
Abstract
Background:
There are little available data about the impact of geriatric nutritional risk index (GNRI) on clinical outcomes following endovascular therapy (EVT) in chronic limb-threatening ischemia (CLTI) regarding the severities of renal dysfunction (RD).
Aims:
The aim of this study is to evaluate the impact of GNRI on clinical outcomes following EVT in CLTI regarding the severities of RD.
Methods:
We enrolled 705 consecutive CLTI cases treated with EVT between January 2010 and December 2019 at our hospital. The GNRI on admission was calculated as follows: [14.89 × albumin (g/dL)] + [41.7 × (body weight/ideal body weight)]. Study population were divided into 2 groups based on the median GNRI: low group (GNRI < 92) and high group (GNRI ≥ 92). Next, study population was divided to 3 groups according to estimate glomerular filtration rate (eGFR), which was defined as early RD group (60 ≤ eGFR), advanced RD group (15 ≤ eGFR < 60), and end-stage renal dysfunction (ESRD) group (eGFR < 15). The primary endpoint was 2-year amputation-free survival (AFS).
Results:
The median follow-up duration was 25.2 months. Amputation-free survival was significantly lower in the low GNRI group regardless of any severities of RD (59.1% vs 90.2%, Log Rank P<0.001 in early RD group, 59.6% vs 80.8%, Log Rank P=0.011 in advanced RD group, 32.8% vs 61.1%, Log Rank P<0.001 in ESRD group).
Conclusion:
The decrease of GNRI could predict clinical outcomes in CLTI following EVT regardless of any severities of RD based on eGFR.
Clinical Impact
The decrease of geriatric nutritional risk index was associated with worse outcomes in chronic limb-threatening ischemia following endovascular therapy regardless of any severities of renal dysfunction. Because both renal dysfunction and chronic limb-threatening ischemia could potentially have any inflammation, the geriatric nutritional risk index, which can reflect both nutrition-related risks and inflammation severity, can be a plausible marker in predicting adverse events after endovascular therapy in chronic limb-threatening ischemia patients with renal dysfunction.
Keywords
Introduction
Chronic limb-threatening ischemia (CLTI) is the most advanced form of peripheral artery disease (PAD) regarding morbidity and mortality. 1 On the other hand, renal dysfunction (RD) is a major risk factor for PAD and is associated with severe PAD requiring revascularization and higher amputation rates.2,3 Survival and amputation free rate get worse as the RD get more severe. 4
Revascularization for diseased limb, including surgical bypass and endovascular therapy (EVT), is the option for limb salvage. 5 Because there are some patients with CLTI requiring EVT for the treatment because of the difficulty of surgical bypass under general anesthesia due to age, multiple comorbidities, and general condition in daily clinical practice, EVT is suggested as safe and feasible option.6–8 However, even if the revascularization is successfully performed, the clinical outcomes remain poor because of high mortality and major amputation rates. 9 The patient’s nutritional status is crucial due to the limb salvage.10–12
In recent years, geriatric nutritional risk index (GNRI) was developed as a simple and accurate tool to assess nutritional status based on serum albumin and ideal body weight calculated as kilogram per square meter and to predict the risk of morbidity and mortality. 13 The GNRI is also strongly associated with clinical outcomes following EVT in patients with CLTI with RD and end-stage renal dysfunction (ESRD) requiring dialysis14–16 and have significant correlations with RD. 17 However, there are little available data about the impact of GNRI on clinical outcomes following EVT in patients with CLTI by the severities of RD. Therefore, we evaluated the impact of GNRI on clinical outcomes following EVT in patients with CLTI by the severities of RD.
Methods
Study Population
This is an observational, single-center, and retrospective study. We identified 705 consecutive patients with CLTI treated with EVT between January 2010 and December 2019 at our hospital. We excluded 15 patients with follow-up less than 30 days. Demographic, clinical, interventional, and follow-up data were retrospectively collected from electronic medical records as well as from medical examinations. Furthermore, all study patients received standard wound care by the plastic surgeon of our hospital after EVT. The GNRI on admission was calculated on admission as follows: [14.89 × albumin (g/dL)] + [41.7 × (body weight/ideal body weight)]. 13 Ideal body weight was calculated using the Lorentz formula: height (cm) − 100 − ([height (cm) − 150]/4) for men or height (cm) − 100 − ([height (cm) − 150]/2.5) for women. The weight to ideal body weight ratio was set to 1 if the patient’s body weight exceeded the ideal body weight. 13 The previous paper defined 4 grades of nutrition-related risk: GNRI < 82, 82 ≤ GNRI < 92, 92 ≤ GNRI < 98, and 98 ≤ GNRI. 13 In this article, we defined 2 groups as follows: the low GNRI group (GNRI < 92) and the high GNRI group (GNRI ≥ 92). In addition, study population was divided into 3 groups according to an estimate glomerular filtration rate (eGFR),which was defined as early RD group (60 mL/min/1.73 m2 ≤ eGFR), advanced RD group (15 ≤ eGFR < 60 mL/min/1.73 m2), and ESRD group (eGFR < 15 mL/min/1.73 m2). 18 The eGFR was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula. 19 Diabetes mellitus was defined according to the definition of the American Diabetes Association as follows 20 : (1) fasting plasma glucose of at least 126 mg/dL (7.0 mmol/L), or (2) 2 hour plasma glucose of at least 200 mg/dL (11.1 mmol/L) during an oral glucose tolerance test, or (3) glycated hemoglobin of at least 6.5% (48 mmol/mol), or (4) presence of classic symptoms of hyperglycemia or hyperglycemic crisis with random plasma glucose of at least 200 mg/dL (11.1 mmol/L). Hypertension was defined as blood pressure ≥140/90 mm Hg or use of an antihypertensive drug. Dyslipidemia was defined as low-density cholesterol ≥140 mg/dL or use of a lipid-lowering drug. The institutional review board at our hospital approved this retrospective study and waived the requirements for informed consent.
Study Endpoints and Definitions
The primary endpoint was amputation-free survival (AFS) from all causes at 2 years after EVT. The AFS was a composite endpoint defined as survival without ipsilateral major amputation. Major amputation was defined as an above-the-ankle amputation. The secondary endpoints were overall survival (OS), major amputation rate, and reintervention rate at 2 years after EVT. The OS is defined as survival from all causes with or without major amputation.
Statistical Analysis
Values are reported as the mean ± standard deviation. Differences in categorical variables between 2 groups were analyzed using the χ2 test, and Cochran-Mantel-Haenszel general association test was used to test the difference in the proportions among 3 groups. Continuous variables were compared using the unpaired t-test between 2 groups and analysis of variance was used to test the difference in the means among the three groups. Time-to-event data were analyzed using the Kaplan-Meier method and log-rank test. Multivariate Cox regression analysis was performed to determine the independent predictors of composite adverse events. A Cox proportional hazard model analysis was performed to calculate hazard ratios (HRs) and 95% confidence intervals (CIs) for the association between the GNRI-based malnutrition status and survival without ipsilateral major amputation, adjusted for the age, gender, diabetes mellitus, left ventricular ejection fraction, and Rutherford classification 5 or 6. The selection of variables for the multivariate analysis was based on previous reports. 15 Findings were considered significant at p<0.05. All statistical analyses were performed using SPSS version 26.0 (IBM Corp., Armonk, New York).
Results
Study Population
In the present study, 698 consecutive patients who underwent EVT for de novo CLTI were identified. The study flow chart is shown in Figure 1. As mentioned previously, we divided into 2 groups based on the median GNRI: the low GNRI group (GNRI < 92) and the high GNRI group (GNRI ≥ 92). The study population was analyzed in 3 groups as mentioned earlier: early RD group (n = 120), advanced RD group (n = 180), and ESRD group (n = 390). All patients in ESRD the group were treated with hemodialysis.
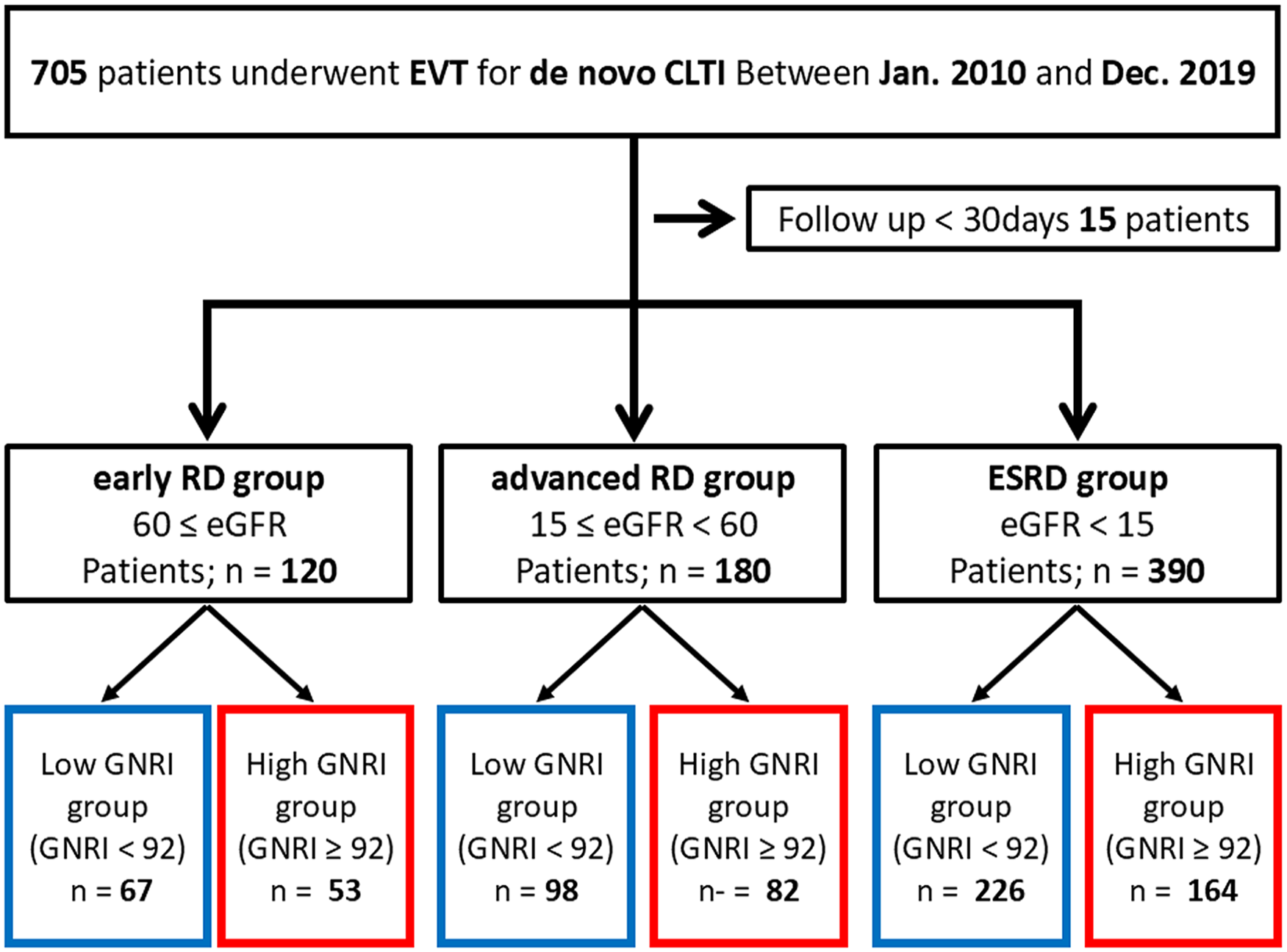
Study flow chart. EVT, endovascular therapy; CLTI, chronic limb-threatening ischemia; RD, renal dysfunction; GNRI, geriatric nutritional risk index.
Baseline Patient Characteristics
Baseline patient characteristics are summarized in Tables 1 and 2. The low GNRI group was more likely to be older in ESRD group. There was no gender difference between 2 groups in each cohort. Body mass index was significantly lower in the low GNRI group in all cohorts. The low GNRI group in early and advanced RD groups had lower ankle brachial index and the prevalence of more severe Rutherford classification before EVT. The high GNRI group was more likely to have dyslipidemia in early RD and ESRD cohort. The low GNRI group was more likely to have the higher value of C-reactive protein in all cohorts. In this retrospective study, some data could not be confirmed due to loss of records and removal or death of patients. The unidentified records were obliged to be missing value.
Clinical Background.
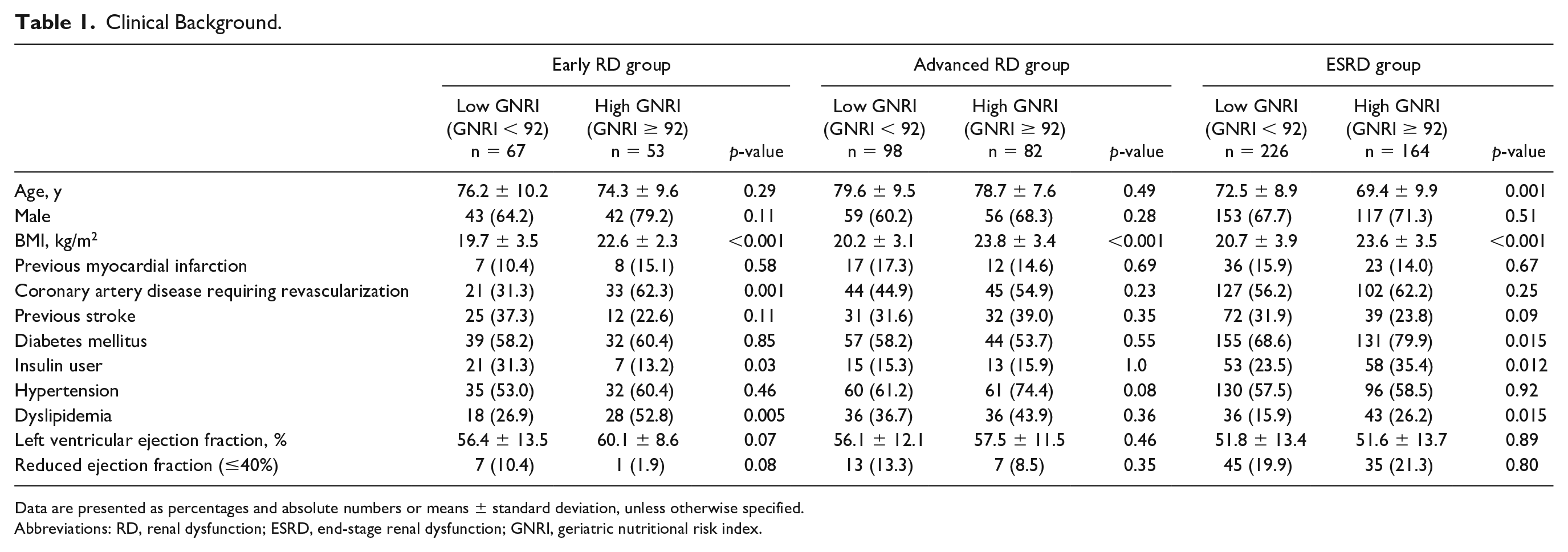
Data are presented as percentages and absolute numbers or means ± standard deviation, unless otherwise specified.
Abbreviations: RD, renal dysfunction; ESRD, end-stage renal dysfunction; GNRI, geriatric nutritional risk index.
Clinical Presentation, Medication, and Laboratory Data.
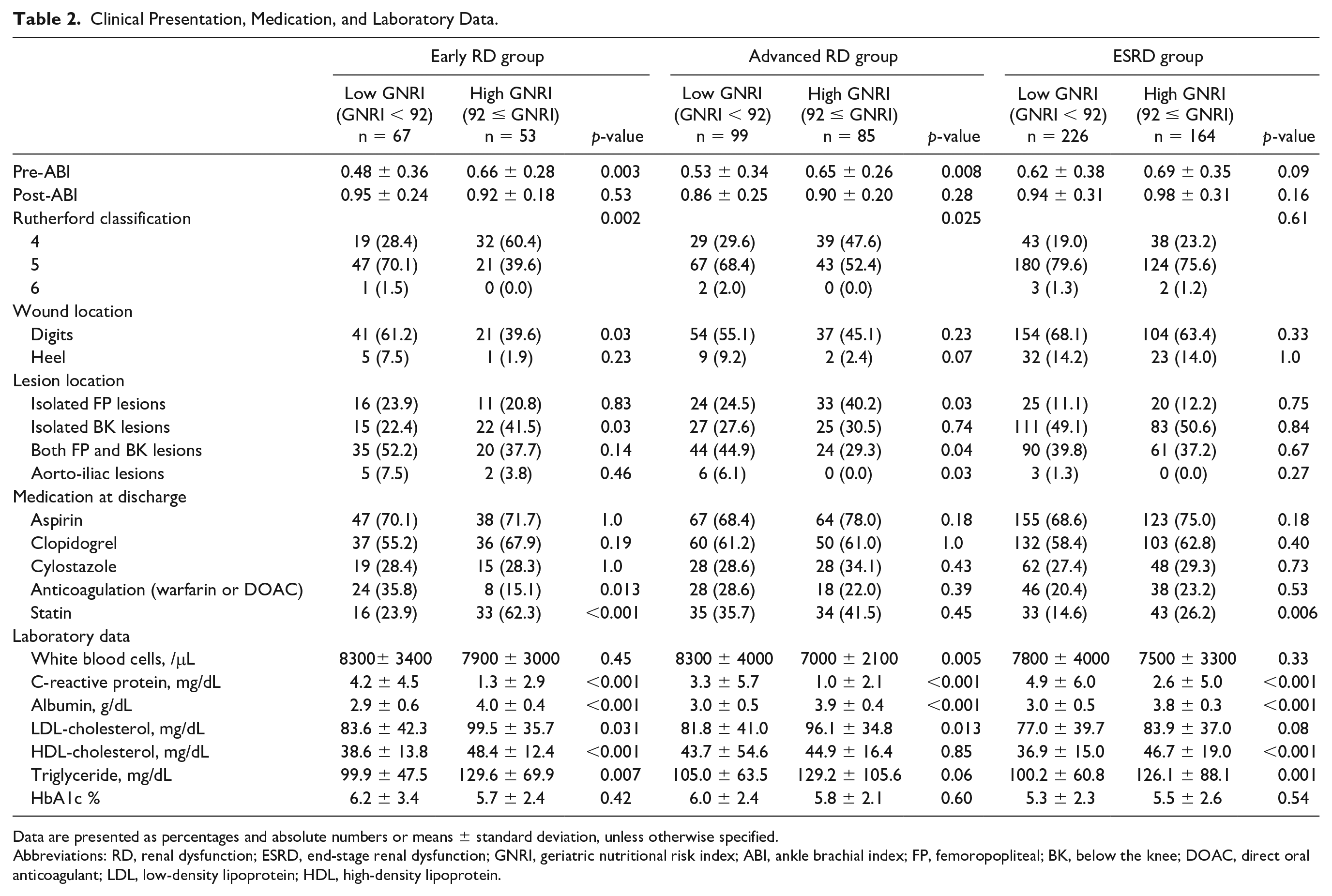
Data are presented as percentages and absolute numbers or means ± standard deviation, unless otherwise specified.
Abbreviations: RD, renal dysfunction; ESRD, end-stage renal dysfunction; GNRI, geriatric nutritional risk index; ABI, ankle brachial index; FP, femoropopliteal; BK, below the knee; DOAC, direct oral anticoagulant; LDL, low-density lipoprotein; HDL, high-density lipoprotein.
Clinical Outcomes
The median follow-up duration was 25.2 (IQR: 7.8-44.7) months. Table 3 summarizes clinical outcomes among 3 cohorts. Kaplan-Meier curves of AFS and OS in each RD group are shown in Figure 2. Both AFS and OS was significantly lower in the low GNRI group regardless of the severities of RD. Major amputation rate was significantly higher in the ESRD group. The reintervention rate was similar regardless the severities of RD.
Clinical Outcomes.
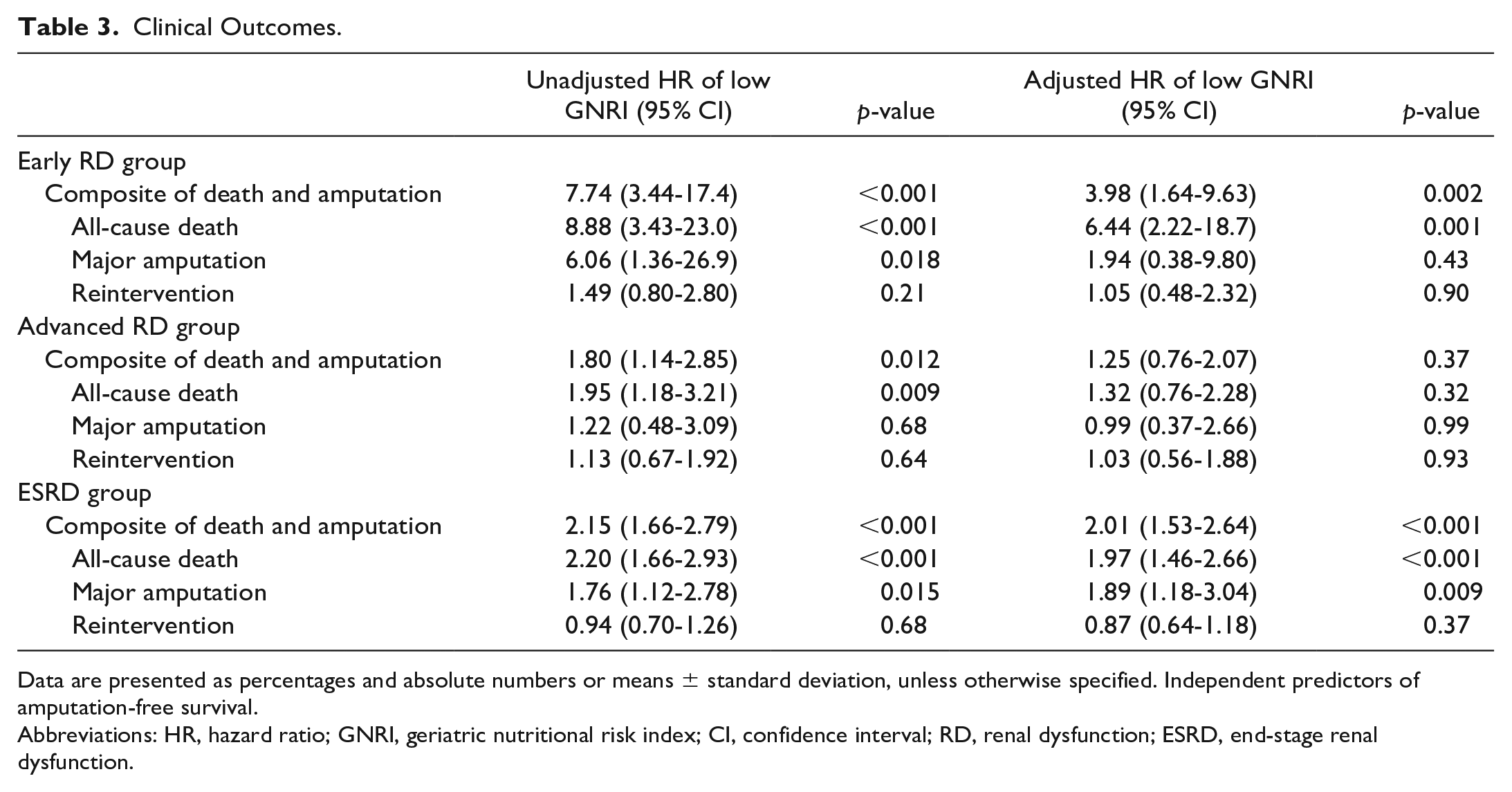
Data are presented as percentages and absolute numbers or means ± standard deviation, unless otherwise specified. Independent predictors of amputation-free survival.
Abbreviations: HR, hazard ratio; GNRI, geriatric nutritional risk index; CI, confidence interval; RD, renal dysfunction; ESRD, end-stage renal dysfunction.
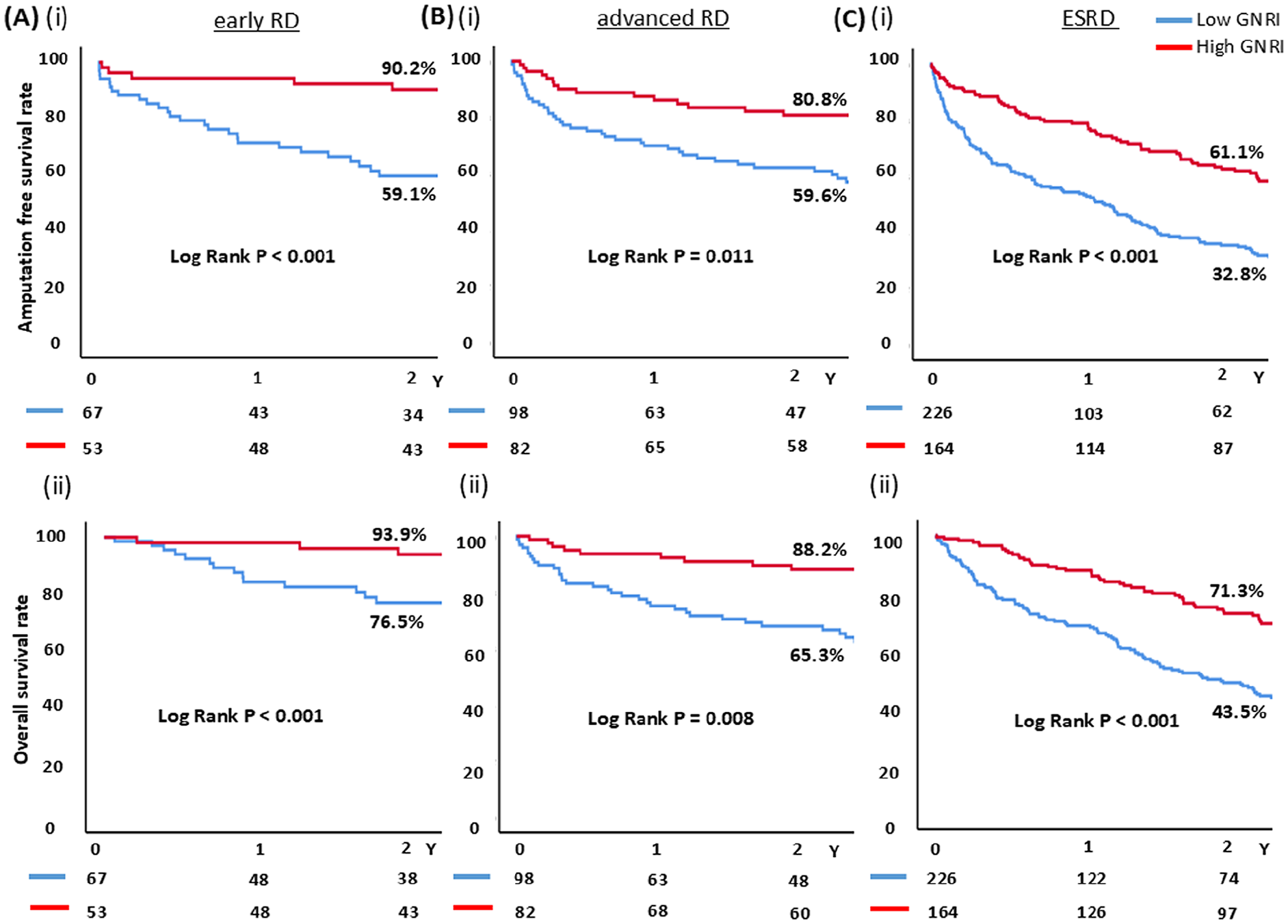
Kaplan-Meier curves among 3 subgroups. (A) early RD group, (B) advanced RD group, and (C) ESRD group. (i) Amputation-free survival, (ii) overall survival. low GNRI group (blue line), high GNRI group (red line). RD, renal dysfunction; GNRI, geriatric nutritional risk index.
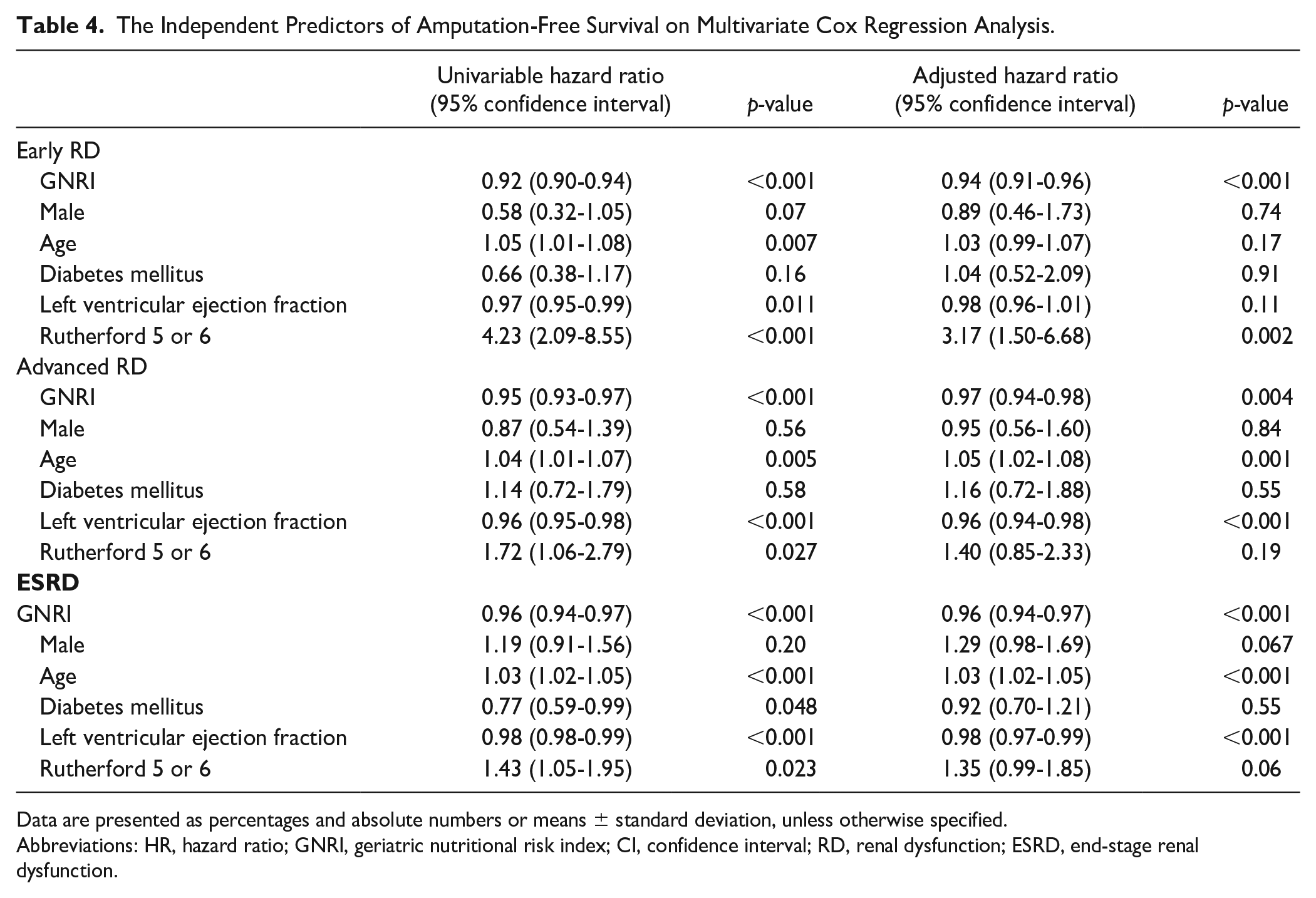
Multivariate Cox regression analysis demonstrated that GNRI was identified as an independent predictor of AFS regardless of the severities of RD (Table 4). Adjusted HR of GNRI is 0.94, 95% CI (0.91-0.96, p<0.001) in early RD group; 0.97, 95% CI (0.94-0.98, p=0.004 in advanced RD group; and 0.96, 95% CI (0.94-0.97, p<0.001) in ESRD group.
The Independent Predictors of Amputation-Free Survival on Multivariate Cox Regression Analysis.
Data are presented as percentages and absolute numbers or means ± standard deviation, unless otherwise specified.
Abbreviations: HR, hazard ratio; GNRI, geriatric nutritional risk index; CI, confidence interval; RD, renal dysfunction; ESRD, end-stage renal dysfunction.
Discussion
The present study demonstrated that the low GNRI was associated with worse clinical outcomes in patients with CLTI following EVT regardless of any severities of RD.
First, many previous papers reported that GNRI is strongly associated with mortality and morbidity after revascularization in patients with CLTI.14–16,21,22 Because nutrition, such as dietary amino acids, vitamins and minerals, is an epigenetic signal that can actively influence every step of the limb salvage, 23 the evaluation of the nutrition-related risk is important in patients with CLTI.11,12 Our results added that the evaluation of GNRI was important to predict clinical outcomes in patients with CLTI following EVT regardless of any severities of RD.
Second, the previous papers reported that low albumin level (<3.0 g/dL) was also identified as independent predictors for all-cause mortality 24 and one of the factors predicting clinical failure on multivariate analysis in patients with CLTI. 25 On the other hand, the ASPEN position paper makes clear that hypoalbuminemia is a poor marker of nutritional status and is an important marker of inflammation. 26 Hence, GNRI can also reflect the severity of inflammation because serum albumin is included in the formula. The patients with CLTI could potentially have any inflammation such as wound infection and osteomyelitis, as a previous paper reported that total of 70% of limb losses were due to uncontrollable infection. 25 The present study also suggested that the low GNRI group was more likely to have the higher value of C-reactive protein regardless of the severities of RD. This result is consistent with the previous findings mentioned earlier. Therefore, because it is important to evaluate both the nutrition-related risk and the severity of inflammation in predicting the clinical outcomes of patients with CLTI, GNRI can be a plausible predictor of adverse events after EVT in patients with CLTI.
Third, Garimella et al 3 also reported that RD is associated not only with severe PAD but also with higher rates of limb amputation. As well known, although the comorbidities are quite different by the severities of RD, previous papers about GNRI in patients with CLTI have evaluated only a subset of patients with RD.14,27 Renal dysfunction, especially ESRD required hemodialysis, is a significant risk factor associated with OS after treatment of CLTI.14,28–30 Recent study reported that the lower the eGFR, the lower is the GNRI, 17 and the more severe the RD, the worse are the clinical outcomes. 4 No studies have sufficiently evaluated the clinical importance of nutrition-related risk by the severities of RD. RD also has any chronic inflammation such as oxidative stress even in the early stage. 31 This study suggested that C-reactive protein levels were higher than normal limits even in the early RD group, regardless of high or low GNRI. This result is consistent with the previous findings. Therefore, the GNRI, which can reflect both nutrition-related risks and inflammation severity as mentioned earlier, is reasonable to predict clinical outcome even in patients with RD.
Finally, to our best knowledge, the low GNRI was associated with worse clinical outcomes in patients with CLTI following EVT regardless of any severities of RD because previous papers about GNRI in patients with CLTI have evaluated only a subset of patients with RD.14,27 The GNRI could reflect not only the nutrition-related risk but also the aspect of chronic inflammation. 26 Because both RD and CLTI could potentially have any inflammation,25,31 the GNRI, which can reflect both nutrition-related risks and inflammation severity, can be a plausible marker in predicting adverse events after EVT in patients with CLTI with RD. Our findings are obtained from real-world practice and can be useful reference for decision-making in treatment strategy of patients with CLTI in daily clinical practice.
Study Limitations
The main limitation of this study was the lack of randomization and the retrospective, observational study. We could not evaluate the details of procedures (eg, sub-intimal or true-lumen tracking procedure), frailty of patients, WIfI score, and social determinants of health and the quality of wound care. However, our hospital has a plastic surgery department, and all patients in this study received standard wound care by the plastic surgeon.
Conclusions
The decrease of GNRI could predict clinical outcomes in CLTI following EVT regardless of any severity of RD based on eGFR.
Footnotes
Author Contributions
Yusuke Watanabe MD, corresponding author.
Toru Naganuma PhD, study design, data collection.
Satoko Tahara PhD, data collection, supervision.
Masaaki Okutsu PhD, data analysis, data collection.
Koji Hozawa MD, supervision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was conducted according to the principles of the Declaration of Helsinki (64th WMA General Assembly, Fortaleza, Brazil, 2013) and in accordance with the applicable guidelines, regulations, and acts.