iliac vein stenosis. At the same time, the criteria for hemodynamic significance of LCIV stenosis developed in the study and the results obtained suggest about the reliability of selected venographic signs of the significance of LCIV narrowing.
Conclusions
Hemodynamically significant LCIV compression, which required stenting, was observed in 19.3% of patients with PVI. Treatment of patients with a combination of LCIV compression and PVI involves the staged use of endovascular interventions: the LCIV stenting as the first-line procedure, and if symptoms of the disease persist for 6 months after stenting, the LGV embolization should be performed. The LGV embolization as the primary treatment method in patients with a combination of LCIV compression and PVI seems unacceptable. Further multicenter randomized clinical trials are warranted to confirm the findings.
Footnotes
Author Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.