
Abstract
Objective:
Establish a predictive tool for assessing post-iliac vein stent placement (IVSP) patency loss within 1 year.
Background:
Post-IVSP stent surveillance is vital for detecting stent malfunction and guiding interventions. Despite extensive research on vascular patency after IVSP, individual risks for patency loss remain understudied.
Materials and Methods:
We developed a predictive model for assessing patency loss risk within 1 year after IVSP using data from 162 patients. Cox regression and the Boruta method identified risk factors, leading to the construction of a random forest (RF) model. We validated the model’s performance using testing data and developed a user-friendly risk tool, the Etiology-Stenosis-Age-Length (ESAL) Classification.
Results:
The RF model demonstrated excellent performance, with high sensitivity, specificity, and negative predictive value. Risk factors identified included younger age, post-thrombotic lesions, short-segment occlusions, and preoperative target lesion occlusion. Shapley Additive exPlanations analysis and Cox regression enhanced model interpretability.
Conclusions:
We present a novel, intuitive model for assessing patency loss risk after IVSP. The ESAL classification provides clinicians with a practical tool to identify high-risk patients. Future research should focus on larger, more representative cohorts to validate and refine the model.
Clinical Impact
How will this change clinical practice?
The risk of iliac vein stent patency loss within one year post-placement can be predicted in advance.
What does it mean for the clinicians?
The newly introduced Etiology-Stenosis-Age-Length (ESAL) Classification offers clinicians a practical and user-friendly tool for identifying high-risk patients who may experience patency loss after iliac vein stent placement.
What is the innovation behind the study?
Researchers have successfully developed a predictive model for assessing the risk of iliac vein stent patency loss within one year post-placement.
Keywords
Introduction
In recent years, deep venous stenting has become increasingly popular as a primary approach for managing acute or chronic venous obstruction, encompassing conditions such as acute iliofemoral deep vein thrombosis and non-thrombotic iliac vein lesions (NIVL).1,2 Previously, studies confirmed the safety and effectiveness of a stent design incorporating braiding and laser-cutting techniques. 3 Consistent with prior investigations, approximately 10% of patients encounter loss of patency in the target vessel within 1 year following iliac vein stent placement (IVSP),4–6 referred to herein as IVSP with patency loss.
Presently, there exists a comprehensive understanding of the factors influencing target vessel restenosis post-IVSP. Common hurdles encountered by IVSP include compression from neighboring structures (such as the right common iliac artery in May-Thurner syndrome) or venous fibrosis, culminating in patency loss. 7 Patency status primarily correlates with the etiology and obstructive nature of the treated post-thrombotic syndrome lesion (either occlusive or nonocclusive). 8 A thorough review by Raju, 9 encompassing peer-reviewed literature, demonstrated patency rates for the non-thrombotic (NT) group ranging from 90% to 100%, while the post-thrombotic (PT) group exhibited rates between 74% and 89%. Furthermore, a 2019 study investigating the safety and effectiveness of the Veniti Vici Venous Stent System also highlighted higher patency rates in the NT group compared to the PT group. 5 The question of whether the stent should traverse the inguinal ligament remains contentious, despite several significant studies indicating that patency rates post-IVSP are independent of inguinal ligament crossing.8,10,11 Notably, the guidelines advise against stenting below the inguinal ligament and beyond the common femoral confluence. 12 Certain influencing factors have been excluded in some studies, suggesting that the total stent length at the 6-month follow-up post-IVSP is not a risk factor for intrastent thrombosis in NIVL and PT-type lesions. 13
To sum up, patency loss following IVSP is primarily attributed to specific clinical features, underscoring the need for practical predictive tools. For IVSP patients, considering the heightened risk of patency loss and the attendant risks and costs of re-intervention, there is a pressing need for thrombosis prevention and early identification of high-risk individuals for restenosis. Such an approach facilitates timely adjustments in treatment strategies, thereby playing a pivotal role in disease progression mitigation and enhancing patient quality of life. Presently, no suitable risk model exists to quantitatively assess the likelihood of patency loss post-IVSP. The objective of this study is to identify and evaluate factors associated with patency loss post-IVSP, construct a predictive model, and assess its accuracy and efficacy. In addition, there is a plan to establish a practical clinical tool to fill the current clinical gap.
Materials and Methods
Study Design and Participants
This diagnostic/prognostic study followed the Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD) reporting guidelines. 14 The overall workflow chart is depicted in Figure 1. This study is a prospective cohort study that utilized data from a previous investigation on the safety and effectiveness of IVSP. 15 Initially, a sample of 171 individuals, approximately 60 years old, who underwent IVSP for iliac vein obstruction between 2020 and 2021, was included. Subsequently, 162 patients completed the 12-month follow-up, with 9 patients excluded due to missing follow-up data. Among these individuals, imaging confirmed loss of patency in 14 patients at the 12-month follow-up. The study obtained approval from the Institutional Review Board at each study center, and all patients provided informed consent.
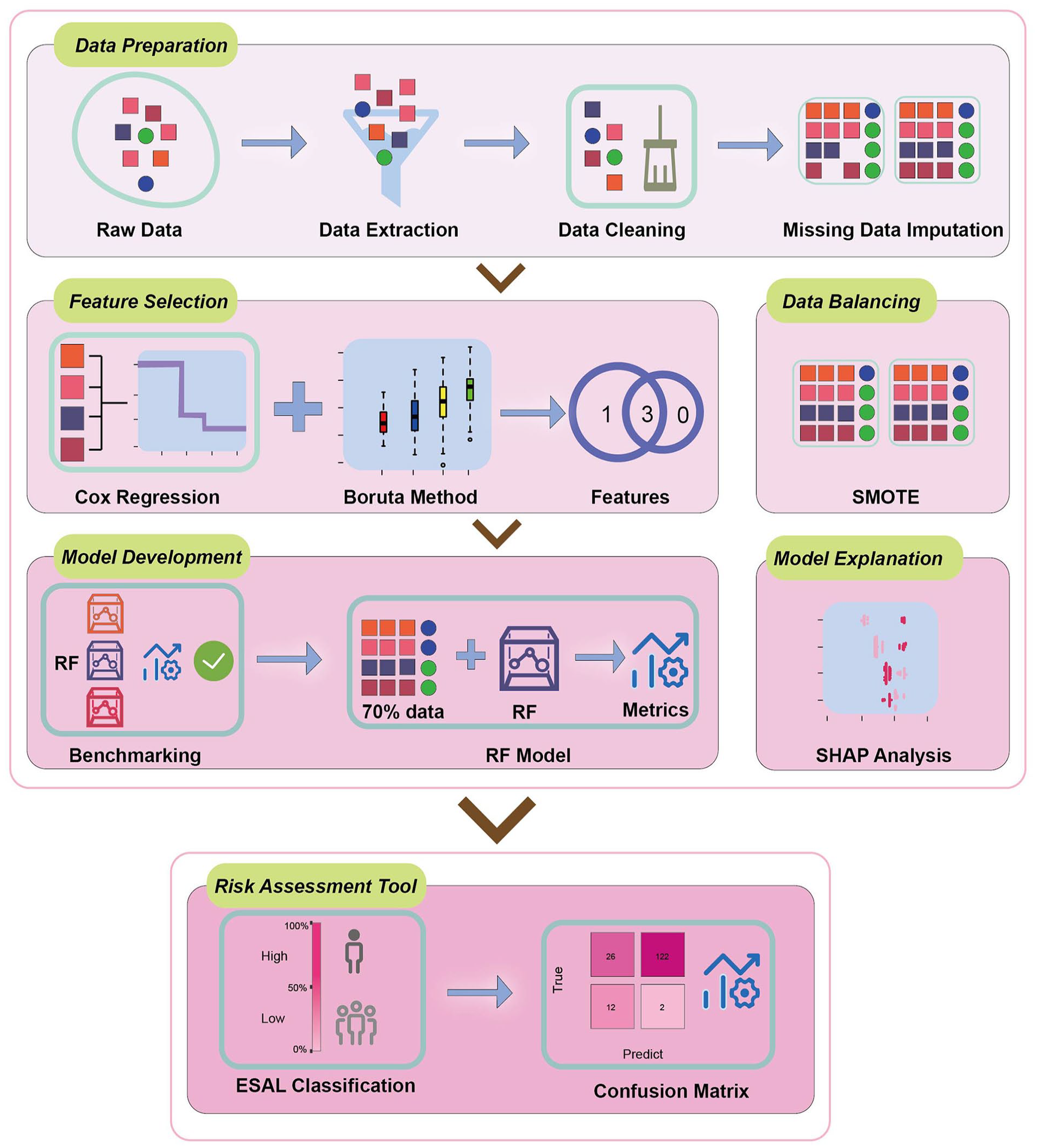
Schematic of the study workflow. SMOTE, Synthetic Minority Oversampling Technique; RF, random forest; SHAP, Shapley Additive exPlanations; ESAL, Etiology-Stenosis-Age-Length.
Outcome Variable
After IVSP, standard antithrombotic therapy was administered,15,16 and follow-up assessments of target vessel patency were conducted at 6 and 12 months. The primary outcome was the 12-month primary patency, defined as freedom from occlusion or in-stent restenosis and freedom from surgical or endovascular intervention to maintain patency.
Candidate Predictors
During the perioperative period, certain baseline variables were chosen as candidate predictor factors. General variables included age, gender (male and female), body mass index, and smoking history (never, former, and current). Medical history encompassed the presence or absence of diabetes, hypertension, coronary heart disease, pulmonary embolism (within the last 6 months), and stroke. Information regarding the target vessel and stent included lesion etiology, lesion location, as well as the diameter, length, and degree of stenosis of the target lesion (pre- and postoperatively). In addition, the length and diameter of the stent used during the procedure were recorded. Baseline venous clinical assessment included the Clinical-Etiology-Anatomy-Pathophysiology (CEAP) C classification, venous clinical severity score, and Chronic Venous Insufficiency Questionnaire-14 score. Administration of antithrombotic therapy exceeding 6 months during the 12-month follow-up period was also considered a candidate predictor factor. Furthermore, preoperative laboratory results reflecting the patient’s physical condition were included, such as white blood cell count, red blood cell count, hemoglobin, platelet count, albumin, alanine aminotransferase (ALT), aspartate transaminase (AST), creatinine, blood glucose, total bilirubin, activated partial thromboplastin time, prothrombin time, thrombin time, and international normalized ratio (INR).
Feature Engineering
Before training the models, the data underwent preprocessing. The data’s missingness is depicted in Supplemental Figure 1, where 16 variables exhibited minor data gaps, with the highest percentage of missing data in a variable reaching 4.32%. Multiple imputation was employed to address the missing values. 17 Variables with variances equal to or close to 0 were removed. Out of the 35 variables listed in the Materials and Methods section, none were excluded. Analysis of numerical predictive factors revealed a strong correlation between red blood cell count and hemoglobin (correlation coefficient = 0.81) and between ALT and AST (correlation coefficient = 0.80). Consequently, both RBC count and AST were excluded as variables. The most important variables for predicting IVSP with patency loss were selected using the Boruta method. 18 The Boruta method is a feature selection algorithm that identifies relevant variables by iteratively comparing the importance of real features to randomized, shadow features. Significant factors identified through multivariate Cox regression were also chosen as predictive factors for the model. Out of all the variables, 4 were considered important and inserted into the machine learning (ML) model. While the number of ML prediction models is rapidly increasing, few achieve good interpretability, and convenient use is limited.19–21 Therefore, simplification was applied before variables entered the model using the “cutoff” package to find cutoff values. Specifically, continuous variables were transformed into categorical variables, including age (≥55 and <55 years), lesion length (≥110 and <110 mm), and diameter stenosis (occlusion and stenosis).
Prediction Models
In the final preprocessing stage, the data were balanced with the Synthetic Minority Oversampling Technique. 22 The oversampling method was based on the calculation 148/14 ≈ 10. Thus, a set was generated with 10 times the number of IVSP with patency loss compared to the original dataset, totaling 140 cases. Supplemental Figure 2 provides detailed information on the distribution of observations by category in the balanced and imbalanced datasets.
After preprocessing, the next step involved a benchmark experiment to find a suitable model. Due to the small overall sample size, the balanced dataset underwent 1000 iterations of bootstrap resampling. The following 5 ML models were trained: logistic regression, random forest (RF), support vector machine, k-nearest neighbors, and regression tree. 23 These models are commonly applied in medical binary classification problems.19,24 Subsequently, the RF model was utilized, and the balanced dataset was randomly divided into a training dataset comprising 70% of the samples (98 cases of IVSP with patency loss and 104 cases of patent IVSP without patency loss) and a testing dataset comprising 30% of the samples (42 cases of IVSP with patency loss and 44 cases of IVSP without patency loss). 19 This model is used in classification and regression problems and belongs to what are known as ensemble methods, which can be used to construct multiple models and combine them to reach a final result. The RF model is robust and has been widely used in the health field in recent years due to its good predictive capacity. 25 The performance of models was assessed using receiver-operating characteristic (ROC) and precision-recall curves, as well as metrics, including area under the curve (AUC), accuracy, specificity, sensitivity, positive predictive value (PPV), and negative predictive value (NPV). Calibration curves were applied to evaluate the performance of the RF model. Shapley Additive exPlanations (SHAP) is a valuable tool for the tree-based model method. 26 Herein, SHAP was used to explain the output of the ML models and display the positive or negative impact of each variable on the prediction of IVSP with patency loss.
Statistical Analysis
Data were analyzed using R version 4.2.1. Survival curves for patency were determined using the Kaplan–Meier method. Cox regression model was used for multivariate analysis of time to event, and hazard ratios (HRs) were reported with a 95% confidence interval (CI). All variables with a p value <0.05 in univariate analysis were selected for multivariate Cox regression analysis. Continuous variables were presented as mean ± standard deviation with a range of values, while categorical variables were presented as numbers and percentages. The Pearson’s Chi-squared test and Fisher exact tests were used for categorical variables, and the Wilcoxon rank sum test was used for continuous variables. All p values were considered significant if <0.05.
Results
General Characteristics
The patency rate determined from imaging data for 162 patients at 12 months is depicted in Figure 2. The median follow-up time was 364 days. Among individuals with a patent IVSP at baseline, 8.64% were assessed to have lost patency in the target vessel during the 12-month follow-up. At baseline, the average age was 59 ± 9 years, and the gender ratio was approximately equal. Among the 14 individuals with loss of patency, 12 belonged to the PT-type lesion group, and they exhibited more severe preoperative diameter stenosis (Table 1). The Boruta method identified 4 important predictors, namely lesion etiology, preoperative diameter stenosis, age, and lesion length (Supplemental Figure 3). Multivariate Cox regression revealed 3 statistically significant predictors: lesion etiology (HR = 5.54, 95% CI 1.14–27.0), age (HR = 0.94, 95% CI 0.89–0.99), and lesion length (HR = 1.02, 95% CI 1.01–1.03; Table 2). It is evident that these 3 variables overlap to some extent, indicating the suitability of these variables as predictive factors.
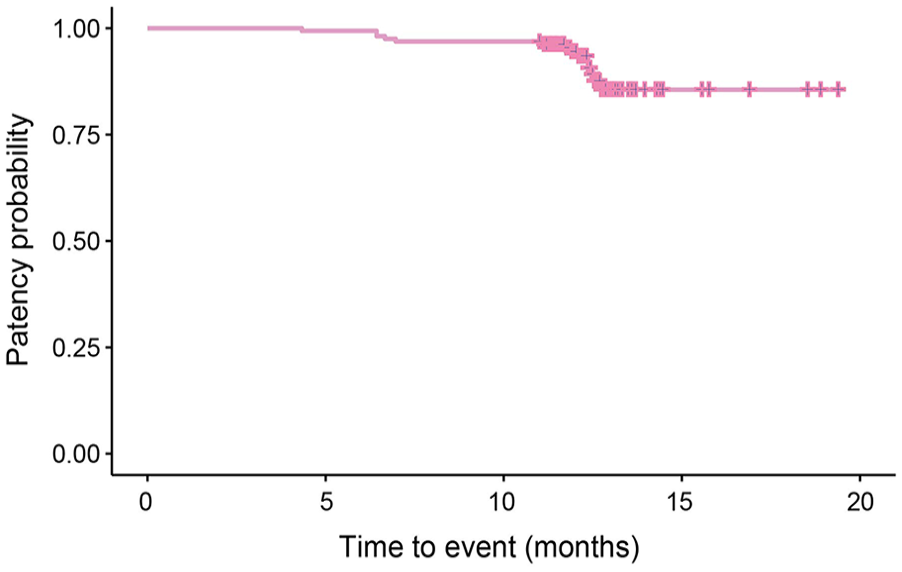
Primary patency Kaplan–Meier curve for the 162 patients with 12 months patency results.
Baseline Characteristics of the Study Population.
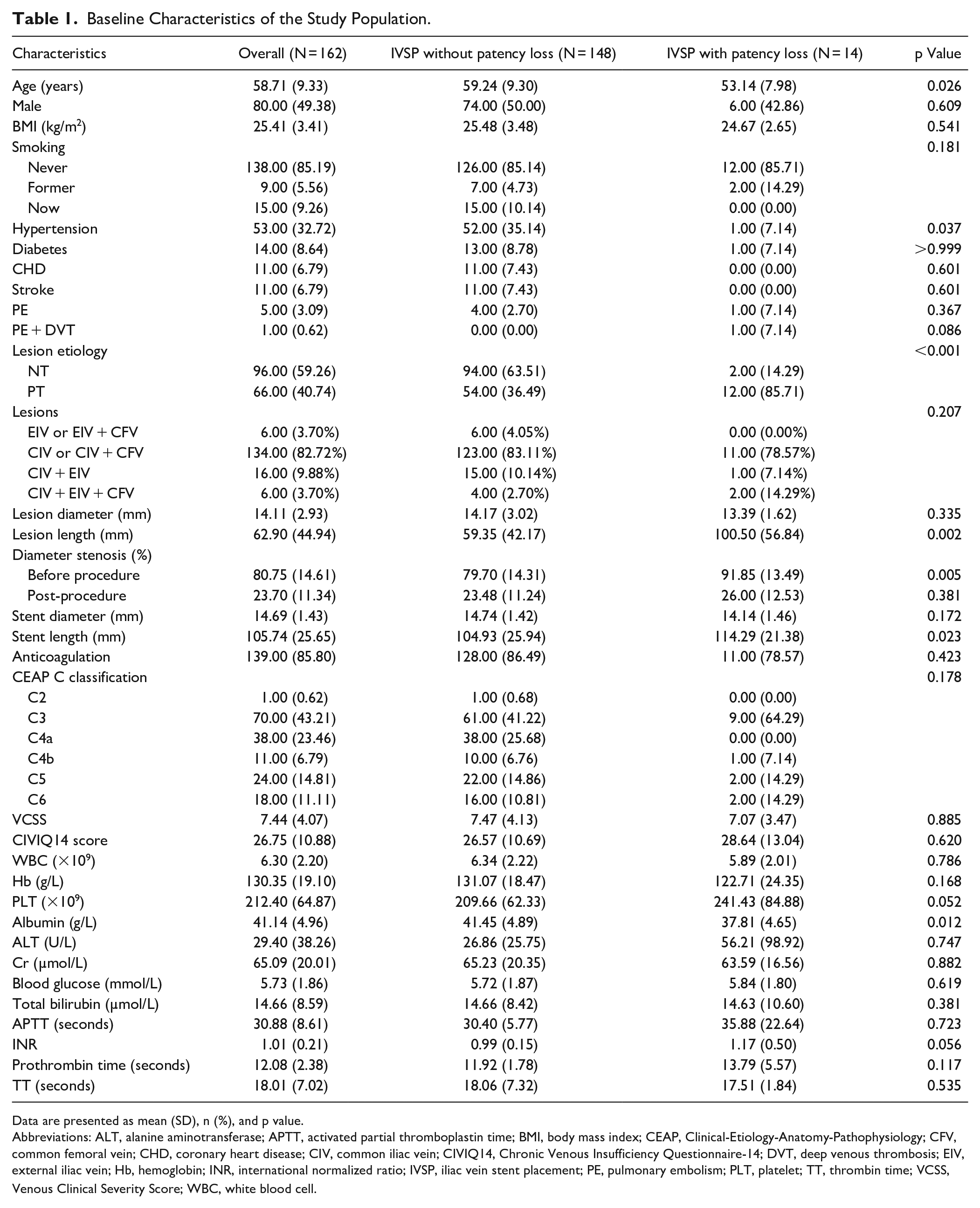
Data are presented as mean (SD), n (%), and p value.
Abbreviations: ALT, alanine aminotransferase; APTT, activated partial thromboplastin time; BMI, body mass index; CEAP, Clinical-Etiology-Anatomy-Pathophysiology; CFV, common femoral vein; CHD, coronary heart disease; CIV, common iliac vein; CIVIQ14, Chronic Venous Insufficiency Questionnaire-14; DVT, deep venous thrombosis; EIV, external iliac vein; Hb, hemoglobin; INR, international normalized ratio; IVSP, iliac vein stent placement; PE, pulmonary embolism; PLT, platelet; TT, thrombin time; VCSS, Venous Clinical Severity Score; WBC, white blood cell.
Cox Regression Analysis of Factors Associated With Loss of Patency After Iliac Vein Stent Placement.
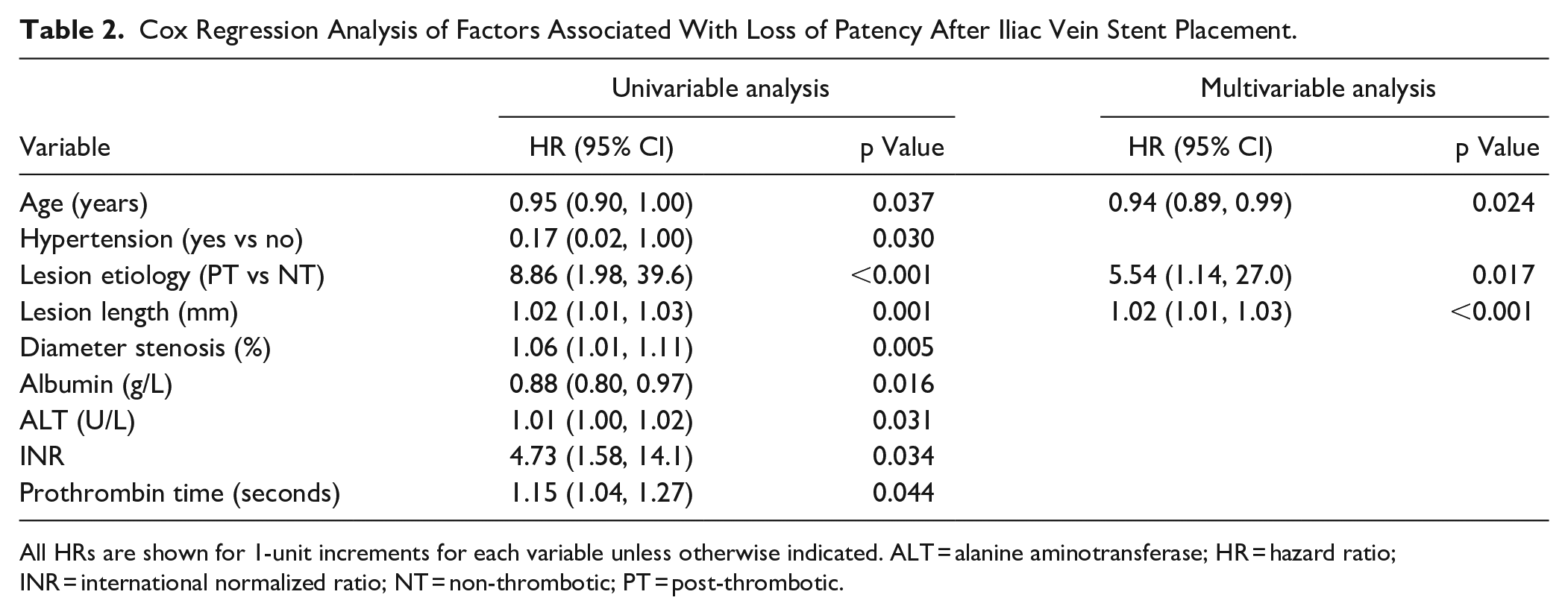
All HRs are shown for 1-unit increments for each variable unless otherwise indicated. ALT = alanine aminotransferase; HR = hazard ratio; INR = international normalized ratio; NT = non-thrombotic; PT = post-thrombotic.
Benchmarking
Table 3 displays the performance of ML models trained on a balanced dataset based on different metrics. Figure 3 shows the ROC curve and precision-recall (PR) curve with the respective AUC values for the 5 ML models trained with balanced data. A balanced dataset was utilized, and metrics for evaluating model performance were deemed appropriate; thus, no adjustments to the thresholds were made. Most models exhibited good performance, with the RF model demonstrating the most robust and favorable performance. The performance of the RF model is as follows: AUC (0.90), Precision-Recall area under the curve (PRAUC; 0.88), Accuracy (0.85), Specificity (0.81), Sensitivity (0.89), PPV (0.82), and NPV (0.88).
Performance of the Models Trained With Balanced Dataset Based on Different Metrics.
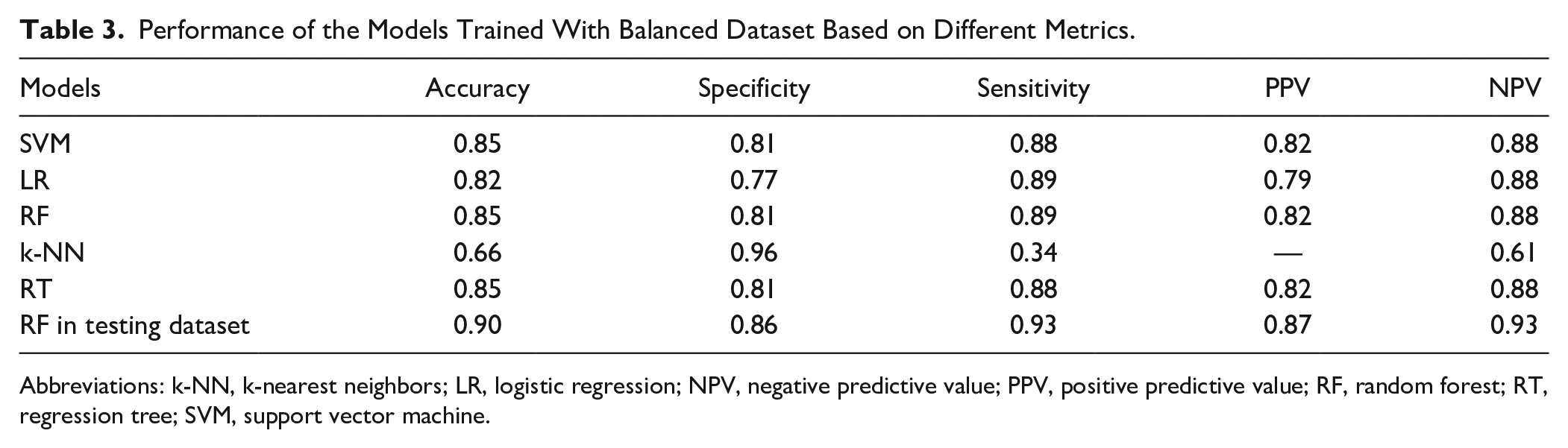
Abbreviations: k-NN, k-nearest neighbors; LR, logistic regression; NPV, negative predictive value; PPV, positive predictive value; RF, random forest; RT, regression tree; SVM, support vector machine.
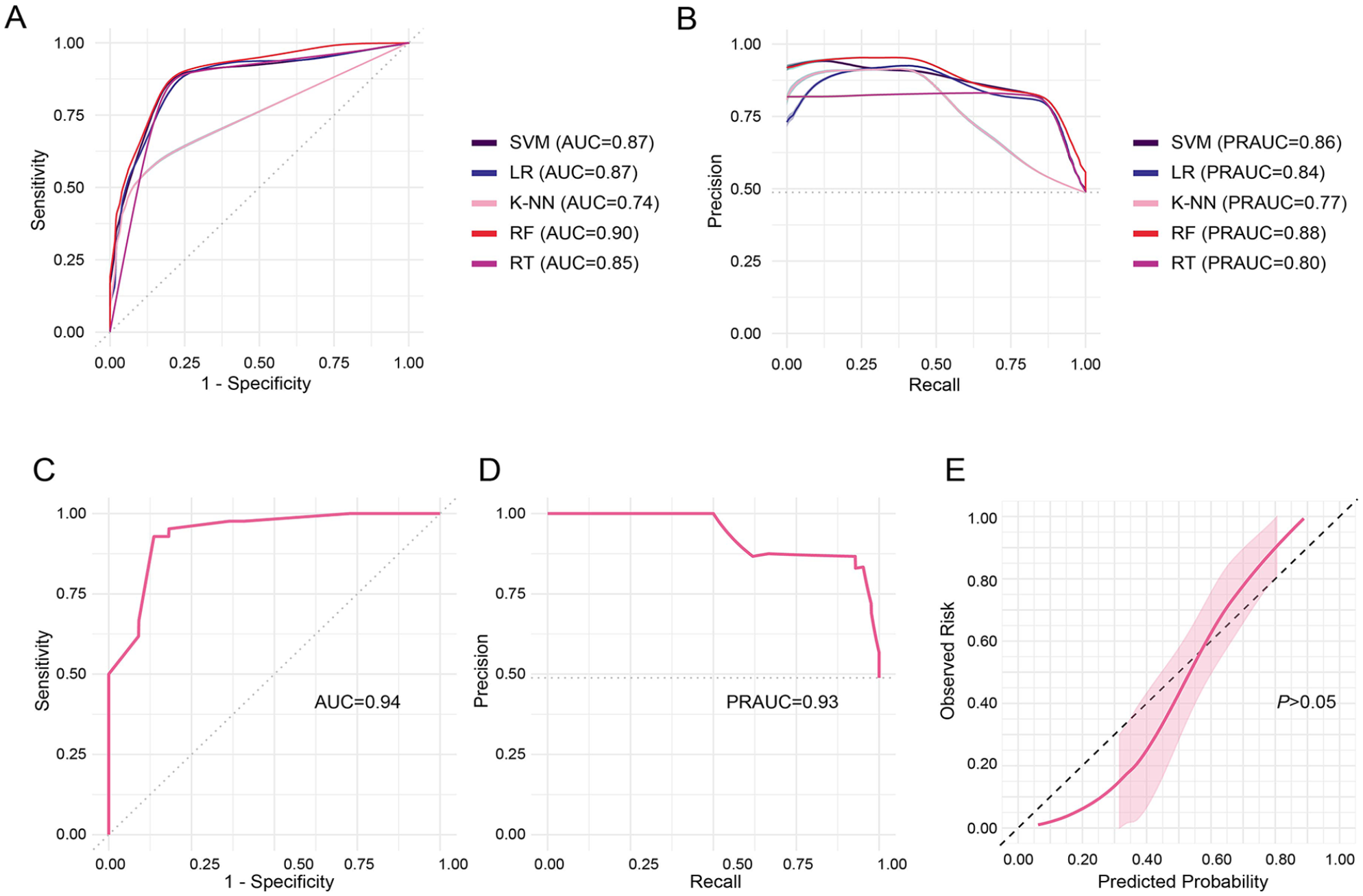
Receiver-operating characteristic curves (A) and precision-recall curves (B) of the models trained with balanced data. Receiver-operating characteristic curve (C), precision-recall curve (D), and calibration curve (E) of the RF model tested with testing dataset. LR, logistic regression; RF, random forest; SVM, support vector machine; k-NN, k-nearest neighbors; RT, regression tree; AUC, area under the receiver-operating characteristic curve; PRAUC, precision-recall area under the curve.
RF Model Performance
Next, the balanced dataset was divided into a training set and a testing set to establish and validate the RF model. Figure 3 illustrates the ROC curve and PR curve of the RF model tested with the testing dataset. In the testing set, the RF model exhibited excellent performance: AUC (0.94), PRAUC (0.93), Accuracy (0.90), Specificity (0.86), Sensitivity (0.93), PPV (0.87), and NPV (0.93) (Table 3). Calibration curve analysis was conducted to evaluate the consistency between the actual and predicted incidence of IVSP with patency loss. The model’s performances were obtained with a predefined random seed. The results indicated that the curve of the RF model fitted well with the standard curve (Figure 3E). The Brier score for the calibration curve is 0.15.
SHAP Analysis
The SHAP method was utilized to elucidate visually how the variables in the model influence IVSP with patency loss. Figure 4A presents potential features assessed by the normalized SHAP value and the importance levels of these features for IVSP with patency loss. A positive SHAP value indicates a positive contribution to the target variable (IVSP with patency loss), while a negative SHAP value suggests a negative contribution. Figure 4B was generated by considering both positive and negative SHAP values.
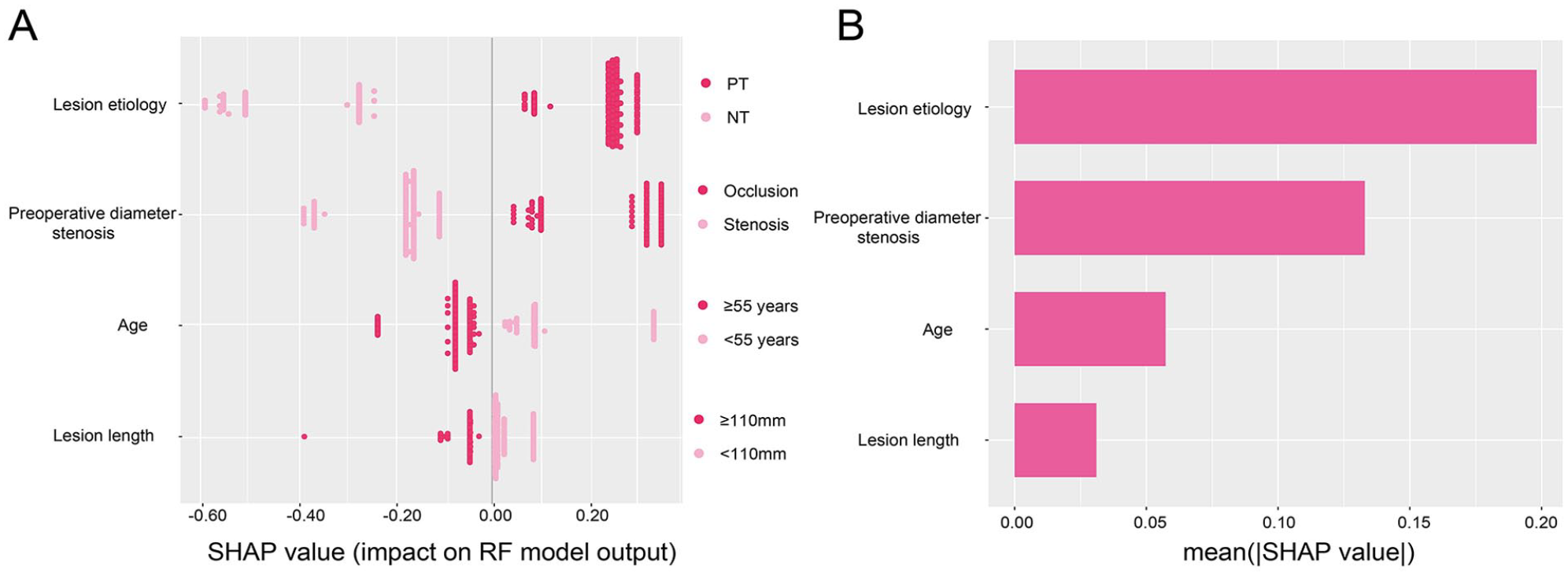
SHAP analysis of the RF model for screening predictors. Feature importance plot according to normalized SHAP values (A). Each point represents a patient. SHAP contribution of each prediction in plot (B). SHAP, Shapley Additive exPlanations; RF, random forest; PT, post-thrombotic; NT, non-thrombotic.
The aforementioned analysis revealed that lesion etiology, preoperative diameter stenosis, and age were the 3 most crucial predictive features for IVSP with patency loss. This observation aligns with the trends observed in the Boruta algorithm results obtained earlier (Supplemental Figure 3). The explanatory power of these 3 indicators for IVSP with patency loss is 19.8%, 13.2%, and 5.69%, respectively. Therefore, patients with thrombotic-type lesions, preoperatively occluded lesions, and age less than 55 years are at an increased risk of losing patency within 1 year after IVSP. With the exception of lesion length, which has the lowest importance, this finding is consistent with the results of the Cox regression.
Risk Assessment Tool
Considering the practicality of the model, our predictive factors demonstrate straightforward patterns. Through variable derivation, all 4 variables are binary, resulting in 16 possible scenarios for the patients. Thus, we simulated a standard matrix containing 16 samples representing 16 patterns of predictive factors. Utilizing the RF model constructed earlier, we predicted the probability of IVSP patency loss for each sample. Samples with a probability greater than 50% were categorized as high-risk patients, while those with a probability less than 50% were categorized as low-risk patients. Consequently, we devised a clinical tool for assessing the risk of patency loss within 1 year after IVSP, named the Etiology-Stenosis-Age-Length (ESAL) Classification (Figure 5A). Subsequently, we applied the clinical tool to predict imbalanced data, resulting in a confusion matrix (Figure 5B). At this juncture, the model’s performance is as follows: Accuracy (0.83), Specificity (0.82), Sensitivity (0.86), PPV (0.32), and NPV (0.98). Models with high NPV may exhibit low PPV, which is reasonably justifiable to some extent. Most indicators demonstrate a satisfactory model, thus, no threshold adjustments were made. The model’s characteristic lies in its ability to accurately identify positive and negative patients, albeit with a high rate of misdiagnosis. Nonetheless, it remains clinically significant.
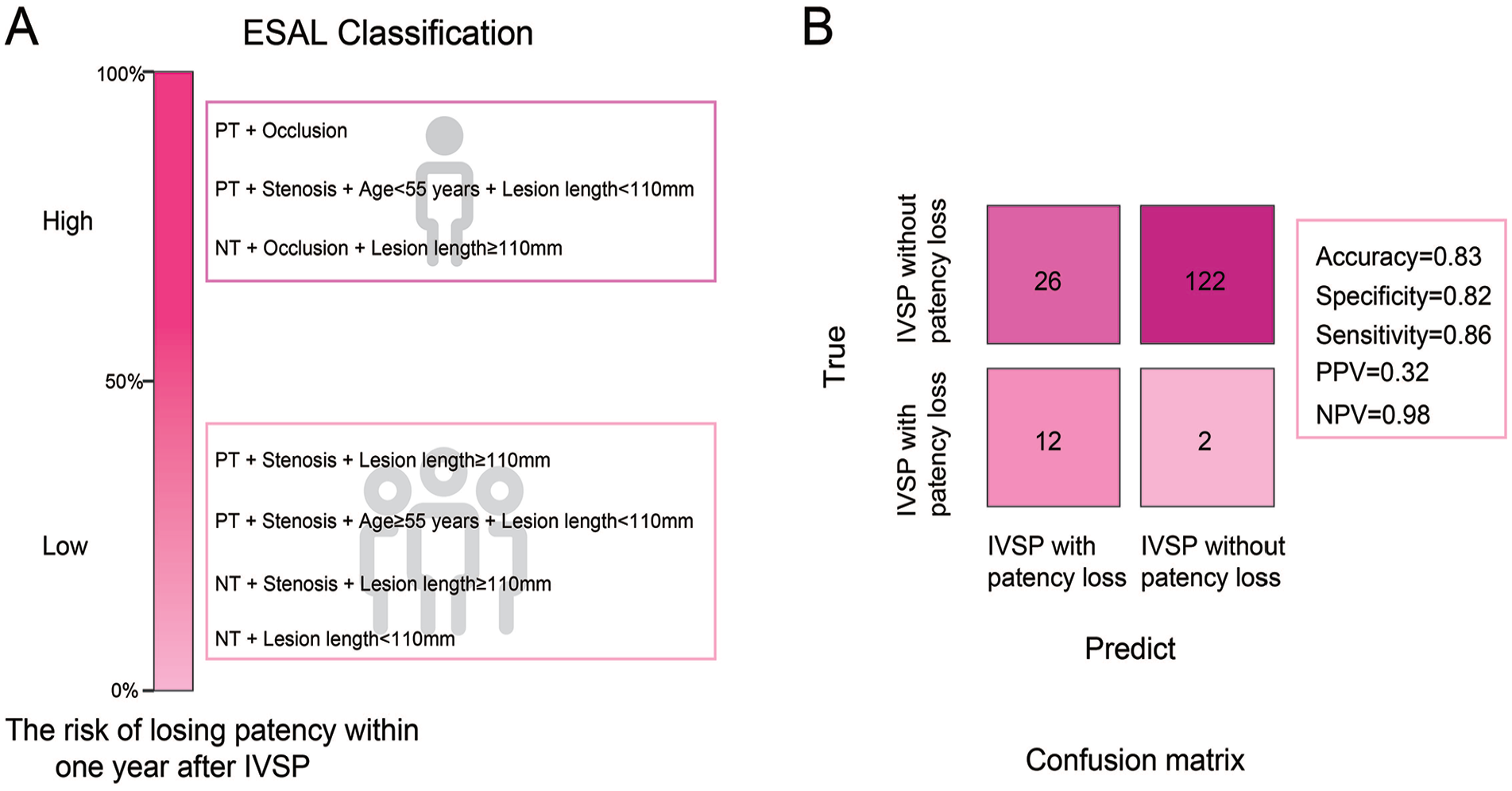
The developed clinical tool for assessing the risk of losing patency within 1 year after IVSP (A). The confusion matrix illustrates the predictive results of the RF model in imbalanced data (B). ESAL, Etiology-Stenosis-Age-Length; IVSP, iliac vein stent placement; RF, random forest; PT, post-thrombotic; NT, non-thrombotic; NPV, negative predictive value; PPV, positive predictive value.
Discussion
Post-IVSP stent surveillance is crucial for promptly detecting stent malfunction and considering interventions in the appropriate clinical context. 27 As mentioned earlier, many studies have investigated factors affecting vascular patency after IVSP.5,8,13 However, limited research has focused on assessing individual risks for patency loss after IVSP. Combining Cox regression analysis and the Boruta method, we identified several independent risk factors associated with patency loss after IVSP, including younger age, PT-type lesions, short-segment lesions, and preoperative target lesion occlusion. Based on these 4 factors, we selected the RF model with excellent performance after benchmarking. Subsequently, we split the data, constructed a risk prediction model for patency loss after IVSP using the training set, and validated the model using the test set, achieving high levels of performance indicators. Finally, we developed a simple risk tool called the ESAL classification and effectively tested this tool using imbalanced data, which to some extent reflects the stability of the data before and after balancing. It is important to note that this tool demonstrates high sensitivity, specificity, and NPV in practical use but may have a higher “misdiagnosis rate.” In summary, this study contributes to enhancing patients’ understanding of their individual risk levels and emphasizes the importance of regular check-ups and disease management for high-risk patients.
Our research has also identified this as a clinically dominant phenotype-driven process, which appears suitable for predictive analysis, unlike phenotypes determined by other multidimensional features. 28 Lesion etiology plays a significant role in the model we constructed. Previous studies have reported inconsistent findings regarding whether there is a difference in patency after IVSP between NT and PT patients, but the current view tends to suggest that PT patients have lower long-term patency rates than NT patients, although the reasons are still unclear.5,9,29,30 Preoperative target vessel occlusion may represent the severity of tissue damage at baseline, which could affect stent support. There are 2 other slightly less important features. It is difficult to provide a reasonable explanation for age, and uncertainty regarding conclusions about age cannot be ruled out here. Our study also found that patients with short-segment occlusions are more likely to experience patency loss within 1 year compared to those with long-segment occlusions (>110 mm). Of course, this is the pattern observed when lesion length is considered a predictor. In association analyses, lesion length is identified as a risk factor for loss of patency following IVSP. Although the cutoff point for this length still needs to be confirmed, previous studies have shown that stent crossing over the inguinal ligament may lead to improved patency rates,1,31 provided that there is a good correlation between lesion length and stent length. Overall, the current model is the result of the “cooperation” of these 4 features, and a single explanation is not very convincing. Furthermore, we know that these 4 features cannot be directly intervened with, which also limits our analysis of their interactions.
The increasing availability of data and software frameworks to create predictive models has allowed the widespread adoption of ML in many applications. However, the high predictive performance of such models often comes at the cost of interpretability. 32 We enhanced the interpretability of the model using SHAP analysis and Cox regression, making it more transparent and increasing clinicians’ confidence in its use. We utilized a nationwide multicenter cohort, which further boosted clinicians’ confidence. Most predictive models lack practicality and simplicity,19,33 and we addressed this issue here. While numerous studies have confirmed the safety and effectiveness of certain venous stents,4–6 the ESAL classification requires further validation in these cohorts. Similar studies are scarce or lack comparability, highlighting the need for more research and systematic reviews in the future. Our study also has some limitations, the most significant being the small sample size, lack of good population representativeness, and poor generalizability. Due to cost considerations, although such studies are numerous, large-scale cohorts are lacking, and future collaboration is needed. The ESAL classification may have a high “misdiagnosis rate” in practical use, requiring careful interpretation. In addition, we do not believe that the ESAL classification can be easily applied to other countries or regions, but its validation is still necessary.
In summary, we have developed a responsible ML model and a clinical tool for stratifying the risk of patency loss within 1 year for IVSP patients. The ESAL classification is simple and user-friendly, with the potential for widespread adoption. Future progress will require more representative cohorts for support.
Supplemental Material
sj-jpeg-1-jet-10.1177_15266028251325393 – Supplemental material for ESAL: A Tool for the Explanatory Prediction of Loss of Patency Within 1 Year After Iliac Vein Stent Placement
Supplemental material, sj-jpeg-1-jet-10.1177_15266028251325393 for ESAL: A Tool for the Explanatory Prediction of Loss of Patency Within 1 Year After Iliac Vein Stent Placement by Chang Sheng, Baihong Pan, Pu Yang and Wei Wang in Journal of Endovascular Therapy
Supplemental Material
sj-jpeg-2-jet-10.1177_15266028251325393 – Supplemental material for ESAL: A Tool for the Explanatory Prediction of Loss of Patency Within 1 Year After Iliac Vein Stent Placement
Supplemental material, sj-jpeg-2-jet-10.1177_15266028251325393 for ESAL: A Tool for the Explanatory Prediction of Loss of Patency Within 1 Year After Iliac Vein Stent Placement by Chang Sheng, Baihong Pan, Pu Yang and Wei Wang in Journal of Endovascular Therapy
Supplemental Material
sj-jpeg-3-jet-10.1177_15266028251325393 – Supplemental material for ESAL: A Tool for the Explanatory Prediction of Loss of Patency Within 1 Year After Iliac Vein Stent Placement
Supplemental material, sj-jpeg-3-jet-10.1177_15266028251325393 for ESAL: A Tool for the Explanatory Prediction of Loss of Patency Within 1 Year After Iliac Vein Stent Placement by Chang Sheng, Baihong Pan, Pu Yang and Wei Wang in Journal of Endovascular Therapy
Footnotes
Acknowledgements
The original data for this study come from a clinical investigation of the safety and effectiveness of venous stents. We would like to express our gratitude to the patients who participated in this clinical study, the investigators, and the data managers.
Author Contributions
C.S.: Conceptualization, Data curation, Formal analysis, Methodology, Validation, Writing—original draft; B.P.: Conceptualization, Methodology; P.Y.: Methodology, Supervision, Writing—review & editing: W.W.: Methodology, Supervision, Writing—review & editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The clinical study was sponsored by Shanghai EndoVas Medical Technology Co., Ltd.
Consent for Publication
All authors disclosed no relevant relationships.
Ethics Approval and Consent to Participate
Ethical approval has been obtained for this research study.
Data Sharing
The datasets used and/or analyzed during the current study are available from the corresponding authors upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.