
Abstract
Objective:
Open repair of ruptured abdominal aortic aneurysms (rAAA) has been increasingly replaced by endovascular aortic repair (EVAR) in many centers. Despite being a minimally invasive procedure, EVAR is associated with a risk of abdominal compartment syndrome (ACS), which can lead to significant morbidity and mortality. This study examines the incidence and clinical manifestation of ACS in a consecutive cohort of rAAA patients treated exclusively with EVAR at Örebro University Hospital over a 12-year period.
Methods:
This is a retrospective analysis of prospectively collected data. We identified 139 patients who had presented to Örebro University Hospital with rAAA between October 2009 and September 2021. Patients with isolated iliac artery, thoracic and thoracoabdominal aortic ruptures, previous aortic interventions (open or endovascular), and patients receiving palliative treatment were excluded. Patients developing ACS after rAAA were compared with those who did not develop ACS.
Results:
A total of 100 patients treated using EVAR were included in this study. ACS was identified in 17 patients, and these were compared with 83 patients who did not develop ACS. Mortality at 30 days was 53% in the ACS group (9/17) and 22% in the No-ACS group (18/83, p = 0.015). Regression analysis showed that advanced age and ACS were independent risk factors for death, with ACS increasing the hazard 4-fold (HR 4.26, CI 1.99–9.10, p < 0.001) and age increasing the hazard by 6% for every year (HR 1.06, CI 1.06–1.1, p = 0.004). The use of aortic balloon occlusion was not independently associated with the development of ACS.
Conclusions:
ACS is a life-threatening complication of rAAA treated using EVAR and a significant number of patients developed ACS with high mortality and complication rates. All rAAA patients treated using EVAR should be monitored closely for ACS and treatment with decompressive laparotomy should be initiated without delay.
Clinical Impact
Open repair of ruptured abdominal aortic aneurysms (rAAA) has been increasingly replaced by endovascular aortic repair (EVAR). Despite being a minimally invasive procedure, EVAR is associated with a risk of abdominal compartment syndrome (ACS), which can lead to significant morbidity and mortality This article investigates abdominal compartment syndrome (ACS) in a cohort of total endovascular treated rAAA in a single centre and the treatment as well as the results, and gives insight on ACS in this patient group and might contribute to better understanding how to treat them and avoid this life-threatening complication.
Keywords
Introduction
Endovascular aortic repair (EVAR) is now the preferred treatment for ruptured abdominal aortic aneurysms (rAAA) due to its demonstrated feasibility in the majority of patients.1 –3 Since October 2009, open surgical repair for rAAA has been completely replaced by EVAR at Örebro University Hospital. This shift aligns with major clinical guidelines and the EndoVascular resuscitation and Trauma Management (EVTM) concept, which underscores the numerous advantages of EVAR in the management of rAAA.4–6
The current study follows the recommendations of the 2019 European Society for Vascular Surgery (guidelines, which have since been updated in 20246,7). The 2024 ESVS guidelines for rAAA introduce several key revisions. EVAR remains the first-line treatment with a Class I recommendation, but the level of evidence has been upgraded to Level A based on robust data from large cohort studies. Additionally, there is now greater emphasis on proper stent graft oversizing, while the use of aortic balloon occlusion (ABO) has been downgraded due to uncertainty regarding its effectiveness. These updates reflect a stronger focus on EVAR, refined emergency management strategies, and improved postprocedure monitoring based on the latest evidence.
Despite the declining incidence of rAAA and the widespread adoption of EVAR, mortality rates remain high.4–11 Patients with rAAA frequently present with advanced age, haemorrhagic shock, arrhythmias, loss of consciousness, and impaired renal function, all of which increase the risk of intra-abdominal hypertension (IAH) and abdominal compartment syndrome (ACS), 2 serious conditions that negatively impact survival.
ACS is a life-threatening complication following rAAA treatment. According to the World Society of the Abdominal Compartment Syndrome (WSACS), ACS is defined as a sustained intra-abdominal pressure (IAP) greater than 20 mmHg, accompanied by new organ failure, and is frequently seen in critically ill and bleeding patients, including those with rAAA.8,12–18 IAH is defined as an IAP elevation between 12 and 25 mmHg (grades I–IV), occurs in 1% to 14% of general intensive care unit (ICU) patients and carries a mortality rate of 40% to 100%.19–23 Among rAAA patients, the incidence of IAH and ACS ranges from 3% to 21%, with mortality rates between 30% and 83%.12,16,17,24–28 Known risk factors for ACS include large-volume resuscitation, the use of ABO, advanced age, acidosis, hypovolemia, hypothermia, sepsis, hemodynamic instability, loss of consciousness, and arrhythmias.17,20,22,29
The aim of this study was, therefore, to evaluate the incidence of ACS and its impact on complications, as well as 24-hour and 30-day mortality, in a consecutive cohort of rAAA patients treated exclusively with EVAR at Örebro University Hospital over a 12-year period.
Methods
This is a retrospective analysis of prospectively collected data concerning rAAA patients treated using EVAR at a single-center. The study was approved by the Regional Ethical Review Board in Uppsala-Örebro Region, Sweden (Dnr 2015/233and 2021-04782 EPM, Sweden). A detailed description of the cohort and surgical technique has been previously reported. 10 For the purpose of this study, all patients treated in this cohort were reviewed by a team of 3 vascular surgeons to ensure data quality. Medical reports of each patient were re-examined, cross-examined, and compared with the local surgical registry and the Swedish National Registry for Vascular Surgery (Swedvasc). 30 After excluding nontreated patients, as described in our former study, 100 patients were identified. The inclusion/exclusion criteria for the study cohort, the flowchart of the study, and technical aspects have been previously published, 10 but a brief summary of inclusion/exclusion criteria are as follows: patients with previous aortic surgical interventions (open or endovascular, n = 26) were excluded, as were patients considered palliative (n = 13). Of those palliative patients, 9 had previously declined treatment, which was documented in their medical records. Furthermore, 4 patients (4/13, 3.5%) were considered unfit for surgical treatment, both endovascular and open repair, due to poor prognosis, such as a combination of old age (mean 89 years), advanced comorbidities, and complicated anatomy, such as multiple aneurysms in various branches of the aorta. Five patients arriving with prolonged and ongoing cardiopulmonary resuscitation (CPR), which was terminated before reaching the operating room, were excluded from this study. All patients in whom surgical treatment was started were included (n = 100). Computed tomography angiography (CTA) was performed from aortic arch to the femoral arteries on all patients preoperatively.
ABO was placed in the descending thoracic aorta just above the visceral and renal arteries (Zone 1 or Ishimaru zones) with total or partial aortic occlusion as described in detail within the EVTM concept4,5,31,32 in hemodynamically unstable patients. EVAR was performed under local anesthesia and permissive hypotension in order to decrease the risk of postoperative complications. Postoperatively, all patients were monitored using a strict ICU protocol for the detection of complications. This included routine measurement of urinary bladder pressure with a Foley Manometer device (Holtech Medical, Charlottenlund, Denmark) to identify IAH performed upon ICU admission and subsequently at least every 4 hours throughout the ICU stay. IAP measurements were not consistently recorded in patients with normal IAP, those who died immediately after surgery, those who passed away shortly after ICU admission before IAP could be measured, and those who underwent immediate abdominal decompression in the operating room due to clinical indications. The decision for decompression was based on a markedly tense abdomen and a large retroperitoneal hematoma observed on the preoperative CTA. These patients also had hemodynamic instability and poor diuresis, further necessitating abdominal decompression. IAH was graded clinically as follows: grade I: IAP 12 to 15 mmHg, grade II: IAP 16 to 20 mmHg, grade III: 21 to 25 mmHg, grade IV >25 mmHg.15–18 Early conservative treatment with pain relief, colloids, diuretics, and neuromuscular blockade was given to patients as described in the WSACS guidelines.18,33 Patients with ACS, as defined by WSACS and ESVS guidelines,6,34 were identified and retrospectively reviewed. The ACS diagnoses was based on IAP measurement and clinical findings such as urinary output, blood pressure measurement, tense abdomen, and respiratory failure. Unfortunately, the peak airway pressure was not always documented, but it is one of the parameters monitored in critically ill patients in the ICU.
Patients with ACS underwent immediate laparotomy and were managed with an open abdomen using either a Bogota bag or vacuum-assisted wound closure. A second-look procedure was performed 24 hours after laparotomy. Fascia and wound closure were carried out once the patient was hemodynamically stable and abdominal tension was resolved.
Statistical Analysis
Chi-square test or Fisher’s exact test were used to compare the categorical data of the ACS and No-ACS groups, while Mann–Whitney U test was used to compare continuous and ordinal data between the 2 groups. Univariate analysis was used to compare patients who died and those who survived. Significant factors having a loose p-value of <0.1 were then entered into a backward stepwise logistic regression model to define factors affecting 30-day mortality. Survival analysis was performed as described in a former publication. 35 For the overall survival analysis, the endpoint was defined as the time between the EVAR and the date of death. Those who were alive at the end of the follow-up (up to 10 years) were defined as alive, while those who were lost to follow-up or could not be contacted were censored. Kaplan–Meier analysis was used to analyze the survival of the ACS group and the No-ACS group. The 2 survival curves were compared using the log-rank test. The Cox Proportional Hazards regression model was used to assess the association of the independent hazard risk factors with death. Statistical analysis was performed using SPSS (Version 26; IBM Corp., Armonk, NY, USA). A p-value of <0.05 was accepted as statistically significant.
Results
None of the patients in this cohort died in the hybrid operating room. IAP measurements were documented during the postoperative period in 66% of patients (66/100). Patients with ACS (n = 17) were compared with patients without ACS. Patient characteristics, postoperative data, and mortality are shown in Tables 1 and 2. There were no significant differences between the groups regarding age, sex, and previous medical conditions such as diabetes mellitus, cardiac disease, and renal disease. Although patients with ACS had a higher rate of ABO usage, there was no significant difference between the 2 groups. The rate of postoperative 30-day complications was 53% (9/17) in the ACS group compared to 22% (18/83) in the No-ACS group (p = 0.015). No myocardial infarction or cerebrovascular complications occurred in the ACS group but 4% (5/83) of the No-ACS group suffered cardiac infarction and 3% (4/83) cerebrovascular lesions, which were not statistically significant. Laparotomy was performed in 94% (16/17) of the patients with ACS, while only 1 patient in the No-ACS group, who developed multiorgan failure, died before abdominal decompression could be performed. There was a significant difference in ICU stays longer than 5 days between the groups. Mortality data and the Kaplan–Meier survival curves are reported in Table 3 and Figure 1. Mortality within 24 hours was 24% (4/17) in the ACS group and 18% (15/83) in the No-ACS group (p = 0.734). However, mortality at 30 days, 90 days, 1 year, and 3 years was statistically significant between the 2 groups (Table 2). The univariate analysis of the statistically significant factors between the patients who died and those who survived at 30 days is reported in Table 3. These significant factors were hypotension (p = 0.001), CPR (p = 0.019), the use of ABO (p < 0.001), ACS (p = 0.015), and if a laparotomy was performed (p < 0.001). Table 4 shows the logistic regression model predicting 30-day mortality. The model was highly significant (p < 0.001), having a Nagelkerke R Square of 0.44. Laparotomy was the only significant factor predicting the 30-day mortality with an odds ratio of 19.56. The Cox regression analysis for independent risk factor of death is reported in Table 5. There were 2 statistically significant hazard risk factors: age (p = 0.004) and ACS (p < 0.001). Having ACS multiplies the hazard of death by 4.26 when compared with those who did not have ACS. Advanced age increases the hazard of death by 6% for every year. The Kaplan–Meier curves of overall survival for those who had ACS and those who did not are reported in Figure 1. The survival of these 2 groups was significantly different. The median survival time using the reverse Kaplan–Meier curves was 1 month in the ACS group and 71 months in the No-ACS group (Log-rank test p < 0.0001).
Characteristics of Patients With and Without ACS After Endovascular Treatment for rAAA Between October 2012 and September 2021 and Postoperative Data.
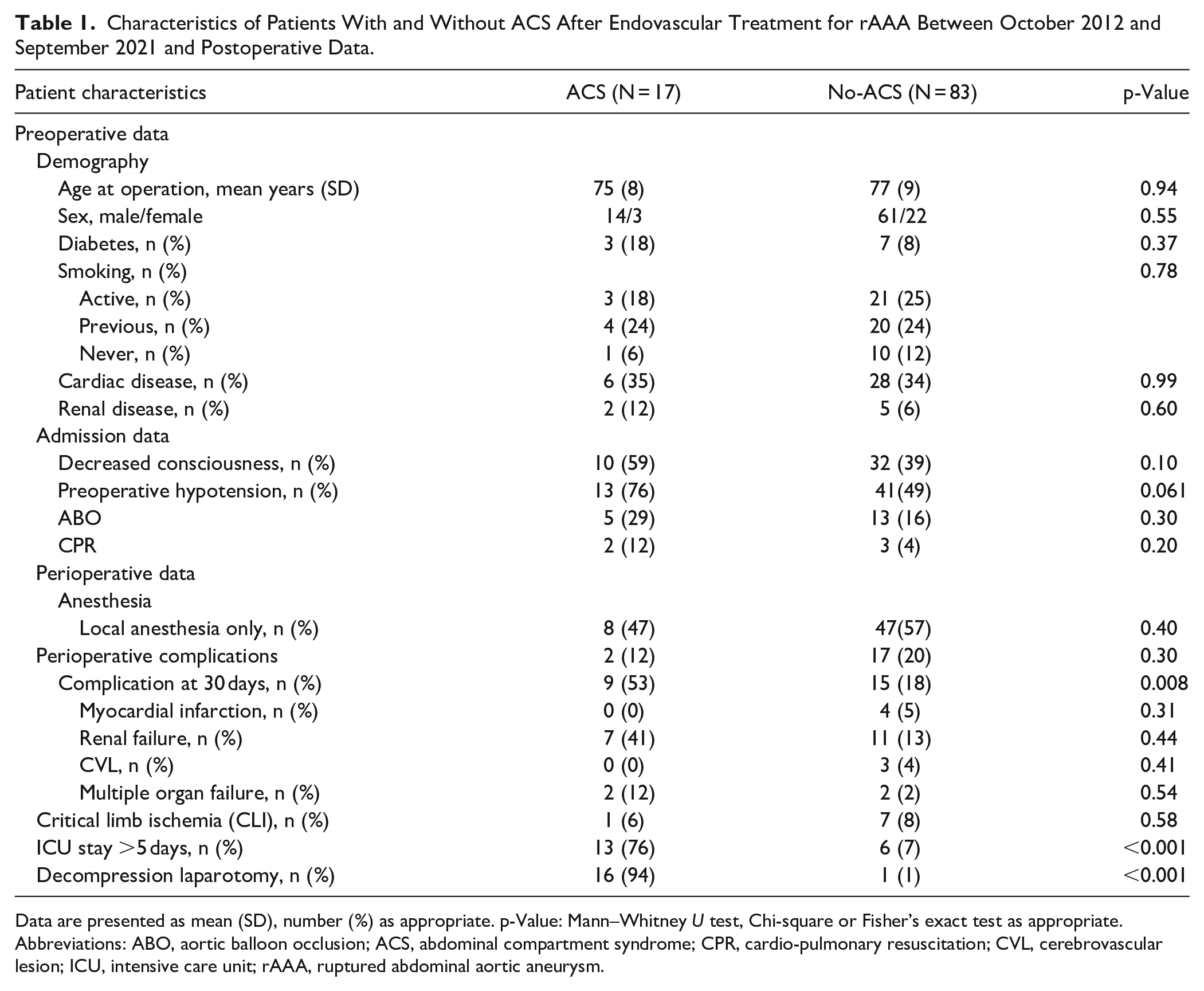
Data are presented as mean (SD), number (%) as appropriate. p-Value: Mann–Whitney U test, Chi-square or Fisher’s exact test as appropriate.
Abbreviations: ABO, aortic balloon occlusion; ACS, abdominal compartment syndrome; CPR, cardio-pulmonary resuscitation; CVL, cerebrovascular lesion; ICU, intensive care unit; rAAA, ruptured abdominal aortic aneurysm.
Mortality Data for All Patients Treated With EVAR for rAAA Between October 2012 and September 2021.
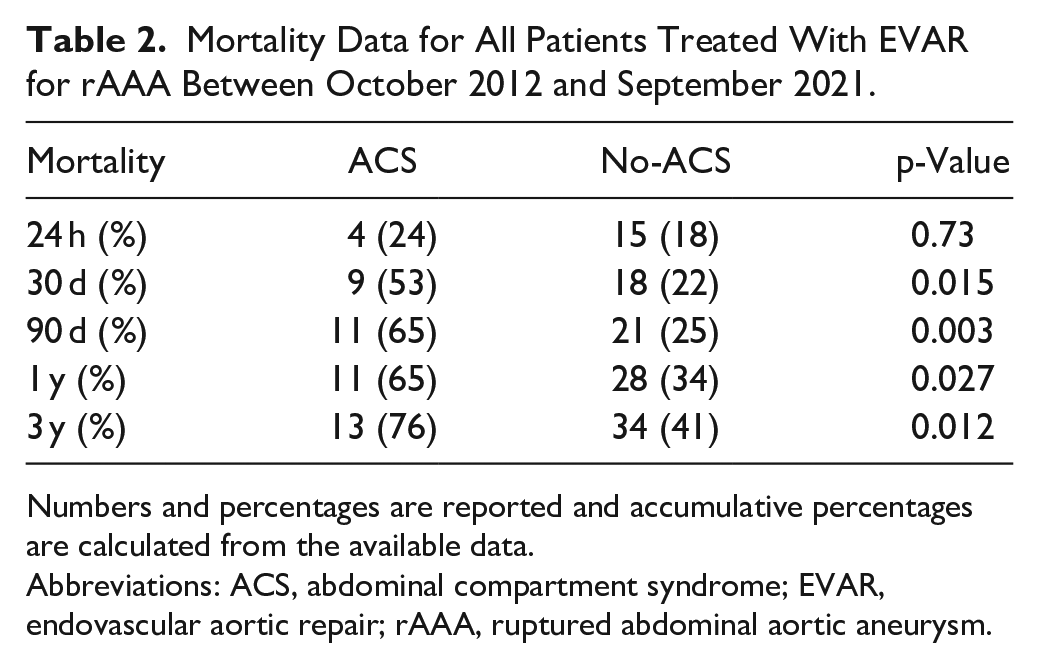
Numbers and percentages are reported and accumulative percentages are calculated from the available data.
Abbreviations: ACS, abdominal compartment syndrome; EVAR, endovascular aortic repair; rAAA, ruptured abdominal aortic aneurysm.
The Univariate Analysis Showing the Statistically Significant Perioperative and Postoperative Factors Between the Patients Who Died and Those Who Survived.
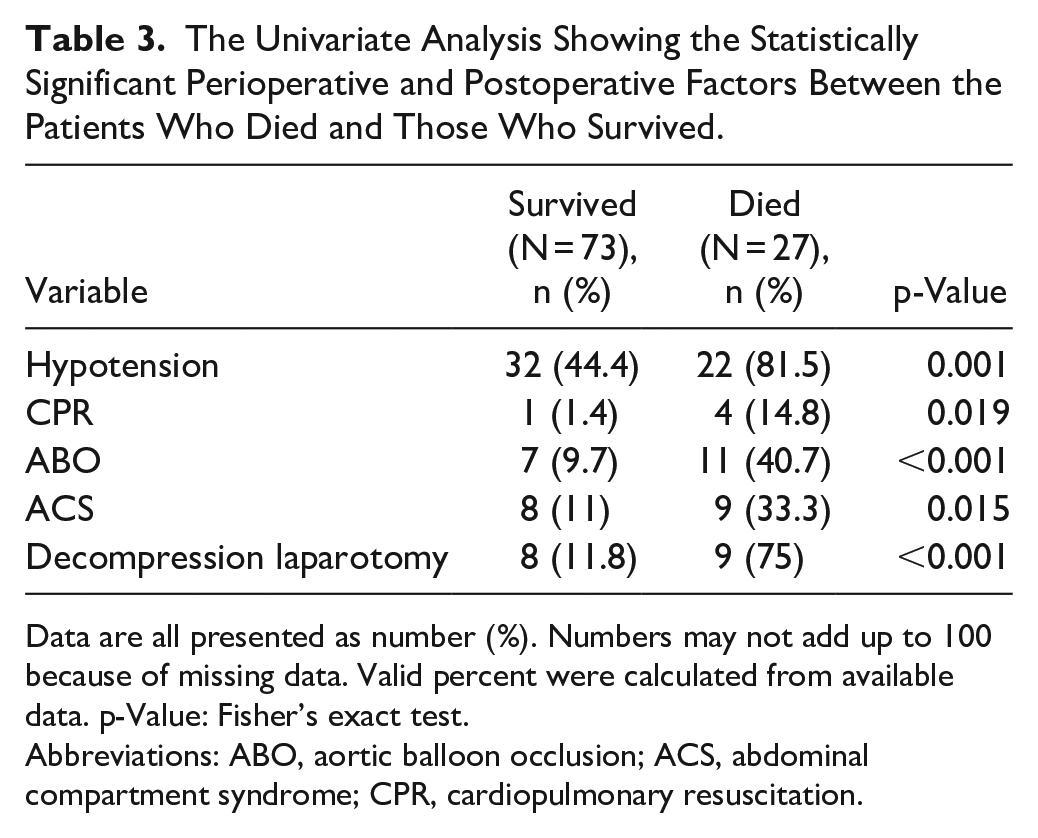
Data are all presented as number (%). Numbers may not add up to 100 because of missing data. Valid percent were calculated from available data. p-Value: Fisher’s exact test.
Abbreviations: ABO, aortic balloon occlusion; ACS, abdominal compartment syndrome; CPR, cardiopulmonary resuscitation.
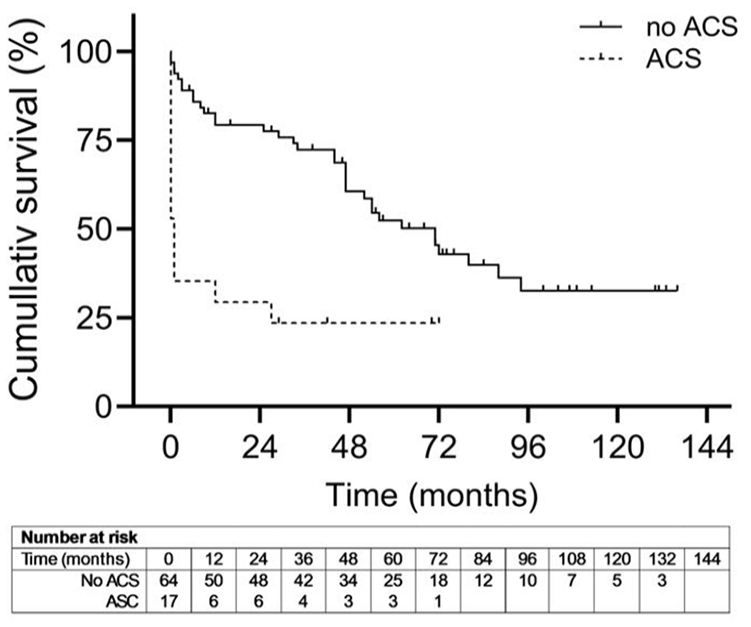
Kapalan-Meier curves of overall survival for those who had abdominal compartment syndrome(ACS)(dotted line) and those who did not (No-ACS)(continuos line).
The Backward Stepwise Logistic Regression Model Showing the Factors Predicting the 30-Day Mortality of the Studied Cohort.
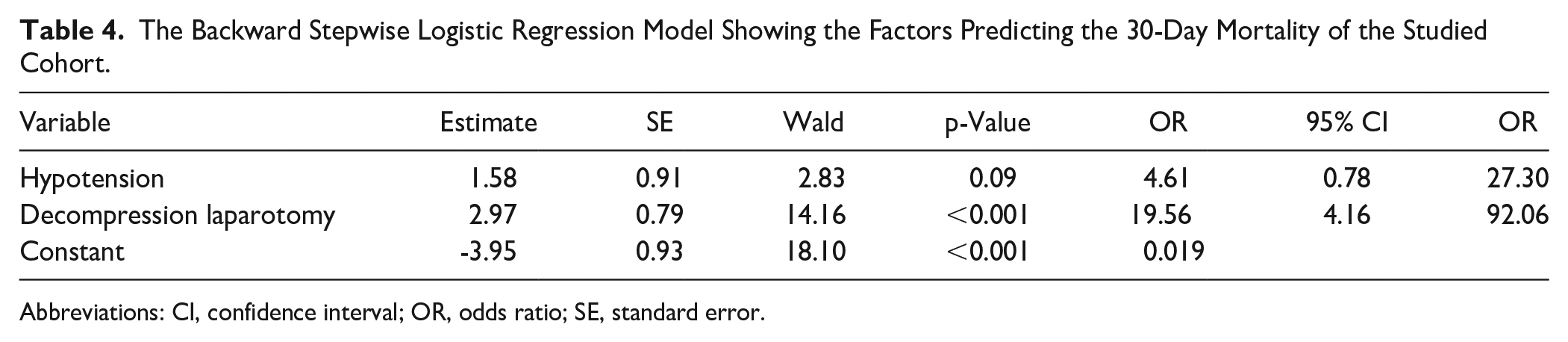
Abbreviations: CI, confidence interval; OR, odds ratio; SE, standard error.
Cox Regression Analysis for Independent Risk Factor of Death.
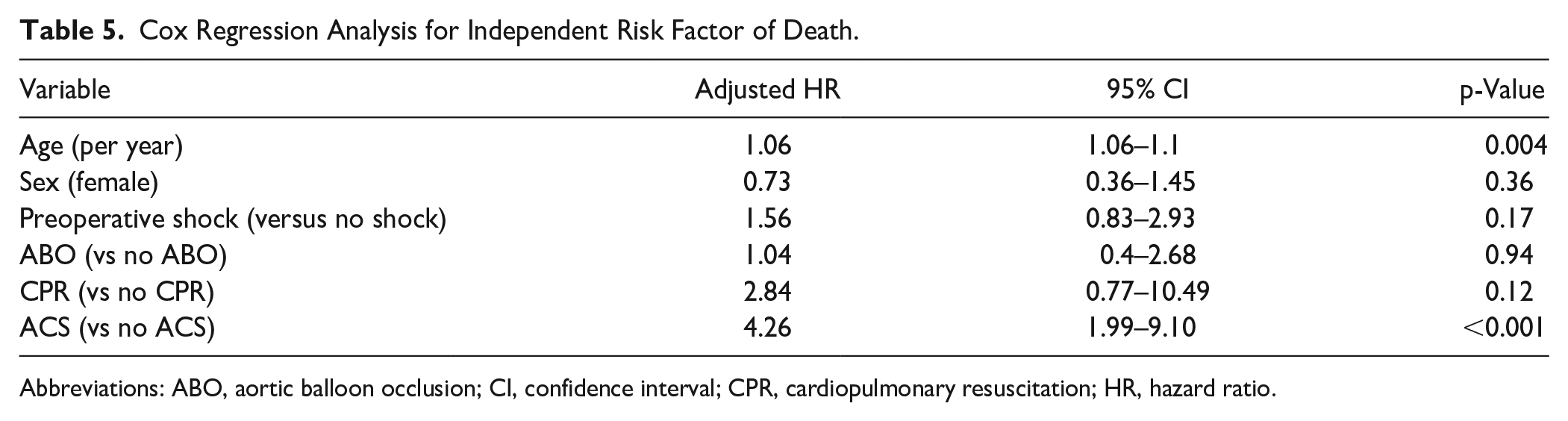
Abbreviations: ABO, aortic balloon occlusion; CI, confidence interval; CPR, cardiopulmonary resuscitation; HR, hazard ratio.
Discussion
The use of endovascular techniques, such as EVAR for rAAA, is increasing globally as these methods continue to evolve, becoming the treatment of choice in many centers. However, treatment should be individualized based on both patient and institutional factors, ensuring that endovascular, open, and hybrid options are available for all patients. Open surgery remains a crucial treatment modality, even at the current center. It is also important to distinguish between elective and ruptured AAA cases, as multiple studies and ESVS guidelines1–3,6,7 support EVAR as the superior approach for rAAA.
With the introduction of endovascular treatment for rAAA, IAH, with or without ACS, has emerged as an increasingly recognized complication. Concerns have been raised that the incidence of ACS may be higher after endovascular treatment compared to open repair of rAAA, largely due to the nature of the procedure and the presence of residual retroperitoneal hematoma. Reported incidence rates of ACS following EVAR range from 7% to 30%16,36; however, reliable data specifically on ACS after EVAR for rAAA are limited. Most studies compare open and endovascular approaches without focusing on ACS development after endovascular repair. Several studies have attempted to determine the incidence of ACS in small patient cohorts or with limited follow-up.16,28,36
To the best of our knowledge, this is the first study examining ACS in a consecutive cohort of patients treated exclusively with endovascular repair for rAAA. We demonstrated an ACS incidence of 21%, which aligns with previously reported rates. The development of ACS after rAAA has a profoundly negative impact on survival, with mortality rates ranging from 67% to over 80% among patients who require decompression laparotomy, according to several studies.13,36,37 While some reports suggest no clear association between ACS and mortality, a meta-analysis by Karkos et al did not show a statistically significant relationship, although mortality rates were notably higher in patients with ACS. 37 Miranda et al reported no significant association between the development of ACS and mortality; however, these findings may be due to the study’s small sample size. Of 25 patients who underwent EVAR for rAAA, only 3 patients were diagnosed with ACS, and the diagnosis was based on criteria that did not strictly align with the WSACS definition. 38
In our study, 30-day mortality was 53% in the ACS group compared to 22% in the No-ACS group, confirming that ACS is a major contributor to mortality in these patients. This finding is consistent with other reports, which also show a clear association between ACS and both 30- and 90-day mortality.36–40 Early detection and intervention for ACS are critical for improving outcomes. However, laparotomy as a treatment for ACS can lead to complications, including re-bleeding, infections, intra-abdominal abscess formation, ileus, and respiratory failure. 39 In this study, laparotomy was the only independent predictor of short-term mortality (within 30 days) in the logistic regression model, with the procedure increasing odds of death 20-fold. Despite its high mortality, laparotomy remains the treatment of choice in patients with ACS, and prompt intervention is essential, even though the procedure itself is associated with significant risks. Advanced age was a factor negatively impacting the risk of mortality. Previous studies have identified age as an independent predictor of mortality in patients undergoing both endovascular and open surgery for rAAA.13,40 Our study demonstrated that ACS increased the hazard of death 4-fold compared with patients without ACS, and that the hazard of death increased by 6% for each additional year of age, in line with findings from other studies. Other independent risk factors, such as preoperative shock, female gender, and CPR, have been identified in previous studies but were not the focus of detailed analysis in this study.13,16,41,42
When assessing whether a patient has developed ACS, it is crucial to monitor high IAP and the onset of new organ dysfunction. Several risk factors that have been associated with ACS development in patients undergoing EVAR, such as aortic balloon placement, have been highlighted in previous studies, but not show a significant association with ACS development in our cohort. 36 This may be due to the small sample size of our ACS patients. Only 2 previous studies have explored the impact of ACS on mortality after endovascular repair,8,36 and both reported significantly higher mortality rates in patients with ACS than in patients without ACS.8,36 Our findings support these conclusions, despite the study’s limitations, including IAP measurements in only 66% of patients, a relatively small sample size, and its retrospective design. Reduced survival after laparotomy following ACS implies substantial postoperative complications, leading to prolonged hospital stay and or morbidity. Although laparotomy was an independent predictor of short-term mortality in our analysis, it remains crucial to promptly recognize and treat ACS with laparotomy when indicated. Using modern techniques and management protocols to optimize patient outcomes.
Limitations of the Study
There are some obvious limitations to this study due to the retrospective design and lack of a control group. Due to incomplete data registration, we did not analyze time aspects for rAAA symptoms and treatment (or surgical time) or fluid balance that might influence ACS; we will perform this analysis in a separate ongoing study. This study is a single-center study, and the number of patients with ACS is limited. Finally, some of the patients who were treated during 2021 have not yet reached the 3-year follow-up; however, censoring would have addressed this issue. Furthermore, studies in a larger population are needed to characterize the relationship of risk factors with ACS development.
Conclusions
In a cohort of patients receiving total endovascular treatment for rAAA, a significant number of patients developed ACS with high mortality and complication rates. ACS and laparotomy are associated with high mortality in patients treated for rAAA using EVAR.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethic Statement
The study was approved by the Regional Ethical Review Board in Uppsala-Örebro Region, Sweden (Dnr 2015/233 and 2021-04782 EPM, Sweden).