
Abstract
Background:
Endovascular revascularization of below-the-knee lesions is a crucial treatment for patients with chronic limb-threatening ischemia (CLTI). However, the optimal approach to revascularizing infrapopliteal arteries remains uncertain. This study aims to compare the safety and efficacy outcomes of various endovascular treatment modalities for infrapopliteal artery disease and provide an evidence-based update through a network meta-analysis.
Methods:
We performed a systematic literature search in MEDLINE, EMBASE, and the Cochrane Database for randomized controlled trials published between January 01, 2005, and January 12, 2025. The study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and was prospectively registered in PROSPERO database (CRD42022323480). The primary safety outcome was major adverse events defined as a composite of all-cause death, major amputation, and any re-intervention of the target limb at 30 days. The primary efficacy outcomes included freedom from composite of major amputation, target lesion occlusion, and clinically driven target lesion revascularization (CD-TLR) and primary patency defined as freedom from binary restenosis and CD-TLR at 6 months. The network meta-analysis was conducted in the frequentist framework using random effects model and conventional percutaneous transluminal angioplasty (PTA) as the reference intervention. Treatment effects were reported as odds ratio (OR) with 95% confidence interval (CI) compared with conventional PTA and interventions were ranked using P-scores.
Results:
Twenty-three studies including 3091 patients treated with PTA, paclitaxel drug-coated balloons (DCB), drug-eluting stents (DES), bare metal stents (BMS), bioresorbable vascular scaffold (BVS), and atherectomy were included. There were no significant differences in the primary safety outcome between different treatment modalities. At 6 months, DCB, atherectomy with DCB, and DES produced the largest benefit for primary efficacy outcomes. DCB (OR, 3.68; 95% CI, 1.37–9.92) had a higher freedom from the primary composite, and atherectomy with DCB (OR, 7.65; 95% CI, 1.03–56.98) and DES (OR, 5.48; 95% CI, 1.54–19.49) had higher primary patency compared with PTA. At 12 months, the benefit of atherectomy with DCB was sustained for primary patency, and BVS was ranked first for freedom from the primary composite. There was no benefit of BMS compared with PTA at any timepoint.
Conclusions:
This network meta-analysis evaluating 7 endovascular treatment modalities provides evidence of improved efficacy outcomes with DCB, atherectomy with DCB, DES, and BVS compared with PTA for treating infrapopliteal lesions in patients with CLTI.
Clinical Impact
Local antiproliferative drug delivery, whether by balloon-expandable sirolimus/everolimus DES or paclitaxel DCB or everolimus BVS, is necessary to improve patency and efficacy outcomes for the treatment of infrapopliteal artery disease. Furthermore, combining atherectomy with drug delivery shows promising potential. Emerging endovascular targeted drug delivery therapies with limus-based DCB or scaffolds promise to provide greater drug transfer efficiency and a more effective therapeutic alternative that overcomes the limitations of metallic stents in one of the most challenging vascular beds.
Introduction
Chronic limb-threatening ischemia (CLTI), the most severe form of peripheral artery disease (PAD), affects approximately 6.5 million people globally and is often linked to below-the-knee (BTK) artery disease.1,2 CLTI is characterized by chronic ischemic rest pain, ulcers, or gangrene, with poor outcomes if untreated: 25% mortality, 30% amputation, and only 45% survival with both limbs at 1 year. The 5-year mortality rate exceeds 60%. 3
Revascularization of infrapopliteal arteries is a Class I recommendation for CLTI patients to improve blood flow, promote wound healing, and lower the risk of amputation.4,5 About 75% of CLTI patients—around 4.8 million—are candidates for endovascular therapy. 1 Though revascularization incurs upfront costs, it is considered cost-effective by reducing long-term expenses associated with amputations and disability.6,7 Furthermore, the BEST-CLI trial showed that both surgical and endovascular revascularization significantly improved patient-reported outcomes, including quality of life (QoL) measures related to disease severity and physical, mental, and social function. 8
Endovascular interventions for infrapopliteal artery disease are particularly challenging due to multilevel artery disease, smaller vessel size, diffuse and long lesions, calcium burden, impaired runoff, elastic recoil, risk of dissection, and high restenosis rates. 2 Despite inherent limitations, percutaneous transluminal angioplasty (PTA) with a plain (nondrug-coated) balloon has been the mainstay technique for decades. Emerging technologies such as drug-eluting stents (DES), drug-coated balloons (DCB), bioresorbable vascular scaffolds (BVS), plaque modification devices, and Philips Tack postangioplasty dissection repair systems have the potential to improve the efficacy of endovascular interventions for BTK artery disease and change clinical practice guidelines.
A comprehensive analysis of the evidence for safety and efficacy outcomes of different endovascular treatment modalities for BTK disease constitutes the prerequisite groundwork to better understand the status quo and pave the way for future developments in the field. With this in mind, we performed a systematic review and network meta-analysis focused on meaningful and contemporary outcomes evaluating the safety and efficacy of currently available treatments for infrapopliteal artery disease up to 12 months after the procedure. We aimed to provide comparative outcomes of different treatment modalities based on network-derived pooled direct and indirect evidence.
Methods
Search Strategy and Data Abstraction
This network meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement guidelines 9 and was prospectively registered in the PROSPERO database (CRD42022323480). We performed a comprehensive literature search in MEDLINE (PubMed), EMBASE, and the Cochrane Database of Systematic Reviews using the following search terms: “peripheral artery disease,” “artery occlusive disease,” “critical limb ischemia,” “below the knee,” “infrapopliteal arteries,” “anterior tibial arteries,” “posterior tibial arteries,” “crural arteries,” “angioplasty,” “percutaneous transluminal angioplasty,” “plain old balloon angioplasty,” “atherectomy,” “drug-coated balloon,” “cutting balloon,” “scoring balloon,” “lithotripsy,” “bare-metal stent,” “drug-eluting stent,” and “scaffold” (Supplemental Table 1). The search was restricted to randomized controlled trials (RCTs) published in English between January 2005 and January 12, 2025. Three investigators independently screened titles/abstracts for eligibility criteria. Discrepancies were resolved by a fourth investigator (D.T.). The studies were selected if they met the following selection criteria: (1) patients were treated for infrapopliteal artery disease; (2) the studies were RCTs comparing at least 2 endovascular intervention modalities for infrapopliteal lesions; (3) prespecified outcomes were reported per each arm included in the study. Studies were excluded if the target lesions and outcomes were not limited to infrapopliteal lesions. When overlapping data were identified across multiple publications of the same study, only the publication with the most relevant data was selected. The bibliographies of all potentially relevant publications were also searched for additional eligible articles.
Three independent investigators abstracted data on prespecified patient/lesion characteristics and outcomes from the included studies. Abstracted data were reviewed by a fourth investigator, and discrepancies were resolved by consensus.
Quality Assessment
The risk of bias for each RCT included in the analysis was evaluated by 2 independent investigators using the RoB 2 tool, a revised version of the Cochrane Collaboration’s tool for assessing risk of bias. 10 Five domains of potential bias were assessed: randomization process, deviations from intended interventions, missing outcome data, measurement of outcome, and selection of reported result. Disagreements in quality assessment were resolved by consensus with a third investigator.
Prespecified Outcomes
The primary safety outcome was a composite of MAE defined as a composite of all-cause death, major amputation, and any re-intervention of the target limb at 30 days. The primary efficacy outcomes were freedom from composite of major amputation, target lesion occlusion, and CD-TLR and primary patency, defined as freedom from binary restenosis and CD-TLR at 6 months.
Secondary outcomes included efficacy outcomes at 12 months and major amputation, target lesion occlusions, CD-TLR, and all-cause death at 6 and 12 months. Primary patency definitions for all studies included in the analysis are provided in Supplemental Table 2.
Statistical Analyses
Endovascular interventional modalities for BTK disease were compared simultaneously in a single analysis by combining both direct and indirect evidence across a network of studies. The network meta-analysis was conducted in the frequentist framework using random effects model and conventional PTA as the reference intervention. Network diagrams were generated with the size of the nodes proportional to the number of patients for each treatment node, and the lines were weighted according to the number of studies available for each comparison. Treatment effects were reported as odds ratio (OR) with 95% confidence interval (CI) compared with conventional PTA and presented in forest plots. Consistency between direct estimate and indirect estimate, the latter being estimated from the entire network, for each comparison was evaluated using the node-splitting method and presented in forest plots. Interventions were ranked using P-score, a frequentist version of the surface under the cumulative ranking curve score (SUCRA). 11 P-Scores are based on point estimates and standard errors of the network meta-analysis estimates and measure the certainty that an intervention is better than another intervention, averaged over all competing interventions, and indicate which intervention is more or less likely to produce the largest benefits. P-Score values vary from 0 to 1; with a higher P-score value indicating a higher ranking. Because P-scores focus on point estimates of effect and do not consider the significance of treatment effect, the likelihood of being a better option was determined based on CIs for each paired comparison.11,12
Publication bias for each reported outcome was assessed by visual inspection of funnel plot asymmetry and p-value assessed by Egger’s test; a p-value>0.05 indicates a low risk of bias. Meta-regression analysis was conducted to explore the association between outcomes and patient baseline and lesion characteristics. All statistical analyses were performed using R software (R Foundation for Statistical Computing). The network meta-analysis was conducted using Netmeta package, version 4.1.2. p-values<0.05 were considered statistically significant without adjustment for multiplicity.
Results
The literature search resulted in 1455 publications. After screening and eligibility assessment for inclusion criteria, 23 studies with a total of 3091 patients were selected and included in the analysis (Figure 1). Among these 23 RCTs,13 –35 7 interventional modalities were investigated: conventional PTA, DCB, DES, BMS, BVS, atherectomy with PTA, and atherectomy with DCB (Table 1). Of the 3091 patients, 1460 were in the DCB versus PTA studies (n = 8),16 –21,31,32 50 were in DCB versus DES (n = 1), 29 538 were in the DES versus PTA (n = 3),26,30,34 351 were in DES versus BMS studies (n = 3),13,15,25 235 were in BMS versus PTA studies (n = 4),14,22,23,27 and 261 were in BVS versus PTA (n = 1) (Table 1). 33 A few small sample size studies included atherectomy as adjunctive therapy in combination with conventional PTA (50 patients; n = 1), 28 and DCB (146 patients; n = 2).24,35 Among the 3 studies reporting the use of atherectomy, there were 2 types: directional 24 and orbital.28,35 All DCB studies evaluated paclitaxel DCBs. Baseline patient and lesion characteristics, and data availability for primary and secondary outcomes for each study included in the analysis are presented in Table 1. In general, most patients were elderly men with diabetes mellitus and hypertension, presenting with symptomatic CLTI and a Rutherford category ≥4. The proportion of patients with chronic kidney disease, reported in 15 studies, ranged from 8% to 60%. Lesion length varied by treatment type: 90 to 170 mm (weighted average 116.5 ± 93.3 mm) for DCB, 21 to 68 mm (weighted average 35.5 ± 30.3 mm) for DES, 24 to 34 mm for BMS, 43.8 ± 31.8 mm for BVS, 101 to 191 mm (weighted average 151.5 ± 100.5 mm) for atherectomy + DCB and 91 mm for atherectomy with PTA. Weighted average chronic total occlusion rates, based on data from 17 studies, were 45.5% for DCB, 33.5% for DES, 33.4% for BMS and 50% for atherectomy with DCB. Most studies reported the use of dual antiplatelet therapy before and for 1 to 6 months after the procedure, followed by monotherapy for up to 12 months or longer.
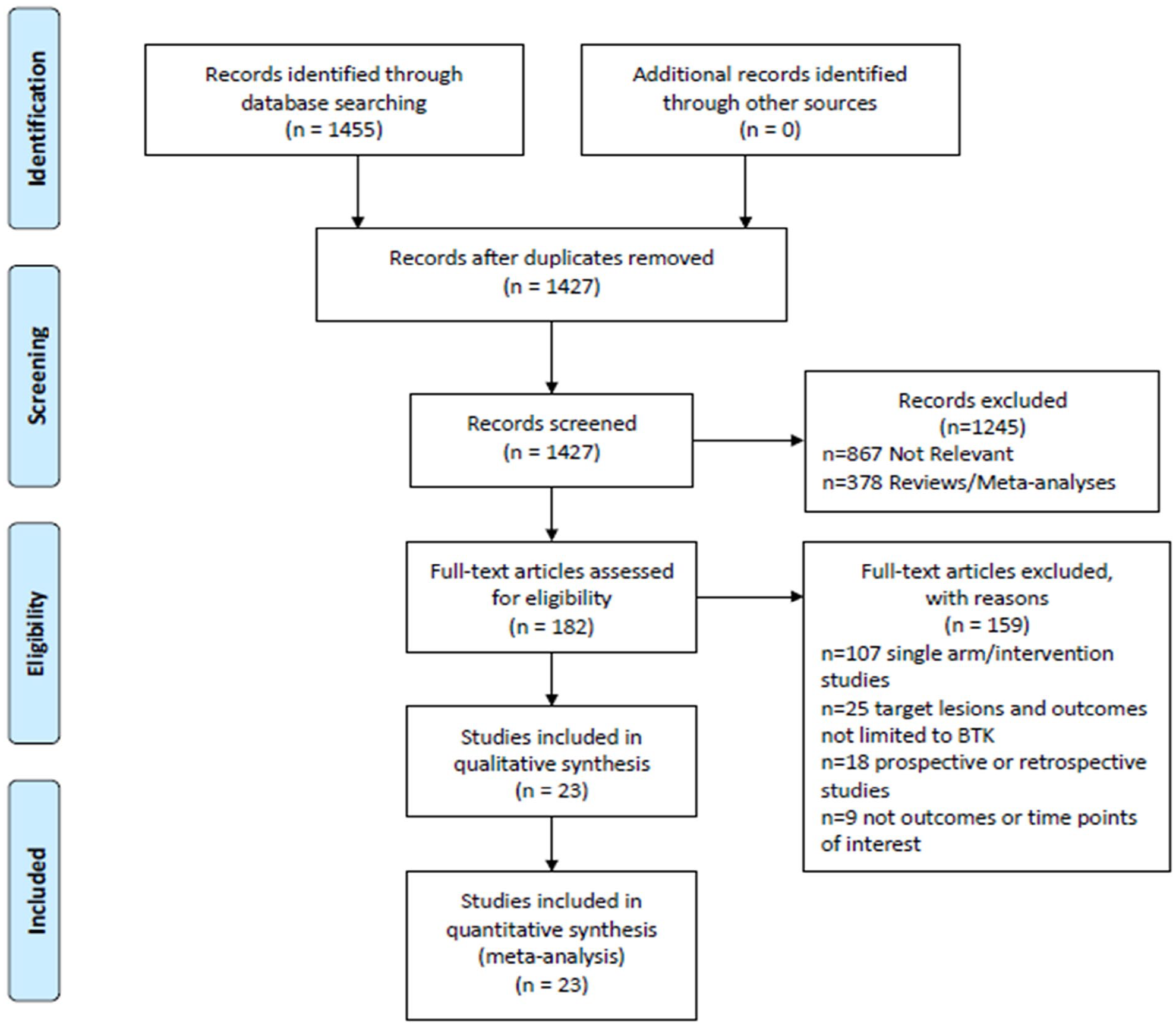
PRISMA flow chart of literature search and study selection.
Baseline Characteristics and Reported Outcomes.
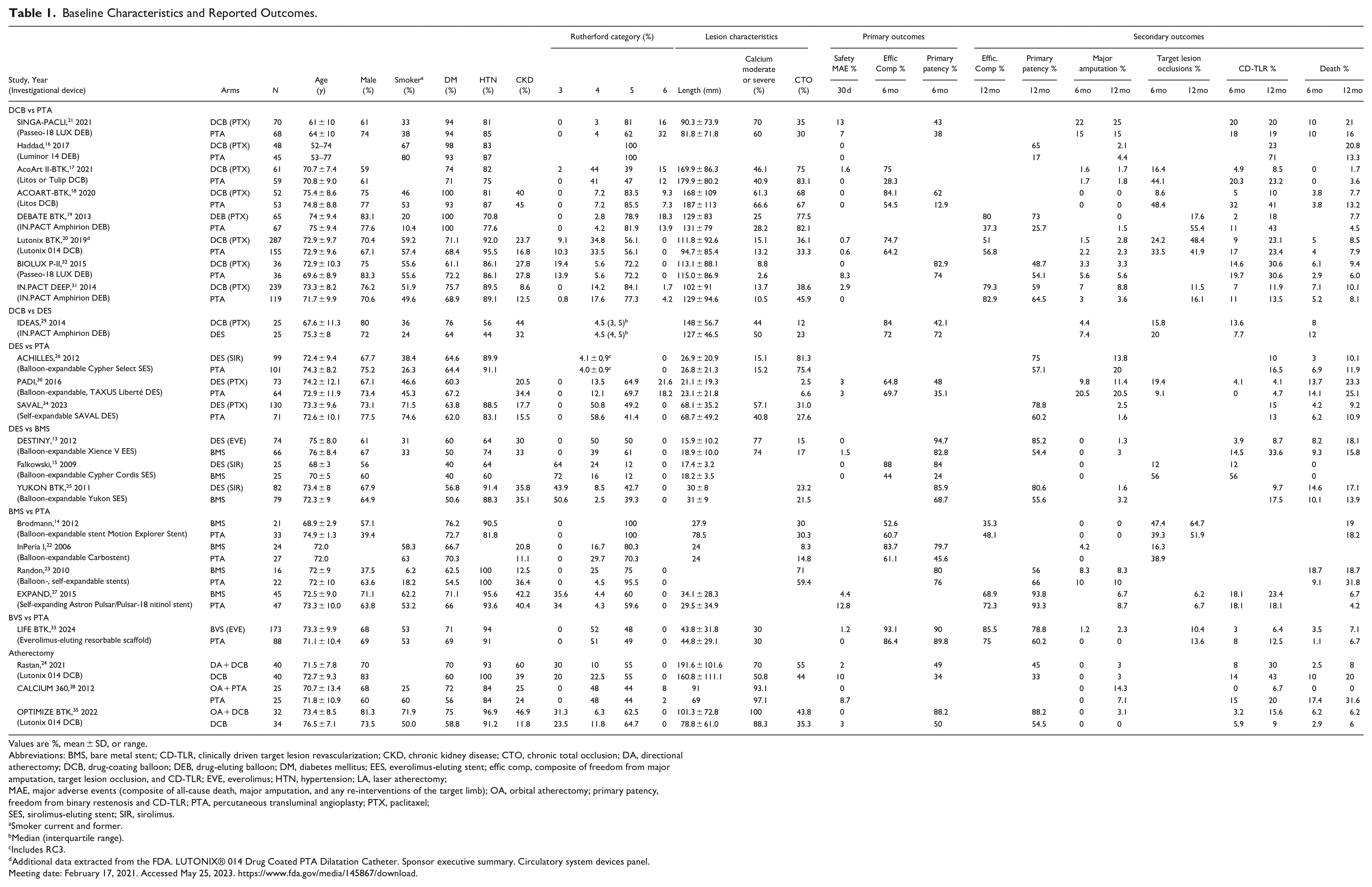
Values are %, mean ± SD, or range.
Abbreviations: BMS, bare metal stent; CD-TLR, clinically driven target lesion revascularization; CKD, chronic kidney disease; CTO, chronic total occlusion; DA, directional atherectomy; DCB, drug-coating balloon; DEB, drug-eluting balloon; DM, diabetes mellitus; EES, everolimus-eluting stent; effic comp, composite of freedom from major amputation, target lesion occlusion, and CD-TLR; EVE, everolimus; HTN, hypertension; LA, laser atherectomy; MAE, major adverse events (composite of all-cause death, major amputation, and any re-interventions of the target limb); OA, orbital atherectomy; primary patency, freedom from binary restenosis and CD-TLR; PTA, percutaneous transluminal angioplasty; PTX, paclitaxel; SES, sirolimus-eluting stent; SIR, sirolimus.
Smoker current and former.
Median (interquartile range).
Includes RC3.
Additional data extracted from the FDA. LUTONIX® 014 Drug Coated PTA Dilatation Catheter. Sponsor executive summary. Circulatory system devices panel. Meeting date: February 17, 2021. Accessed May 25, 2023. https://www.fda.gov/media/145867/download.
The Cochrane tool RoB 2 (The Cochrane Collaboration) was used to assess the risk of bias for the RCTs included in the analysis. Overall, 22 studies had low risk of bias; some concerns were identified in 1 study (Supplemental Figure 1).
Network Meta-Analysis
Primary Safety Outcome
The 30-day MAE composite was reported in 12 studies with 7 interventions [Figure 2(a)]. Compared with PTA, there was no significant treatment effect of any of the other interventions on the occurrence of MAE [DES (OR, 0.52; 95% CI, 0.09–2.97), DCB (OR, 1.62; 95% CI, 0.67–3.96), BVS (OR, 2.69; 0.13–56.54), BMS (OR, 0.46; 95% CI, 0.10–2.08), atherectomy with PTA (OR, 0.18; 95% CI, 0.01–3.86), atherectomy with DCB (OR, 0.43; 95% CI, 0.06–3.29)].
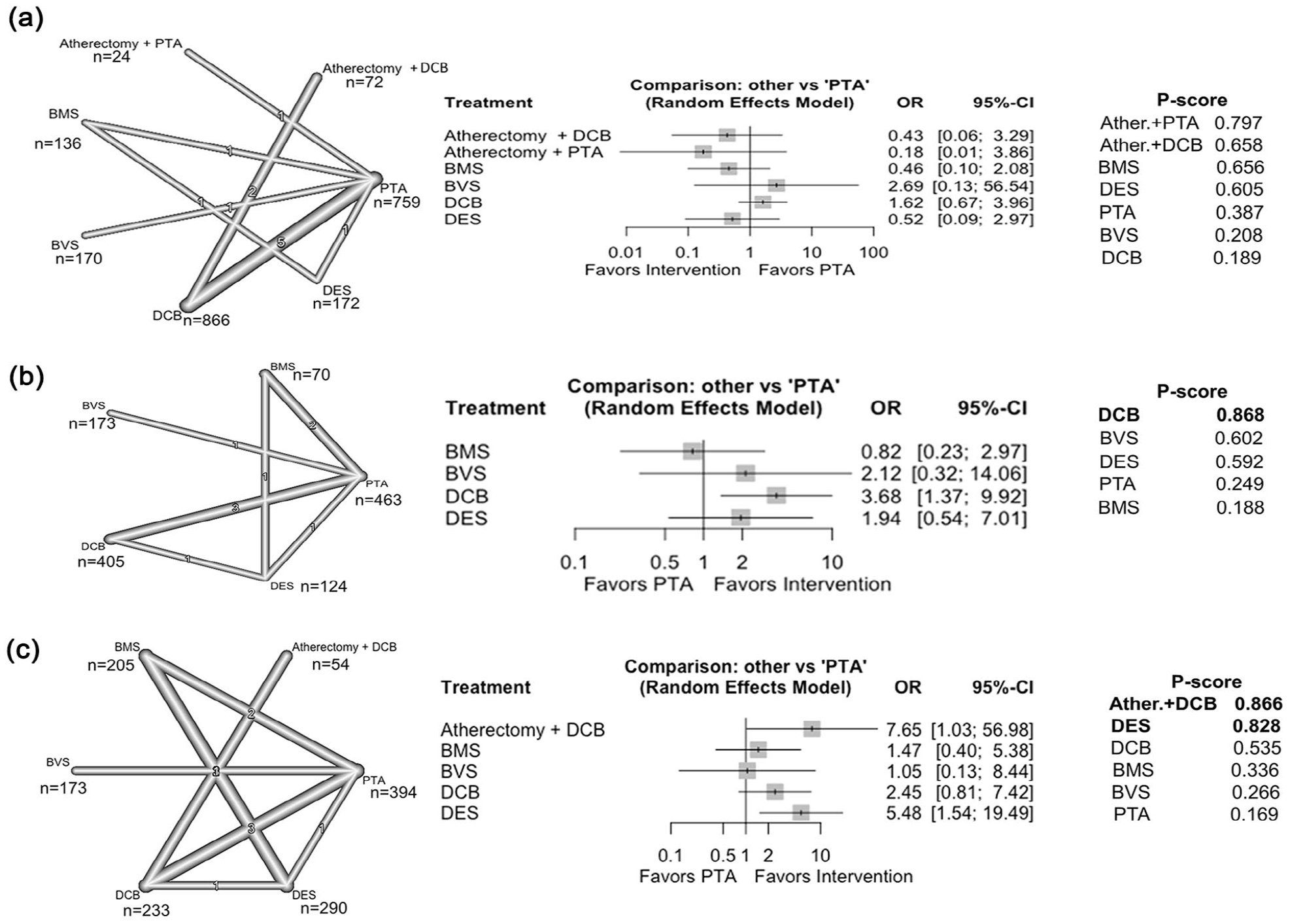
Network diagrams, forest plots, and P-scores for primary outcomes. (a) Safety: major adverse events (MAE; composite of all-cause death, any reinterventions, major amputations) at 30 days, (b) efficacy freedom from major amputation, target lesion occlusion, and CD-TLR at 6 months, and (c) efficacy primary patency defined as freedom from binary restenosis and CD-TLR.
Primary Efficacy Outcome
Freedom from composite of major amputation, target lesion occlusion, and CD-TLR at 6 months was reported in 9 studies with 5 interventions [Figure 2(b)]. Compared with PTA, patients treated with DCB (OR, 3.68; 95% CI, 1.37–9.92) had significantly better odds of freedom from the primary composite. DCB was ranked first with a higher P-score (0.868), followed by BVS (0.602) and DES (0.592) [Figure 2(b)]. Primary patency defined as freedom from binary restenosis and CD-TLR at 6 months was reported in 8 studies with 6 interventions [Figure 2(c)]. Compared with PTA, atherectomy with DCB (OR, 7.65; 95% CI, 1.03–56.98) and DES (OR, 5.48; 1.54–19.49) had significantly better primary patency at 6 months. Based on P-scores, atherectomy with DCB and DES were more likely to produce the largest benefit (0.866 and 0.828, respectively) followed in ranking by DCB (0.535).
Secondary Outcomes at 6 months
Compared with PTA, treatment with DCB (OR, 0.29; 95% CI, 0.09–0.94) had lower odds of target lesion occlusion and a reduced trend in CD-TLR (OR, 0.58; 95% CI, 0.32–1.04) (Figure 3). Based on P-score ranking, DCB was ranked first and DES second in reducing target lesion occlusion (0.903 and 0.599, respectively). Atherectomy with PTA was ranked first and atherectomy with DCB second in reducing CD-TLR (0.809 and 0.678), and DES was more likely to produce the largest benefit in reducing major amputations (0.864). There were no significant treatment effects with respect to all-cause death at 6 months.
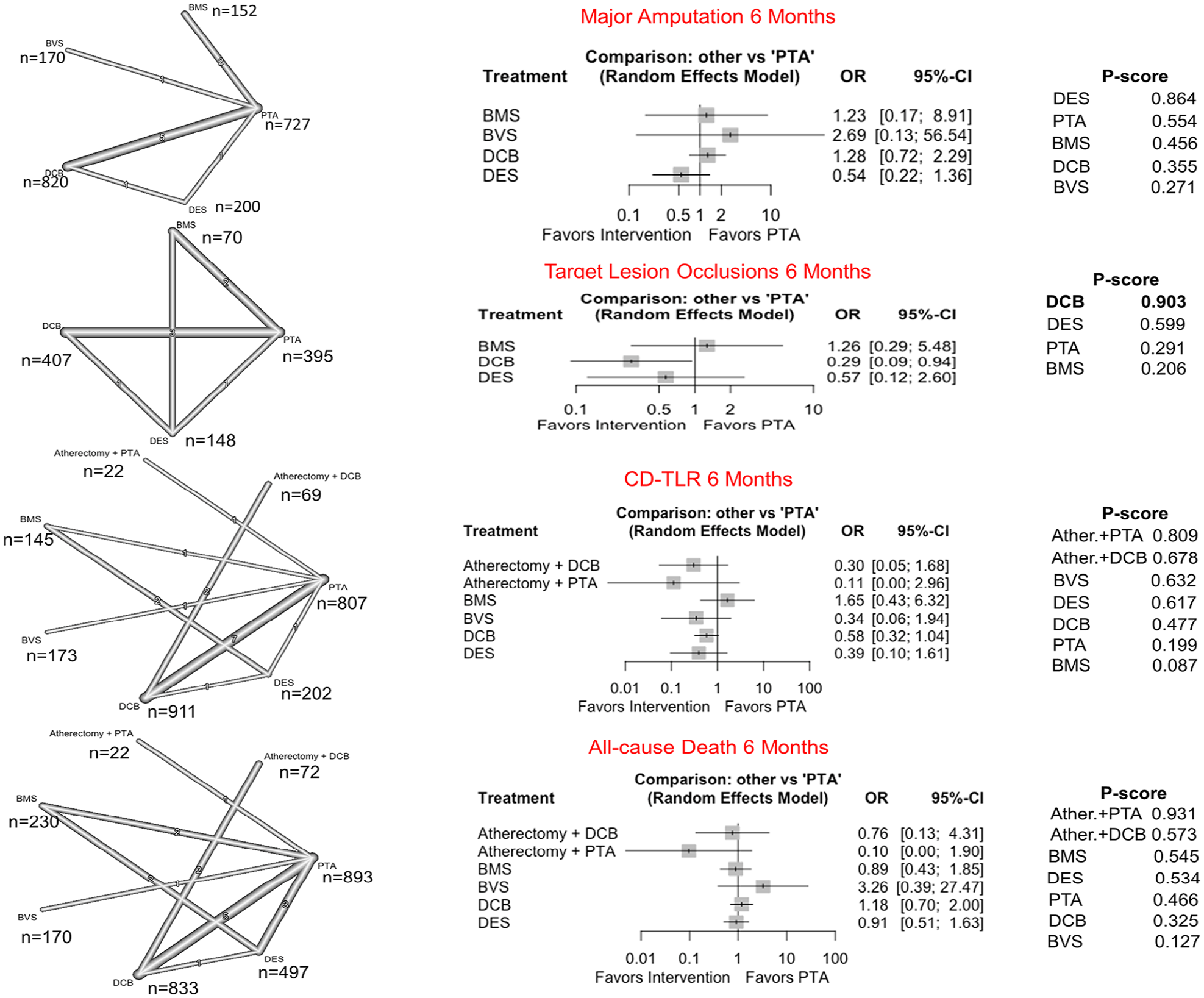
Network diagrams, forest plots, and P-scores for secondary outcomes at 6 months.
Secondary Outcomes at 12 months
Compared with other interventions, BVS was more likely to offer a greater benefit for freedom from the primary composite of major amputation, target lesion occlusion, and CD-TLR (0.720) (Figure 4). Atherectomy with DCB was more likely to be the best option to improve primary patency (0.941) and had a significant treatment effect compared with PTA (OR, 7.13; 95% CI, 1.05–48.44). Based on P-scores, at 12 months, DES was ranked first for reducing major amputations (0.895) and DCB for reducing target lesion occlusions (0.734). Atherectomy with PTA was ranked first, and DCB second (0.724 and 0.688, respectively) in reducing CD-TLR, although only DCB had a significant treatment effect compared with PTA (OR, 0.47; 95% CI, 0.28–0.79) (Figure 4).
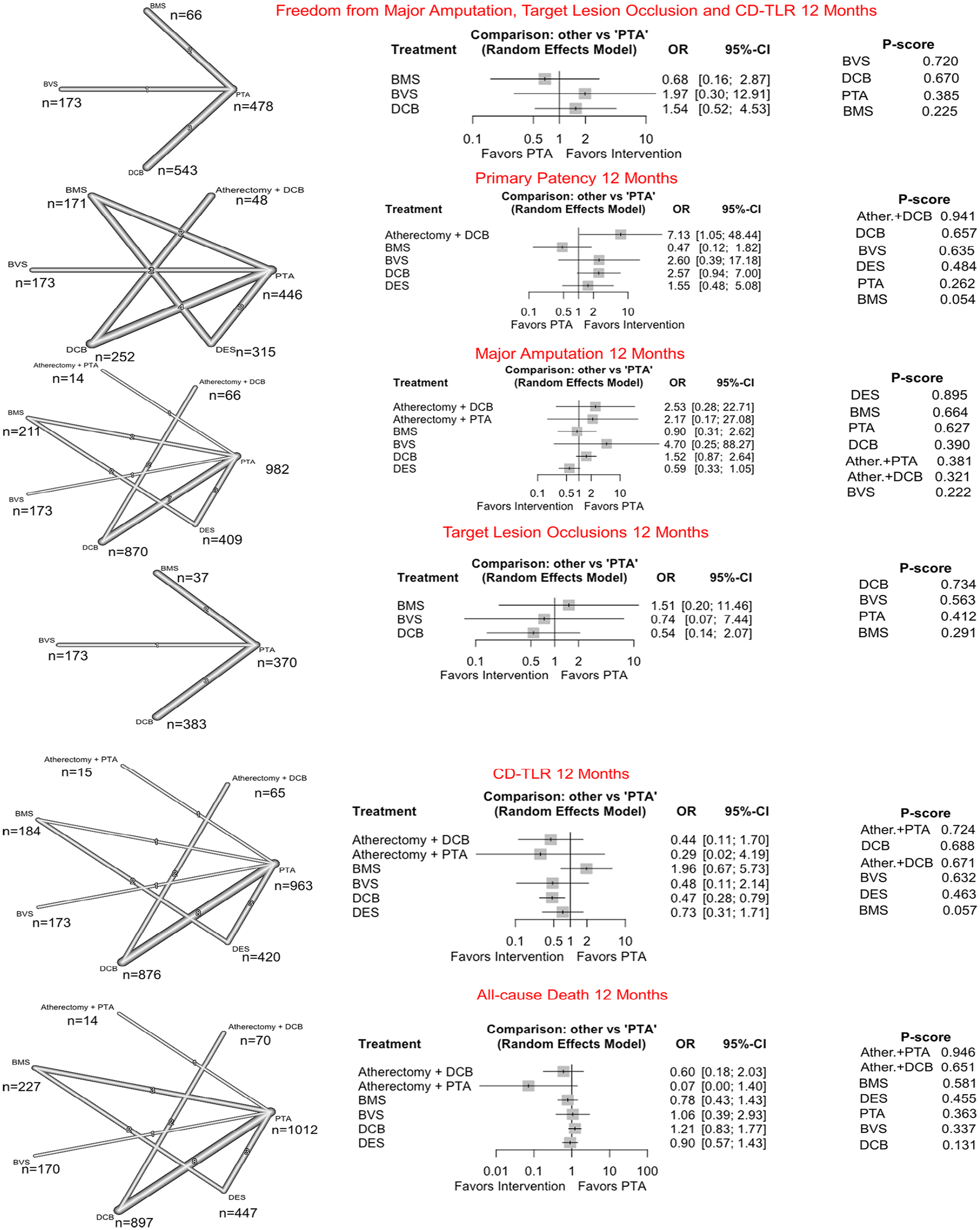
Network diagrams, forest plots, and P-scores for secondary outcomes at 12 months.
There was no evidence of inconsistency between direct and indirect estimates for all outcomes, as determined by node-splitting methods (Supplemental Figures 2, 4, and 6). Publication bias was low for all outcomes at all time points (Supplemental Figures 3, 5, and 7).
Sensitivity Analyses
To evaluate the potential impact of excluding Amphirion DCB (withdrawn from the market due to safety concerns)19,29,31 and SAVAL DES (the only self-expanding DES, 34 which did not meet efficacy end point) we conducted sensitivity analyses, as appropriate. Excluding studies on the IN.PACT Amphirion DCB and SAVAL DES resulted in significant treatment effects, with BVS (OR, 1.97; 95% CI, 1.04–3.75) improving freedom from the primary composite of major amputation, target lesion occlusion, and CD-TLR at 12 months, and DCB (OR, 0.42; 95% CI, 0.19–0.90) and atherectomy with DCB (OR, 0.13; 95% CI, 0.02–0.82) demonstrating reduced CD-TLR at 6 months (Figure 5 and Supplemental Figures 8 and 9).
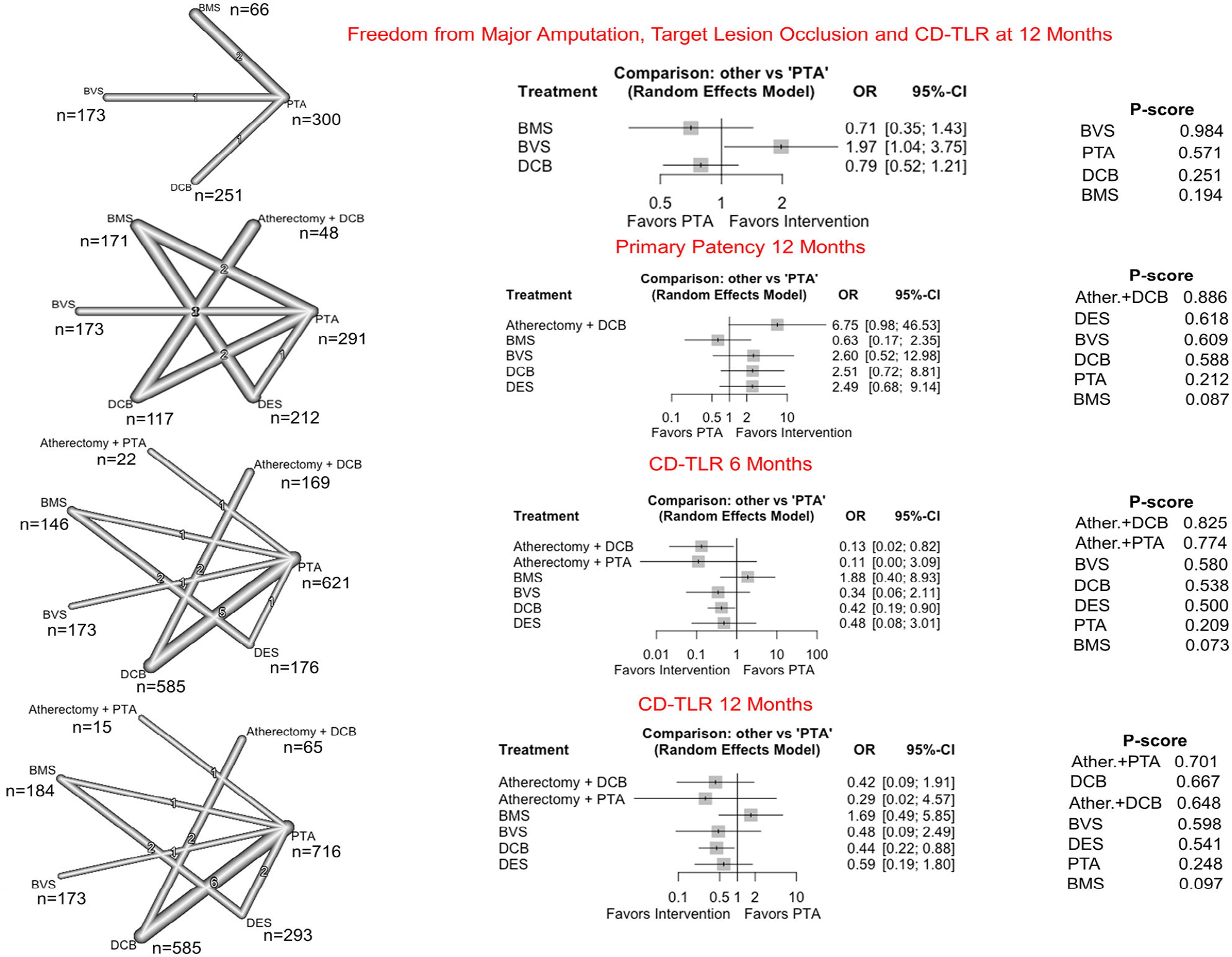
Network diagrams, forest plots, and P-scores for sensitivity analyses by removing studies reporting outcomes for Amphirion DCB and SAVAL DES.
Meta-Regression Analysis
Meta-regression analysis for 12-month outcomes was conducted using baseline patients characteristics [age, male sex, diabetes, chronic kidney disease, smoking status, Rutherford category 5 or 6 (tissue loss), Rutherford category 4 (ischemic pain)] and lesion characteristics (lesion length and chronic total occlusions) (Table 2). Chronic kidney disease was associated with an 8-fold increase in CD-TLR (p = 0.049) and almost 36-fold increase in risk of major amputation (p = 0.017). Longer lesion length was associated with a 34% increase in CD-TLR (p = 0.003), and a 35% decrease in primary patency (p = 0.003). Chronic total occlusion may increase CD-TLR up to 3 times (p = 0.061).
Meta-Regression Analysis for 12-month Outcomes.
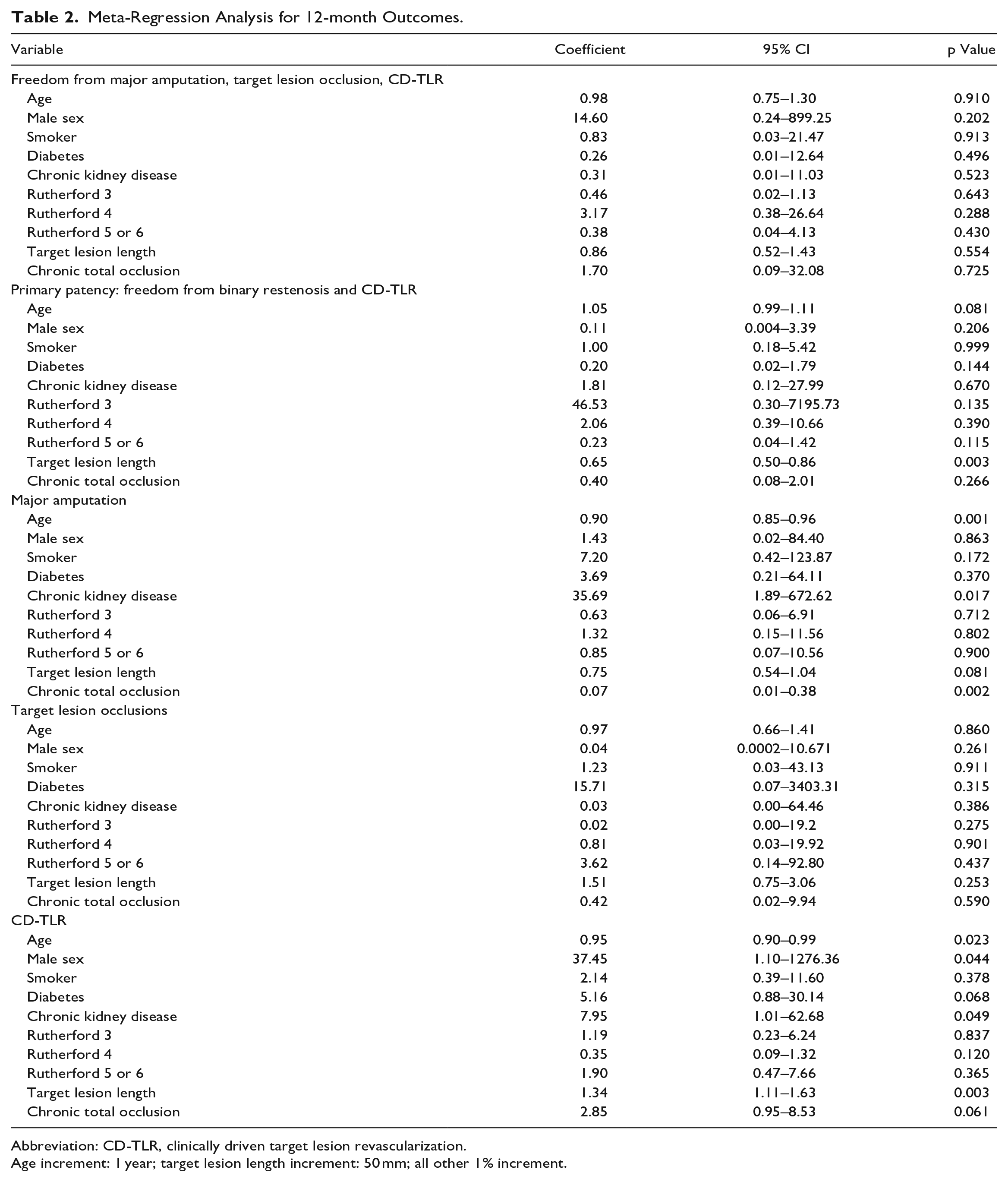
Abbreviation: CD-TLR, clinically driven target lesion revascularization.
Age increment: 1 year; target lesion length increment: 50 mm; all other 1% increment.
Discussion
This study-level network meta-analysis is the largest RCT-based meta-analysis of BTK artery interventions, including evidence from 23 RCTs with a total of 3091 patients. Almost 85% of these patients were included in studies evaluating 4 major treatment modalities: conventional PTA, DCB, DES, and BMS; 8% were included in 1 study evaluating BVS versus PTA; and 6% were included in 3 studies assessing atherectomy with DCB or PTA.
This network meta-analysis shows no significant differences in 30-day MAEs between the treatment modalities compared with PTA, suggesting that all interventions are of similar safety. At 6 months, our results indicate that DCB, atherectomy with DCB, and DES were more likely to be better options for primary efficacy end points and produced the largest benefit (Table 3). Compared with PTA, DCB improved freedom from composite of major amputation, target lesion occlusion, and CD-TLR 3.7-fold, and reduced target lesion occlusion by 71%. At the same time atherectomy with DCB and DES improved primary patency by 7.5- and 5.5-fold and atherectomy with DCB reduced CD-TLR by 87%. At 12 months, the benefit of atherectomy with DCB was sustained for primary patency, BVS was ranked as the first treatment modality for freedom from composite, and DCB reduced CD-TLR by 53% (Table 3). There was no benefit of BMS compared with PTA at any timepoint. There were no differences in all-cause death between treatment modalities at 6 or 12 months after the procedure. Meta-regression analysis suggests that chronic kidney disease, longer lesion length, and chronic total occlusion still predict worse outcomes at 1 year after intervention (Table 2). While RCTs lack intentional patient selection, meta-regression may offer insights for risk stratification, though its role in guiding personalized vascular therapy remains exploratory.
Interventions Ranking for Primary and Secondary Efficacy Outcomes.
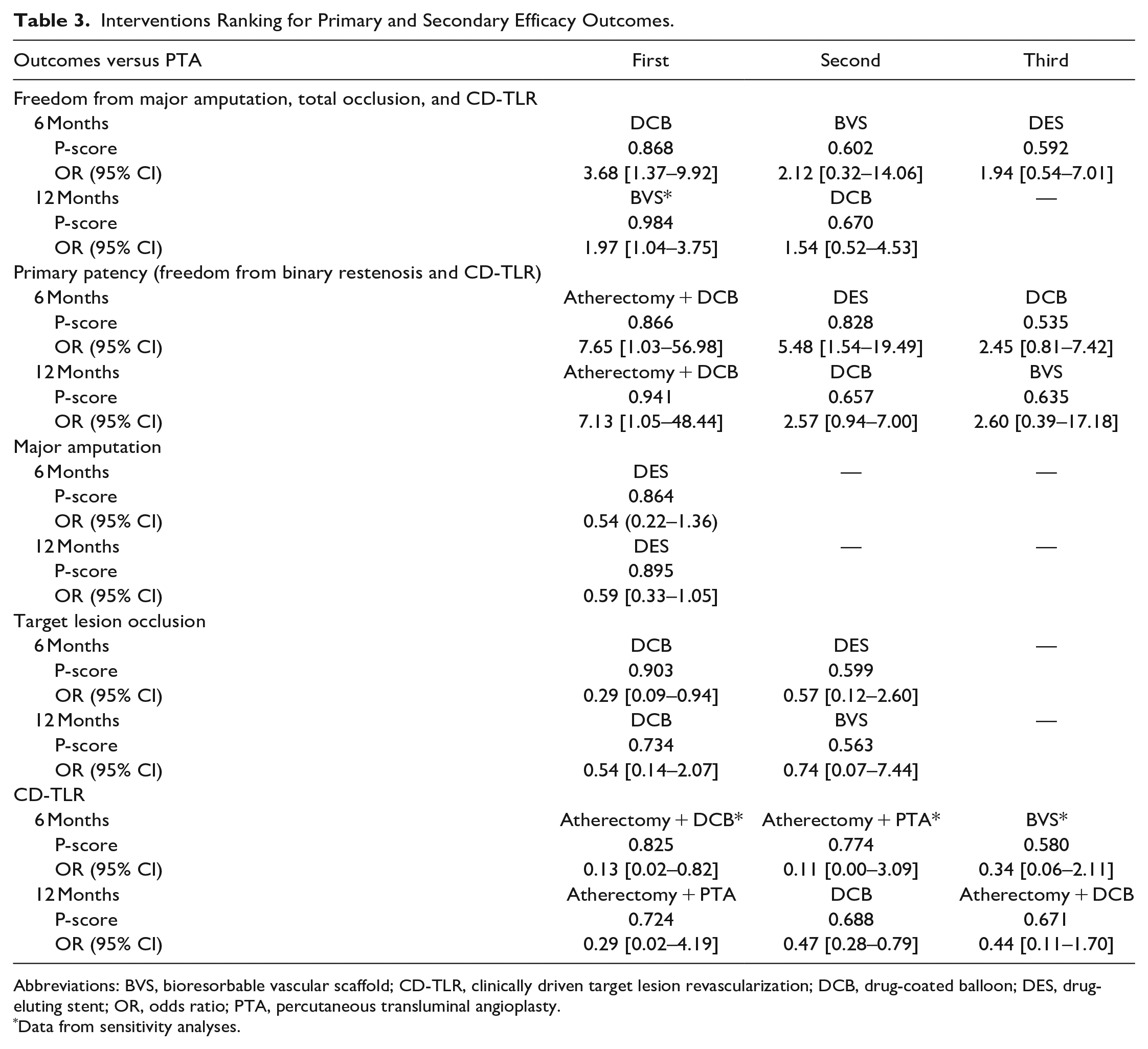
Abbreviations: BVS, bioresorbable vascular scaffold; CD-TLR, clinically driven target lesion revascularization; DCB, drug-coated balloon; DES, drug-eluting stent; OR, odds ratio; PTA, percutaneous transluminal angioplasty.
Data from sensitivity analyses.
Infrapopliteal artery disease presents distinctive histopathological characteristics that make endovascular interventions technically challenging. Unlike coronary lesions, infrapopliteal lesions tend to be long and diffuse, severely calcified, and involve chronic total occlusions. Both intimal and medial calcifications are very common, with the most severe calcifications leading to a higher prevalence of bone formation. 36 Comorbidities such as diabetes mellitus and chronic kidney disease exacerbate the severity of vascular calcifications in CLTI patients.36,37
In contemporary clinical practice, conventional PTA with plain balloons remains the standard endovascular modality for BTK revascularization; however, barotrauma to the vessel wall, elastic recoil, and flow-limiting dissections result in aggressive intimal hyperplasia and restenosis, leaving stand-alone PTA a suboptimal approach.38,39 While BMS offers the mechanical support needed to address dissections and acute recoil, restenosis rates remain high. 39 Consequently, BMS have been reserved for bail-out indications to prevent acute vessel closure after suboptimal PTA. 40 Nevertheless, as confirmed in our meta-analysis, the results with BMS are disappointing and provide no apparent advantage over PTA alone. Drug-eluting devices such as DES, DCB, and BVS provide targeted drug release that prevents intimal hyperplasia and reduces the risk for re-occlusion. 41
Most of the DES investigated in BTK interventions were balloon-expandable DES originally designed for coronary interventions—mostly sirolimus/everolimus DES (Table 1). Superior outcomes of coronary DES in BTK lesions have been reported in 3 major RCTs (ACHILLES, 26 YUKON BTK, 25 and DESTINY 13 ). A meta-analysis of 9 RCTs demonstrated increased primary patency with DES up to 2-year follow-up and no differences in major amputation and all-cause mortality rates compared with PTA or BMS. 42 Moreover, a meta-analysis evaluating PTA, BMS, DCB, and DES in BTK lesions showed a significantly better 12-month primary patency with DES (83.6%; 95 CI%, 78.4–88.8) among the other interventions and no difference in major amputation rates 43 ; however, the primary patency benefit of DES is blunted in longer lesion lengths, and major amputation rates are primarily determined by the proportion of CLTI patients rather than the type of intervention. 43 In our network meta-analysis, DES showed larger benefit for primary patency at 6 months but not at 12 months. As our analysis included the SAVAL DES, a self-expanding paclitaxel-eluting stent designed for BTK interventions that did not meet the primary efficacy end point of 12-month primary patency (68% DES vs 71% PTA), 34 we assessed whether the exclusion of the SAVAL study improves the 12-month primary patency benefit demonstrated previously with balloon-expandable DES. In the sensitivity analysis, the exclusion of the SAVAL study increased the overall benefit of DES for 12-month primary patency (P score: 0.618 vs 0.484); however, the treatment effect remained not significant (OR 2.49; 95% CI, 0.68–9.14) (Figure 5). The disparate results of the self-expanding DES in the SAVAL trial compared with traditional coronary balloon-expandable DES highlights the need for distinct device-specific evaluations for BTK interventions and is a reminder that one should never assume a class effect among these devices.
DCB offers clear technical advantages over DES in BTK, particularly in avoiding a metallic scaffold prone to external compression, deformation, and thrombosis and for treatment of longer lesions. In addition, DCB can be used in anatomic flexion points where severe compression can lead to stent fracture and complications prohibiting reintervention.44,45 To date, only RCTs with paclitaxel DCB have provided comparative safety and efficacy outcomes in BTK interventions, and the evidence has been conflicting. The IN.PACT DEEP RCT did not demonstrate superiority of DCB for CD-TLR or late lumen loss at 12 months compared with PTA and raised safety concerns due to a higher amputation rate in the DCB group, 31 although 5-year outcomes did not show a difference in major amputation rates between groups. Consequently, the IN.PACT Amphirion DCB for BTK treatment was withdrawn from the market in 2013. 31 In the BIOLUX P-II, the Passeo-18 LUX paclitaxel DCB had numerically better primary patency compared with PTA, but major amputation at 6 months were comparable to those with PTA. 32 The Lutonix BTK pivotal trial demonstrated improved freedom from major amputation, target lesion occlusion, and CD-TLR at 6 months for DCB versus PTA (74.5% vs 63.5%; p = 0.02) 20 ; however, the benefit was not sustained at 12 months or beyond. The Lutonix DCB was not granted FDA approval for BTK indication due to insufficient evidence of efficacy and benefit. 46 Nonetheless, striking favorable outcomes were reported in the DEBATE-BTK trial, where the IN.PACT Amphirion DCB reduced restenosis, CD-TLR, and target vessel occlusion rates at 1 year compared with PTA in a diabetic population. 19 Similarly, in the AcoArt II-BTK and the ACOART-BTK trials, DCB demonstrated better efficacy outcomes compared with PTA.17,18 A meta-analysis published in 2020 including 3 RCTs (IN.PACT DEEP, BIOLUX P-II, Haddad 2017) and a retrospective study found no significant difference in TLR rates between paclitaxel DCB and standard PTA at 12 months. 47 With 8 RCTs included in our network meta-analysis, paclitaxel DCB did not show a reduction in CD-TLR at 6 weeks, but it had a significant treatment effect at 12 months, although it was ranked second after atherectomy with PTA. In the IDEAS RCT, the only RCT comparing DES versus paclitaxel DCB in long lesions, there were no significant differences between groups regarding lesion re-occlusions, CD-TLR, or amputation rates, although the restenosis rate was lower in the DES group. 29 Given the safety concerns that led to the withdrawal of the In.PACT Amphirion DCB from the market, we investigated whether its exclusion would improve DCB outcomes. Notably, by excluding the IN.PACT DEEP RCT, DEBATE-BTK trial, and IDEAS RCT, we found that DCB demonstrated significantly reduced CD-TLR compared with PTA (Figure 5).
Network meta-analyses have the advantage of combining the direct and indirect evidence from different head-to-head comparisons into a single unified analysis. Prior network meta-analyses support better efficacy outcomes with DES and DCB compared with PTA.48 –51 A recent network meta-analysis including 11 studies and 1330 patients showed that both DCB and DES improved primary patency at 12 months. Based on the SUCRA score, DCB was considered the best treatment for primary patency and TLR and DES for major amputation. 51 Our analysis at 12 months showed DES as the treatment modality most likely to produce the largest benefit in reducing major amputations, while DCB was the only treatment that significantly reduced CD-TLR compared with PTA, although it was ranked second after atherectomy with PTA.
The only BVS investigated in BTK intervention is the Esprit BTK, an everolimus-eluting resorbable scaffold. Esprit BTK scaffold is the only US FDA-approved option for patients with CLTI and infrapopliteal artery disease. In the LIFE BTK RCT, BVS was superior to PTA for the primary efficacy end point defined as freedom from major amputation, occlusion of the target vessel, CD-TLR, and binary restenosis of the target lesion at 1 year (74% vs 44%). 33 In our network meta-analysis, BVS was the best treatment modality for the efficacy composite of freedom from major amputation, target lesion occlusion, and CD-TLR at 12 months (Table 3). Further data are needed to provide statistical evidence regarding treatment effect for other end points when compared with the other treatment modalities in the network.
Adjunctive atherectomy may debulk intimal and medial calcification, improve vascular remodeling, and allow a more effective drug delivery into the arterial wall 37 ; however, a few studies have assessed the efficacy of atherectomy in a randomized fashion. Our data suggest that adjunctive use of atherectomy with PTA or DCB is safe and primary patency and CD-TLR rates are improved compared with PTA. A prior network meta-analysis found that atherectomy with PTA or DCB was the best treatment to reduce TLR and improve primary patency, based solely on the SUCRA scores. 48 In our updated analysis, we showed that atherectomy with DCB had the largest benefit and significant treatment effect for primary patency at both 6 and 12 months, and atherectomy with PTA was the best treatment to reduce CD-TLR, but the treatment effects were not statistically significant. Our findings suggest that atherectomy combined with PTA/DCB holds a great potential to improve the efficacy of endovascular treatment for BTK lesion. Further RCTs are necessary to yield statistical significance.
Comparative data on the impact of different treatment modalities on QoL measures and cost-effectiveness remain limited. Three studies—SINGA-PACLI, 52 Lutonix BTK, 20 and BIOLUX P-II 32 —used the EQ-5D (EuroQol 5 Dimensions) self-reported questionnaire to evaluate QoL differences between DCB and PTA at 6 or 12 months postprocedure. No significant differences between DCB and PTA were reported. Similarly, the SAVAL study found no differences in EQ-5D improvement between DES and PTA. 34 However, the Vascular Quality of Life Questionnaire-6, a disease-specific QoL measure for CLTI patients, showed significant improvement across all domains at all time points in the DES group, while the PTA group demonstrated improvements in all domains except the social domain. 34 Additionally, Rastan et al. 24 found that the Walking Impairment Questionnaire showed no significant differences between atherectomy + DCB and DCB alone, either at baseline or during follow-up. 24 DCB in the SINGLA-PACLI trial was not cost-effective compared to PTA from both societal and health sector perspectives, although the study was not powered for a cost-effectiveness endpoint. 52 In the LIFE BTK RCT, the BVS achieved a 64% probability of cost-effectiveness at a US$10,000 willingness-to-pay threshold compared to PTA. 53 The cost-effectiveness of BVS is attributed to its benefit in delaying the need for repeat revascularization.
Important advances are ongoing to overcome the technical challenges and improve outcomes in the treatment of infrapopliteal artery disease. Recent advances in DCB technology for BTK treatment offer promise. Therapeutic success of DCB relies on several factors including type of drug, dosage, excipient, coating, pharmacokinetic profile, transfer efficiency, and tissue retention. Paclitaxel has been the drug of choice for DCB due to its strong lipophilic characteristics and propensity for retention in the vessel wall; however, the majority of paclitaxel delivered via DCB (~80%) does not reach the target site; ~16% is retained on the balloon, with estimates that as little as 3% to 5% is transferred into the vessel.54,55 In most cases, the concentration of paclitaxel in the tissue after 28 days is below the therapeutic effect (1 µg/g) (Supplemental Table 3). Sirolimus is an alternative to paclitaxel DCB with a “safer” profile, but it is less lipophilic; therefore, it is poorly retained into the tissue. New balloon coating technologies have emerged to increase the transfer and tissue retention of sirolimus with sustained therapeutic levels in arterial tissue compared with paclitaxel (Supplemental Table 3).
Limitations
This study has some limitations. First, this network meta-analysis inherits the limitations of a study-level analysis, including variations in inclusion criteria, baseline characteristics, end point definitions, and use of different eluting devices or drugs. Additionally, the potential retrieval of individual patient data from the included RCTs could have provided more granular insights into outcomes but was not considered at this time. Second, with only a few RCTs investigating atherectomy, the atherectomy with DCB includes both orbital atherectomy and directional atherectomy, while atherectomy with PTA includes only orbital atherectomy. Third, although our analysis was intended to include cutting balloons, scoring balloons, lithotripsy, and Tack devices, they were investigated in single-arm studies with no comparator arm; therefore, they were excluded from the analysis.
Conclusion
This network meta-analysis of endovascular treatment modalities for BTK arterial disease provides evidence that local antiproliferative drug delivery, whether by balloon-expandable DES or BVS or paclitaxel-coated DCB, is necessary to improve patency and efficacy outcomes. Furthermore, combining atherectomy with drug delivery shows promising potential. Emerging endovascular targeted drug delivery therapies with limus-based DCB or scaffolds promise to provide greater drug transfer efficiency and a more effective therapeutic alternative that overcomes the limitations of metallic stents in one of the most challenging vascular beds.
Supplemental Material
sj-pdf-1-jet-10.1177_15266028251344809 – Supplemental material for Safety and Efficacy of Endovascular Treatment Modalities for Below-the-Knee Arterial Disease: A Systematic Review and Network Meta-analysis
Supplemental material, sj-pdf-1-jet-10.1177_15266028251344809 for Safety and Efficacy of Endovascular Treatment Modalities for Below-the-Knee Arterial Disease: A Systematic Review and Network Meta-analysis by Daniela Tirziu, Amr Saleh, Haocheng Huang, Narjes Akhlaghi, Thomas J. Breen, Sahil A. Parikh, Kenneth Rosenfield, Ehrin J. Armstrong, Patrick J. Geraghty, Marianne Brodmann, George L. Adams, Daniel Snyder, Robert S. Zilinyi, S. Elissa Altin, Helen Parise and Alexandra J. Lansky in Journal of Endovascular Therapy
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Daniela Tirziu: None. Amr Saleh: None. Haocheng Huang: None. Narjes Akhlaghi: None. Thomas Breen: None. Sahil A. Parikh: Institutional Research Support: Abbott Vascular, Acotec, Boston Scientific, Concept Medical, MedAlliance, Reflow Medical, Surmodics, Shockwave Medical, TriReme Medical, and Veryan Medical; Advisory Board: Abbott Vascular, Boston Scientific, Cordis, Medtronic and Philips; Consulting: Canon, BD Bard, Inari, Penumbra, R3 and Terumo; Equity: Advanced NanoTherapies, Encompass Vascular, and eFemoral. Kenneth Rosenfield is a consultant/scientific advisory board member for Althea Medical, Angiodynamics, Boston Scientific, Contego, InspireMD, Magneto, Mayo Clinic, Neptune Medical, Philips, Summa Therapeutics, Surmodics, Thrombolex, Terumo, and Truvic; reports institutional grants from National Institutes of Health and Boston Scientific; reports equity in Accolade, Access Vascular, Aerami, Althea Medical, Contego, Cruzar Systems, Embolitech, Endospan, InspireMD, JanaCare, Magneto, Orchestra, PQ Bypass, Prosomnus, Shockwave, Summa Therapeutics, Thrombolex, Truvic, and Valcare; and is a board member for National PERT Consortium, a not-for-profit 501(c) (3) organization dedicated to advancing treatment and improving outcomes in pulmonary embolism. Ehrin Armstrong: Consultant: Abbott Vascular, Boston Scientific, Endologix, MedAlliance, Medtronic, Philips, Shockwave Medical. Patrick J. Geraghty: Equity—MedAlliance SA, Aveera, Protexa, Pulse Therapeutics. Marianne Brodmann: Consulting for Medtronic, Philipps, Biotronik, Boston Scientific, BD Bard, Shockwave. George L. Adams: CMO: Cordis; Consultant: CSI, Philips, Abbott, Shockwave, Cook. Daniel Snyder: None. Robert S. Zilinyi: None. S. Elissa Altin: None. Helen Parise: Consulting fees—Intact Vascular, Inc. (now Philips Image Guided Therapy), TriReme Medical LLC, and Veryan Medical Ltd. Alexandra J. Lansky: Consulting fees MedAlliance.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.