
Abstract
Purpose:
The purpose of this study was to collect all the available evidence concerning technical success and early and mid-term clinical outcomes of physician-modified endografts (PMEGs) for the treatment of aortic arch pathologies in zones 0 to 2.
Material and methods:
We performed a systematic review to identify all the eligible studies that reported outcomes to the PMEGs for aortic arch pathologies in zones 0 to 2 and then conducted a qualitative synthesis and meta-analysis of the results. The main outcomes were technical success, mortality, stroke rate, bridging stents’ complications, and reintervention rate. We estimated pooled proportions and 95% confidence intervals (CIs).
Results:
A total of 134 study titles were identified by the initial search strategy, of which 14 (zone 0 n=6; zone 1 n=1; zones 1 t o2: n=7) were considered eligible for inclusion in the meta-analysis. A total of 777 patients (80% male; 62±6 years) were identified among the eligible studies. The pooled technical success for the PMEG in zone 0 was 96.6% (95% CI=93.9%-98.2%), whereas in zones 1 to 2 was 95.9% (95% CI=92.9%-97.6%). The pooled 30-day mortality was 4.6% (95% CI=2.0%-10%) and 4.3% (95% CI=2.2%-8.2%) for zones 0 and 1 to 2, respectively, whereas the prevalence of late mortality was 8.2% (95% CI=4.7%-14%) and 3.4% (95% CI=1.9%-6%). The pooled stoke rate was 3.7% (95% CI=2.1%-6.4%) in zone 0 and 2.7% (95% CI=1.4%-5%) in zones 1 to 2. The early reintervention rate was 3.5% (95% CI=1.5%-8.0%) and 4.2% (95% CI=2.4%-7.2%) for zones 0 and 1 to 2, respectively, whereas during the mean follow-up of 26 months was 8.5% (95% CI=3.0%-21%) and 1.9% (95% CI=0.8%-4.3%). The pooled bridging’s stent instability was 3.9% (95% CI=1.1%-12.9%) in zone 0 and 3.2% (95% CI=1.8%-5.8%) in zones 1 to 2.
Conclusions:
Endovascular repair of aortic arch pathologies using PMEGs seems to present a satisfactory level of technical success and a low mortality rate. To attain clearer conclusions, further research employing randomized controlled trials, longer-term follow-up, and consistent reporting of results is warranted.
Clinical Impact
This systematic review and meta-analysis of observational studies analyzed the short- and mid-term outcomes of aortic arch aneurysm and/or dissection using physician-modified endografts. It separately examined the outcomes from zones 0 and 1-2 of the aortic arch. Fourteen studies (n=777 patients) were included. Overall technical success rates were 96.6% for zone 0 and 95.9% for zone 1-2. Regarding early mortality and stroke rates, no significant differences were observed, while late mortality was higher in patients in zone 0. The late reintervention rate favored patients treated with PMEGs in zone 1-2. The physician-modified technique appears to be an excellent and rapidly available alternative for the treatment of aortic arch diseases.
Introduction
Open surgical aortic arch repair (OSAAR) represents the gold standard treatment option for patients suffering from aortic arch diseases.1,2 Despite improvements due to increased experience and technical advancement, the mortality and morbidity rates are still considerable.1,2 Two studies reported that the open aortic arch population had a 30-day mortality rate of 5% and an in-hospital morbidity rate of 12%, respectively.1,2 These outcomes may be prohibitive for high surgical risk patients who need a surgical treatment.
The recent consensus paper from the European Societies of Vascular Surgery and Cardio-Thoracic Surgery proposed that patients unfit for open repair but possessing appropriate anatomy should be considered eligible for an endovascular repair in aortic arch zone 0 according to the Ishimaru and Mitchell classification.3,4 This applicability of endovascular repair in this population includes minimizing surgical trauma, avoiding cardiac arrest and cardiopulmonary bypass, and thus reducing the mortality and morbidity rate. 3
Compared with the open approach, the parallel stent-graft technique, branched and fenestrated techniques, including custom-made devices (CMD), or in situ laser fenestration have shown acceptable mortality, complication, and reintervention rates.5,6 In selected vascular centers, custom-made devices for zone 0 of aortic arch have been used; however, the waiting time of 6 to 8 weeks from manufacturing to delivery makes them unsuitable for emergent and urgent situations.5,7
One additional option is the physician-modified endografts (PMEGs) technique, which, in expert centers, delivers acceptable mortality and morbidity rates.8 –10 The current study aimed to collect all the available evidence concerning technical success and early and mid-term clinical outcomes of PMEG for the treatment of aortic arch pathologies in zones 0 to 2.
Material and Methods
Protocol and Registration
The present meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines. 11 The following medical databases were systematically searched: MEDLINE (database provider PubMed; from 1966 to May 2024), EMBASE (database provider Ovid; from 1980 to May 2024), and Google Scholar and Cochrane Central Register of Controlled Trials (May 2024). A snowball process of the reference lists of the eligible studies was performed after retrieval of the relevant reports from the search of the databases. The protocol of the present study was registered in the PROSPERO public database prior to the study initiation (CRD42024549327).
Search Method
In all the possible combinations, we used the following search terms: ([physician-modified] OR [surgeon-modified] OR [handmade] OR [back-table]) AND ([endograft] OR [stent-graft]) AND ([aortic arch] OR [zone O] OR [zone 1] OR [zone 2]) AND ([aortic aneurysm] OR [dissection]). All English-language scientific studies related to PMEGs for aortic arch pathologies reported up to May 2024 were potentially eligible. Two authors independently screened the titles and abstracts obtained from the search against the inclusion criteria. Disagreements were resolved through consensus or by discussion, with a third senior reviewer serving as final arbitrator. The full reports for all studies that appeared to meet the inclusion criteria or where there was any uncertainty were obtained. Two reviewers further analyzed the full-text articles against the study inclusion criteria, with any discrepancies resolved by discussion and/or referral to a third one of us before the data were finally analyzed. In addition, the reference lists of reviews were searched to identify further studies for inclusion. After the identification of the eligible studies, data were extracted independently by 2 authors using a pre-designed datasheet and uploaded into it following confirmation of agreement of the data.
Inclusion and Exclusion Criteria and Data Extraction
Studies reporting on patients submitted to aortic arch pathologies in zones 0 to 2 and PMEGs were included in the present meta-analysis. In addition, studies of the same surgical group that provided outcomes in different aortic arch zones were also included. All types of study designs were included if they provided procedural details and follow-up outcomes. Studies providing data for aortic arch pathologies treated with other devices (custom-made fenestrated and/or branched, or in situ laser fenestration, or parallel endografts), or stent grafts with in situ created fenestrations using needles, radiofrequency, or laser catheters were excluded. The following were also excluded: studies providing mixed data with other surgical techniques, review, or case reports/series. Studies without follow-up data were also excluded. In addition, in the case of metachronous reports from the same surgical group, only the latest report or the one with the largest number of patients was included to avoid overlapping study cases.
Data Extraction Process
The following data were extracted: first author’s name, country (where the study was undertaken), study year and design (prospective, retrospective), recruitment period, total number of patients, mean age, and number of male patients. The baseline data, including cardiovascular risk factors (ie, smoking history, hypertension, dyslipidemia, diabetes mellitus) and other comorbidities (ie, chronic obstructive pulmonary disease, history of cerebrovascular event, coronary disease, chronic renal failure), were also extracted. Moreover, data were collected regarding surgical urgency (ie, elective, emergent), type of aneurysm or dissection, other aortic pathologies, type of modified endograft, number of bridging stents, total operative, fluoroscopy time (minutes), contrast medium volume (mL), length of hospital stay, and in the intensive care unit.
Statistical Analyses
End points definition, data synthesis, and treatment effects
The outcome rates in patients undergoing PMEG implantation in the aortic arch were estimated for each study and reported as the proportion of patients with the corresponding outcome among all patients treated with PMEGs.
The main outcomes (early <30 days or late >30 days) were technical success, the mortality rate, stroke rate, bridging stent complications, and early and late reintervention. Technical success is defined as successful delivery and deployment of the PMEG, successful side branch catheterization and placement of bridging stents, patency of the PMEG and side branches, and absence of type I-III endoleaks on completion of angiography. 12 Bridging stent graft (BSG) instability was defined by any related complication, leading to aneurysm rupture, death, occlusion, component separation or reintervention to maintain BSG patency, or endoleak. 13 The stroke definition was different by the authors with the frequent being the clinical presentation of stroke, whereas only a few articles described neurological consultations or imaging to confirm the condition.
Values of the concomitant outcomes were subsequently appropriately calculated, expressed as proportions and 95% confidence intervals (CIs), and thereafter transformed into quantities according to the Freeman-Tukey variant of the arcsine square root transformed proportion. The pooled effect estimates were calculated as the back-transformation of the weighted mean of the transformed proportions, using the Der Simonian-Laird weights of random effects model and expressed as percentage proportions.
Quality assessment, heterogeneity, and publication bias
The assessment of methodologic quality of each study was assessed by 2 authors (G.I.K. and M.C.), using the Newcastle-Ottawa scale (NOS). 14 The Newcastle-Ottawa scale was developed to assess the quality of the studies using the star system (maximum of 9 stars), in which a study was judged using 3 broad perspectives: (1) selection of the study groups; (2) comparability of the groups; and (3) ascertainment of the outcome of interest. We used a formal statistical test for heterogeneity (I 2 test). Overall study risk of bias was deemed as high, some concerns, or low according to the NOS score and plots created using the risk-of-bias visualizations (ROBINS-I) tool (Supplementary Figure 1). 15 Studies were deemed to be at high risk of bias overall if any domain (selection criteria, comparability, or outcome) received a high risk of bias rating. In addition, the risk of bias was assessed by visual inspection of funnel plots and using the Egger regression test. The Comprehensive Meta-analysis statistical software, version V4 (Englewood, New Jersey), was used for analysis.
Results
Identification of Relevant Studies
A total of 134 study titles were identified by the initial search strategy. The review of titles and abstracts revealed that 90 studies were irrelevant at the first screening stage. An additional 44 reports were evaluated further. Of the eligible studies, 30 were excluded for one or more of the following reasons: studies providing mixed outcomes with other endovascular techniques (n=3); studies providing no follow-up data (n=2); review (n=1); case reports or series (n=8); irrelevant (n=1); no English studies (n=1); and studies with duplicated data (n=14). Finally, after applying these exclusions, 14 studies (zone 0 n=6; zone 1 n=1; zones 1-2: n=7)10,16 –28 with an overall 777 patients were identified as potentially eligible for inclusion in the systematic review and meta-analysis (Figure 1). In addition, in the current meta-analysis are included studies from the same surgical group; however, they described the outcomes of interest in different aortic arch zones each time.10,16,20,21,23,26 –28 Moreover, the only study 16 that reported outcomes in zone 1 was incorporated with the others studies, which reported mixed outcomes for zones 1 to 2. All the eligible studies included in the present meta-analysis are presented in Table 1.
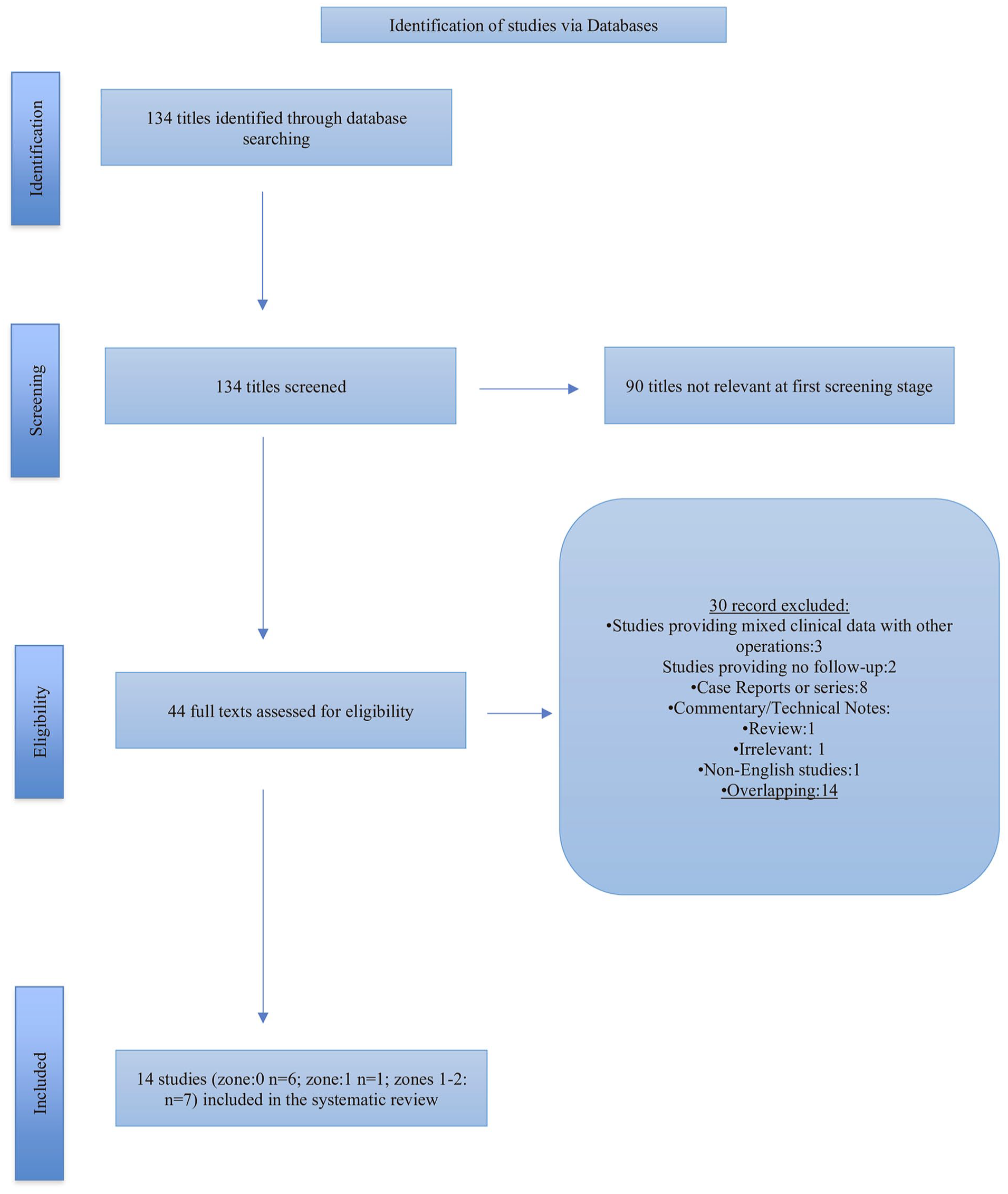
Study flow chart (“Preferred Reporting Items for Systematic Reviews and Meta-Analysis” diagram).
Baseline Characteristics of the Eligible Studies.
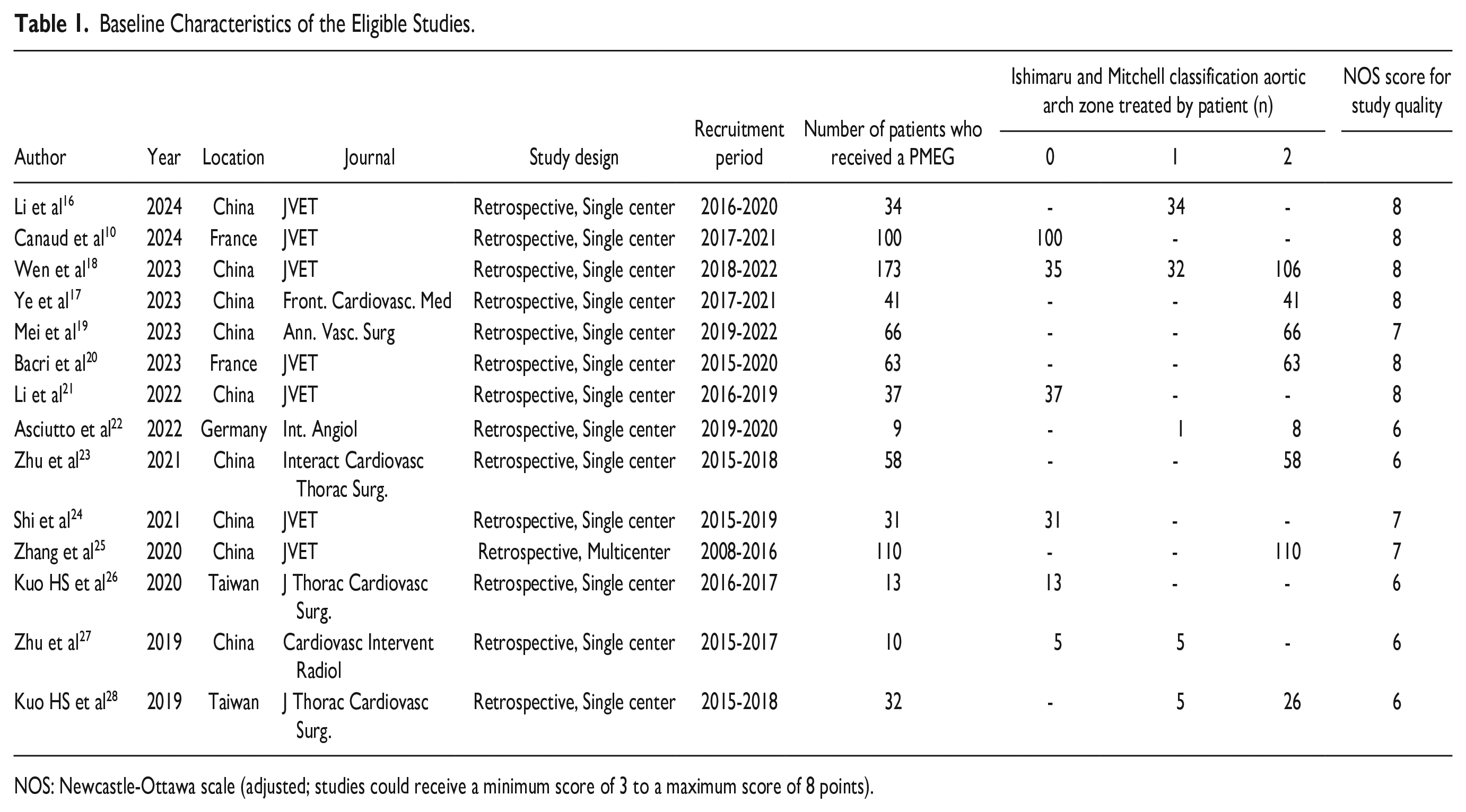
NOS: Newcastle-Ottawa scale (adjusted; studies could receive a minimum score of 3 to a maximum score of 8 points).
Study Characteristics
The baseline study characteristics of the 14 eligible studies10,16 –28 including the current systematic review are presented in Table 1. Of these, 6 studies10,18,21,24,26,27 reported outcomes in zone 0, whereas 8 studies16,17,19,20,22,23,25,28 in zones 1 to 2 of the aortic arch, of these 1 study for zone 1 and 7 studies for zone 2. The included studies had been reported from 2019 to 2024. Of the 777 patients (zone 0; n=364; 67±4 years; zones 1-2; n=413; 59±4 years) included in our systematic review, 618 (80%) were men. The mean age ranged from 54 to 73 years. Of them, 75% (580 of 777) had hypertension, 18% (140 of 777) had coronary artery disease, 12% (98 of 777) dyslipidemia, 11% (85 of 777) chronic kidney disease, and 10% diabetes (77 of 777), whereas 30% (234/777) were active smokers.
The most common indication for treatment was dissection in 57% (60% in zone 0, 40% in zones 1-2) of the cases (446 of 777). Of them, 58% (259 of 446) were after type B aortic dissection, 24% (108 of 446) residual type A dissection, and 11% (47 of 446) type A, whereas 7% (32 of 446) non-A and non-B. In addition, 33% (261/777) of the cases were aneurysms, of whom 47% limited in zone 0 and 53% limited in zones 0 to 2. Other aortic arch pathologies have been recorded in 7% (88% in zone 0; 12% in zones 1-2), whereas type Ia endoleak in 3% (77% zone 0; 23% zones 1-2) after previous thoracic endovascular aortic repair. Of the procedures, 85% had been elective, 12% had been emergent, and 3% had been urgent.
Regarding the PMEG deployment in aortic arch zones, 28% were deployed in sealing zone 0, 10% in sealing zone 1, and 62% in the zone 2. The most common modified device was the Valiant (53%) (Medtronic Vascular, Santa Rosa, California), followed by Ankura (31%) (LifeTech, Shenzhen, China), Bolton Relay (10%) (Terumo Corporation, Vascutek Ltd, Inchinnan, UK), and Zenith ZTEG (6%) (Cook Medical Inc, Bloomington, Indiana).
An overall number of 768 BSGs were used for perfusion of the supra-aortic vessels. Of them, 107 (14%) for the innominate artery, 160 (21%) for the left common carotid artery, and 501 (65%) for the left subclavian artery. The most common BSG used was the Fluency (n=214; Bard Peripheral Vascular, Tempe, Arizona),16,18,25 between the eligible studies followed from Viabahn (n=64; W.L. Gore & Associates, Flagstaff, Arizona),16,18,25 Lifestream (n=37; Bard), 20 VBX (n=16; W.L. Gore & Associates),22,25 and Omnilink Elite (n=16; Abbott Vascular, Santa Clara, California).18,20,25 One study reported the use of Endurant (Medtronic Vascular), and Ankura Iliac limb extension (n=3; LifeTech). 18 However, most of the eligible studies (65%) had not provided additional data.
The mean operative time ranged from 79 to 207 minutes (zone 0=85-207 minutes; zones 1-2=79-188 minutes), the mean fluoroscopy time ranged from 18 to 49 minutes (zone 0=20-49 minutes; zones 1-2=18-30 minutes), whereas the contrast medium ranged from 69 to 165 mL (zone 0=82 to 165 mL; zones 1-2=69-153). The mean length of stay ranged from 5 to 15 (zone 0=8-15 days; zones 1-2=5-15 days) days, and intensive care unit stay ranged from 1 to 14 days (zone 0=1-14 days; zones 1-2=1-3 days). The mean follow-up ranged from 12 to 52 months (zone 0=11-28 months; zones 1-2=12-52 months).
Meta-Analysis
Main Outcomes
Prevalence of technical success
The pooled technical success for the PMEG in zone 0 was 96.6% (95% CI=93.9%-98.2%, Figure 2A) in 6 studies.10,18,21,24,26,27 The publication bias was not significant (coefficient=0.12; standard error [SE]=1.07; p=0.90). In zones 1 to 2, the prevalence of technical success was 95.9% (95% CI=92.9%-97.6%, Figure 2B) in 8 studies.16,17,19,20,22,23,25,28 The publication bias was significant (coefficient=2.62; SE=0.71; p=0.03).
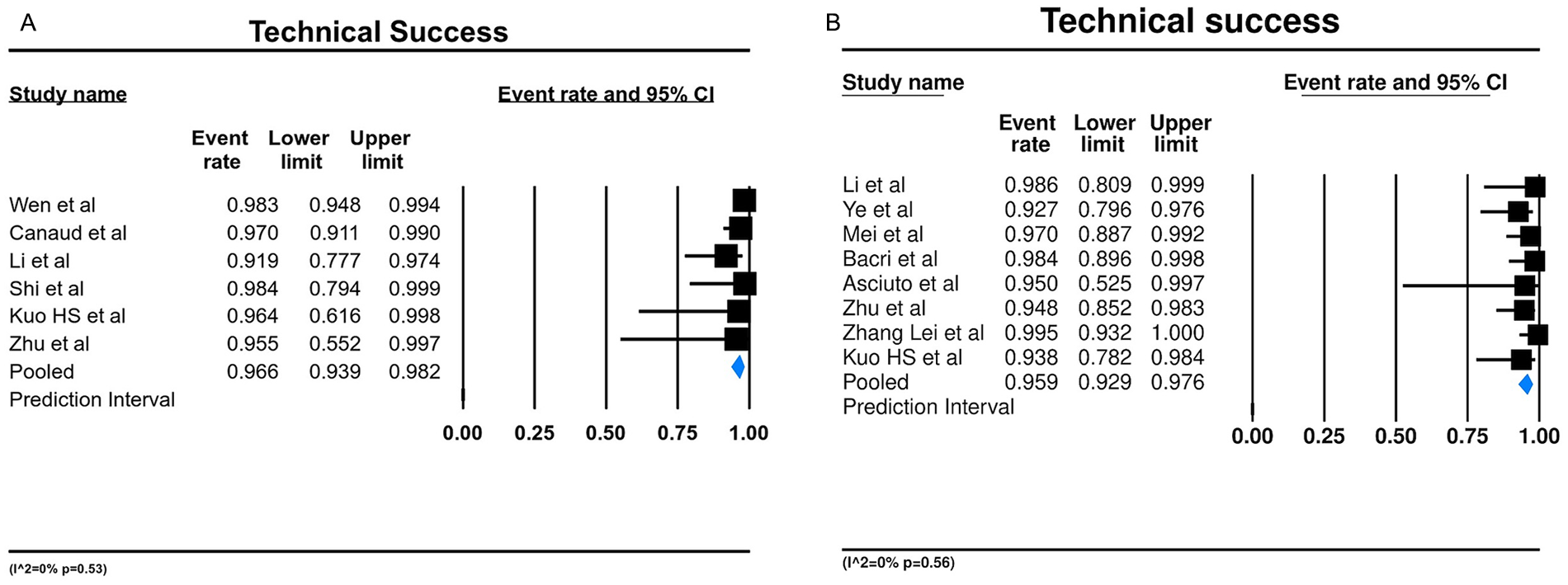
Forest plot presenting the meta-analysis of technical success rate for (A) zone 0 and (B) zones 1 to 2. Event rates in the individual studies presented as squares, with 95% confidence interval (CIs) presented as extending lines. The pooled event rate with its 95% CI is depicted as a diamond. ES, effect estimate.
Prevalence of mortality
The pooled 30-day mortality was 4.6% (95% CI=2.0%-10%, Figure 3A) in zone 0 among the eligible studies.10,18,21,24,26,27 No significant publication bias was recorded (coefficient=0.12; SE=2.15; p=0.90). For the zones 1 to 2, the pooled 30-day mortality rate was 4.3% (95% CI=2.2%-8.2%, Figure 3B).16,17,19,20,22,23,25,26 The publication bias was significant (coefficient=3.39; SE=0.68; p=0.01).
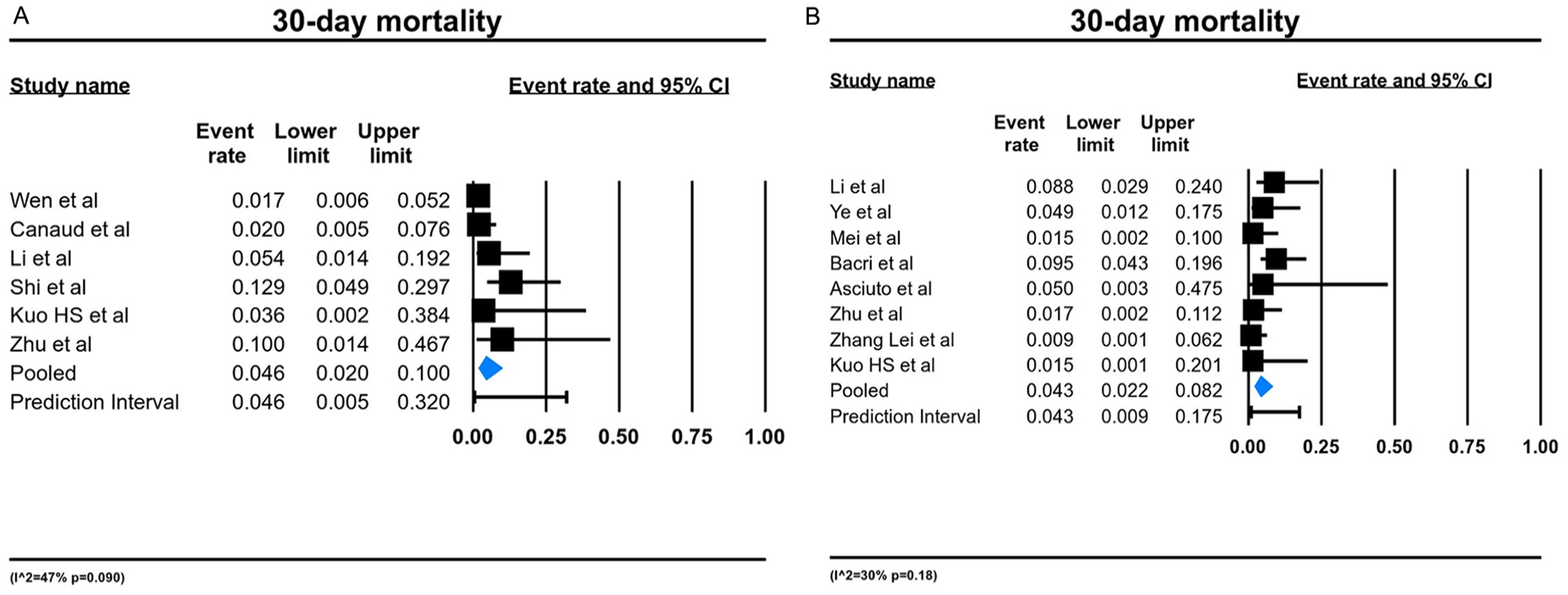
Forest plot presenting the meta-analysis of 30-day mortality for (A) zone 0 and (B) zones 1 to 2. Event rates in the individual studies presented as squares, with 95% confidence interval (CIs) presented as extending lines. The pooled event rate with its 95% CI is depicted as a diamond. ES, effect estimate.
Prevalence of stroke
The pooled rate of stroke was 3.7% (95% CI=2.1%-6.4%, Figure 4A) in zone 0 in 6 studies.10,18,21,24,26,27 The publication bias was not significant (coefficient=0.48; SE=0.96; p=0.65). The prevalence of stroke in zones 1 to 2 was 2.7% (95% CI=1.4%-5%, Figure 4B) in 8 studies.16,17,19,20,22,23,25,28 No significant publication bias was recorded (coefficient=1.71; SE=0.64; p=0.13).
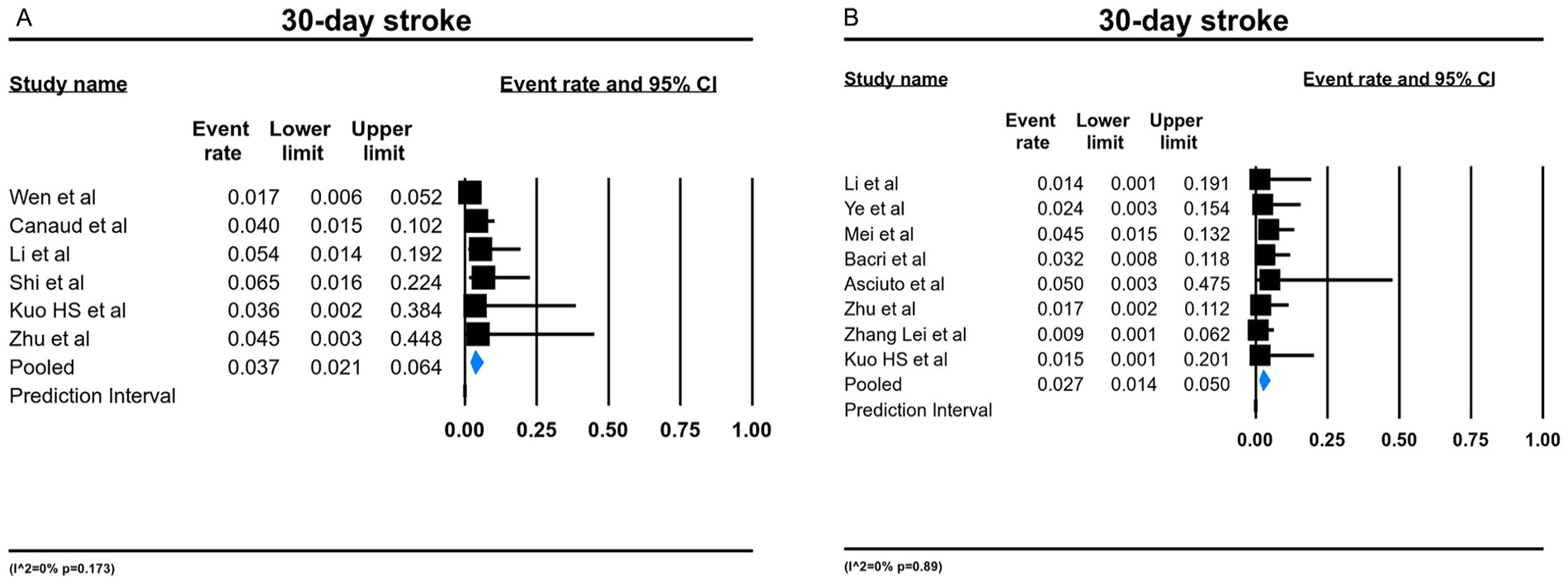
Forest plot presenting the meta-analysis of 30-day stroke rate for (A) zone 0 and (B) zones 1 to 2. Event rates in the individual studies presented as squares, with 95% confidence interval (CIs) presented as extending lines. The pooled event rate with its 95% CI is depicted as a diamond. ES, effect estimate.
Secondary Outcomes
Prevalence of 30-day reintervention rate
The pooled 30-day reintervention prevalence was 3.5% (95% CI=1.5%-8.0%, Figure 5A) for zone 0 of the aortic arch in 6 studies.10,18,21,24,26,27 The publication bias was not significant (coefficient=1.53; SE=0.85; p=0.86). In the zones 1 to 2, the pooled 30-day reintervention rate was 4.2% (95% CI=2.4%-7.2%, Figure 5B) among the eligible studies.16,17,19,20,22,23,25,28 The publication bias was not significant (coefficient=1.93; SE=0.77; p=0.10).
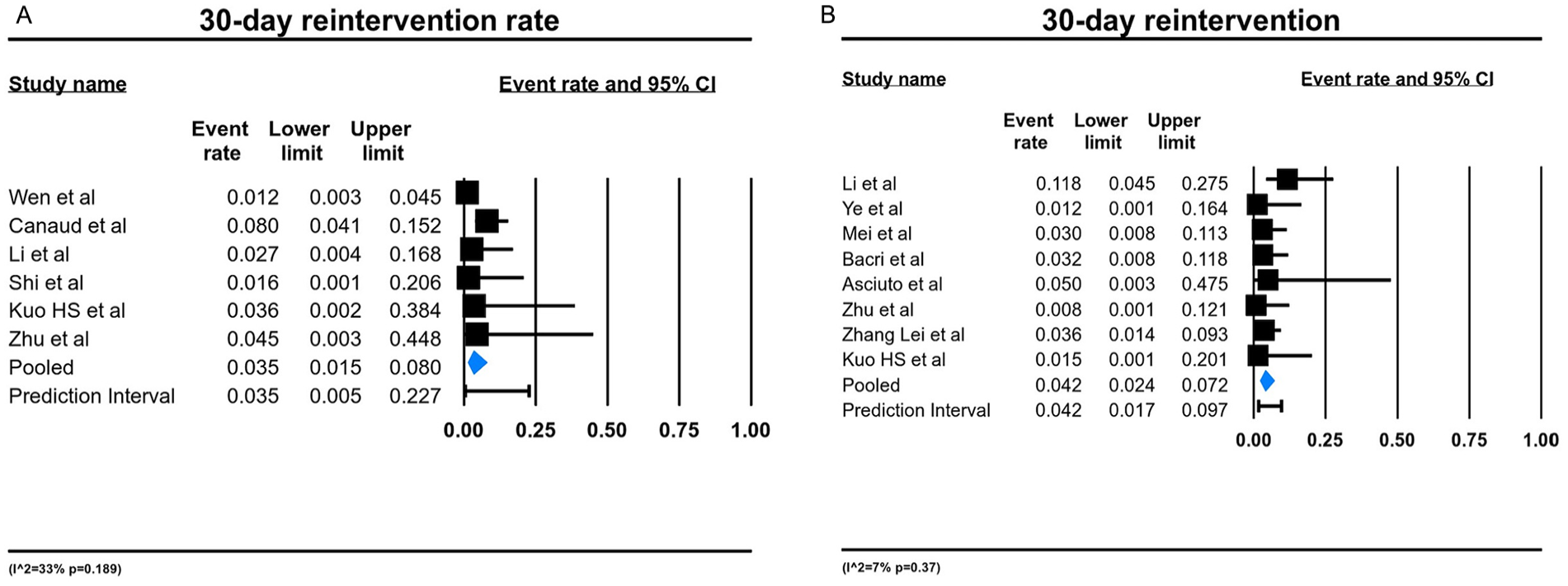
Forest plot presenting the meta-analysis of 30-day reintervention rate for (A) zone 0 and (B) zones 1 to 2. Event rates in the individual studies presented as squares, with 95% confidence interval (CIs) presented as extending lines. The pooled event rate with its 95% CI is depicted as a diamond. ES, effect estimate.
Prevalence of late mortality
The late mortality rate was 8.2% (95% CI=4.7%-14%, Supplementary Figure 2a) for zone 0.10,18,21,24,26,27 The publication bias was not significant (coefficient=0.54; SE=1.66; p=0.61). For the zones 1 to 2, the pooled rate of late mortality was 3.4% (95% CI=1.9%-6%, Supplementary Figure 2b). The publication bias was not significant (coefficient=1.64; SE=0.80; p=0.15).16,17,19,20,22,23,25,28
Prevalence of late reintervention
The pooled late reintervention rate was 8.5% (95% CI=3.0%-21%, Supplementary Figure 3a) for zone 0 in 6 studies.10,18,21,24,26,27 The publication bias was not significant (coefficient=0.18; SE=2.21; p=0.86). The pooled late reintervention rate was 1.9% (95% CI=0.8%-4.3%, Supplementary Figure 3b) for zones 1 to 2 among the eligible studies.16,17,19,20,22,23,25,28 The publication bias was not significant (coefficient=2.15; SE=1.54; p=0.07).
Prevalence of bridging stent instability
The pooled bridging stent instability rate was 3.9% (95% CI=1.1%-12.9%, Supplementary Figure 4a) in zone 0 in 6 studies.10,18,21,24,26,27 The publication bias was not significant (coefficient=1.14; SE=1.98; p=0.51). The prevalence of bridging stent instability for zones 1 to 2 was 3.2% (95% CI=1.8%-5.8%, Supplementary Figure 4b). No significant publication bias was recorded in the eligible studies (coefficient=1.75; SE=0.61; p=0.13).
Discussion
In the current systematic review and meta-analysis, we identified all published studies that reported on the outcomes of PMEG devices for the treatment of aortic arch pathologies. Our aim was to present an update on PMEG since the last published international guidelines by the European Society of Vascular Surgery and the European Association of Cardiothoracic Surgery. 3 These guidelines reported that patients unfit for open surgery and with suitable anatomy, requiring a zone 0 treatment, should be considered for endovascular aortic arch repair (recommendation 30, class IIa, level B). 3
An endovascular approach provides an alternative for high-risk patients who need treatment in the aortic arch, offering acceptable outcomes. De Rango et al 29 reported comparable outcomes regarding the perioperative mortality and stroke rates between open surgical repair and endovascular aortic arch repair. Recently, a multicenter study reported excellent results on 3 inner-branch custom-made devices. 30 The technical success rate was 100%, whereas the early mortality and stroke rate were 5%, respectively. These outcomes have recently been supported by another meta-analysis relying on the fenestrated and branched custom devices. 6 Despite these encouraging outcomes, custom-made devices are hampered by the lengthy manufacturing duration (6-8 weeks) and are unsuitable in emergent and urgent situations. In addition, their high cost and limited availability in many countries pose challenges. 18
Physician-modified endografts represent an alternative, off-label, option in the endovascular armamentarium are available for emergent cases, eliminating several drawbacks of open surgery, such as the need for hypothermic circulatory arrest or cardiopulmonary bypass, which can be dreadful for high-risk patients.
Concerning our primary endpoints, technical success was 96.6% in zone 0 and 95.9% in zones 1 to 2. These outcomes coincide with those reported recently of custom-made fenestrated and branched endografts (95.9%); however, in this study, the authors did not provide data separately for zone 0 and zones 1 to 2. 6 On the contrary, in experienced hands, the technical success of the PMEG could be higher reaching up to 98%.18,20 Canaud et al 10 reported their outcomes using PMEG with double fenestrations in 100 patients in zone 0. The technical success was 97% in this series. In the same trend, one more study for zone 0 confirmed an excellent technical success rate of 98%. 18 The authors attributed this high rate to device design, careful performance, and some technical details such as the stent alignment and the cardiac output reduction. 18 In addition, they proposed that the stent alignment is the “key” for PMEG performance. The long distance between the femoral artery and aortic arch, as well as the curvature of the arch, made the alignment difficult. For this reason, the authors proposed that during the delivery of the stent graft, the front grip should be kept fixed and the fenestration always faced on the same side. 18 Moreover, to achieve high technical success, a significant role is played by maneuvers that reduce the cardiac output, enabling accurate deployment for the graft. These maneuvers, including rapid ventricular pacing, pharmacological hypotension, inferior vena cava balloon occlusion, transient adenosine-induced cardiac asystole, and the Munich Valsalva Implantation Technique, have shown promising results and are considered excellent adjuncts for the deployment of the endograft to the aortic arch.31,32
The pooled 30-day mortality rate in the current study was 4.6% after treatment in zone 0 and 4.3% after treatment in zones 1 to 2. Comparing these results with open surgical repair, some studies reported an 11% perioperative mortality rate after total aortic arch replacement.2,33,34 This rate was observed in experienced centers with a high volume of daily cases; in less experienced hands, the rate might be higher. Similarly, a recently-published study comparing OSAAR with debranching hybrid surgical aortic arch repair found a pooled rate of 10% for both techniques, despite the fact that OSAAR includes younger patients. 35 These figures may highlight that although the PMEG technique is not widely adopted yet and probably is in a learning curve period, it may offer an early advantage to high-risk patients.10,20
Of interest were our results regarding the late mortality rate between the zone 0 and zones 1 to 2. In zone 0, the late pooled mortality rate was 8.2% compared with 1.5% in zones 1 to 2. Considering that the zone 0 group included older patients and data on aortic-related mortality or potential risks, such as frailty and/or malignancy are absent from the eligible studies, it was not possible to draw safety conclusions.
The most dreadful event during an endovascular treatment in the aortic arch is the stroke. It has been reported in rates between 0% and 14% with the most known mechanisms to be the solid emboli released after manipulation in the aortic arch, air emboli released from the delivery system, and coverage of the arch vessels.3,36,37 In the present study, the pooled rate was 3.7% for zone 0 and 2.7% for zones 1 to 2. However, an isolated higher (6.5%) rate has also been recorded. 24 In the same trend was also the stroke rate after custom-made fenestrated and branch devices. 6 In 18 eligible articles with 571 patients, the pooled stroke rate was 6.2%. To overcome this significant rate, carotid protection devices have been proposed. Some reports have indicated their use in patients at high risk of stroke, and no neurological deficits occurred after the procedure.38,39 However, these results are still limited only in case reports, and robust data are missing to establish their benefit.
Endoleak detection represents the “Achille heels” of the endovascular repair that leads to high reintervention rates. In another meta-analysis conducted a few years ago, the early reintervention rate was 9% for the custom-made devices. 40 The authors attributed this rate to the presence of type Ia endoleak and the progression of aortic disease, which necessitated extension of the covering length. In our study, the early reintervention rate was similar (3.5% vs 4.2%) between zone 0 and zones 1 to 2. Of interest remained the higher late reintervention rate of 8.5% in zone 0 and at 1.9% in zones 1 to 2. This may reflect the fact that covering a higher aortic arch requires more manipulations and the use of more bridging stents than in the distal aortic arch. In addition, the aortic arch pathology seems to be steadily developing and is linked to the point at which the endograft will be deployed within the aortic arch.
Limitations
The current study had several limitations, mainly mirroring the limitations of the included studies. First, most of the studies were retrospective, whereas none of them reported how missing data were managed. As a result, the findings of the current review should be evaluated with caution as the quality of the included studies may have affected the outcomes of this analysis. Second, due to the lack of standardization of the technique, various aortic endografts and bridging stents were used. This heterogeneity may either overestimate or underestimate the current results. Larger studies employing only 1 type of modified stent grafts and bridging stents may be necessary to draw definitive conclusions regarding the safety of the technique. Third, strong heterogeneity can be found in the reasons for intervention: different pathologies were included, but separated data on the outcomes were not available; hence, further analysis should be undertaken to better analyze different clinical entities. Finally, outcomes of patients with proximal landing zone 0 have been collected, but comparisons could not be made, because separated data for zone 1 and 2 cases could not be retrieved, highlighting the need for dedicated studies for each landing zone, which could be performed.
Conclusions
Endovascular repair of aortic arch pathologies using PMEGs seems to present a satisfactory level of technical success together with a progressively-reduced load in terms of early death. Their application in the distal aortic arch seems to present more favorable outcomes regarding late reintervention and mortality rates. The available evidence still reflects findings from specialized centers and is constrained by numerous limitations. To attain clearer conclusions, further research employing randomized controlled trials, longer-term follow-up, and consistent reporting of results is warranted.
Supplemental Material
sj-jpeg-1-jet-10.1177_15266028241292485 – Supplemental material for Endovascular Repair of Aortic Arch Zones 0 to 2 Using Physician-Modified Endografts: A Systematic Review and Meta-Analysis
Supplemental material, sj-jpeg-1-jet-10.1177_15266028241292485 for Endovascular Repair of Aortic Arch Zones 0 to 2 Using Physician-Modified Endografts: A Systematic Review and Meta-Analysis by Georgios I. Karaolanis, Vladimir Makaloski, Silvan Jungi, Mevlut Celik, Michel J. Bosiers and Drosos Kotelis in Journal of Endovascular Therapy
Supplemental Material
sj-jpg-2-jet-10.1177_15266028241292485 – Supplemental material for Endovascular Repair of Aortic Arch Zones 0 to 2 Using Physician-Modified Endografts: A Systematic Review and Meta-Analysis
Supplemental material, sj-jpg-2-jet-10.1177_15266028241292485 for Endovascular Repair of Aortic Arch Zones 0 to 2 Using Physician-Modified Endografts: A Systematic Review and Meta-Analysis by Georgios I. Karaolanis, Vladimir Makaloski, Silvan Jungi, Mevlut Celik, Michel J. Bosiers and Drosos Kotelis in Journal of Endovascular Therapy
Supplemental Material
sj-jpg-3-jet-10.1177_15266028241292485 – Supplemental material for Endovascular Repair of Aortic Arch Zones 0 to 2 Using Physician-Modified Endografts: A Systematic Review and Meta-Analysis
Supplemental material, sj-jpg-3-jet-10.1177_15266028241292485 for Endovascular Repair of Aortic Arch Zones 0 to 2 Using Physician-Modified Endografts: A Systematic Review and Meta-Analysis by Georgios I. Karaolanis, Vladimir Makaloski, Silvan Jungi, Mevlut Celik, Michel J. Bosiers and Drosos Kotelis in Journal of Endovascular Therapy
Supplemental Material
sj-jpg-4-jet-10.1177_15266028241292485 – Supplemental material for Endovascular Repair of Aortic Arch Zones 0 to 2 Using Physician-Modified Endografts: A Systematic Review and Meta-Analysis
Supplemental material, sj-jpg-4-jet-10.1177_15266028241292485 for Endovascular Repair of Aortic Arch Zones 0 to 2 Using Physician-Modified Endografts: A Systematic Review and Meta-Analysis by Georgios I. Karaolanis, Vladimir Makaloski, Silvan Jungi, Mevlut Celik, Michel J. Bosiers and Drosos Kotelis in Journal of Endovascular Therapy
Footnotes
Authors’ Note
The protocol of the present study was registered in the PROSPERO public database prior to the study initiation (CRD42024549327). Two authors (G.I.K. and M.C.) independently screened the titles and abstracts obtained from the search against the inclusion criteria. Disagreements were resolved through consensus or by discussion, with a third senior reviewer (V.M.) serving as final arbitrator. Two reviewers (G.I.K. and M.C.) further analyzed the full-text articles against the study inclusion criteria, with any discrepancies resolved by discussion and/or referral to a third one of us (V.M.) before the data were finally analyzed. After the identification of the eligible studies, data were extracted independently by 2 authors (G.I.K. and M.C.) using a pre-designed datasheet and uploaded into it following confirmation of agreement of the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.