
Abstract
Objective:
This study aimed to evaluate the efficacy and safety of stent placement after percutaneous recanalization of superior vena cava (SVC) stenosis in maintenance hemodialysis patients.
Methods:
Adult maintenance hemodialysis patients hospitalized at a university-affiliated tertiary hospital due to SVC stenosis from January 2016 to June 2023 were prospectively included. The efficacy and safety of percutaneous blunt/sharp SVC recanalization combined with SVC stent placement were observed. The patients’ demographic information and laboratory examination data, stent placement success rate, surgery-related complications, and long-term vascular access patency rate were also recorded and analyzed. The study was approved by the institutional ethics committee (2015-201) and registered at http://www.chictr.org.cn (registry number: ChiCTR-ONN-16007790).
Results:
A total of 58 patients were included in the study with an average age of 54.79±13.42 years. Percutaneous SVC recanalization was successful in 53 cases, with a success rate of 91.38%, including 37 cases of traditional recanalization and 16 cases of sharp recanalization. Among 53 hemodialysis patients who underwent SVC recanalization, 14 patients successfully received covered stents and 38 patients received bare metal stents, achieving a stent placement success rate of 98.1%. One patient encountered stent displacement into the heart immediately after implantation, causing intra-operative cardiac tamponade, who was successfully rescued by thoracotomy. Fifty-two patients were followed-up for median period of 26 months (cuffed catheter: 25 patients, arteriovenous fistula [AVF]: 27 patients). The overall 2-year vascular access patency rate was 33.2% (cuffed catheter: 22.2%, AVF: 41.7%, p=0.414). There was no statistically significant difference in the 2-year vascular access patency rate between the traditional recanalization group and the sharp recanalization group (34.1% vs 31.1%, p=0.731) and between bare metal stent group and covered stent group (38.1% vs 21.4%, p=0.248).
Conclusion:
Percutaneous SVC recanalization with stent placement is an effective treatment strategy that can provide viable vascular access for maintenance hemodialysis patients with SVC stenosis. Cautions should be paid to potential life-threatening complications such as stent displacement and cardiac tamponade.
Clinical Impact
Superior vena cava (SVC) stenosis is a common central venous occlusive lesion in maintenance hemodialysis patients. Whether stent should be implanted simultaneously following SVC recanalization is still lacking research. This pilot cohort study suggested that percutaneous SVC recanalization with stent placement was an effective treatment strategy which provides satisfactory vascular access for hemodialysis. We further found that SVC sharp recanalization with subsequent stent implantation was a feasible treatment, with the 2-year vascular access patency comparable to the traditional SVC recanalization group. This study also highlighted endovascular SVC recanalization should be performed with caution, and appropriate balloon sizes should be selected to avoid SVC rupture or stent displacement.
Introduction
Superior vena cava (SVC) stenosis is a common condition in which the SVC, a major vein that carries deoxygenated blood from the upper body to the heart, becomes narrowed. This narrowing is often caused by central venous catheterization and can lead to severe venous hypertension and vascular access dysfunction. 1 Symptoms of SVC stenosis include swelling of the face, neck, and arms, shortness of breath, and coughing. Currently, the main treatment method for SVC stenosis is percutaneous SVC recanalization, using a catheter to open up the narrowed SVC. Stent placement is a further procedure that involves the insertion of a small metal mesh tube into the SVC to keep it open. It is possible that stent placement may be more effective than percutaneous SVC recanalization alone. A recent meta-analysis suggested that stenting is an effective intervention for benign and malignant stenosis of the SVC and other central vein segments, with 81.5% of stents retaining patency at 6 to 12 months. 2 However, given the high incidence of in-stent restenosis, 3 whether stent placement should be performed simultaneously in maintenance hemodialysis patients is still under debate. 4 More research is needed to determine the optimal treatment strategy for SVC stenosis. In this study, our hypothesis was to verify that whether percutaneous SVC recanalization with subsequent stenting is an effective treatment strategy to provide viable vascular access for maintenance hemodialysis patients.
Materials and Methods
Patient Selection
This is a prospective cohort study that enrolled hemodialysis patients who received percutaneous recanalization of the SVC and subsequent stent implantation in a university-affiliated tertiary hospital from January 2016 to June 2023. Patients who were admitted for vascular access dysfunction were screened for eligibility according to the following criteria: (1) aged 18 or above, (2) on maintenance hemodialysis for at least 3 months, (3) presented with hemodialysis vascular access dysfunction with/without symptoms of SVC syndrome, (4) diagnosed as SVC stenosis or occlusion by digital subtraction angiography (DSA) or computed tomography angiography (CTA). Patients were excluded from the study if they had severe cardiac, hepatic, or cerebral diseases; had severe infection; could not cooperate because of mental health problems; or refused to give inform consent.
A chart review was performed on each patient to identify sex, age, primary disease, dialysis years, and history of previous line insertions. Follow-up information was collected from the outpatient medical record database and the hemodialysis database or by telephone calls to document the current state of dialysis, complications, vascular access patency, and other therapeutic information. The patients were followed-up until the termination of hemodialysis (such as death, renal transplant, or switch to peritoneal dialysis) or the end of the study. The last follow-up was performed in October 2023.
The study was approved by the institutional ethics committee (2015-201) and registered at http://www.chictr.org.cn/ in January 2016 with the registration number: ChiCTR-ONN-16007790. The study was abided by the Declaration of Helsinki and the Declaration of Istanbul. Informed consent was obtained from all participants or his/her legal representative. For data analysis, specific identifiers of protected individual health information were removed from the data set, such as names, geographic subdivisions, and medical record numbers.
Superior Vena Cava Recanalization and Stent Implantation Procedure
Under procedural sedation, a catheter is inserted through a small incision in the skin and guided to the site of stenosis using imaging guidance. Once the catheter is in place, a wire is passed through it and advanced across the site of stenosis. If the occlusion could not be passed by blunt recanalization after multiple attempts, the patient then received sharp recanalization after informed consent using the needle of a 5-F Input Introducer Sheath (Medtronic, Minneapolis, Minnesota). 5 Multiple orthogonal fluoroscopic projections were performed to guide the path of the needle. Once the needle crossed the lesion, venography was performed to rule out extravasation. The wire is then used to guide a balloon (Maxi LD, Cordis, Milpitas, California) to the site of stenosis. The balloon is then inflated to open up the SVC and restore blood flow. A stent of proper size (Wallstent/Wallgraft, Boston Scientific, Natick, Massachusetts, 8 mm-16 mm*60 mm-100 mm) was chosen and advanced through the guidewire to the stenotic lesion and inflated. The stent size was decided with reference to the adjacent normal SVC basing on preprocedural CT, and the diameter is supposed to be 10% to 20% or 1 to 2 mm larger than the venous diameter. Given the aggressive nature of neointimal hyperplasia, tissue might emerge through the bare strut area, we tended to use covered stent when there was long segment stenosis or when there was increased risk of vascular laceration (such as severe calcification). However, when the stenotic lesion involved the orifice of azygos vein or extended into brachiocephalic vein, bare metal stent was usually preferred to preserve the blood flow. After the deployment, the location of the stent was immediately confirmed under DSA to rule out migration. A cuffed catheter might also be implanted through the recanalized and stented SVC (Figure 1). Patients were closely monitored for vital signs postoperatively. No prophylactic antibiotics were provided.
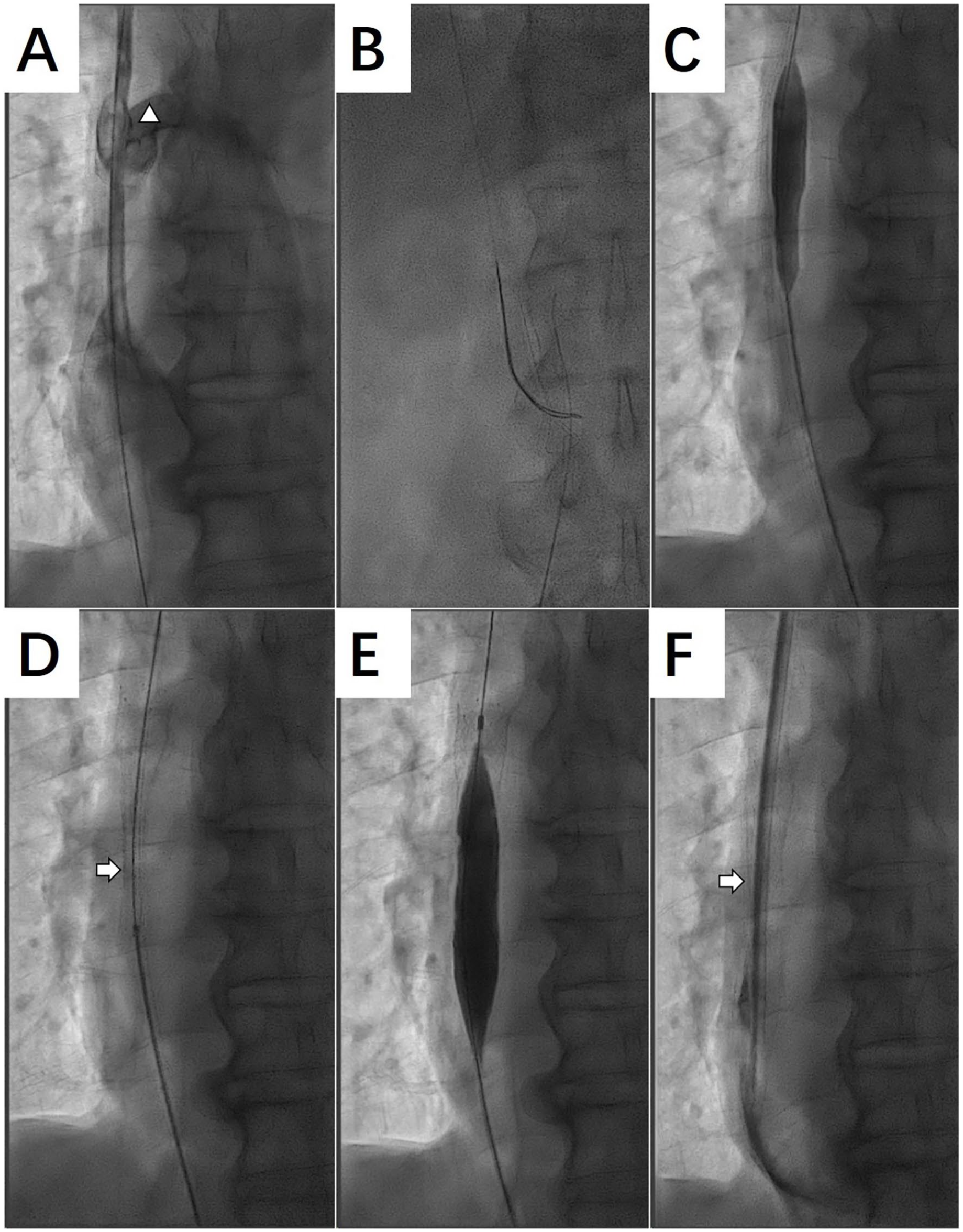
SVC recanalization and stent implantation procedure. (A) SVC stenosis shown by DSA. Triangle: dilated azygos vein. (B) Guidewire passed through the stenotic lesion. (C) Initial balloon dilation of SVC stenosis. (D) Stent advanced to the stenotic lesion. Arrow: stent. (E) Dilation of stent. (F) Cuffed catheter placed through the recanalized and stented SVC. Arrow: stent. SVC, superior vena cava; DSA, digital subtraction angiography.
Data Analysis
The study recorded and evaluated demographic information, clinical outcomes, perioperative and postoperative complications, vascular access patency, and patient prognosis. Perioperative complications were observed and recorded. Vascular access patency was defined as the time from stent implantation to vascular access dysfunction or any intervention to facilitate access function. Continuous measurement data were expressed as the mean±standard deviation or median (range), whereas categorical data were expressed as percentages. Patency rates were calculated using the Kaplan-Meier survival analysis. The data were analyzed using SPSS 19.0 software (SPSS Inc, Chicago, Illinois).
Results
Baseline Characteristics
Our study prospectively enrolled 58 patients between January 2016 and June 2023. The cohort consisted of 42 females and 16 males, with a mean age of 54.8±13.4 years and an average hemodialysis vintage of 84.9±52.0 months. Upon admission, 30 patients were dialyzed through a malfunctional arteriovenous fistula (AVF), 10 patients were dialyzed with a cuffed catheter with unsatisfactory blood flow rate, and 18 patients were dialyzed through a contemporary catheter. Twenty-five patients also presented symptoms of venous hypertension and upper limb/fascial edema. The mean Charlson score was 4.96±1.55. The etiology of end-stage renal disease included diabetic nephropathy (18 patients, 31.0%), chronic glomerulonephritis (12 patients, 20.7%), nephrotic syndrome (10 patients, 17.2%), hypertensive nephropathy (5 patients, 8.6%), lupus nephritis (3 patients, 5.2%), and other/unknown reasons (10 patients, 17.3%). The mean length of SVC stenotic lesion was 13.89±4.09 mm. Thirty-six patients (62.1%) had concomitant stenosis of other central veins. The median time from the onset of clinical symptoms to admission was 1 month. The baseline characteristics are summarized in Table 1.
Basic Characteristics of Included Patients.
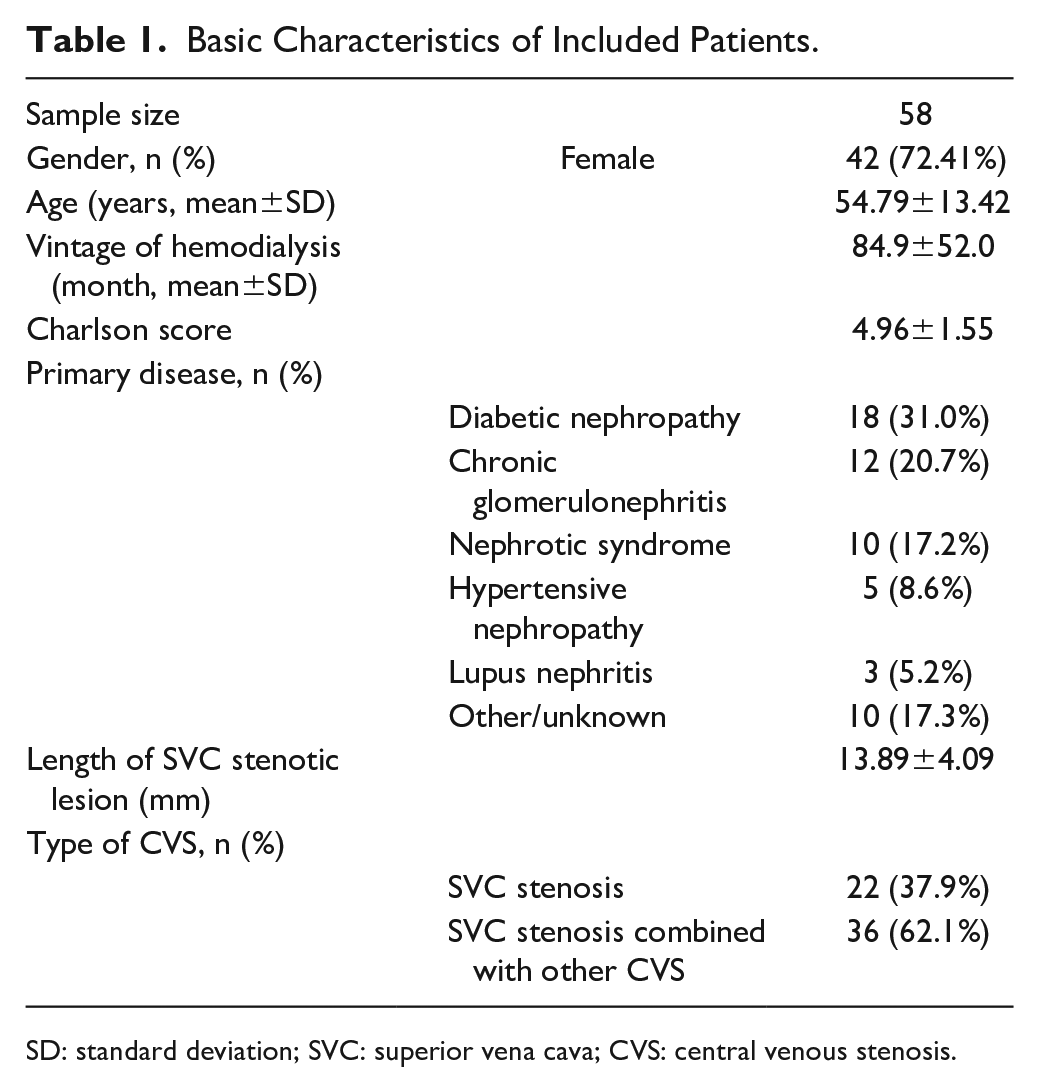
SD: standard deviation; SVC: superior vena cava; CVS: central venous stenosis.
Clinical Outcomes and Safety
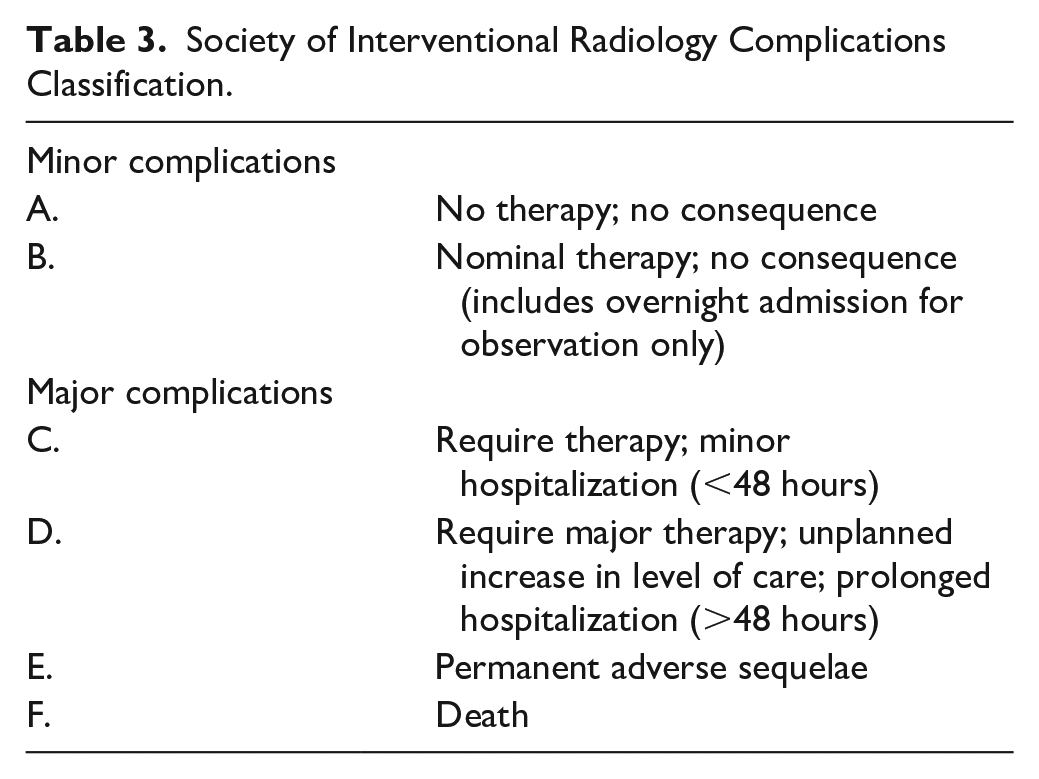
Out of 58 patients, 53 (91.38%) were successfully recanalized. Traditional guidewire and catheter technique were used to recanalize 37 patients, whereas 16 cases were recanalized with sharp recanalization. Stents were successfully placed in 52 patients, with a stent placement success rate of 98.1%. Fourteen patients used covered stents, whereas 38 patients received bare metal stent implantation. After stent placement, 25 patients underwent successful dialysis catheter placement, and the dialysis flow rate was satisfactory. Twenty-seven patients had the AVF function improved or successfully-established AVF. There were 10 episodes of perioperative complications encountered in 10 patients according to the Society of Interventional Radiology (SIR) reporting guidelines. Nine patients (15.5%) presented with mild chest pain and were relieved with oral non–steroid anti-inflammatory drugs (NSAIDs) (SIR Class B). Unfortunately, a 50-year-old female hemodialysis patient encountered stent migration into the right atrium, which resulted in pericardium tamponade and was successfully rescued by emergent thoracotomy (SIR Class D). 6 No other perioperative complications were observed (Tables 2 and 3).
Clinical Outcomes of Patients With Perioperative Complications.
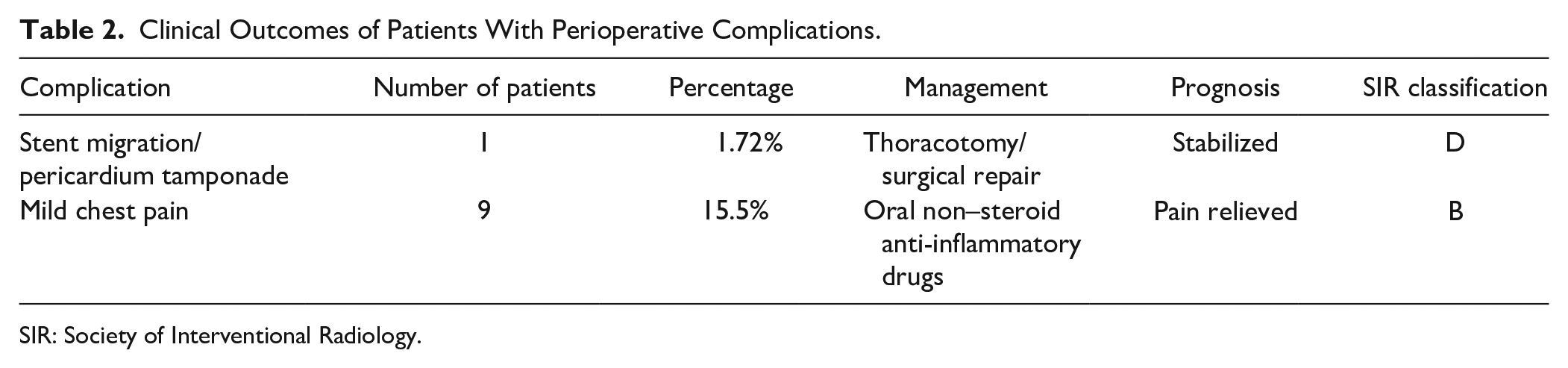
SIR: Society of Interventional Radiology.
Society of Interventional Radiology Complications Classification.
Follow-up and Long-term Vascular Access Patency
Fifty-two patients were followed-up for median period of 26 months (cuffed catheter: 25 patients, AVF: 27 patients). Four patients experienced symptomatic SVC restenosis, whereas 10 other patients encountered stenosis of other central vein segments that required intervention. Cuffed catheter malfunction occurred in 20 patients, who were treated with urokinase locking, interventional angioplasty/catheter adjustment, and antibiotics accordingly. The AVF malfunction occurred in 15 patients, who were treated with thrombolysis, percutaneous transluminal angioplasty, or open thrombectomy. The overall 2-year vascular access patency rate was 33.2% (standard error of the mean: 0.07) (cuffed catheter: 22.2%, AVF: 41.7%, p=0.414). There was no statistically significant difference in the 2-year vascular access patency rate between the traditional recanalization group and the sharp recanalization group (34.1% vs 31.1%, p=0.731), as well as between patients who received bare metal stent and covered stent implantation (38.1% vs 21.4%, p=0.248) (Figure 2).
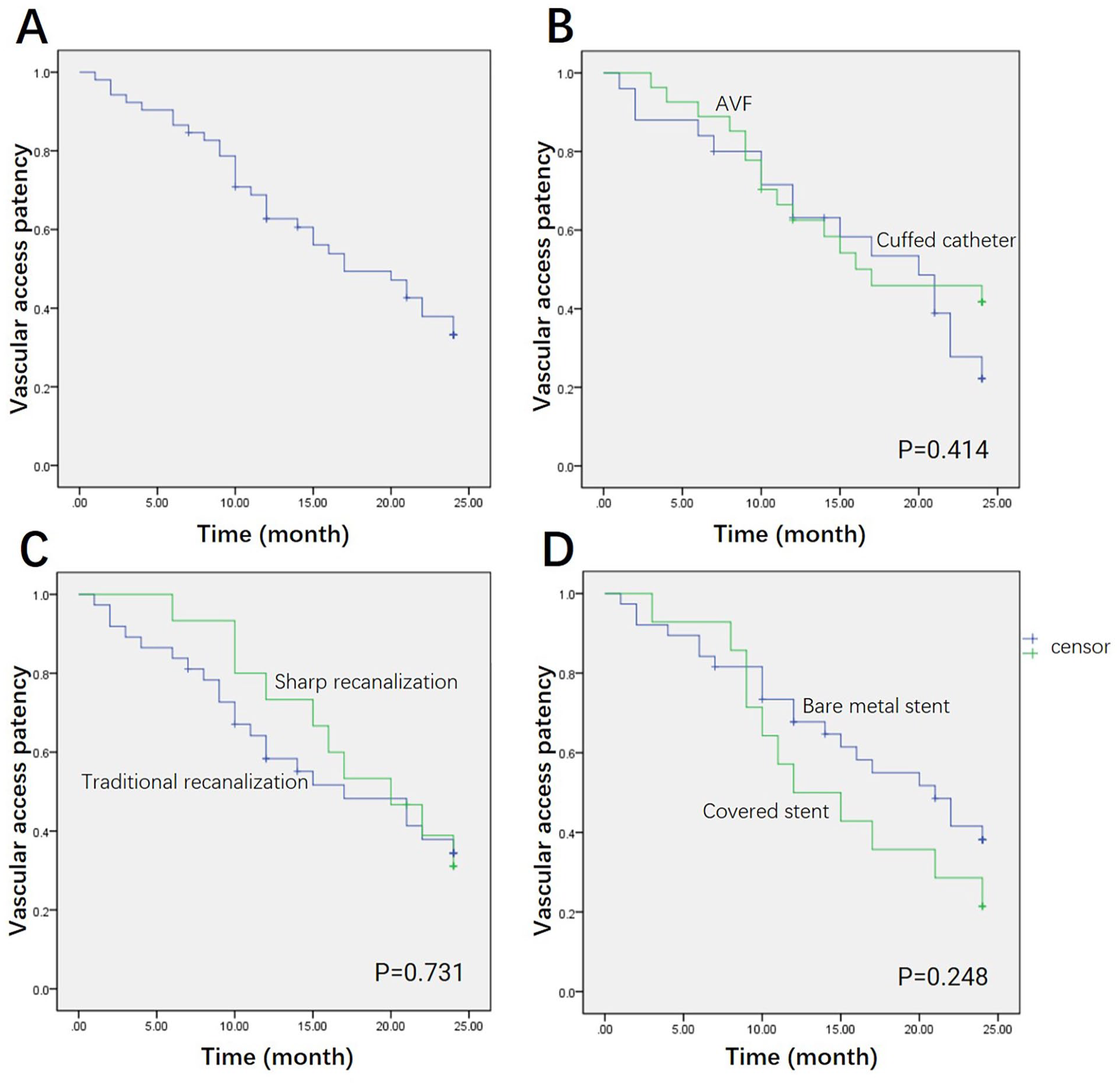
Kaplan-Meier survival analysis for vascular access patency. (A) Overall vascular access patency. (B) Cuffed catheter vs AVF. (C) Traditional recanalization vs sharp recanalization. (D) Bare metal stent vs covered stent. AVF: arteriovenous fistula.
Discussion
In this study of 58 hemodialysis patients with SVC stenosis, percutaneous SVC recanalization achieved a success rate of 91.38%, whereas stents were successfully placed in 52 patients, with a stent placement success rate of 98.1%. The 2-year vascular access patency rate of the patients was 33.2%. There was no statistically significant difference in 2-year vascular access patency rate between patient groups with regard to traditional recanalization and sharp recanalization, or bare metal stent and covered stent. This study suggests that percutaneous SVC recanalization with stent placement is an effective treatment strategy that can provide satisfactory vascular access for maintenance hemodialysis patients with SVC stenosis.
The SVC is formed by the left and right brachiocephalic veins that join behind the first rib juncture, which drains right anterior to the upper mediastinum into the right atrium. 7 The SVC stenosis is a common type of central venous stenotic disease in hemodialysis patients, especially among those who are dialyzed through a central venous catheter, 8 resulting in insufficient dialysis dosage and poor prognosis. 9 Traditionally, open surgery is the classic treatment for SVC stenosis. In recent decades, percutaneous angioplasty has become the mainstream therapeutic option. 4 The guideline recommendation for stent placement in treating central venous stenosis (CVS) is for refractory symptomatic lesions, especially within 3 months and those exhibiting elastic recoil. 10 Stents prevent elastic rebound following interventional angioplasty with balloon dilation and maintain vein patency. 11 It does not only improve short- and long-term outcomes, but also hemodialysis access longevity. Self-expanding stents was shown to be superior to angioplasty alone in managing elastic lesions. 12 The success rate for stent implantation is between 92% and 95%, which echoes the findings in our research.
Bare metal stents had been widely used to secure vessel patency following sharp recanalization in CVS, especially when over-dilation is needed. However, given the aggressive nature of neointimal hyperplasia, tissue might emerge through the bare strut area, which limits the use of bare metal stent in CVS. Therefore, more recent guidelines did not suggest the use of bare metal stent in hemodialysis patients. 13 In a retrospective study of 77 patients, Akkakrisee and Hongsakul 14 found that the 12-month primary vascular access patency of dedicated venous stents was better than bare metal stents (61.8% vs 32.6%; p=0.008). Another kind of widely-used stents, covered stents, have established their role in the treatment of re-stenotic lesions and in the rescue of vascular laceration during balloon dilation. The SIR guidelines do not differentiate between bare metal stent and covered stent for the treatment of CVS, 15 whereas size availability is the major limitation of covered stent’s suitability in the management of CVS. In this study, patients using bare metal stent and covered stent showed a similar 2-year vascular access patency rates. Dedicated research is needed to compare bare metal stent and covered stent in both vascular access patency and patient prognosis among hemodialysis patients.
As the SVC is surrounded by various organs, including trachea, aorta, pulmonary artery, right lung, and pericardial reflection, practitioners should be well aware of the risk of possible procedure-related complications. The stent implantation associated complications were reported to vary between 2% and 5%. 4 In our study, 1 patient suffered stents migration into right atrium and pericardium tamponade, which required thoracotomy and surgical repair of SVC laceration. In hemodialysis patients with CVS, the deformity of central venous system could result in a poor vein-stent apposition, thus promoting stent migration. In hemodialysis patients with a working AVF, the high-volume blood flow also contributes as a driving force for stent migration. Regarding operator error, under-sizing of stents is the most cause for stent migration. 16 Careful measurement of central veins is essential for the selection of stents with proper length and diameter. It is also worth mentioning that, the calcified or fibrotic SVC is particularly prone to laceration during balloon dilation. A compromise sometimes might need to be made between adequate stent size and risk of vessel laceration. Strict eligibility screening and skillful operation are important in minimizing the potential risk of adverse events. As per our observation, other adverse effects were mild ones (chest pain) which were successfully relieved by oral NSAIDs treatment.
Sharp recanalization is a method of forced crossing of CVS when the occlusive lesion cannot be treated with blunt guidewire technique. The procedure is usually performed with the use of a sharp needle or other hard objects to cross the stenosis from one side toward the targeting device on the other side, such as a balloon catheter or a snare. Repeated orthogonal fluoroscopic views to verify positioning are the most important step to guarantee safety. After the crossing step, graded dilation using balloons of increasing diameter is performed followed by venograms to rule out extravasation. Researchers previously reported that sharp recanalization was effective in managing SVC and brachiocephalic vein occlusion in hemodialysis patients, with a success rate ranging from 87.5% to 100%.5,17 In this study, we further found that SVC sharp recanalization with subsequent stent implantation was a feasible strategy, whereas the 2-year vascular access patency rates between the traditional recanalization group and the sharp recanalization group were comparable.
The limitations of our study were as follows. First, this was pilot, single-arm research with a small sample size. Our observation is to be further verified by studies involving more patients. Second, some of the patients in our cohort did not receive regular follow-up imaging tests, the estimation of their vascular access patency based on clinical assessments. Moreover, due to the complex relation between in-stent restenosis and catheter/fistula clotting in hemodialysis patients, we reported overall vascular access patency rates rather than stent patency rates. Third, the lack of a control group without stenting makes it impossible to compare the efficacy and safety of stenting versus no-stenting strategy following SVC recanalization. Prospective controlled studies are needed to investigate the advantages and disadvantages of different therapeutic options for SVC stenosis.
In conclusion, percutaneous SVC recanalization with stent placement is an effective treatment strategy that can provide viable vascular access for maintenance hemodialysis patients with SVC stenosis. Endovascular SVC recanalization should be performed with caution to avoid potential life-threatening complications such as stent displacement and cardiac tamponade. Dedicated controlled studies are warranted to compare different therapeutic strategies, such as stenting vs non-stenting, bare metal stent or covered stent, traditional vs sharp recanalization, on both access patency and patient prognosis among hemodialysis population with CVS.
Footnotes
Author Contributions
Y.Z. contributed to conceptualization and data collection. C.L. contributed to data analyses. W.W. contributed to manuscript writing. T.C. contributed to supervision. All co-authors contributed to writing review/editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Key Research and Development Program of China (2023YFC2411800), Science and Technology Department of Sichuan Province (2024YFHZ0329), “From 0 To 1” Innovation Research Project of Sichuan University (2023SCUH0065), and 135 Project for Disciplines of Excellence, West China Hospital, Sichuan University (2020HXFH014). The funding sources had no involvement in the manuscript.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Consent for Publication
Consent for publication was obtained for every individual person’s data included in the study.