
Abstract
Objective:
Physician-modified endografts (PMEGs) have provided an endovascular approach for repair of complex abdominal aortic aneurysms and thoracoabdominal aortic aneurysms. While the use of polyethylene terephthalate (Dacron)-based grafts is growing, we aimed to evaluate the use and outcomes of a polytetrafluoroethylene (PTFE)-based system for such cases.
Materials and Methods:
In a retrospective, single-center cohort study from November 2021 to June 2024, treatment with physician-modified PTFE endograft for complex abdominal aortic aneurysms and thoracoabdominal aortic aneurysms was assessed. Stent modification and deployment was described and illustrated. Patient demographics, procedural details, and postoperative outcomes were collected and analyzed. Major adverse events, 30-day mortality, reintervention, endoleak, and aortic related mortality were analyzed in this cohort.
Results:
Twenty-nine patients who received physician modified PTFE endograft were included in this study. Of these patients, 25 had urgent or emergent indication for intervention. Of the grafts modified, 83% were conformable thoracic stent graft devices and 17% were excluders. Endoleaks were observed in 24.1% of patients postoperatively; 1 patient had a type 1C endoleak and 6 patients had type 2 endoleak. Reinterventions were necessary in 3 patients. The 30-day survival observed in this study was 96.6% and freedom from total aortic related mortality was 93.1%.
Conclusions:
PTFE-PMEG can be employed with limited risk of endoleak and aortic related mortality. Further study involving long-term follow up and prospective data is necessary.
Clinical Impact
PMEGs are increasingly utilized for patients unfit for open repair of complex abdominal aortic aneurysms and thoracoabdominal aortic aneurysms. Our study provides evidence in support of PMEGs for primarily medically urgent cases of this nature. We report limited complications, including endoleak or aortic related mortality, with a median follow up of over 7 months. While most of the current literature explores the use of Dacron-based grafts for PMEG, our study explores the use of PTFE-PMEG, which provides ease of manipulation and implantation. This technique can be employed with promising outcomes and necessitates further study by other vascular surgeons.
Introduction
Adoption of fenestrated and branched physician-modified endografts (PMEGs) has allowed for advancement in the care of patients medically unfit for open repair of complex abdominal aortic aneurysms and thoracoabdominal aortic aneurysms by providing an endovascular platform for patient-specific aneurysm repair. Recent data published demonstrates that PMEG is a safe and effective treatment option for elective, symptomatic, and ruptured complex aortic aneurysms. 1 Notably, almost all the grafts modified in this international multicenter study were Dacron-based grafts based on the Cook or Medtronic platform.
Since the release of GORE® EXCLUDER® thoracoabdominal branch endoprosthesis (TAMBE) in 2024, the first off-the-shelf device in the United States, surgeons now have the option to repair elective and emergent thoracoabdominal aneurysms or high-risk pararenal aneurysms. 2 Unfortunately, due to its off-the-shelf nature, there are individuals for whom the TAMBE device is unsuitable due to anatomic constraints. These patients still require a PMEG repair as custom-made devices from industry are still being studied and have not yet been disseminated within the United States.
While there are many described techniques for graft modification, most of the literature describes the modification of Dacron-based grafts made of polyethylene terephthalate. 3 The primary reason for this is the ease of modification and the belief that there will be increased fenestration stability due to heat sealing of the Dacron. 4 However, we believe modifying a polytetrafluoroethylene (PTFE)-based system gives a predictable diameter and easier graft manipulation and rotation within the aorta, allowing for ease with implantation. As the nitinol stents are laminated in PTFE, there is naturally a smooth interaction between the aortic wall and graft in our experience compared to grafts in which the nitinol stents interact directly with the aortic wall. This is beneficial, particularly in small true lumens in dissection thoracoabdominal aneurysms, where one must rotate the graft to cannulate vessels at variable clock positions. This article aims to describe a method for modifying a PTFE-based system and its outcomes, highlighting a need for device selection based on aneurysm morphology.
Materials and Methods
Identification of Patients and Outcomes
Our single-center retrospective analysis included 29 patients who received intervention between 2021 and 2024. The University of Maryland PMEG registry was queried for grafts constructed from PTFE. These grafts were all produced by W.L. Gore & Associates (Flagstaff, AZ, USA) and primarily included the Gore® TAG® conformable thoracic stent graft (CTAG). Patient demographics (age, gender), disease morphology (aneurysm, dissection), and indication for repair were extracted from the medical record. Urgent indication included dissection, rupture, saccular, symptomatic, rapid expansion, type 1 endoleak, type 3 endoleak, suture line aneurysm of previous open repair, and cancer. Past medical history, previous aortic operations, and preoperative medical regimens were examined. Postoperative course, including length of stay, in-hospital complications (myocardial infarction, spinal cord ischemia, access complications, lower extremity ischemia, bowel ischemia, and stroke), aortic-related complications, and re-interventions were recorded. The most recent follow-up and imaging of repair were also identified. This study was reviewed and approved by the institutional review board of the University of Maryland (IRB# HP-00050195).
Statistical Analysis
This was a retrospective study of a single cohort of patients receiving PMEG intervention. Descriptive statistics were performed using Excel. Counts with percentages were used for categorical data and medians with interquartile ranges were used for continuous data.
Graft Modification
The back table modification for Gore® TAG® CTAG device begins with careful centerline measurements with 3D reconstruction software (TeraRecon, Inc., Durham, NC, USA) and planning based on the individual’s preoperative computed tomography angiogram (CTA). Based upon these measurements, length from the top of the fabric and clockface measurements are taken to plan the locations of the visceral fenestrations or branches.
Steps of Modification
Steps of modification are explained in Figure 1.
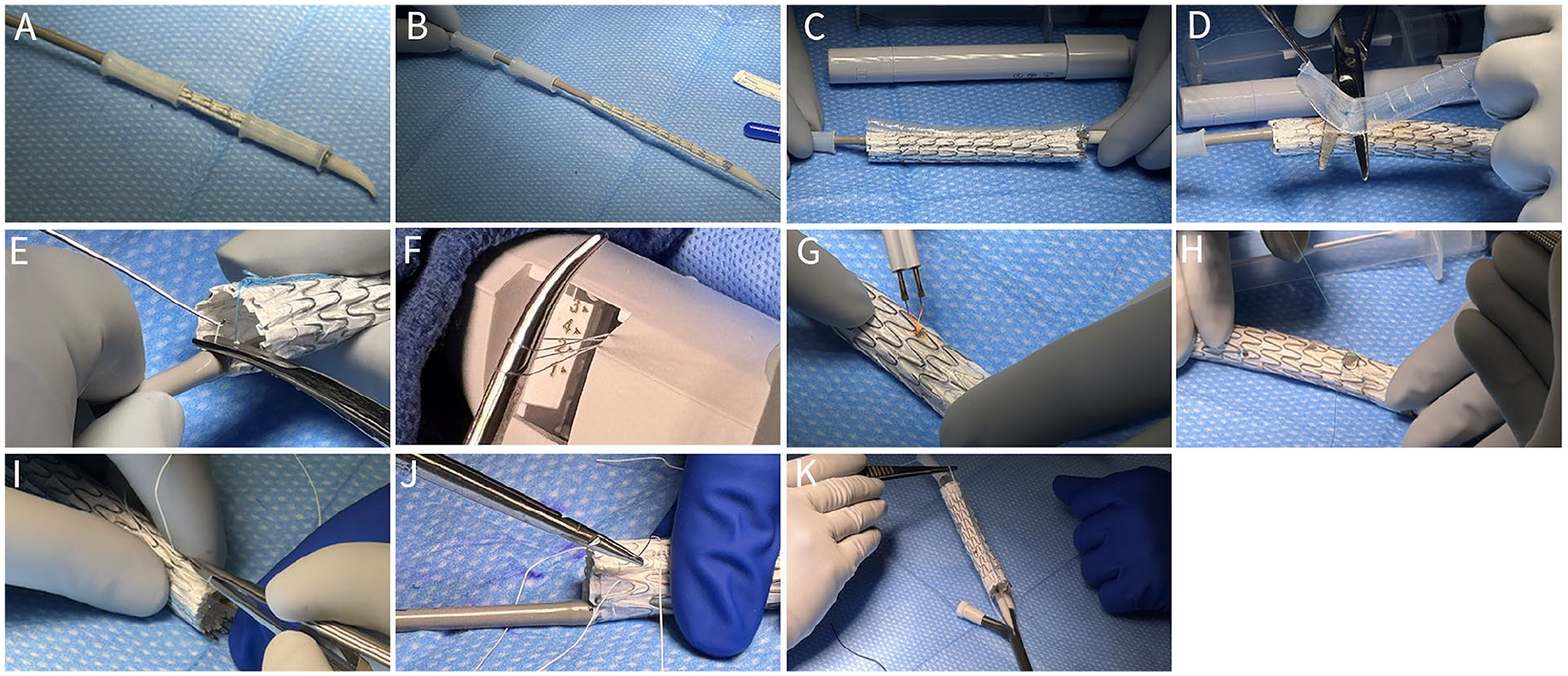
Modification of stent graft. (A) Graft is removed from sterile packaging. (B) Plastic tubes are pulled proximally onto the delivery catheter. (C) Graft is deployed to 50% nominal diameter by deploying the first knob, which unlaces the primary sleeve. (D) Primary sleeve is removed and discarded. (E) Active control fibers are grasped and cut. (F) Deployment line access hatch is opened, and active control fibers from position 4 are extracted. (G and H) Based on the preoperative measurements, fenestrations are created and supported either with a looped snare wire or a 2.5 cm GORE® VIABAHN® self-expanding stent sewn around the fenestration. (I and J) Gortex suture purse-string is placed around the proximal and distal aspect of the graft incorporating the secondary sleeve to facilitate re-sheathing. (K) Peel-away sheath is positioned, and the Gortex suture, which was purse-stringed through the top of the graft, is passed through it, allowing a handle to facilitate re-sheathing into the peel-away. Similarly, the purse-string on the distal aspect of the graft is passed through the plastic tubes. This allows easy re-sheathing without unintentional foreshortening or the secondary sleeve being dislodged. Once re-sheathed, Gortex suture is removed.
Graft Implantation
The graft is then implanted percutaneously through a GORE® DRYSEAL Flex Introducer Sheath (Flagstaff, AZ, USA), which is 65 cm long and typically 2 French sizes larger than the recommended sheath size for the modified Gore CTAG device. The device is then advanced into the dry seal sheath and deployed utilizing a pin-and-pull method, retracting the dry seal sheath over the device. The graft is deployed at 50% of its luminal diameter, allowing easy cannulation of target vessels and manipulation of the graft. The caudal portion of the graft is cannulated from contralateral femoral access, and then, using a steerable sheath, the target vessels are cannulated. Once all target vessels have cannulation wires within them, the graft is fully deployed. The visceral vessels are then stented with covered stent-grafts, typically the GORE® VIABAHN® VBX Balloon Expandable Endoprosthesis (Flagstaff, AZ, USA). We then use a suture-based closure device percutaneously. Completion arteriography is performed to ensure all target vessels are patent with no major endoleak. Intraprocedural fluoroscopy images and completion aortogram are demonstrated in Figure 2.
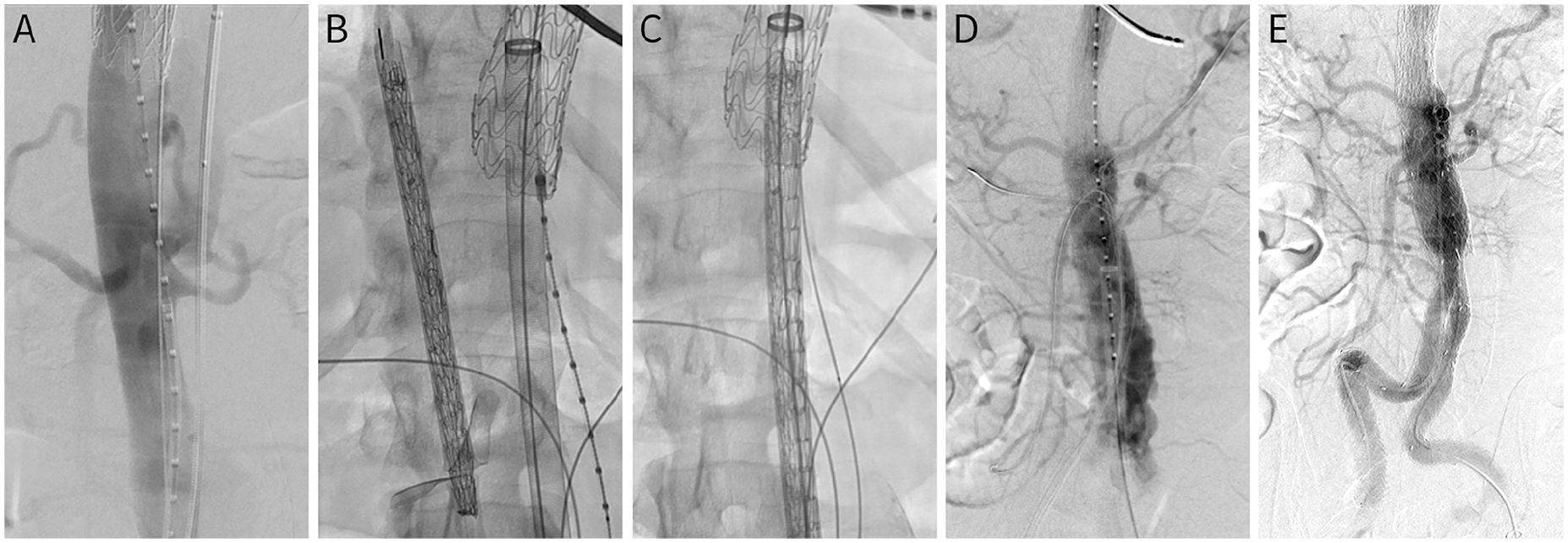
Intraprocedural fluoroscopy of physician-modified endograft. (A) Initial aortogram. (B) Confirmation of device orientation ex vivo. (C) Device alignment within the DrySeal sheath based on renal marking wire. (D) Selective cannulation of visceral vessels. (E) Completion aortogram.
Follow-Up
Patients who underwent urgent implantation due to symptomatic aortic pathology had a CTA performed, ensuring no significant endoleaks requiring secondary intervention before discharge. After discharge, patients were seen and evaluated in our clinic to ensure the access sites were healing as expected. Surveillance imaging was performed at 1-, 3-, and 6-month intervals until stability was noted in the aortic diameter. Patients also underwent concomitant aortic duplexes if body habitus allowed, allowing the transition to ultrasound surveillance.
Results
A total of 29 patients who underwent PMEG were included in this study, 25 of whom had emergency/urgent indications for repair. Patient demographics and comorbidities are listed in Table 1. Most patients were male (72.4%) and white (68.9%), with a median age of 65 years [interquartile range (IQR) 57, 76 years]. Notably, 97% of patients had hypertension. Sixty-two percent of patients had undergone a previous aortic repair. Patients had a median aortic diameter of 58 mm (IQR, 53, 66 mm).
Patient chacteristics and Surgical Indications.
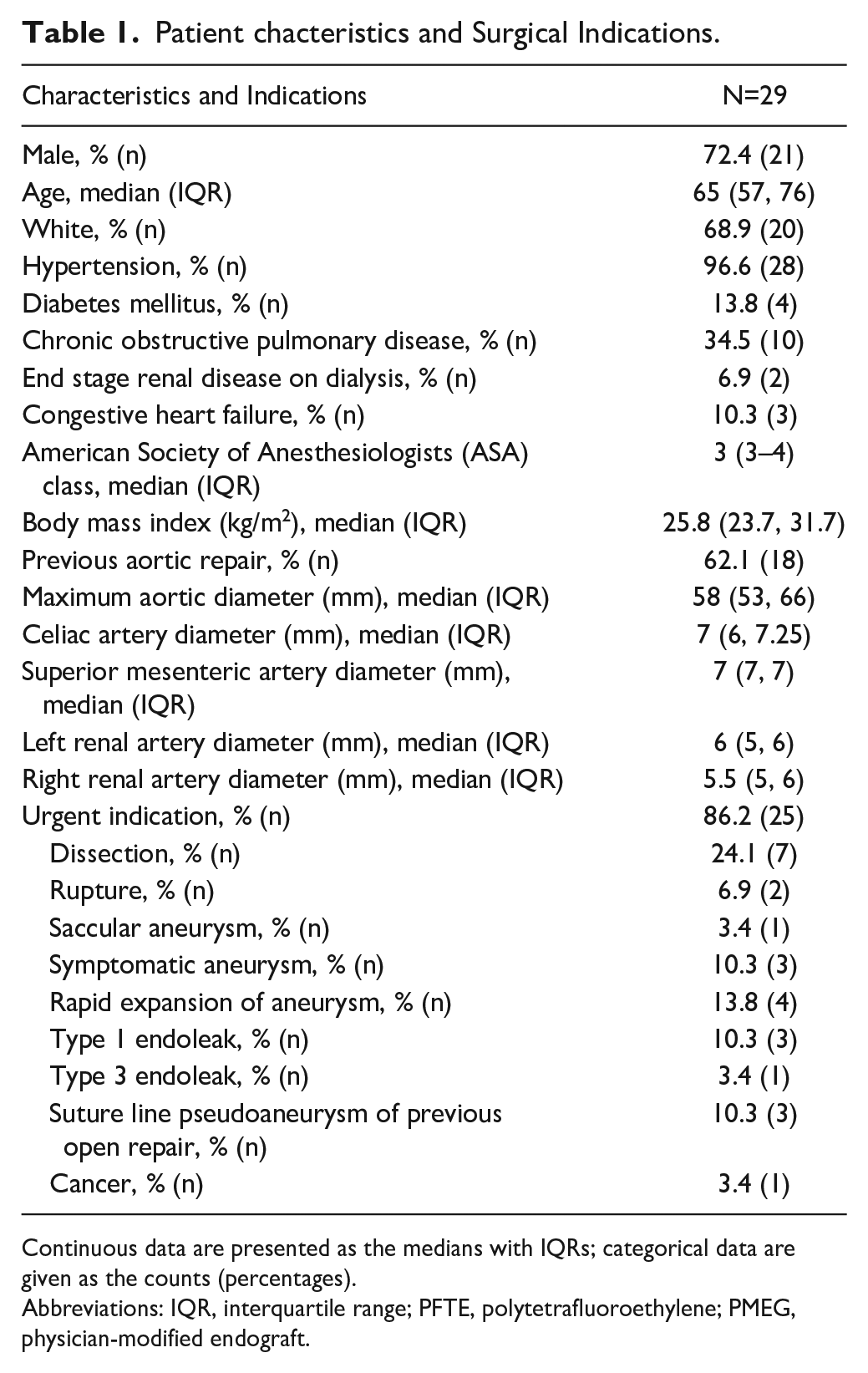
Continuous data are presented as the medians with IQRs; categorical data are given as the counts (percentages).
Abbreviations: IQR, interquartile range; PFTE, polytetrafluoroethylene; PMEG, physician-modified endograft.
Of the grafts modified, 83% were CTAG devices, and 17% were excluders. The median size for the main body was 31 mm (IQR, 28, 34) and median number of fenestrations per graft was 4 (IQR, 3, 4). Intraoperative data showed: 2 patients with upper extremity access, median fluoroscopy time of 104 minutes (IQR, 68, 134), median estimated blood loss of 200 mL (IQR, 150, 312), and 18 patients with use of prophylactic cerebrospinal fluid drain (Table 2).
Procedural Details.
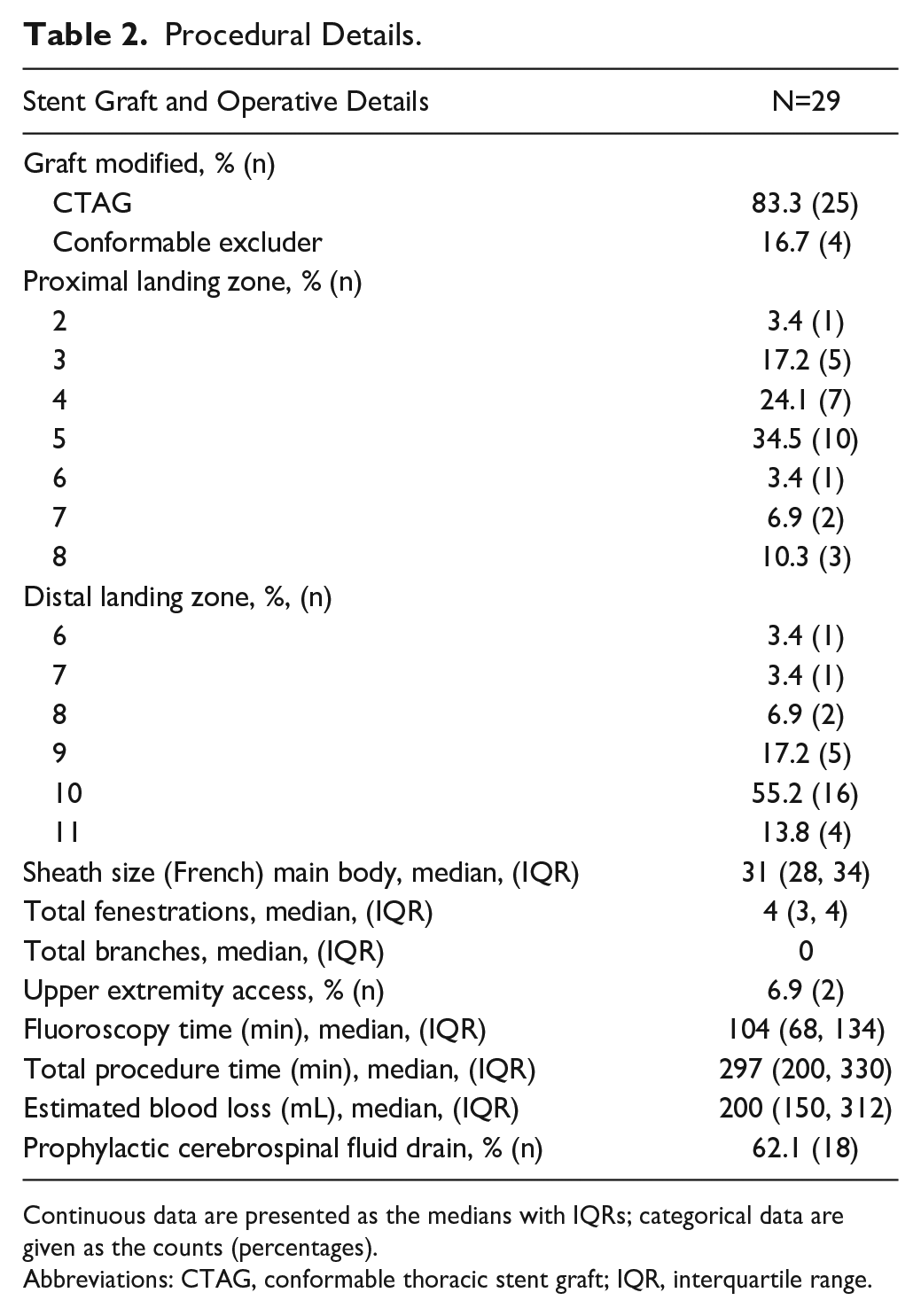
Continuous data are presented as the medians with IQRs; categorical data are given as the counts (percentages).
Abbreviations: CTAG, conformable thoracic stent graft; IQR, interquartile range.
Operative success defined as implantation of the main modified device with accurate deployment of the bridging stents was achieved in 100% of patients. Thirty-day and in-hospital mortality was only 1 patient (3.4%). Endoleaks were observed in 7 patients on postoperative surveillance CTA. One patient had a type 1C endoleak involving the celiac artery, and 6 had type 2 endoleaks. This study did not observe type 1A, 1B, or 3 endoleaks. Only 3 patients required re-intervention, 1 before discharge for a 1C leak treated with the extension of celiac artery bridging stent with no residual leak, and another 4 months postoperatively for a type 2 endoleak via inferior mesenteric artery embolization. Of the 29 patients, 10.3% had access complications.
Additional adverse outcomes included acute kidney injury (1 patient), permanent dialysis (2 patients), and lower extremity ischemia (1 patient). No patients experienced myocardial infarction, venous thromboembolic event, bowel ischemia, stroke, or spinal cord ischemia in this study. Postoperatively, 2 patients were intubated for more than 48 hours, and 2 patients had to return to the operating room. Most patients (86.2%) were discharged to home rather than acute rehabilitation.
Secondary interventions were necessary in 3 patients with a median time to re-intervention of 110 days (IQR, 57, 255 days). Patients had a median follow-up of 223 days postoperatively (IQR, 118, 418 days). Three patients died during follow-up with 2 aortic-related mortalities—1 in a patient who had a palliative procedure for an inoperable mycotic aneurysm nearly 6 months postoperatively, and the other postoperative day 2 after treatment for rupture. Overall, these patients did very well after PTFE-based PMEG, with one of 29 patients suffering a 30-day mortality, one 1C endoleak, and 6 type 2 endoleaks. These patients recovered rapidly and had a median length of stay of only 4 days. The median days to death were 139 (IQR, 70.5, 205.5 days). Two patients were lost to follow-up (Table 3).
Patient Outcomes After PTFE-PMEG.
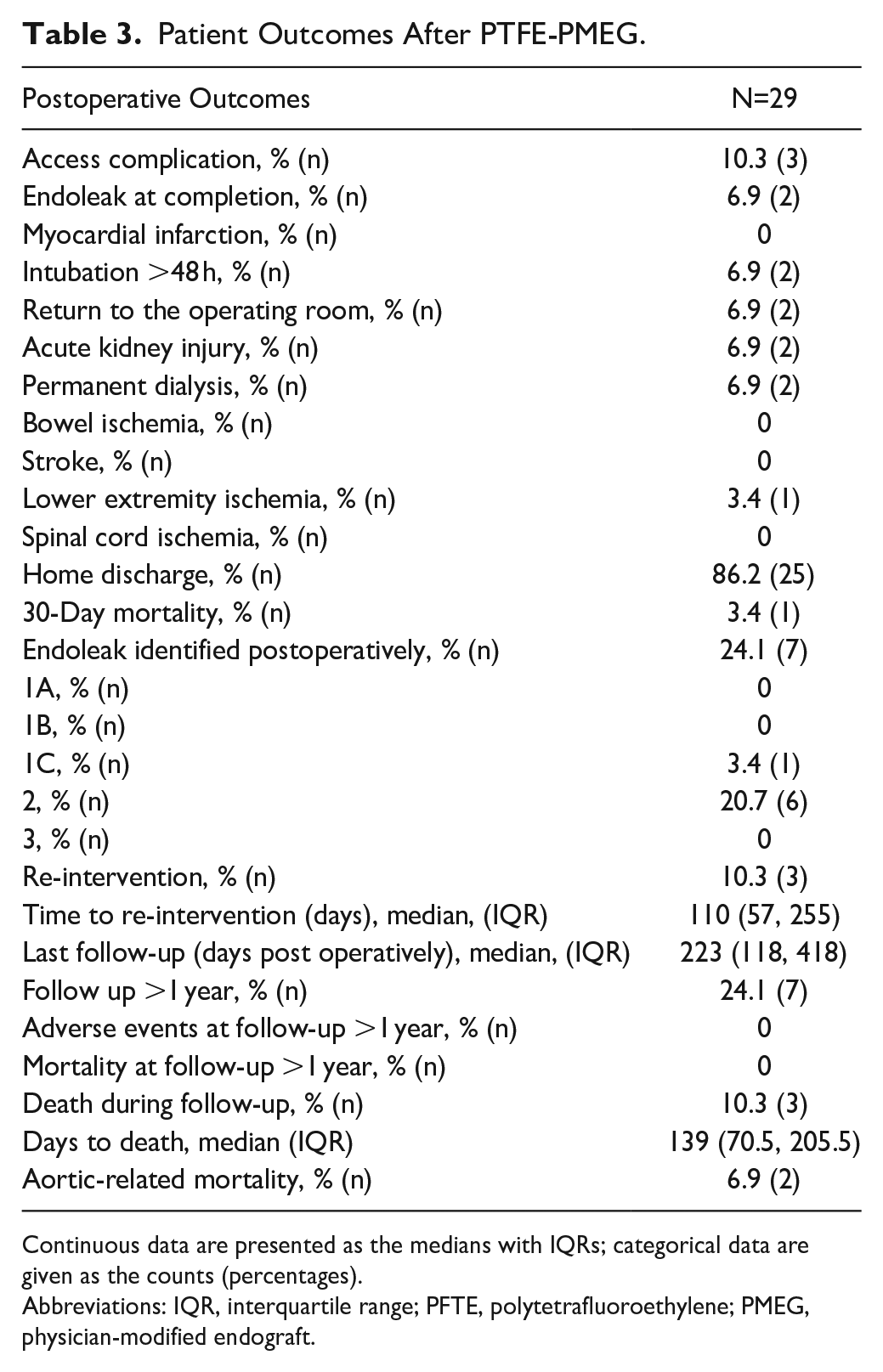
Continuous data are presented as the medians with IQRs; categorical data are given as the counts (percentages).
Abbreviations: IQR, interquartile range; PFTE, polytetrafluoroethylene; PMEG, physician-modified endograft.
Discussion
Physician modification of endografts (PMEG) for managing complex aneurysms has become increasingly more common over the past decade in the United States.1,3,5–10 Use of PMEG has steadily increased in volume across the United States over the past decade as these techniques have improved.1,11,12 Patients with anatomically complex aneurysmal disease who are unsuitable candidates for open surgery are difficult to manage. Historically, these patients unfit for open repair were managed medically with expectant care or were treated with a suboptimal endovascular repair. In the United States, where there is a lack of off-the-shelf devices, PMEGs allow the vascular surgery community to expand treatment options for otherwise high-risk patients. Recent studies have shown PMEGs to have similar outcomes to industry-manufactured custom devices and superior outcomes to parallel grafting, likely due to the decreased incidence of gutter leaks.13–15 Ideally, surgeons in the United States would prefer to utilize off-the-shelf devices; unfortunately, we do not have the same variety of endograft configurations as our international colleagues. Even as new devices are available with shorter delivery times or off-the-shelf branched devices, there will remain a need for PMEGs in patients with unsuitable anatomy. Therefore, we believe PMEGs are a necessary adjunct for modern-day aortic surgeons.
While the first description of a modification of a PTFE-based endograft was published in 2014, no series of outcomes of this technique have been reported. 16 In this study, the safety and efficacy of this technique have been demonstrated. These patients require long-term follow-up and surveillance imaging as there is always the risk of progressive aneurysmal degeneration and component leaks. The follow-up data here are similar to previously described PMEG series regarding endoleak and mortality rates.1,3,9,17–19
Various software platforms are available for creation of PMEGs. Three-dimensional (3D) modeling and image analysis software are commonly utilized in device creation. These software aid in preoperative fenestration sizing and graft design, considering the patient’s unique anatomy and measurements from CT imaging.20,21 Three-dimensional printing may also be used for planning of fenestrations in patients with complicated anatomy and has been used to model angulated portions of the aorta in juxtarenal aortic pathologies. 22 Our experience is limited to the TeraRecon image analysis software (TeraRecon, Inc.), a 3D modeling software which we believe is effective, comprehensive, and more time- and cost-efficient than 3D printed models.
The significant benefit of this technique is the reproducible and reliable size of the graft at the time of modification and implantation. When the primary sleeve is removed from the CTAG device, the graft is at 50% of its nominal diameter, allowing the graft to be modified in a diameter-reduced state. This allows the surgeon to create fenestrations based strictly on clock position rather than calculating arc lengths necessary for modifying Dacron-based grafts. When this is implanted into the patient, there is no concern that graft wall apposition or fabric valleys from posterior diameter reduction will hinder target vessel cannulation. With this, technical success was 100% in this study, without a single target vessel loss.
Regarding the technique employed in this study, the primary difficulty is the need for large iliac arteries for access. This technique cannot be employed in patients with small iliac and femoral arteries because of the large 20 to 24 French sheath required for deployment, though this is similar to the off-the-shelf TAMBE device. 2 Access site complications were higher than average in our series and are described as follows: In one patient, removal of the right groin sheath revealed poor pulsation of the right groin, necessitating cutdown and arterial exposure which showed that ProGlide sutures and a plaque were causing near total occlusion. Arteriotomy was made and the plaque removed, with repair using a bovine patch; the patient recovered well. In the second complication, arterial signal was absent in the right ankle at surgery completion due to popliteal artery embolization. Through left groin access, a Penumbra catheter was used to aspirate the thrombus, and the flow was restored. The final complication was in a patient with good hemostasis of both groins at surgery completion who subsequently coded. After resuscitation, arterial line was placed for monitoring in the critical care unit, resulting in iatrogenic injury to the midportion of the right external iliac artery. This was rapidly stabilized with deployment of 2 covered stents. We highlight that these complications occurred in the first 2 years of this approach, and we had no access site complications as our technique improved between 2023 and 2024. The large sheath needed to implant the modified CTAG device can cause local dissection or failure of the suture-based closure devices, requiring cutdown and either primary or patch repair of the artery. Fortunately, most patients for whom this technique and graft work well are those with dissection thoracoabdominal aneurysms who tend to have large iliac and femoral arteries.
Regarding study design, the primary limitation is the lack of long-term follow-up data, the size of our series, and the lack of operative time metrics and outcomes compared with our Dacron-based PMEG cohort. While the median follow-up for this technique was only 223 days, some patients were surveyed over 2 years. There were no device-related failures during this short interval, though it is unclear how this will play out in the long term. The long-term durability of physician-modified endografts is a widely described limitation in the current literature.18,19,23–25 In addition, 2 patients were lost to follow-up and do not have follow-up information. Our cohort of patients is also small, with only 29 patients. However, we will continue to add to our series and analyze data. Regarding operative time metrics, the improvement and ease of implantation in dissection thoracoabdominal aneurysms is subjective at best at the current time and is indeed based on our aortic center’s experience, where most patients receive Dacron-based PMEG. It would be valuable to conduct a longitudinal prospective study comparing the efficacy and safety of the PTFE-based endograft compared with the Dacron-based endograft in urgent and emergent indications for further generalizability of our findings.
Conclusion
PTFE-PMEG offers a novel technique with multiple benefits, including improved manipulation within the small-diameter flow lumens, which result in improved ease of implantation. The interface between the aortic graft and bridging stent is also very stable due to the PTFE’s ability to conform around the stent. This technique can be employed with good outcomes regarding endoleak incidence and aortic-related mortality. Further validation of this study and need for prospective trials is necessitated.
Footnotes
Data Availability Statement
All data generated or analyzed during this study are included in this published article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Shahab Toursavadkohi and Dr. Mehrdad Ghoreishi are consultants with Gore.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
This study received ethical approval from the University of Maryland institutional review board (IRB# HP-00050195) on September 28, 2011 and reapproval on October 7, 2024.
Consent to Participate
This is an IRB-approved retrospective study, all patient information was de-identified and patient consent was not required.
Consent for Publication
Patient data will not be shared with third parties.