
Abstract
Objectives:
The aim of the study was to investigate the safety and feasibility of branched endovascular arch repair (b-TEVAR) with a custom-made double or triple inner branched arch endograft using a short dilator tip (35 mm) in patients with aortic arch pathologies.
Methods:
Retrospective analysis of all consecutive patients undergoing b-TEVAR with a short dilator tip for the treatment of aortic arch pathologies in a high-volume tertiary center between January 2019 and July 2023. The combined primary endpoint was technical success and perioperative complications caused by the endograft, including tip-induced cardiac injury and trackability issues. Secondary endpoints were major adverse events (MAE), including morbidity, mortality, and reinterventions within 30 days.
Results:
During a 4-year period, 22 patients (median age 72 years, 16 males) were treated with a custom-made double or triple inner-branched TEVAR for different aortic arch pathologies using a short dilator tip (35 mm). After initial exclusive treatment of patients with previous valve replacement, the use of a short dilator tip became standard. Eighteen patients received a triple- and 4 patients received a double-branched endograft. Seventeen patients (77.3%) underwent elective treatment, while 5 patients underwent urgent repair due to contained rupture or symptomatic aneurysms. The technical success was 100%. No tip-induced cardiac mortality and morbidity occurred perioperatively. The trackability of the device was in no case affected by the short tip. Within 30 days, the MAE rate was 45%, including one death. No re-intervention had to be performed.
Conclusion:
Endovascular aortic arch repair with inner-branched arch endografts using a short dilator tip (35 mm) appears to be safe and technically feasible and could potentially reduce the risk of fatal myocardial injuries.
Clinical impact
Due to safe and stable maneuverability and deployment of endograft in zone 0 the use of short dilator tip might have the potential to become standard in endovascular branched arch repair. This is one of the first reports on the use of short dilator tip and associated complications in endovascular branched arch repair.
Keywords
Article Highlights
-
-
Introduction
Open arch replacement has been the standard of care for the treatment of aortic arch pathologies, with a perioperative mortality of 5% and a stroke rate of 7% in selected patient cohorts.1-5 Thus, high-risk patients are disqualified from open surgical treatment due to disproportional operative risk. Development in endovascular techniques offers the creation of new treatment options for arch pathologies in such.6,7 Multiple studies have reported promising results following endovascular treatment of aortic arch aneurysms, especially in patients who are unfit for open surgery.8-10
The endovascular repair of aortic arch pathologies requires a proximal landing in Ishimaru zone 0. Consequently, the aortic valve has to be passed not only with a stiff guidewire to achieve stability but, also, the dilator tip of the delivery system must be advanced to the level of the aortic valve or into the left ventricle to allow a safe landing and sufficient length of the proximal landing zone of the endograft in zone 0. 10
Cardiac complications are common but not well reported in the treatment of endovascular arch repair. In a recent meta-analysis by Spath et al. focusing on the outcomes of fenestrated and branched aortic arch repair, an overall cardiac complication rate of 6.7% and 6.3% in branched repair was reported. 11 In a study by Ju et al., 41 patients suffering from acute and chronic type A aortic dissections were treated with a Cook TX2 system (Cook Medical, Bloomington, Indiana, USA) and a 60 mm regular dilator tip, which had to be advanced in the left ventricle. Four patients (9.7%) experienced supraventricular tachycardia due to mechanical irritations requiring medical conversion. 12 To reduce the potential risk of such complications, the Zenith arch branched endograft can also be manufactured with a short dilator tip of 35 mm. While the use of this short tip may be protective, it could potentially be associated with reduced trackability of the device, making delivery more challenging.
The aim of this study was to investigate the feasibility and safety of the short dilator tip (35 mm) in custom-made double and triple-branched arch endografts for treatment of aortic arch pathologies requiring proximal landing in Zone 0 (Figure 1).
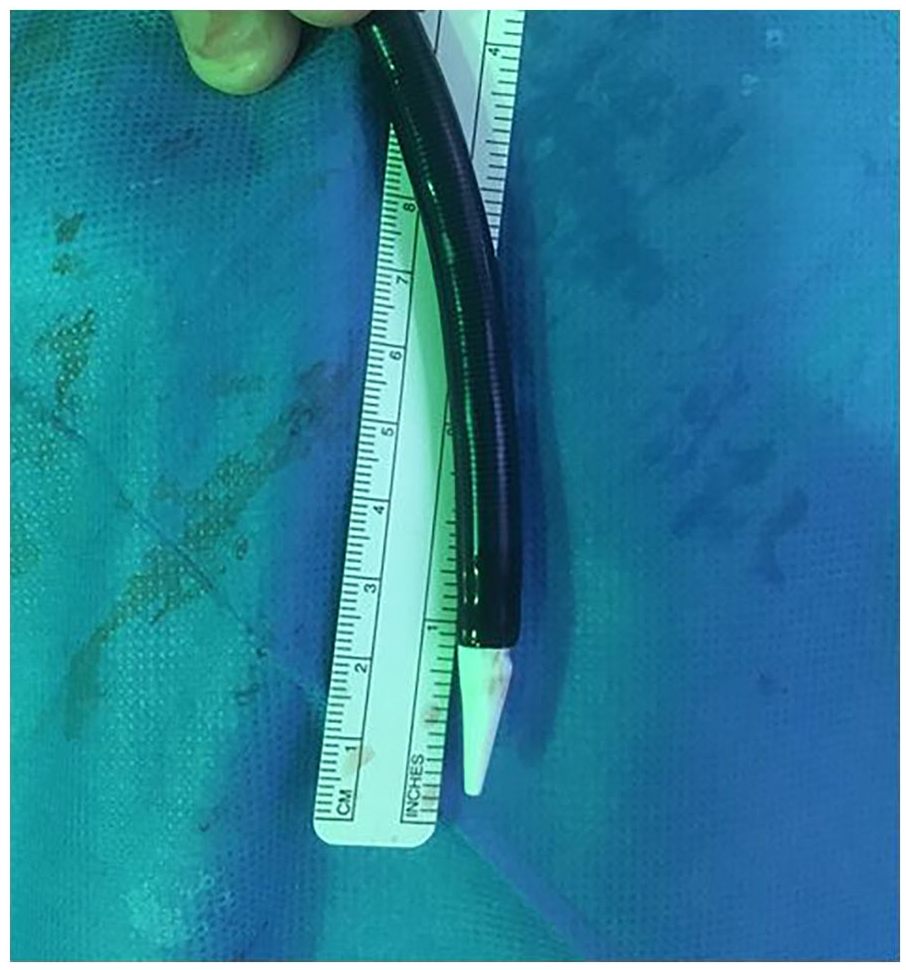
Short dilator tip (35 mm) of a custom-made branched arch endograft (Cook Medical).
Material and Methods
An observational, descriptive, single-center retrospective cohort study was performed. Between January 2019 and July 2023, all consecutive patients treated for different arch pathologies with a double or triple inner-branched TEVAR using a short dilator tip (35 mm) were included (Figure 2). Patients requiring transapical access were excluded. The ethical committee approved the use of patient data for the anonymized retrospective data analysis (registration number 20-148).
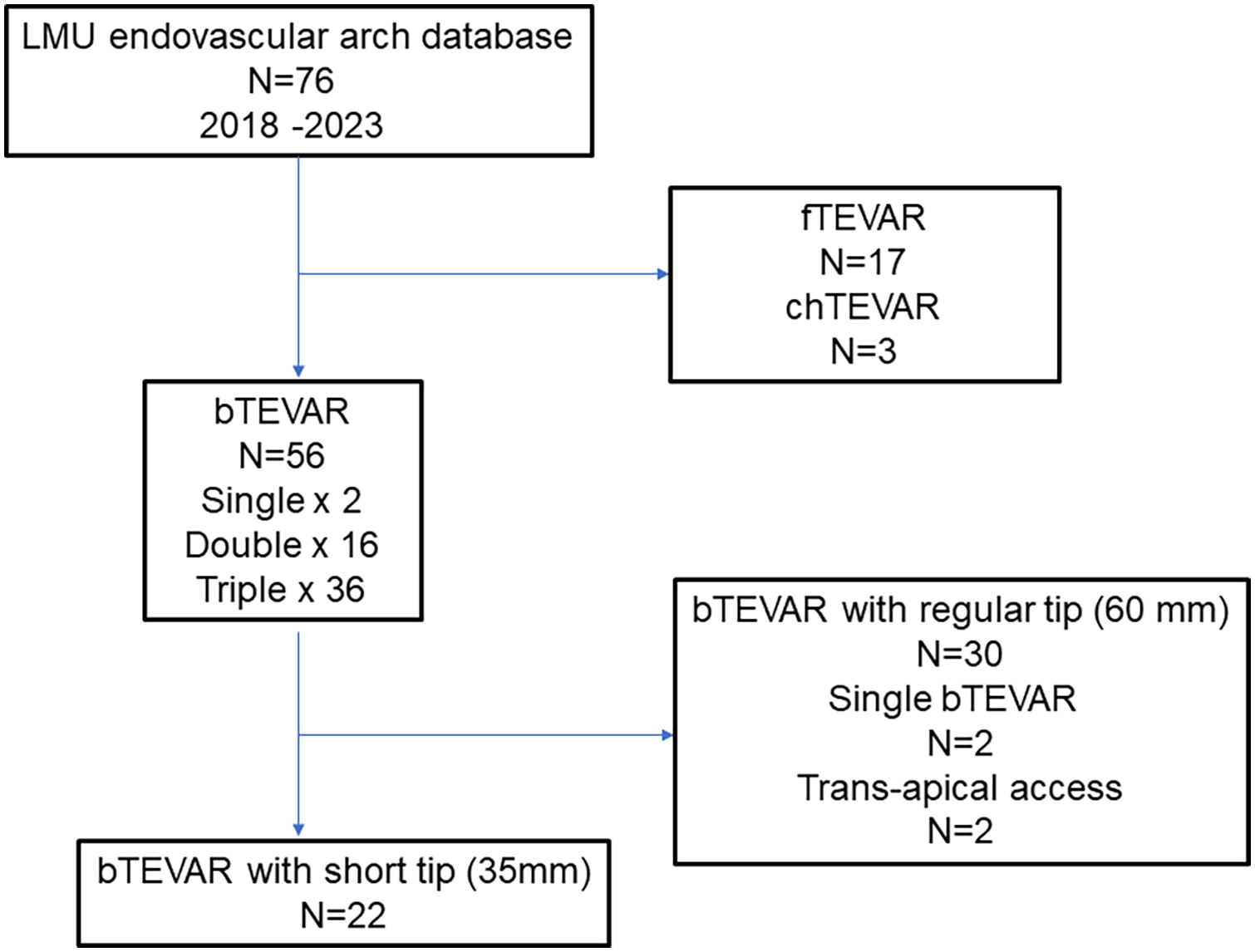
Flowchart for patient selection.
The combined primary endpoint was technical success and perioperative complications caused by the endograft. Technical success was defined as the planned delivery and deployment of the endograft with the connection of all target vessels. 13 Perioperative complications caused by the endograft include cardiac complications like arrhythmias requiring medical or electrical conversion and ventricular perforation due to wire or tip injury resulting in hemodynamic relevant pericardial effusion, or difficulties in trackability.
Secondary endpoints were major adverse events, including respiratory failure, kidney failure, cardiac events, stroke, paraplegia, re-interventions, and death within 30 days. 13
Graft Planning
A dedicated 3D workstation (TeraRecon, San Mateo, California, USA) was used for case planning. Measurements were performed on centerline bases and included the diameter and length of landing zones in the aorta and target vessels. Aortic arch types were measured based on the relationship of the origins of the supraaortic vessels to the parallel plane perpendicular to the outer curvature of the arch. 14 Oversizing of the endograft was planned at 15–30%. The endograft used was the Zenith double or triple arch branch endograft (Cook Medical, Bloomington, Indiana, USA), which is regularly manufactured with a 60 mm dilator tip. Originally, a short dilator tip (35 mm) was targeted only in cases where there was a short landing zone and/or prior biological or mechanical valve replacement to avoid or minimize left ventricular advancement. Since the beginning of 2022, the short dilator tip has been routinely used for all aortic arch endoprostheses.
Implantation Procedure
The main procedure was performed via a bilateral ultrasound-guided percutaneous femoral artery access through which the main endograft and angiographic catheter were advanced into the ascending aorta. In patients presenting a mechanical valve, the Rosen guidewire (Cook Medical, Bloomington, Indiana, USA) and dilator tip were guided laterally (1) to occupy one valve leaflet and (2) to advance the tip through the valvular level safely. 15 For the deployment of the main graft, cardiac output was reduced using the Munich Valsalva (MuVIT) maneuver previously described by the group of Tsilimparis et al.16,17 MuVIT is used in this cohort of patients due to personal preference. The most frequently used procedure for cardiac output reduction in the endovascular ascending aorta, arch, and descending aorta repair is the rapid right ventricular pacing technique. 18 The dilator tip was always kept at the level of the sino-tubular junction or aortic valve (central image). In the case of a short landing zone, the tip was progressively advanced into the left ventricle (Figure 3). After complete deployment of the main graft, the dilator tip and the guidewire were removed. In cases where a double-branched graft was implanted, the surgically exposed right common carotid artery or the right axillary artery and left common carotid artery were used to implant the bridging stents. If a triple-branched prosthesis was implanted, the surgically exposed right common carotid artery or axillary artery and the left common carotid artery were used to implant the stents into the antegrade branches. To avoid access via the left common carotid artery in some cases, the trans-axillary branch-to-branch-to-branch catheterization of supra-aortic vessels was performed. 19 The retrograde branch for LSA is routinely pre-loaded, and the bridging stent was implanted via the femoral access sites. The IA is bridged with a dedicated self-expandable stent graft with a profile of 12-14 Fr, in a design similar to that of iliac limb extensions with a short tip. The LSA and LCCA were bridged with both self-expandable and balloon-expandable covered stents. Additional procedures, such as aneurysm sac embolization or distal stent graft expansion, may be performed as needed.
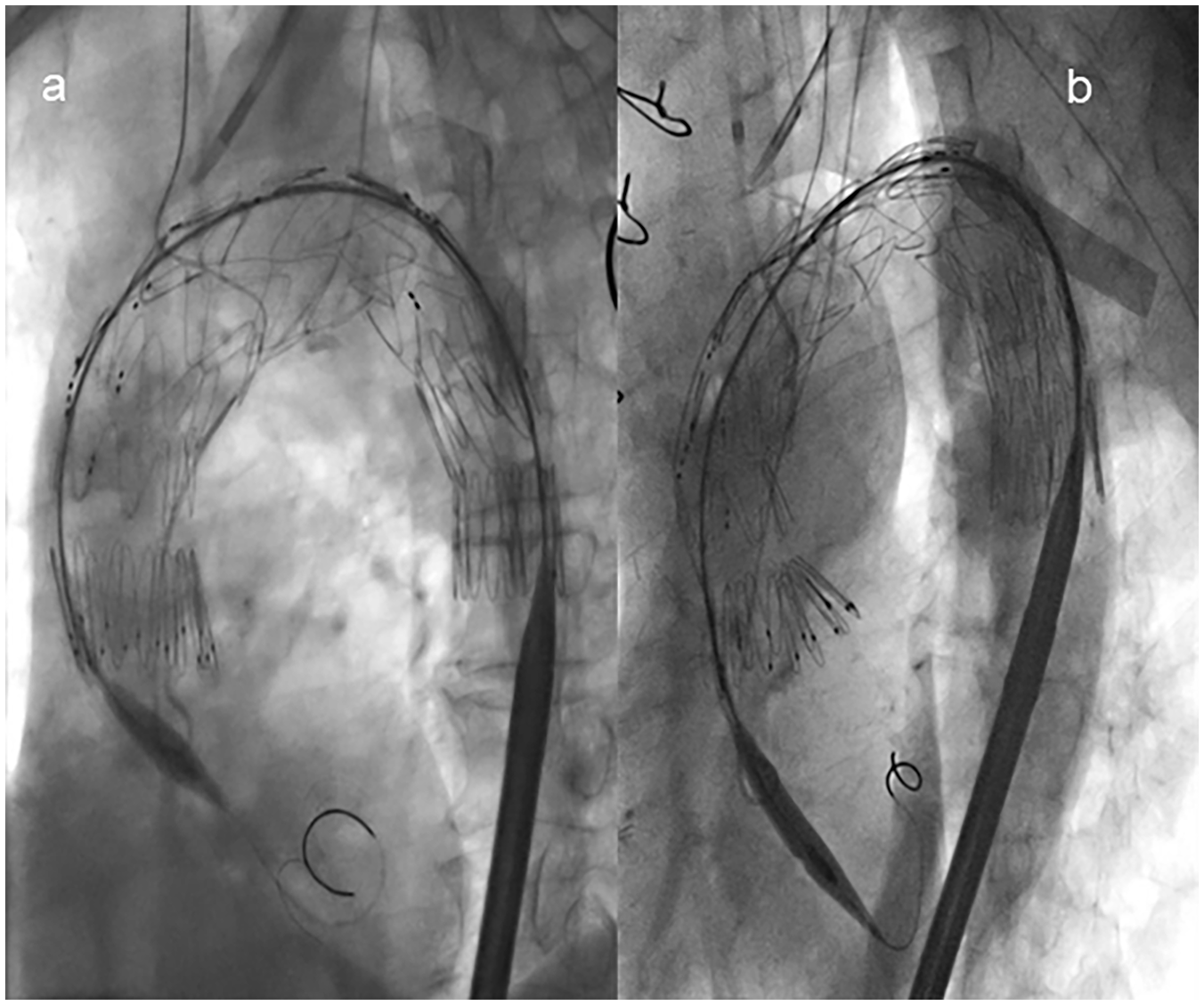
Advancement of dilator tip into left ventricle during endograft deployment:
Statistical Analysis
Statistical analysis was performed with SPSS version 26 (SPSS, Armonk, NY, USA: IBM Corp). Normality was assessed with the Shapiro-Wilks test. Normally distributed variables were expressed as means ± standard deviation (SD), while variables that did not follow a normal distribution were expressed with medians and interquartile ranges (IQR). Categorical data were represented as numbers and percentages.
Results
Within the study period, 22 patients (median age 72, IQR 63–79; 16 males, 73%) underwent endovascular aortic arch repair with the Zenith arch branch device (Cook Medical, Bloomington, Indiana, USA) for different arch pathologies using a short dilator tip (35 mm). Patients’ demographic characteristics are shown in Table 1. Thirteen patients (59%) had a prior ascending and/or arch replacement due to acute type A aortic dissection. Nine patients (41%) were treated due to native degenerative arch pathologies, including, for example, arch aneurysm and penetrating aortic ulcer. Nine patients (41%) had a previous aortic valve replacement (6 biological and 3 mechanical). Seventeen patients (77%) were treated electively, and 5 (23%) required urgent treatment due to a contained rupture using the planned endograft for another patient. The aortic history and indications for treatment are listed in Supplementary Table 1.
Patients’ Demographics and Characteristics.

Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; bTEVAR, branched thoracic endovascular aortic repair; CABG, coronary artery bypass graft; CAD, coronary artery disease; CHF, chronic heart failure; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; CTD, connective tissue disease; PAD, peripheral artery disease; PTCA, percutaneous transluminal coronary angioplasty; TIA, transitory ischemic attack.
Procedural Data
Eighteen patients (82%) received a triple, and 4 patients (18%) a double inner-branched stent-graft.
Preoperative debranching was performed in 4 cases (18%). No simultaneous debranching was necessary. In 3 patients with a double-branched endograft, a left carotid-subclavian-bypass (CSB) was performed. One patient with a double-branched endograft additionally needed a right CSB due to a dissected landing zone in an innominate artery (IA) (Supplementary Table 1). In another patient, right CSB was performed due to an aberrant subclavian artery.
Four patients (18%) needed distal extension with thoracic endovascular aortic repair (TEVAR) due to extended downstream pathologies.
The median length of the proximal landing zone (PLZ) (Zone 0) was 45 mm (34–54 mm). The lengths of the ascending aorta (measured at the outer curvature from the sino-tubular junction to the beginning of the brachio-cephalic trunk) proximal neck diameter (proximal landing zone of endograft), measured at the center line, and the type of arch (type I: 23%, type II: 50%, type III: 27%) are shown in Supplementary Table 2.
Technical success was achieved in all 22 patients (100%). No malignant arrhythmias requiring medical or electrical conversion were observed. No ventricular perforation due to wire or tip injury resulting in hemodynamic relevant pericardial effusion occurred. Median operative time was 259 mins (IQR 231–337). Two patients (9%) had access-related complications and needed local endarterectomy with patch-plasty of the brachial artery due to dissection. No further additional procedures were needed. Additional perioperative data is summarized in Table 2.
Perioperative Data, in-Hospital, 30-Day Major Adverse Events (MAE).

Abbreviations: bTEVAR, branched thoracic endovascular aortic repair; CSFD, cerebrospinal fluid drainage; MAE, major adverse events; MuViT, Munich Valsalva implantation technique; TIA, transitory ischemic attack.
In-Hospital, 30-Day Results
Major adverse events (MAE) occurred in 10 of the 22 patients within 30 days (45%). One patient developed a major disabling stroke perioperatively due to extended manipulation in a 110 mm anastomotic pseudoaneurysm after arch replacement of type A aortic dissection. The second patient with a postoperative major stroke received a triple arch branch repair due to a contained ruptured aortic arch PAU. The patient went to neurologic rehabilitation with partial recovery after discharge. One patient suffered a transient ischemic attack after triple-branched repair of a symptomatic aortic arch aneurysm and was discharged without any residuals. Renal failure occurred in 2 patients (9%). In 1 patient with a distal anastomotic pseudoaneurysm after root, ascending, and hemi-arch replacement, a triple-arch branch repair was performed. The patient suffered from renal failure, which recovered spontaneously without the need for dialysis. The second patient had a preoperative renal insufficiency (Glomerular filtration rate 30 ml/min). Postoperatively, after triple-arch branch repair, the patient needed temporary dialysis with recovery of renal function during a hospital stay. No spinal cord ischemia occurred. No new onset arrhythmias or myocardial infarctions were encountered. In addition, no patient experienced cardiac symptoms or showed pericardial effusion in postoperative CTA (Table 2).
Thirty-day mortality was 4.5% (1/22). The patient suffered from a major stroke after treatment of an anastomotic pseudoaneurysm (110 mm) with dysarthria and left-sided hemiparesis, as previously mentioned. This was later complicated by pneumonia and septic shock. Finally, palliative care was chosen by the family.
Postoperative computed tomography angiography (CTA) showed 1 patient with a very early type Ia endoleak on the second postoperative day but died due to a major stroke, as mentioned. Persistent false lumen perfusion was observed in a patient with chronic type B aortic dissection. False lumen occlusion with a candy plug was performed to achieve false lumen thrombosis during the same hospital stay. In 3 patients, a low-flow type III endoleak was observed. They were treated conservatively with no intervention. These endoleaks resolved spontaneously on follow-up CT scans. All supraaortic target vessels were patent at a 30-day follow-up. The median ICU stay was 2 days (IQR 1–4), and the median hospital stay was 10 days (IQR 8–18). In-hospital and 30-day results are presented in Table 2.
Discussion
Endovascular aortic arch repair with the use of branched devices shows promising results in native aortic arch pathologies.8-10 In recent years, branched endovascular repair is also increasingly used for aortic arch pathologies in patients with prior open ascending and arch repair. 20 However, endovascular arch repair frequently requires landing in zone 0, and thus, the mostly short landing zones necessitate the deployment just above the level of the coronary arteries. Clearly speaking, most arch endografts require crossing of the aortic valve. The distance of advancement into the left ventricle directly depends on the length of the proximal dilator tip. The currently available arch branch devices provide different lengths of proximal dilator tips. For example, the Relay arch branch endograft (Terumo Aortic, Hamburg, Germany) has a dilator tip length between 49 to 51 mm (depending on the diameter of the mainbody 32–46). The delivery system of the ascending module of the 2 modular arch endograft by Nexus (Artivion, Inc., Hechingen, Germany) has a tip length of 40 mm. The regular dilator tip of the inner branched Cook arch endograft (Cook medical) has a length of 60 mm but is also available in a short configuration of 35 mm. In the case of the use of a regular dilator tip (60 mm), the tip advances an additional 25 mm through the aortic valve into the left ventricle compared to the short dilator tip. This might be associated with an increased risk of cardiac irritation and injury, particularly if further advancement in the left ventricle was necessary. Such risk of interference with the endocardium is hypothetically reduced by the use of a short dilator tip compared to the regular dilator tip.
In the study of the current cohort of patients, the use of a short dilator tip (35 mm) in branched endovascular arch repair was evaluated concerning successful delivery of endograft and potential association with cardiac complications.
To achieve adequate deployment of the endograft in zone 0 and avoid type Ia endoleak, it is necessary to place the dilator tip at the level of the aortic valve or pass it into the left ventricle. Spear et al published the technique of the use of a short bullet-nose configuration to avoid passage of a mechanical aortic valve. 21 The Hamburg group recently reported the ascending aorta nose-cone loop technique to avoid valve passage. 22 Our group already reported the successful lateral passage of a mechanical valve. 15 During the treatment of arch pathologies, we advance the dilator tip at least partially through the aortic valve to achieve adequate landing in the mostly short landing zone. With the use of the short dilator tip, we achieved landing in the intended landing zone in all cases, with or without a mechanical prosthesis in place. Only in 1 patient did a type Ia endoleak occur, maybe due to a short landing zone of 25 mm.
Cardiac complications such as malignant arrythmias, endocardial laceration, or left ventricle perforation are not frequently reported in endovascular arch repair; however, they are well documented after endovascular repair of ascending aortic pathologies and cardiologic interventions such as transcatheter aortic valve repair (TAVR). For example, Ju et al reported a high number of severe arrythmias occurring due to contact of the tip with the endocardium that required additional medical treatment and resuscitation. 12 Also, Kratimenos et al reported the same experience during the endovascular treatment of a symptomatic ascending penetrating aortic ulcer. 23 Concerning ventricle injury, Langer et al reported a rate of 0.2–1.1% of wire and device-associated injuries during TAVR procedures in a review of the literature. 24 Left ventricle injuries include ventricle and septum perforation due to stiff guide wire and the device itself. Comparable findings were reported by the CoreValve clinical investigators in a multicenter study including 795 patients receiving a self-expanding TAVR noting wire associated left ventricle perforation rate of 1.3%. 25 In the present study, no perioperative cardiac complications like malignant arrythmia with the need of medical or electrical re-intervention or ventricular rupture have been observed.
To avoid cardiac complications is especially of importance in this cohort of patients that have been considered to be unfit for surgery due to fragile conditions and/or previous cardiac surgery (ascending and/or arch replacement, etc.).
Aneurysmatic and dissected aortic arch anatomy is frequently severely tortuous and angulated with difficult maneuverability of the endograft, 26 which is even more problematic in endovascular aortic arch repair to achieve the endograft delivery into zone 0. The length of the dilator tip might play an important role in terms of stable maneuvering through kinked aorto-iliac anatomy. In the present study, the degree of arch angulation was assessed using the classification described by Casserly et al. 14 No difficulties in trackability and maneuvering of endograft through the aortic passage into the intended landing zone were observed independent of the type of arch.
The 30-day major adverse event rate was found high among the presented cohort. This is both an expression of the technical complexity of repairing aortic arch pathologies endovascularly and, of course, the frailty of patients who did not qualify for open surgical repair in the treated cohort. Stroke is still the major restriction of endovascular arch repair. The reported stroke rates range from 0% to 14% in the recent literature and, thus, remain similar or higher than in open surgical repair.9,27,28 In the present study, disabling strokes were found in 9% (2/22) of the patients, both in patients undergoing emergency treatment. We try to reduce the risk of stroke by (1) minimizing manipulation in the arch and (2) selective clamping of the right carotid artery to control emboli while implanting the bridging stents retrogradely over the right carotid. Our technique changed over time to completely avoid cervical exposure by use of the trans-axillary approach for the innominate artery and the triple branch-to-branch technique to address the left carotid artery. 19
Limitations of the Study
The present study had some notable limitations. The study was a single-center, retrospective study with a limited number of patients. Additionally, we didn`t perform a comparative analysis to arch branch procedures with the use of a regular dilator tip. Nevertheless, the study supports that for safety and trackability a short dilator tip might be considered for standard use, but this has to be proven in multicenter studies with a larger number of patients.
Conclusion
The use of a short dilator tip in endovascular branched arch repair is technically feasible. A short tip provides a safe and stable means to maneuver and deploy the endograft at the planned landing zone without relevant cardiac complications.
Supplemental Material
sj-docx-1-jet-10.1177_15266028241283713 – Supplemental material for The Use of Short Dilator Tip in Endovascular Branched Arch Repair: A Case Series
Supplemental material, sj-docx-1-jet-10.1177_15266028241283713 for The Use of Short Dilator Tip in Endovascular Branched Arch Repair: A Case Series by D. Becker, J. Stana, C. Prendes, A. Ali, M. Pichlmaier, S. Peterss and N. Tsilimparis in Journal of Endovascular Therapy
Supplemental Material
sj-docx-2-jet-10.1177_15266028241283713 – Supplemental material for The Use of Short Dilator Tip in Endovascular Branched Arch Repair: A Case Series
Supplemental material, sj-docx-2-jet-10.1177_15266028241283713 for The Use of Short Dilator Tip in Endovascular Branched Arch Repair: A Case Series by D. Becker, J. Stana, C. Prendes, A. Ali, M. Pichlmaier, S. Peterss and N. Tsilimparis in Journal of Endovascular Therapy
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of thisarticle: NT: Travel and institutional research grants from and proctoring for Cook Medical and Bentley.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.