
Abstract
Purpose:
Aortic stiffness and intraluminal thrombus at baseline have been suggested as potential determinants of the impact of aortic endovascular devices on aortic wall properties. We aim to assess the impact of the endograft and of thrombus load on aortic compliance through the assessment of changes in aortic radial deformation following thoracic endovascular aortic repair (TEVAR).
Materials and Methods:
The 3D geometric models of the aorta at peak systole and end diastole were constructed from both pre- and post-TEVAR 4D flow magnetic resonance imaging (MRI) of aortic aneurysm and dissection patients. Arclength, length-averaged curvature, and true- and whole lumen effective diameters and areas were assessed in different aortic segments (ascending aorta, endografted segment, and all aorta). Aortic radial deformation was defined as percentage change in aortic diameter from diastole to systole. Thrombus load was defined as thrombus volume divided by aortic volume. Spearman’s coefficient (R) was calculated to assess linear correlations.
Results:
The analysis was conducted on 14 patients/TEVAR procedures (n=7 aneurysms, n=7 dissections). Median time between pre- and postoperative MRI was 124.6 ± 81.7 days. Aortic radial deformation significantly decreased in the endografted segment (7.2% ± 3.6% vs 5.0% ± 2.0%, p<0.05), whereas it significantly increased in the ascending aorta (6.2% ± 2.3% vs 14.4% ± 4.0%, p<0.05). No significant impact was observed on axial deformation (length change) and bending pre-to-post-TEVAR in those 2 segments. Regarding changes in geometry, cardiac cycle-averaged ascending aortic diameter was found similar pre-to-post TEVAR (3.7 ± 0.3 cm vs 3.6 ± 0.4, p=0.23). Thrombus load at the level of the diseased thoracic aorta at baseline correlated strongly with the amplification in ascending aorta radial deformation (R=−0.80, R2=0.64), and in an even more significant manner when excluding the 2 patients with a history of prosthetic ascending aorta replacement (R=−0.88, R2=0.77).
Conclusion:
Following TEVAR, aortic radial deformation, is reduced in the stented segment and amplified in the ascending aorta. Greater baseline thrombus load results in lower radial deformation amplification post-TEVAR. These findings highlight the benefit of thrombus load assessment pre-TEVAR and the need for increasing the compliance of future grafts to minimize its impact.
Clinical Impact
Following thoracic endovascular aortic repair (TEVAR), aortic radial deformation, directly related to aortic compliance, is reduced in the stented segment, and amplified upstream in the ascending aorta, likely due to increased stiffness of the endograft, remodeling, and pressure pulse reflection. Thrombus load is found as an effective predictor of aortic radial deformation amplification following TEVAR. This highlights the benefit of thrombus assessment pre-TEVAR and the need for increasing compliance of future graft designs to minimize its impact.
Introduction
Thoracic endovascular aortic repair (TEVAR), developed in the mid-1990s, has rapidly become the gold standard treatment for various descending aortic pathologies including aneurysms, dissections, penetrating ulcers, and blunt traumas. Key advantages of this procedure include its minimal invasiveness and the proven reduction in postoperative morbidity and mortality relative to conventional open surgical repair. 1 Thus, TEVAR indications have been consistently expanding to younger patients and longer coverages with more proximal landing zones allowing total endovascular arch repair.2,3
Despite its increasing prevalence, the effect of TEVAR on aortic biomechanical properties remains to be elucidated for many circumstances. Increased aortic stiffness and compliance mismatch between the stented and the native aortic segments have been implicated as potentially responsible for upstream aortic complications such as aneurysm growth, endoleaks, and stent-induced new entry tear following TEVAR.3 –6 These phenomena have also been cited as potential precursor factors of more debated TEVAR effects such as myocardial function impairment.7–9
A few published papers, limited to small cohorts, have suggested altered aortic motion and wall compliance after TEVAR,10–12 which may constitute early and quantifiable factors that influence remodeling and long-term outcomes. Other aortic characteristics such as aortic stiffness and intraluminal thrombus at baseline have only been partially considered in previous studies and have also been suggested as key determinants of the impact of aortic endovascular devices on aortic wall properties including altered compliance.3,5,13 The aim of this magnetic resonance imaging (MRI)-based study was to assess the biomechanical effects of TEVAR on aortic radial deformation, directly related to aortic compliance, and the potential impact of thrombus load at the level of the diseased thoracic aorta at baseline on these processes.
Materials and Methods
Patient Recruitment
This study was performed on a subset group of patients from the FASCAT (Flow and Structural Changes after TEVAR) cohort. FASCAT is a French prospective monocentric study intended to assess the anatomical, hemodynamic, and biomechanical changes in the aorta and the heart before and after TEVAR. From April 2022 to March 2024, all patients referred for TEVAR as part of the treatment of a subacute or chronic thoracic aortic dissection or aneurysm were eligible. Main exclusion criteria were patients with a contraindication to MRI, patients living more than 200 km away from the investigating center, patients with complex or multiple cardiac surgeries (more than 2 sternotomies) and patients requiring TEVAR placement in a timeframe incompatible with the completion of the MRI. Patient under guardianship, curatorship, court protection or deprived of liberty, and patients objecting to the use of their data for this research were also excluded.
As part of the FASCAT protocol, all included patients were planned to receive a 4D-flow MRI, among other examinations, before and 3 months after the TEVAR procedure. All FASCAT patients who successfully completed the required sequences of pre- and postoperative 4D Flow MRI could be considered as eligible for this aortic deformation study. The FASCAT study received ethical approval from the local ethical committee and consent was obtained for all patients. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
MRI Acquisitions
Patients underwent electrocardiogram (ECG) gated cardiac MRI including aortic MR angiography and 4-dimensional (4D) flow MRI acquisition, performed on a 1.5 T magnet (Optima MR 450 W; General Electric Healthcare, Waukesha, WI, USA) using a 32-channel coil. Contrast-enhanced 4D flow sequences were acquired, encompassing a 3-dimensional (3D) coronal volume that provided complete thoracic coverage. Acquisition parameters were as follows: TR (repetition time) = 4.05–4.12 mseconds, TE (time to echo) = 2.17–2.20 mseconds, flip angle = 12°, velocity encoding (Venc) was set at 200 cm/second, and 30 frames were acquired per cardiac cycle with a spatial in plane resolution of (1.56–1.95) mm × (1.56–1.95) mm and slice thickness of 1.20 to 1.40 mm.
Geometric Modeling
3D geometric models of the aorta at maximum (peak systole) and minimum (end diastole) deformation were constructed from both preoperative and postoperative MRI using the SimVascular software (Open-Source Medical Software Corporation, San Diego, CA, USA). 14 The first step of this approach was to manually create paths along the approximated centerline of the main vessel, here the thoracic aorta, and its branches, the supra-aortic vessels (Figure 1A). To ensure consistency among models, the sino-tubular junction (STJ) and the coeliac trunk were chosen as the inlet and outlet anatomical landmarks, respectively, for all geometric models. As described in previous studies,15,16 the brachiocephalic trunk (BCT) was modeled with the purpose of not only marking the end of the ascending aorta but also being used as a fiducial marker in a Lagrangian coordinate system to be able to transfer the postoperative endografted segment to the preoperative model.
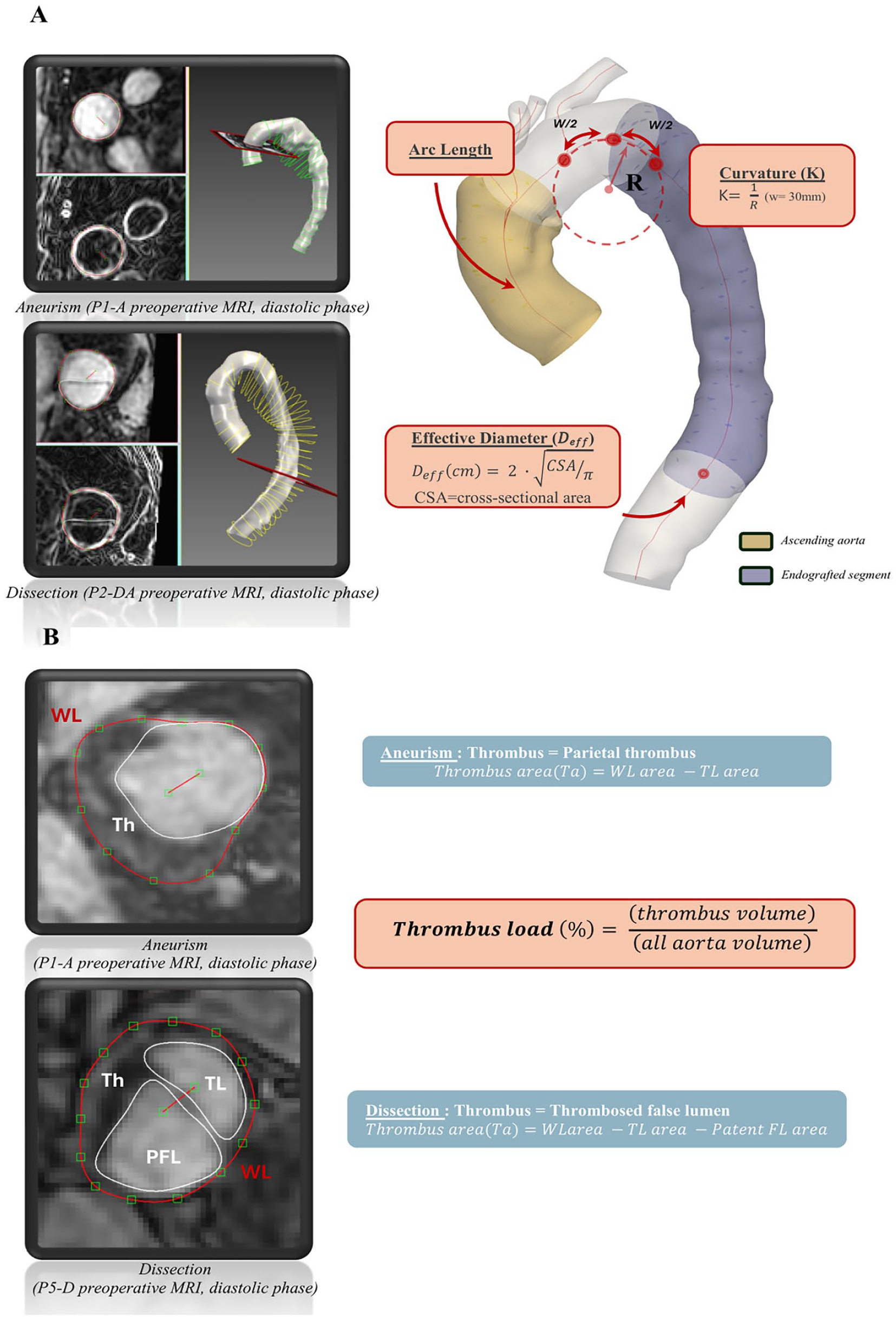
Modeling, metrics quantification and thrombus load assessment. (A) Dual segmentation geometric modeling and metrics quantification and (B) Thrombus load assessment. WL, whole lumen; TL, true lumen; FL, false lumen; PFL, patent false lumen; Th, thrombus.
Paths were cubic-splined and Fourier-smoothed and perpendicular cross-sectional segmentation of the aortic lumen, and all supra-aortic branches was performed from cut planes orthogonal to the paths of each vessel lumen. The active contouring with level-set method was used and manually adjusted. Contours were spaced 10 mm apart along the length of the vessel centerline. To better assess the different components of the dissected or aneurysmal vessels (thrombosed vs patent false lumen, parietal thrombus), a dual lumen modeling protocol was performed as described elsewhere. 17
Region Definition and Quantification of Metrics
In addition to analyzing the whole length of the constructed 3D models, the following subsegments were analyzed separately: (1) ascending aorta (spanning from the STJ to the BCT), (2) endograft location (defined as the endografted segment postoperatively and the corresponding longitudinal segment in the preoperative model defined in relation to a fiducial marker leveraging the Lagrangian coordinate system, as described previously),10,15,16,18,19 and (3) the region in which thrombus was present.
In these segments, a set of metrics was defined to study aortic morphology and deformation before and after TEVAR (Figure 1A). Arclength was defined as the distance of the centerline in 3D between the proximal and distal ends of the studied segment for diastole and systole. The centerline curvature was computed every 1 mm along the segment using a circle-fitting method with a sliding window of 3 cm to reduce noise.15,20 The curvature was then averaged over the segment and reported for diastole and systole, respectively. We quantified the cross-sectional area of the true and whole lumina, and if present, also patent false lumen and thrombus, along the whole length (again, utilizing a sliding span of 3 cm) at both diastole and systole. The true and whole lumen areas were used to compute effective diameters defined as follows:
Presence of thrombus was assessed all along the thoracic aorta (from STJ to the coeliac trunk). Thrombus area was computed slightly differently depending on etiology. For aneurysms, the thrombus area was the parietal thrombus, which was determined by subtracting the patent lumen area from whole lumen area. For dissections, thrombus area was the result of subtracting both true and patent false lumen areas from the whole lumen area (Figure 1B).
In cases where thrombus was present, we leveraged the quantified areas and arclengths to define thrombus load as follows:
For each of those metrics, subgroup analysis was performed for aneurysm and dissection patients independently.
Statistical Analysis
For the analysis of continuous variables, descriptive statistics (means and standard deviations) were calculated. Paired t-tests were performed to assess disparities in continuous variables among patients and a p-value <0.05 was considered as statistically significant. Spearman’s correlation coefficient (R) was calculated to assess the correlations between independent variables in the linear regression model. Coefficient of determination (R2) was used to indicate the proportionate amount of variation between 2 assessed variables in the linear regression model. Statistical analysis was performed using Excel (Microsoft Software 2018, Redmond, USA) and various Python libraries including Numpy, Pandas, Matplotlib, and Pyplot.
Results
Patient Demographics and MRI Acquisitions
Fourteen patients from the FASCAT study successfully completed the required sequences of pre- and postoperative 4D flow MRI and included in this study (Supplemental Figure 1). Median time between pre- and postoperative MRI was 124.6 ± 81.7 days.
Patient and device characteristics are described in Tables 1 and 2. Seven patients received a TEVAR for a subacute or chronic dissection, 7 for descending thoracic aortic or thoraco-abdominal aortic aneurysm. Average length of coverage was 243.6 ± 60.1 mm. In 50% of the cases (n=7/14), proximal sealing was obtained in zone 3.
Patients and Devices’ Characteristics (n=14 Patients).
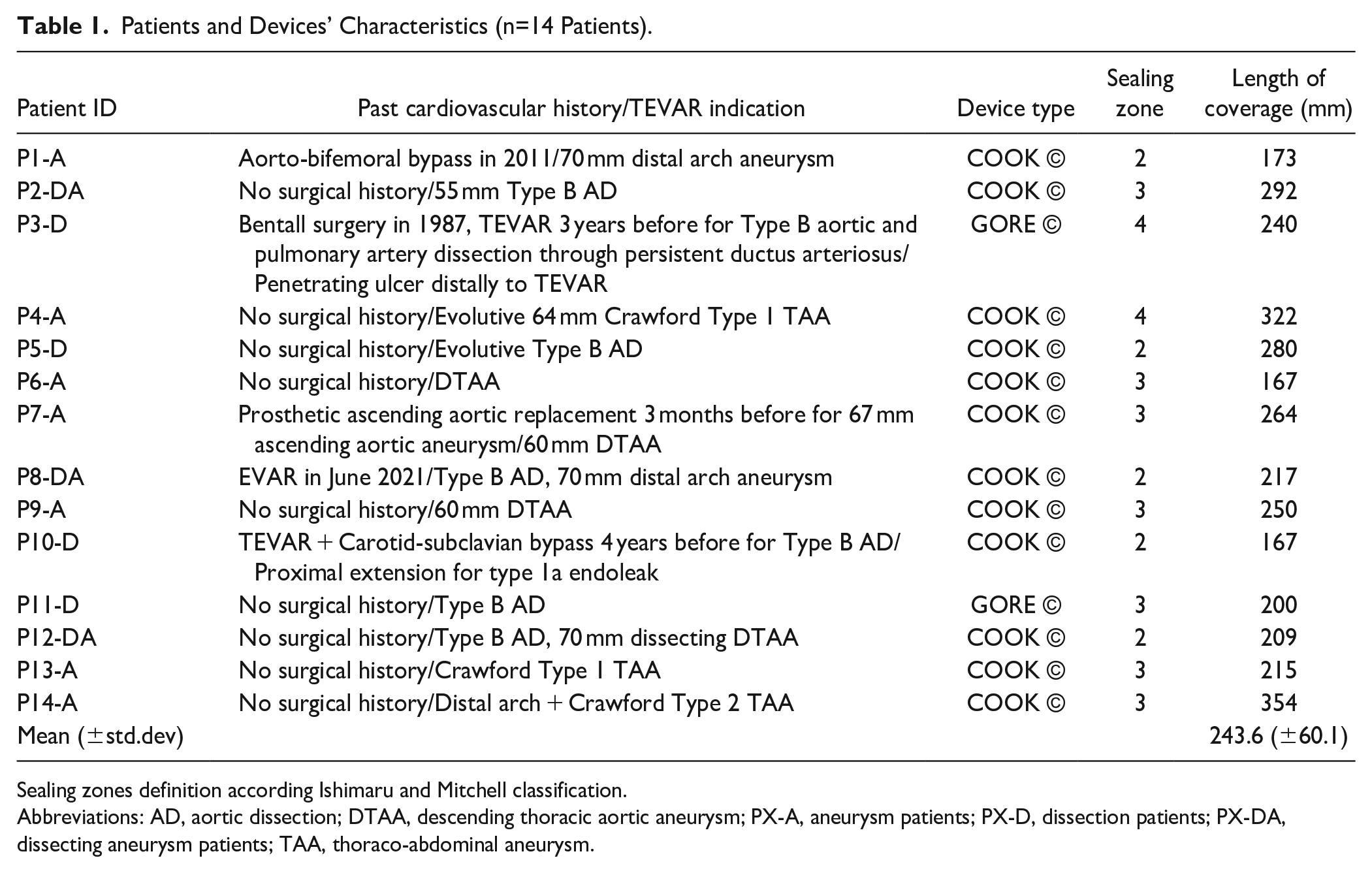
Sealing zones definition according Ishimaru and Mitchell classification.
Abbreviations: AD, aortic dissection; DTAA, descending thoracic aortic aneurysm; PX-A, aneurysm patients; PX-D, dissection patients; PX-DA, dissecting aneurysm patients; TAA, thoraco-abdominal aneurysm.
Patients’ Comorbidities (n=14 Patients).
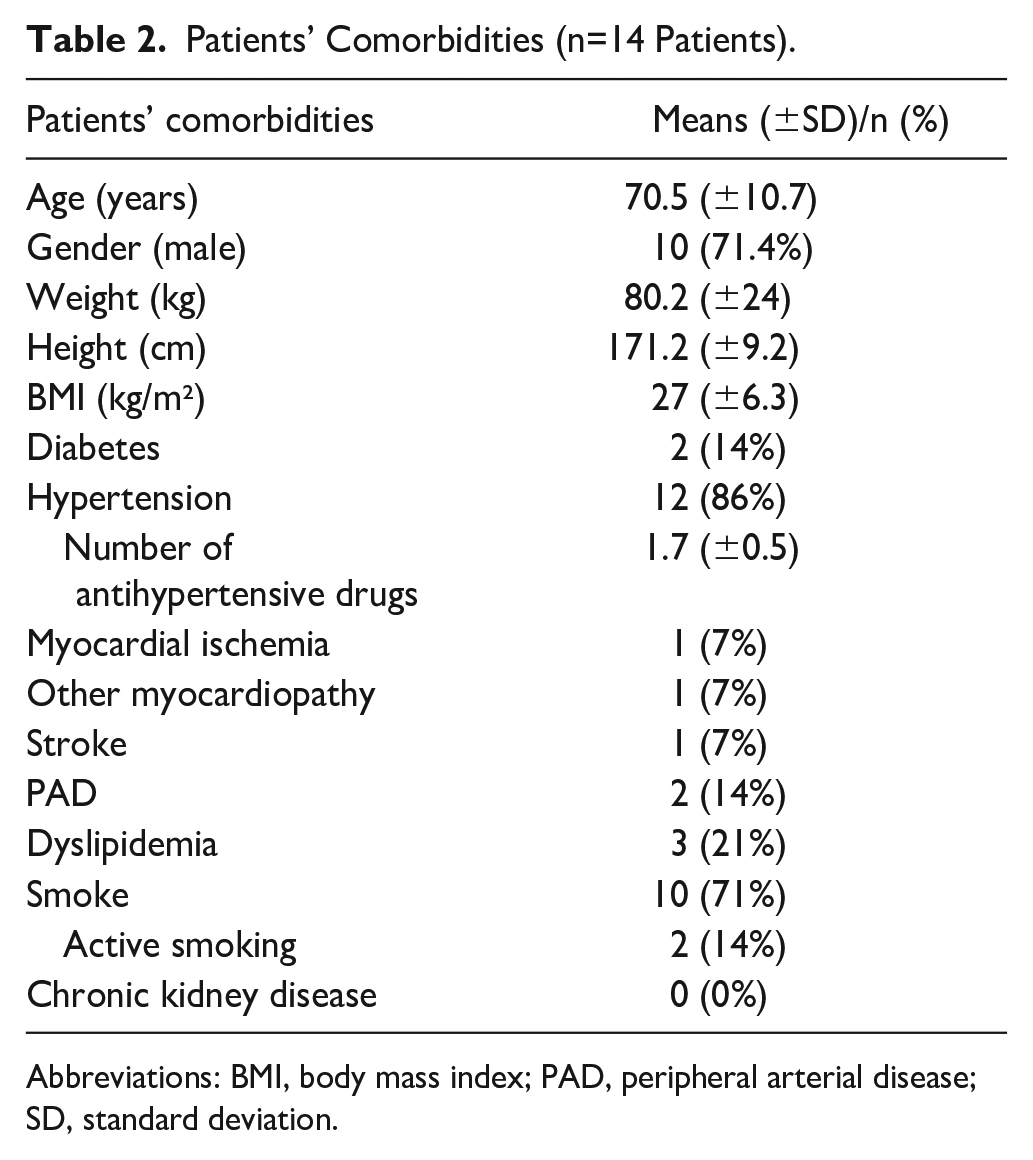
Abbreviations: BMI, body mass index; PAD, peripheral arterial disease; SD, standard deviation.
Multiaxial Deformation of the Endografted Aortic Segment
Metrics quantification in the stented segment is described in Table 3. No statistically significant difference was observed on average bending between pre- and postoperative aortic geometries in this segment. Cross-sectional analysis showed a small but significant sac shrinkage postoperatively (4.7 ± 0.5 cm vs 4.5 ± 0.6 cm in systole, p<0.05). Pulsatility-induced diameter change analysis revealed a decrease in pre-to-postoperative aortic radial deformation in this segment, for both external mean effective diameters (7.2% ± 3.6% vs 5.0% ± 2.0%, p<0.05) and true/patent lumen effective diameters (10.7% ± 5.1% vs 6.2% ± 1.8%, p<0.05).
Multiaxial Cardiac-Induced Deformation of the Endografted Aortic Segment and of the Ascending Aorta (From STJ to BCT).
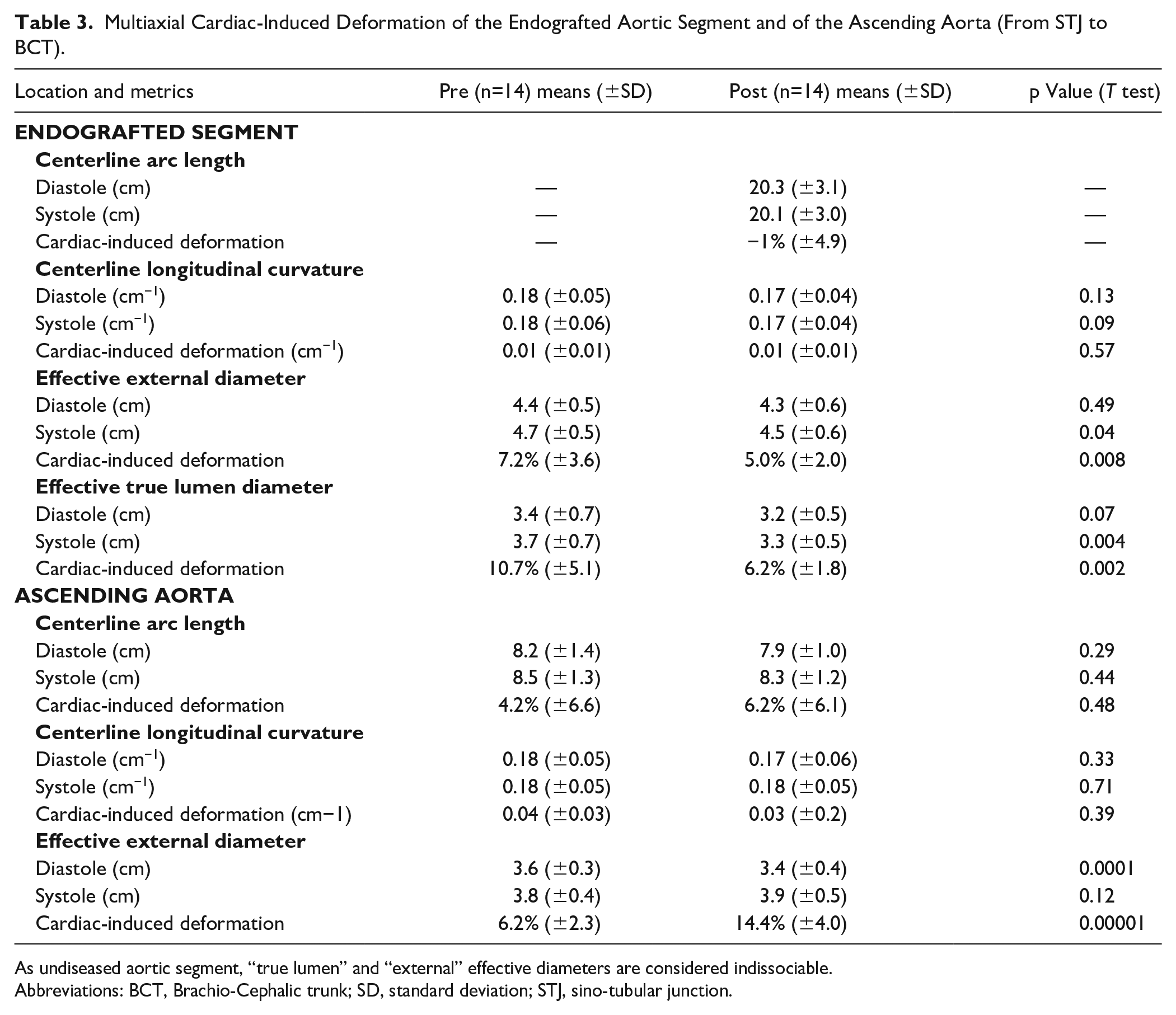
As undiseased aortic segment, “true lumen” and “external” effective diameters are considered indissociable.
Abbreviations: BCT, Brachio-Cephalic trunk; SD, standard deviation; STJ, sino-tubular junction.
Multiaxial Deformation of the Ascending Aorta, Upstream of TEVAR
Metrics quantification in the ascending aortic segment is described in Table 3. No statistically significant differences were observed in axial arclength and average bending between pre- and postoperative ascending aortic geometries. Radial deformation showed a significant increase from pre- to postoperative geometries in this aortic segment (6.2% ± 2.3% vs 14.4% ± 4%, p<0.05).
Effect of Thrombus Load at Baseline
Pre- and postoperative thrombus load assessment for each patient is described in Table 4. Cardiac cycle-averaged thrombus load at the level of diseased thoracic aorta almost doubled from pre-to-post TEVAR (14.0% ± 13.4% vs 25.9% ± 14%, p<0.05). Regarding thrombus location, in 5 out of 14 patients (35.6%) the thrombus assessed preoperatively ended being fully covered by the endograft postoperatively, both proximally and distally. For 8 patients (57.1%), the proximal end of the thrombus was covered by the endograft, but the distal end was not covered. For 1 patient, thrombosed regions persisted both proximally and distally to the predicted position of the endograft (shaggy thoracic aorta). A significant negative correlation was found between thrombus load at baseline and amplification in radial deformation in the ascending aorta (R=−0.80, R2=0.64). This correlation increases upon excluding patients with a history of prosthetic ascending aorta replacement (R=−0.88, R2=0.78) in which ascending aortic motions might be altered (Figure 2).
Cardiac-Averaged Thrombus Load Assessment.
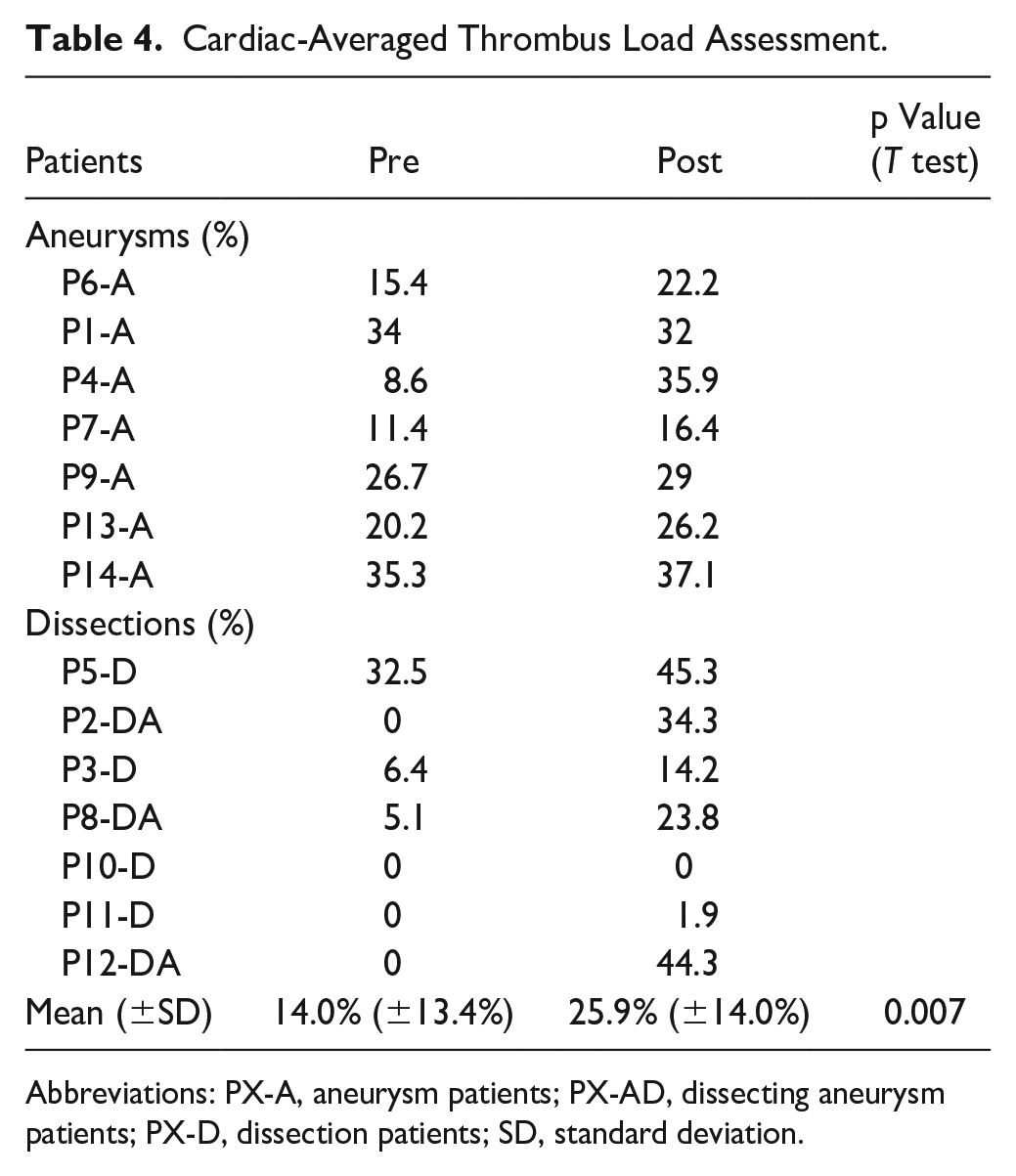
Abbreviations: PX-A, aneurysm patients; PX-AD, dissecting aneurysm patients; PX-D, dissection patients; SD, standard deviation.
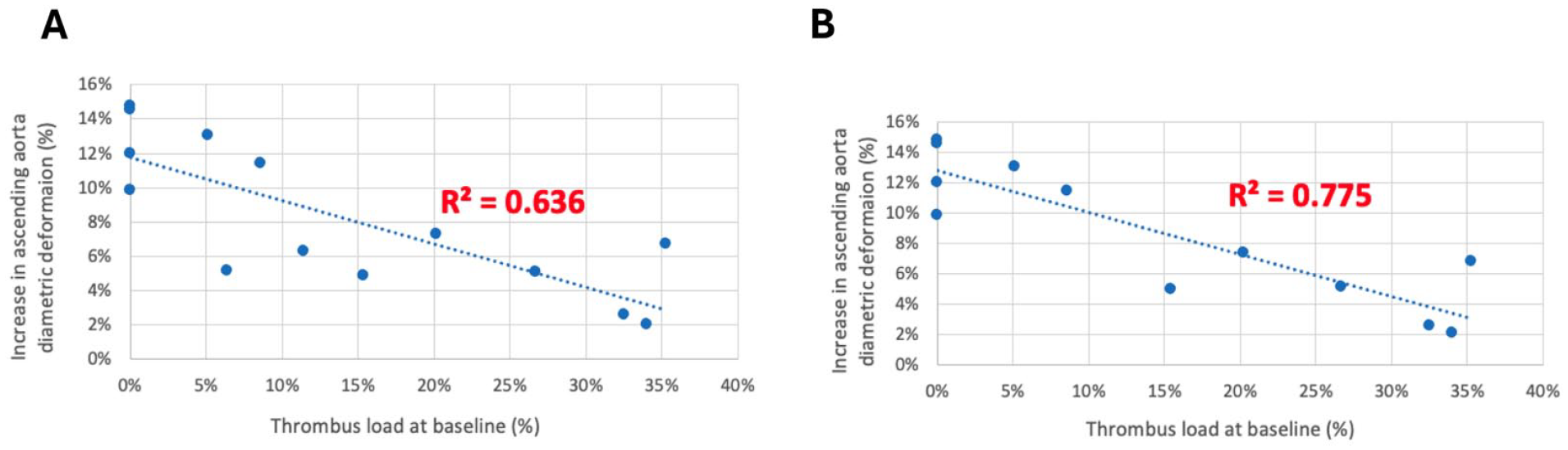
Correlation analysis between preoperative thrombus load and modification in cardiac-induced diametric deformation in ascending aorta. (A) Thrombus load at baseline versus increase in ascending aorta diametric deformation pre-to-post TEVAR (n=14 patients). (B) Thrombus load at baseline versus increase in ascending aorta diametric deformation pre-to-post TEVAR (excl. prosthetic ascending aorta replacement, n=12 patients).
Subgroups Analysis
Results of subgroup analysis for each outcome are presented in Supplemental Table 1 and Supplemental Figure 2. Same trends are found, in both aneurysms and dissections groups, for each parameter, as compared to the whole cohort. Decrease in cardiac-induced radial deformation in the endografted segment pre-to-post TEVAR was greater in the dissections group (11.8% ± 6.4% vs 6.4% ± 1.3%, p<0.05) as compared to the aneurisms group (8.9% ± 2.5 vs 5.7% ± 2.2%, p<0.05; Supplemental Table 1). Similarly, increase in cardiac-induced radial deformation in the ascending aorta pre-to-post TEVAR was greater in the dissections group (5.0% ± 1.2% vs 14.8% ± 4.7, p<0.05) as compared to the aneurisms group (7.5% ± 2.4% vs 13.7% ± 2.7%, p<0.05; Supplemental Table 1). Thrombus load at baseline was negatively correlated with increase in ascending aorta radial deformation in a stronger manner in the dissection subgroup as compared to dissections’ (R2=0.63 vs R2=0.37).
Discussion
The current MRI-based study suggests that TEVAR alters aortic radial deformation not only in the endografted segment as expected but also somewhat surprisingly in the ascending aorta upstream of the device. More specifically, we found a significant decrease in the endografted segment’s radial deformation of about 30% from pre- to post-TEVAR (7.2% ± 3.6% vs 5.0% ± 2.0%, p<0.05). This has already been described in a similar range in a few published papers, based on computed tomography (CT)-based analysis, and may be partially explained by the TEVAR-related increase in aortic stiffness and subsequent tissue remodeling.10,12,21,22 In addition, the thrombus assessment determined that cardiac cycle-averaged thrombus volume almost doubled from pre- to post-TEVAR (14.0% ± 13.4% vs 25.9% ± 14%, p<0.05). As the thrombus is principally located at the endografted segment level postoperatively, due to the aneurysmal sac and/or dissection exclusion, this may also partially explain the reduction in cross-sectional motion at this level.
On top of the effect of the device on the endografted segment’s motion, our study confirms the impact of TEVAR on the adjacent unstented ascending aorta, with an amplification of radial deformation of approximately 100% from pre- to post-TEVAR (6.2% ± 2.3% vs 14.4% ± 4.0%, p=0.00001), probably due to pressure pulse reflection from the stiffened endograft region. A few previous CT-based studies suggested an increase in pulsatile wall stresses after TEVAR in segments adjacent to the device.10–12 Nauta et al showed that the pulsatile circumferential strain tended to increase (26%) proximal to the stent-graft at the STJ level, on a population of 8 aneurysm patients after TEVAR. Suh et al reported that distal ascending aorta near the aortic arch exhibited increased amplitudes of inner surface and centerline curvatures, accompanied by an increased amplitude of cross-sectional eccentricity, on 11 patients, following TEVAR. 10 Our findings corroborate the hypothesis that the ascending aorta may leverage the loss of the pulsatile Windkessel effect of the stented segment, where the increased impedance of the endografted segment is compensated by an increase in upstream ascending aorta pulsatility, to maintain kinetic energy storage over the cardiac cycle.11,23 This is of particular importance in light of the fact that the ascending aorta is often referred to the “third ventricle.” The observed increase in circumferential strain in the ascending aorta may theoretically lead to upstream pressure overload, increased cardiac afterload, and altered ventriculo-aortic coupling, although conflicting results on that are described in the current literature.8,9,24–28 Further assessments of the cardiac impacts of TEVAR are required to better understand these effects and related adaptation processes.
Among other consequences, higher aortic wall stresses concentrations, which could be found in a stiffer aorta or in the case of increased radial deformation, have been linked to higher risk of aneurysm formation and/or aneurysm growth acceleration.29,30 Finite element models have also explored the negative effect of increased wall stresses on aortic wall outcomes.31,32 Raaz et al demonstrated that segmental aortic stiffening in an established murine elastase-induced aortic aneurysm model can precede upstream aneurysm growth due to compliance mismatch. 33 Similarly, Nauta et al found that TEVAR-induced radial stiffening resulted in a radial strain mismatch in the proximal thoracic aorta in a porcine model. 6 Those axially tethering forces during the systolic circumferential expansion of the adjacent compliant wall segments, increasing stresses in the wall, may also partially explain upstream aortic complications following TEVAR such as aneurysm growth, endoleaks, or retrograde dissections.4,6,34,35 Further studies will be required, however, to specifically link this increase in aortic radial deformation to longer-term aortic outcomes.
Although significant amplification in ascending aortic radial deformation was observed in our study, and thus conceivably higher ascending aortic wall stresses, no impact on aortic geometry, and more specifically, on cardiac cycle-averaged ascending aortic diameter was found pre-to-post TEVAR (3.7 ± 0.3 cm vs 3.6 ± 0.4 cm, p=0.23). One type 1a endoleak was observed in our cohort at follow-up completion, successfully treated by an adjunct of a proximal module, 3 months after the index procedure. The fact that these types of complications were not observed in our cohort can obviously be explained by the relatively short median time between pre- and postoperative assessment in our study (124.6 ± 81.7 days). However, considering this literature, other parameters such as aortic stiffness at baseline are also suggested as key components of the remodeling processes that seem to occur following TEVAR.
Thrombus load was assessed in our study to evaluate if, and to what extent, descending aortic stiffness at baseline may play a role in the postoperative mechanical effects of TEVAR. Our study found a significant negative correlation between preoperative thrombus load at the level of diseased thoracic aorta and the pre-to-post TEVAR amplification of ascending aortic radial deformation (R=−0.80, R2=0.64), that is, the higher the thrombus load at baseline, the smaller the increase in ascending aortic deformation that was observed postoperatively. As thrombus is greater in aneurysms patients one could argue that thrombus load acts as a confounding factor. However, subgroups analysis showed that (1) the strong negative correlation between thrombus load and increase in aortic radial deformation was also found in the dissection patients (Supplemental Figure 2) and (2) we did not find any significant differences between the increase in radial deformation in aneurysm versus in dissection patients (p=0.12) (Supplemental Table 1). Although the biomechanical effects of intraluminal thrombus (ILT) on the pathogenesis and natural history of aortic aneurysms (aneurysmal growth, risk of rupture) have been widely debated in the literature, the link between the presence of ILT, increased aortic stiffness and a decrease in the peak wall stress seems widely accepted.13,36,37 It is noteworthy that the dichotomous protective and deleterious role of ILT mostly relies on the fact that even though ILT reduces peak stresses in the wall, it may also simultaneously alter the strength of the wall by inducing localized hypoxia and wall weakening. 31 Our results support the hypothesis that from a purely mechanical point of view, high thrombus load at baseline can potentially account for a cushioning effect that reduces wall stresses in the endografted segment, thereby reducing the impact of the device’s stiffness itself. This correlation was found to be even stronger upon excluding the 2 patients with past medical history of ascending aortic prosthetic replacement (R=−0.88, R2=0.77). The knitted polyester grafts used for surgical open repair are relatively noncompliant and deform less diametrically with pulsatile pressure compared to the native aorta.5,38
Our study has a number of limitations. First, as in the case of most cohort studies on TEVAR, our cohort includes a mixed population with different pathologies, aneurysms and dissections, which do not share the same wall biomechanics at baseline. 39 However, our subgroups analysis confirmed similar trends in both groups. Impact of the endograft on the aortic motion seemed greater in dissection cases, which may be explained by the increased elasticity of aortic tissue in the dissection’s patients and lower thrombus load at baseline. Larger cohorts will be required to compare the behavior of the aortic wall in both pathologies.
Second, like most similar CT-based studies, our study is based on a relatively small sample of patients, although it remains in the highest ranges of cohorts’ sizes presented in literature.10,40,41 Third, with a median follow-up of a little more than 4 months, we acknowledge that only short-to mid-term outcomes are captured. Finally, unlike most teams working on pulsatility-induced aortic deformation, our study was not based on ECG-gated CT but on MRI with lower spatial resolution and potential imaging artifacts.
If our results are confirmed on a longer term and larger scale, our study could have notable clinical as well as industrial impacts. First, because of the augmentation of compliance upstream of the endograft, close follow-up of the ascending aorta and arch following descending TEVAR is important. Second, the cushioning effect of thrombus suggests that the preoperative aortic stiffness modulates the effect of the endograft on aortic biomechanics, meaning that aortic stiffness at baseline could be a new gauge for complication risk from compliance mismatch following TEVAR. Those at risk may include patients presenting “less stiff” aortas, such as those presenting with no thrombus, fibroelastic tissue disorders, and/or younger patients. Also, patient-specific detection could lead to more personalized approaches for device selection or adjusting endograft compliance to better match aortic stiffness. Lastly, this data could be a call to action for manufacturers to develop devices that better match native aortic compliance.
Conclusion
As a result of TEVAR, aortic radial deformation is reduced in the stented aortic segment, likely due to increased stiffness of the endograft and wall remodeling, but is amplified upstream in the ascending aorta, likely due to pressure pulse reflection. Thrombus load at baseline may serve as an interesting predictor of ascending aortic radial deformation amplification following TEVAR. These findings highlight the benefit of thrombus load assessment pre-TEVAR and underscore the need for increasing the compliance of future graft designs in order to minimize longer-term aortic complications following TEVAR.
Supplemental Material
sj-docx-1-jet-10.1177_15266028251339347 – Supplemental material for Impacts of Thoracic Endovascular Aortic Repair and Thrombus Load on Aortic Radial Deformation
Supplemental material, sj-docx-1-jet-10.1177_15266028251339347 for Impacts of Thoracic Endovascular Aortic Repair and Thrombus Load on Aortic Radial Deformation by Alexandra Hauguel, Johan Bondesson, Arshid Azarine, Kianosh Kasani, Abdul I. Barakat, Stephan Haulon and Christopher P. Cheng in Journal of Endovascular Therapy
Supplemental Material
sj-docx-2-jet-10.1177_15266028251339347 – Supplemental material for Impacts of Thoracic Endovascular Aortic Repair and Thrombus Load on Aortic Radial Deformation
Supplemental material, sj-docx-2-jet-10.1177_15266028251339347 for Impacts of Thoracic Endovascular Aortic Repair and Thrombus Load on Aortic Radial Deformation by Alexandra Hauguel, Johan Bondesson, Arshid Azarine, Kianosh Kasani, Abdul I. Barakat, Stephan Haulon and Christopher P. Cheng in Journal of Endovascular Therapy
Supplemental Material
sj-tiff-3-jet-10.1177_15266028251339347 – Supplemental material for Impacts of Thoracic Endovascular Aortic Repair and Thrombus Load on Aortic Radial Deformation
Supplemental material, sj-tiff-3-jet-10.1177_15266028251339347 for Impacts of Thoracic Endovascular Aortic Repair and Thrombus Load on Aortic Radial Deformation by Alexandra Hauguel, Johan Bondesson, Arshid Azarine, Kianosh Kasani, Abdul I. Barakat, Stephan Haulon and Christopher P. Cheng in Journal of Endovascular Therapy
Supplemental Material
sj-tiff-4-jet-10.1177_15266028251339347 – Supplemental material for Impacts of Thoracic Endovascular Aortic Repair and Thrombus Load on Aortic Radial Deformation
Supplemental material, sj-tiff-4-jet-10.1177_15266028251339347 for Impacts of Thoracic Endovascular Aortic Repair and Thrombus Load on Aortic Radial Deformation by Alexandra Hauguel, Johan Bondesson, Arshid Azarine, Kianosh Kasani, Abdul I. Barakat, Stephan Haulon and Christopher P. Cheng in Journal of Endovascular Therapy
Footnotes
Declaration of Conflicting Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.H. is a consultant and has intellectual property for Cook Medical. The other authors do not declare any potential conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We strongly thank the Engineering for Health (E4H) Interdisciplinary Center of Institut Polytechnique de Paris for financial support through their Medical Fellows Program financed by the ANR grant ExcellencES “Science and Technology at Polytechnique Paris (STeP2).”
Ethical Approval and Informed Consent
This study received ethical approval from local ethical committee, IRB approval #00012157, on April 20th, 2022 and informed consent was obtained for all patients.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.