
Abstract
Purpose:
Prevalence of abdominal aortic aneurysms (AAAs) increases with age. Previous trials confirm that elective endovascular aneurysm repair (EVAR) is an effective intervention for AAA. However, few elderly patients were recruited into randomized trials, whereas in contemporary clinical practice, elective repair is commonly performed on octogenarians. We evaluated the safety and outcome of elective EVAR in elderly patients to inform clinical practice and vascular service provision.
Methods:
A systematic review and meta-analysis of studies reporting risk of complications and death in patients undergoing elective EVAR was performed (PROSPERO CRD: 42022308423). Observational studies and interventional arms of randomized trials were included if the outcome rates or raw data were provided. Primary outcome was 30-day mortality. Secondary outcomes were longer-term mortality, 30-day major adverse events, and aneurysm-related mortality. Primary and secondary outcomes were compared between octogenarians and non-octogenarians. Exclusion criteria were emergency procedures, non-infrarenal aneurysms, and lack of octogenarian data.
Results:
A total of 41 studies were eligible from 10 099 citations, including 10 national and 5 international registries, 26 retrospective studies, and our own prospective cohort. The analysis included 208 997 non-octogenarians (mean age=70.19 [SD=0.62]) and 106 188 octogenarians (mean age=83.75 [SD=0.35]). The 30-day mortality post-elective EVAR was higher in octogenarians (1.08% in non-octogenarians, 2.31% in octogenarians, odds ratio [OR]=2.27 [2.08-2.47], p<0.0001). Linear regression demonstrated a 0.83% increase in 30-day mortality for every 10-year age increase above 60 years old. Mortality for octogenarians increased significantly during follow-up: 11.35% (OR=1.87 [1.65-2.13], p<0.001), 22.80% (OR=1.89 [1.52-2.35], p<0.001), 32.00% (OR=1.98 [1.66-2.37], p<0.001), 47.53%, and 51.08% (OR=2.40 [1.90-3.03], p<0.001) at 1-through-5-year follow-up, respectively. The 30-day major adverse events after elective EVAR were higher in octogenarians (OR=1.75-2.83, p<0.001).
Conclusions:
Octogenarians experience higher but acceptable peri-operative morbidity and mortality compared with younger patients. However, 3-year to 5-year survival is very low among octogenarians. Our findings challenge the notion of routine intervention in elderly patients and support very careful selection for elective EVAR. Many octogenarians with peri-threshold (<6 cm) AAAs may derive no benefit from EVAR due to limited 3-year to 5-year overall survival and low risk of aneurysm rupture with conservative management. An adjusted threshold for intervention in octogenarians may be warranted.
Clinical Impact
Octogenarians with infra-renal AAA are increasingly managed with elective EVAR. Previous studies have demonstrated that EVAR is safer than open repair for octogenarians, with lower peri-operative mortality and major adverse events. However, randomised trials, on which much of contemporary evidence is based, recruited a relatively younger population of participants. This systematic review and meta-analysis provides a contemporary synthesis of the literature comparing outcomes in octogenarians to younger patients. The results of this analysis, together with low rupture rates amongst octogenarians in existing literature, question the benefit of routine elective intervention for peri-threshold aneurysms and an adjusted threshold for intervention in octogenarians may be warranted.
Keywords
Introduction
Abdominal aortic aneurysms (AAAs) are increasingly a disease of the elderly, particularly in the aging population. Elective aneurysm repair, performed in asymptomatic patients, aims to avoid the often-fatal complication of aneurysm rupture, but repair itself carries significant associated morbidity and mortality. Randomized control trials have demonstrated that endovascular aneurysm repair (EVAR) has a similar short-to-medium-term efficacy to open repair, but with reduced peri-operative morbidity and mortality. 1 In the elderly, EVAR is regarded as the more suitable treatment option, with amplified reductions in peri-operative mortality and complications compared with open repair among this age group.2,3 However, in the landmark trials demonstrating the efficacy of EVAR, mean age of randomized patients was between 69 and 74 years old, 4 - 7 likely under-representing over 80-year-olds who now make up a significant proportion of EVAR procedures.
All-cause mortality increases in frequency with age, with non-aneurysm mortality outweighing mortality from rupture. 8 Elective EVAR is performed on asymptomatic patients and does not give long-term improvement in quality of life, 9 with reduced quality of life in the event of complication. 10 Furthermore, the recovery period following EVAR is prolonged for octogenarians with short-term and medium-term outcomes carrying greater consequence. 11 Thus, this brings into question whether the benefits of EVAR seen in younger patients translate into the elderly population. This systematic review and meta-analysis was performed to evaluate outcomes after elective EVAR in the octogenarian population and compare these with younger patients.
Methodology
The data that support the findings of this publication are available from the corresponding author on reasonable request.
Search Strategy and Selection Criteria
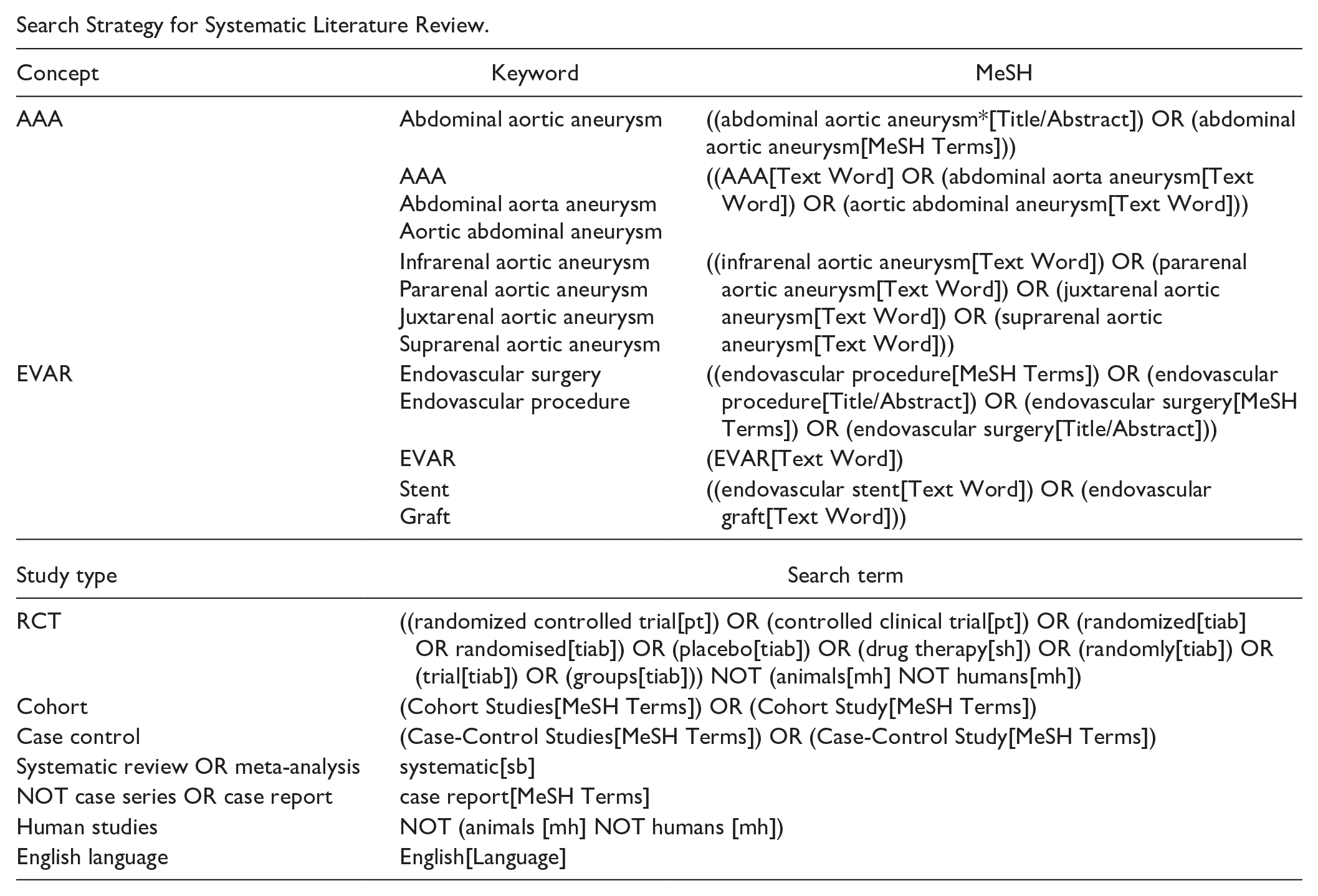
A systematic review and meta-analysis (PROSPERO ID: CRD42022308423) of studies reporting post-EVAR mortality in patients with non-ruptured infrarenal AAA, with reference to patients over 80 years of age, was performed. The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) and Meta-Analysis of Observational Studies in Epidemiology (MOOSE) reporting guidelines were followed throughout (Supplemental Table S1 and Figure 1). We performed a literature search through major databases (MEDLINE, Embase, CENTRAL, and Clinical trials.gov) from their inception to May 2024, with limits to English language papers, to identify relevant studies. A predetermined search strategy using combinations of search terms for infrarenal AAA, EVAR, and elderly patients was employed (Appendix); terms were amended in line with specific search features of each database. The results of each search were imported into Rayyan.ai software, which was used for duplicate removal and screening. Automated duplicate removal was checked by independent review (S.V.-B. and F.K.). Prospective and retrospective cohort studies and randomized control trials reporting outcomes after elective EVAR were included. Studies were included if post-EVAR mortality was reported for at least 1 of short-term (30-day) or longer-term (1, 2, 3, 4, 5 years). Studies were excluded if they did not differentiate between elective, urgent, and ruptured procedures, if they did not differentiate between infrarenal and juxtarenal or suprarenal aneurysms, if they did not report outcomes separately for standard infrarenal and complex endovascular procedures, or if they did not include octogenarian data. In cases of multiple reports from the same population, the last published study reporting relevant data was included. Two independent reviewers (S.V.-B. and F.K.) screened titles and abstracts of studies to determine whether the studies met inclusion criteria. Full-text eligibility was performed on screened first-round publications. Discrepancies in abstract screening were resolved by full-text review and, if still present, by a third investigator (Y.Y.R.L.). Agreement between observers in assessment of study eligibility was very high (99%; kappa=0.84; SE=0.09; p<0.001). Data extraction was performed on publications that passed both rounds of screening (S.V.-B. and Y.Y.R.L.) and tabulated in a standardized Excel file. Data were manually collected to record first author, year of publication, study design, study setting, study population, patient demographics, and relevant outcome measures. A Newcastle-Ottawa score was calculated for each study (Supplemental Table S2). For the purposes of this analysis, no attempts were made to contact authors for further or missing data.
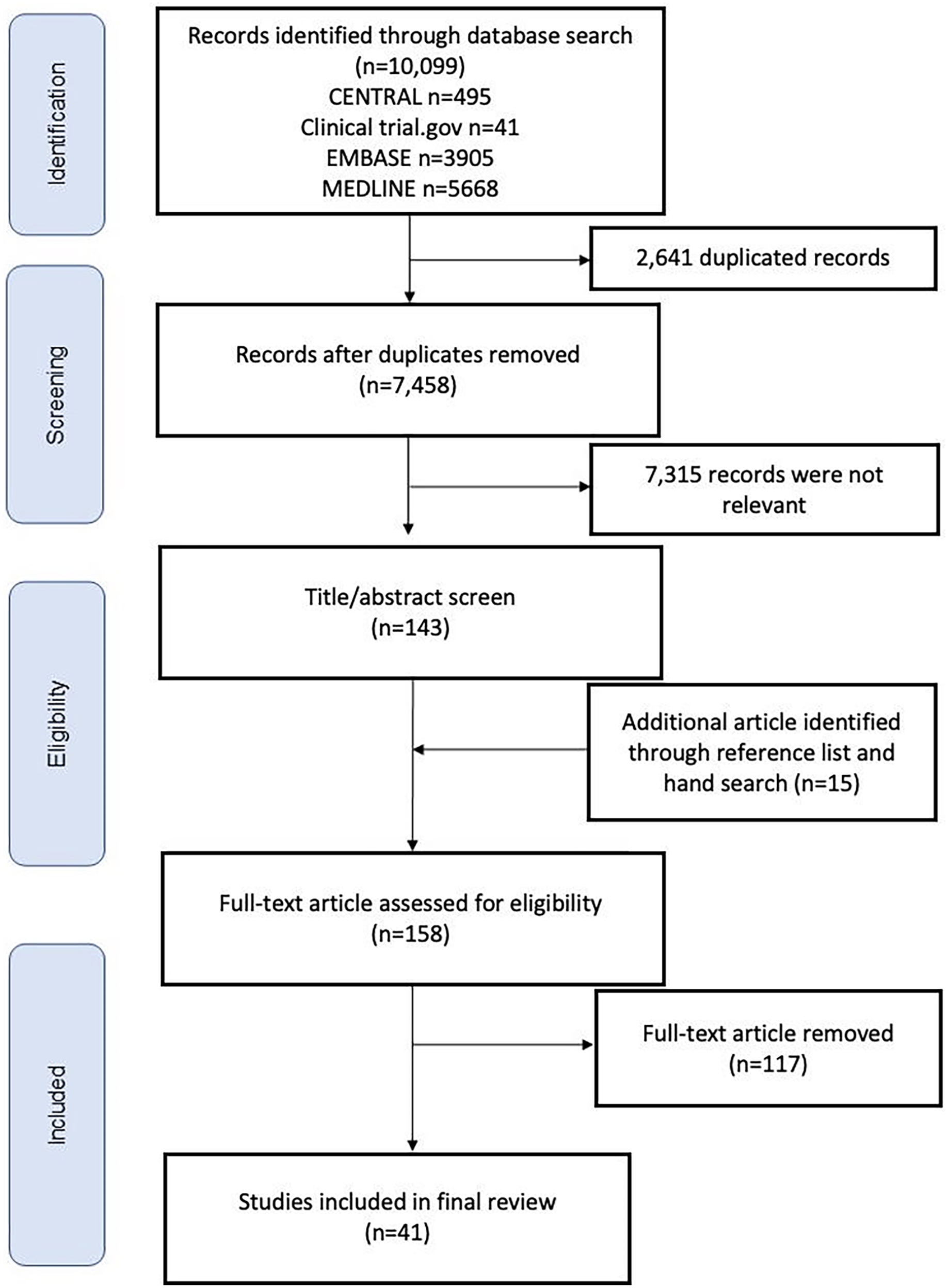
PRISMA diagram.
Outcomes and Definitions
The primary outcome was 30-day post-operative mortality. Secondary outcomes were long-term post-operative mortality (reported at 1, 2, 3, 4, and 5 years), long-term aneurysm-related mortality, and 30-day post-operative major adverse events (defined as pooled adverse cardiac events [myocardial infarction, angina, and arrythmia], myocardial infarction alone, pulmonary complications, renal complications, and cerebrovascular events). Major adverse events not reported in line with existing standards 12 or not reported individually were excluded. The 30-day and long-term post-operative mortalities were reported as percentages. Where available, the raw data were used to calculate these if not reported directly.
Statistical Analysis
Statistical analysis was performed using the Review Manager software version 5.4, The Cochrane Collaboration, 2020. Meta-analysis was performed using Mantel-Haenszel random effects statistical methods. Effect measures were calculated as odds ratios (ORs). Study and total confidence intervals are reported at 95%. The pooled analysis was stratified by patient age under 80 years (referred to as non-octogenarians or younger patients) and over 80 years (referred to as octogenarians). Assessment of heterogeneity was performed using Cochran’s Q test and an I2 statistic calculated for each analysis. Within the systematic review, weighted means and standard deviations are reported. p-values were considered significant at <0.05 throughout. Confidence intervals are presented as 95% throughout unless stated otherwise.
Results
The literature search yielded 10 099 citations (including 2641 duplicates), from which 41 papers were eligible for inclusion. Hand-searching of reference lists was performed but did not yield any further articles for inclusion. The studies included were 26 retrospective studies (22 single centers, 4 multicenters), 10 national registries, and 5 international registries. 13 - 53 A total of 35 studies included patients undergoing elective AAA repair only, and 6 studies included all unruptured, non-emergency AAA repairs. Most of the cohorts were from North America (n=20) and Europe (n=13), with 5 international and 3 from Asia. In addition, from our own institution, the Thames Valley Vascular Network (TVVN), prospective individual patient-level registry data with long-term outcome were included. The year of publication, data collection period, country of study, study design, and number of participants are shown in Supplemental Table S3.
Data from 208 997 non-octogenarians (mean age=70.19 [SD=0.62]) and 106 188 octogenarians (mean age=83.75 [SD=0.35]) were included in the analysis. Where reported, octogenarians were less frequently male (79.88% [79.64%-80.12%] vs 89.36% [89.23%-89.49%]; p<0.001) and the mean aneurysm size was larger in octogenarians (59.75 mm [SD=2.53]) than non-octogenarians (57.58 mm [SD=1.51]; p<0.001) (Supplemental Table S3). A summary of comorbidities, where reported, is included in the Supplementary Material (Supplemental Table S4).
Thirty-Day Post-operative Mortality
Systematic review included 36 studies reporting 30-day post-operative mortality after elective EVAR in octogenarians, and prospective data from TVVN were included, yielding data from 84 409 octogenarians. Five studies did not report 30-day post-operative mortality so were not included. Risk of 30-day post-operative mortality including all data for octogenarians was 2.21% (2.10%-2.29%) (Table 1). Data from 281 372 patients (21 studies and prospective data from TVVN), including 72 689 octogenarians and 208 683 non-octogenarians, were included in the meta-analysis of peri-operative mortality. Risk of 30-day post-operative mortality was 1.40% (1.36%-1.44%) overall, and 1.08% (1.04%-1.13%) in non-octogenarians (2256 events in 208 683 patients) vs 2.31% (2.20%-2.42%) in octogenarians (1679 events in 72 689 patients), demonstrating higher mortality in octogenarians with OR=2.27 [2.08-2.47, p<0.0001] (Figure 2). Sub-analysis was performed with regard to study type, and the results were found to be similar when comparing registries (OR=2.27 [2.06-2.49, p<0.0001]) and cohort studies (OR=2.34 [1.76-3.10], p<0.0001) (Supplementary Figure 1a and b).
Systematic Review of 30-Day and Longer-Term Post-Operative Mortality Risk for Octogenarians.

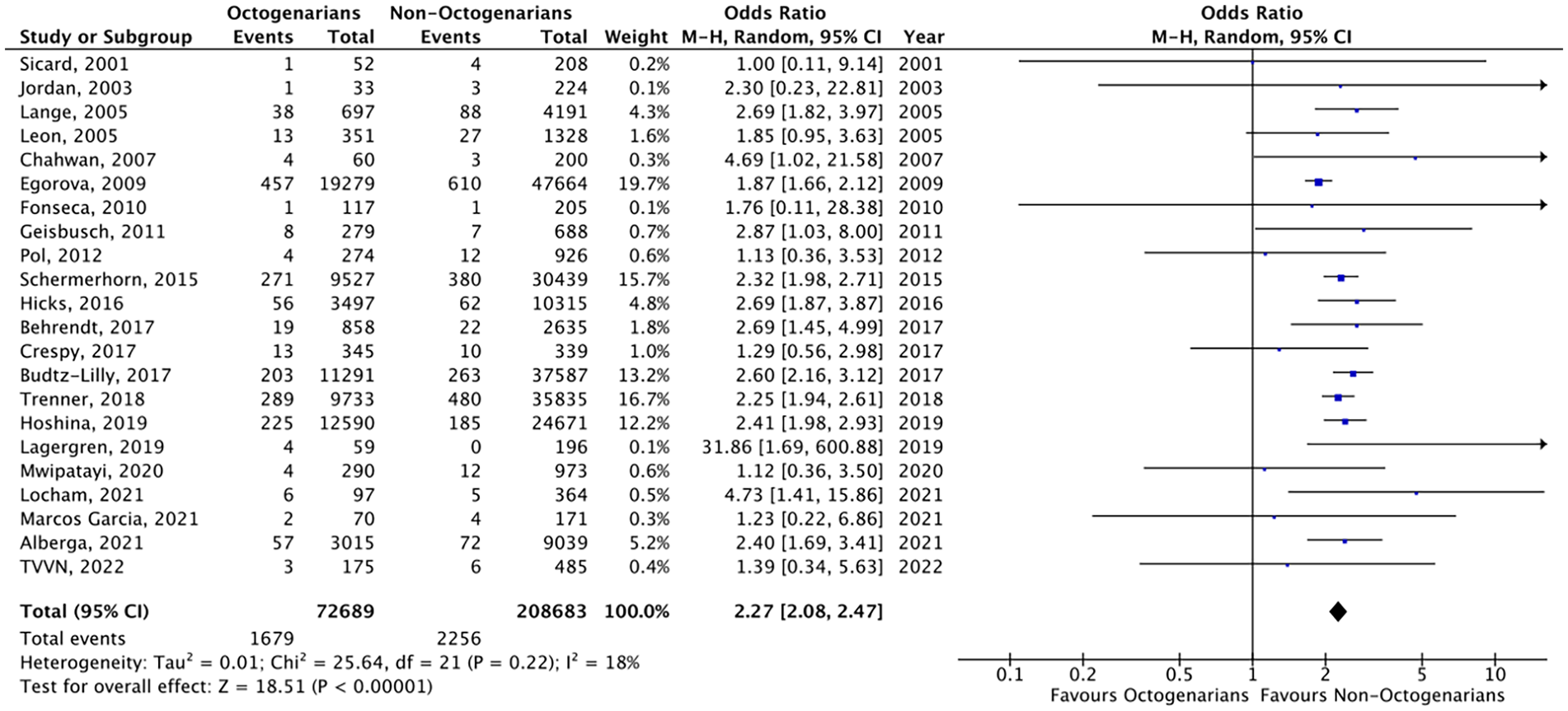
Meta-analysis of 30-day post-operative mortality risk, stratified by age cut-off of 80 years.
Using publicly available data, 54 we have attempted to account for the expected background 30-day mortality in each age group. The population baseline 30-day mortality was 0.17% for non-octogenarians and 0.65% for octogenarians. When adjusted, the risk of 30-day post-operative mortality was 1.11% (1.07%-1.15%) overall and 0.92% (0.88%-0.96%) in non-octogenarians (1911 excess events in 208 294 patients) vs 1.65% (1.56%-1.75%) in octogenarians (1194 excess events in 72 213 patients). There remained a significantly higher 30-day post-operative mortality despite the correction for expected baseline mortality [X2 (2, N=280 507)=265.34, p<0.0001].
Five age-stratified studies (181 386 patients) revealed a linear relationship between 10-year increase in age (60-69, 70-79, and >80) and 30-day post-operative mortality risk. Among these studies, risk of 30-day post-operative mortality was 0.78% (0.69%-0.89% [32 196 patients]) in the 60- to 69-year-old age group, 1.39% (1.32%-1.47% [98 186 patients]) in the 70- to 79-year-old age group, and 2.44% (2.31%-2.58% [51 004 patients]) in the over 80-year-old age group [X2 (2, N=181 386)=500.81, p<0.0001]. Comparing 70 to 79 years to over 80 years olds yielded OR=1.86 [1.66-2.09, p<0.0001] and comparing 60 to 69 years and over 80 years olds yielded OR=3.32 [2.72-4.02, p<0.0001] (Figure 3A and B). For each decade increase, there was a 0.83% increased risk of 30-day post-operative mortality (p=0.098).
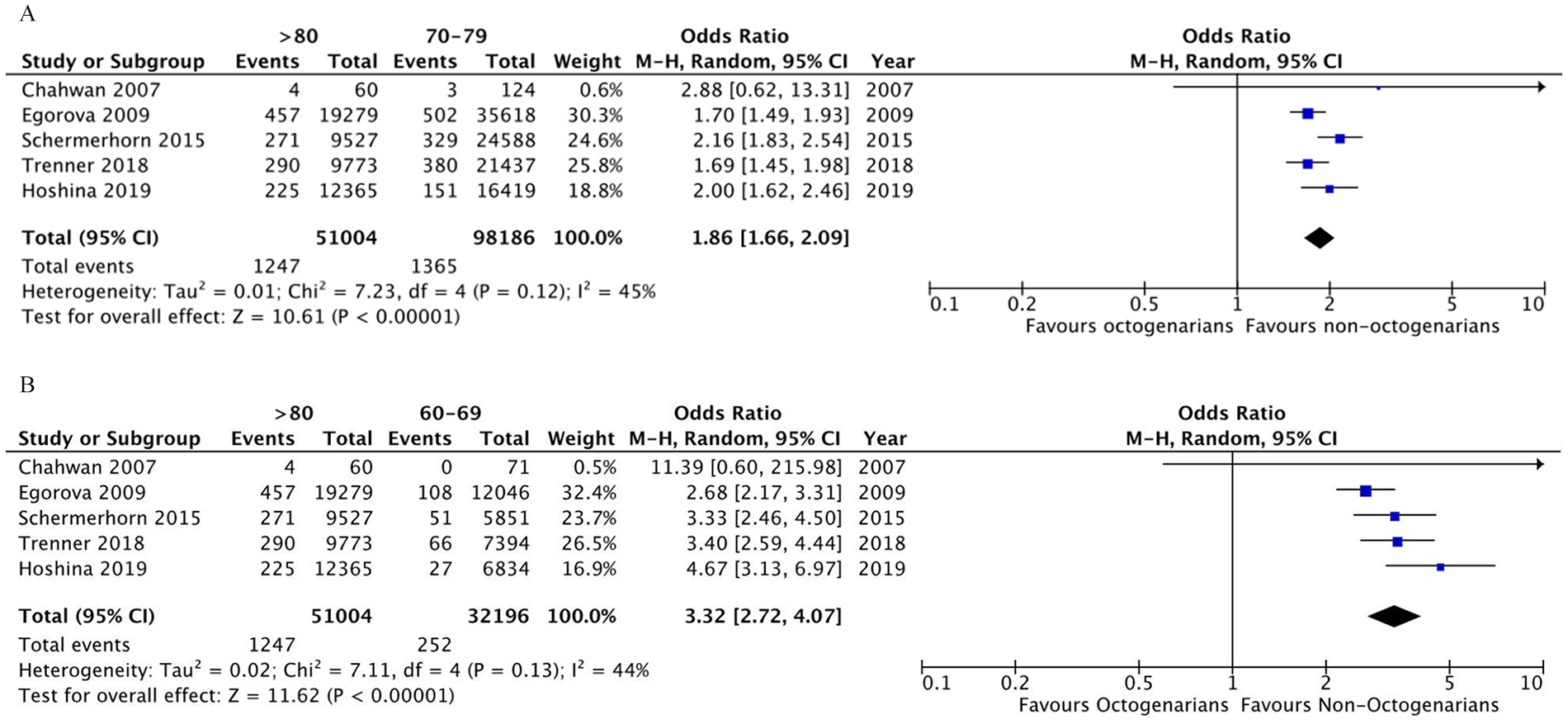
Meta-analysis and pooled estimate of 30-day post-operative mortality risk in age-stratified studies using cut-offs 60 to 69 and 70 to 79 and compared to >80: (A) 70 to 79 vs >80 and (B) 60 to 69 vs >80.
Across all studies, the pooled estimate of 30-day post-operative mortality risk decreased across the periods of analysis overall, from 1.67% (1.58%-1.76% [76 776 patients]) prior to 2015 to 1.30% (1.25%-1.35% [204 596 patients]) from 2015 onwards [X2 (1, N=281 372)=56.35, p<0.0001]. The 30-day post-operative mortality risk significantly decreased in non-octogenarians, 1.36% [1.26%-1.46%] to 0.98% [0.93%-1.03%], X2 (1, N=208 683)=54.04, p<0.0001, and to a lesser extent in octogenarians, 2.49% [2.29%-2.71%] to 2.23% [2.11%-2.37%], X2 (1, N=72 689)=4.41, p=0.036.
Long-term All-Cause Mortality
Long-term all-cause mortality data were reported at 1, 2, 3, 4, and 5 years post-elective EVAR. Several studies reported on follow-up longer than 5 years; however, these were single studies at each time point and therefore not included in the analysis due to lack of comparison. Systematic review of longer-term all-cause mortality for octogenarians was at 1 year 9.61% (9.35%-9.87% [22 studies, 48 900 octogenarians]), at 2 years 15.55% (14.88%-16.23% [13 studies, 11 153 octogenarians]), at 3 years 28.83% (26.47%-31.22% [11 studies, 1434 octogenarians]), at 4 years 41.65% (37.72%-45.58% [4 studies, 601 octogenarians]), and at 5 years 51.27% (49.29%-53.26% [15 studies, 2426 octogenarians]) (Table 1). Meta-analysis was performed at 1, 2, 3, and 4 years post-elective EVAR comparing octogenarians to non-octogenarians. Meta-analysis was not performed at 4 years post-elective EVAR due to no studies reporting 4-year data in the non-octogenarian group. Risk of 1-year all-cause mortality was 7.74% (7.53%-7.95%) overall (60 370 patients) and 6.20% (5.98%-6.44%) in non-octogenarians (2629 events in 42 377 patients) vs 11.35% (10.90%-11.83%) in octogenarians (2043 events in 17 993 patients), with OR=1.87 [1.65-2.13, p<0.0001] (Figure 4A). Across the studies, 1-year all-cause mortality risk significantly decreased from prior to 2015 compared with 2015 onwards in non-octogenarians, 7.21% [6.54%-7.94%] to 6.06% [5.82%-6.31%], X2 (1, N=42 377)=10.54, p=0.001, and in octogenarians, 12.01% [10.54%-13.66%] to 10.17% [9.81%-10.55%], X2 (1, N=27 384)=5.76, p=0.016. Risk of 2-year all-cause mortality was 15.71% (14.39%-17.12%) overall (2725 patients) and 13.01% (11.60%-14.57%) in non-octogenarians (257 events in 1975 patients) vs 22.80% (19.94%-25.94%) in octogenarians (171 events in 750 patients), with OR=1.89 [1.52-2.35, p<0.0001] (Figure 4B). Risk of 3-year all-cause mortality was 21.88% (20.49%-23.34%) overall (3226 patients) and 18.14% (16.63%-19.75%) in non-octogenarians (427 events in 2354 patients) vs 32.00% (28.98%-35.16%) in octogenarians (279 events in 872 patients), with OR=2.01 [1.67-2.40, p<0.0001] (Figure 4C). Risk of 5-year all-cause mortality was 36.94% (35.35%-38.56%) overall (3468 patients) and 30.23% (28.41%-32.12%) in non-octogenarians (711 events in 2352 patients) vs 51.08% (48.14%-54.00%) in octogenarians (570 events in 1116 patients), with OR=2.40 [1.90-3.03, p<0.0001] (Figure 4D). A single study (Fonseca et al 24 ) was excluded from the meta-analysis beyond 1-year mortality due to exceptionally low reported long-term mortality.
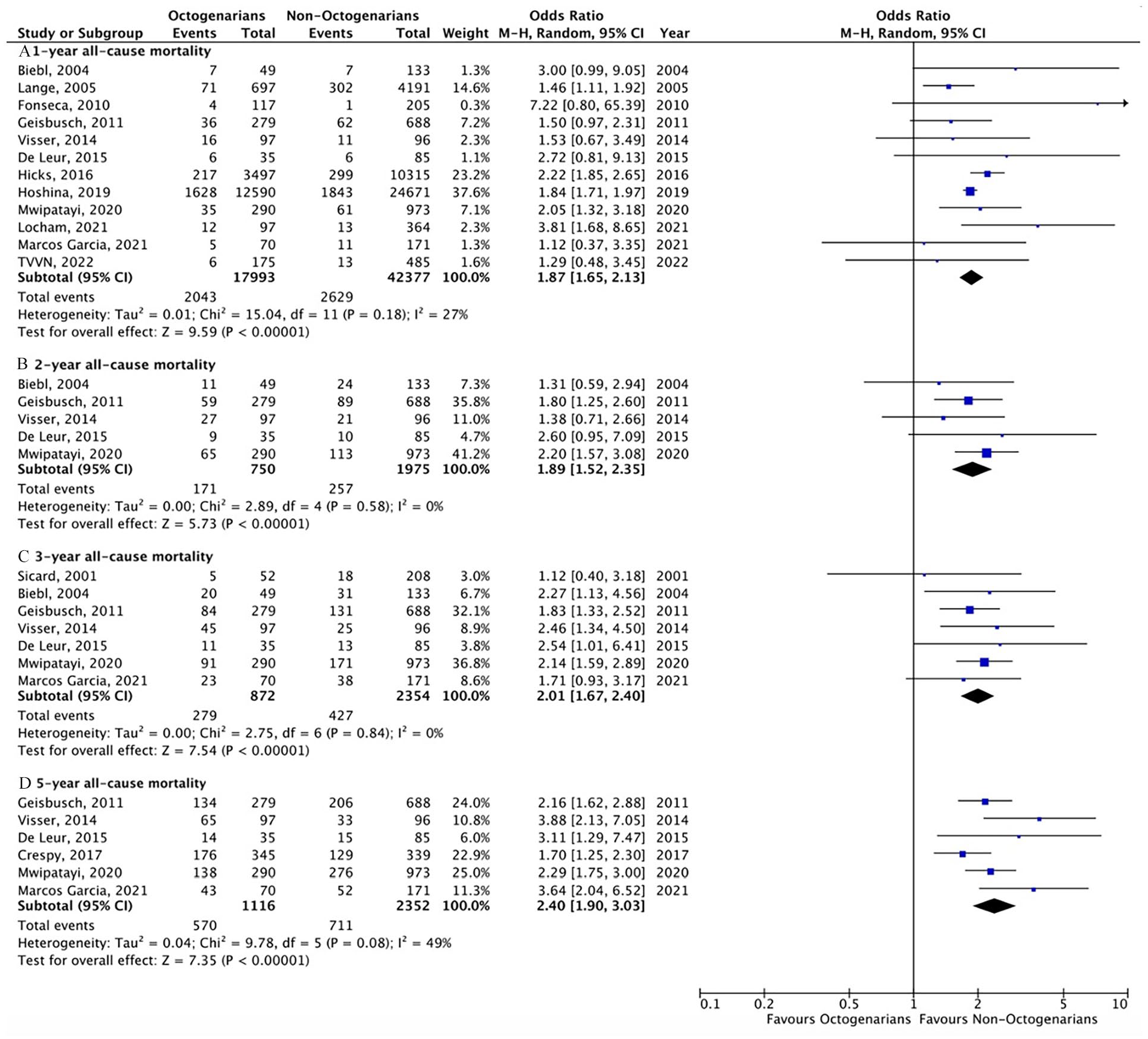
Meta-analysis of 1, 2, 3, and 5 year post-elective EVAR all-cause mortality, stratified by age cut-off of 80 years: (A) 1 year; (B) 2 years; (C) 3 years, and (D) 5 years.
Thirty-Day Post-elective EVAR Major Adverse Events
The 30-day post-elective EVAR major adverse events were collected, where reported, across all studies. Owing to heterogeneous reporting of outcomes across the studies, data were only collected where clearly presented and defined in line with previous reporting standards. 12 Systematic review of 30-day post-elective EVAR complications in octogenarians revealed the risk of unspecified cardiac complications was 4.09% (3.58%-4.65% [13 studies, 5263 octogenarians]), myocardial infarction was 1.96% (1.62%-2.38% [7 studies, 5144 octogenarians]), cerebrovascular event was 1.93% (1.56%-2.38% [14 studies, 4356 octogenarians]), renal dysfunction was 3.49% (3.13%-3.90% [19 studies, 8875 octogenarians]), and respiratory dysfunction was 2.52% (2.21%-2.87% [18 studies, 8805 octogenarians]) (Supplemental Table S5). Meta-analysis was performed for individual complications comparing octogenarians to non-octogenarians. Risk of 30-day unspecified cardiac complication was 4.31% (3.96%-4.69%) overall and 3.64% (3.28%-4.04%) in non-octogenarians (342 events in 9392 patients) vs 6.84% (5.91%-7.89%) in octogenarians (171 events in 2501 patients), with OR=2.51 [1.54-4.09, p=0.0002] (Figure 5A). Risk of 30-day myocardial infarction was 1.19% (1.05%-1.35%) overall and 0.93% (0.79%-1.09%) in non-octogenarians (143 events in 15 383 patients) vs 1.96% (1.62%-2.38%) in octogenarians (101 events in 5144 patients), with OR=2.16 [1.67-2.80, p<0.0001] (Figure 5B). Risk of 30-day cerebrovascular event was 2.24% (1.95%-2.58%) overall and 1.85% (1.56%-2.20%) in non-octogenarians (129 events in 6963 patients) vs 3.95% (3.10%-5.02%) in octogenarians (63 events in 1594 patients), with OR=2.83 [2.07-3.86, p<0.0001] (Figure 5C). Risk of 30-day renal dysfunction was 2.64% (2.46%-2.84%) overall and 2.25% (2.05%-2.46%) in non-octogenarians (463 events in 20 596 patients) vs 3.98% (3.51%-4.50%) in octogenarians (242 events in 6084 patients), with OR=1.75 [1.49-2.05, p<0.0001] (Figure 5D). Risk of 30-day respiratory dysfunction was 1.90% (1.74%-2.07%) overall and 1.61% (1.44%-1.79%) in non-octogenarians (326 events in 20 269 patients) vs 2.87% (2.48%-3.32%) in octogenarians (177 events in 6170 patients), with OR=1.97 [1.45-2.68, p<0.0001] (Figure 5E).
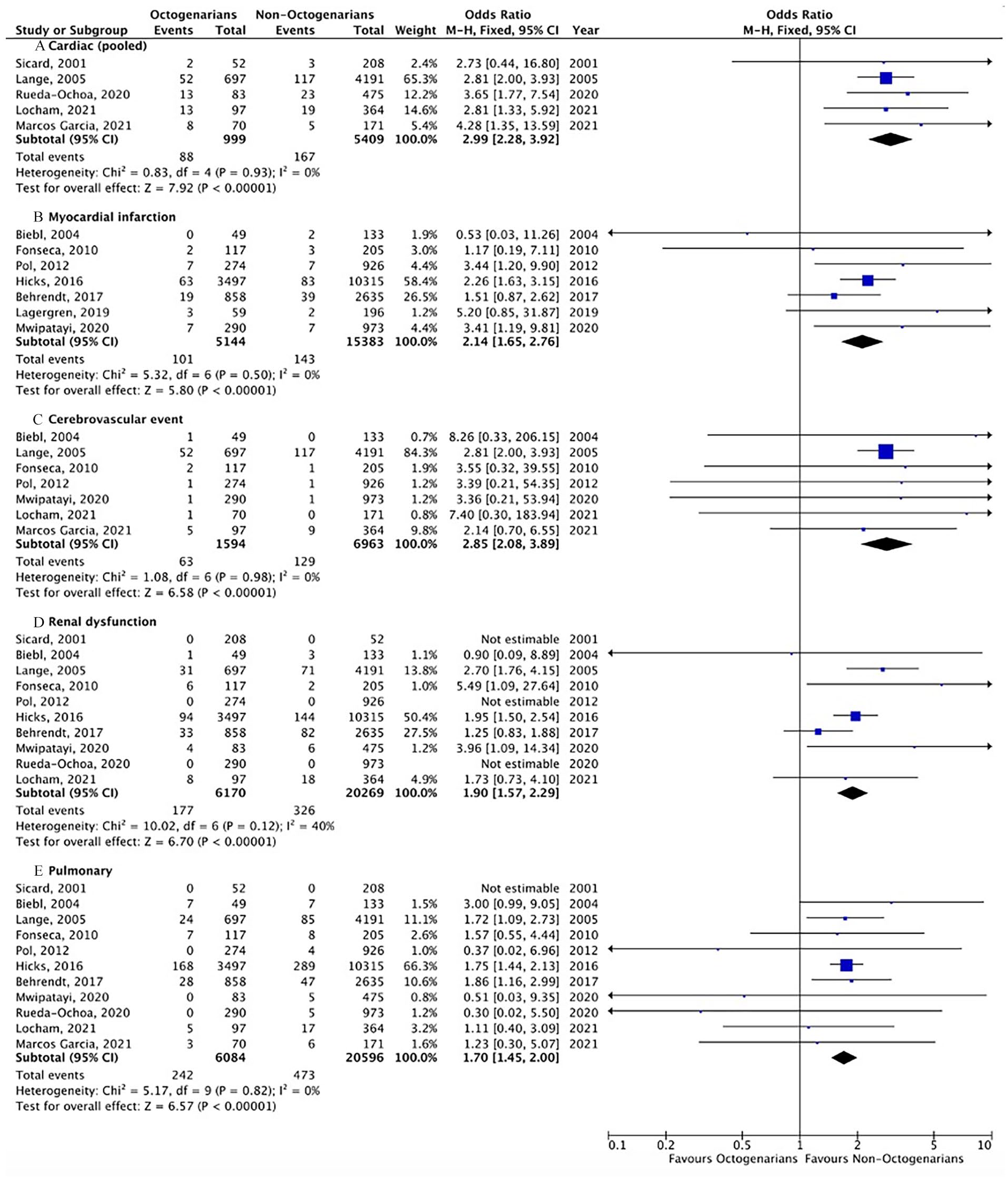
Meta-analysis of 30-day post-operative major adverse events, stratified by age cut-off of 80 years: (A) cardiac (pooled); (B) myocardial infarction; (C) cerebrovascular event; (D) renal dysfunction; and (E) pulmonary.
Five-Year Post-elective EVAR Aneurysm-Related Mortality
Systematic review identified 9 studies including 1599 octogenarians reporting on 5-year post-elective EVAR aneurysm-related mortality, with a risk of 2.23% (1.58%-3.10%). A single study (Prenner et al 25 ) reported an aneurysm-related mortality of 7.1% at 5 years, which when excluded from the analysis yielded a risk of 1.00% (0.54%-1.73%) in octogenarians (13 events in 1277 patients). A similar 5-year post-elective EVAR aneurysm-related mortality of 0.97% (0.63%-1.49%) was reported for non-octogenarians (20 events in 2062 patients). Owing to the paucity of events and reporting of data among the studies identified in the systematic review, only 33 events and 9 of 41 studies, the decision was made not to perform meta-analysis on these data. These data are in line with prior reports of 5-year elective EVAR outcomes and demonstrates that EVAR is durable in octogenarians and younger patients in the 5-year timescale.4-7
Discussion
This meta-analysis demonstrates that octogenarians undergoing elective EVAR suffer more frequent peri-operative morbidity and mortality than their younger counterparts. Despite management of their aneurysms and minimal long-term aneurysm-related mortality, octogenarians undergoing EVAR experience a 5-year all-cause mortality of over 50%. Octogenarians have experienced less improvement in outcomes over time compared with younger patients. These findings have important clinical implications.
First, the linear trend in increasing 30-day post-operative mortality with age agrees with the notion that, in addition to numerical age, frailty and comorbidity have important roles in determining post-operative outcomes.55,56 When comparing octogenarians and younger patients, the relative increased risk of peri-operative death is significant, but the absolute increase per decade of age is marginal, agreeing with previous published data that EVAR is safe in the majority of patients across the spectrum of age with modest comorbidity.4-7
Second, despite advancements in peri-operative medicine 57 and EVAR techniques,58,59 improvements in 30-day post-operative mortality over time are modest in octogenarians compared with younger patients. This could be explained by patient selection in the octogenarian population, particularly after the results of the EVAR-2 trial which may have deterred surgeons from performing EVAR on very comorbid and elderly patients. 60 In support of this, our analysis finds that the prevalence of comorbidities in patients selected for EVAR is similar in octogenarians and younger patients, suggesting that the least comorbid octogenarians are being selected for EVAR.
Third, the combination of higher frequency of major adverse events and low 5-year aneurysm-related mortality suggests that morbidity is concentrated in the short-term for octogenarians. This finding is important in octogenarians’ decision-making, as life expectancy is shorter, and quality of life takes longer to recover in this population. 11 In addition, octogenarians are at higher risk of developing endoleaks61,62 that necessitate intervention to mitigate the risk of late rupture,63,64 and both ongoing surveillance 65 and intervention 66 impact quality of life. Considering together this increased burden from surveillance and re-intervention, longer time to recover quality of life, 11 and our finding of higher post-operative adverse events, octogenarians appear relatively more impacted by short-term adverse events than younger patients.
Finally, all-cause mortality in octogenarians is high, with over 50% of octogenarians not surviving beyond 5 years. This finding is fundamental in determining whether octogenarians derive benefit from EVAR. Octogenarians are typically considered for EVAR over open repair due to the significantly higher per-operative morbidity and mortality with an open approach in this population. 3 However, patients unfit for open repair have previously been demonstrated to not derive survival benefit from any intervention. 60 In keeping with this, meta-analysis demonstrates no difference in 36-month and 60-month survival between octogenarians undergoing EVAR or open repair, 3 suggesting that all-cause mortality is unchanged by the approach to aneurysm repair. In addition, in our analysis octogenarians undergoing EVAR do not reach life expectancy of the healthy population, 67 bringing into question which octogenarians will derive survival benefit from elective EVAR.
The incidence of rupture in untreated octogenarians strongly affects the application of the results of our meta-analysis. Historically, rupture rates were relatively high, particularly for large aneurysms. The EVAR-2 trial reported an incidence of 9.7 and 17.4 ruptures per 100 patient-years of follow-up for <6 and >6 cm aneurysm, respectively. 60 More recent meta-analyses suggest that the risk of rupture by AAA size is decreasing over time.8,68,69 One meta-analysis of 11 studies reported annual rupture rates of 3.5%, 4.1%, and 6.3% for 5.5 to 5.9 cm, 6.0 to 6.9 cm, and >7.0 cm aneurysms, respectively, 8 and a recent cohort study of 1033 patients 68 reported a 3-yearly rupture rate of 2.2%, 6.0%, and 18.4% for 5.5 to 6.0 cm, 6.1 to 7.0 cm, and >7.0 cm, respectively. AAA growth rates have been reported to be lowest among older patients. 70 In our analysis, mean aneurysm diameter was 5.9 cm. We have confirmed that following elective EVAR, 30-day mortality for octogenarians was 2.28%, and although long-term aneurysm-related mortality was low, 3-year all-cause mortality was over 30%. Therefore, when a 2% to 3% 3-year AAA rupture risk with conservative management is contemplated, elective intervention for octogenarians demands careful consideration and caution.
To determine which octogenarians may derive benefit from elective intervention will require individual patient data meta-analysis, allowing higher granularity analysis of the impact of comorbidities, which are likely, along with age, to contribute to adverse outcomes.
Limitations
Our analysis has several limitations that affect the ability to draw conclusions from these data. First, beyond 30-day mortality, there is increasingly infrequent reporting of mortality data and incomplete reporting of numbers at risk in the Kaplan-Meier data. Where numbers at risk are reported, there is substantial loss to follow-up, which could represent octogenarians who feel they are well enough not to require further follow-up. Second, reporting of data outside of mortality is inconsistent across studies. There is no consensus on reporting complications between studies, and therefore, it is impossible to be sure that all complications were captured in every study or that these classifications are the same across studies. Third, we have not compared data on EVAR-specific complications or re-intervention, for which there are 3 reasons: EVAR-specific complications and re-interventions were frequently reported relating to the whole study group and were not stratified by age; complications and re-interventions were reported at differing time points making them incomparable; and across the data collection period, the consensus on the management of endoleaks has changed such that across the studies, re-intervention rates would have varied independent of the age of patients. Fourth, earlier data will have been from surgeons and radiologists less familiar with EVAR, as the technology developed and became more widespread. However, despite these limitations, many patients in our study came from registries, which are generally considered most representative of underlying populations. Where compared, the results of registries alone were not significantly different from the population as a whole.
Conclusions
This meta-analysis provides an extensive review of the literature encompassing data from over 300 000 patients. The 30-day mortality is 2-fold higher after elective EVAR for octogenarians when compared with younger patients, and there is a linear increase in 30-day mortality with increasing age. Most octogenarians die of non–aneurysm-related causes, and all-cause mortality at 5 years is over 50%. For octogenarians, when considering the low risk of rupture in peri-threshold aneurysms managed conservatively, the high peri-operative morbidity and mortality, and the low 3-year to 5-year overall survival, the benefit of elective intervention is questionable. In particular, for octogenarians with peri-threshold aneurysms less than 6 cm in diameter, there may be no benefit derived from elective EVAR and a higher threshold for intervention may be warranted.
Supplemental Material
sj-docx-2-jet-10.1177_15266028241283669 – Supplemental material for The Safety and Outcomes of Elective Endovascular Aneurysm Repair in the Elderly: A Systemic Review and Meta-Analysis
Supplemental material, sj-docx-2-jet-10.1177_15266028241283669 for The Safety and Outcomes of Elective Endovascular Aneurysm Repair in the Elderly: A Systemic Review and Meta-Analysis by Sebastian Vaughan-Burleigh, Ya Yuan Rachel Leung, Faaraz Khan, Patrick Lintott and Dominic P. J. Howard in Journal of Endovascular Therapy
Supplemental Material
sj-docx-3-jet-10.1177_15266028241283669 – Supplemental material for The Safety and Outcomes of Elective Endovascular Aneurysm Repair in the Elderly: A Systemic Review and Meta-Analysis
Supplemental material, sj-docx-3-jet-10.1177_15266028241283669 for The Safety and Outcomes of Elective Endovascular Aneurysm Repair in the Elderly: A Systemic Review and Meta-Analysis by Sebastian Vaughan-Burleigh, Ya Yuan Rachel Leung, Faaraz Khan, Patrick Lintott and Dominic P. J. Howard in Journal of Endovascular Therapy
Supplemental Material
sj-docx-4-jet-10.1177_15266028241283669 – Supplemental material for The Safety and Outcomes of Elective Endovascular Aneurysm Repair in the Elderly: A Systemic Review and Meta-Analysis
Supplemental material, sj-docx-4-jet-10.1177_15266028241283669 for The Safety and Outcomes of Elective Endovascular Aneurysm Repair in the Elderly: A Systemic Review and Meta-Analysis by Sebastian Vaughan-Burleigh, Ya Yuan Rachel Leung, Faaraz Khan, Patrick Lintott and Dominic P. J. Howard in Journal of Endovascular Therapy
Supplemental Material
sj-docx-5-jet-10.1177_15266028241283669 – Supplemental material for The Safety and Outcomes of Elective Endovascular Aneurysm Repair in the Elderly: A Systemic Review and Meta-Analysis
Supplemental material, sj-docx-5-jet-10.1177_15266028241283669 for The Safety and Outcomes of Elective Endovascular Aneurysm Repair in the Elderly: A Systemic Review and Meta-Analysis by Sebastian Vaughan-Burleigh, Ya Yuan Rachel Leung, Faaraz Khan, Patrick Lintott and Dominic P. J. Howard in Journal of Endovascular Therapy
Supplemental Material
sj-pdf-1-jet-10.1177_15266028241283669 – Supplemental material for The Safety and Outcomes of Elective Endovascular Aneurysm Repair in the Elderly: A Systemic Review and Meta-Analysis
Supplemental material, sj-pdf-1-jet-10.1177_15266028241283669 for The Safety and Outcomes of Elective Endovascular Aneurysm Repair in the Elderly: A Systemic Review and Meta-Analysis by Sebastian Vaughan-Burleigh, Ya Yuan Rachel Leung, Faaraz Khan, Patrick Lintott and Dominic P. J. Howard in Journal of Endovascular Therapy
Supplemental Material
sj-tiff-6-jet-10.1177_15266028241283669 – Supplemental material for The Safety and Outcomes of Elective Endovascular Aneurysm Repair in the Elderly: A Systemic Review and Meta-Analysis
Supplemental material, sj-tiff-6-jet-10.1177_15266028241283669 for The Safety and Outcomes of Elective Endovascular Aneurysm Repair in the Elderly: A Systemic Review and Meta-Analysis by Sebastian Vaughan-Burleigh, Ya Yuan Rachel Leung, Faaraz Khan, Patrick Lintott and Dominic P. J. Howard in Journal of Endovascular Therapy
Footnotes
Appendix
Search Strategy for Systematic Literature Review.
| Concept | Keyword | MeSH |
|---|---|---|
| AAA | Abdominal aortic aneurysm | ((abdominal aortic aneurysm*[Title/Abstract]) OR (abdominal aortic aneurysm[MeSH Terms])) |
| AAA Abdominal aorta aneurysm Aortic abdominal aneurysm |
((AAA[Text Word] OR (abdominal aorta aneurysm[Text Word]) OR (aortic abdominal aneurysm[Text Word])) | |
| Infrarenal aortic aneurysm Pararenal aortic aneurysm Juxtarenal aortic aneurysm Suprarenal aortic aneurysm |
((infrarenal aortic aneurysm[Text Word]) OR (pararenal aortic aneurysm[Text Word]) OR (juxtarenal aortic aneurysm[Text Word]) OR (suprarenal aortic aneurysm[Text Word])) | |
| EVAR | Endovascular surgery Endovascular procedure |
((endovascular procedure[MeSH Terms]) OR (endovascular procedure[Title/Abstract]) OR (endovascular surgery[MeSH Terms]) OR (endovascular surgery[Title/Abstract])) |
| EVAR | (EVAR[Text Word]) | |
| Stent Graft |
((endovascular stent[Text Word]) OR (endovascular graft[Text Word])) | |
| Study type | Search term | |
| RCT | ((randomized controlled trial[pt]) OR (controlled clinical trial[pt]) OR (randomized[tiab] OR randomised[tiab]) OR (placebo[tiab]) OR (drug therapy[sh]) OR (randomly[tiab]) OR (trial[tiab]) OR (groups[tiab])) NOT (animals[mh] NOT humans[mh]) | |
| Cohort | (Cohort Studies[MeSH Terms]) OR (Cohort Study[MeSH Terms]) | |
| Case control | (Case-Control Studies[MeSH Terms]) OR (Case-Control Study[MeSH Terms]) | |
| Systematic review OR meta-analysis | systematic[sb] | |
| NOT case series OR case report | case report[MeSH Terms] | |
| Human studies | NOT (animals [mh] NOT humans [mh]) | |
| English language | English[Language] | |
Prior Presentations
The safety and outcomes of elective endovascular aortic stenting in the elderly: A systematic review and meta-analysis of clinical outcomes, Charing Cross Vascular Symposium, London, UK, April 26, 2023. The safety and outcomes of elective endovascular aortic stenting in the elderly: A systematic review and meta-analysis of clinical outcomes, Vascular Society Annual Scientific Meeting, Dublin, Ireland, November 22, 2023.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This Study was funded by the National Institute for Health Research (NIHR) Oxford Biomedical Research Centre (BRC), The views expressed are those of the author(s) and not necessarily those of the National Health Service (NHS), the NIHR, or the Department of Health.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.