
Abstract
Purpose:
Our study aims to determine optimal sizing of below-the-knee (BTK) artery angioplasty without intravascular ultrasound (IVUS), compensating for conventional angiography underestimation by selecting a balloon size one size larger than the 1-to-1 angiographic sizing.
Materials and Methods:
Our study is a retrospective, single-center study. Patients were separated into 2 groups as over and angiographic reference group which the over group is larger balloon diameter selection (0.5-mm larger balloon diameter selection), and angiographic reference group is 1-to-1 balloon diameter selection by angiographic images. Primary end point was the target vessel reocclusion, whereas major and minor amputation was the secondary end point.
Results:
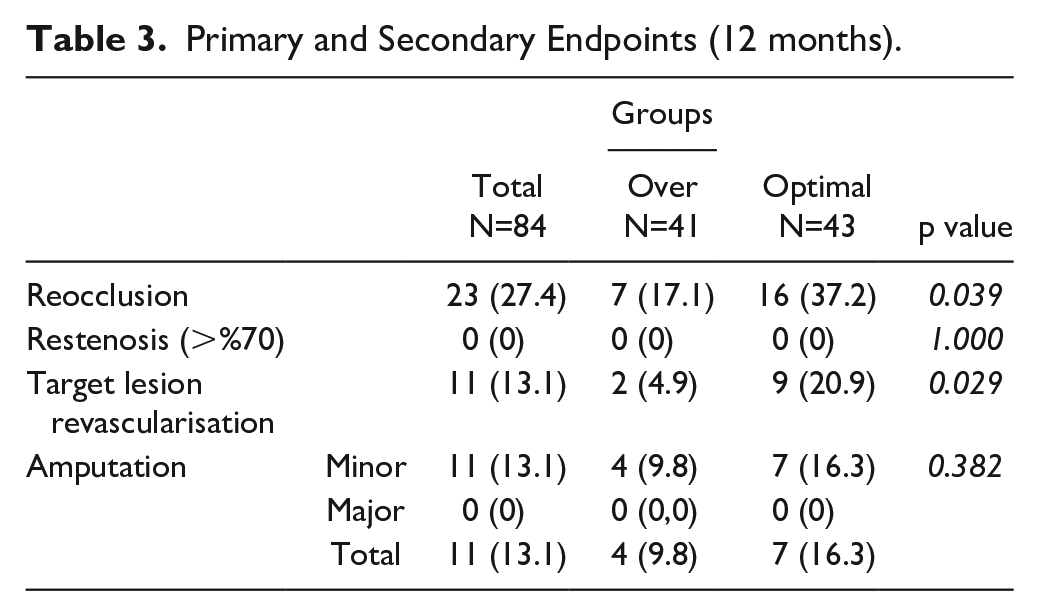
Eighty-four patients with occluded BTK lesions treated with balloon angioplasty (Opt=43, Over=41). Primary patency was 62.8% at 12 months in angiographic reference group and 82.9% in over group (p=0.039). Amputation rate at 1-year follow-up was 9.8% in angiographic reference group and 16.3% in over group (p=0.382). TLR rate is 4.9% in over group versus 20.9% in angiographic reference group (20.9%) at 1-year follow-up (p=0.029).
Conclusion:
Our study demonstrates that oversizing the balloon diameter by one size larger in BTK artery angioplasty, guided by conventional angiography, results in a higher patency rate and a lower target lesion revascularization (TLR) rate, while amputation rate remains statistically similar between the 2 groups.
Clinical Impact
Our study highlights the importance of compensating for conventional angiography’s underestimation in BTK artery angioplasty by using a balloon size one size larger than the 1-to-1 angiographic sizing. Our findings demonstrate that oversizing the balloon leads to significantly higher patency rates and lower TLR rates, with no increase in amputation risk. This approach provides a practical, cost-effective solution for clinicians performing angioplasty without IVUS, allowing for better vessel treatment and outcomes in patients with chronic limb-threatening ischemia. Clinicians can implement this strategy to optimize long-term results in BTK interventions.
Introduction
Peripheral arterial disease (PAD) involving the below-the-knee (BTK) arteries poses a significant challenge in endovascular interventions. Accurate sizing of BTK vessels is crucial for achieving successful outcomes in angioplasty procedures. Vessel sizing is mostly performed using angiography; however, it has been observed that conventional angiography underestimates the true size of BTK vessels. 1 This underestimation may lead to inadequate balloon sizing, compromising the effectiveness of angioplasty and may potentially result in adverse clinical outcomes such as reocclusion and amputation. To address the issue of sizing accuracy, intravascular ultrasound (IVUS) has been used as a valuable tool to accurately assess vessel dimensions.1,2 However, IVUS is not routinely available in all centers. Therefore, there is a need to explore alternative approaches to optimize sizing in BTK angioplasty without relying on IVUS. In this study, we propose an innovative approach to compensate for the underestimation of BTK vessel size by conventional angiography. By selecting the balloon diameter with a one additional size, we can achieve better clinical outcomes compared to an angiographic 1:1 sizing approach. This study has the potential to improve clinical outcomes and may guide interventional centers where IVUS is not readily available.
Patient Population
Our study is a retrospective single-center study. Eighty-four patients with BTK lesions undergoing balloon angioplasty in patients with Rutherford class 4 or higher at our center were screened for enrollment. Occlusion of BTK vessel with a successful endovascular intervention was the inclusion criteria. Contraindication to combined antiplatelet treatment and acute limb ischemia were the exclusion criteria. Patients were separated into 2 groups as over and angiographic reference group, which the over group is one size larger balloon diameter selection and angiographic reference group is 1-to-1 balloon diameter selection due to angiographic images. In the over group, a balloon size that is one size larger is selected (0.5 mm larger balloon diameter selection) compared to the size chosen for the 1-to-1 angiographic measurement. There was not statistically difference of cardiovascular risk factors and procedural characteristics between the 2 groups (Table 1). Reocclusion at 1-year follow-up at target vessel was the primary end point, whereas major and minor amputation was the secondary end point.
Procedural Data.
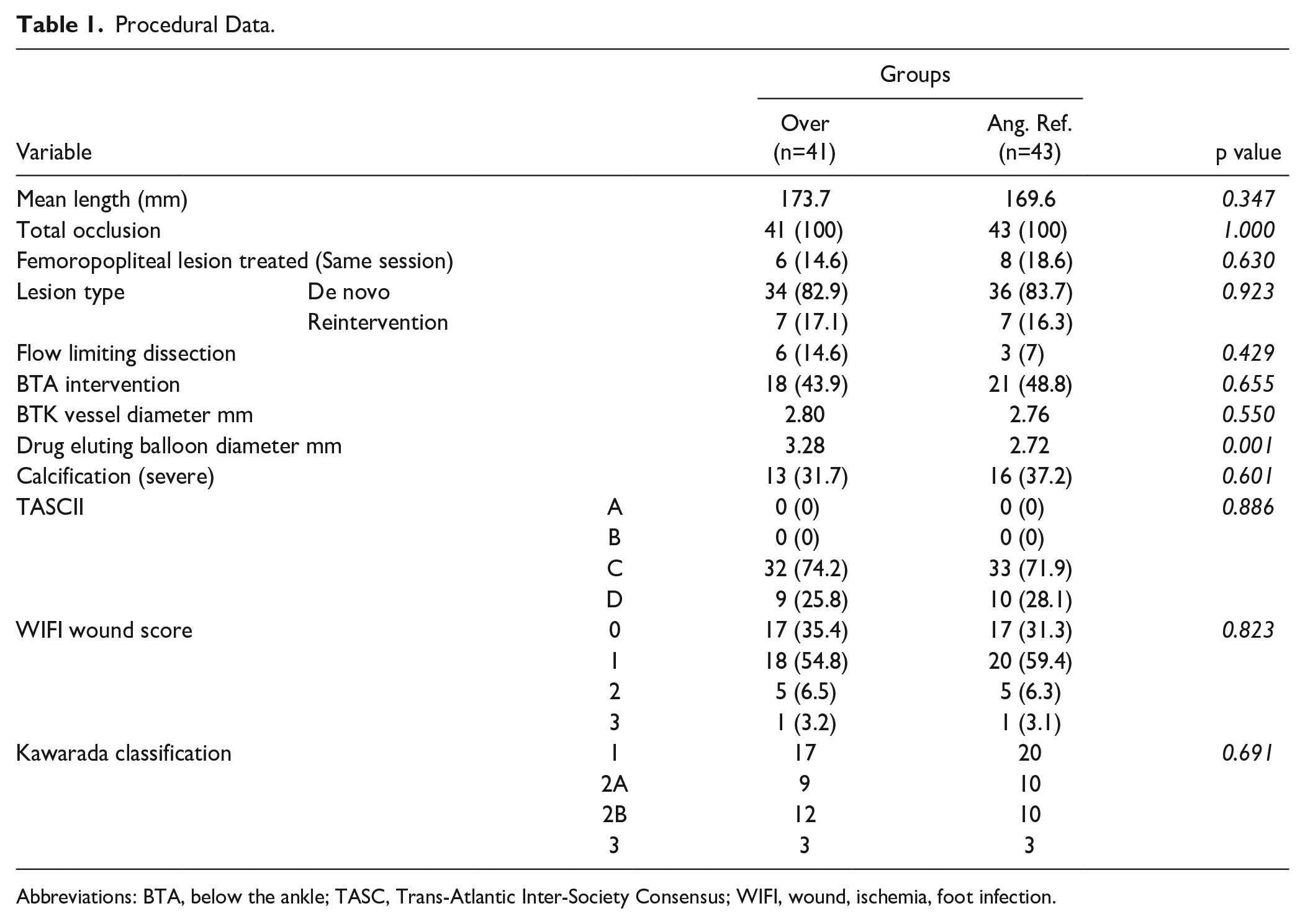
Abbreviations: BTA, below the ankle; TASC, Trans-Atlantic Inter-Society Consensus; WIFI, wound, ischemia, foot infection.
Methods
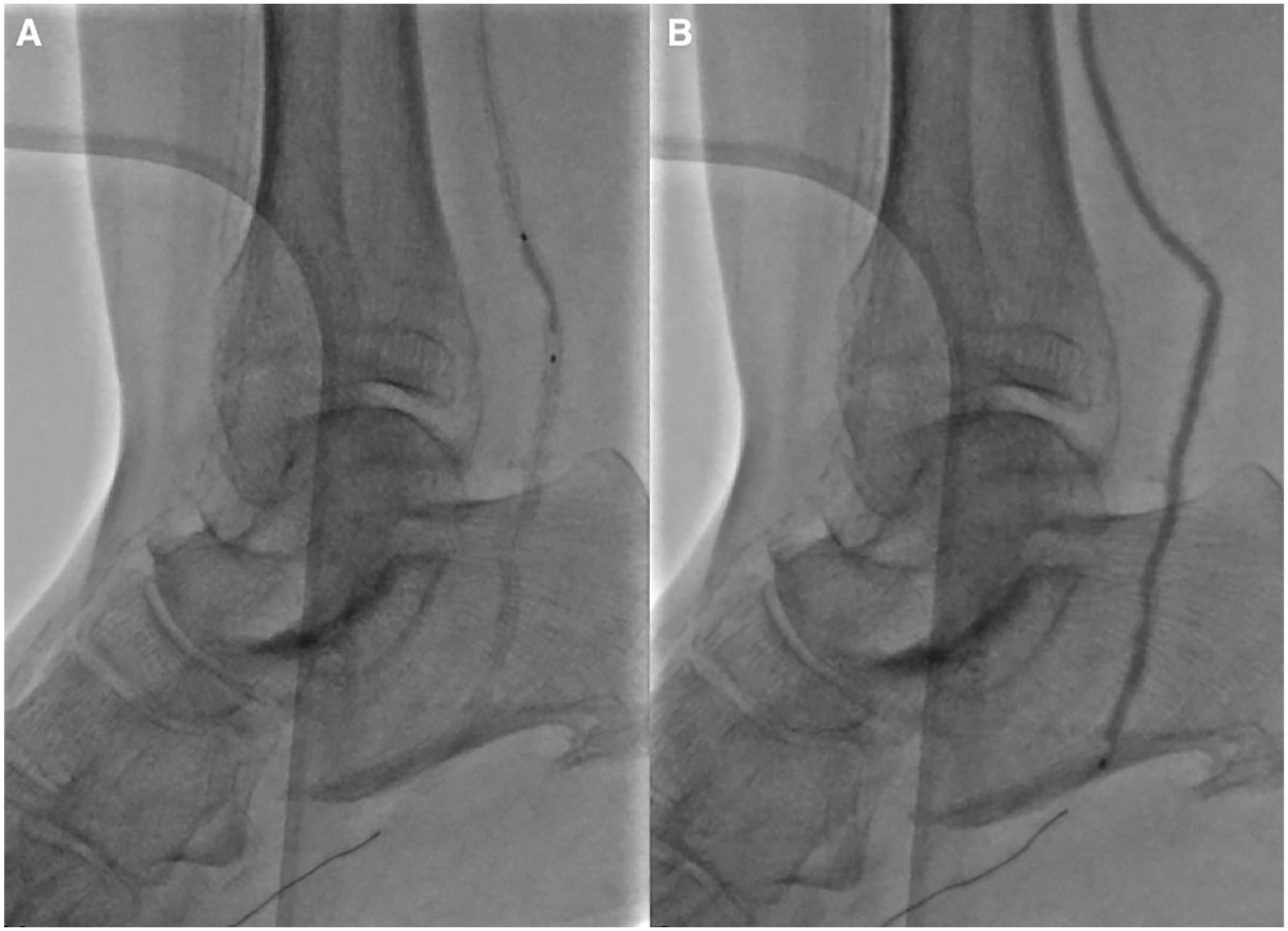
This study complies with the principles outlined in the Declaration of Helsinki. The study received approval from the local ethics committee (Hospital committee no: AEK 23/006). We used the antegrade femoral approach as the preferred method in all patients, while the transpedal retrograde approach was employed in 8 patients (antegrade femoral approach failure) during the same session Figure 1). Prior to the intervention, all patients underwent preoperative ultrasound (USG) evaluation. Below-the-knee lesions were initially assessed and quantified using USG in all patients, and in 50 patients, further evaluation was conducted using computed tomography angiography (CTA) before the intervention. Finally, digital subtraction angiography (DSA) was performed for all patients to assess and guide the intervention.

Photographic and angiographic images of retrograde transpedal approach.
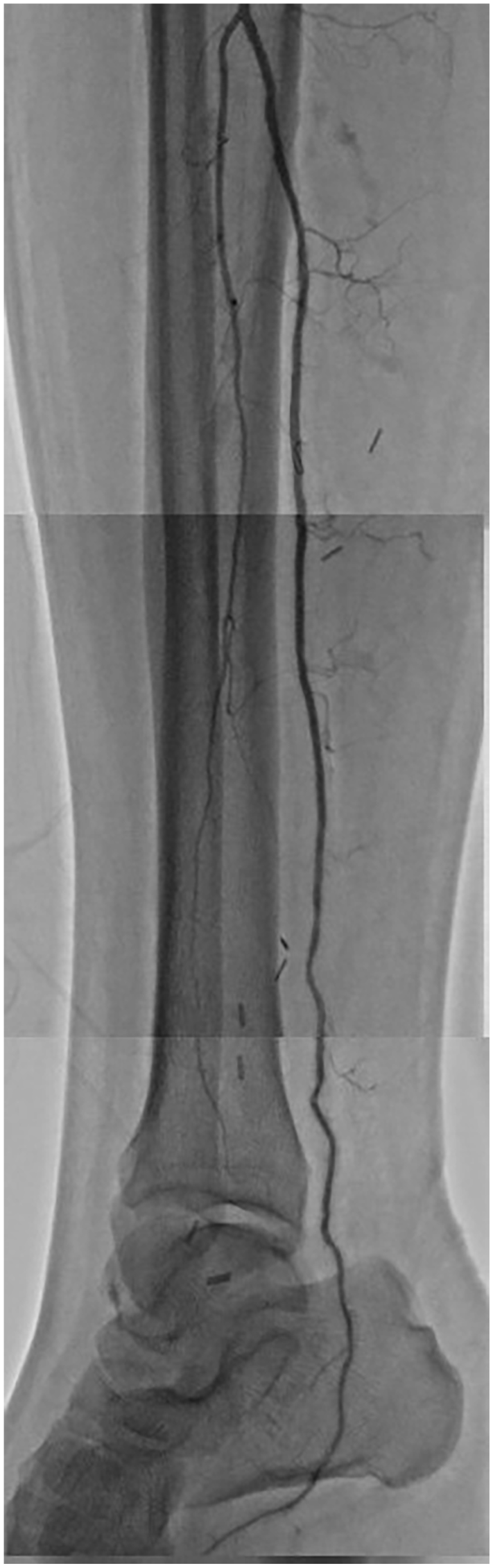
After the diagnostic angiography was performed, intravenous heparin (100 IU/kg) was administered to the patients (Figure 2). To cross the lesions, a crossing catheter (0.018 inch) was used in conjunction with a guide wire (0.018 inch) in all patients. Following successful crossing of the occluded lesion, a guidewire exchange was performed, replacing the 0.018 guidewire with a 0.014 guidewire to continue through the pedal arch (with also 0.014 crossing catheter where needed). Although it is not a standard method, based on our experience, particularly in cases involving calcific and tortuous vessels, we used coronary artery balloons for predilatation in situations where standard peripheral balloons were unable to cross the lesions (Figure 3). Drug-eluting balloon (DEB) angioplasty after predilatation with standard balloon angioplasty (SBA) was further intervention. Drug-eluting balloons used at diameter of 2.5 to 4.0 mm and a length of 40 to 200 mm. We evaluated the vessel reference diameter using quantitative coronary analysis (QC, calibration was based on guiding and microcatheters) and selected the diameter of the DEB accordingly. The DEB that we preferred was high-dose DEB with nominal paclitaxel densities and coated with nanotechnologies, enabling maximal transfer of the drug to the arterial wall while minimizing transit loss. In the over group, a DEB with a diameter one size larger was selected, while in the angiographic reference group, a 1-to-1 DEB diameter selection was made based on angiographic images. When multiple balloons were used per lesion, the overlap zone between them was maintained at a minimum of 5 mm. In general, we favored inflation times of up to 3 to 4 minutes. If flow-limiting dissection or residual stenosis of greater than 50% was present, an additional prolonged dilation of up to 3 minutes was performed. After all, a final angiography concluded the procedure (Figure 4). Patients with and below the ankle critical lesions (Over N=18; angiographic reference, N=21) underwent percutaneous transluminal angioplasty (PTA). Femoral access site hemostasis managed with manual compression. Pedal access site hemostasis also managed with manual compression. Procedural data are summarized in Table 1. Dual antiplatelet therapy consisting of aspirin (100 mg per day) and clopidogrel (75 mg per day) for 3 months and proper medication for risk factors such as coronary artery disease, hypertension, and hyperlipidemia were given after endovascular therapy (EVT). One-week postdischarge, aspirin was discontinued, and at the 3-month mark, clopidogrel was replaced with aspirin in the patients using new oral anticoagulant (NOAC). Wound care was received in a wound center. During follow-up, patients were evaluated with Doppler USG examination, whereas angiography performed in patients when indicated.

Angiography before intervention, posterior tibial artery occluded and severely calcific.
Over group: treatment of severely calcific and tortuous lesion in the posterior tibial artery with coronary artery balloon (A), followed by POBA 1:1 long angioplasty (B).
Final angiography of occluded posterior tibial artery: over group.
Statistical Analysis
Data were reported as mean, standard deviation, median, frequency, and ratio. Student’s t test was used for the comparison of normally distributed parameters. Mann-Whitney U-test was used for the comparison of nonnormally distributed parameters. Fisher’s exact test and Yates’ continuity correction test were used for comparison of qualitative data. Wilcoxon signed ranks test was used to test the difference between preop and postop values. The results were evaluated in 95% confidence interval and at a significance level of p<0.05.
Results
A total of 84 patients who underwent EVT for BTK lesions were included in our institution’s study, with 41 patients in the over group and 43 patients in the angiographic reference group. There was no statistical difference of cardiovascular risk factors and procedural characteristics between the 2 groups (Table 2). None of the interventions required bailout stent implantation. Reocclusion occurred in 23 cases (over=7, optimal=16). Among the patients with reocclusion, 11 required reinterventions, all except 1 (in the angiographic reference group) were successfully managed with endovascular therapy (2 in the over group and 8 in the angiographic reference group). Eleven minor amputations were performed in 11 patients, all of whom had baseline wounds (over=4, optimal=7) (Table 3). Nine cases of flow-limiting dissection were observed, and these were all treated with an additional balloon dilatation (over=6, optimal=3). The flow limiting dissections were FLIPI (flow limitations in peripheral interventions) grade 2 and 3. During the initial treatment, extravasation was seen during guide-wire positioning in 5 patients, with 2 occurring at the posterior tibial artery and 3 at the anterior tibial artery. All cases were managed by employing prolonged balloon dilatation (over=3, optimal=2). In addition, there were 6 cases of access-related hematoma, all of which resolved with digital pressure.
Baseline Demographics.
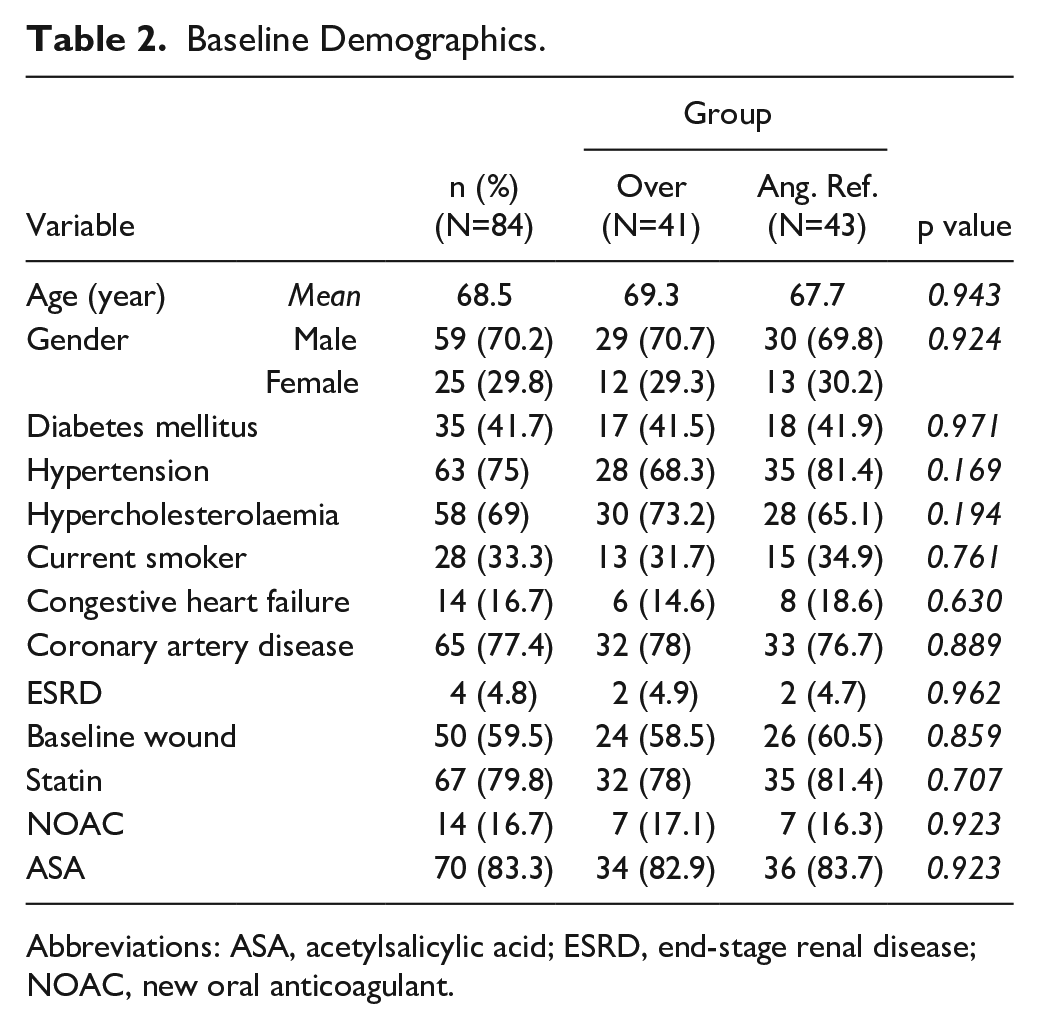
Abbreviations: ASA, acetylsalicylic acid; ESRD, end-stage renal disease; NOAC, new oral anticoagulant.
Primary and Secondary Endpoints (12 months).
Discussion
Conventional angiography can underestimate BTK artery diameter by up to 30%, affecting balloon angioplasty efficacy.1,2 While IVUS accurately assesses BTK vessel dimensions, it is not universally available. To address this, we retrospectively analyzed BTK angioplasty patients using 2 sizing strategies: 1 employing a balloon diameter one size larger (0.5mm) than 1:1 and the other using 1:1 sizing. Although the oversizing group had more flow-limiting dissections, the difference was not statistically significant, possibly due to angiographic imaging underestimation. Our aim was to achieve better procedural success with a low amputation rate and maintain long-term artery patency by compensating for vessel size underestimation since using a balloon appropriate for the vessel diameter would result in better lesion dilation, reduced likelihood of elastic recoil, and decreased transit loss due to the drug in DEB and effectively penetrating the arterial wall.
In patients with BTK artery lesions, often presenting with extensive arteriosclerotic disease, EVT is preferred over bypass surgery due to factors like concomitant diseases and advanced age. For those with BTK lesions and critical limb ischemia, EVT is recommended as the primary approach for stenotic lesions and short occlusions, with surgery reserved for long occlusions per European Society of Cardiology (ESC) guidelines. 3 American College of Cardiology/American heart association (ACC/AHA) guidelines advise an interdisciplinary care team to evaluate revascularization options. 4 The notable The Best Endovascular vs Best Surgical Therapy in Patients with Critical Limb Ischemia (BEST-CLI) study compared outcomes of EVT and surgical interventions in CLI patients. 5 It found that patients with chronic limb-threatening ischemia (CLTI) and adequate single-segment great saphenous vein length for bypass surgery had fewer repeat interventions and lower risk of major adverse limb events than those undergoing endovascular therapy. However, the study’s preference for bypass surgery may not reflect outcomes achievable by experienced CLTI experts, suggesting potential proficiency gaps in endovascular techniques among certain operators. In addition, the study primarily involved vascular surgeons, potentially limiting the representation of diverse physicians treating CLTI. Furthermore, enrolled patients had lower-to-moderate-risk CLTI and were younger than the average CLTI population, and endovascular therapy utilization was suboptimal, with less use of drug-coated balloons and drug-eluting stents. In conclusion, it is important to note that the choice of treatment should be individualized based on the specific characteristics and needs of each patient, as determined by the health care provider.
Drug-eluting balloon angioplasty has shown better outcomes mostly related to patency rate compared to SBA in multiple studies in BTK lesions.6 –9 However, there have been studies comparing SBA and DEB interventions in BTK lesions, which have shown that the efficacy of DEB is comparable to SBA.10,11 The variation in amputation rates observed in the IN.PACT DEEP trial is believed to be attributed to differences in wound care management. The use of different DEBs, with variations in paclitaxel concentrations, excipients, and drug release mechanisms, can influence the biological effects and antirestenotic properties within the vessel wall. These factors potentially account for the discrepancies in patency rates observed among studies using DEB angioplasty. While drug-eluting stents may be considered as an alternative to DEBs in BTK interventions, their utilization is limited by the length and complexity of BTK lesions. 12 Therefore, in our study, despite being less frequently used compared to the previous decade, DEB interventions in BTK are still conducted. Considering that all lesions are Trans-Atlantic Inter-Society Consensus (TASC) C and D lesions, and more than half of the patients have baseline wounds, we opted for DEB angioplasty.
Recent advancements in atherectomy, lithotripsy devices, cutting balloon, and scoring balloon catheters have shown promising results in improving patency rates while reducing complications.13,14 However, based on our prior experiences, we have refrained from using atherectomy devices as an adjunctive therapy due to the occurrence of perforations and flow-limiting dissections in BTK arteries. 13 In addition, the current cost of lithotripsy catheters has limited their usage in our practice. Nevertheless, further research is necessary to assess the effectiveness and safety of these newer devices specifically in the context of BTK lesions.
A meta-analysis raised safety concerns about paclitaxel in BTK interventions, citing increased risk of death or limb loss during the first year. 15 The actual causes remain unclear, but potential mechanisms include paclitaxel embolization. Atherosclerotic lesions hinder drug transfer and increase wash-off into circulation. 15 Calcific lesions may require plaque modification before DEB angioplasty. Recent studies indicate DEB’s safety and efficacy in BTK lesions.16 –18 Future studies should compare DEBs based on technology and drug type, with or without adjunctive therapies.
In studies focusing on BTK interventions, it is crucial to emphasize that the amputation rate holds greater clinical significance than the patency rate. While patency, or the open and unobstructed state of the treated artery, is an important factor, the ultimate goal of BTK interventions is to preserve limb functionality and prevent amputations. In our study, 8 amputations occurred within the first 2 months, with 4 in the over group and 4 in the angiographic reference group, all of which had baseline wounds and were planned amputations. The remaining 3 amputations, which were observed at the 10th and 11th month, were in the angiographic reference group. While there was no statistical difference observed between the 2 groups, it is important to acknowledge that the lack of distinction may be attributed to the limitations of our study, such as a relatively small sample size and a shorter follow-up duration. It is possible that with a larger sample size and a longer follow-up period, there could potentially be discernible differences between the 2 groups in terms of long-term amputation rate outcomes.
Limitations
The retrospective nature, relatively small sample size and a shorter follow-up duration is the major limitations of this study. Another limitation is that angiography is superior to DUS for detecting binary restenosis during follow-up. However, in our clinic, angiography is reserved for symptomatic patients with evidence of restenosis on doppler ultrasonography.
Conclusion
Our study demonstrates that increasing the balloon diameter by one size larger in BTK angioplasty, as determined by conventional angiography, results in a higher patency rate and a lower TLR rate. However, amputation rate remains statistically similar between the groups. Amputation is a critical outcome with profound implications for the quality of life of patients. Therefore, it is imperative to conduct further and more extensive research, involving larger populations and longer follow-up periods, to accurately assess the impact of sizing strategies on amputation outcomes in this specific population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.