
Abstract
Background:
The aim of this study is to explore the value of different systemic inflammatory response indicators in the long-term prognosis of type B aortic dissection (TBAD) patients undergoing thoracic endovascular aortic repair (TEVAR).
Methods:
This study retrospectively reviewed the case data of 540 patients with TBAD at our center from January 2013 to January 2019. Based on the occurrence of aorta-related adverse events (ARAEs) during follow-up, patients were divided into two groups: the ARAEs group and the non-ARAEs group. Univariate and multivariate analyses identified preoperative systemic inflammatory response index (SIRI) and C-reactive protein-to-albumin ratio (CAR) as independent risk factors for ARAEs. The SIRI-CAR score was then developed using these indicators. Receiver operating characteristic (ROC) curve analysis was employed to determine the optimal thresholds for SIRI and CAR in predicting ARAEs, then allowing for the classification of patients into high and low groups. Kaplan-Meier survival curves were used to compare survival status among patients with different SIRI, CAR, and SIRI-CAR score during follow-up, while cumulative hazard curves were used to assess the risk of various types of ARAEs among patients with differing SIRI-CAR scores.
Results:
In this study, 127 patients experienced ARAEs during follow-up. Univariate and multivariate analyses identified preoperative SIRI and CAR as independent risk factors for ARAEs. ROC curve analysis showed that the SIRI-CAR score provided superior predictive value for ARAEs compared to using SIRI and CAR separately. Kaplan-Meier survival curves revealed significantly lower ARAE-free survival rates in patients with high SIRI, high CAR, and high SIRI-CAR scores during follow-up. Additionally, cumulative hazard curves highlighted significant differences in the risk of various ARAEs among patients with different SIRI-CAR score, with the risk increasing as the score rose.
Conclusion:
Preoperative SIRI and CAR are associated with the long-term prognosis of TBAD patients undergoing TEVAR, demonstrating good prognostic value. Additionally, the SIRI-CAR score, which combines both indicators, can more effectively predict the risk of long-term ARAEs.
Clinical Impact
This study provides valuable insights into the role of systemic inflammatory response indicators in predicting the long-term prognosis of TBAD patients undergoing TEVAR). By identifying key inflammatory biological indicators, clinicians can better stratify risk, personalize treatment, and monitor post-operative recovery more effectively. The incorporation of these indicators into clinical practice could enhance early intervention strategies, improve patient outcomes, and potentially reduce complications. The innovation lies in the focus on inflammatory responses, offering a novel prognostic tool to guide management decisions for these high-risk patients.
Keywords
Introduction
With the rapid development of minimally invasive intervention techniques, thoracic endovascular aortic repair (TEVAR) has become the preferred treatment for the majority of type B aortic dissection (TBAD).1,2 Despite the minimal trauma and rapid postoperative recovery associated with TEVAR, it is inevitable that some serious postoperative complications may occur, which could have a certain impact on patient prognosis. Therefore, the prognostic outcomes of TBAD patients still require more attention.
Over the past few decades, an increasing number of studies have confirmed the value of biological indicators in disease diagnosis and prognosis. Consequently, many indicators have been widely applied in clinical diagnosis and treatment. 3 Research on the prognosis of TEVAR has been more focused on the anatomical and morphological characteristics of the aortic vasculature, as well as changes in imaging findings during follow-up.4 –7 In recent years, many studies have begun to elucidate the potential associations between certain key pathophysiological changes in the pathogenesis of aortic dissection (AD) and its prognosis, particularly inflammation response.8,9 Inflammation response, as one of the most crucial pathophysiological changes during the occurrence of AD, exerts a significant influence on the pathogenesis of AD. Many research findings have also indicated a close relationship between the systemic inflammatory response level in AD patients and their prognosis.10–12
Biological indicators of systemic inflammatory response include C-reactive protein (CRP), neutrophils, lymphocytes, monocytes, and platelets, while albumin level is also considered part of systemic inflammatory response. There are currently many inflammation scoring systems constructed based on these biological indicators. One type is an inflammation scoring system based on CRP and albumin, such as the CRP-to-albumin ratio (CAR). Another type is based on peripheral blood cell counts, such as neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), monocyte-to-lymphocyte ratio (MLR), systemic immune inflammation index (SII), and systemic inflammatory response index (SIRI). Both types of systemic inflammatory response indicators have been shown to effectively predict the prognosis of various tumors and cardiovascular diseases.13–20
However, the value of different systemic inflammatory response indicators in the prognosis of patients with TBAD undergoing TEVAR has not been clearly elucidated, and it remains unclear whether their individual or combined application can increase predictive efficacy. Therefore, this study aimed to investigate the potential value of different systemic inflammatory response indicators in the long-term prognosis of TBAD patients undergoing TEVAR.
Materials and Methods
Study Population
The study included TBAD patients who undergoing TEVAR consecutively at our center from January 2013 to January 2019. Inclusion criteria were as follows: (1) age>18 years, (2) diagnosis of type B aortic dissection confirmed by thoracoabdominal computed tomography aortography (CTA), (3) undergoing TEVAR treatment. Exclusion criteria were: (1) TBAD patients who had previously underwent open surgical or hybrid surgical treatment, (2) pre-existing conditions affecting the count of inflammatory response indicators, such as malignancies, hematological disorders, systemic autoimmune diseases, and long-term use of anti-inflammatory or immunosuppressive therapy, (3) patients with significant data missing.
Definition of Systemic Inflammatory Response Indicators
The CAR is defined as the ratio of CRP count to albumin count. The NLR is defined as the neutrophil count by the lymphocyte count. The MLR is defined as the monocyte count by the lymphocyte count. The PLR is defined as the platelet count by the lymphocyte count. The SII is defined as the platelet count multiplied by NLR. The SIRI is defined as the monocyte count multiplied by NLR. Blood samples were collected from all patients prior to medication for blood tests.
Outcomes Ascertainment
The endpoints during follow-up included all-cause mortality, aorta-related mortality, and aortic complications requiring reintervention. ARAEs included stent-related complications (stent stenosis, occlusion, migration), abdominal organ or lower limb ischemia, aortic expansion >5 mm, and formation of an entry flow (type I, II, R), reintervention and death during follow-up. The entry flow was defined according to the criteria specified by the Society for Vascular Surgery. 21 All data were obtained from the hospital’s electronic medical record system. Follow-up data was assessed based on the final medical records or telephone or Wechat interviews.
Data Collection
All clinical data were collected by two experienced clinicians: one was responsible for entering data from the electronic medical records system, while the other conducted random checks. Preoperative clinical variables included demographic data (sex, age, body mass index), preoperative risk factors and comorbidities (hypertension, diabetes, etc.), and preoperative laboratory results (leukocyte, neutrophil, monocyte, lymphocyte, etc.). Follow-up data included follow-up time, survival status, reintervention, false lumen thrombosis condition, and the occurrence of ARAEs (aortic expansion >5 mm, abdominal organ or lower limb ischemia, stent-related complications, and entry flow).
Statistical Analysis
Data were analyzed using SPSS (version 25.0, IBM, USA) and R (version 4.2.1). In univariate analysis, continuous variables were expressed as mean ± standard deviation or median (interquartile range) and compared using Student’s t-test or Mann-Whitney U-test. Categorical variables were expressed as frequencies or percentages and compared using chi-square tests or Fisher’s exact tests. Receiver operating characteristic (ROC) curve analysis determined the optimal thresholds for continuous variables. Independent risk factors for postoperative ARAEs were identified using Cox proportional hazards regression analysis, with variables having p<0.1 in univariate analysis further included in multivariate analysis. Kaplan-Meier survival curves were used for survival analysis, cumulative hazard curves assessed risk probabilities, and the Log-rank test was applied for comparisons. A two-sided p<0.05 was considered statistically significant.
Results
Comparison of Preoperative Clinical Characteristics Between the two Groups
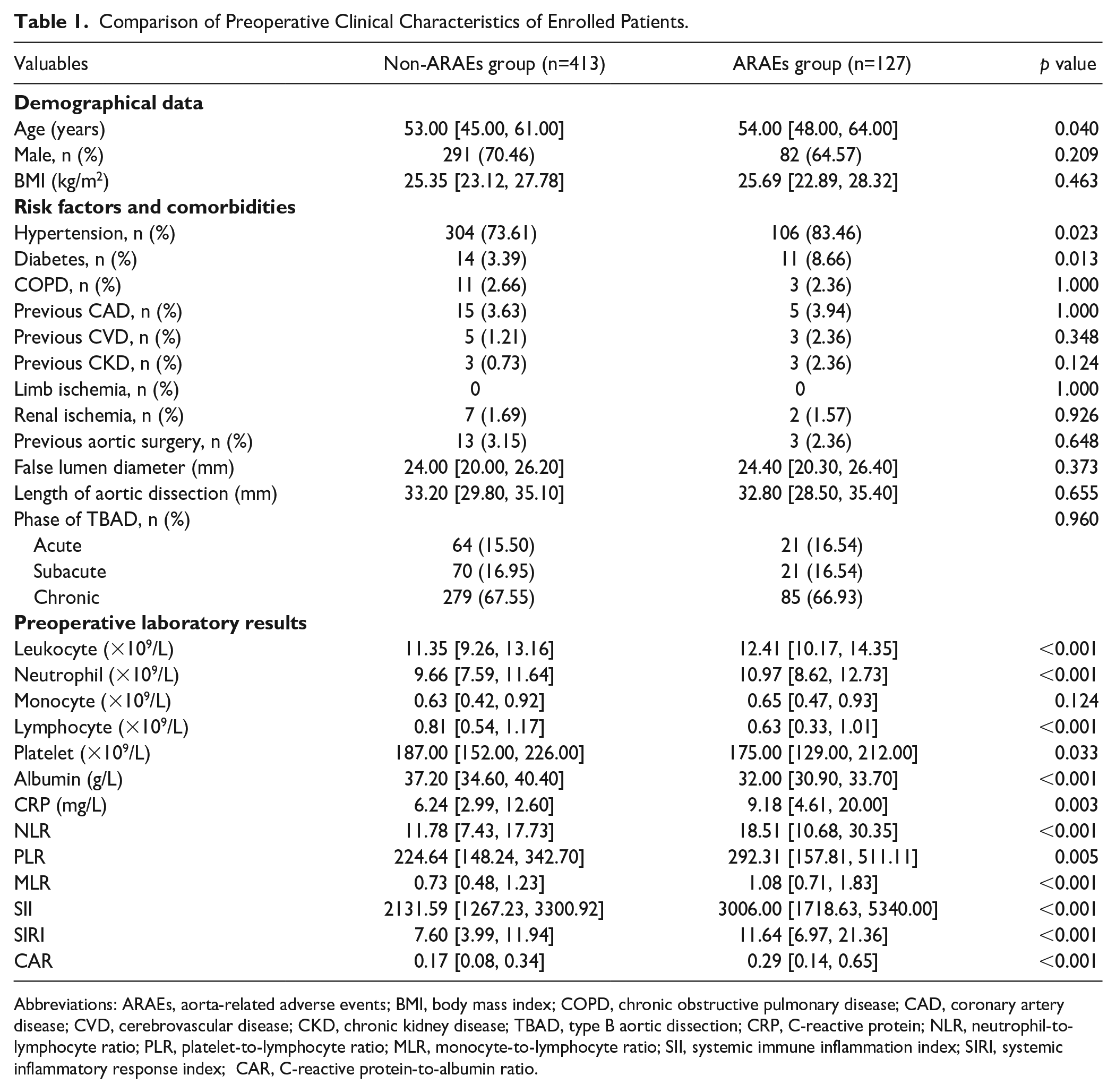
The inclusion and exclusion process is illustrated in Figure 1. A total of 540 TBAD patients who undergoing TEVAR were included in the study, with an average age of 53.10 ± 10.28 years, and 69.1% of the patients were male. During the follow-up, 127 patients experienced ARAEs, with an average median follow-up duration of 67.00 (50.00, 86.00) months. Univariate analysis results indicate that patients in the ARAEs group were older [54.00 (48.00, 64.00) vs 53 (45.00, 61.00)] with higher preoperative comorbidities of hypertension (83.46% vs 73.61%) and diabetes (8.66% vs 3.39%). Laboratory results showed that patients in the ARAEs group had significantly higher preoperative white blood cell and neutrophil counts, elevated CRP levels, as well as significantly lower lymphocyte and platelet counts, and reduced serum albumin levels (Table 1).
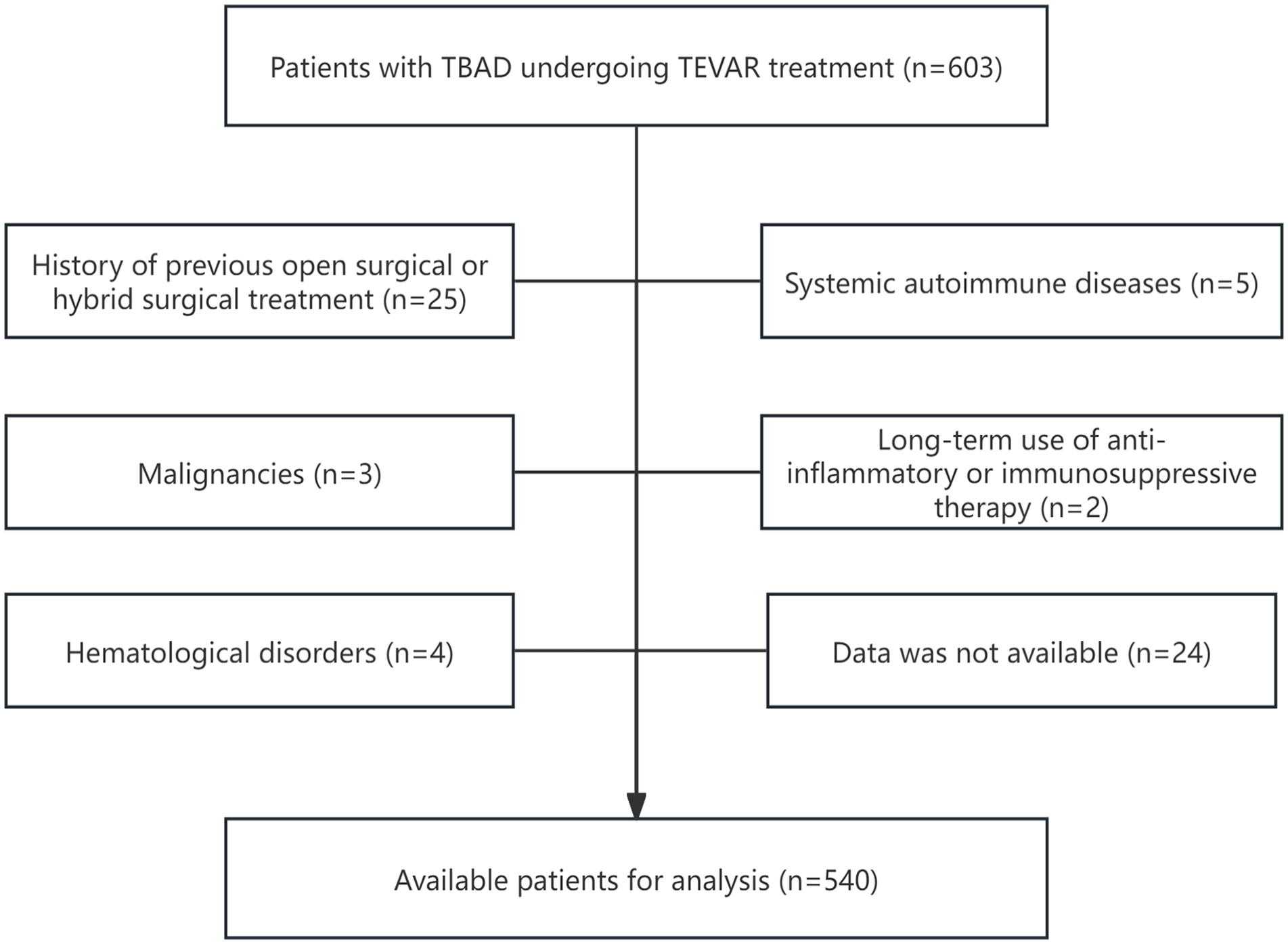
Flowchart of the patients’ inclusion and exclusion.
Comparison of Preoperative Clinical Characteristics of Enrolled Patients.
Abbreviations: ARAEs, aorta-related adverse events; BMI, body mass index; COPD, chronic obstructive pulmonary disease; CAD, coronary artery disease; CVD, cerebrovascular disease; CKD, chronic kidney disease; TBAD, type B aortic dissection; CRP, C-reactive protein; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; MLR, monocyte-to-lymphocyte ratio; SII, systemic immune inflammation index; SIRI, systemic inflammatory response index; CAR, C-reactive protein-to-albumin ratio.
Cox Proportional Hazards Regression Analyses and Subgroup Analysis of ARAEs
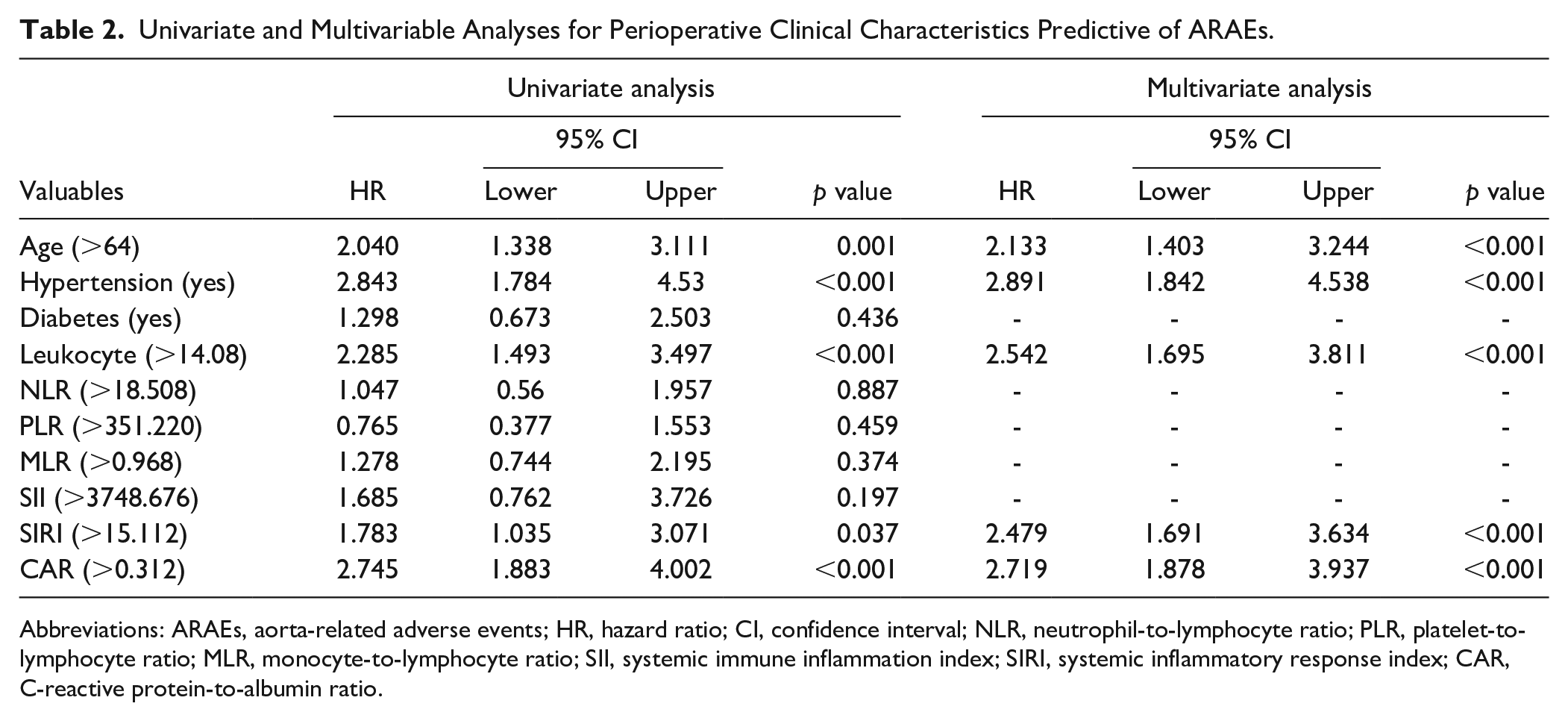
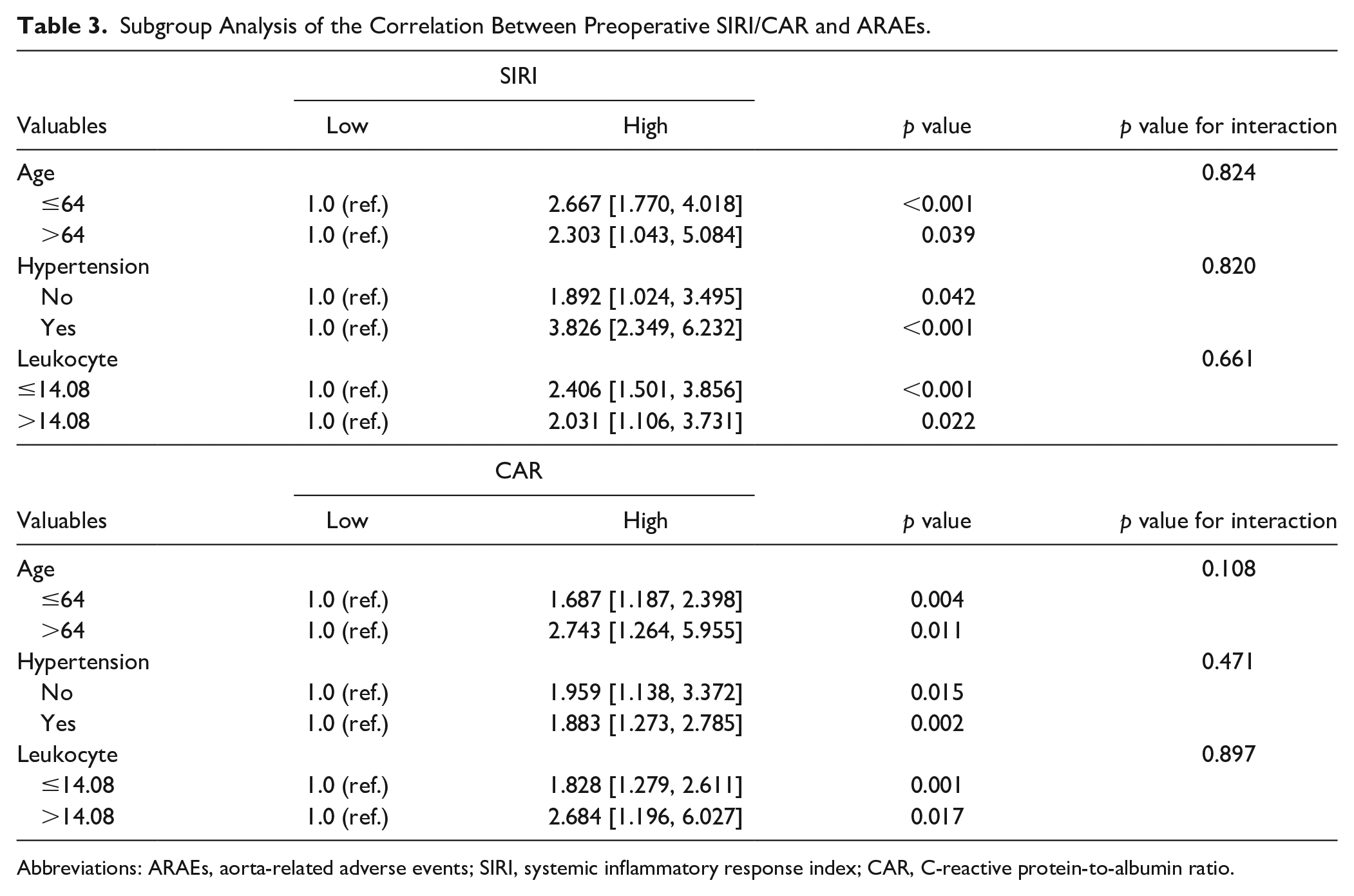
ROC curve analysis was used to convert continuous variables with p<0.1 from univariate analysis into categorical variables, which were then included in the multivariate analysis. After adjusting for confounding factors, cox proportional hazards regression analysis revealed that age (>64), hypertension, leukocyte (>14.08), SIRI (>15.112), and CAR (>0.312) are independent risk factors for postoperative ARAEs (Table 2). Subgroup analysis was conducted to determine the correlation between systemic inflammatory response indicators (SIRI and CAR) and ARAEs across comorbidities and different parameters, and the results are shown in Table 3. Stratification factors did not have a significant impact on the relationship between SIRI/CAR and ARAEs (interaction p>0.05). In all subgroups, SIRI >15.112 and CAR >0.312 were closely associated with an increased incidence of postoperative ARAEs in TBAD patients.
Univariate and Multivariable Analyses for Perioperative Clinical Characteristics Predictive of ARAEs.
Abbreviations: ARAEs, aorta-related adverse events; HR, hazard ratio; CI, confidence interval; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; MLR, monocyte-to-lymphocyte ratio; SII, systemic immune inflammation index; SIRI, systemic inflammatory response index; CAR, C-reactive protein-to-albumin ratio.
Subgroup Analysis of the Correlation Between Preoperative SIRI/CAR and ARAEs.
Abbreviations: ARAEs, aorta-related adverse events; SIRI, systemic inflammatory response index; CAR, C-reactive protein-to-albumin ratio.
ROC Curve Analysis of Systemic Inflammatory Response Indicators in Predicting ARAEs
ROC curve analysis compared the potential value of different preoperative systemic inflammatory response indicators for predicting postoperative ARAEs (Supplementary Figure 1). The results indicated that among the peripheral blood cell-based indicators, SIRI had the optimal predictive value with an AUC of 0.671 [95% CI (0.613, 0.726)]. In contrast, CAR based on CRP and albumin had an AUC of 0.631 [95% CI (0.577, 0.683)] (Supplementary Table 1). The combined SIRI-CAR score, derived from both indicators, further improved predictive performance with an AUC of 0.685 [95% CI (0.635, 0.735)] (Figure 2).
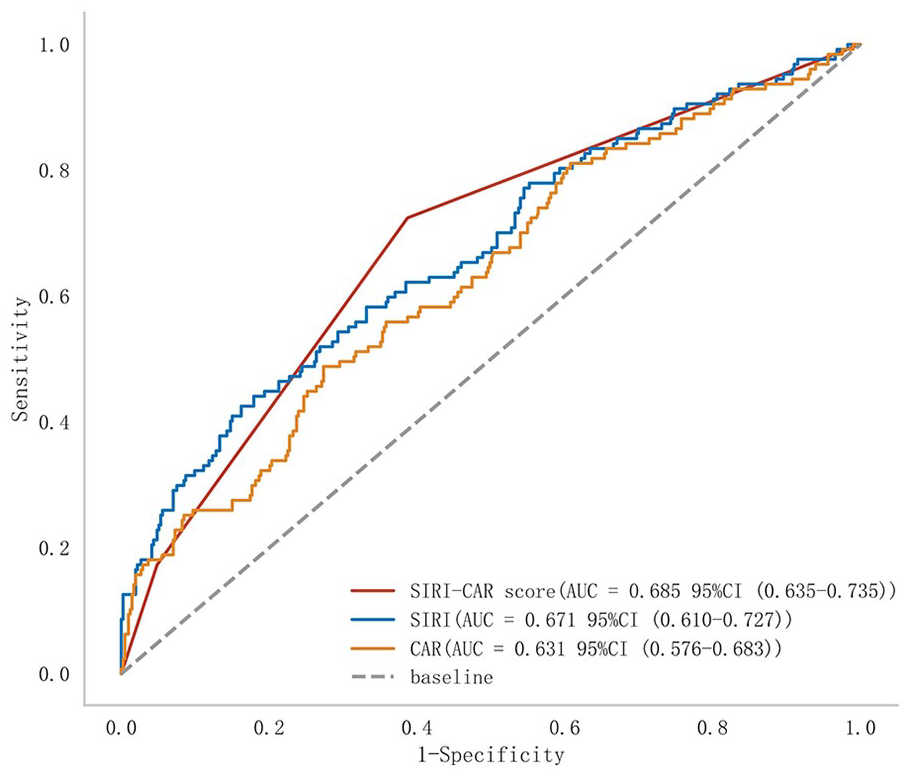
Comparison of ROC curves for combined indicators and single indicators. (ROC, receiver operating characteristic; SIRI, systemic inflammatory response index; CAR, C-reactive protein-to-albumin ratio).
Comparison of Long-Term ARAEs-Free Survival Status Between the Different SIRI, CAR, and SIRI-CAR Scores Groups
After identifying SIRI and CAR as independent risk factors for ARAEs, patients were further categorized based on the optimal thresholds determined by ROC curve analysis: into a high SIRI group (>15.112) and a low SIRI group (≤15.112), as well as a high CAR group (>0.312) and a low CAR group (≤0.312). Additionally, a novel composite systemic inflammatory response indicator, the SIRI-CAR score, was developed. Patients simultaneously classified as both low SIRI and low CAR were assigned a SIRI-CAR score of 0, those in both high SIRI and high CAR groups received a SIRI-CAR score of 2, and the remaining patients were assigned a SIRI-CAR score of 1. Kaplan-Meier survival analysis was then used to compare ARAEs-free survival status among these groups to explore the value of different preoperative systemic inflammatory response indicators (SIRI, CAR, and SIRI-CAR score) in the long-term prognosis of TBAD patients undergoing TEVAR. The results in Figure 3 indicated that patients in the low SIRI and low CAR groups had significantly higher ARAEs-free survival rates compared to those in the high SIRI and high CAR groups. Moreover, among patients with different SIRI-CAR scores, those with a SIRI-CAR score of 0 had notably higher long-term ARAEs-free survival rates compared to those with scores of 1 and 2 (log-rank test, p<0.05).
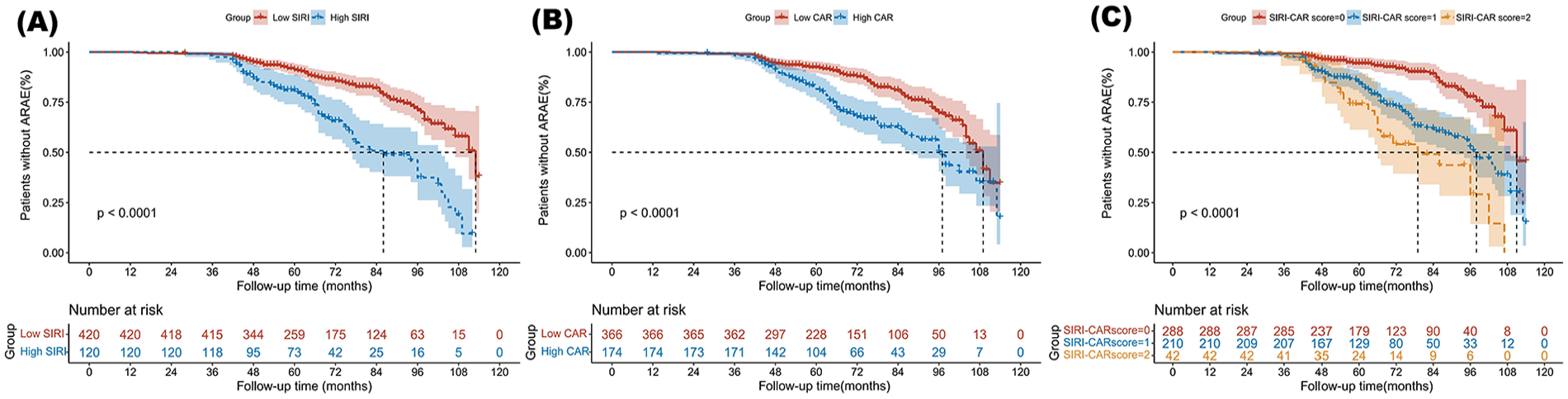
Kaplan-Meier analysis compared the survival status for ARAEs-free among different groups. (A) Kaplan-Meier analysis compared the survival condition for ARAEs-free between high SIRI group and low SIRI group; (B) Kaplan-Meier analysis compared the survival condition for ARAEs-free between high CAR group and low CAR group; (C) Kaplan-Meier analysis compared the survival condition for ARAEs-free between different SIRI-CAR score groups. (ARAEs, aorta-related adverse events; SIRI, systemic inflammatory response index; CAR, C-reactive protein-to-albumin ratio).
Prognostic Value of Preoperative SIRI-CAR Score
To further investigate the prognostic value of the SIRI-CAR score in TBAD patients undergoing TEVAR, we compared clinical outcomes during follow-up among patients with different scores. The results are summarized in Table 4, which show that as the SIRI-CAR score increases, the incidence of various types of ARAEs significantly rises. Additionally, the cumulative hazard curves indicate that the risk of different types of ARAEs varies significantly among patients with different SIRI-CAR scores (Figure 4).
The Comparison of Follow-up Clinical Outcomes Between Patients in Different Preoperative SIRI-CAR Scores Groups.
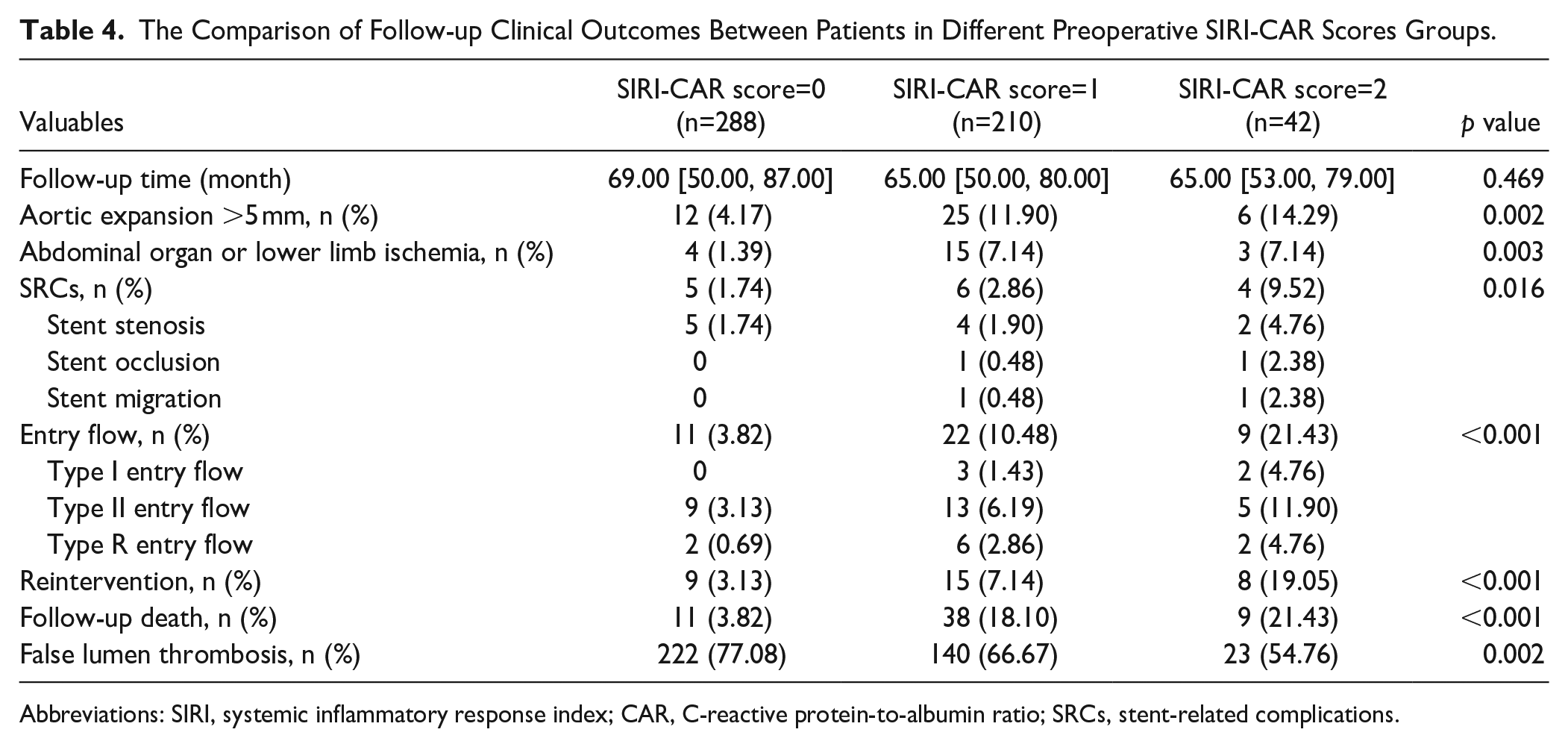
Abbreviations: SIRI, systemic inflammatory response index; CAR, C-reactive protein-to-albumin ratio; SRCs, stent-related complications.
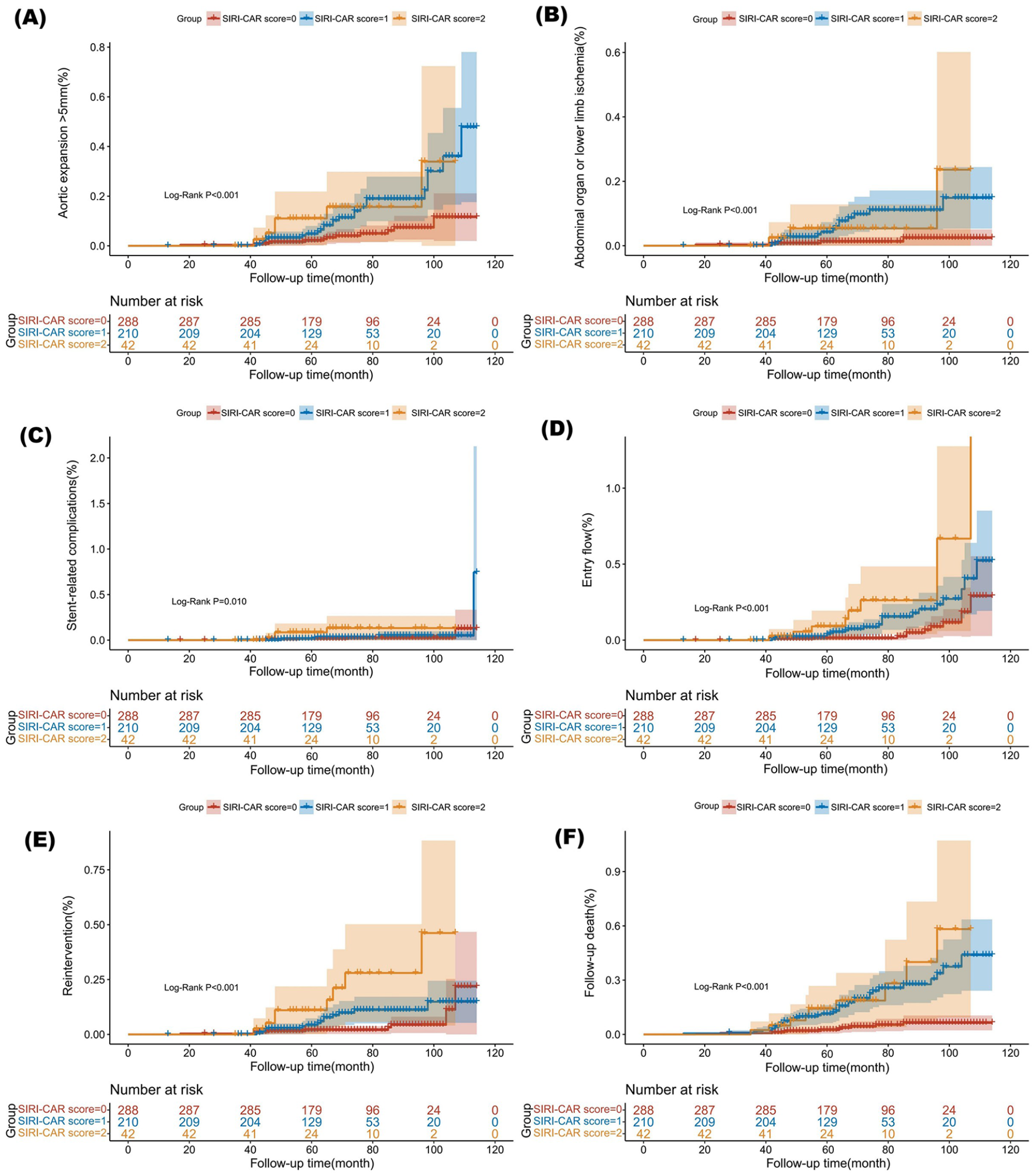
The cumulative hazard curves of different SIRI-CAR scores for various types of ARAEs. (A) Cumulative hazard curve of aortic expansion >5 mm; (B) Cumulative hazard curve of abdominal organ or lower limb ischemia; (C) Cumulative hazard curve of stent-related complications; (D) Cumulative hazard curve of entry flow; (E) Cumulative hazard curve of reintervention; (E) Cumulative hazard curve of follow-up death. (ARAEs, aorta-related adverse events; SIRI, systemic inflammatory response index; CAR, C-reactive protein-to-albumin ratio).
Discussion
Although TEVAR has proven effective in addressing the majority of complex TBAD, the potential risk of ARAEs postoperatively means not all patients achieve satisfactory long-term aortic remodeling outcomes. Therefore, early identification of high-risk ARAEs patients, timely adjustment of diagnosis, treatment, and follow-up strategies to minimize the risk of ARAEs occurrence as much as possible, is crucial for improving the long-term prognosis of TBAD patients treated with TEVAR.
Serum biological indicators, as a simple and reliable prognostic assessment tool, are now widely used in predicting the prognosis of various diseases. 3 ,10–12 By analyzing the level changes of these biological indicators, it is possible to more accurately assess patient prognosis and predict potential risks of complications. This aids in guiding clinical decision-making for health care professionals. Systemic inflammatory response is a major pathophysiological change in the mechanism of AD; an increasing amount of clinical evidence indicates a close correlation between preoperative systemic inflammatory response levels and the prognosis outcomes of TBAD patients undergoing TEVAR.8,9 Existing studies have confirmed that systemic inflammatory response indicators based on peripheral blood cells, such as NLR and SII, can effectively predict prognosis outcomes in AD patients. However, most of these studies often focus on the relationship between single indicators and prognosis, which does not fully reflect the potential value of systemic inflammatory response indicators in predicting prognosis, particularly in TBAD patients.
This study is the first to compare the prognostic value of different types of systemic inflammatory response indicators in patients with TBAD undergoing TEVAR. Through multivariate and subgroup analyses, we identified SIRI and CAR as independent risk factors for postoperative ARAEs. Based on these two indicators, we developed a new systemic inflammatory response score, the SIRI-CAR score. The results of the AUC comparison showed that the SIRI-CAR score performed better in predicting postoperative ARAEs compared to either of the individual components. The combined use of these two systemic inflammatory indicators further enhances its prognostic value.
Originally applied in predicting the survival rate of pancreatic cancer patients after chemotherapy, 22 SIRI has now been confirmed for its value in the prognosis of cardiovascular diseases through numerous studies.23,24 As a novel systemic inflammatory response indicator composed of peripheral blood cells, the impact of SIRI on prognosis is primarily related to the cellular functions of three leukocyte subtypes within its composition. Neutrophils, monocytes, and lymphocytes play crucial roles in systemic inflammation and immune activation. As the main effector cells of inflammation, variations in their levels are often closely associated with the degree of inflammatory response. 8 Therefore, elevated levels of SIRI often signify a more intense inflammatory response and an imbalance in immune regulation within the body. Increased systemic inflammation promotes the progression of AD, leading to vascular wall damage and infiltration of inflammatory cells, thereby affecting vascular stability and increasing the risk of aortic dilation or even rupture.
The mechanism of CAR’s impact on the prognosis of cardiovascular diseases is not yet clear. Existing studies mostly focus on exploring the individual effects of CRP or albumin on prognosis outcomes. Yao et al 25 reported that CRP/albumin is an effective predictive factor for mortality in patients with chronic obstructive pulmonary disease complicated by heart failure. However, whether CAR still has predictive value for the prognosis of patients with AD requires further investigation. As an acute-phase reactant, CRP plays a crucial protective role in the body’s natural immune processes. While traditionally viewed as a nonspecific inflammatory marker, the role of serum CRP in predicting the prognosis of patients with AD has garnered increasing attention in recent years. Existing research has thoroughly demonstrated the short-term and long-term prognostic value of CRP in various subtypes of AD.26,27 Albumin, as an important nutritional assessment marker, also reflects the level of inflammation to some extent. Increased systemic inflammatory response leads to reduced albumin synthesis and increased breakdown. Reports by Zeng et al 27 have also confirmed the association between low albumin levels and adverse outcomes during hospitalization and long-term mortality in patients with TBAD. Therefore, CAR, as a composite form of CRP and albumin, comprehensively reflects the body’s immune-inflammatory and nutritional status. Its preoperative elevation suggests that clinicians should enhance perioperative nutritional support for patients, aiming to improve the body’s nutritional and immune-inflammatory status as much as possible, and to mitigate the risk of potential ARAEs.
The SIRI-CAR score is a novel risk assessment tool that integrates two different systemic inflammatory response indicators, offering a more comprehensive evaluation of systemic inflammation through different pathways. This approach addresses the limitations of relying on single indicators to reflect complex inflammatory states. The SIRI-CAR score is not only reliable and efficient but also easy to calculate, thereby minimizing additional burdens on both patients and clinical staff. This makes it particularly useful for broader clinical applications, especially in economically and medically underserved areas.
For patients with elevated SIRI-CAR scores, clinicians should consider adopting more proactive monitoring and treatment strategies. These may include administering anti-inflammatory medications (such as corticosteroids or statins) either preoperatively or postoperatively to reduce vascular inflammation, developing more refined surgical plans, and utilizing advanced stent systems to minimize mechanical complications. Additionally, tailored follow-up plans should be established for high-risk patients to reduce the long-term risk of ARAEs and enhance overall prognosis.
This study has the following limitations: (1) As a single-center retrospective study, there are inherent selection biases, and the conclusions need further validation through multicenter randomized clinical trials; (2) The specific mechanisms of SIRI, CAR, and SIRI-CAR score in predicting long-term outcomes after TEVAR are not yet clear. Therefore, further exploration of their potential molecular biology mechanisms may provide a more comprehensive insight into their prognostic value; (3) When assessing long-term prognosis through systemic inflammatory status, it is necessary to combine other perioperative hematological markers and traditional predictive factors such as imaging examinations to more effectively predict the clinical outcomes of patients. Despite these limitations, our study still confirms the potential value of different systemic inflammatory response indicators in predicting the long-term prognosis of TBAD patients undergoing TEVAR. It also provides crucial clinical evidence for the relationship between systemic inflammatory status and the prognosis of TBAD patients undergoing TEVAR.
Conclusion
Preoperative SIRI and CAR may be considered as independent risk factors for TBAD patients undergoing TEVAR. The SIRI-CAR score can predict the risk of post-TEVAR ARAEs occurrence and demonstrates superior prognostic efficacy compared to using either indicator alone.
Supplemental Material
sj-docx-1-jet-10.1177_15266028241305953 – Supplemental material for The Value of Different Systemic Inflammatory Response Indicators in the Long-term Prognosis of Type B Aortic Dissection Patients Undergoing Thoracic Endovascular Aortic Repair
Supplemental material, sj-docx-1-jet-10.1177_15266028241305953 for The Value of Different Systemic Inflammatory Response Indicators in the Long-term Prognosis of Type B Aortic Dissection Patients Undergoing Thoracic Endovascular Aortic Repair by Linfeng Xie, Xinfan Lin, Yuling Xie, Siying Luo, Qingsong Wu, Zhaofeng Zhang, Zhihuang Qiu and Liangwan Chen in Journal of Endovascular Therapy
Supplemental Material
sj-jpg-1-jet-10.1177_15266028241305953 – Supplemental material for The Value of Different Systemic Inflammatory Response Indicators in the Long-term Prognosis of Type B Aortic Dissection Patients Undergoing Thoracic Endovascular Aortic Repair
Supplemental material, sj-jpg-1-jet-10.1177_15266028241305953 for The Value of Different Systemic Inflammatory Response Indicators in the Long-term Prognosis of Type B Aortic Dissection Patients Undergoing Thoracic Endovascular Aortic Repair by Linfeng Xie, Xinfan Lin, Yuling Xie, Siying Luo, Qingsong Wu, Zhaofeng Zhang, Zhihuang Qiu and Liangwan Chen in Journal of Endovascular Therapy
Footnotes
Author Contributions
L.X., X.L., and Y.X. designed the study and submitted the manuscript. L.X., X.L., and Y.X. prepared the first draft of the manuscript and did the literature review. S.L. and Z.Z. collected the clinical data and performed the statistical analysis. Q.W., Z.Q., and L.C. provide technical support. All authors read and approved the final manuscript.
Data Availability
The data from this study will not be shared publicly. All data included in this study are available upon request by contact with the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was sponsored by the Fujian Provincial Special Reserve Talents Fund (2021-25).
Ethical Approval
The study has been approved by the Ethics Committee of Fujian Medical University Union Hospital (No. XH2023-028) and complies with the Helsinki Declaration. Due to the retrospective nature of the study, the requirement for informed consent has been waived.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.