
Abstract
Objectives:
Percutaneous old balloon angioplasty is still the preferred treatment for the treatment of below-the-knee (BTK) arteries in chronic limb-threatening ischemia (CLTI). In the case of a suboptimal angioplasty result, a bailout stenting is required. So far, few data are available to assess the outcomes of bailout stenting after BTK angioplasty. This study aims to investigate the 1-year efficacy and safety after implantation of a polymer everolimus-eluting stent (PEES) as bailout stenting for BTK repair in patients with CLTI in a real-world setting.
Design:
This was a national multicenter prospective observational study.
Methods:
Patients with CLTI (Rutherford 4 to 6) BTK lesions (including P3) and requiring a bailout PEES due to dissection, thrombosis, or residual stenosis ≥30% after angioplasty were included. The freedom of a major adverse limb event at 12 months of the target limb was the primary endpoint.
Results:
XIENCE assessed 106 limbs (CLTI, 96.2%; chronic total occlusion, 2.8%) in 106 patients (mean age 77.1 years; males, 71.7%; diabetes mellitus, 66.9%; chronic kidney failure, 36.8%) with CLTI undergoing PEES stenting as a bailout for BTK lesions. Bailout stenting was required after 75.5% and 26.4% of residual stenosis and dissection, respectively. The mean diameter and length of the PEES were 3 mm and 3.4 ± 0.5 cm, respectively. At 1 year, the freedom of a major adverse limb event was 79.6% (95% CI, 71.5%-88.7%), the major amputation rate was 6.2% (95% CI, 1.3%-11%), and the target revascularization rate was 14.9% (95% CI, 6.5%-22.5%).
Conclusions:
In CLTI patients with BTK lesions, PEES stenting showed safety and efficacy as bailout stenting for BTK arterial lesions. This confirms the need for PEES stenting in a real-world practice.
Clinical Impact
The XIENCE study introduces the PEES as an effective bailout stenting option for patients with CLTI undergoing BTK revascularization, particularly for lesions under 4 cm. The study focuses on real-world cases where POBA alone is insufficient, demonstrating that PEES significantly improves outcomes by enhancing limb salvage and reducing the need for major amputations. For clinicians, this innovation offers a precise, size-adaptable solution, especially in cases where bailout stenting is required for short, focal lesions, improving both clinical and procedural results.
Keywords
Introduction
Chronic limb-threatening ischemia (CLTI) is the most severe form of lower limb peripheral arterial disease (PAD). Indeed, CLTI presents an increased risk of both 1-year amputation rate and 1-year mortality rate, which can range from 15% to 20% and 15% to 40%, respectively. 1 The prevalence of CLTI increases sharply with age, from 3% in those aged less than 60 years to >20% in those older than 79 years. 2 According Nehler et al, 11% of patients with PAD will present with CLTI, and their quality of life and lower extremity function will deteriorate over time.2,3
Lower limb revascularization is imperative to avoid amputation. In patients who are unfit for open surgery or without an available adequate great saphenous venous conduit, endovascular repair with revascularization could be considered as a first option. 4 In contrast, for the femoropopliteal segment, multiple trials failed to show the benefit of drug-coated devices for the endovascular treatment of below-the-knee (BTK) arteries in diffuse lesions.5-7 However, currently, there is evidence supporting the use of drug-eluting stents (DESs) in the treatment of focal disease (<4 cm) in infrapopliteal arteries. 8 Most of the DESs for BTK applications were initially designed for the use in the coronary arteries. They are composed of a balloon-expandable stent as a platform and a coating controlling drug release. However, in daily practice, BTK lesions are long, diffuse, or involve the tibial artery bifurcation. Percutaneous old balloon angioplasty (POBA) is still the preferred treatment for such lesions. In the case of a suboptimal angioplasty result (eg, residual stenosis, dissection, or thrombosis), a bailout stenting is required. Despite the frequency at which these complex lesions are encountered, few data are available to guide us in the use of DESs as bailout.
The XIENCE study is a national multicenter prospective observational registry in a real-world setting. The study is designed to assess the safety and the efficacy of a polymer everolimus eluting stent (PEES) as bailout stenting for BTK endovascular treatment in patients with CLTI.
Methods
Study design
XIENCE is a prospective national multicenter and noncontrolled study involving 16 centers. The study is designed to assess, in a real-world setting, the safety and the efficacy of a polymer everolimus-eluting stent (PEES) as bailout stenting for BTK endovascular treatment in patients with CLTI.
The study complied with the Declaration of Helsinki and was conducted in accordance with the French Good Clinical Practice guidelines. The study was approved by the local institutional review board. Participation in this registry was offered to patients after the procedure. Information was provided verbally, and all patients were notified and consented. This included their consent to the anonymous processing of their data.
Patients
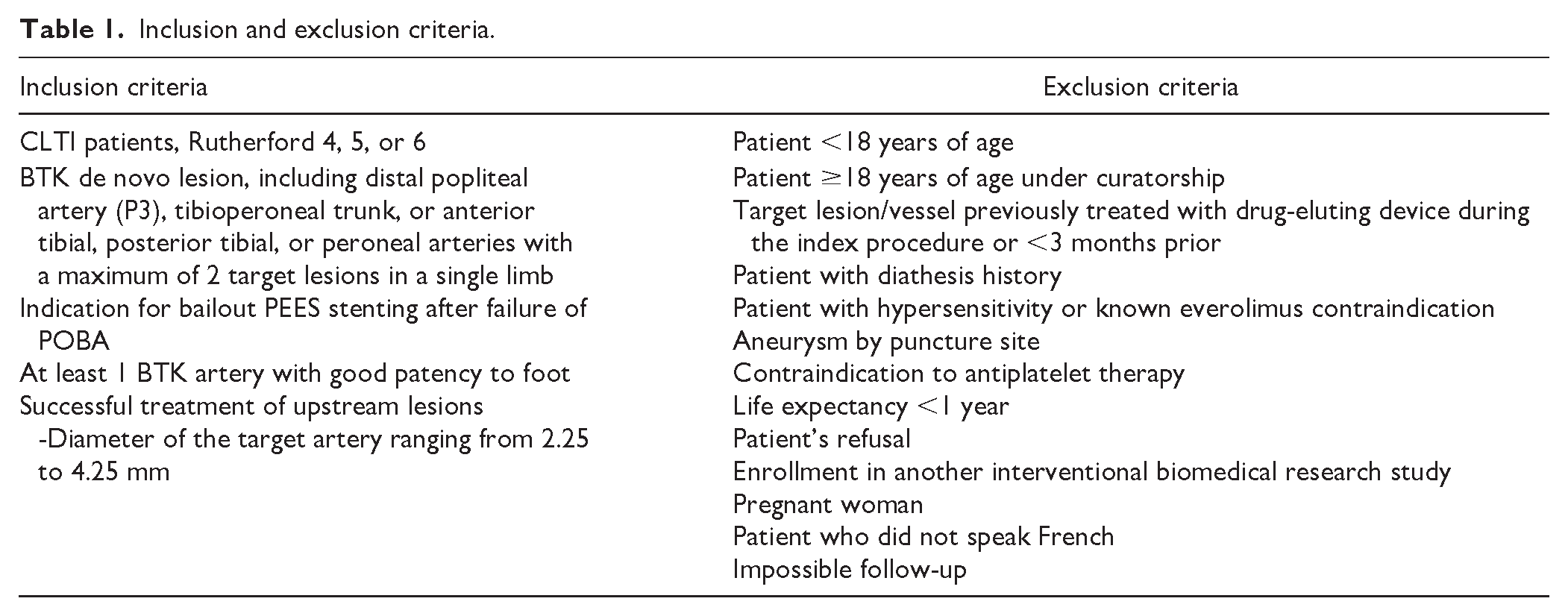
Study inclusion and exclusion criteria are provided in Table 1. Briefly, patients eligible for enrollment included adults with symptomatic lower limb PAD responsible for CLTI (Rutherford 4 to 6 in the target limb) and presenting with de novo BTK arterial lesions. Patients were further required to meet intraprocedural inclusion criteria. Specifically, target lesions located in the distal popliteal artery (P3), tibioperoneal trunk, and anterior tibial, posterior tibial, or peroneal arteries with a maximum of 2 target lesions per single limb were allowed. Lesions with ≥50% diameter stenosis were considered for the trial when their length was ≥40 mm and they arose in target vessels with diameters of 2.25 to 4.25 mm. Patients treated by POBA with an indication for provisional bailout stenting were included. Bailout stenting with a PEES was advised when residual stenosis of the treated lesion was >30% (by visual assessment) and there was flow-limiting dissection (by visual assessment) or thrombosis.
Inclusion and exclusion criteria.
In our study, we did not assess the wound, ischemia, and foot infection score for trophic disorders in patients. However, because most of our patients were classified as Rutherford category 4, 5, or 6, their wound, ischemia, and foot infection scores were likely at least between 2 and 3. This suggests a moderate to high risk of amputation, underscoring the severity of the condition.
Key exclusion criteria were life expectancy <1 year, a history of diathesis or contraindications to antiplatelet therapy, and hypersensitivity or known contraindication to everolimus.
Based on the results of the DESTINY clinical trial, the rate of patients having a major adverse limb event can be estimated at 9.4% at 1 year (8% target lesion reintervention [TLR] and 1.4% amputation). 9 Considering a first species risk alpha of 5%, 91 patients need to be evaluated to obtain an estimator with an accuracy of 6%. If we consider that 20% of patients will not be evaluable at 12 months, we need to include 110 patients in the prospective cohort.
Intervention
The study device was the XIENCE Prime BTK (Abbott, Abbott Laboratories, Inc, Santa, CA). The XIENCE Prime BTK has 3 components. The MULTI-LINK VISION stent platform, the polymer coating (poly[vinylidene fluoride-co-hexafluoropropylene]), and everolimus, an antiproliferative drug. The polymer coating of the XIENCE Prime BTK consists of a primer and a drug polymer reservoir layer The polymer of the thin primer layer is poly(n-butyl methacrylate); its adhesive properties ensure firm binding of the drug layer to the device. The drug reservoir layer is composed of poly[vinylidene fluoride-co-hexafluoropropylene] combined with everolimus. It controls drug release but also contributes to the blood and vascular tissue compatibility of the device. 10 The XIENCE Prime BTK is available in multiple sizes, offering lengths ranging from 8 to 38 mm and diameters varying between 2.25 and 4.0 mm, allowing for precise adaptation to the specific needs of each patient. Designed in cobalt-chromium alloy, the XIENCE Prime BTK combines robustness and biocompatibility, ensuring optimal durability and performance. The innovative design of the XIENCE Prime BTK stent includes an ultrathin mesh structure, providing exceptional flexibility and navigability while ensuring excellent support of the arterial wall. 11
Plain old balloon angioplasty was performed with commercially available balloon catheters, chosen at the investigator’s discretion, and done based on the device instructions and standard of care. Drug-coating balloons were not permitted. If flow-limiting dissection or residual stenosis of the treated lesion >30% occurred following the index angioplasty, bailout PEES placement was performed. A maximum implantation of 2 XIENCE Prime BTK systems per artery and 2 stents per limb was allowed. Additional interventions in the target limb were permitted for above-the-knee inflow treatment during the index procedure. Inflow lesions were treated according to the investigator’s standard procedures using commercially available devices. Drug-eluting device use was permitted for inflow lesions. Interventions must have been deemed successful (eg, absence of distal embolization and optimal inflow restoration) prior BTK treatment.
Follow-up protocol
The follow-up was accomplished at 1, 6, and 12 months after PEES implantation. History check, physical examination, assessment of the clinical category of CLTI according to the Rutherford system, and a duplex-scan investigation were realized at each timepoint. All clinical surveillance events, postoperative complications, and rehospitalizations for cardiovascular causes were recorded. Missing data were noted. A patient was considered lost to follow-up only when the following conditions were met: nonattendance at the scheduled consultations, failure of telephone contact (over a minimum period of 1 month), no reply to requests by mail (minimum of 2 letters), or failure of a search for information on a possible death from the general practitioner or from the city where the patient was born. Anticoagulant and antiplatelet medications were prescribed prior to, during, and after the procedure according to the investigators’ standard procedures. Antiplatelet therapy was reported at 12 months, with acetylsalicylic acid being the most common. Clopidogrel, which is recommended as a first-line treatment in European guidelines, 12 was reported for 28% of patients at 12 months. Dual antiplatelet therapy was reported by 60% at 1 month and 28% at 12 months (Figure 1).
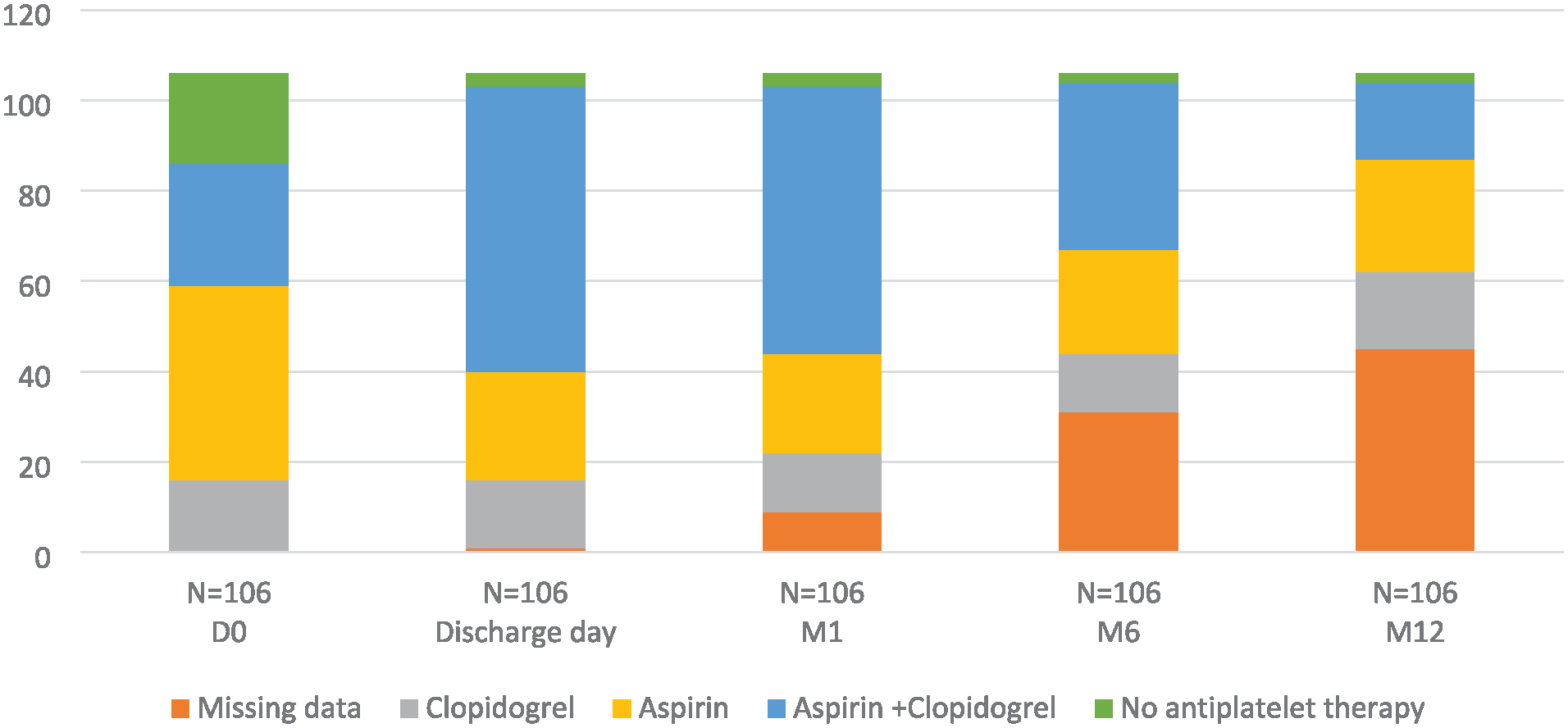
Individual antiplatelet therapy.
Antiplatelet medication prescription after the procedure was consistent with current local clinical practice and the instructions for use for each device. European guidelines recommend dual antiplatelet therapy for at least 1 month after stent implantation regardless of bare-metal stent (BMS) or DES type. Based on the instructions for use, dual antiplatelet therapy after DES implantation is required for a minimum of 60 days. 12
Endpoints and definitions
The primary endpoint assessed was the freedom from a major adverse limb event at 12 months. Major limb adverse event was defined as a major event in the treated limb, including a major amputation (ankle level or above) or a TLR during the study period. Secondary endpoints included the technical success during the index procedure, defined as the absence of residual stenosis >30%, flow-limiting dissection, or thrombosis of the target lesion. Limb salvage was defined by the absence of major amputation. Major cardiovascular events were defined by death, myocardial infarction, or stroke. Target limb reintervention was clinically driven and defined as reintervention performed for lesions with ≥50% diameter stenosis related to the treated area (including 1 cm above and below the lesion) after documentation of recurrent clinical symptoms. Primary sustained clinical improvement was defined as a sustained wound healing and rest pain resolution without the need for repeated TLR in surviving patients. Primary patency was defined as a duplex ultrasound peak systolic velocity ratio of ≤2.4 in the absence of any percutaneous or surgical reintervention in the treated segment or in adjacent areas. In-stent restenosis was assessed by duplex ultrasound and was defined as restenosis of more than 50% and a peak systolic velocity index of >2.4 at the target lesion. The diagnosis of stent thrombosis was considered when a complete occlusion was seen on duplex scan without any previous sign of restenosis. Sustained hemodynamic improvement was defined by the persistence of an improvement with an ankle brachial index of ≥0.15 during follow-up compared with the preoperative value without the need for reintervention at the TLR level.
Statistical analyses
Among enrolled patients, those with major noninclusion criteria were excluded from statistical analysis. Continuous variables are presented as means ± SDs. Minimum and maximum were added for PEES length and diameter. Categorical variables are presented as count and percentages. Paired t tests were used to compare baseline and 12-month ankle brachial index data. McNemar’s test was used to analyze improvement according to the Rutherford category. The Kaplan-Meier method was used to evaluate time-to-event data for global survival, target lesion revascularization, freedom from major adverse limb events, primary patency, limb salvage, and sustained clinical improvement over the 12-month follow-up period. All P values are 2-sided; P < 0.05 indicated a statistically significant difference. All statistical analyses were performed using SAS (SAS Institute, Cary, NC) version 9.4.
Results
Patients
Between May 2018 and June 2019, 120 patients were prospectively enrolled in the study, and 106 were analyzed. The 12-month follow-up flowchart is shown in Figure 2. Follow-up at 1, 6, and 12 months was completed for 102, 86, and 72 patients, respectively. The mean age of patients was 77.1 ± 11 years, with high proportions of comorbidities such as diabetes, hyperlipidemia, and hypertension. All included patients presented with CLTI (Rutherford 4 to 6), and 5 patients presented with claudication. The American Society of Anesthesiologists score was mostly evaluated at 3. Baseline patient characteristics are presented in Table 2.
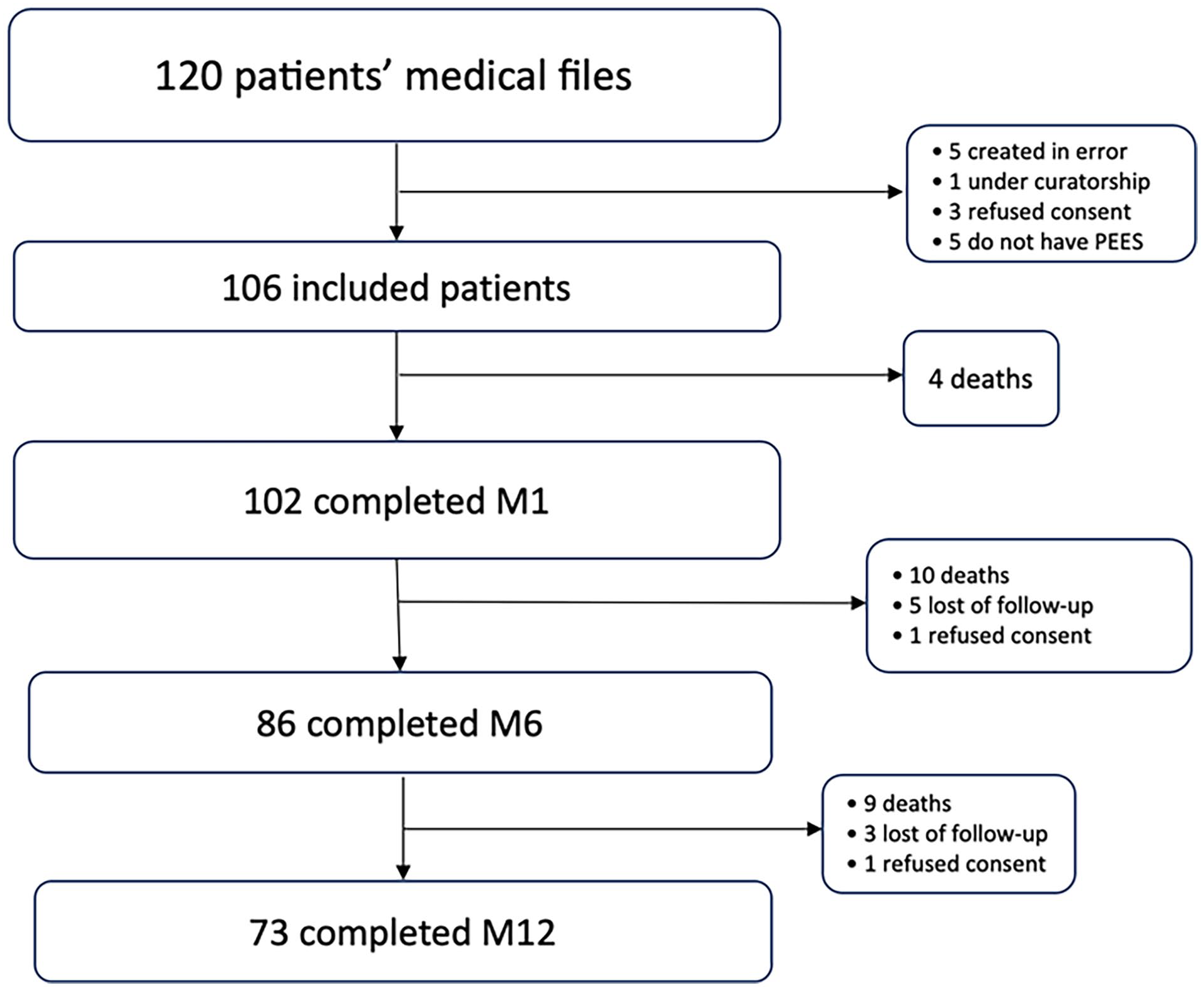
Flowchart.
Baseline patient characteristics.

Procedures
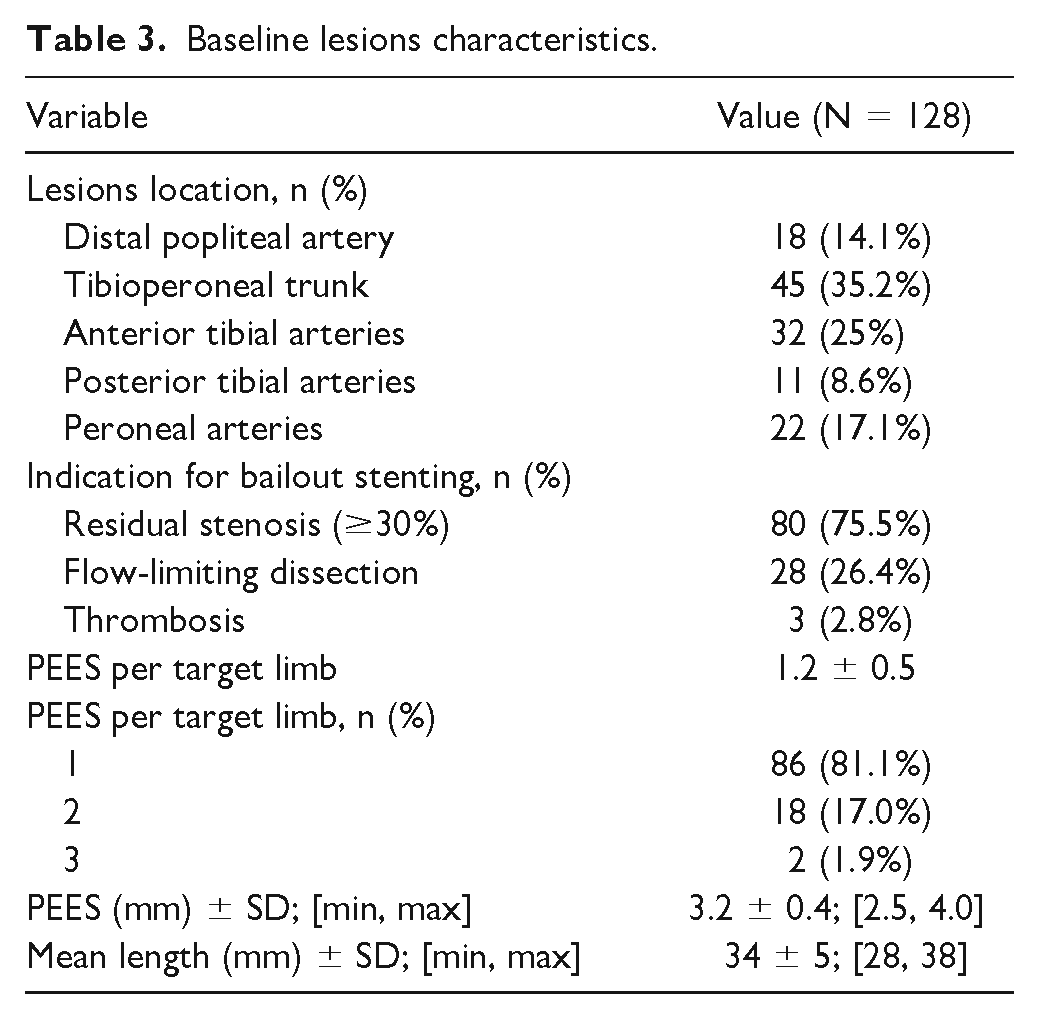
Procedures were mainly performed under local anesthesia with sedation or under locoregional anesthesia (85.8%) using an anterograde ipsilateral approach (66%). A retrograde ipsilateral approach was required in 4.7% of the index procedures. In 42.5% of the cases (n = 45), an upstream lesion was treated. In total, 128 PEES were implanted in 106 target limbs (Table 3). Bailout stenting was mostly required for residual stenosis (75.5%). Mainly the tibioperoneal trunk and the anterior tibial artery were treated (35.2% and 25%, respectively). The mean stent length and diameter were 34 ± 5 mm and 3 mm, respectively. Technical success was achieved in 97.6% of the cases (n = 124).
Baseline lesions characteristics.
Effectiveness and safety
A total of 72 patients were assessed for the primary effectiveness endpoint. At 1 year, the survival rate was 76.6%. The major adverse cardiovascular events rate was 25.3%, including 23 deaths, 3 myocardial infarctions, and 1 stroke. The freedom from a major adverse limb event at 12 months was 79.6% (95% CI, 71.5%-88.7%; Figure 3A). Major amputations and the TLR rate at 12 months were 6.2% (95% CI, 1.3%-11%) and 14.9% (95% CI, 6.5%-22.5%), respectively. The limb salvage rate was 93.8% at 12 months (Figure 3B, C). Among patients with major reinterventions, a total of 16 reinterventions were performed, including 13 endovascular procedures and 3 open-surgery interventions. All reinterventions were outperformed for recurring CLTI symptoms. The primary patency rate at 12 months was 79.5% (95% CI, 71.4%-88.5%; Figure 3C). At 1 year, the in-stent restenosis and thrombosis rates were 20.5% and 12.1%, respectively. Over time, a significant sustained hemodynamic improvement was noted from baseline to 1 year (P < 0.001).
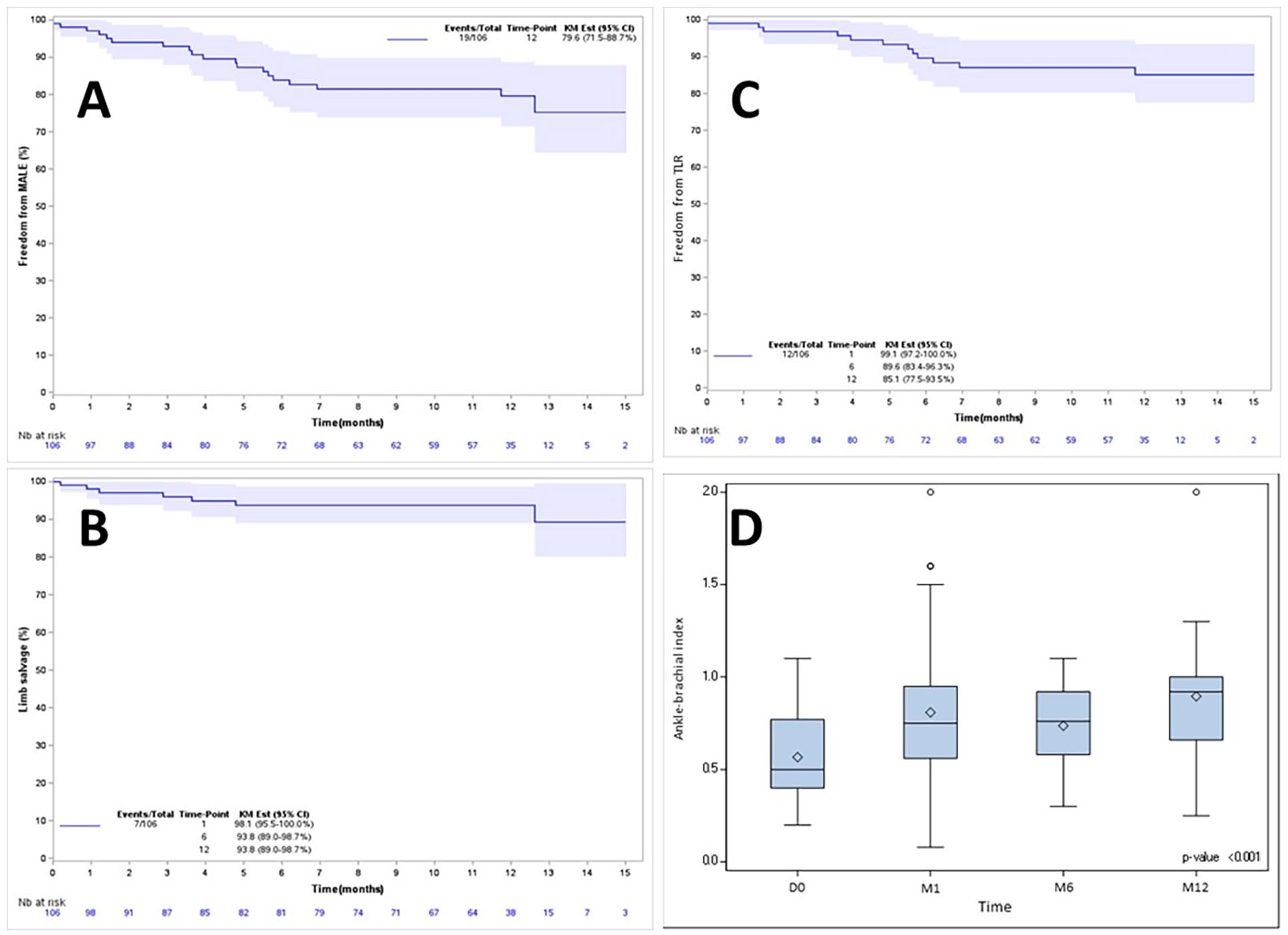
Kaplan-Meier estimates of the rates of freedom from major limb adverse events (A), limb salvage (B), target lesion revascularization (C), and ankle brachial index (D).
Rutherford changes
The distribution of Rutherford categories at each follow-up visit is shown in Figure 4. Most patients presented as Rutherford category of 3 or less by 6 months. At 12 months, 43% of patients were asymptomatic, and 67.57% of patients presented as Rutherford category of 3 or less. At 12 months, the primary and secondary sustained clinical improvements at 1 year were 45.1% and 35.3%, respectively.
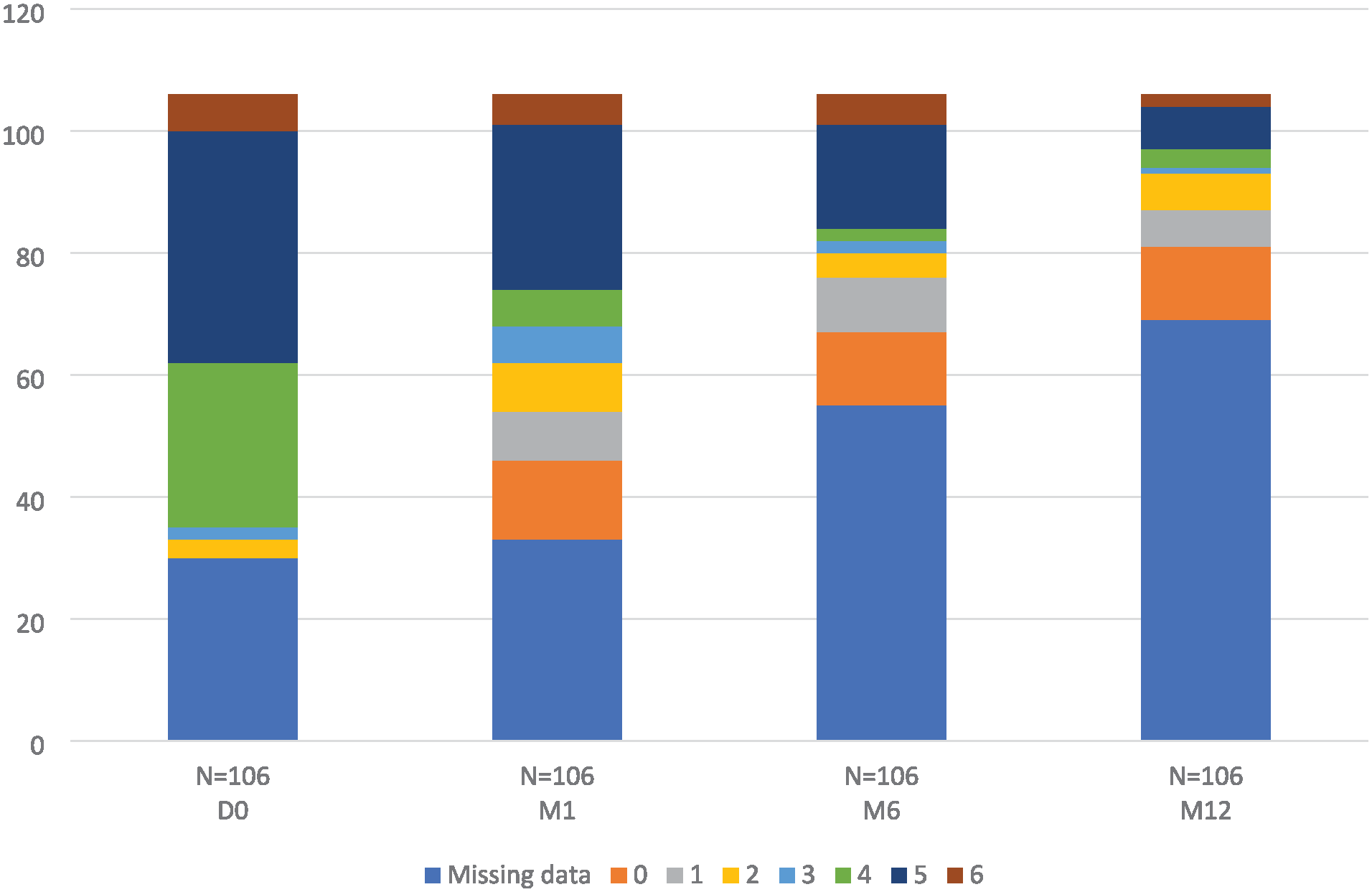
Rutherford categories changes.
Discussion
This study is a postmarket registry designed to assess the efficacy and safety of XIENCE Prime PEES within the CLTI population when bailout stenting was required. The study showed that PEES stenting provides favorable outcomes at 1 year, particularly in terms of major amputation. This observation was combined with a high survival rate after CLTI revascularization considering a high-risk population. These results confirm the need for PEES stenting for bailout to improve clinical and morphologic outcomes.
Critical limb-threatening ischemia patients are at risk for major amputation from progression of the atherosclerotic disease. Revascularization of CLTI patients is based on open surgery when an adequate great saphenous vein is available. 4 When an adequate great saphenous vein is not available, endovascular treatment could be an option. Currently, drug-eluting therapy appears as a valuable option for the femoropopliteal level but not for the BTK segment.13,14 Indeed, randomized, controlled trials (RCTs) did not show that drug-eluting devices are efficient compared with POBA to decrease the major amputation rate. For instance, drug-coating balloons have failed to show any superiority to POBA in RCTs.6,7 Recently, paclitaxel-eluting nitinol stent did not show any benefit compared with POBA in BTK artery lesions up to 140 mm in length. 15 Despite the lack of evidence in favor of drug-eluting devices for long BTK lesions, there is an accumulated body of evidence supporting the use of drug-eluting balloon–expandable stents in the treatment of focal lesions <4 cm in diameter of infrapopliteal arteries. 8 For instance, the YUKON RCT compared polymer-free sirolimus-eluting stents versus BMSs in the treatment of focal BTK de novo lesions. 16 The trial included 161 patients. The mean target lesion length was 31 ± 9 mm. Amputation rates were 2.6% and 12.2% (P = 0.03) in the polymer-free sirolimus–eluting stent and the BMS group, respectively. The YUKON and DESTINY RCTs were similar in terms of study design, using a BMS in the control group but using sirolimus instead of everolimus as the drug for the YUKON and DESTINY studies, respectively. 17
Today, DESTINY is still the main RCT to assess the safety and effectiveness of primary stenting by PEES. DESTINY included 140 patients, 74 in the PEES group and 66 in the BMS control group. The mean lesion length in the PEES group was 15.9 ± 10.2 mm. Twelve-month TLR and primary patency rates were 9% and 85%, respectively. Three major amputations were reported. In our study, we observed a trend to have a higher TLR rate (14.9% vs 9%) and a lower patency rate (79.5% vs 85%). However, these trends could be explained by the design of the study. Indeed, this study had a prospective registry design for a real-world setting, whereas DESTINY was an RCT with more selected patients and with a more rigorous strategy that is not always representative of regular practice. For example, the target lesions in DESTINY seemed to be longer than in our study (34 ± 5 mm vs 15.9 ± 10.2 mm) with a similar diameter (3 mm). Moreover, our study was designed to assess the efficacy and safety of PEES stenting as a bailout. Indeed, in DESTINY, primary stenting was indicated after vessel predilatation, whereas in our study, a PEES was implanted in the case of suboptimal angioplasty (eg, residual restenosis, flow-limiting dissection, or thrombosis). Interestingly, it has been shown that severe dissection during procedures employing balloon angioplasty only affect long-term patency. 18 Finally, although loss of patency may result in a failure to heal an ischemic wound and a major amputation, numerous other variables could alter the outcome and are confounders in interpreting the results of the study, such as the pedal vascular reservoir, the infection status, and the wound care program, which all may impact limb salvage. We cannot exclude that the size of XIENCE registry was not sufficient to adequately reflect the heterogeneity of the CLTI disease spectrum. Additionally, wound care was left to the centers to determine. This highlights the need for a standardized protocol to guide wound care and to improve devices assessment.
Polymer everolimus-eluting stents could be compared with sirolimus-eluting stents for BTK lesions. Both sirolimus and everolimus are inhibitors of the mammalian target of rapamycin and are used as immunosuppressants after organ transplantation. 19 In comparison with everolimus, sirolimus has lower bioavailability. In a recent meta-analysis, Fong et al identified 10 studies including 995 patients with sirolimus-eluting stents. 20 In this meta-analysis, only 3 RCTs were identified. Similarly, the meta-analysis reported that most patients were older than 70 years of age with a high rate of diabetes mellitus. At 1 year, 3 pooled studies yielded a primary patency rate of 82.8% (95% CI, 78.3%-87.6%). The 12-month TLR rate across 4 studies was 9.6% (95% CI, 6.4%-13.4%). These results compare with the DESTINY RCT. This is also in line with findings in coronary disease, where a meta-analysis did not show significant differences between both drugs in terms of clinical efficacy and safety. 21
Our study presents some limitations. First, this is a nonrandomized study with no control group. The recruitment was terminated after achieving the sample size necessary for the designed power. However, the number of patients evaluated at 1 year did not reach the target. Different types of biases may have occurred. For example, during the follow-up, patients were assessed by their treating interventionalist, and consequently, we cannot fully exclude the influence of measurement bias inherent to a study with open-label design. Selection bias may have occurred. To evaluate the risk of selection bias, screen failures were not documented throughout the inclusion period.
Second, the extent of vessel calcification in the stented segments was not studied, which may impact the assessment of the stent’s efficacy and long-term outcome. Without these data, it is challenging to fully understand how calcification may affect stent deployment, expansion, and the potential for restenosis. Future studies should aim to include an evaluation of vessel calcification to provide a more comprehensive understanding of the stent’s performance in various calcified environments.
To conclude, the use of the PEES device yielded satisfactory results in terms of patency, TLR, and limb salvage at 1 year, reducing exposure to a major event in the treated limb. These data suggest that the PEES is a safe and efficient device in CLTI patients when bailout stenting is required. Serious consideration should be given in the real-world setting to the use of PEES stenting for focal BTK lesions of <4 cm when bailout stenting is required.
Footnotes
Acknowledgements
We thank Eric Ducasse (CHU de Bordeaux, Service de chirurgie vasculaire, Bordeaux, F-33076 France) and Sébastien Penillon (MEDIPOLE de Savoie, 73190 Challes-les-Eaux, France) for including patients in this study. We thank the CHU de Nantes, Institut du thorax, Nantes, F-44093; Béatrice Guyomarc’h (biostatistician); David Lair (clinical chief of XIENCE registry); and Joelle Martin-Gauthier (clinical research technician of XIENCE registry) for their great support during this study.
Declaration of Conflicting Interests
William Sebbag, Antoine Sauguet, Serge Declemy, Tom Lecorvec, Jérôme Brunet, Nellie Della Schiava, Jonathan Sobocinski, and Eric Steinmetz have no conflict of interest to disclose. Yann Gouëffic reports research funding from Abbott, Boston Scientific, Cook, General Electric, and WL Gore and personnal fees and grants from Abbott, Biotronik, Boston Scientific, Medtronic, Penumbra, Terumo, and WL Gore (medical advisory board, educational course, speaking).
Funding
This work was supported by Abbott.