
Abstract
Purpose:
Description of physician-modified endograft technique and its advantages using the TREO stent graft system.
Technique:
After partial back-table deployment of the TREO endograft, fenestrations are created using a scalpel and reinforced with a double snare loop and running suture. The distance between the Z-shaped stents of the TREO main body of almost 20 mm allows for more flexible placement of multiple fenestrations and easier and faster re-sheathing. The technique is illustrated with physician modification of a TREO aortic cuff and bifurcated endograft in three patients with juxtarenal aortic aneurysms or type Ia endoleak after previous endovascular aortic aneurysm repair.
Conclusion:
Physician modification of the TREO stent graft system can be safely performed, making it an excellent additional option to treat juxtarenal aneurysms.
Clinical Impact
The TREO stent graft system offers various sizing options including different main body lengths and diameters, thus increasing applicability. Larger distance between the main body’s stents facilitates placement of multiple physician-modified fenestrations. Re-sheathing is easier and faster due to the low number of main body stents which have to be re-sheathed. Therefore, the TREO stent graft system is an excellent platform for the physician-modified technique.
Introduction
Fenestrated endovascular aortic repair (FEVAR) is a well-established, safe, and durable treatment option for juxtarenal abdominal aortic aneurysms (AAAs). 1 Custom-made devices (CMDs) as well as physician-modified endografts (PMEGs) have shown excellent results in experienced centers.1,2 PMEG has some advantages over CMDs including instant availability, lower cost, and greater customization to the patient’s unique anatomy, while it requires advanced knowledge of FEVAR and great familiarity of the PMEG technique itself. 3 For the treatment of juxtarenal AAA, bifurcated endografts are mostly modified, while different stent graft systems have been utilized for physician-modification. For juxtarenal AAA, the fenestrations are created on the proximal part of the main body for inclusion of reno-visceral vessels. Greater distances between the stent rings in the proximal part increases the possibilities of placing the fenestrations without the risk of a stent ring crossing the fenestration. 4
The TREO stent graft system (Terumo Aortic, Sunrise, FL) is a newer-generation, trimodular, bifurcated device, consisting of nitinol Z-shaped stents and polyester fabric, which has shown excellent midterm results in infrarenal AAA. 5 Unique features include dual active proximal fixation and barbs at the main body’s limb overlap zone to prevent limb dislodgement. More sizing options increase applicability including 8 different proximal diameters ranging from 20 to 36 mm and 3 different main body and cuff lengths of 50, 70, and 90 mm and 40, 55, and 70 mm, respectively. Furthermore, the stent graft system is characterized by a great distance between the main body’s Z-shaped stent rings and the 50-, 70-, and 90-mm-long main body reinforced with only 3, 4, and 5 stent rings, respectively. Finally, the delivery system is low profile with 18F outer diameter for the 20- to 28-mm main body and 19F for the 30- to 36-mm main body. The aim of this technical note is to describe the advantages of PMEGs using the TREO stent graft system.
Technique
The technique is demonstrated in three patients (mean age 74 years, one woman) undergoing endovascular aortic repair for juxtarenal aortic aneurysm or treatment of type Ia endoleak after EVAR, with PMEG using the TREO stent graft system (Figures 1-3). All procedures were performed in a hybrid operating room with a fixed imaging system (Philips Healthcare, Best, the Netherlands). Patients were under general anesthesia and systemic heparinization (activated clotting time ≥250 seconds).
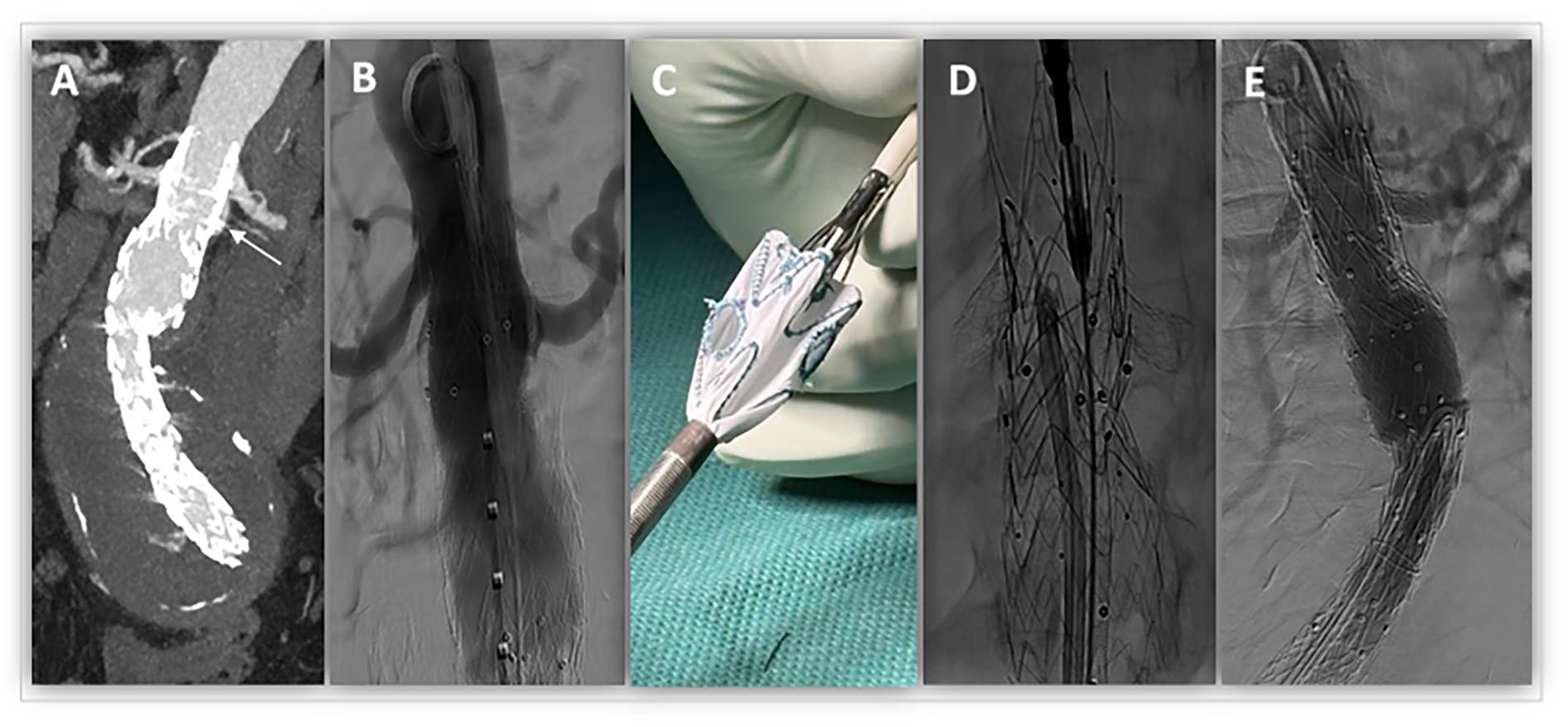
(A, B) A 71-year-old female with a type Ia endoleak after previous endovascular aortic repair due to a symptomatic aneurysm underwent proximal extension with a two-fold physician-modified fenestrated TREO cuff with a length of 55 mm. Proximal landing zone length from the lowest renal artery up to the superior mesenteric artery was 25 mm. (C, D) Fenestrations were created for the right renal artery 10 mm from the top of the graft with a diameter of 7 mm, and for the left renal artery, 20 mm from the top with a diameter of 6 mm. Both fenestrations were created between the first and the second stent rings and were bridged from a femoral access with balloon-expandable covered stents (Advanta V12; Atrium Medical Corporation, Merrimack, NH) using a 7F steerable sheath (Oscor, Palm Harbor, FL). (E) Final angiography showed complete exclusion of the aneurysm without any endoleak and patent bridging stents.
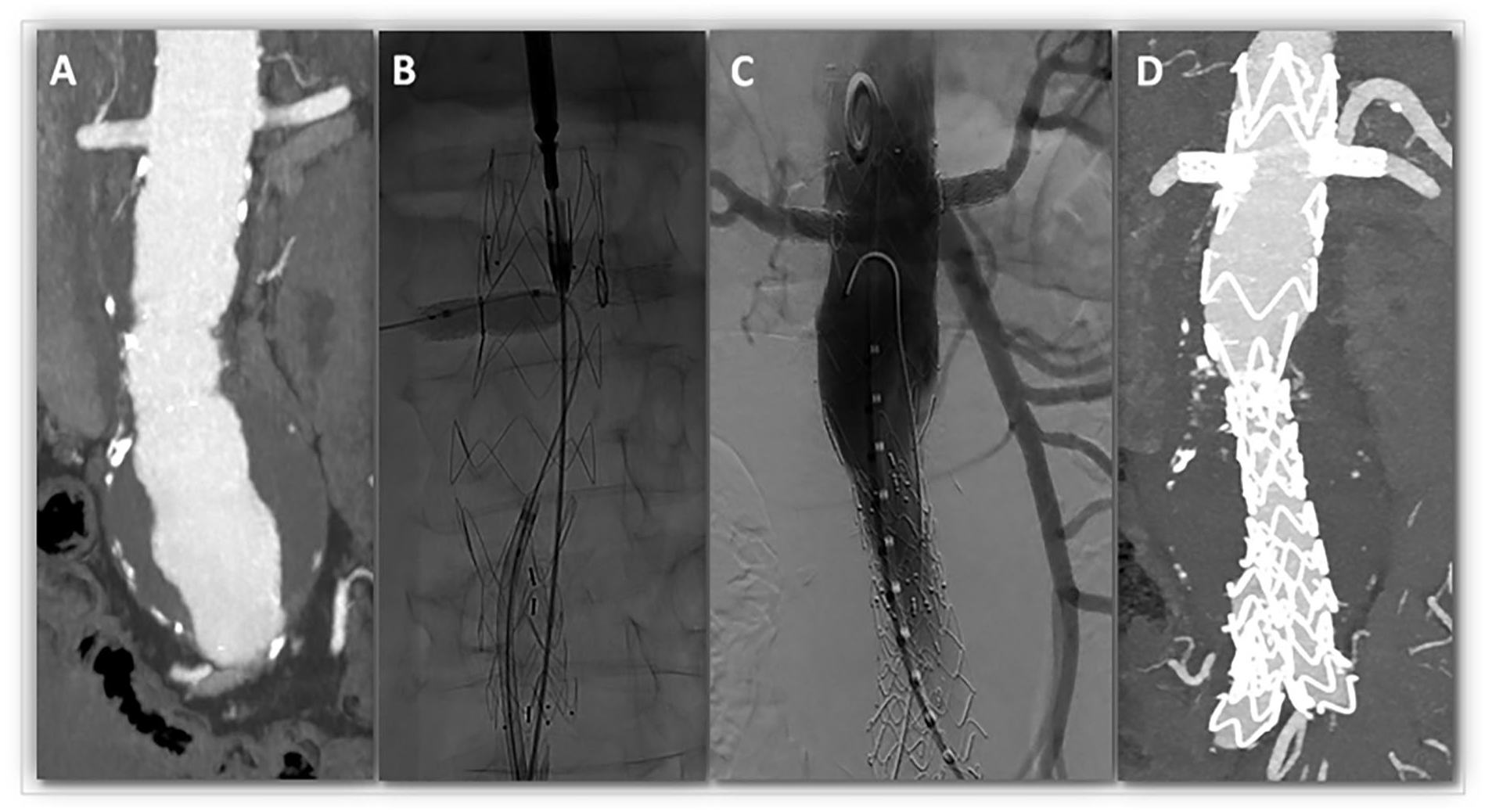
(A) A 68-year-old male with a juxtarenal aortic aneurysm of 60 mm diameter was treated with a two-fold physician-modified fenestrated TREO bifurcated endograft with a 70-mm main body length including four stent rings. Proximal landing zone length below the superior mesenteric artery was 25 mm. (B) Fenestrations for the left renal artery was created 10 mm below the top of the endograft with a diameter of 6 mm, and for the right renal artery, 13 mm from the top of the graft with a diameter of 7 mm. Both fenestrations for the renal arteries were created between the first and the second stent rings and bridged with balloon-expandable covered stents (Advanta V12, Atrium Medical Corporation, Merrimack, NH). (C, D) Final angiography and follow-up computer tomography angiography showed open bridging stents without any endoleak.
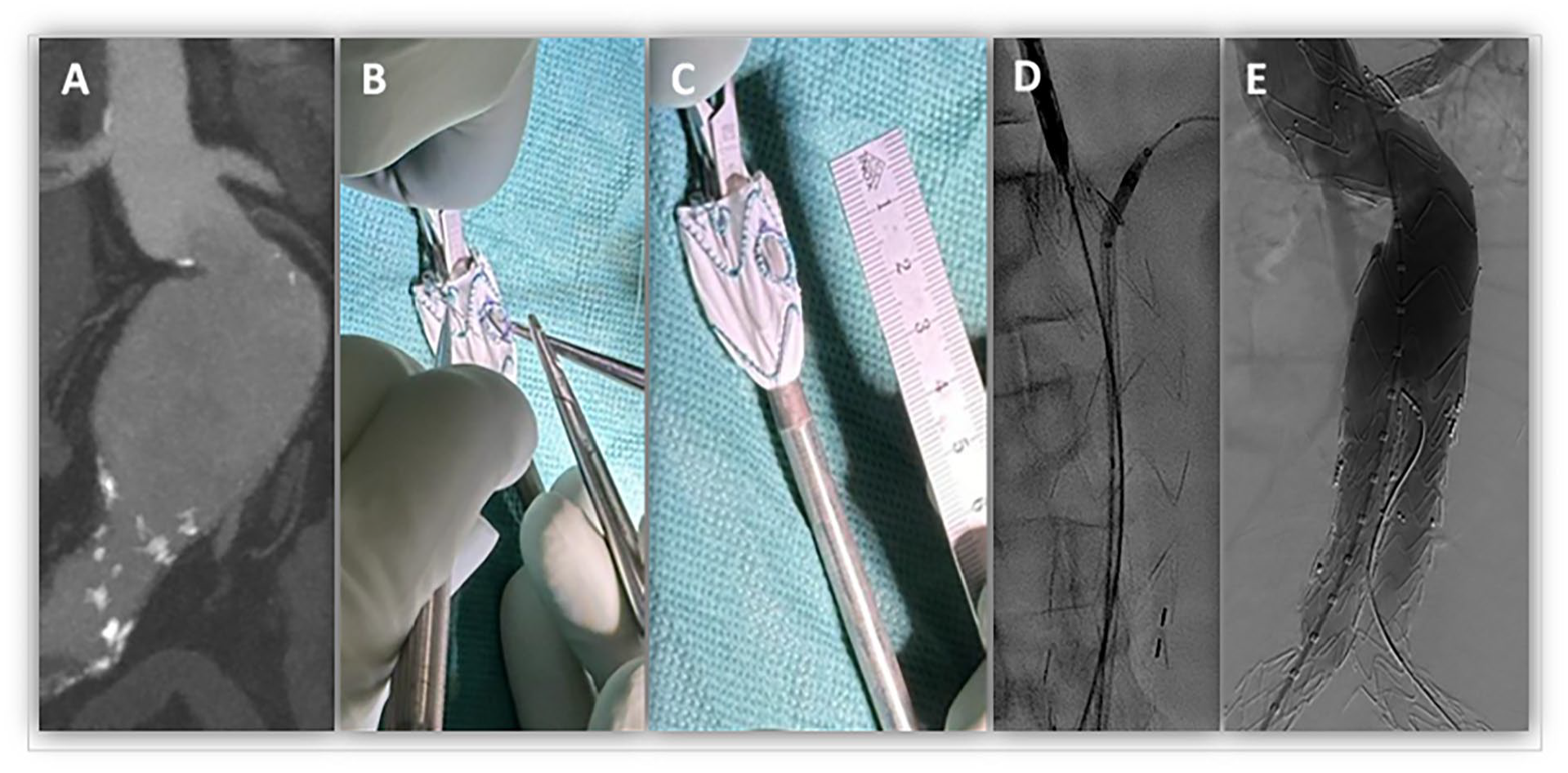
(A, B, C) An 82-year-old male patient with an infrarenal aortic aneurysm with a neck length of 15 mm and an infrarenal angle of 70° underwent single fenestrated physician-modified endograft for the left renal artery to increase the proximal sealing zone by 18 mm using a TREO bifurcated graft with a body length of 90 mm. The fenestration was created 7 mm from the top of the endograft with a diameter of 7 mm. (D) The tip capture was left closed until successful placement of the balloon-expandable covered stent within the fenestration (Advanta V12, Atrium Medical Corporation, Merrimack, NH). (E) Final angiography showed a patent bridging stent for the left renal artery without type I or III endoleak.
The physician-modification technique has been previously described in detail.3,6 Meticulous preoperative planning involves centerline-adjusted computer tomography angiography measurements including distances between reno-visceral vessels and sizes and clock angles of target vessel origin. After partial deployment of the first stent graft rings on a back table, proximal markers are used to orientate on the endograft, and a curved clamp is utilized to unfold the fabric for placement of the fenestrations (Figure 3C). This includes a snare double loop reinforcement which has shown increased strength and durability. 7 For implantation, bilateral percutaneous common femoral artery access is obtained. After partial endograft deployment with the tip capture left closed, the contralateral gate is cannulated, and target vessels are catheterized sequentially with a 7F steerable sheath and bridged with balloon-expandable covered stents which are flared to 8 to 12 mm into the main body. The tip capture is released after catheterization of the last target vessel and prior bridging stent deployment to allow fenestration alignment with the target vessel. The intervention is finalized with standard extension of the main body with bilateral endograft limbs.
Discussion
PMEG has become a well-established, safe, and durable treatment option with excellent midterm results in experienced centers. 8 However, the technique heavily depends on the physicians’ expertise regarding indication, preoperative planning, sizing, modification, and device implantation. In addition, PMEG still lacks standardization with different approaches and endograft platforms used.
The new-generation TREO stent graft system provides several innovations including different main body lengths with increased distances between the stent rings. Different main body lengths allow for variable positioning of the endograft bifurcation, which may decrease limb graft compression and kinking as highlighted in case 3. The special main body feature with three to five stent rings results in almost 20 mm distance of unsupported fabric, which facilitates placement of multiple fenestrations for reno-visceral target vessels, without compromising their position toward stents. Furthermore, fewer stent rings make re-sheathing easier and faster. In comparison, the Medtronic Endurant II main body is supported with five stent rings on a length of 50 mm, resulting in somewhat shorter space between stent rings, which can interfere with placement of fenestrations. Furthermore, with longer main bodies up to 90 mm in a bifurcated TREO main body, even treatment of more extensive aneurysms like suprarenal or type IV thoracoabdominal aortic aneurysms with a single bifurcated endograft could be feasible. This is also supported by the TREO’s delivery system shaft length of 49 cm, which allows access to the descending aorta with abdominal endografts. This could reduce overlapping zones, complexity of the intervention, and additional costs. Finally, an 18F or 19F delivery system outer diameter might increase its applicability in patients with difficult access anatomies.
We modified both bifurcation and cuff endografts, depending on the pathology extension. The above-mentioned advantages apply for all aortic cuffs and bifurcated endografts. The main difference is that cuffs have to be deployed completely for physician modification in case of distal-lying fenestrations, which makes the re-sheathing more demanding and time-consuming. Bifurcated endograft require only partial deployment of the main body. Both types contain proximal fixation with hooks, which are kept together until tip capture release. The tip capture can be used to support the curve of a steerable sheath during delivery of the bridging stents, especially in case of a steep downward angle. If necessary, additional upper extremity access can be used, and the fenestration can be catheterized through the closed tip capture.
Advances of the TREO endograft do not seem to affect technical success rates or safety, as the CMD fenestrated TREO has demonstrated comparable results with other stent graft types. 9 After the introduction of the fenestrated TREO system in our department in elective patients with excellent outcomes, we initiated the physician-modification technique of the off-the-shelf TREO devices with high technical success and excellent early results.
Footnotes
Author Contributions
Dimitrios David Papazoglou: Conceptualization; Investigation; Visualization; Writing–original draft. Georgios Ioannis Karaolanis: Investigation; Visualization; Writing–original draft and review & editing. Drosos Kotelis: Methodology; Writing–review & editing. Vladimir Makaloski: Conceptualization; Methodology; Writing–review & editing; Supervision.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Vladimir Makaloski is consultant and proctor for Terumo.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Due to the retrospective nature and low patient number, no ethical approval was necessary for this publication.
Informed Consent
All patients provided written informed consent for the use and publication of their health-related data.