
Abstract
Objectives:
To evaluate outcomes of patients with complex aortic aneurysms (cAAs) undergoing fenestrated/branched endovascular aortic aneurysm repair (f/b-EVAR) using a combination of endoprostheses from different manufacturers.
Methods:
The study is a 2-center retrospective analysis of prospectively maintained databases of patients with cAAs undergoing f/b-EVAR using a combination of endoprostheses from different manufacturers from 2013 to 2023. Primary endpoints included technical success, major adverse events and reintervention rates. Technical success was defined as implantation of the device without type I or type III endoleak or conversion to open repair. Secondary endpoints included mortality and mid-term device performance.
Results:
During this time, 353 patients with cAAs underwent f/b-EVARs at both centers. Of these, 80 (22.7%) required use of a combination of devices from 4 different manufacturers for repair. Fifty-one (64%) were treated for thoracoabdominal aortic aneurysms and 29 (36%) for pararenal aneurysms. Majority (74%) were male with a median age of 75 (69, 81) years and aneurysm size of 65 (59, 72) mm. Thirty-five (44%) patients required a proximal thoracic stent graft—W.L. Gore (17), Cook, Medtronic, and Terumo (6), respectively. Seventy-seven (96%) patients required a bifurcated device, including Cook Flex (34), Gore (40), and Medtronic (3). Twelve patients underwent common iliac artery aneurysm repair with a Gore iliac branched endoprosthesis. One hundred fifty-four limbs were implanted: Gore: 68, Cook: 82 and Medtronic: 4. Three hundred fourteen target vessels were incorporated. Median operating room time, estimated blood loss, fluoroscopy time and dose were 209 (186, 278) minutes, 100 (50, 663) mL, 77 (59, 100) minutes, 2385 (1415, 3885) mGy, respectively. Three endoleaks were observed on completion angiography—2 type Ic and 1 type IIIa—all of which resolved at 1 month. Fifteen MAEs were observed in 11 patients at 30 days, including 3 (3.9%) deaths, 7 renal insufficiency, 1 renal failure requiring dialysis, 2 MI and paraplegia, respectively. At a median follow-up of 400 (85, 1132) days, there were 8 reinterventions for endoleaks in 7 patients.
Conclusions:
The use of mixed devices proximal and distal to f/b-devices built to treat patients with cAAs is safe and has good mid-term results.
Clinical Impact
While not yet formally assessed in randomized clinical trials or endorsed by the Food and Drug Administration (FDA), the practice of utilizing devices from various manufacturers to address complex aortic anatomy is widespread in everyday clinical settings, yet outcomes remain insufficiently documented. To our knowledge, ours is the first manuscript demonstrating that the use of endoprostheses from different manufacturers for treating patients with complex aortic aneurysms is both safe and yields favorable mid-term results. This frequently employed strategy warrants further exploration through meticulously designed clinical trials, aiming to furnish vascular specialists with a well-founded guideline based on robust clinical evidence.
Keywords
Introduction
Since the initial endograft implantation in 1987 by Volodos and colleagues in a patient with post-traumatic aneurysm and Parodi’s successful use of tubular polyester grafts mounted on a Palmaz stent to exclude infrarenal abdominal aortic aneurysms in 5 high surgical risk patients in 1990, endografts have undergone continued refinement. The aim has been to address a diverse range of anatomic challenges encountered in clinical practice.1–4 Despite significant progress, hurdles persist. This challenge primarily stems from anatomical constraints such as aortic angulation, tortuosity, size discrepancy between the proximal and distal aorta, as well as variations in access/iliac artery dimensions.
As expertise in endovascular therapy has expanded, patients with increasingly complex anatomies are now being treated using this minimally invasive approach. This advancement owes much to the strategic combination of devices from different manufacturers, which effectively surmount anatomical constraints in some cases. Primarily observed in the infrarenal space, the utilization of a blend of endografts from different manufacturers to exclude aortic aneurysms has demonstrated efficacy.5–8 It is notable that the vascular community still lacks guidance from the Food and Drug Administration (FDA) and the Society for Vascular Surgery on this topic. Furthermore, there remains a dearth of literature examining outcomes of patients with complex aortic aneurysms (cAAs) treated using a combination of devices sourced from different manufacturers.
The aim of this 2 center study was to evaluate the performance and impact of using a mixture of devices from different manufacturers to treat patients with cAAs undergoing treatment using physician-modified fenestrated and branched endografts (f/b-endografts) built on the Cook Zenith platform.
Materials and Methods
Study Design, Aneurysm Classification, and Inclusion Criteria
The study is an Institution Review Board approved, retrospective analysis of prospectively maintained databases of patients with juxtarenal, pararenal, paravisceral, and thoracoabdominal aortic aneurysms undergoing fenestrated/branched endovascular aortic aneurysm repair (f/b-EVAR) using combination of endoprostheses from various manufacturers between the years 2013 to 2023 at 2 institutions. One of the 2 centers has a Food and Drug Administration (FDA) approved Physician Sponsored Investigational Device Exemption (Ps-IDE) for endovascular treatment of patients with complex aortic aneurysms utilizing fenestrated and branched stent grafts, and the other has an Institution Review Board approval to treat patients with complex aortic aneurysm utilizing physician-modified stent grafts.
To facilitate description, juxtarenal, pararenal, and paravisceral aortic aneurysms were grouped together and labeled as pararenal aneurysms (PRAA). Thoracoabdominal aneurysms (TAAA) were classified based on Crawford classification (Extent I-IV). Included patients underwent repair of a cAAs (PRAA and TAAA) using a combination of endoprostheses from 2 or more manufacturers and had at least one postoperative computed tomography angiography (CTA) or non-contrast computed tomography scan and visceral arteries/branches duplex (Figure 1). Data collected included subject demographics, cardiovascular risk factors, type of stent grafts used, reintervention rates, long-term device performance, and survival.
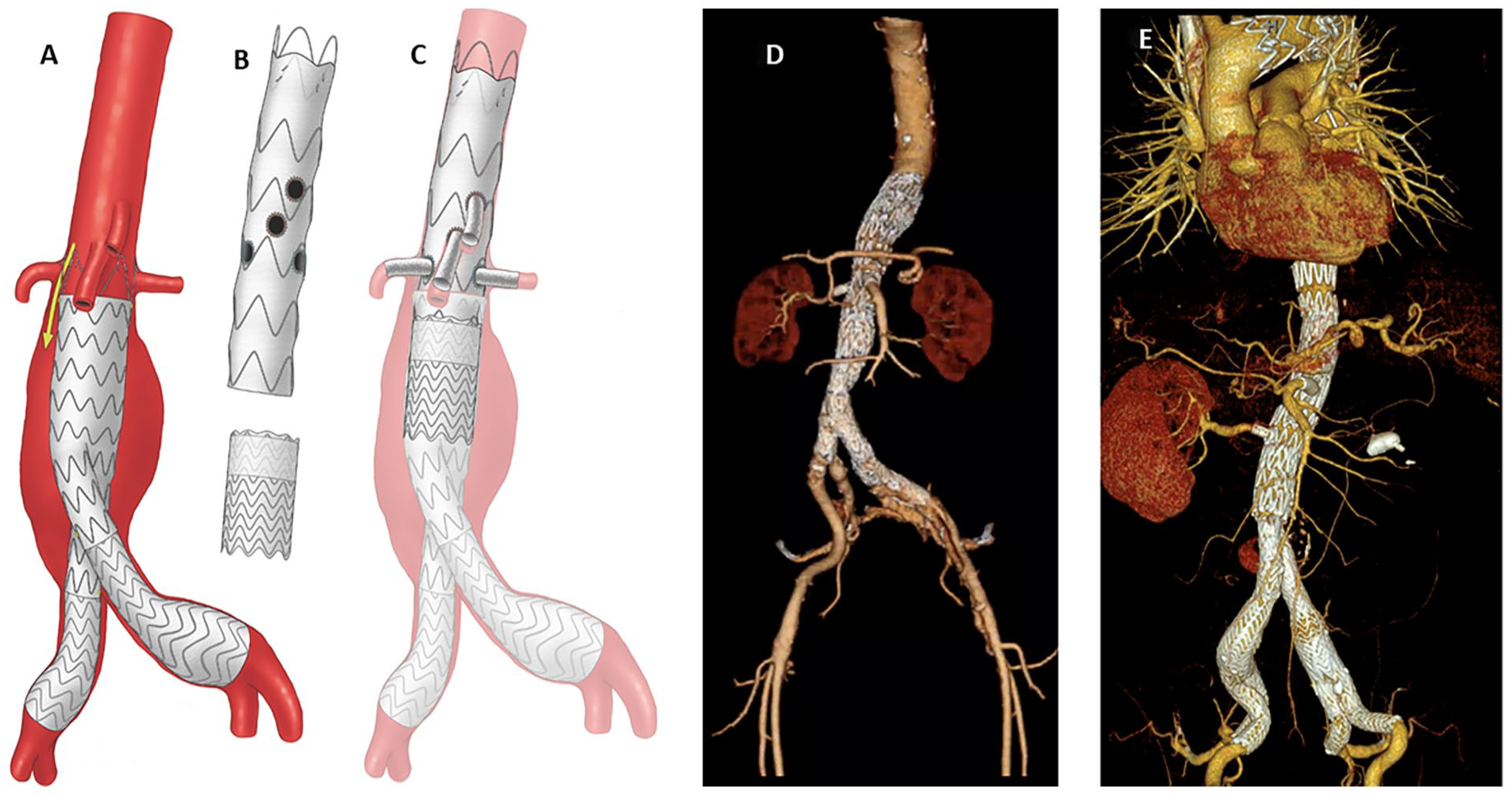
A-D. Illustration and 3-dimensional rendering of 2 patients with complex aortic aneurysms treated using a combination of devices from different manufacturers (A) illustration of a patient with failed previous endovascular repair. Note that the patient was treated with a Gore bifurcated endoprosthesis. (B) illustration of the physician-modified fenestrated device based on the Cook Zenith platform, in this case, Cook Alpha thoracic stent graft and a Gore endoprosthesis aortic cuff. (C). Illustration showing completion of repair. The fenestrated cuff, made from a Cook Alpha thoracic endoprosthesis, was implanted and landed into the existing failed Gore endoprosthesis. To ensure long-term repair integrity, a Gore cTAG cuff is used to bridge the 2 devices. 1D is the actual 3-dimensional reconstruction highlighted in the illustration (Figure 1A-C). Figure 1E is a 3-dimensional rendering in a patient with a Crawford extent II thoracoabdominal aortic aneurysm and bilateral common iliac artery aneurysms that was treated with a Cook Alpha thoracic stent graft proximally, followed by a Cook TX2 for the fenestrated component and a Gore bifurcated endoprosthesis and bilateral Gore internal iliac branched devices.
Preoperative evaluation and stent graft configuration
CTA was analyzed using TeraRecon (Aquarius, Foster City, CA) or 3Mensio (Pie Medical Imaging B.V., Maastricht, The Netherlands) to obtain measurements used for case planning, device implantations and post-implantation analysis. All fenestrated and branched endografts (f/b-endografts) used were based on the Cook Zenith Platform, including Cook Alpha, Cook TX2, and Cook Fenestrated devices (Cook Group, Incorporated, Bloomington, IN). The choice of proximal (thoracic) device, bifurcated components, and iliac limbs used were left to the treating surgeon’s discretion and were mostly driven by anatomic constraints and device availability.
Stent graft sizing, overlap, choice of distal bifurcated stent graft and bridging stent grafts
With the exception of 1 patient, we avoided the practice of individually sizing stent grafts from different manufacturers one-to-one. Instead, our approach involved oversizing by 1 or preferably 2-stent graft sizes (ie, place a 36 or 38 Cook/Medtronic device into a 34 Gore cTAG and vice-versa). Most importantly, we aimed to maximize overlap between components, exceeding the traditional 2 sealing stents, to ensure sealing integrity and prevent long-term component separation. Physician-modified fenestrated/branched devices were uniformly based on the Cook platform. For bifurcated devices, we preferred the Gore Excluder AAA Endoprosthesis due to its perceived advantages over the Cook Zenith Flex AAA endoprosthesis. Atrium iCAST was the bridging stent graft of choice for all fenestrations, with Gore Viabahn VBX stent grafts being utilized only in a handful of cases. Branches were bridged using a combination of Gore Viabahn stent graft distally with or without an iCAST or VBX stent graft proximally into the portal. Aspirin 81 mg daily for life was the antiplatelet therapy of choice, and clopidogrel was only used if the patient required it for other medical reasons.
Device implantation, spinal cord protection, collected data, endoleak definitions and study endpoints
All procedures were performed in a hybrid operating room by a team led by a single primary surgeon at both institutions. Whenever needed, f/b-endografts were modified on the day of the operation but prior to bringing the patient into the operating room or while general anesthesia was being induced and lines placed. All fenestrated devices were based on the Cook Zenith platform (Cook Medical, Inc. Bloomington, IN). Physician-modified branched devices were created by sewing a Gore Viabahn stent graft to the side of a Cook Zenith stent graft (Cook Alpha, Cook TX2, or Cook Zenith fenestrated) to create a branch or portal. With the exception of symptomatic aneurysms, patients with Crawford extent I-III TAAA underwent a staged repair starting with implantation of the thoracic endograft, followed 3 or more weeks later by the implantation of the f/b-endograft and bifurcated component. The practice of prophylactic spinal drain placement has been long abandoned in favor of routine use of motor evoked and somatosensory evoked potential. Similarly, the use of brachial approach for implantation of branched devices has been abandoned in favor of total femoral approach using steerable sheaths and “no kick back” technique. Our approach to the implantation of f/b-endografts has been previously reported.9–12 Data collected included type of device used for the thoracic, fenestrated/branched, bifurcated, and iliac components, number of vessels targeted and successfully incorporated, procedure time, radiation dose, intensive care unit (ICU) and hospital length of stay (HLOS), procedure (30-day) related complications, long-term reintervention rate and freedom from reintervention.
Endoleaks were classified based on a previous report by Karkkainen et al as follows—type Ia and Ib—defined as endoleak arising from proximal and distal graft attachment, respectively. Type Ic, IIIb, and IIIc were defined as target vessel endoleaks. Type IIIa endoleak is defined as occurring between the overlap of 2 separate aortic or aortic and iliac artery components and was of primary interest of this manuscript. Type IV and V endoleak were due to graft porosity and endotension, respectively. 13 Renal insufficiency was defined as postoperative reduction of glomerular filtration rate (GFR) >30% from the baseline value at 30 days. Spinal cord ischemia (SCI) was defined as a new postoperative lower extremity neurologic deficit and classified either as paraplegia or paraparesis. Paraplegia was defined as complete inability to move lower extremities. Paraparesis was defined as weakness of lower extremities requiring assistance to stand or ambulate. Outcomes were reported according to the Society for Vascular Surgery reporting standards for endovascular aortic repair of aneurysms involving the renal-mesenteric arteries. 14
The study endpoints included technical success, long-term component separation (type IIIa endoleak), reintervention rate, and freedom from reintervention. We define technical success as implantation of f/b-endograft with no evidence of type Ia/b/c or type III endoleak or conversion to open surgical repair. Secondary endpoints included all-cause mortality and device integrity.
Statistical analysis
The collected data were compared between the PRAA and TAAA patients. Continuous variables were expressed as median [IQR] and were compared using the Wilcoxon rank sum test. Categorical variables were expressed as frequencies (percentages) and compared using Pearson’s chi-square or Fisher’s exact test. The probability of freedom from reintervention was estimated using the Kaplan-Meier method and compared between groups using the log-rank test. All tests used a critical value of 0.05. Data were analyzed using R version 4.3.0 (R Core Development) in the RStudio 2023 (Posit Software, PBC) environment.
Results
During this time, 353 patients with cAA underwent repair f/b-EVARs at both centers. Of these, 80 (22.7%) patients required use of a combination of devices from 4 different manufacturers to complete the repair. Fifty-one (64%) were treated for TAAA, and 29 (36%) required repair for PRAA. Majority (74%) were male with a median age of 75 (IQR 69, 81) years with aneurysm size of 65 (IQR 59, 72) mm. Compared to those undergoing TAAA repair, patients undergoing repair of PRAA were older (76 years vs 73 years, p=0.026) and were more likely to have diabetes mellitus (21% vs 3.9%, p=0.024). Seventy-two patients (90%) were ASA score 3 or 4 (Table 1).
Demographics and Cardiovascular Risk Factors of Patients Undergoing Fenestrated/Branched Endovascular Repair Using a Mixture of Devices From Different Manufacturers.
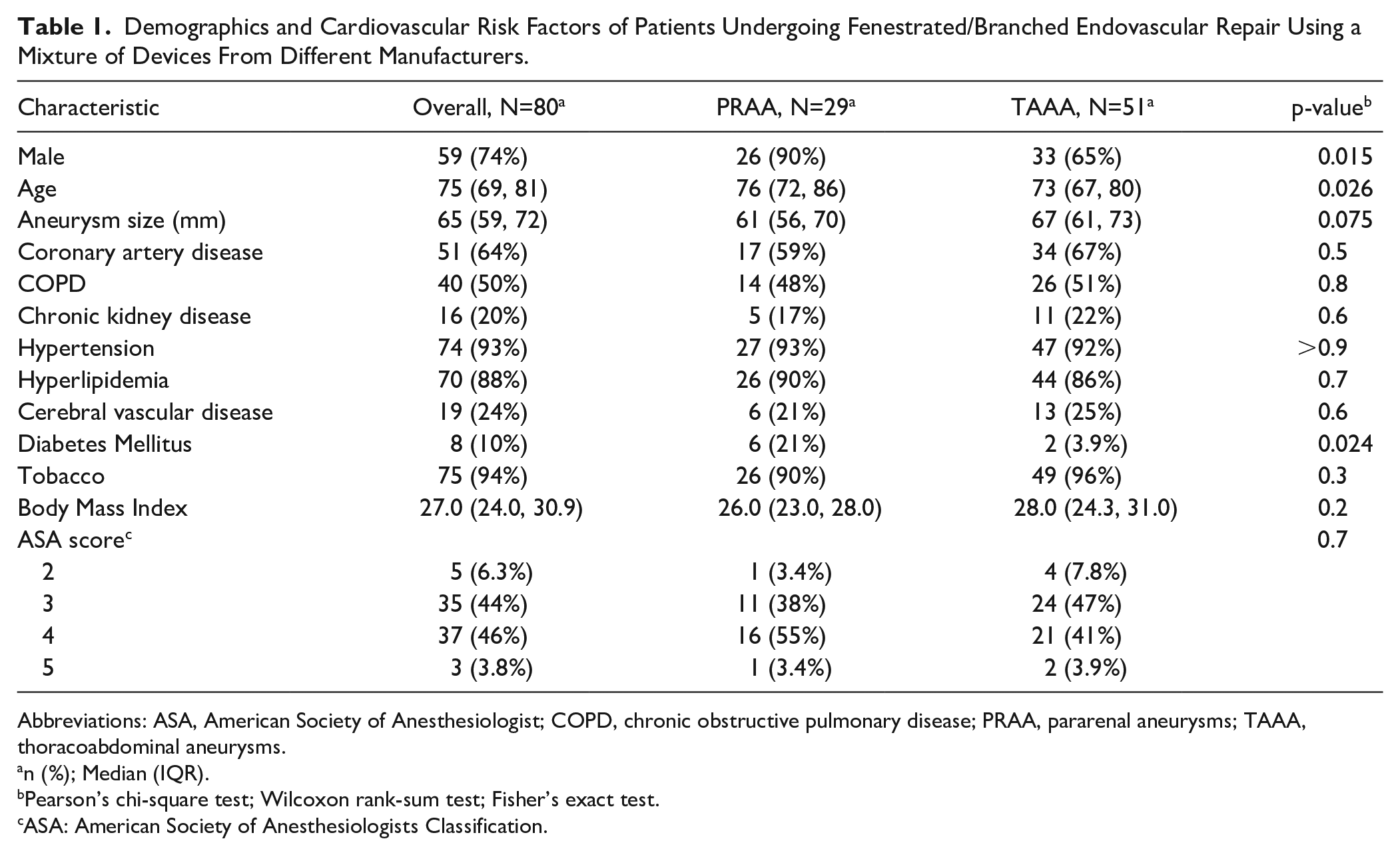
Abbreviations: ASA, American Society of Anesthesiologist; COPD, chronic obstructive pulmonary disease; PRAA, pararenal aneurysms; TAAA, thoracoabdominal aneurysms.
n (%); Median (IQR).
Pearson’s chi-square test; Wilcoxon rank-sum test; Fisher’s exact test.
ASA: American Society of Anesthesiologists Classification.
All f/b-endografts were based on the Cook Zenith platform (Cook Medical, Inc. Bloomington, IN), including Cook Alpha thoracic stent graft, Cook TX2 and Cook Zenith Fenestrated stent grafts. Thirty-five (44%) patients required proximal thoracic endografting that overlapped with the f/b-devices proximally, including 17 Gore TAG or cTAG (W.L. Gore, Inc., Newark, DE), 6 Cook Zenith TX2 or Cook Alpha thoracic, Medtronic Valiant (Medtronic, Dublin, Ireland), Terumo Bolton RelayPro (Terumo Aortic, Inchinnan, UK), respectively. Seventy-seven patients (96%) required a bifurcated device distal to the f/b-component, including Cook Flex (n=34), Gore bifurcated endoprosthesis (n=40), Medtronic (n=3), and 1 patient with a persistent type III endoleak required treatment with a Gore aortic cuff with resolution of the endoleak. Twelve patients underwent concomitant (n=10) or delayed (n=2) repair of common iliac artery aneurysm with a Gore iliac branched endoprosthesis (IBE), with 1 patient requiring bilateral IBEs. A total of 154 limbs were used, including 82 Cook ZSLE, 68 Gore limbs, and 4 Medtronic limbs (Table 2).
Intraoperative Variables of Patients Undergoing Fenestrated/Branched Endovascular Repair Using a Mixture of Devices From Different Manufacturers.
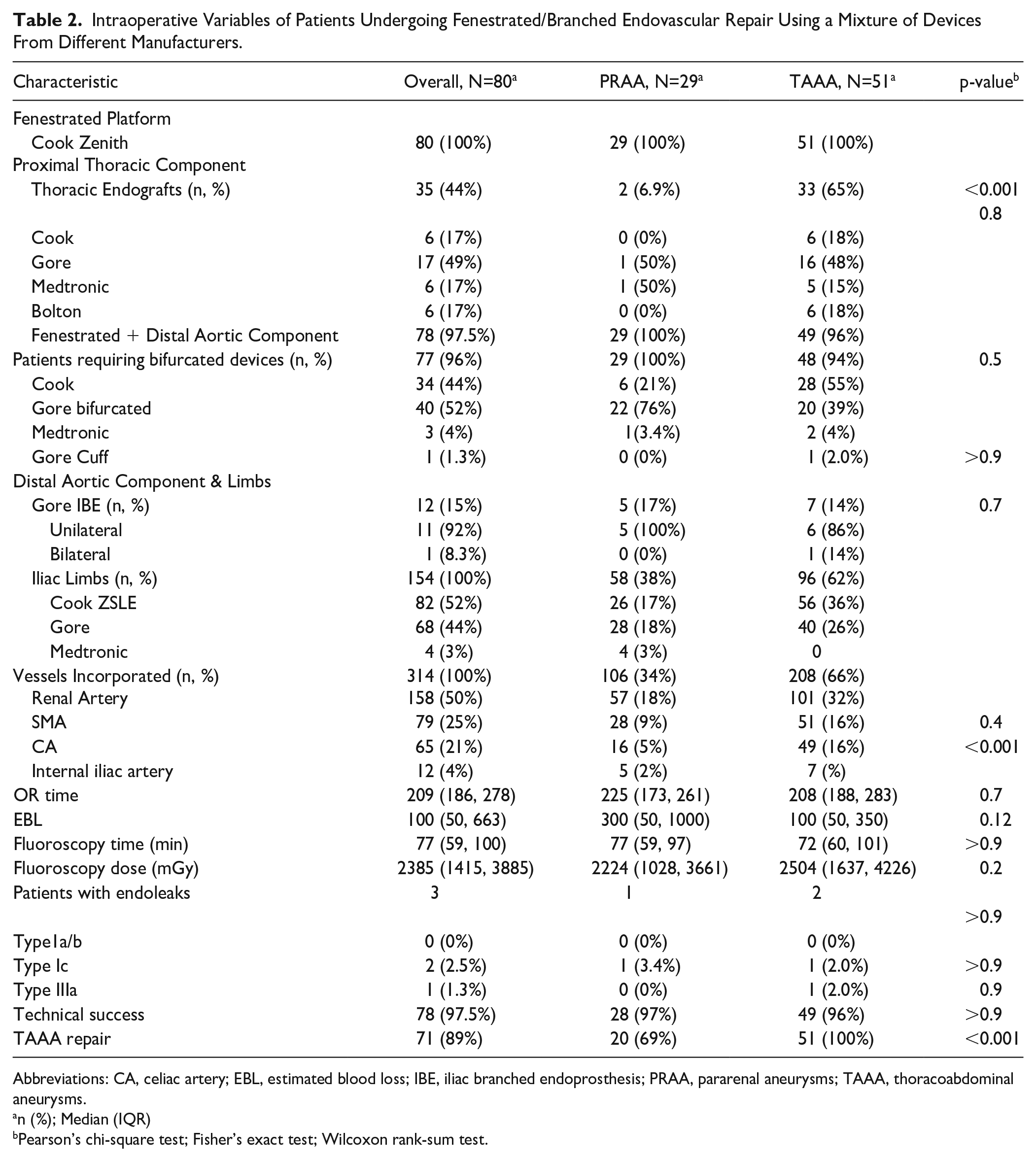
Abbreviations: CA, celiac artery; EBL, estimated blood loss; IBE, iliac branched endoprosthesis; PRAA, pararenal aneurysms; TAAA, thoracoabdominal aneurysms.
n (%); Median (IQR)
Pearson’s chi-square test; Fisher’s exact test; Wilcoxon rank-sum test.
Three hundred fourteen arteries were targeted and successfully incorporated, including 158 renal arteries, 79 superior mesenteric arteries (SMA), 65 celiac arteries (CA) and 12 internal iliac arteries. Median operating room time, estimated blood loss (EBL), fluoroscopy time and dose were 209 (186, 278) minutes, 100 (50, 663) mL, 77 (59, 100) minutes, 2385 (1415, 3885) mGy, respectively. There were in total 3 endoleaks—2 type Ic and 1 type IIIa—noted on completion angiography, all of which resolved on the first postoperative CTA, bringing the overall technical success to 97.5% (Table 2).
Fifteen MAEs occurred in 11(14%) patients including death in 3 patients, renal insufficiency in 7, renal failure requiring dialysis in 1, myocardial infarction, and paraplegia in 2 patients, respectively. No difference (p>0.9) in MAEs was noted between patients undergoing repair of PRAA and TAAA. Median ICU and HLOS were 1.0 (1, 2.75) and 2.0 (2, 4) days, respectively (Table 3).
Thirty-Day Outcomes of Patients Undergoing Fenestrated/Branched Endovascular Repair Using a Mixture of Devices From Different Manufacturers.
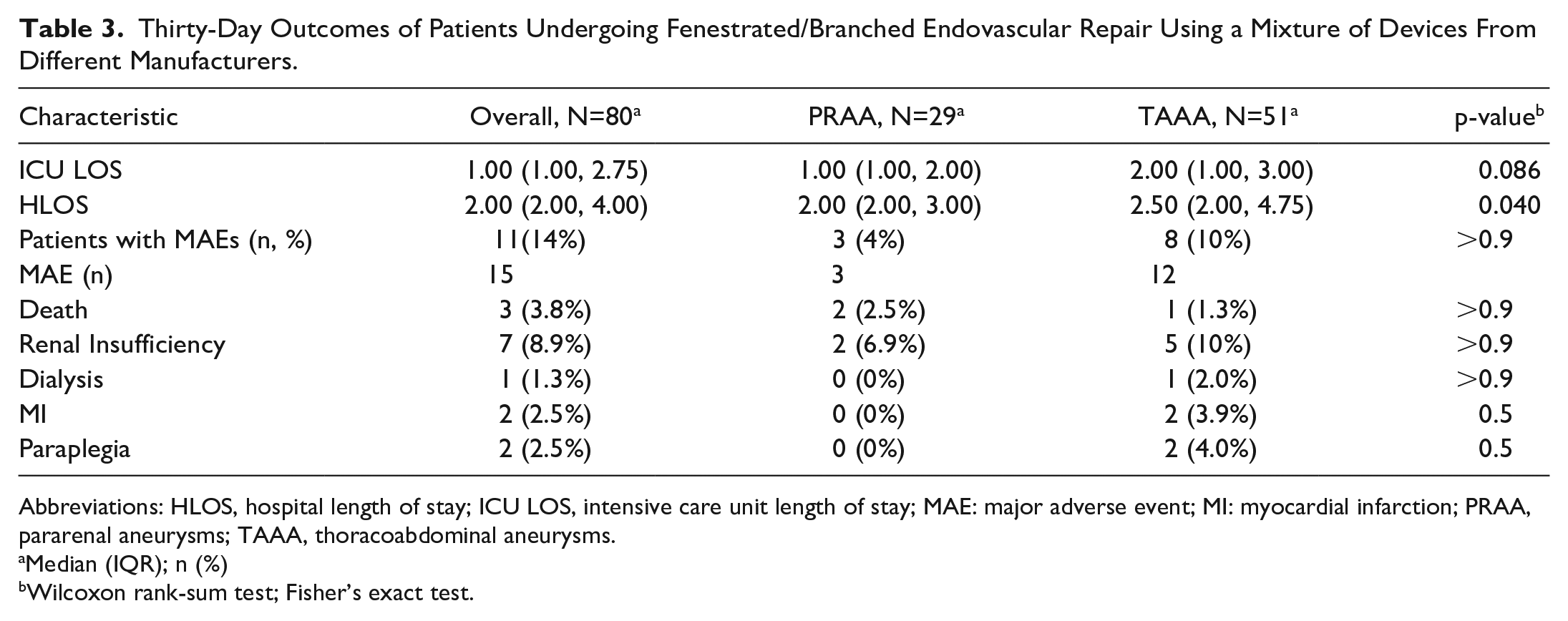
Abbreviations: HLOS, hospital length of stay; ICU LOS, intensive care unit length of stay; MAE: major adverse event; MI: myocardial infarction; PRAA, pararenal aneurysms; TAAA, thoracoabdominal aneurysms.
Median (IQR); n (%)
Wilcoxon rank-sum test; Fisher’s exact test.
At a median follow-up of 400 (85, 1132) days, 7 (9%) patients required reinterventions for type IIIa endoleak (n=1), type IIIc endoleak (n=2), type Ib endoleak (n=1) and type Ic endoleak (n=4). Long-term aortic-related mortality was 0%, and all-cause mortality was 8.8%. Estimated probability of freedom from reintervention at 1, 3, and 8 years was 95.3% (CI: 90.3%, 100%), 89.5% (CI: 80.8%, 99.2%), and 74.6% (CI: 51.4%, 100%), respectively (Figure 2).
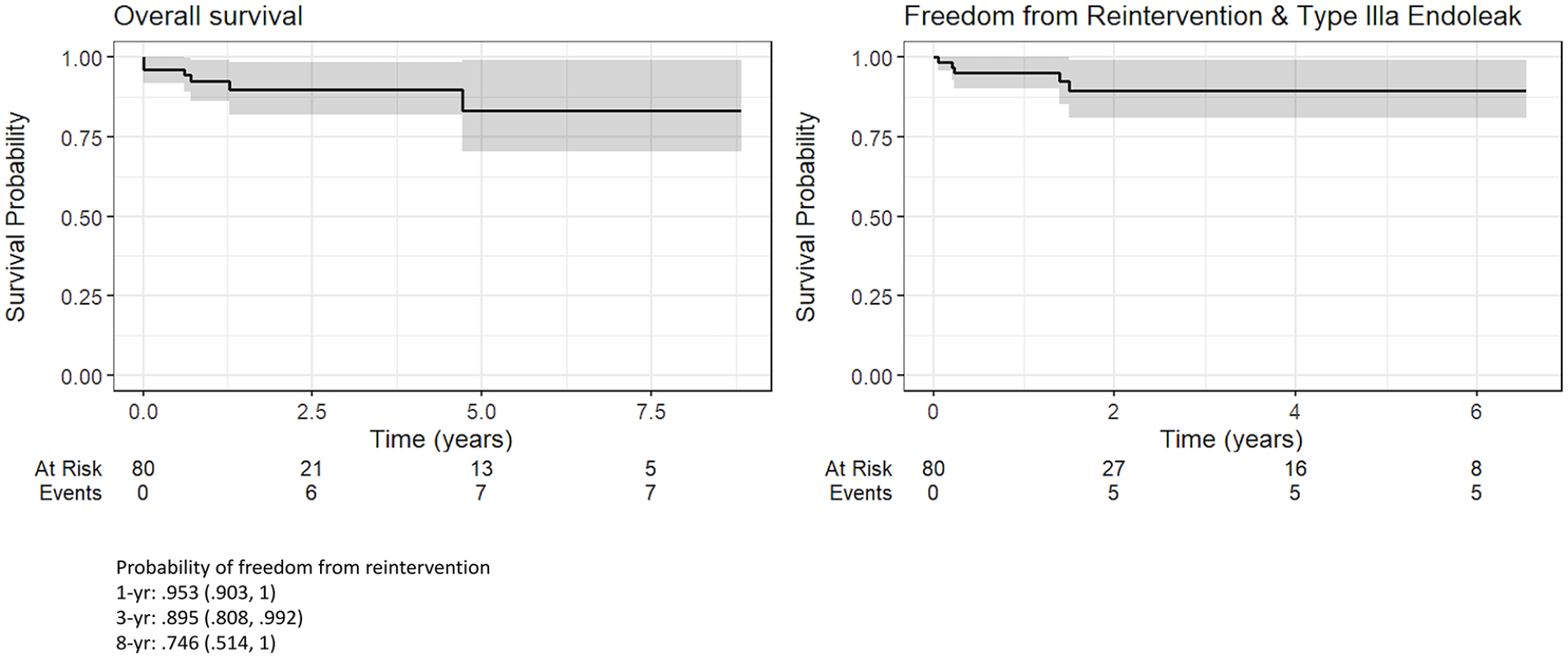
Kaplan Meier curves depicting survival, freedome from reintervention and type IIIa endoleak of the entire cohort of patients with complex aortic aneurysm treated using a combination of endoprosthesis from different manufacturers.
Discussion
Significant strides in device design have been made since endografts were incorporated into vascular specialists’ armamentarium. While considerable efforts persist in the quest to develop a device capable of accommodating all anatomical variations, there is a growing question among some as to whether the solution lies in amalgamating existing devices to achieve the most optimal patient outcomes. Saraidaridis et al highlighted that in patients undergoing endovascular infrarenal aortic aneurysm repair (EVAR) utilizing a blend of endoprostheses from different manufacturers, the absence of demonstrable endoleaks on completion angiography signaled comparable long-term rates of endoleak (36% vs 34%) and secondary interventions (18% vs 14%) to those treated with standard endografts. 6 Our investigation further reinforces this notion, particularly in patients undergoing cAAs repair using a combination of endografts from different manufacturers. Our data indicates that the practice of incorporating devices from different manufacturers is safe, as evidenced by our low overall incidence of type IIIa endoleak of 1.3% and freedom from reintervention at 1, 3, and 8 years of 95.3%, 89.5%, and 74.6% respectively (Table 4, Figure 2).
Long-Term Outcomes of Patients Undergoing Fenestrated/Branched Endovascular Repair Using a Mixture of Devices From Different Manufacturers.
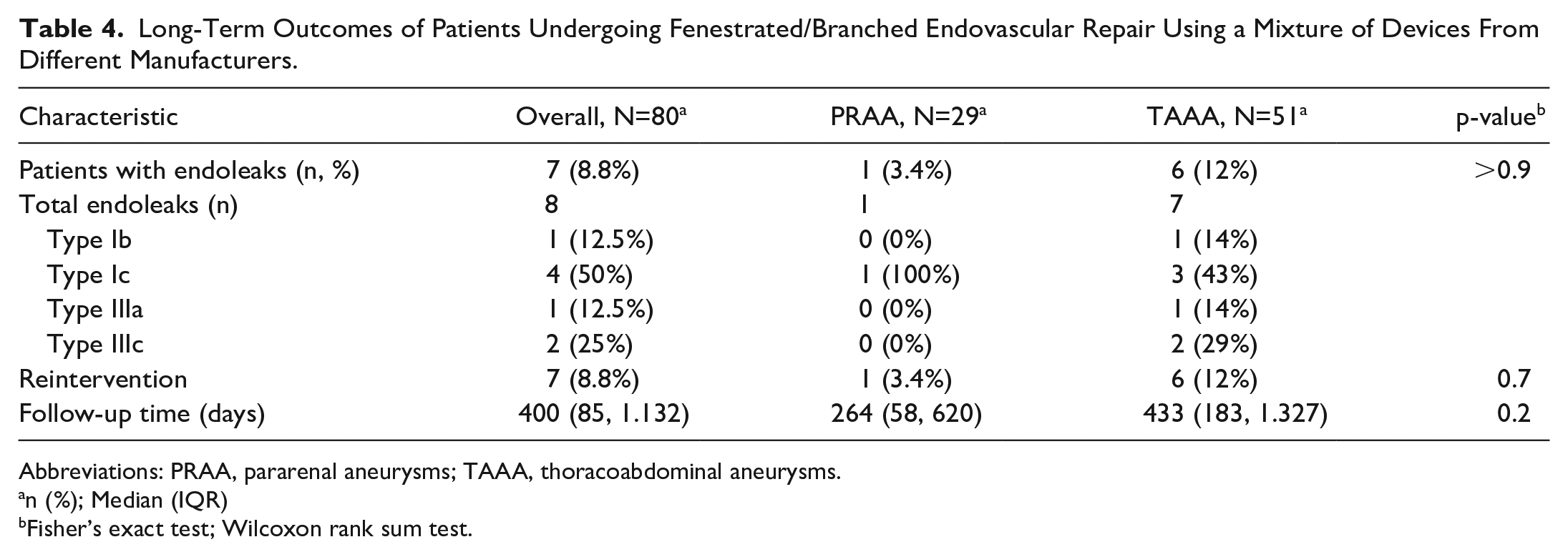
Abbreviations: PRAA, pararenal aneurysms; TAAA, thoracoabdominal aneurysms.
n (%); Median (IQR)
Fisher’s exact test; Wilcoxon rank sum test.
Incidence of type IIIa endoleak in randomized controlled trials and prospective registries ranges from 3% to 4.5%.15–17 However, in a series by Castelli et al 18 that included 173 patients undergoing EVAR for infrarenal aortic aneurysms, incidence of type IIIa endoleak was 12.1%. Factors associated with development of type IIIa endoleak, in this series, included aortic tortuosity, decreased device component overlap, large preoperative aortic diameter and tobacco abuse. This incidence of 12.1% is higher than that reported in randomized controlled trials including the EVAR 1 trial and the OVER trial as well as prospective registries such as the EUROSTAR.15–17 It is important to note that all patients included in the series by Castelli et al were treated using the Endologix platform, an implant with a relatively small market share in the United States and that was once recalled (AFX) in 2018 by the FDA due to its high incidence of type III endoleak. Our overall incidence of type IIIa endoleak of 1.3% (1 case out of 80 patients) is significantly lower than that reported in randomized control trials and Castelli et al, further validating our conclusion that the use of mixed devices is not associated with increase rate of component separation.
Type IIIa endoleaks are a known occurrence, observed in up to 25% of patients on completion angiography following cAA repair with f/b-devices. 19 Fortunately, the majority resolve spontaneously, requiring intervention only in rare instances. In a comprehensive study encompassing 328 patients undergoing f/b-EVAR, Karkkainen et al 13 reported 1% late type IIIa endoleak over a mean follow-up period of 24 ±21 months. In our own series, 1 (1.3%) experienced late type IIIa endoleaks, requiring reintervention. This occurred approximately 2 years post index procedure in a patient with a tortuous thoracic aorta and large TAAA. He was found to have separation of the thoracic (Gore cTAG) and the fenestrated component (Cook Alpha) on follow-up CTA, despite excellent aneurysmal exclusion with 2-stent (4 cm) overlap between these 2 components and decreasing aneurysmal sac on previous postoperative CTAs. Notably, the new type IIIa endoleak occurred following substantial reduction in aneurysm sac size and aortic remodeling, corroborating observations by Castelli et al. 18
Reintervention following f/b-EVAR is required in as many as 25% of patients, with a significant proportion attributed to target vessel complications such as endoleaks, occlusion, and kinking rather than type IIIa endoleak. This was certainly the case with patients included in our series. Note that only 1 patient underwent reintervention for type IIIa. Most interventions were related to side branch attachment (type Ic and type IIIc). In both patients who presented with type IIIc endoleak, fenestrations were initially bridged with Atrium iCAST stent grafts. The exact reason for separation could not be determine but both patients had aneurysm sac growth and the repairs were easily rescued by placing an additional Atrium iCAST stent graft with good result. In a contemporary series of patients undergoing f/b-EVAR, freedom from reintervention ranges between 63 to 90% at 3 years.13,20–23 Our overall freedom from reintervention at 1, 3, and 8 years of 95.3%, 89.5%, and 74.6%, respectively (Figure 2) and a reintervention rate of 9% compares favorably to other series encompassing patients treated for cAAs using devices from a single manufacturer.13,20–23
Among the patients included in our series, 51(64%) presented with aneurysms classified anatomically as TAAA. Notably, 71 patients (89%) underwent “thoracoabdominal repairs,” defined as the deployment of the f/b-device in the thoracic aorta with a minimum of 2 sealing stents positioned above the celiac trunk, as depicted in Figure 1. Within this cohort, 2 patients exhibited a shared origin of the SMA and CA, while in 2 others, the CA was occluded, resulting in a total of 65 patients undergoing a dedicated CA stenting. Our preference for deploying f/b-devices above the CA stems from several observations. First, studies have demonstrated that while incorporating ≥ 3 vessels during f/b-EVAR leads to increased operative time and fluoroscopy doses, the overall technical success rate, estimated blood loss, mortality, incidence of SCI and MAEs remain comparable to those in patients undergoing 1 or 2 vessel repairs. 24 Second, such a repair strategy facilitates more straightforward subsequent interventions in the event of proximal disease progression.
Two patients with PRAA required a thoracic stent graft placement in conjunction with f/b-devices. Both patients had “shaggy aorta” above CA, necessitating extension of the repair proximally. In these cases, as with all patients with Crawford extent I-III TAAA, repair was staged. Initial thoracic stent graft placement is followed by implantation of the f/b-device at least 3 weeks later.
Eleven patients (14%) experienced a total of 15 (19%) MAEs, comprising myocardial infarction in 2, renal insufficiency in 7, SCI in 2, and 3 fatalities—2 in the PRAA group and 1 in the TAAA group (Table 3). Among the TAAA cases, 2 patients developed SCI (1 case of paraparesis and another of paraplegia). Paraparesis occurred in a patient undergoing an elective Crawford extent II TAAA repair. He was able to be rescued after urgent placement of a spinal drain and other adjunctive measures and is now able to walk with a cane. Paraplegia occurred in a patient undergoing second-stage repair of Crawford extent I TAAA, complicated by SMA perforation causing severe hypotension. She developed paraplegia on the second postoperative day. Despite offering a spinal drain, the patient declined aggressive measures and succumbed to multisystem organ failure. Our 30-day mortality of 3.8%, 15 MAEs occurring in 11 (14%) patients, and reintervention rate of 9% are in line with those reported in contemporary series of patients undergoing f/b-EVAR.21,23–25 More importantly, there have been no instances of aortic-related mortality in patients who survived their index hospitalization.
A few technical aspects are worth discussing when it comes to mixing devices from different manufacturers. First and foremost is the issue of sizing and overlap. In all cases except 1 within this cohort, stent grafts were oversized by 5 to 12%. For instance, a 36 or 38 mm stent graft was deployed into a 34 mm stent graft from another manufacturer. Ensuring an overlap of more than 2 sealing stents was crucial to prevent long-term component separation, which can occur as the aorta remodels around the stent graft, especially in tortuous anatomy. Notably, the single case of component separation in our series—which occurred in a patient with very tortuous anatomy—underscores the importance of this practice.
Another critical aspect is the selection of the distal bifurcated device used alongside the physician-modified Cook Zenith fenestrated/branched device. Initially, both centers exclusively used the Zenith Flex AAA endoprosthesis, necessitating partial unsheathing of the device and removal of suprarenal stents before implantation. However, this approach has largely been abandoned in favor of the Gore Excluder AAA endoprosthesis at both centers, a device that lacks suprarenal fixation stents and features a shorter nose cone, minimizing the risk of renal artery bridging stent compression or displacement during deployment.
While our study offers valuable insights, it is important to acknowledge its limitations. One notable constraint is the relatively short overall follow-up duration. Furthermore, although the data were prospectively collected, our analysis is retrospective in nature. This lack of control introduces the possibility of biases influencing our findings. We recognize the potential for bias, as it is plausible that outcomes may have been influenced using devices from different manufacturers. However, as practicing vascular surgeons, we often encounter situations where we must combine devices from different manufacturers due to inventory constraints or supply chain issues. Despite these challenges, the knowledge that mixing devices from different manufacturers yields favorable mid-term results should offer reassurance to vascular surgeons navigating the complexity of device selection.
Conclusions
Mixing endografts from different manufacturers to treat complex aortic aneurysms using fenestrated and branched endografts has proven safe and has yielded favorable mid-term outcomes. As with any endovascular intervention, lifelong monitoring of these patients is essential to detect and manage potential late failures due to disease progression or device fatigue. Moreover, our findings warrant validation through larger cohorts and extended follow-up.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J.M.—Use of investigational device in an FDA-approved IDE (G220004), Consultation for W.L. Gore and Medtronic; H.H.: none; E.C.: none; J.G.: none; R.M.C.: none; E.S.: none, N.S.: none; M.A.R.: consultation for GE imaging.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: R.M.C. was supported by KL2TR001448.
Clinical Trial Registration
ClinicalTrial.gov NCT05531084.