
Abstract
Objective:
To present the current outcomes of fenestrated and branched endovascular aneurysm repair (F/BEVAR) for rescue of proximal endograft failure after endovascular aneurysm repair (EVAR). A systematic review of the currently published literature on F/BEVAR for failed EVAR is undertaken, and the eligible studies are combined into a meta-analysis with the intention of evaluating the safety, efficacy, and the durability of this treatment option.
Materials and Methods:
A systematic review of the literature up to September 2024 was performed according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (CRD42024590847). Studies were included in the meta-analysis if they reported ≥10 patients and at least one of the major outcomes was stated. Primary endpoint was technical success (efficacy). Secondary endpoints included 30-day/in-hospital mortality and morbidity (safety) and survival and reinterventions rate (durability). Methodological quality and robustness of the results of the eligible articles were assessed according to Joanna Briggs Institute (JBI’s) critical appraisal tool.
Results:
A total of 16 studies with overall 1079 patients were included. The pooled estimate for technical success was 94.4% (95% CI 92.5–95.8), whereas for the 30-day/in-hospital mortality 3.9% (95% CI 2.9–5.4). Permanent paraplegia was developed in a pooled rate of 1.6% (95% CI 0.8–3.0), whereas a cerebrovascular event in a pooled rate of 1.5% (95% CI 0.9–2.8). An acute renal function impairment requiring new onset dialysis occurred with a pooled rate of 4.4% (95% CI 3.2–6.1). Postoperative respiratory failure was observed with a pooled estimate of 7.2% (95% CI 5.5–9.4). The pooled estimate for 12-month overall survival was 88% (95% CI 83.4–91.4), and the pooled estimate for 24- and 36-month survival were 79.8% (95% CI 75.6–83.4) and 72.2% (95% CI 66.7–77.2), respectively. Freedom from reintervention was estimated at 83.7% (95% CI 79.9–86.9) for 12 months, 75.8% (95% CI 61.0–86.2) for 24 months and 59.3% (95% CI 36.5–78.7) for 36 months.
Conclusion:
This study showed that F/BEVAR is a feasible, safe, and reliable strategy for achieving proper proximal endograft sealing when previous EVAR has failed. The midterm survival of these patients is acceptable, whereas reinterventions are not negligible.
Clinical Impact
This work summarizes the current experience with fenestrated and branched endovascular aneurysm repair for the rescue of failed endovascular aneurysm repair in the most contemporary meta-analysis including 16 studies with a total of 1079 analyzed patients. Feasibility of the method is proven with a technical success of 94.4%, whereas a 30-day/in-hospital mortality of 3.9% was recorded. The compromised survival and freedom from reinterventions rates (72.2% and 59.3% for 36 months, respectively) pose, however, concerns regarding durability of the method.
Keywords
Introduction
In the past decade, the treatment of infrarenal abdominal aortic aneurysms (AAAs) has predominantly shifted toward the endovascular aneurysm repair (EVAR) as opposed to open surgical repair, with excellent postoperative results especially seen in the reduction of short-term mortality. 1 However, it is not an operation without complications, and as experience is accumulated, increasing data underline this concern. The need for reintervention after standard EVAR has been documented to be >20% as the follow-up period is extended and is correlated with decreased patient survival. 2 The loss of proximal sealing can occur after disease progression, graft deployment outside instructions for use, poor graft placement, and extreme graft oversizing. Results are a stent-graft migration and an endoleak type Ia, which is associated with elevated sac pressure and subsequent continued risk of rupture, necessitating complex correction techniques.3,4
The current guidelines recommend that in such a setting endovascular modalities should be the initial attempt, when technically feasible.5,6 Despite the rising incidence of failed EVAR, a conversion to open repair is still associated with considerable mortality and morbidity rates, as an involvement of renal and visceral arteries, as well as, a wider aortic exposure is usually required in older patients.7,8 Therefore, several endovascular strategies have been applied to rescue a failing EVAR. These include a simple aortic cuff implantation, 9 embolization techniques,10 –12 or recently the use of endoanchors13,14 in cases of favorable infrarenal neck anatomy. However, in cases of unfavorable infrarenal neck, more complex modalities are required for extending the proximal sealing zone. Adopting the chimney technique15 –17 offers an off-the-shelf endovascular solution with the inherent risk for persistent endoleak and not fully elucidated long-term outcomes.
On the other hand, fenestrated and branched EVAR (F/BEVAR), which emerged as new techniques to treat more complicated cases with an endovascular approach, are being used with increasing frequency for the rescue of failed EVAR over the last decade.18–33 The early experience with F/BEVAR to rescue failing EVAR underlined the unique technical difficulties, due to the presence of the previous EVAR stent-graft, that can pose considerable challenges.34,35 As new era vascular surgeons will have to deal more and more frequently with failed EVAR, it is important to advance understanding of the use of F/BEVAR for rescue of proximal endograft failure.
Objective of this study is to present the current outcomes of F/BEVAR for rescue of proximal endograft failure after infrarenal EVAR. A systematic review of the currently published literature on FEVAR/BEVAR for failed EVAR is undertaken, and the eligible studies are combined into a meta-analysis with the intention of evaluating the safety, efficacy, and the durability of this treatment option.
Materials and Methods
Study Protocol and Registration
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and the Meta-analyses of Observational Studies in Epidemiology (MOOSE) guidelines were applied for the design, conduction, and reporting of this meta-analysis.36,37 In addition, the present meta-analysis has been registered in PROSPERO public database prior to study initiation (CRD42023473403).
Eligibility Criteria
A study was considered eligible for the present meta-analysis if
Reported on the application of F/BEVAR for treatment of failed EVAR. At least one target vessel (TV; including renal arteries, coeliac trunk, or mesenteric arteries) had to be included with either a branched (including side branch, inner branch, antegrade, and retrograde) or fenestrated device (custom-made, off-the-shelf, physician modified).
Included ≥10 patients. With the intention of averting the bias of learning curve, small case series and case reports were excluded.
At least one of the major outcomes (primary technical success, postoperative complications, mortality, reinterventions rate) was stated.
Articles in languages other than English were excluded. Animal studies were not included. Reports on failed EVAR treatment by conventional surgical or other endovascular approaches (ie, Chimney technique, endoanchors) were also excluded. Moreover, studies reporting on treatment of failed previous FEVAR were not included in the present review.
Furthermore, several studies included patients with failed EVAR treated with F/BEVAR as a subset of the entire study cohort. These were included in the present review if separate data for this patient subgroup was provided. When multiple publications on the same patient population were identified or study populations overlapped, only the latest report was included, unless the reported outcomes were mutually exclusive.
Search Strategy
A multiple electronic search up to September 2024 was performed in Medline (database provider PubMed), Web of Science Core Collection, EMBASE (database provider Ovid), and Cochrane Central Register of Controlled Trials databases for articles reporting on FEVAR/BEVAR for failed EVAR. These databases were searched with an unrestricted search strategy using exploded medical subject heading terms (MeSH) “failed EVAR,” “endoleak type Ia,” “aortic aneurysm,” “endovascular repair,” “fenestrated,” “branched,” “physician modified stent-graft,” “surgeon modified stent-graft,” or combination of them. All studies were independently assessed by 2 reviewers at the title and abstract levels, and the full text of the studies was retrieved. Disagreements were resolved through consensus. In addition, a “snowball process” was conducted in the reference lists of the investigated articles to capture additional eligible articles.
Data Extraction Process
Data were independently extracted by 2 reviewers and collected into a pre-designed data extraction form. The following data were extracted: first author’s name; centre; publication year; study design; recruitment period; total number of patients; participants demographics and baseline characteristics; maximal aneurysm diameter; time interval from the index procedure; design of stent-grafts used (custom-made, off-the-shelf, physician modified); setting of the procedure (rupture, symptomatic, large diameter or rapid growth, or elective); intraoperative details (adjunctive procedures, number of TVs total procedure duration, fluoroscopy time, contrast agent volume). Primary outcome data (efficacy) included technical success, defined as successful deployment of the main aortic graft, successful catheterization of all fenestration(s)/branches, and deployment of the intended bridging stents/stent grafts into the TV(s), with patency of the endograft and all TVs without any endoleak (EL) type I or type III as evidenced by intraoperative completion angiography. 38 Further outcome variables (safety) included in-hospital or 30-day mortality, postoperative neurological complications (stroke or transient ischemic attack; paraplegia or paraparesis), myocardial infarction, respiratory failure requiring prolonged ventilation (>24 hours or re-intubation), renal failure requiring dialysis, and bowel ischemia requiring surgery. Durability outcome data included follow-up period; late complications and reinterventions, endoleak detection during follow-up, survival, TV patency, and freedom of reintervention. In case of discrepancies in obtained results, the relative articles were re-analyzed by the 2 reviewers and consensus was reached.
Quality Assessment of the Eligible Studies
Methodological quality and robustness of the results of the eligible articles were assessed according to Joanna Briggs Institute (JBI’s) critical appraisal tool evaluating the following domains: definition of inclusion criteria, description of study population, reporting of interventional parameters, reporting of outcomes or follow-up results, and statistical analysis applied 39 (Supplemental Table 1).
Statistical Analysis
Standard descriptive statistics [reported as mean with 95% confidence interval (CI)] were used to summarize demographical and baseline data of the recruited patients from all eligible studies. Furthermore, separate meta-analyses were carried out on all included studies for technical success, neurological complications (stroke, TIA, paraplegia), as well as 30-day/in-hospital mortality, and survival and freedom of reintervention rates. For events during follow-up (late reinterventions, late endoleaks), we calculated the incidence rates (IRs) with 95% CIs per 100 patient-years (p-ys) as the number of patients with outcome events occurring during the specific time period divided by the total number of p-ys. In contrast to crude percentages, IRs take into account differences in the follow-up duration among the eligible studies. The corresponding crude percentages and IRs (95% CIs) were, thereafter, transformed into quantities using the Freeman–Tukey variant of the arcsine square root transformed proportion. 40 The pooled effect estimates were calculated as the back-transformation of the weighted mean of the transformed proportions, using inverse arcsine variance weights for the fixed-effects model and DerSimonian–Laird weights for the random effects model. 41 Heterogeneity among studies was estimated by chi-squared test and Cochran Q score (reported as I2) and corresponding Egger’s regression tests were used as a measure of estimating publication bias. 42 Sensitivity analysis was performed regarding the design of the used stent-grafts (manufactured or physician modified). The meta-analysis was conducted by using the Comprehensive Meta-analysis Package (Biostat, Englewood, NJ, USA) statistical software.
Results
The initial electronic research yielded a total of 404 study titles; 7 further studies were identified through the “snowball” process. The review of the titles and abstracts revealed that 177 studies were irrelevant at the first screening stage. Thus, 234 reports were evaluated further. Of these, 218 were excluded for 1 or more of the following reasons: provided data on chimney technique (n = 9); reported on open repair (n = 55); provided data on F/BEVAR after failed FEVAR (n = 6); case reports, technical notes, or case series with >10 patients (n = 18); editorial and review articles (n = 6); provided mixed data on de novo AAAs and failed EVAR (n = 51); were irrelevant (n = 53); reported on overlapping patients population (n = 14; Figure 1). Finally, 16 studies,18–33 with a total of 1079 patients (1838.70 p-ys), were deemed eligible for inclusion in the meta-analysis (Table 1 and Figure 1).
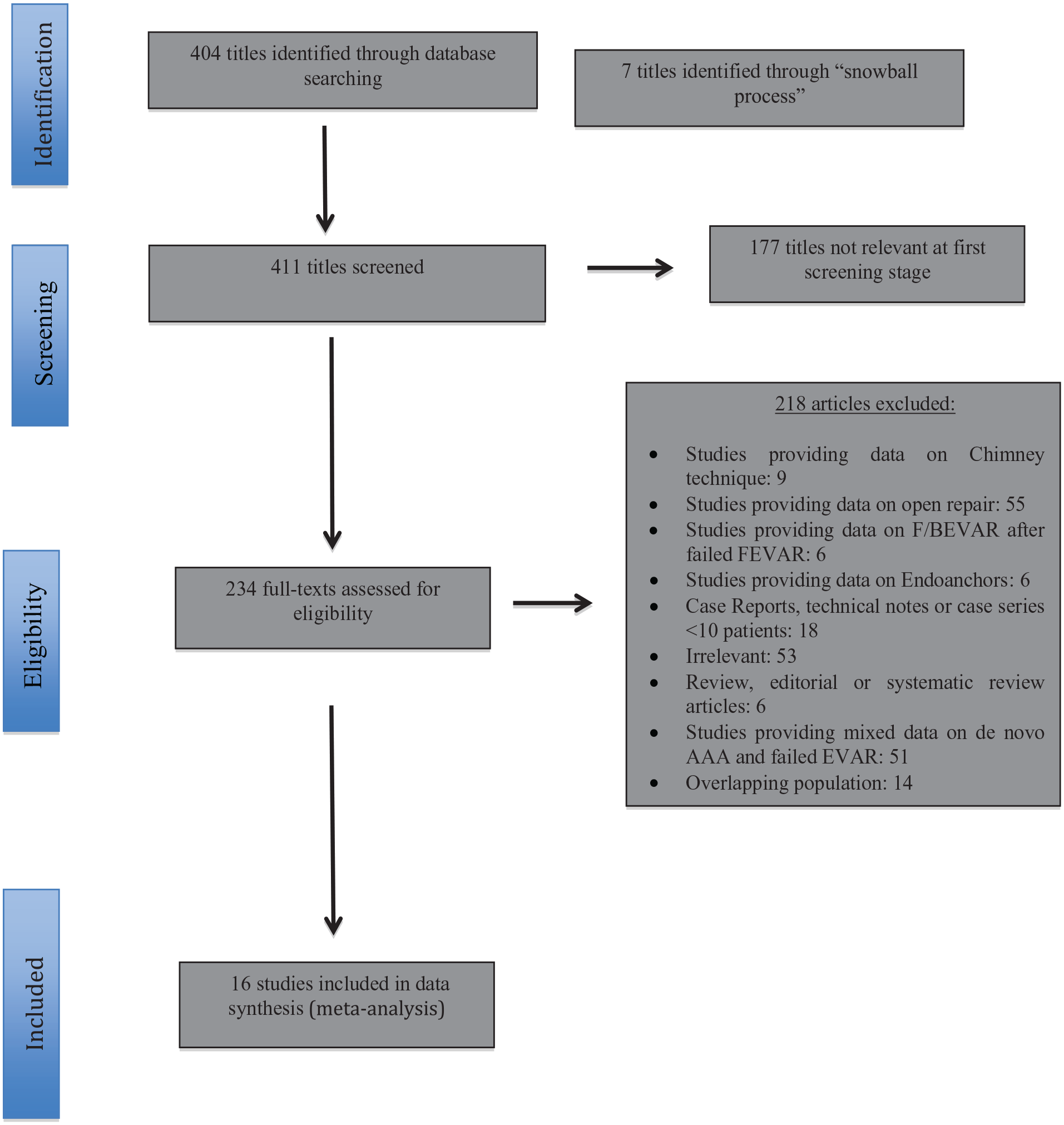
Study flow chart (“Preferred Reporting Items for Systematic reviews and Meta-Analysis” diagram).
Baseline Characteristics of the 16 Eligible Studies Included in the Meta-Analysis.
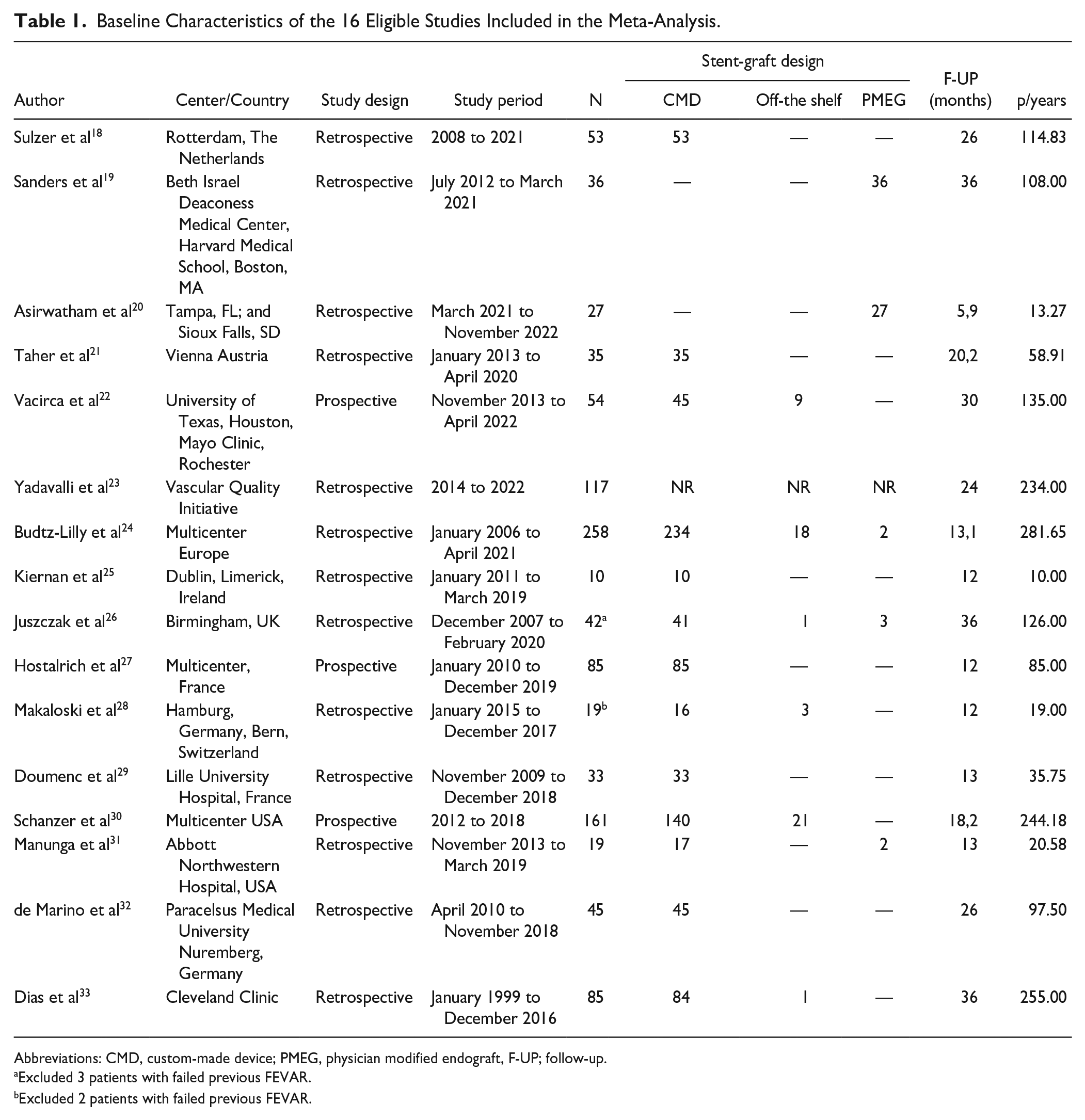
Abbreviations: CMD, custom-made device; PMEG, physician modified endograft, F-UP; follow-up.
Excluded 3 patients with failed previous FEVAR.
Excluded 2 patients with failed previous FEVAR.
Among the 1079 patients included in our analysis, 950 (88.0%) were men, and the mean age was 76.1 years (95% CI 74.7–77.6 years). Patient demographics and comorbidities are provided in Table 2. The mean maximum aneurysm diameter was 69.8 mm (95% CI 67.6–72.1), whereas the mean time interval from initial EVAR procedure was 66.8 months (95% CI 48.9–84.7 months). The vast majority of the patients (94.2%) were operated on an elective setting, whereas 4.5% and 1.3% of the patients were operated on an urgent or emergent setting, respectively. A variety of fenestrated or branched stent-grafts were used: 87.3% of the patients received a stent-graft with a custom-made design, 7.3% of the patients were treated with a physician-modified endograft (PMEG), and 5.4% were treated with off-the-shelf branched devices. The pooled estimate for mean fluoroscopy time was 73.8 minutes (95% CI 64.3–83.4 minutes, I2 = 66.9%), a mean of 124.3 ml (95% CI 111.4–137.1 ml, I2 = 87.8%) of iodinated contrast agent was used and the pooled estimated for the mean OR duration was 161.6 minutes (95% CI 114.3–747.8 minutes, I2 = 99%).
Demographics and Baseline Characteristics of the Analyzed Patients.
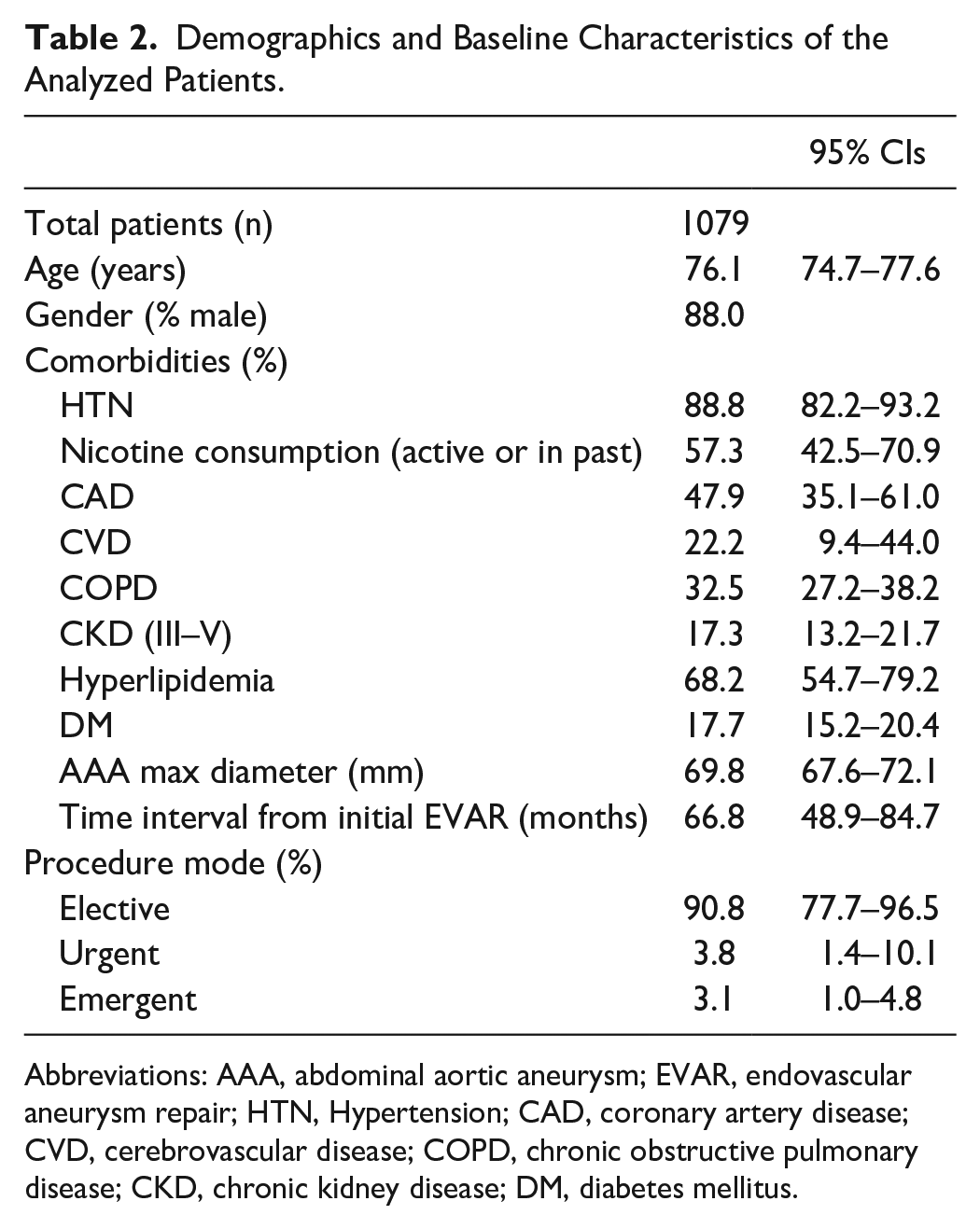
Abbreviations: AAA, abdominal aortic aneurysm; EVAR, endovascular aneurysm repair; HTN, Hypertension; CAD, coronary artery disease; CVD, cerebrovascular disease; COPD, chronic obstructive pulmonary disease; CKD, chronic kidney disease; DM, diabetes mellitus.
Regarding TVs data were provided in 9 studies18,20,22,25,27,28,31–33 with a total of 1390 vessels being incorporated in the repairs with either a fenestration (84.9%), a branch (directional or inner; 10.6%), or a scallop (4.4%).
Outcomes
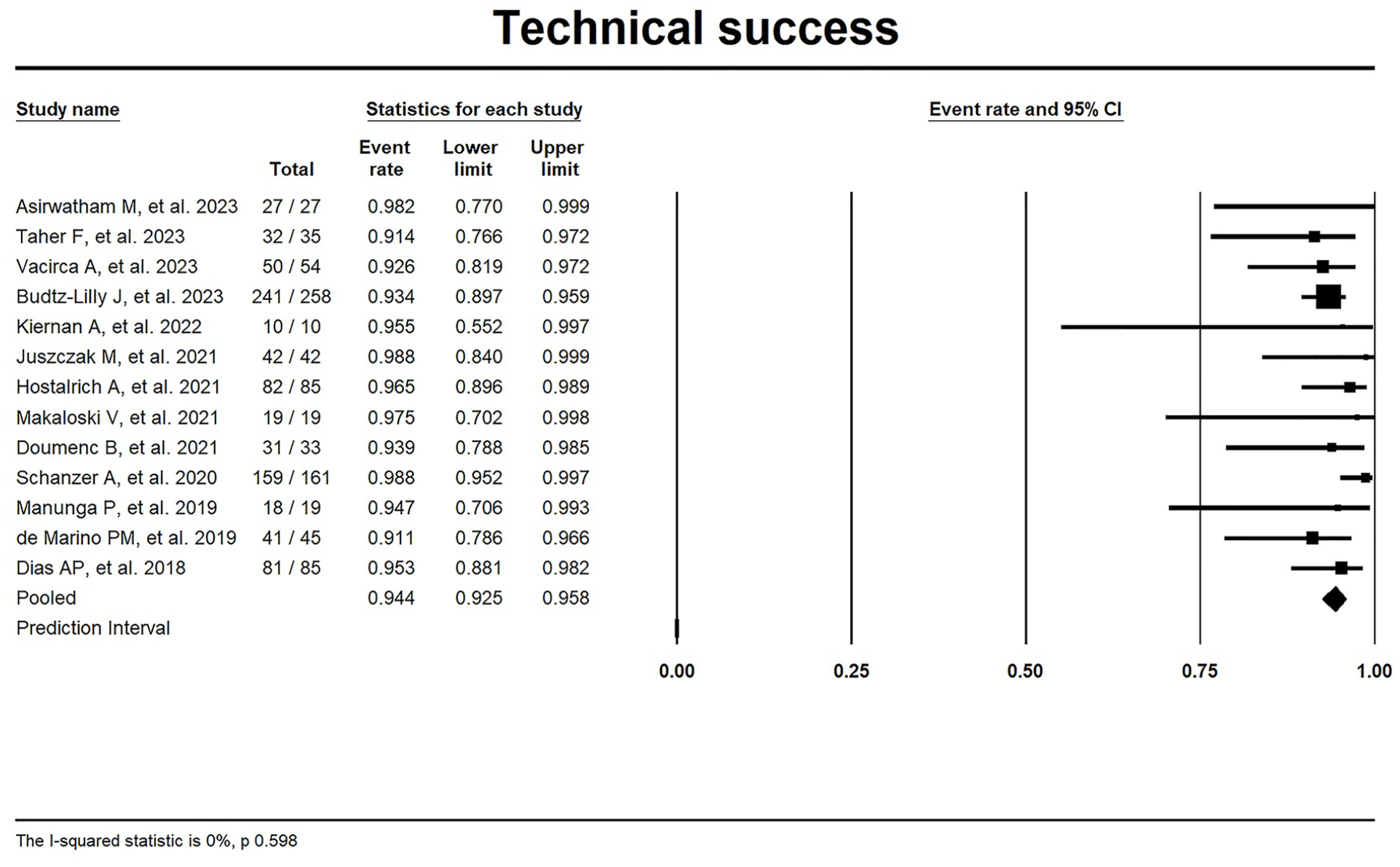
Forest plot for technical success.
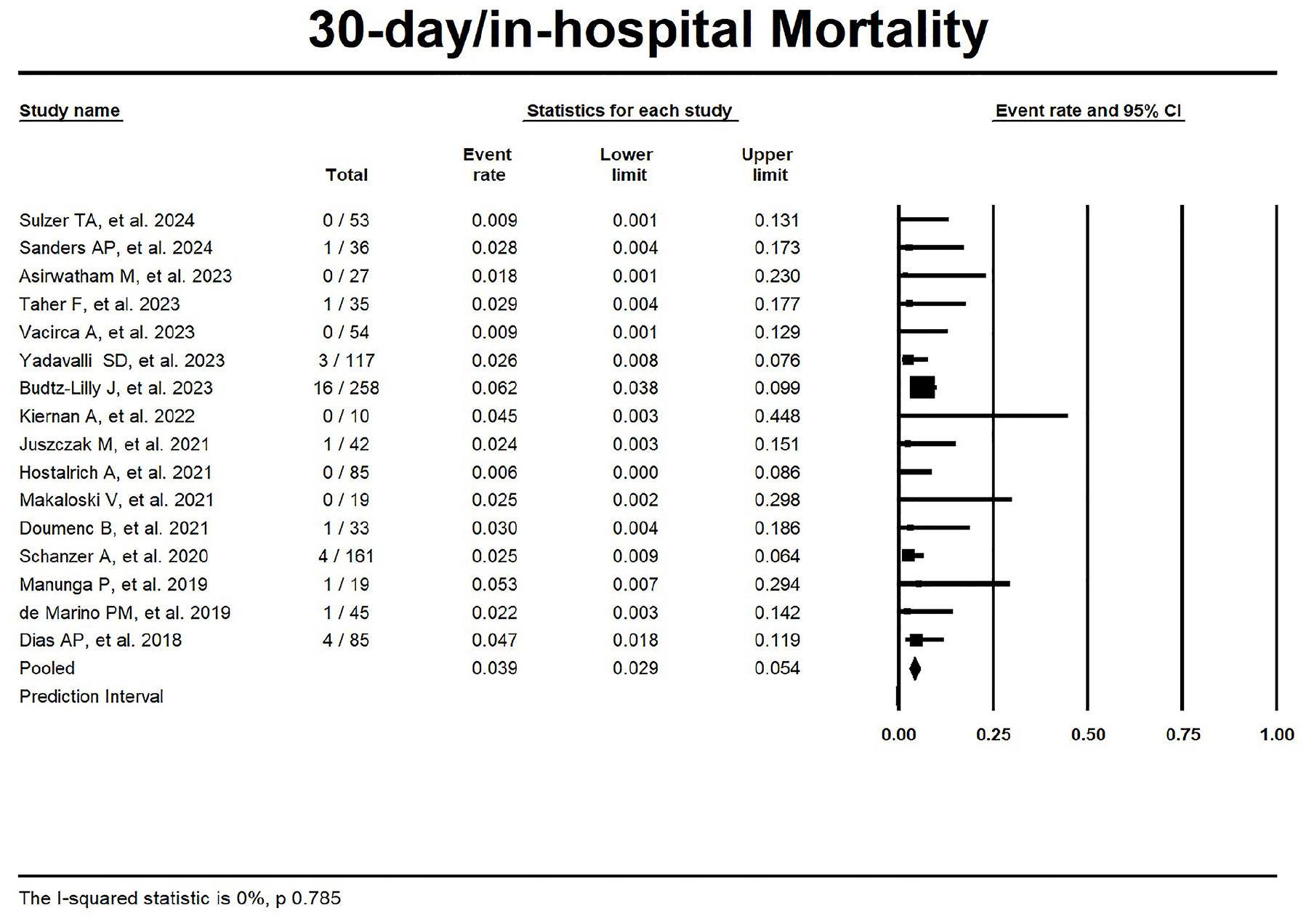
Forest plot for 30-day/in-hospital mortality.
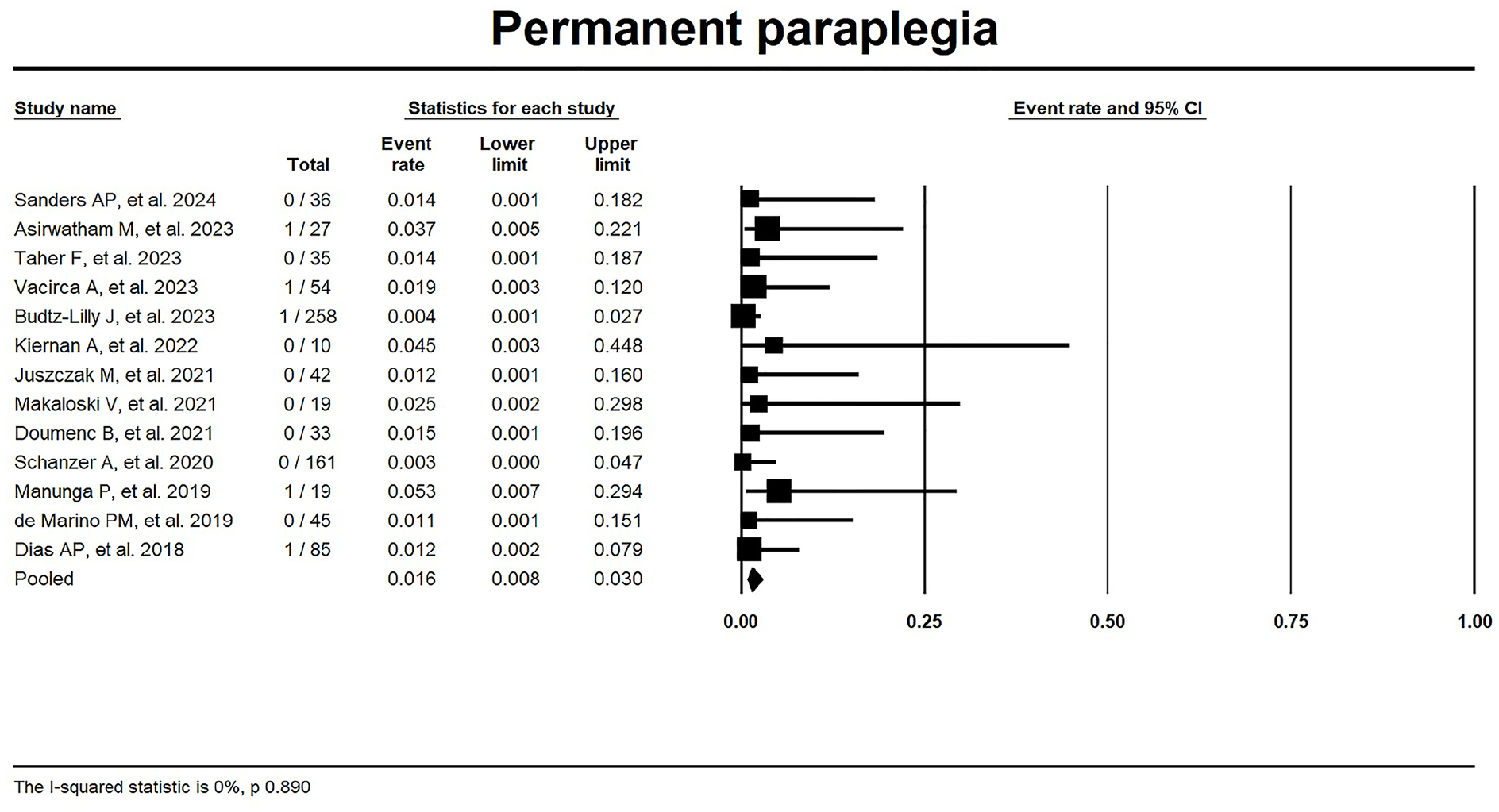
Forest plot for permanent paraplegia.
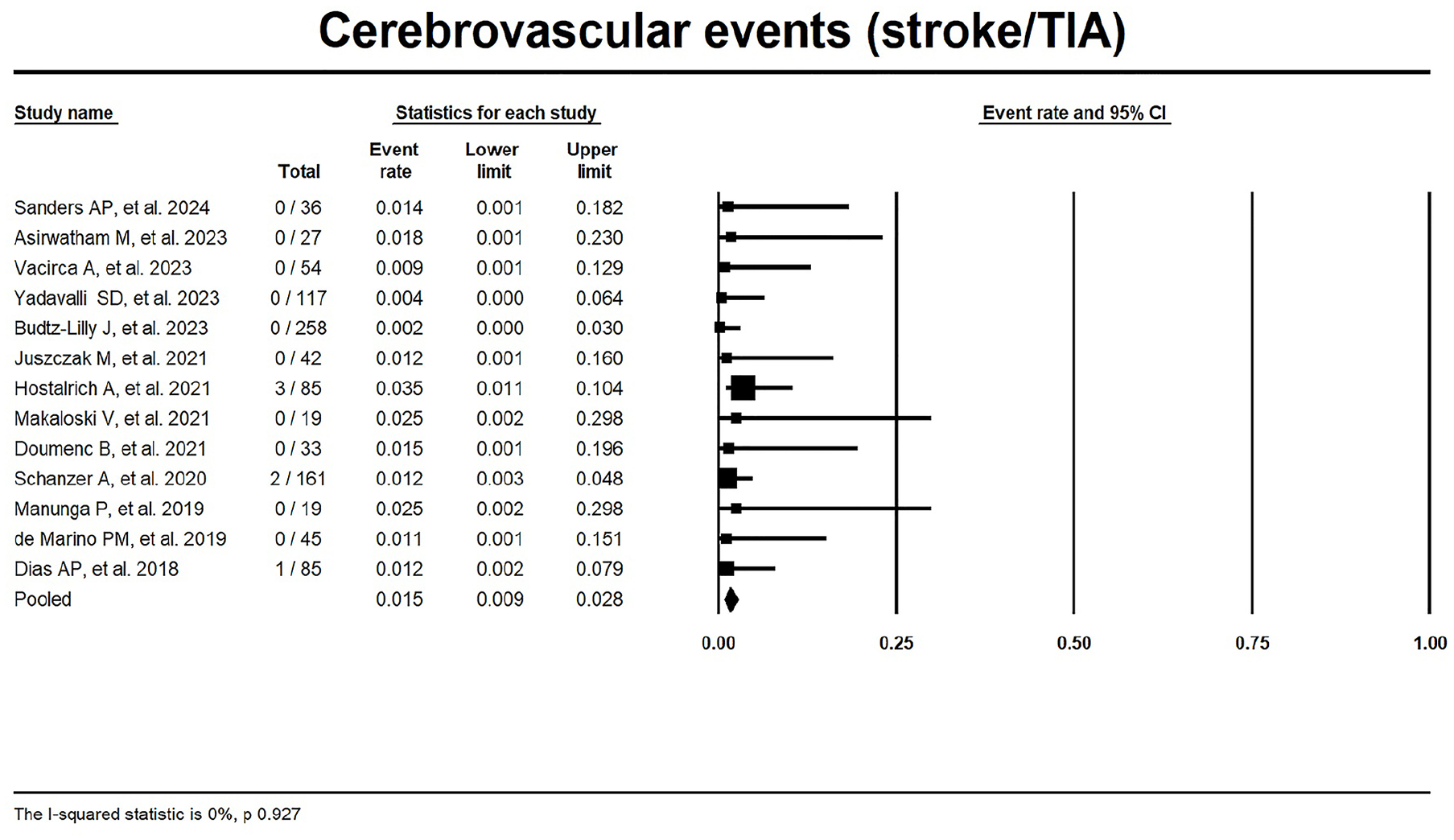
Forest plot for cerebrovascular events (stroke/TIA).
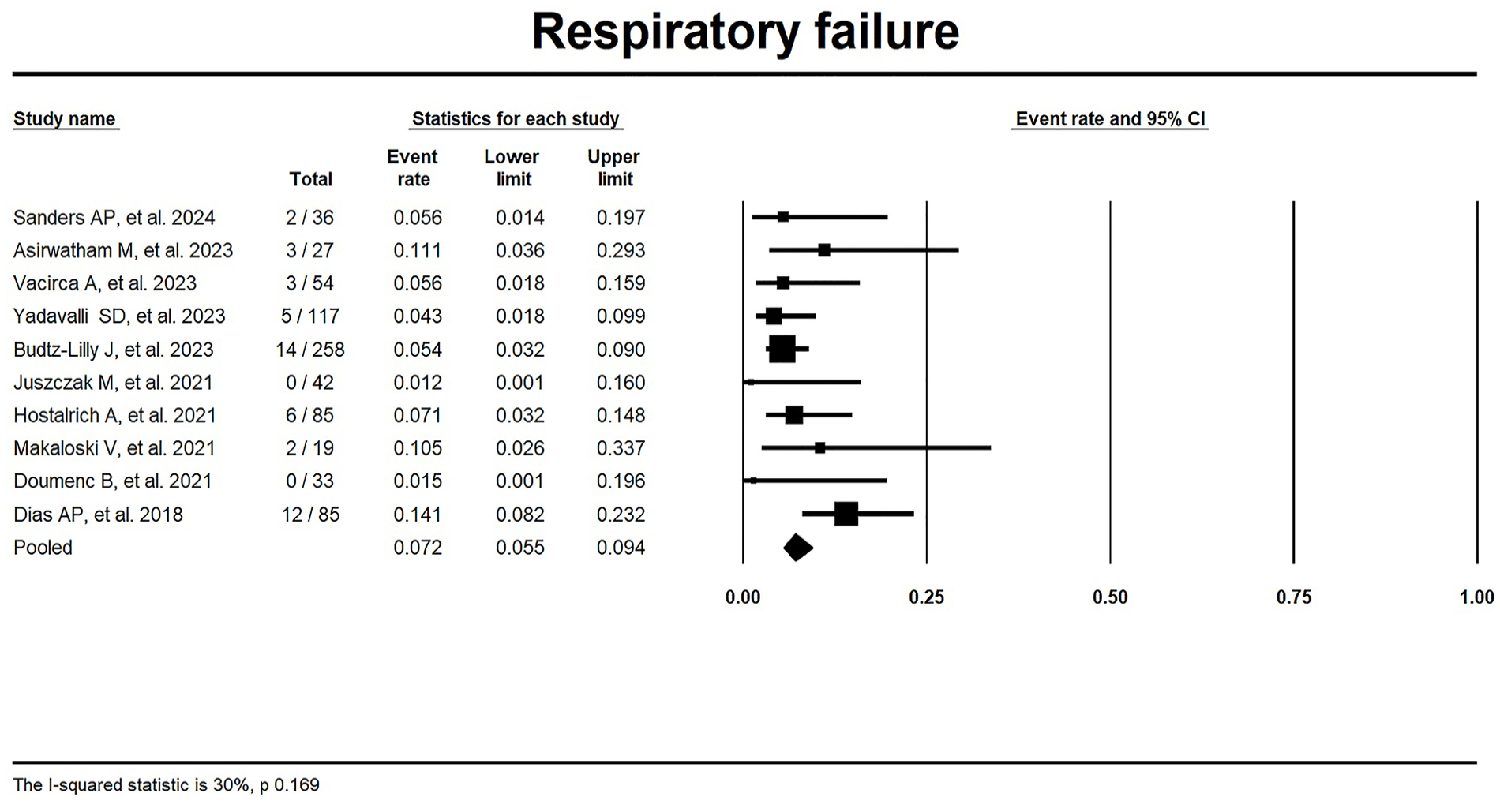
Forest plot for respiratory failure requiring prolonged mechanical ventilation or re-intubation.
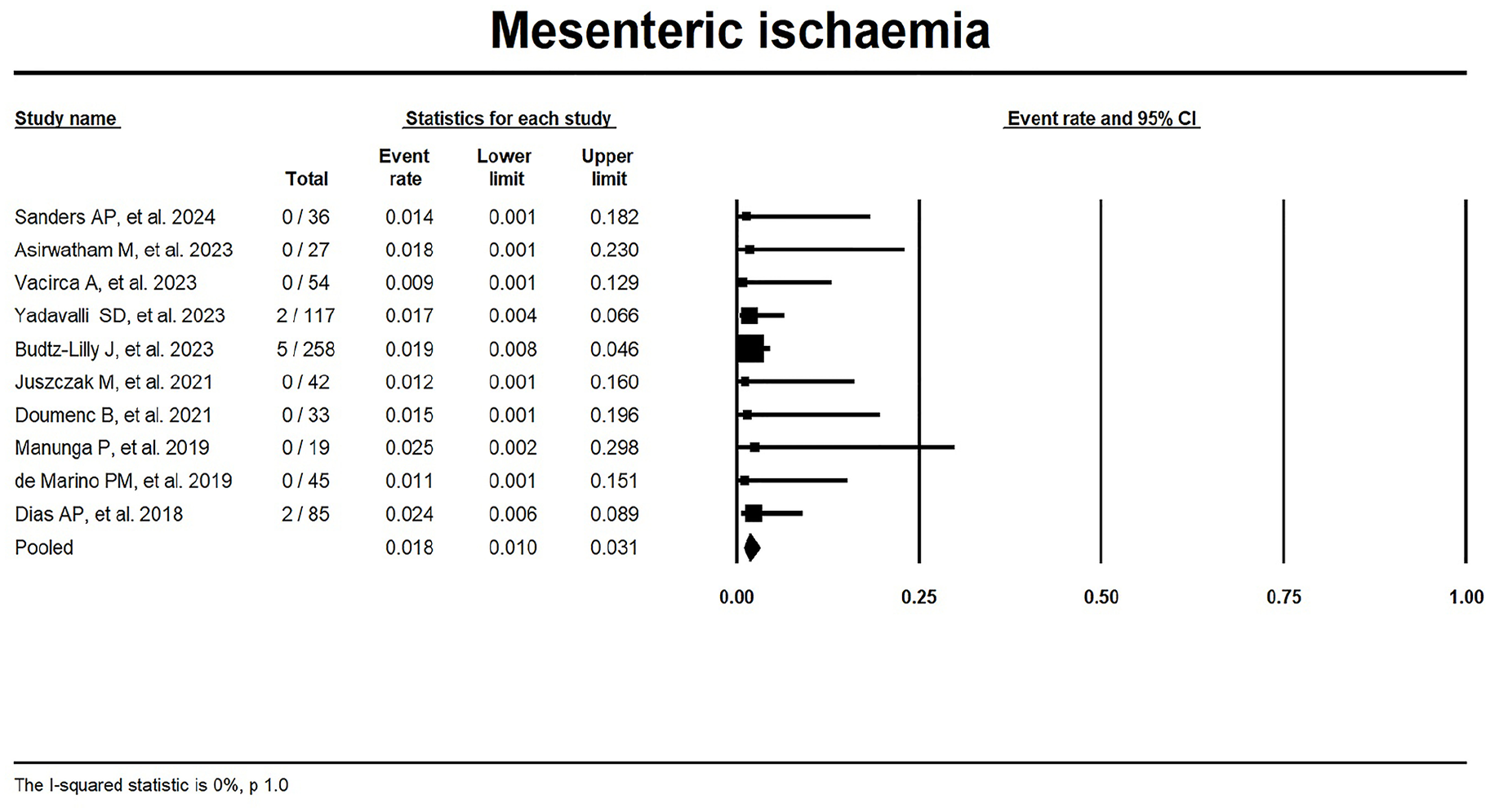
Forest plot for mesenteric ischemia.
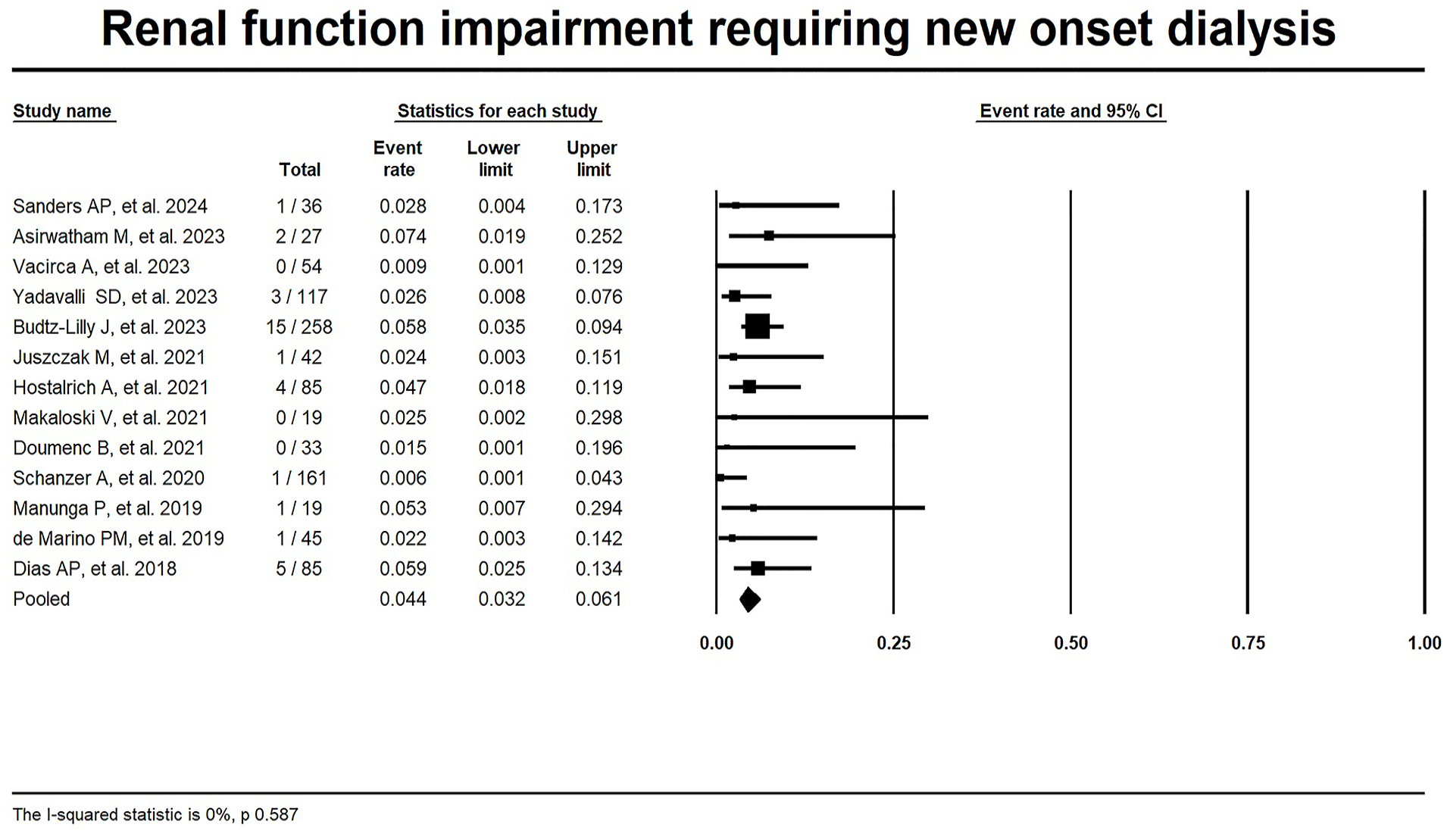
Forest plot for renal function impairment requiring new onset dialysis.
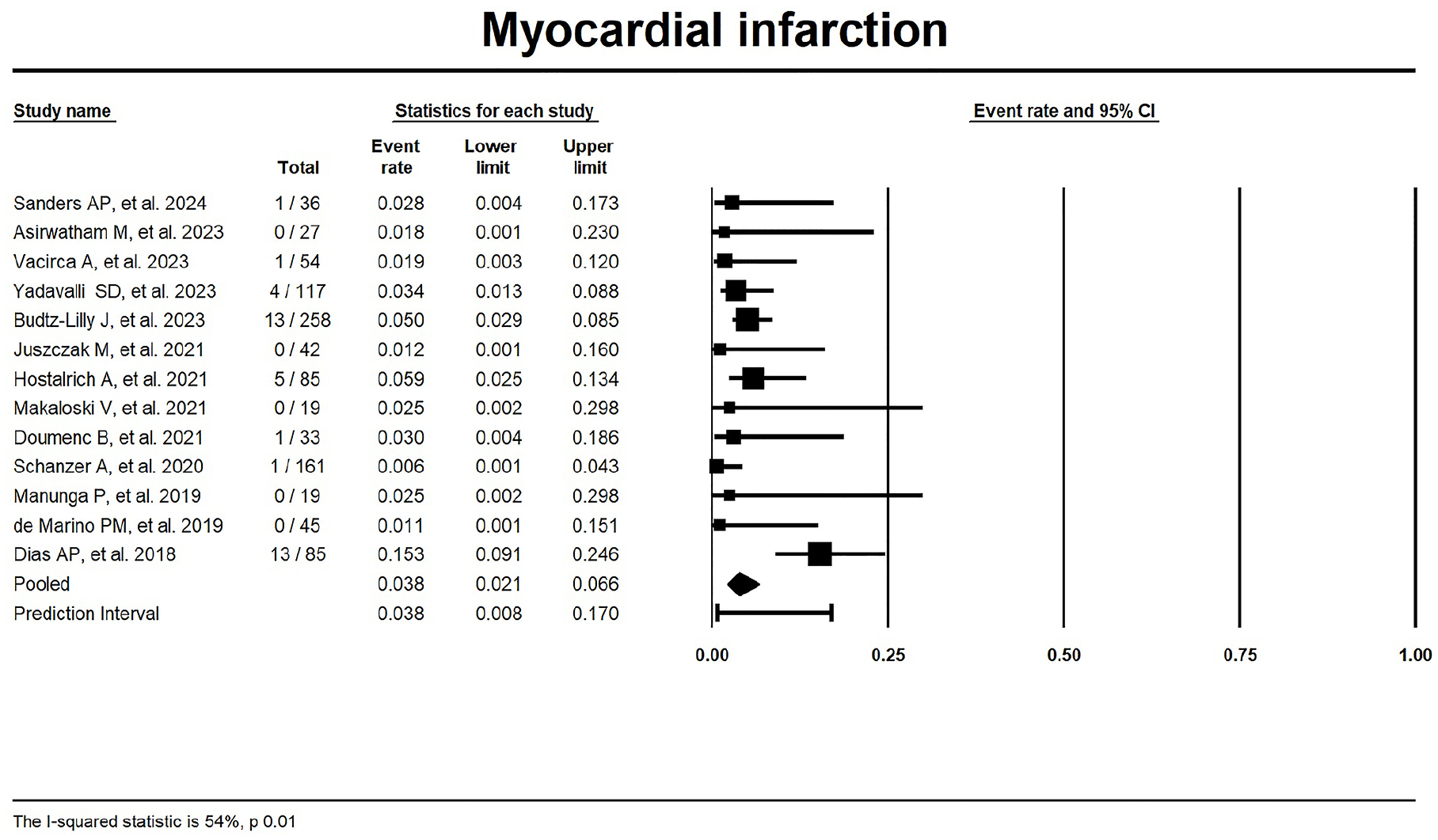
Forest plot for myocardial infarction.
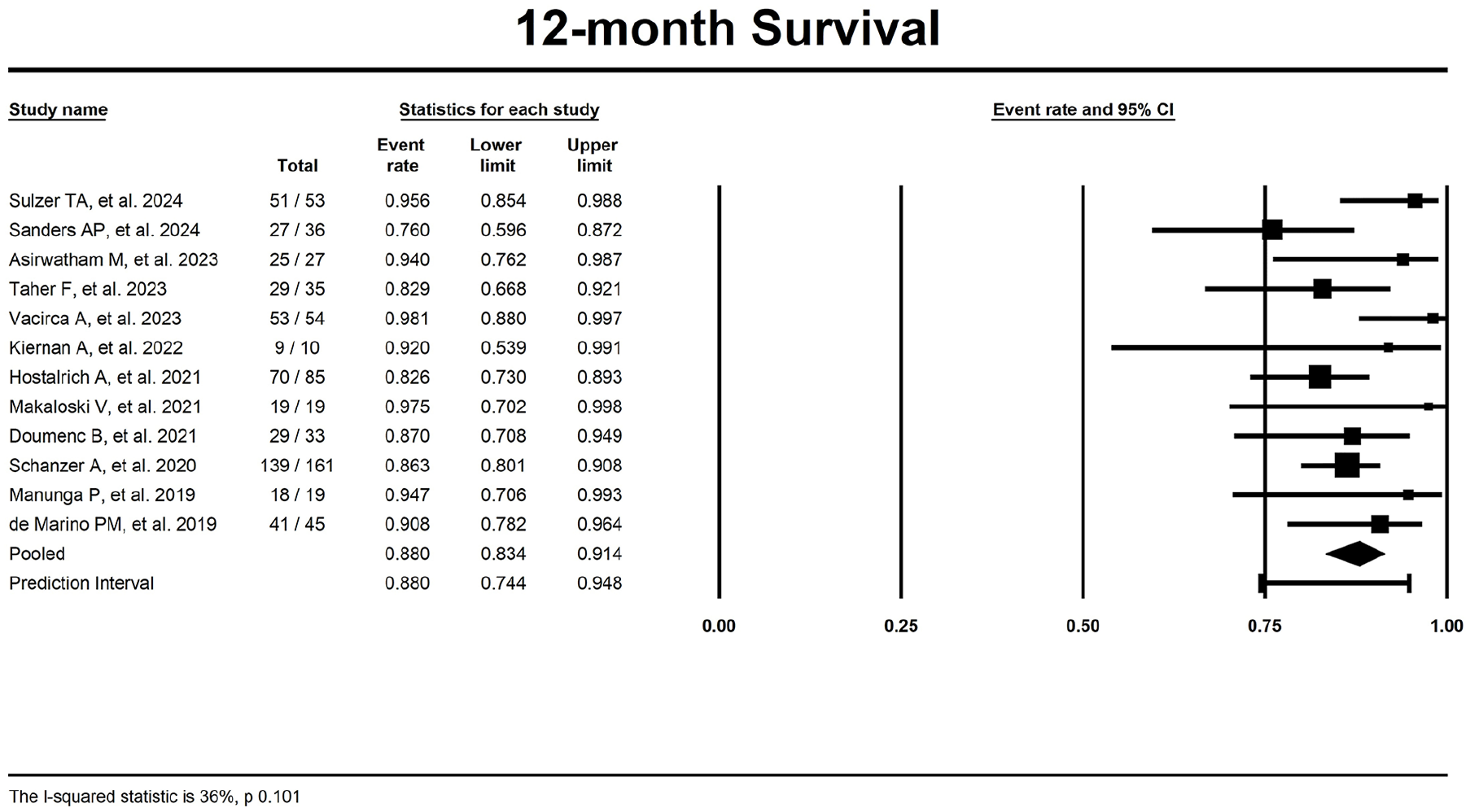
Forest plot for 12-month overall survival.
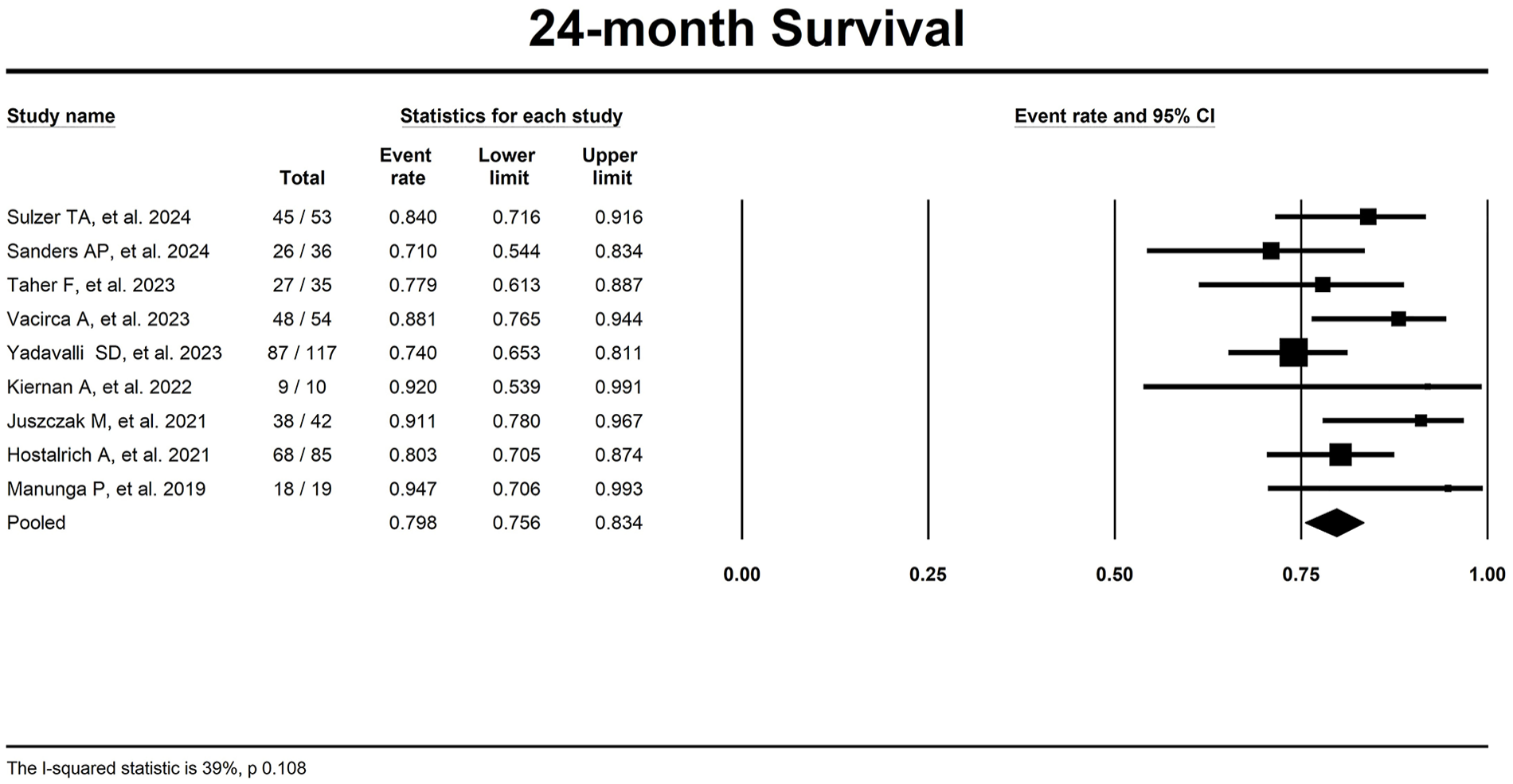
Forest plot for 24-month overall survival.
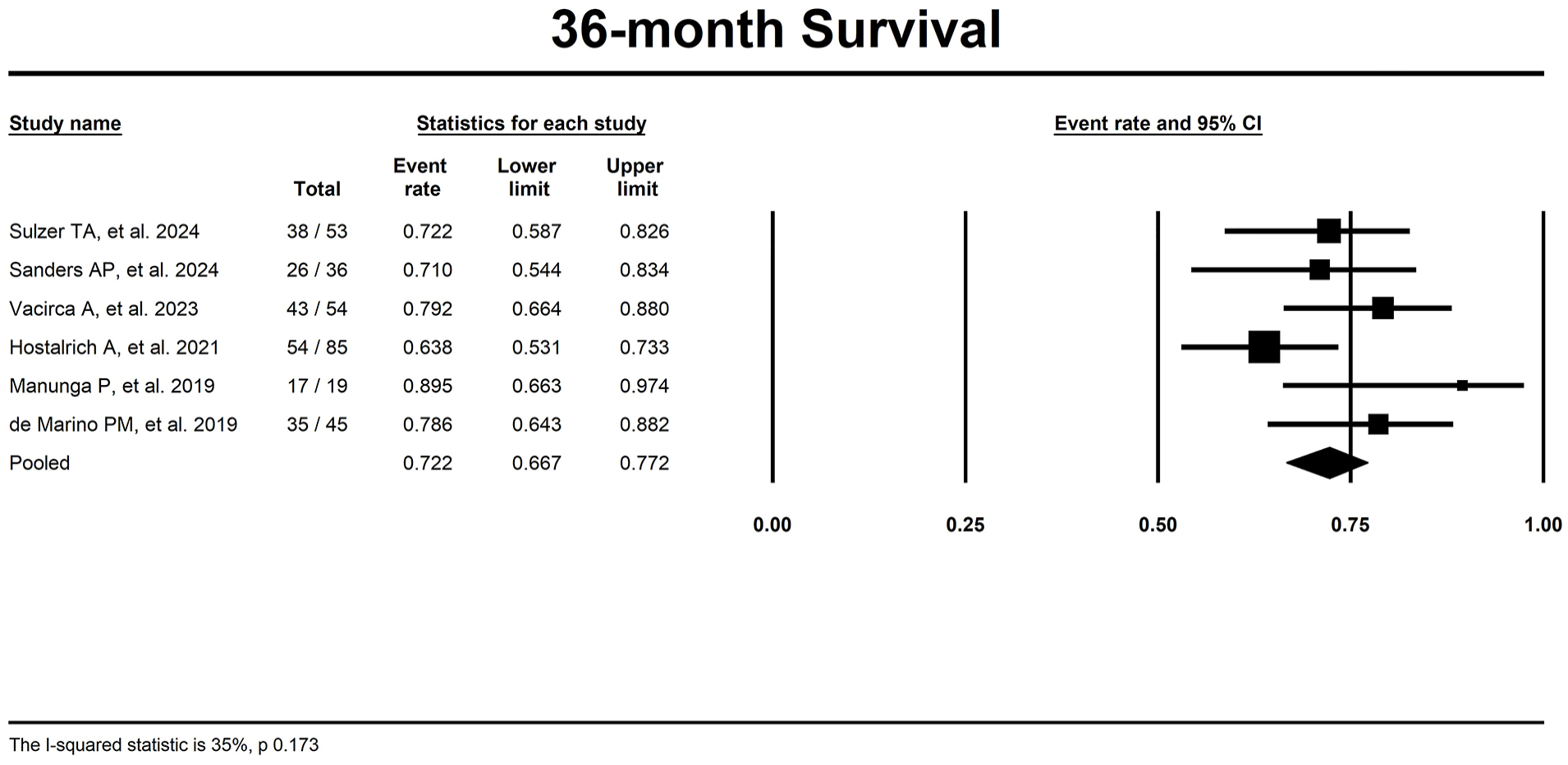
Forest plot for 36-month overall survival.
TV patency data were provided in 7 studies18,20,27,28,30–32 for 12 months with a pooled estimate of 97.4% (95% CI 96.4–98.2, I2 = 9%; Figure 13).
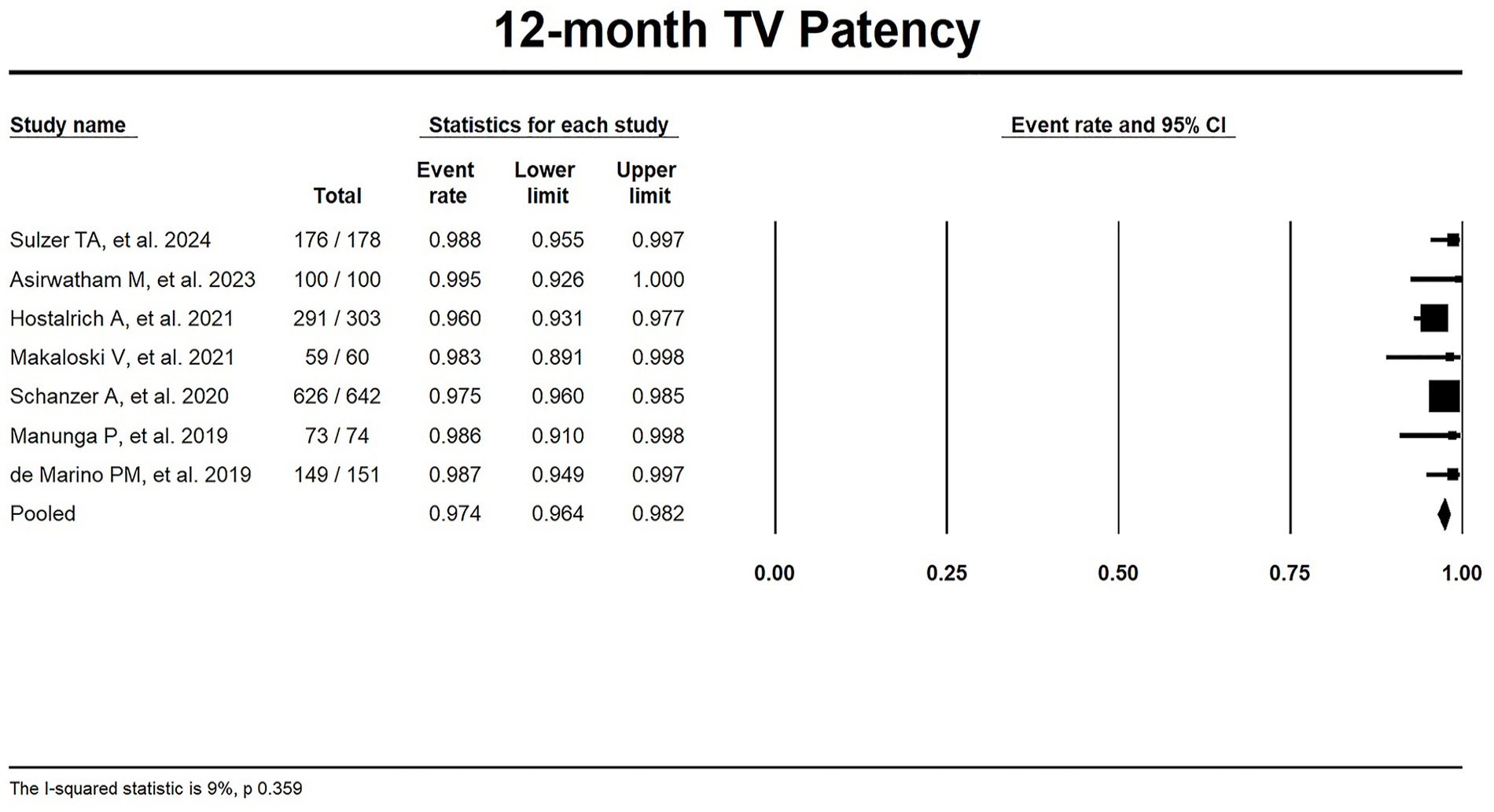
Forest plot for 12-month target vessel patency.
Freedom from reintervention was estimated at 83.7% (95% CI 79.9–86.9, I2 = 0%) for 12 months,18–20,25,27,28,30–32 75.8% (95% CI 61.0–86.2, I2 = 84%) for 24 months18,19,23,26,27 and 59.3% (95% CI 36.5–78.7, I2 = 89%) for 36 months18,19,27,32 (Figures 14–16).
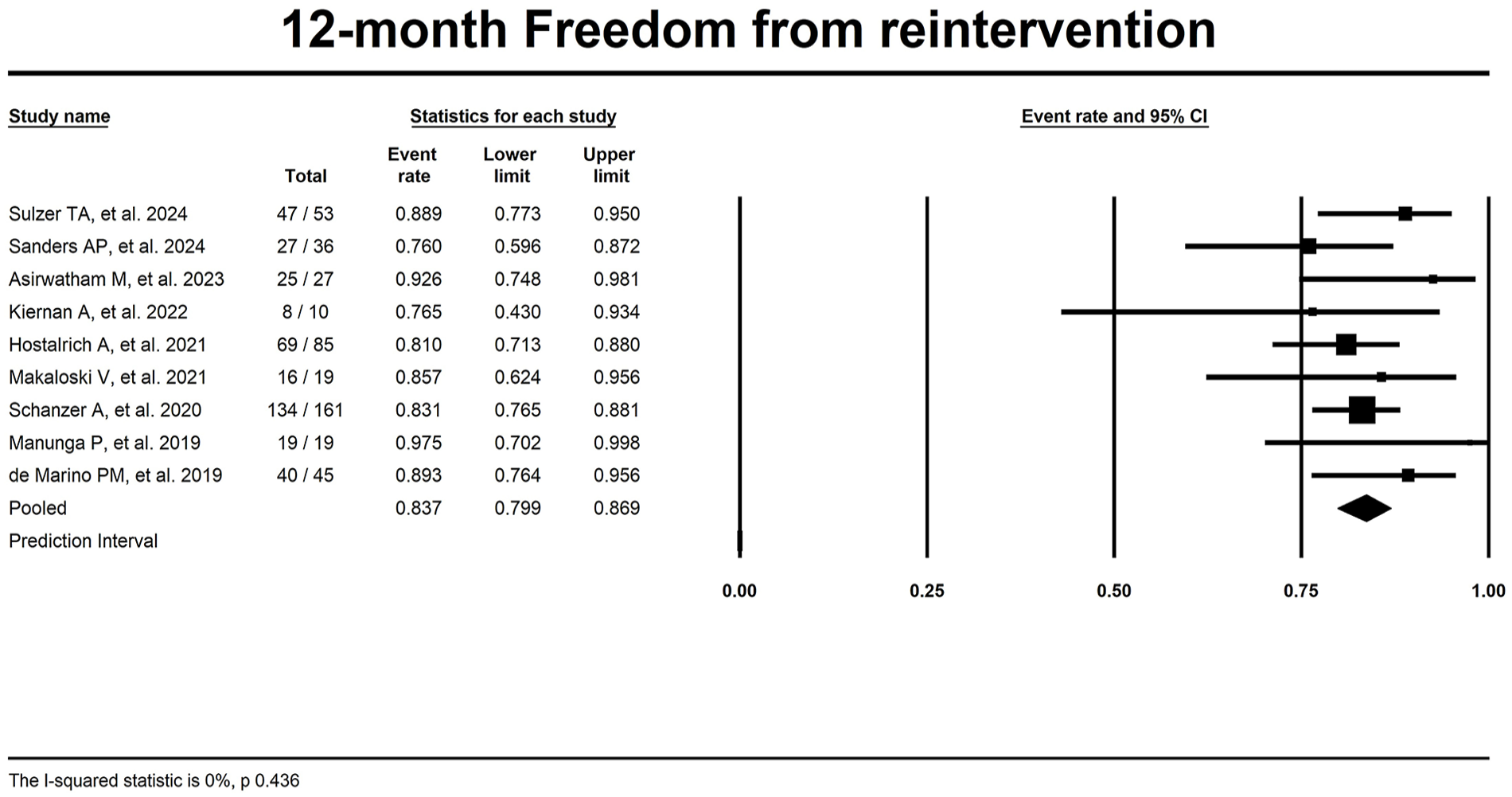
Forest plot for 12-month freedom from reintervention.
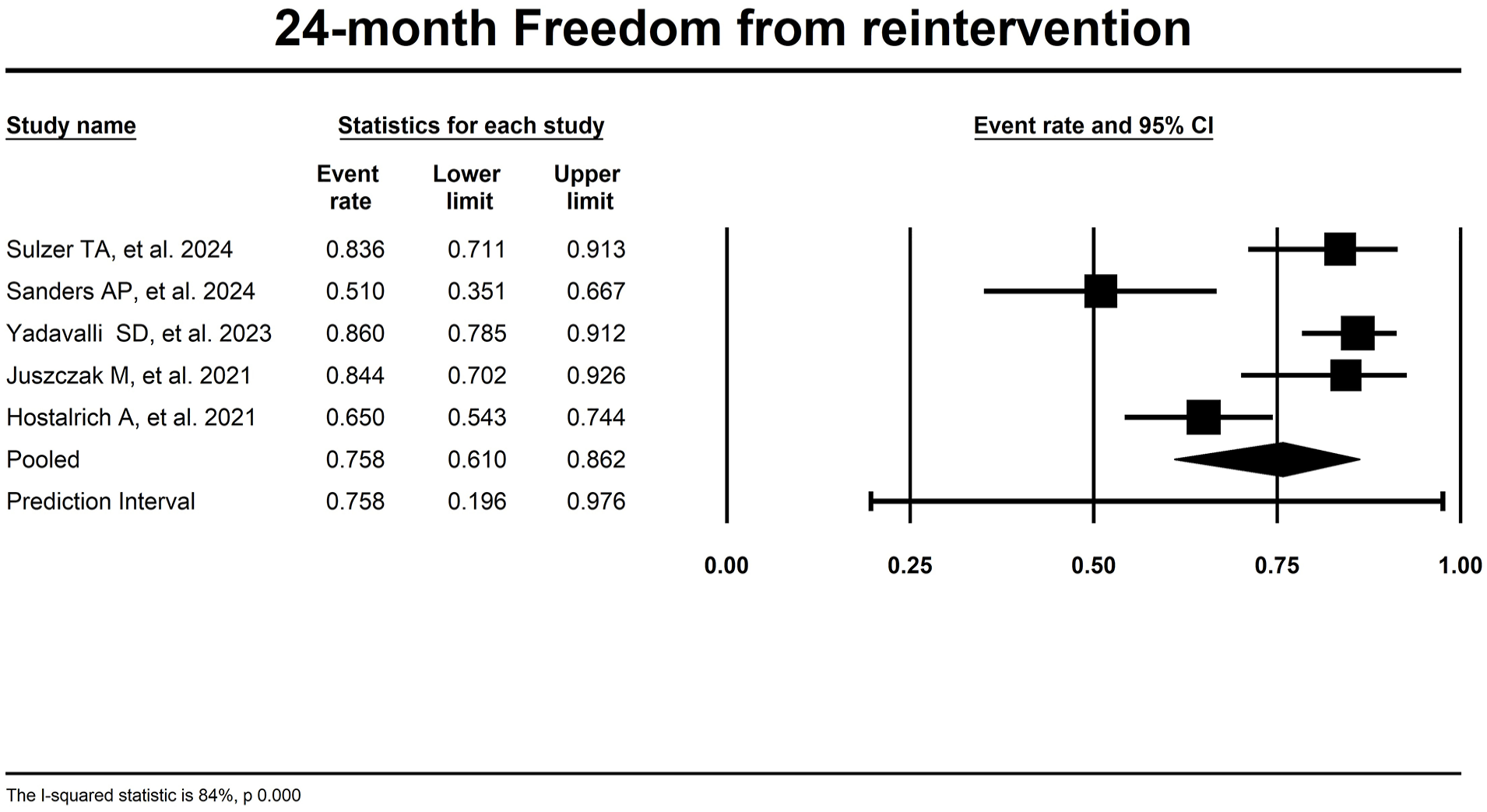
Forest plot for 24-month freedom from reintervention.
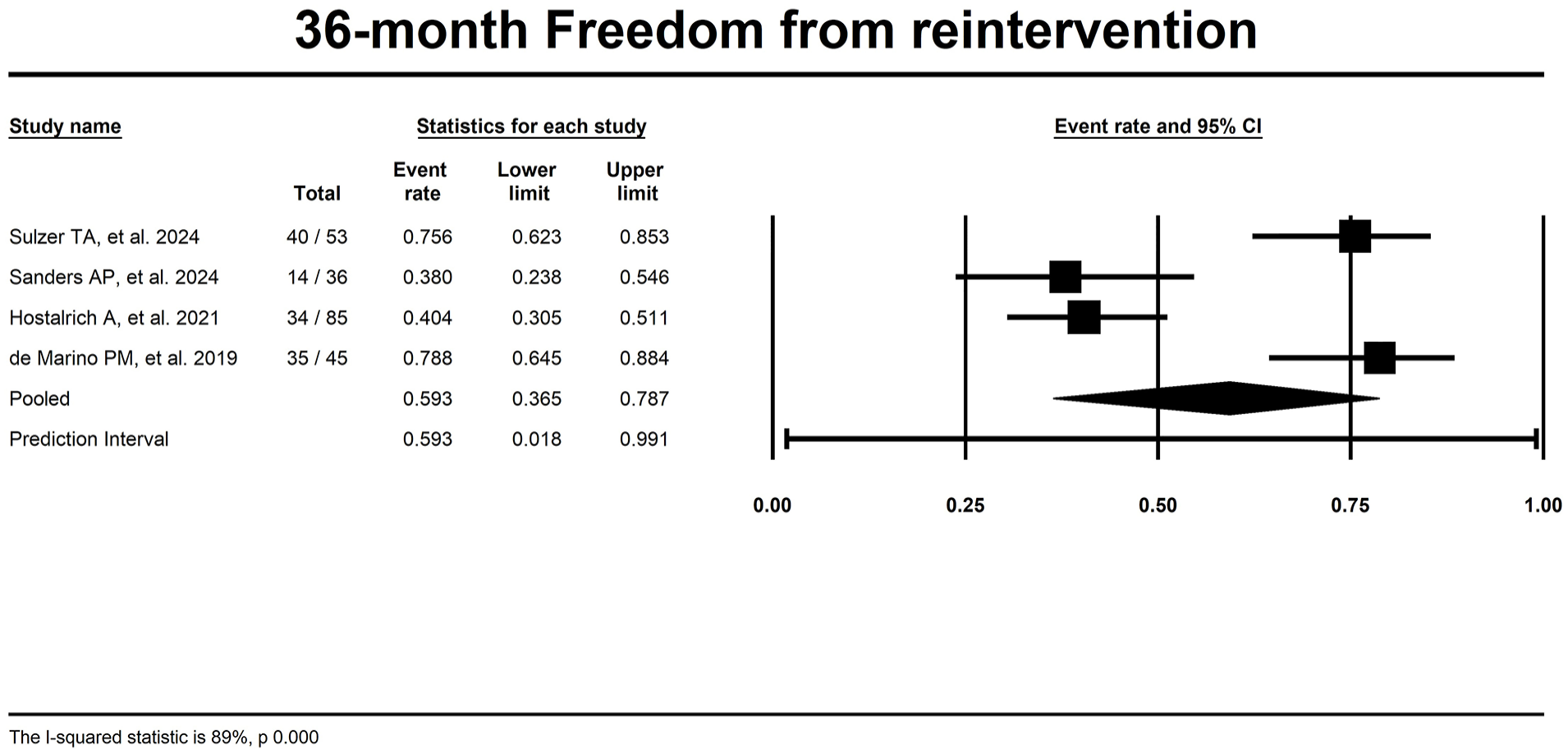
Forest plot for 36-month freedom from reintervention.
The pooled re-interventions IR per 100 p-ys was 15.2 (95% CI 9.6–23.1, I2 = 84%) (Figure 17), whereas the pooled IR per 100 p-ys for type I/III endoleak was 6.3 (95% CI 4.7–8.3, I2 = 30%; Figure 18).
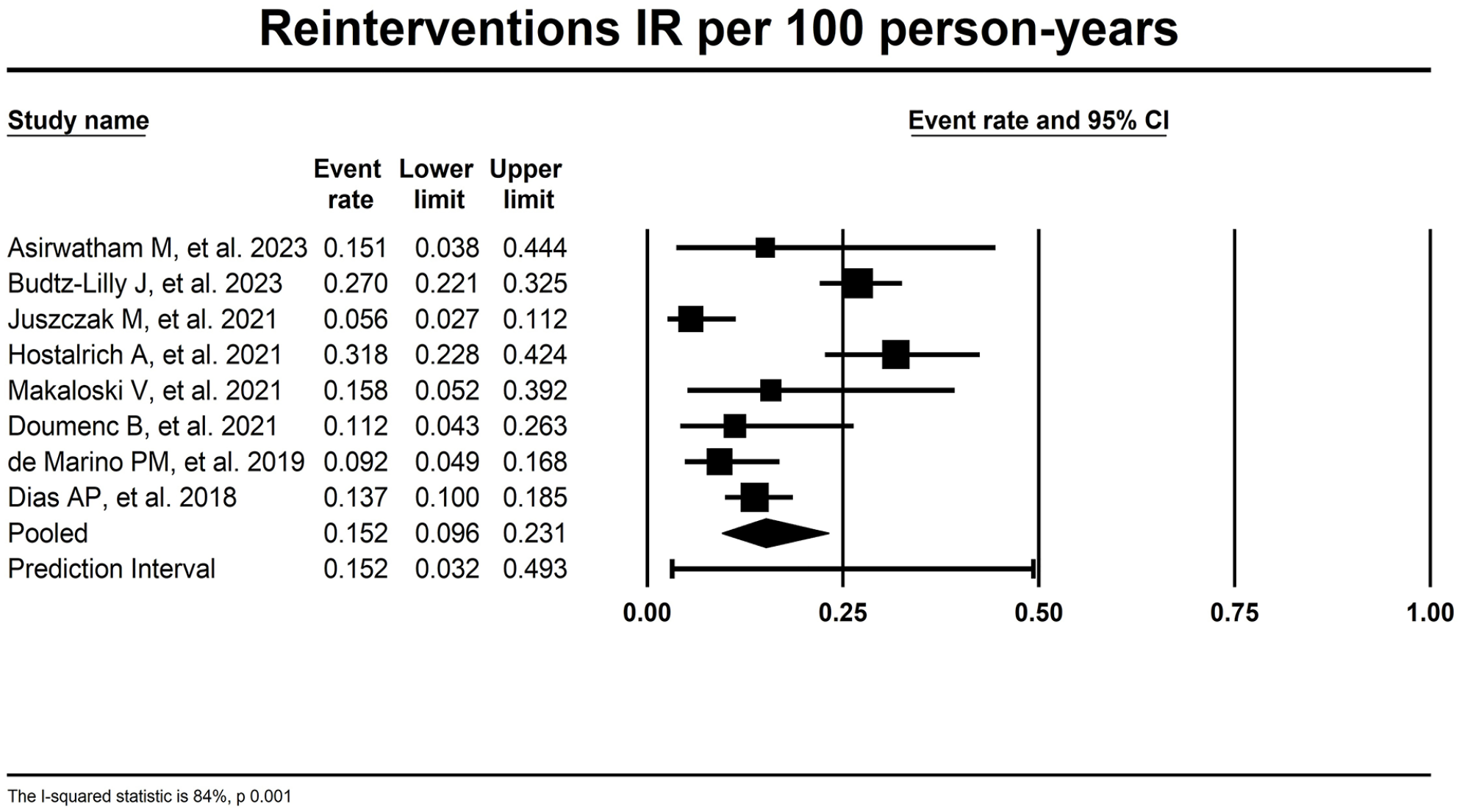
Forest plot for re-interventions IR per 100 p-ys. IR, incidence rates; p-ys, patient-years.
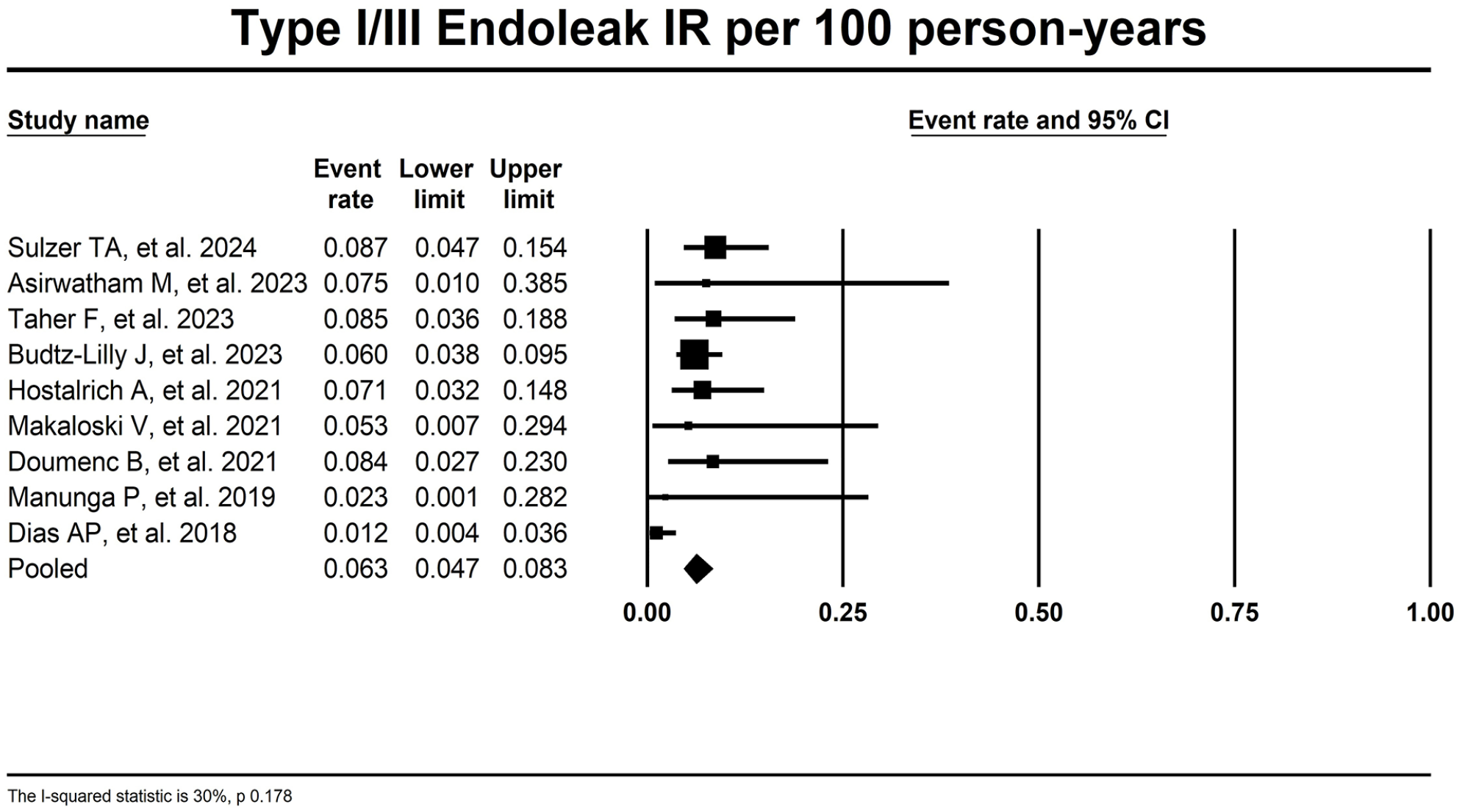
Forest plot for type I/III endoleak IR per 100 p-ys. IR, incidence rates; p-ys, patient-years.
Data regarding the aneurysm sac behavior after treatment were available for only 269 patients. Among them, in 62 patients (23.0%) a sac regression at least 5 mm was observed; in 87 patients (32.3%), the sac remained stable; and an increase of more than 5 mm was observed in 41 patients (15.2%).
Sensitivity Analysis
Sensitivity analysis was performed for technical success rate, 30-day/in-hospital mortality rate, 12-month survival, 12-month TV patency rate, and 12-month freedom from reintervention rate. Overall, a tendency toward better outcomes regarding technical success and 30-day/in-hospital mortality was found if studies with CMD, and/or off-the-shelf stent-grafts were excluded. Results of sensitivity analysis are detailed in Table 3.
Sensitivity analysis
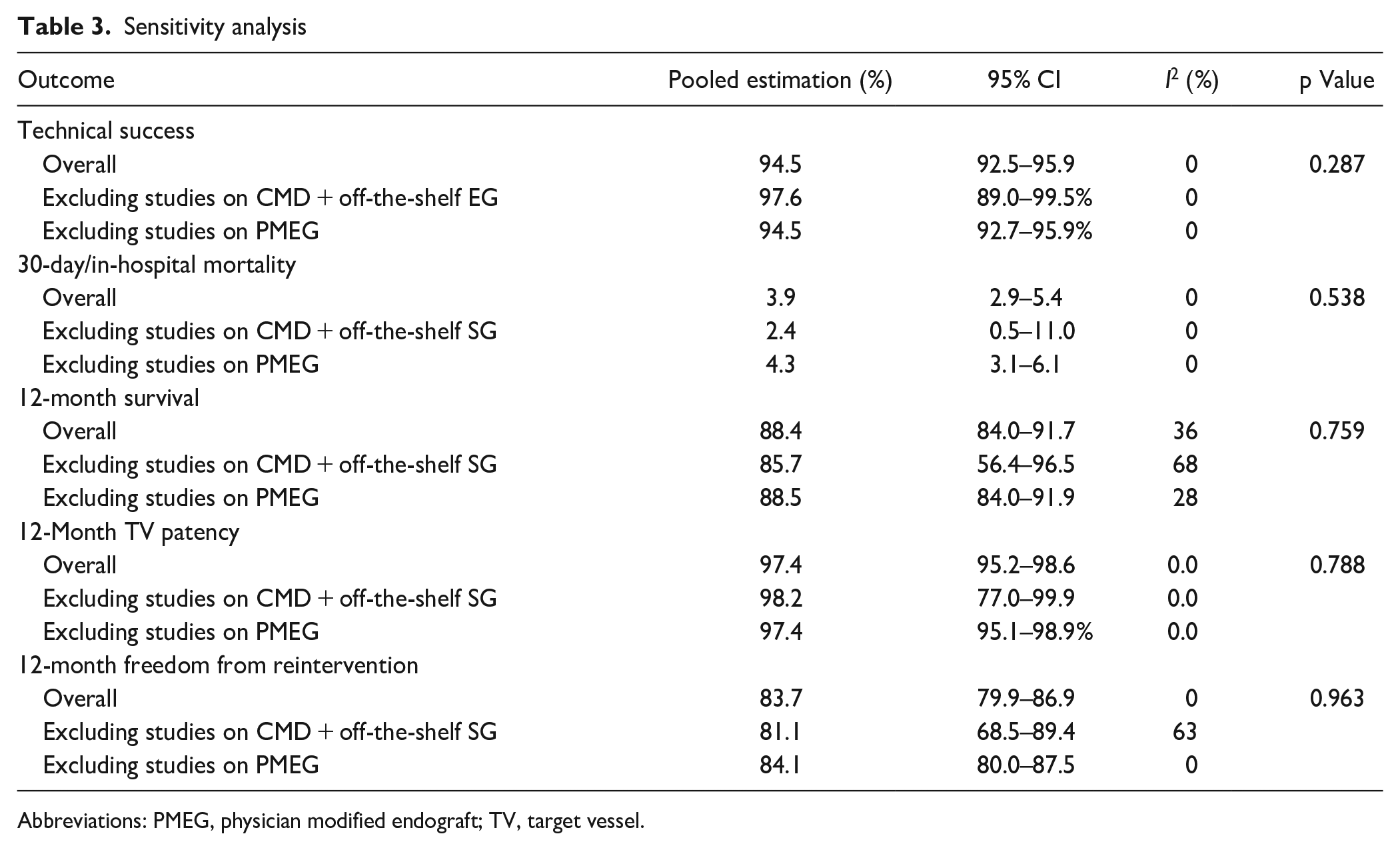
Abbreviations: PMEG, physician modified endograft; TV, target vessel.
Discussion
This meta-analysis provides the most contemporary insight into the use of F/BEVAR for rescue of proximal endograft failure after infrarenal EVAR. According to our findings, the method demonstrated favorable results regarding efficacy (technical success rate of 94.4%) and reasonable results regarding safety (30-day/in-hospital mortality rate of 3.9%, postoperative permanent paraplegia rate of 1.6%, new onset dialysis rate of 4.4%). The results representing midterm durability (overall survival and freedom from reintervention of 88%, 79.8%, 72.2% and 83.7%, 75.8%, 59.3% after 12, 24, and 36 months, respectively), however, posed several concerns.
Even though technical success was high (pooled rate of technical failure 5.6%), a few challenges need to be addressed. In particular, the most common reason recorded for not achieving technical success was failure to complete catheterization/stent deployment. This is to be expected since the presence of a prior endograft provides less intraluminal space, which in turn hinders maneuverability of wires and catheters, and friction between the endografts. Another obstacle to successful cannulation is possible TV occlusion, as well as the presence of suprarenal uncovered struts of the initial graft. Even though wires may pass through, it may be impossible to deform a strut enough for a sheath to pass. Visceral and renal artery catheterization can also be more demanding because of poorer image quality, owning to the overlapping of stent grafts and markers.27,31,34 Access difficulties also pose an inherent challenge, due to an earlier graft not allowing the new stent-graft to be advanced and accurately deployed. As a result, the only choice left perioperatively is an open conversion which inevitably puts the patient at higher risk. This was recorded in 2 patients in our study.24,27 Moreover, a stent graft component can be dislodged, thus compromising the overlap between the previous graft and the new one and/or diminishing the working length within the previous graft. 34
These technical challenges, posed by the presence of the EVAR stent-graft, could be associated with increased duration of the operation, which is a risk factor for postoperative respiratory failure. This could explain the high-pooled estimate for postoperative respiratory failure of 7%. In fact, the studies with the highest rates of postoperative respiratory failure by Dias et al 33 (14.1% and by Makaloski et al 28 (10.5%) reported also the longest procedural times (median 374 and 406 minutes, respectively). Similarly, in a recent meta-analysis on F/BEVAR for the treatment of chronic postdissections aneurysms, which also can be associated with prolonged operation times, the postoperative respiratory failure was recorded with a pooled estimate of 5.5%. 43
A recent review study by Nana et al 44 analyzed the literature concerning re-intervention with F/B-EVAR after failed previous EVAR, reported an overall 30 day mortality rate of 2.2%, which is almost the half from the 3.9%, retrieved from 16 studies in the present meta-analysis; it must be mentioned that they investigated on a smaller number of patients (total of 423 patients vs 1079 in the present study) and did not perform a weighted analysis of the results.
Moreover, this study tackled to get long-term data, which brought to light a concerning fact. The pooled rate for 3-year overall survival was 72.2%. One could assume that given the mean age of 76 years at the time of F/BEVAR, some patients have reached their life expectancy. Similarly, a recent meta-analysis comparing open conversion versus F/B-EVAR after failed EVAR, which had shown comparable results with our study regarding technical success, safety, and early mortality, recorded an overall survival of 81.6% at 18 months after F/B-EVAR for failed EVAR. 45 Interestingly, the overall survival for the patients treated with open conversion was 92.5% at 18 months. Regarding long-term survival, a recent report from the “Italian North-east Registry of surgical conversion after EVAR” describes an overall survival of patients treated due to an endoleak of 54% at 5 years. 46 This signifies that the disease progression itself can be associated with increased cardiovascular all-cause mortality, although patients treated with open conversion may be highly selected and healthier than those receiving a F/BEVAR. Moreover, the recorded freedom from reintervention of 83.7% for 12 months, 75.8% for 24 months, and 59.3% for 36 months, which is in accordance to the re-intervention rate of 26%, described by Esposito et al, 45 could also contribute to the concerning rate of survival, although there is evidence supporting the benign nature of the secondary interventions. 30 Further, given the high pooled rate for TV patency at 12 months, one could expect that the majority of the re-interventions were performed for correction of endoleak and associated pressurized aneurysm sack.
Another interesting finding shown from the sensitivity analysis is the trend toward better outcomes regarding technical success and 30-day/in-hospital mortality in studies reporting on PMEG for rescue of failed EVAR. This may be explained by the fact that in the recent years increased technical skills and accumulated experience on the advanced endovascular procedures has been gained in several centers which mainly use PMEGs for rescue of failed EVARs, especially in urgent setting. 47 On the other hand, concerns regarding durability of the PMEGs historically were raised. Our findings, however, failed to depict a difference regarding midterm durability, which is in consistency with recent reports on the use of PMEG for the treatment of de novo juxtarenal AAAs. 48
It is acknowledged that the inherent limitations of a meta-analysis study, that is, heterogeneity among studies, also applied to our study. A selection bias may have also been introduced because of the retrospective nature of the eligible studies, while the reporting differences may have led to reporting bias and compromise the validity of the results. Although technical parameters regarding the index EVAR procedure would have been valuable to evaluate the cause of EVAR failure and identify potential predisposing factors, relative data were not provided in the eligible studies. In addition, data regarding the extent and the urgency of the repair and the number of incorporated TVs per patient were not clearly and homogenously described in the eligible studies. Similarly, only a few studies provided data regarding the distal landing zone (cuff, bifurcated, bifurcated with inverted limb, etc) and did not differentiate outcomes between fenestrations, branches, which limited further analysis. Further, data regarding the aneurysm sac behavior after treatment were available for only 25% of the analyzed patients; therefore, these results should be interpreted with caution. Moreover, follow-up periods were not homogeneous in between the studies, which precluded accurate medium- and long-term data analysis at specific time points. However, in order to overcome the significant differences between follow-up periods among eligible studies, we have reported IR per 100 p-ys, instead of crude rates.
Conclusions
This study has shown that F/BEVAR is a feasible, safe, and reliable strategy for achieving proper proximal endograft sealing when previous EVAR has failed, with high technical success and low mortality rates during the short-term postoperative period. The midterm survival of these patients is also acceptable. However, meticulous planning and surveillance adherence are still essential, as reinterventions are not negligible, especially regarding TV instability.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Registration on Prospero database
CRD42024590847
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.