
Abstract
Purpose:
The complexity of fenestrated and branched endovascular aneurysm repair (F/BEVAR) has been linked to substantially longer procedural duration compared with standard endovascular aneurysm repair (EVAR). These complex procedures rely heavily on fluoroscopic guidance, leading to prolonged radiation exposure for both patients and operators. Given the potential risks associated with high radiation doses, this meta-analysis aimed to assess and compare patient radiation exposure between EVAR and F/BEVAR and evaluate time trends.
Methods:
Mendeley reference manager was used by 2 independent reviewers to evaluate articles identified in the MEDLINE, Cochrane Library, and Scopus databases over a 7-year period. A meta-analysis was conducted under Preferred Reporting Items for Systematic Reviews and Meta-Analyses criteria using the medical subject headings (MeSH) terms “AAA,” “aortic aneurysm,” and “radiation” to search and index journal articles systematically. Only full-text, English-language publications reporting radiation data on humans treated with standard EVAR or F/BEVAR were included. The SPSS statistical package was employed to generate fluoroscopy time (FT), kerma-area product (KAP), and cumulative air kerma (CAK) regression lines. The STATA statistical software was used to perform the meta-analysis and present the forest plots.
Results:
Seventy-two articles, encompassing 92 EVAR and F/BEVAR studies, were eligible for inclusion in this meta-analysis. The pooled mean values were lower in standard EVAR compared with the more complex F/BEVAR cases for FT (26.05 vs 77.51 minutes; p<0.001), KAP (131.34 vs 209.50 Gycm2; p=0.010), and CAK (806.76 vs 2798.61 mGy; p<0.001). This translates to a 197.5% increase in FT, a 59.5% increase in KAP, and a 246.9% increase in CAK for F/BEVAR compared with EVAR. Except for the increase in KAP during F/BEVAR procedures (r=0.531, p=0.028), all investigated parameters showed a decreasing trend over time for both EVAR (FT: r=–0.037, p=0.810; KAP: r=–0.098, p=0.540; CAK: r=–0.115, p=0.740) and F/BEVAR (FT: r=–0.387, p=0.034; CAK: r=–0.377, p=0.037).
Conclusion:
This meta-analysis highlights the substantial increase in radiation exposure associated with F/BEVAR compared with standard EVAR. Even though there is a clear paucity of rigorous, high-quality studies, the considerable radiation burden associated with F/BEVAR underscores the need for optimization efforts that minimize patient exposure without compromising procedural success.
Clinical Impact
This article provides information for better understanding of how patient intraoperative radiation exposure varies between the standard and the more complex endovascular aneurysm repair procedures using fenestrated and branched devices. This meta-analysis identified trends and heterogeneities in the fluoroscopy time, kerma-area product, and cumulative air kerma values among the studies. The regression lines deliver a clearer picture of the radiation exposure trends over the last years, offering insights into improving surgical techniques and patient safety by providing guidance on how to balance between the technical demands of complex devices and technology of the C-arm systems with the need to minimize patients’ radiation doses.
Introduction
Currently, the broad eligibility criteria for endovascular intervention allow the vascular surgeons to perform, not only standard, but also complex endovascular repair of aneurysms with hostile anatomy, accompanied by exceptional technical success rates and long-term outcomes. 1 Standard endovascular aneurysm repair (EVAR) is typically performed to exclude elective infrarenal abdominal aortic aneurysms (AAAs) using bifurcated stent-grafts. 2 The term “complex aortic aneurysm” refers to the treatment of more challenging aneurysms of the middle and upper abdominal aorta that involve any combination of its visceral branches, such as renal, superior mesenteric, or coeliac vessels and, therefore, will mostly cover repair of juxtarenal, pararenal, paravisceral, and thoracoabdominal aortic aneurysms. 3 Complex aortic aneurysms are managed utilizing innovative methods that preserve side branch patency, including fenestrated EVAR (FEVAR), branched EVAR (BEVAR), and chimney or parallel stenting techniques.4,5 Custom-made, off-the-shelf, and physician-modified endografts are used for this purpose.6,7
Regardless of the procedure’s complexity, EVAR interventions require the application of ionizing radiation, either by means of computed tomography angiographies (CTAs) for pre-treatment planning and post-treatment surveillance or in the form of intraoperative fluoroscopy guidance.8,9 In particular, for challenging EVAR cases, and until radiation-free techniques, such as fiberoptic endoluminal navigation becomes broadly available, the intraprocedural fluoroscopic exposure of the patient and personnel remains worrisome.10,11 In nonstandard interventions where prolonged fluoroscopy times (FTs) are usually involved, the resultant peak skin dose (PSD) or cumulative air kerma (CAK) may surpass the 2 gray (Gy) threshold for deterministic effects and lead to radiation-induced skin injuries to patients.12,13 Unlike deterministic effects, stochastic effects of radiation lack a minimum dose threshold, with carcinogenesis probability increasing proportionally to cumulative exposure. 14 While reported radiation-induced malignancies in EVAR procedures remain rare, younger and healthier patients face higher lifetime risks due to prolonged latency periods of stochastic effects, necessitating thorough informed consent regarding alternatives, such as open repair. 15
In line with the European Directive 2013/59/EURATOM, 16 several authors reported patient and occupational doses and established reference levels for various fluoroscopically-guided interventional (FGI) procedures, with the vast majority of EVAR-related studies incorporated in the literature reviews conducted by Monastiriotis et al 17 and Dindyal et al, 18 as well as in the systematic reviews of Hertault et al 19 and de Ruiter et al. 20 However, the scope of the previous reviews was limited by the absence of evaluation in FT, kerma-area product (KAP) and CAK temporal trends, particularly for F/BEVAR interventions.
The present systematic review and meta-analysis aim to summarize the current literature regarding radiation dose to patients during standard EVAR and F/BEVAR procedures in the abdominal and the thoracoabdominal segment of the aorta. A direct comparison of radiation exposure between standard EVAR and F/BEVAR is made, isolating the impact of procedural complexity, whereas the pooled estimates and regression lines for FT, KAP, and CAK ascertains whether advancements in imaging and techniques have reduced patient doses over the past 7 years.
Materials and Methods
A systematic review and meta-analysis were conducted to evaluate and compare the levels of radiation exposure experienced by patients during standard (EVAR) and complex (F/BEVAR) aortic interventions. The approach of the present work was based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 21
Databases and Search Terms
The studies were identified through a comprehensive search of electronic databases and by reviewing the bibliographic references of relevant articles. A search was run in the National Library of Medicine’s MEDLINE database (using the PubMed interface), Cochrane library and Scopus from January 2018 to April 2024. The last search was conducted on May 1, 2024. There were no language constraints on the first screening. Keywords were chosen utilizing medical subject headings (MeSH) for PubMed and Cochrane and MeSH/Emtree for Scopus. The databases were searched with an unrestricted search strategy, applying exploded MeSH and keywords combined with the Boolean operators “AND” or “OR” to retrieve relevant reports, as included in Supplemental Table S1 (see Appendix). The International Prospective Register of Systematic Reviews (PROSPERO) database was preferred to register the protocol of our work (ID: CRD420251069417).
Study Selection, Risk, and Publication Biases
Mendeley software (Elsevier B.V., Amsterdam, The Netherlands) was employed to gather the studies identified in all database searches. Duplicates were removed using the Ablebits Duplicate Remover add-in (4Bits Ltd, Gomel, Belarus) in Microsoft Excel, version 2021 (Microsoft Corp., Redmond, Wash). No search was conducted to retrieve any unpublished data or abstracts. Two reviewers (F. E. and C. P.) performed eligibility assessment independently in an unblinded standardized manner. Any discrepancies in the inclusion of studies were resolved through consensus. The ROBVIS (Risk Of Bias VISualization) web application combined with the ROBINS-I V2 (Risk Of Bias In Non-randomised Studies—of Interventions, Version 2) 22 tool were employed to create the risk-of-bias assessment figures in the form of “traffic light” (Supplemental Figure S1) and weighted bar plots (Supplemental Figure S2) (see Appendix). Publication bias was assessed by visual inspection of funnel plots asymmetry and quantitatively with Egger’s linear regression test (Supplemental Figures S3–S5) (see Appendix).
Inclusion and Exclusion Criteria
All articles reporting radiation exposure in humans during standard EVAR and F/BEVAR were eligible for review. Non-English articles, in vitro, animal, phantom and simulation studies, editorials, letters to the editor, presentations, and abstracts were excluded. Articles, including isolated common iliac artery aneurysms, infected or inflammatory AAAs, ruptured aneurysms, unified results between standard EVAR, and F/BEVAR interventions as well as unified results between intact and ruptured aneurysms were also excluded. Furthermore, patients with prior history of open or endovascular repair for AAA were debarred. Studies reporting patient sample smaller than 20 were not considered, whereas reviews were excluded to avoid duplication of data but used as a source of potential eligible articles. Studies prior to 2018 were excluded to avoid overlapping of data and results with a previous systematic review 19 reporting dosimetric data of endovascular aortic operations. Studies providing insufficient or unconvertable data were excluded, too.
Data Items and Definitions
Data extracted included study information (year of publication, study design, number of cases, and patient/staff-oriented) and procedure characteristics (imaging system, procedure and fluoroscopy durations, and radiation doses). Fluoroscopy time (FT), KAP, and CAK constitute the investigated dose parameters. FT (reported in minutes) corresponds to the total “beam on” time, KAP (also known as dose-area product, reported in Gycm2) is a surrogate measurement for the total amount of radiation energy imparted to the patient while CAK (also known as reference air kerma, reference dose or skin dose, reported in mGy) is used as an estimator of harmful tissue reactions.
Temporal Trend Lines and Meta-Analysis
Articles reporting patient intraoperative dosimetric data regarding EVAR and F/BEVAR procedures were analyzed. Prior to the conduction of temporal trend lines and meta-analysis, each substudy contained within the articles of Tables 1 and 2 was considered as a separate case for inclusion. Spearman’s rho (r) nonparametric test was used to measure the strength and direction of association that exists between each dosimetric quantity and date of publication. A p value of 0.050 was considered statistically significant. Analyses were performed using SPSS Statistics version 25.0.0.1 (SPSS Inc, Chicago, Illinois). The SPSS statistical package created the regression lines via the locally estimated scatterplot smoothing function. Due to the heterogeneity of the reported dosimetric data, median (interquartile range) values were converted to mean ± standard deviation utilizing the appropriate estimation methods as suggested by Wan et al. 23
Studies Reporting Patient Intraoperative Dosimetric Data in Standard EVAR Procedures.

Abbreviations: EVAR, endovascular aneurysm repair; FT, fluoroscopy time; KAP, kerma-area product; CAK, cumulative air kerma; NA, not available.
Data are presented as mean ± standard deviation or median (interquartile range) unless indicated otherwise.
Mean (range).
Median (range).
Studies Reporting Patient Intraoperative Dosimetric Data in F/BEVAR Procedures.

Abbreviations: F/BEVAR, fenestrated/branched endovascular aneurysm repair; FT, Fluoroscopy time; KAP, kerma-area product; CAK, cumulative air kerma; NA, not available.
Data are presented as mean±standard deviation or median (interquartile range) unless indicated otherwise.
Median (range).
To perform the meta-analysis, mean and standard deviation from each study were extracted or calculated and standard errors were appropriately calculated for the 3 quantities of interest (FT, KAP, and CAK). Pooled mean with 95% confidence interval (CI) were thereafter calculated using random effects restricted maximum likelihood model for the 3 outcomes, separately for the groups of EVAR and F/BEVAR and comparison between them was performed using z-test. The STATA statistical software v.18 (Stata Corp., LP, USA) was used for the analysis.
Results
Following the aforementioned methodology, the search resulted in the identification of 858 publications, 74 of which specifically examined our primary objective of assessing and comparing patient intraoperative radiation dose in EVAR and F/BEVAR procedures. From these publications, 92 studies met our inclusion criteria and were analyzed in the systematic review (Figure 1).
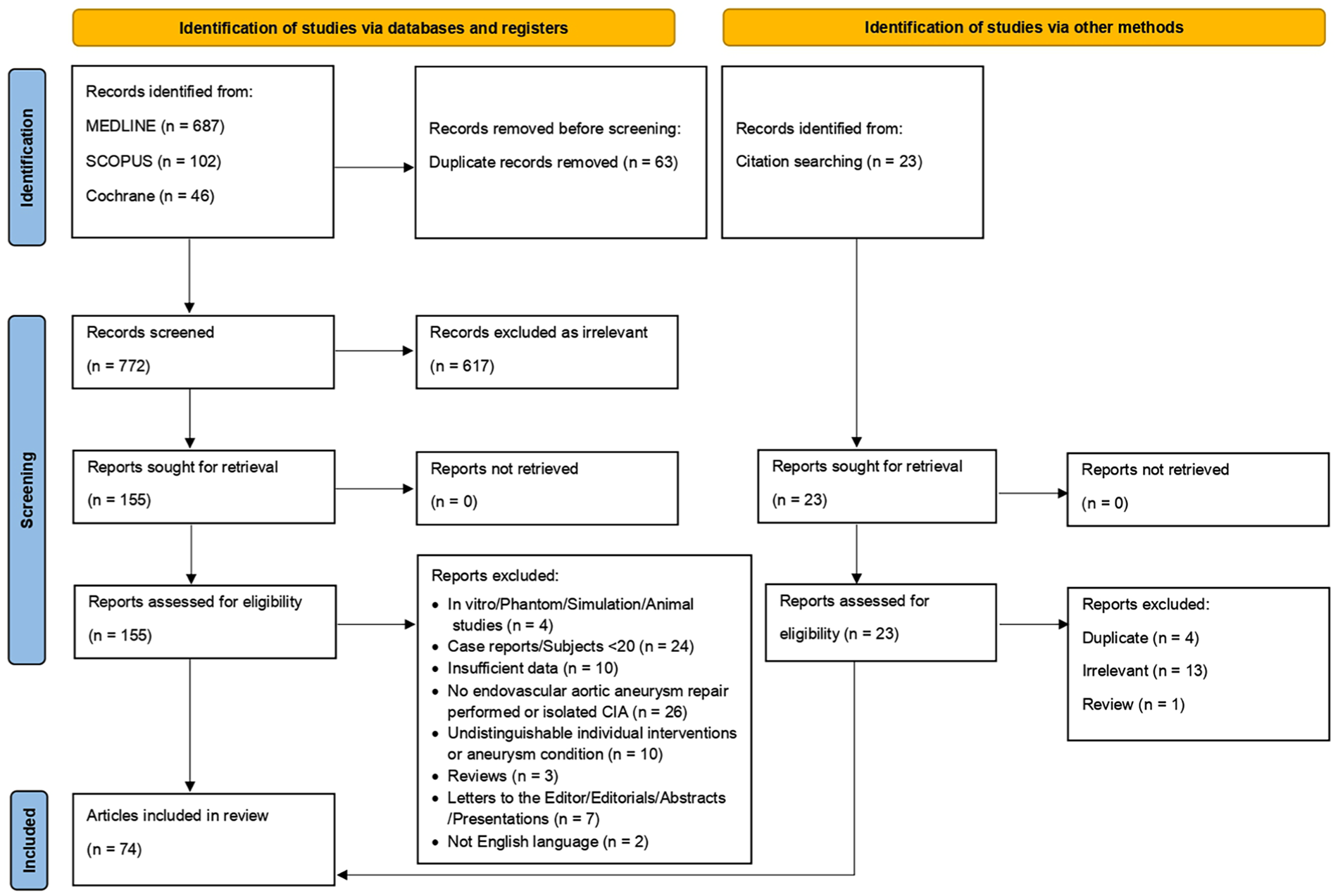
Flowchart displaying the selection of publications reporting patient radiation dose during standard EVAR and F/BEVAR interventions. EVAR, endovascular aneurysm repair; F/BEVAR, fenestrated/branched endovascular aneurysm repair.
Standard EVAR Studies
Fifty-two studies reporting patient doses for standard EVAR were included in the study analysis (Table 1). Of these studies, 21 were performed inside a hybrid suite with floor- or ceiling-mounted imaging systems, 9 inside conventional theaters using mobile C-arms whereas 2 studies were conducted inside both types of operating rooms. Operating room type was not available in 11 publications. Forty-six (88.5%) studies have reported FT values, 42 (80.8%) have reported KAP values, and 11 (21.2%) have reported CAK values.
F/BEVAR Studies
A total of 40 F/BEVAR studies were included in the analysis (Table 2). Of the studies reporting operating room type, 96.4% were carried out in hybrid suites. The operating room type was unavailable in 12 publications. Fluoroscopy time (FT), KAP, and CAK values were reported in 30 (75%), 17 (42.5%), and 31 (77.5%) studies, respectively.
FT, KAP, and CAK Trend Lines in Standard EVAR and F/BEVAR Procedures
A decreasing trend was observed for FT for all studies included in our analysis (both EVAR and F/BEVAR) (r=–0.136, p=0.240), and separately for standard EVAR procedures (r=–0.037, p=0.810). Regarding the F/BEVAR procedures, a decreasing trend was observed (r=–0.387, p=0.034) (Figure 2).
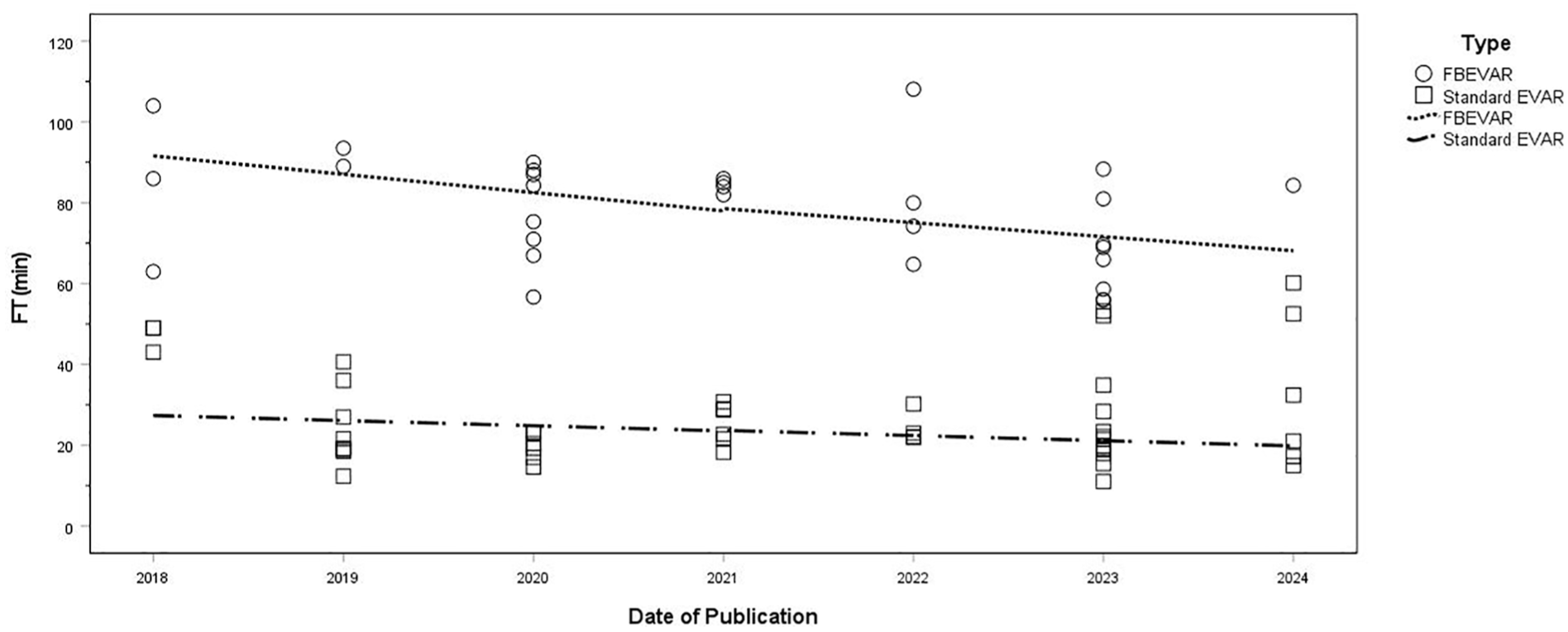
Mean FT trend lines in standard EVAR and F/BEVAR procedures during the past 7 years. EVAR, endovascular aneurysm repair; F/BEVAR, fenestrated/branched endovascular aneurysm repair; FT, fluoroscopy time.
An increasing trend was observed for KAP for all studies included in our analysis (both EVAR and F/BEVAR) (r=0.023, p=0.860). Concerning standard EVAR procedures, a decreasing trend was observed for KAP values (r=–0.098, p=0.540) (Figure 3). F/BEVAR interventions showed an increase over time (r=0.531, p=0.028) (Figure 3).

Mean KAP trend lines in standard EVAR and F/BEVAR procedures during the past 7 years. EVAR, endovascular aneurysm repair; F/BEVAR, fenestrated/branched endovascular aneurysm repair; KAP, kerma-area product.
Similar to the FT trend, a decreasing tendency was also noticed for CAK values when all studies included in our analysis (both EVAR and F/BEVAR) were considered (r=–0.261, p=0.095) (Figure 4). A decreasing trend was additionally observed for CAK values of standard EVAR interventions (r=–0.115, p=0.740) (Figure 4). With respect to F/BEVAR procedures, a decreasing trend was noticed for CAK values (r=–0.377, p=0.037) (Figure 4).

Mean CAK trend lines in standard EVAR and F/BEVAR procedures during the past 7 years. EVAR, endovascular aneurysm repair; F/BEVAR, fenestrated/branched endovascular aneurysm repair; CAK, cumulative air kerma.
Each circle and square symbol in Figure 2–4 illustrates the reported values included in the standard EVAR and F/BEVAR studies, as appropriate. The general trends are represented by the dashed (standard EVAR and F/BEVAR samples) and continuous regression lines (overall sample).
FT, KAP, and CAK Forest Plots in Standard EVAR and F/BEVAR Procedures
Mean (95% CI) FT values for all eligible studies are presented in Figure 5. The pooled mean (95% CI) FT for the entire cohort was 46.80 minutes (40.49–53.12 minutes). A difference (p<0.001) equivalent to a 197.5% increase was found between the pooled mean FT after standard EVAR (FT: 26.05 minutes; 95% CI: 22.82–29.28 minutes), compared with F/BEVAR (FT: 77.51 minutes; 95% CI: 72.83–82.20 minutes). A between-group and within-group heterogeneity was recorded (all p<0.001). The 75th percentile FT values for standard EVAR and F/BEVAR are equal to 31.16 and 87.25 minutes, respectively.
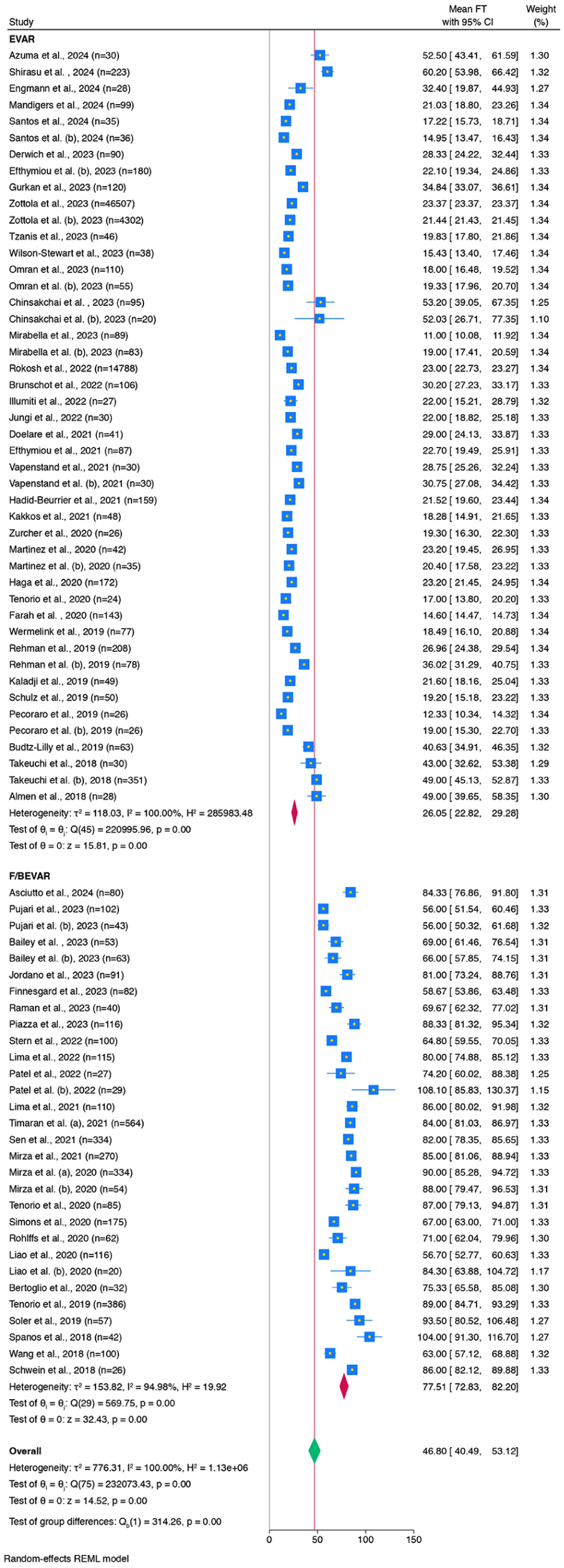
FT forest plot for standard EVAR and F/BEVAR interventions. EVAR, endovascular aneurysm repair; F/BEVAR, fenestrated/branched endovascular aneurysm repair; FT, fluoroscopy time; CI, confidence interval; REML, restricted maximum likelihood.
The mean (95% CI) KAP was 131.34 Gycm2 (95.06–167.63 Gycm2) for standard EVAR and 209.50 Gycm2 (160.53–258.47 Gycm2) for F/BEVAR, pointing to a percentage increase of 59.5 (p=0.010). The pooled mean (95% CI) KAP for the entire cohort was 154.23 Gycm2 (123.52–184.94 Gycm2), as shown in Figure 6. A heterogeneity in KAP values was observed between and within the 2 groups (all p<0.001). The 75th percentile KAP values for standard EVAR and F/BEVAR are equal to 204.23 and 314.10 Gycm2, respectively.
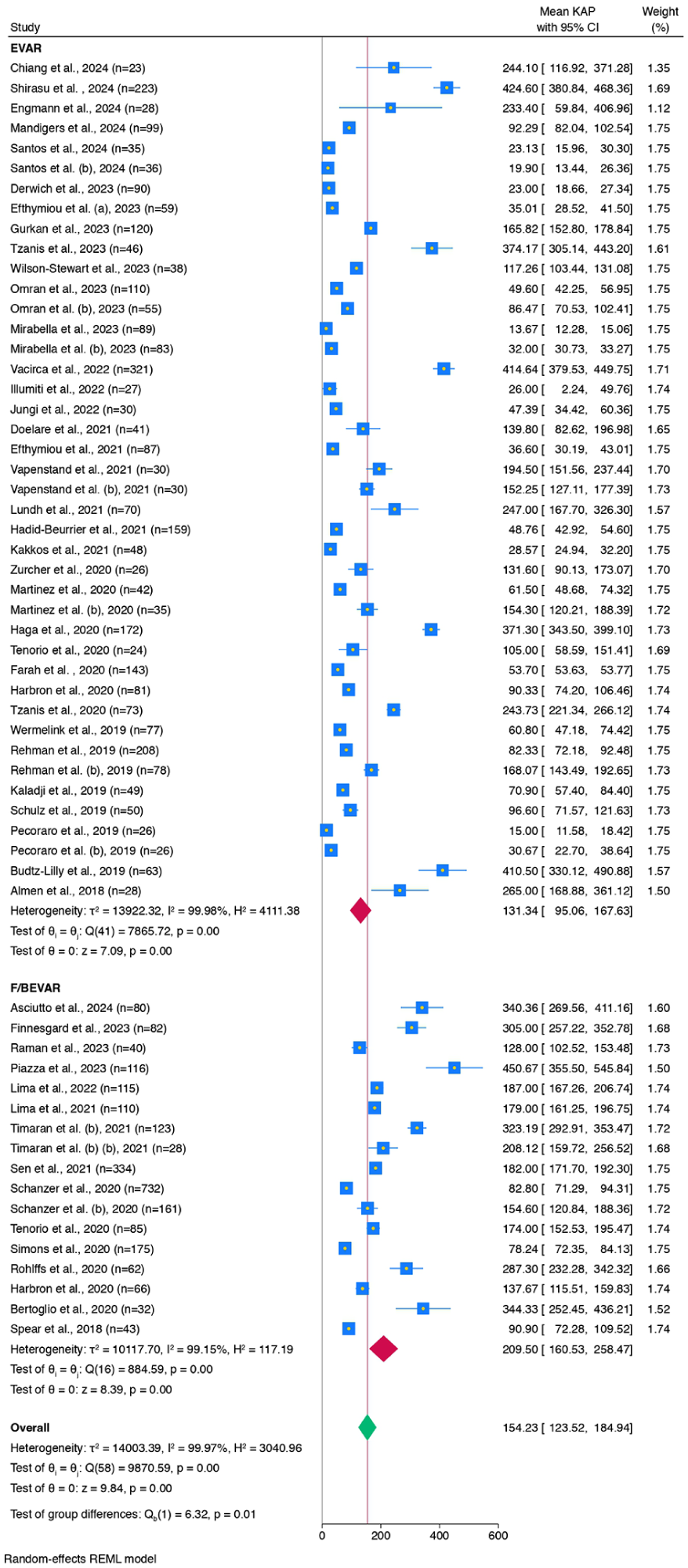
KAP forest plot for standard EVAR and F/BEVAR interventions. EVAR, endovascular aneurysm repair; F/BEVAR, fenestrated/branched endovascular aneurysm repair; KAP, kerma-area product; CI, confidence interval; REML, restricted maximum likelihood.
A difference in pooled CAK was recorded between standard EVAR and F/BEVAR (p<0.001). More specifically, the pooled mean (95% CI) CAK was 806.76 mGy (452.44–1161.08 mGy) for standard EVAR and 2798.61 mGy (2412.46–3184.77 mGy) for F/BEVAR, a substantial increase of 246.9%. The pooled mean (95% CI) CAK among all studies was 2276.84 mGy (1875.75–2677.93 mGy) (Figure 7). A between-group and within-group heterogeneity (all p<0.001) was also recorded for standard EVAR and F/BEVAR procedures. The 75th percentile CAK values for standard EVAR and F/BEVAR are equal to 1230.67 and 3600.00 mGy, respectively.
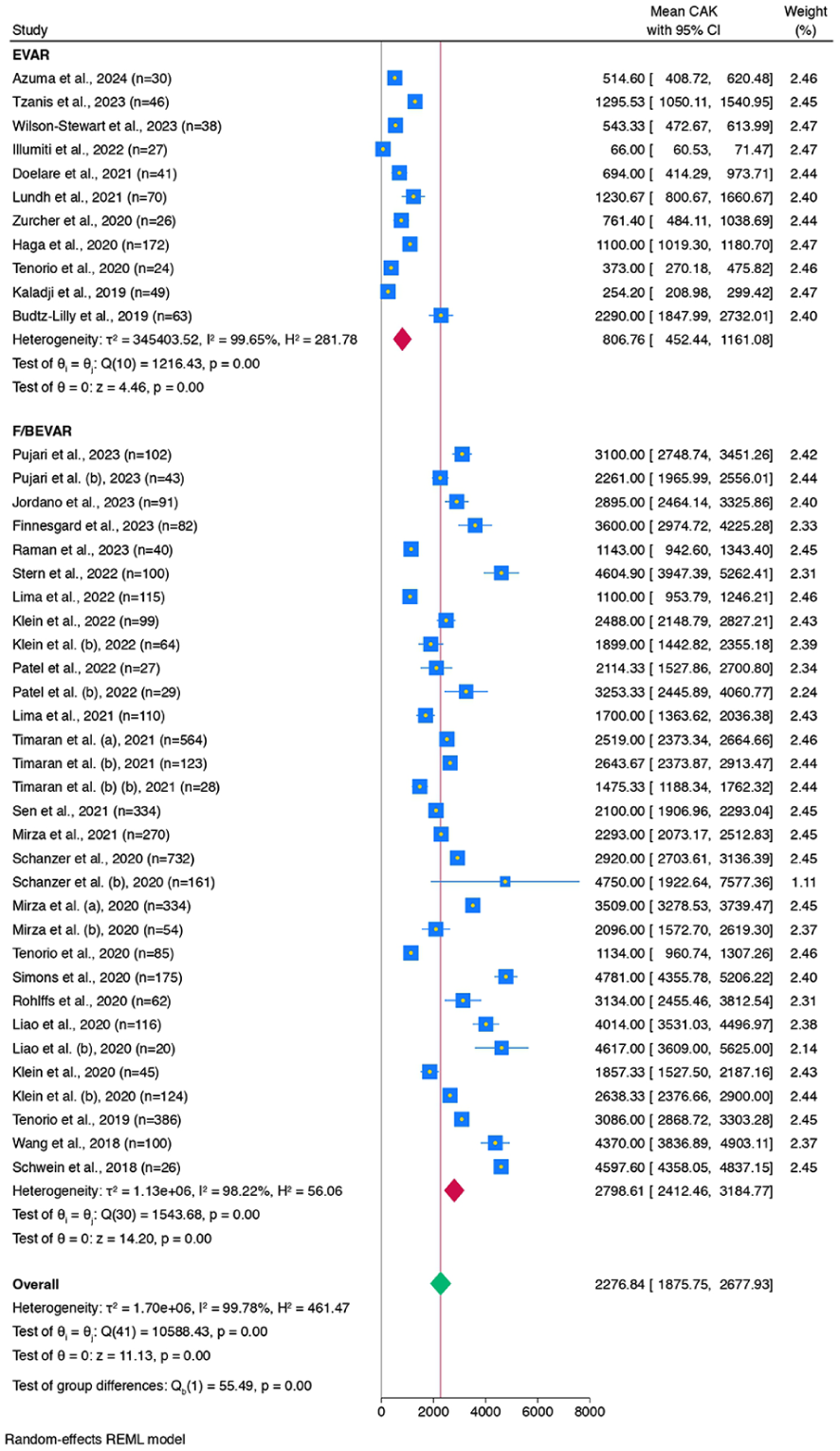
CAK forest plot for standard EVAR and F/BEVAR interventions. EVAR, endovascular aneurysm repair; F/BEVAR, fenestrated/branched endovascular aneurysm repair; CAK, cumulative air kerma; CI, confidence interval; REML, restricted maximum likelihood.
Sensitivity Analysis
A sensitivity analysis was also performed to assess whether the forest plots were affected by including studies where median values were converted to means. No significant difference between standard EVAR and F/BEVAR groups was found for mean KAP values (p=0.680). However, in the total group (Figure 4), this difference was significant (p=0.010). This discrepancy may be attributed to the fact that after excluding studies with converted median values, the mean value of each group fell within the CI of the other group, a finding not observed in the overall analysis. For FT and CAK values, the differences between the 2 groups remained significant (p<0.001).
Discussion
This comprehensive research analyzes intraoperative radiation exposure to patients during EVAR and F/BEVAR procedures in terms of FT, KAP, and CAK reported in the literature over the past 7 years.
Wide variations in the reported patient dose values were seen in this systematic review, verifying the plethora of factors that affect the dosimetric results, namely, the complexity of the procedure, the experience and training of staff, as well as the type of fluoroscopic equipment utilized. Fluoroscopic guidance during EVAR interventions poses potential health hazards to patients and endovascular staff and may lead to what are known as deterministic or stochastic effects. The exponential growth in the FGI procedures conducted in the course of the past years justifies the rising concern of the endovascular surgery society and calls for a, all the more, radiation safety culture promotion.96,97 Diagnostic reference levels (DRLs) and trigger levels 14 are recognized and important tools for optimizing patient radiation protection. As supplements to professional judgment, DRLs may indicate whether the patient exposure is unusually high or unusually low while the trigger levels have been established by the European Society of Radiology to detect clinically relevant skin harm and trigger, if necessary, appropriate post-procedural follow-ups. 14 For interventional radiology procedures in adult patients, the suggested trigger levels for FT, KAP, and CAK are 60 minutes, 500 Gycm2, and 5 Gy, respectively. Not included herein due to insufficient data, a PSD of 3 Gy serves as an additional threshold value used to trigger patient follow-up.
Of the reported FT values, the defined trigger level of 60 minutes has been surpassed in 1 of 46 (2.2%) EVAR and in as many as 26 of 30 (86.7%) studies with F/BEVAR interventions. The reported KAP and CAK values did not surpass the respective trigger level in either EVAR or F/BEVAR studies. The pooled mean FT values for the entire cohort (46.80 minutes) and standard EVAR (26.05 minutes) were lower than the suggested trigger level by 22% and 56.6%, respectively, whereas for F/BEVAR (77.51 minutes), the relevant threshold is surpassed by 29.2%. Of note, the peak FT value of 108.10 minutes transcends the relevant threshold by 80.2%. The pooled mean KAP values for the entire cohort (154.23 Gycm2), standard EVAR (131.34 Gycm2), and F/BEVAR (209.50 Gycm2) are also considerably less than the suggested trigger level by 69.2%, 73.7%, and 58.1%, respectively, whereas the maximum KAP value recorded (450.67 Gycm2) approaches 90% of the 500 Gycm2 threshold. Likewise, the pooled mean CAK values for the overall sample (2276.84 mGy), standard EVAR (806.76 mGy), and F/BEVAR (2798.61 mGy) are only part of the suggested 5 Gy trigger level (45.5%, 16.1%, and 56%, respectively). However, it should be emphasized that both the overall and the F/BEVAR pooled mean CAK values exceed the 2 Gy benchmark for transient erythema (skin reddening), while the peak CAK value recorded herein (4781.00 mGy) reaches 95.6% of the 5 Gy threshold for clinical follow-up. Most studies performed extensive follow-ups, but mainly regarding 30-day mortality, endoleak freedom, sac regression and target vessel patency; post-operative examinations for potential patient radiation-induced skin damage were not reported.
The mean FT (11.00 minutes) and KAP (13.67 Gycm2) values included in the study of Mirabella and associates 39 are the lowest values reported during standard EVAR procedures and the lowest overall and correspond to 89 patients who underwent elective EVAR for the treatment of asymptomatic AAA using the speed-gate cannulation technique. Similarly, the exceptionally low mean CAK of 66.00 mGy reported by Illuminati et al 43 is the lowest during standard EVAR procedures and the lowest included herein and corresponds to a series of 27 patients with favorable anatomy who submitted to an elective fully ultrasound-assisted EVAR with either a mobile or a fixed C-arm. The mean FT value of 108.10 minutes included in the study of Patel et al 76 was the highest reported in the F/BEVAR group and corresponds to 29 patients treated for pararenal, type IV or more complex thoracoabdominal aortic aneurysms (TAAAs) with their visceral vessels cannulated via an anterograde upper extremity access. Piazza et al 72 reported the highest mean KAP value (450.67 Gycm2) on 116 patients selected from the ItaliaN Branch Registry of E-nside EnDograft (INBREED) and treated with a novel off-the-shelf pre-loaded inner branched thoracoabdominal stent-graft device (E-nside, Artinian). The highest mean CAK value (4781.00 mGy) was reported by Simons et al 85 and corresponds to a cohort of 175 patients submitted to complex F/BEVAR for the treatment of either intact or symptomatic juxtarenal, pararenal, and TAAAs. As expected, the values of the investigated dose parameters reported in the F/BEVAR group are the greatest included in this systematic review. It is well known that the F/BEVAR procedures are commonly associated with several modifiable and uncontrolled anatomical, clinical, or technical factors which affect not only the complexity and the long-term efficacy of the intervention but increase the patient exposure to ionizing radiation as well.32,50,57
The decreasing trend for FT in all groups indicates standardization of “beam on” usage over the 7-year period, independently of the procedures’ complexity. This is also reflected by the decreasing trend observed in CAK values for all groups considering that the CAK is directly proportional to FT. The decreasing trend in KAP values for standard EVAR procedures is probably associated with the remarkably lower median KAP values (45.20 vs 147.10 Gycm2) when these procedures were performed with conventional compared with hybrid equipment (Mann-Whitney test, p<0.001), although the median FT values exhibit an insignificant increase (21.90 vs 21.20 minutes) for conventional equipment (Mann-Whitney test, p=0.680). When comparing FT and CAK trend lines for standard EVAR and F/BEVAR procedures, it is observed that the later results in higher FT and CAK values during all years but exhibit a steepest reduction over the 7-year period than the standard EVAR procedures. While the decreasing FT demonstrates procedural efficiency improvements (eg, refined cannulation techniques and standardized device deployment), the increase in KAP for the F/BEVAR procedures indicates the need to exploit and implement the imaging and dose-saving capabilities the C-arm equipment offers. The increase in KAP values for F/BEVAR procedures is mainly associated with the usage of hybrid equipment in most of these studies. However, no information is available regarding F/BEVAR procedures performed with conventional equipment and it is not feasible to extract a conclusion regarding the effect of equipment on KAP values. Nevertheless, it is likely that the inherent anatomic complexity of F/BEVAR procedures demands larger irradiation fields to simultaneously visualize multiple visceral branches, stent-graft components, and proximal/distal sealing zones, while existing imaging detector technology struggles to accommodate these expanded fields without patient dose penalties. Modern C-arm systems equipped with intelligent collimation represent a breakthrough in radiation safety for complex endovascular procedures. These platforms utilize real-time image processing algorithms to automatically adjust collimation boundaries based on live anatomical recognition, dynamically minimizing irradiated fields while preserving critical visualization. In a previously reported systematic review by Hertault et al, 19 the KAP values recorded between 2008 and 2018 (regarding both standard and complex EVAR studies) demonstrated a decreasing trend over time (statistical significance was unavailable).
Even for the regression lines that display a decreasing trend, efforts should always be made so that the clinical practice is in line with the ALARA (As Low As Reasonably Achievable) principle. The ALARA principle remains a cornerstone of radiation safety in endovascular procedures, yet its documentation in the literature is inconsistent. While universally endorsed, explicit adherence is rarely addressed; only 26% of the studies included in our analysis provided direct compliance. This ambiguity reflects the absence of standardized metrics for ALARA implementation, despite its theoretical prominence. In practice, however, many interventional specialists likely employ dose-optimization techniques routinely, even without formal protocolization. Common strategies include low-frame-rate fluoroscopy, beam collimation, minimized patient-detector distance, avoidance of geometric magnification, and judicious use of digital subtraction angiography (DSA). Moreover, institutional quality control can be strengthened by analyzing procedure-specific radiation metrics. The 75th percentile values for FT, KAP, and CAK—31.16 minutes, 204.23 Gycm2, and 1230.67 mGy for standard EVAR, compared with 87.25 minutes, 314.10 Gycm2, and 3600.00 mGy for F/BEVAR procedures in this study—allow institutions to monitor procedural efficiency, assess radiation exposure trends, and identify outliers that may require protocol adjustments to enhance patient safety and operational consistency. Emerging technologies, such as image fusion further reduce reliance on live fluoroscopy, exemplifying ALARA’s implicit integration into modern workflows.
Image fusion technology represents a paradigm shift in EVAR, overcoming traditional limitations of fluoroscopic guidance through intelligent integration of preoperative CTA and real-time imaging. This advanced modality superimposes high-resolution 3D aortic reconstructions onto live fluoroscopy, enabling precise endograft deployment and branch vessel cannulation while substantially reducing intraoperative contrast demands. A key benefit is its radiation-sparing effect, achieved by decreasing reliance on prolonged fluoroscopy and repetitive DSAs. Nevertheless, technical challenges persist, including potential registration errors from respiratory motion or aortic remodeling, necessitating meticulous quality control. While this technology enhances procedural safety, its efficacy remains operator-dependent, requiring specialized training to maximize workflow efficiency and radiation optimization. Among the 52 standard EVAR studies reviewed, only 3 (6%) reported the use of fusion imaging for procedural guidance.58,60,61 Notably, Wermelink et al 58 demonstrated the feasibility of fusion imaging in a conventional operating room using a mobile C-arm, achieving a 95.5% registration success rate, suggesting a viable alternative to hybrid operating suites. In contrast, 17 of 40 (43%) F/BEVAR studies incorporated fusion imaging, reflecting its more frequent adoption in complex endovascular repairs. Overall, 22% of the analyzed studies utilized fusion guidance. Previous investigations have assessed the isolated influence of fusion imaging in endovascular repair, with Ahmad et al 98 evaluating EVAR and Bailey et al 68 analyzing FEVAR, with both concluding that its use resulted in a nonsignificant reduction in FT. The meta-analyses demonstrated that F/BEVAR procedures result in higher pooled mean FT (3-fold), KAP (1.6-fold), and CAK (3.5-fold) values compared with standard EVAR interventions. Vascular surgeons should be aware that in F/BEVAR procedures the pooled mean FT was above the 60 minutes of trigger level proposed by ESR-CIRCE (European Society of Radiology-Cardiovascular and Interventional Radiological Society of Europe) guidelines. 14 However, the pooled mean KAP and CAK values were below the thresholds of 500 Gycm2 and 5000 mGy, respectively.
The larger increases in mean KAP values for F/BEVAR compared with standard EVAR procedures are mainly associated with the use of fixed angiography systems in most of these procedures. These systems are generally equipped with large flat-panel detectors providing the ability for larger radiation field sizes and x-ray generators providing higher radiation outputs than the conventional C-arms. Heterogeneity analysis showed that all the groups exhibited significant heterogeneity as determined with τ2 and I2 statistics and homogeneity test of θ i =θ j . The pooled mean FT is slightly more heterogenic than pooled mean KAP and CAK values in standard EVAR group while in F/BEVAR group the heterogeneity of FT is smaller than the KAP and CAK values. Although there was heterogeneity in the pooled outcomes, further exploration via meta-regression analysis was not feasible due to the inconsistent or absent reporting of relevant covariates among the included studies. This underscores the importance of standardized data reporting in radiation-focused endovascular studies to enable more informative comparative analyses.
The evolution of endovascular procedures demands a radical transformation toward harmonizing technical efficacy with patient radiation safety. Central to this effort is the standardization of training programs, which must address both procedural proficiency and radiation stewardship, particularly in complex interventions, namely, F/BEVAR. Emerging low-dose protocols, such as ultra-low frame rate (1–2 pulses per second [pps] for surveillance phases and 4–5 pps for DSAs) and carbon dioxide-guided angiography, demonstrate dual benefits: significant radiation reduction and mitigation of contrast-induced nephropathy, offering a safer alternative to conventional iodinated agents. Furthermore, integrating advanced imaging modalities, such as intravascular ultrasound, electromagnetic navigation, and magnetic resonance imaging (MRI) fusion, can reduce reliance on fluoroscopy, while technologies like Fiber Optic RealShape and artificial intelligence-driven robotic systems promise submillimeter precision with minimal radiation exposure. Augmented reality overlays and real-time dose-tracking algorithms further enhance safety by providing instantaneous feedback on cumulative KAP/CAK metrics, enabling proactive threshold adjustments. However, widespread adoption hinges on overcoming barriers, such as cost, training gaps, partial fluoroscopy, and interoperability between hybrid theater systems. Future research should prioritize multicenter trials to validate these technologies’ cost-efficacy and long-term outcomes, ensuring they translate into scalable, standardized clinical practice.
Limitations
On top of the limited number of high-quality studies, the moderate risk of bias and the significant heterogeneity among the articles included in our work constitute potential factors languishing the pooled estimates of the meta-analysis. Several of the exclusion criteria included herein, such as full-text, English- and published-only studies, while ensuring methodological rigor in our quantitative analysis, add a potential selection bias in our outcomes. In addition, several mean dosimetric values comprised in the current analysis were product of conversions that may introduce inaccurate results. Moreover, the radiation exposure metrics reported in this study reflect procedures performed predominantly in hybrid operating rooms with advanced imaging capabilities, including optimized dose modulation and high-resolution fluoroscopy. While these findings demonstrate achievable benchmarks in well-resourced settings, their generalizability to environments utilizing mobile C-arms or conventional operating suites may be limited. Furthermore, the ROBINS-I assessment revealed that the primary risks of bias stemmed from incomplete dosimetric reporting (D5) and outcome measurement inconsistencies (D6), particularly for KAP values in F/BEVAR studies. While intervention classification (D3) and confounding (D1) were well addressed, the heterogeneity in radiation dose data, likely aggravated by measurement variability, warrants cautious interpretation of pooled estimates, especially for KAP comparisons between EVAR and F/BEVAR. Finally, the noninclusion of occupational exposure together with the absence of radiation dose evaluation during thoracic aneurysm repair procedures constitute notable gaps, and both should be addressed in the near future.
Conclusion
The broad variation in the reported dosimetric values of the studies assessed reflects the plethora of contributing factors that affect a successful EVAR procedure. The regression lines revealed that all the dose parameters investigated decrease over time, apart from the KAP during F/BEVAR interventions. Furthermore, this meta-analysis highlights the substantial increase in radiation exposure associated with F/BEVAR compared with standard EVAR. However, the conclusions are tempered by the limited number of high-quality studies meeting inclusion criteria, hinting the actual radiation burden may be even higher than reported in the current research. As F/BEVAR interventions gain wider adoption, concerted efforts to minimize radiation dose must be prioritized. Key strategies include implementing optimized imaging protocols, refining procedural techniques, and enhancing operator training in radiation safety principles. This work shall increase vascular surgeons’ radiation protection awareness and may serve as a dose-reduction tool for staff and patients during EVAR procedures.
Supplemental Material
sj-docx-1-jet-10.1177_15266028251380519 – Supplemental material for A Systematic Review and Meta-analysis of Intraoperative Patient Dosimetric Data in Standard Endovascular Repair for Infrarenal Abdominal Aortic Aneurysms Versus Fenestrated and Branched Endovascular Procedures for Thoracoabdominal Aortic Aneurysms
Supplemental material, sj-docx-1-jet-10.1177_15266028251380519 for A Systematic Review and Meta-analysis of Intraoperative Patient Dosimetric Data in Standard Endovascular Repair for Infrarenal Abdominal Aortic Aneurysms Versus Fenestrated and Branched Endovascular Procedures for Thoracoabdominal Aortic Aneurysms by Fotios O. Efthymiou, Christos F. Pitros, Vasileios I. Metaxas, Constantine N. Antonopoulos, Christos P. Dimitroukas, Stavros K. Kakkos, George S. Panayiotakis and Konstantinos G. Moulakakis in Journal of Endovascular Therapy
Supplemental Material
sj-docx-2-jet-10.1177_15266028251380519 – Supplemental material for A Systematic Review and Meta-analysis of Intraoperative Patient Dosimetric Data in Standard Endovascular Repair for Infrarenal Abdominal Aortic Aneurysms Versus Fenestrated and Branched Endovascular Procedures for Thoracoabdominal Aortic Aneurysms
Supplemental material, sj-docx-2-jet-10.1177_15266028251380519 for A Systematic Review and Meta-analysis of Intraoperative Patient Dosimetric Data in Standard Endovascular Repair for Infrarenal Abdominal Aortic Aneurysms Versus Fenestrated and Branched Endovascular Procedures for Thoracoabdominal Aortic Aneurysms by Fotios O. Efthymiou, Christos F. Pitros, Vasileios I. Metaxas, Constantine N. Antonopoulos, Christos P. Dimitroukas, Stavros K. Kakkos, George S. Panayiotakis and Konstantinos G. Moulakakis in Journal of Endovascular Therapy
Supplemental Material
sj-jpeg-3-jet-10.1177_15266028251380519 – Supplemental material for A Systematic Review and Meta-analysis of Intraoperative Patient Dosimetric Data in Standard Endovascular Repair for Infrarenal Abdominal Aortic Aneurysms Versus Fenestrated and Branched Endovascular Procedures for Thoracoabdominal Aortic Aneurysms
Supplemental material, sj-jpeg-3-jet-10.1177_15266028251380519 for A Systematic Review and Meta-analysis of Intraoperative Patient Dosimetric Data in Standard Endovascular Repair for Infrarenal Abdominal Aortic Aneurysms Versus Fenestrated and Branched Endovascular Procedures for Thoracoabdominal Aortic Aneurysms by Fotios O. Efthymiou, Christos F. Pitros, Vasileios I. Metaxas, Constantine N. Antonopoulos, Christos P. Dimitroukas, Stavros K. Kakkos, George S. Panayiotakis and Konstantinos G. Moulakakis in Journal of Endovascular Therapy
Supplemental Material
sj-jpg-4-jet-10.1177_15266028251380519 – Supplemental material for A Systematic Review and Meta-analysis of Intraoperative Patient Dosimetric Data in Standard Endovascular Repair for Infrarenal Abdominal Aortic Aneurysms Versus Fenestrated and Branched Endovascular Procedures for Thoracoabdominal Aortic Aneurysms
Supplemental material, sj-jpg-4-jet-10.1177_15266028251380519 for A Systematic Review and Meta-analysis of Intraoperative Patient Dosimetric Data in Standard Endovascular Repair for Infrarenal Abdominal Aortic Aneurysms Versus Fenestrated and Branched Endovascular Procedures for Thoracoabdominal Aortic Aneurysms by Fotios O. Efthymiou, Christos F. Pitros, Vasileios I. Metaxas, Constantine N. Antonopoulos, Christos P. Dimitroukas, Stavros K. Kakkos, George S. Panayiotakis and Konstantinos G. Moulakakis in Journal of Endovascular Therapy
Supplemental Material
sj-jpg-5-jet-10.1177_15266028251380519 – Supplemental material for A Systematic Review and Meta-analysis of Intraoperative Patient Dosimetric Data in Standard Endovascular Repair for Infrarenal Abdominal Aortic Aneurysms Versus Fenestrated and Branched Endovascular Procedures for Thoracoabdominal Aortic Aneurysms
Supplemental material, sj-jpg-5-jet-10.1177_15266028251380519 for A Systematic Review and Meta-analysis of Intraoperative Patient Dosimetric Data in Standard Endovascular Repair for Infrarenal Abdominal Aortic Aneurysms Versus Fenestrated and Branched Endovascular Procedures for Thoracoabdominal Aortic Aneurysms by Fotios O. Efthymiou, Christos F. Pitros, Vasileios I. Metaxas, Constantine N. Antonopoulos, Christos P. Dimitroukas, Stavros K. Kakkos, George S. Panayiotakis and Konstantinos G. Moulakakis in Journal of Endovascular Therapy
Supplemental Material
sj-jpg-6-jet-10.1177_15266028251380519 – Supplemental material for A Systematic Review and Meta-analysis of Intraoperative Patient Dosimetric Data in Standard Endovascular Repair for Infrarenal Abdominal Aortic Aneurysms Versus Fenestrated and Branched Endovascular Procedures for Thoracoabdominal Aortic Aneurysms
Supplemental material, sj-jpg-6-jet-10.1177_15266028251380519 for A Systematic Review and Meta-analysis of Intraoperative Patient Dosimetric Data in Standard Endovascular Repair for Infrarenal Abdominal Aortic Aneurysms Versus Fenestrated and Branched Endovascular Procedures for Thoracoabdominal Aortic Aneurysms by Fotios O. Efthymiou, Christos F. Pitros, Vasileios I. Metaxas, Constantine N. Antonopoulos, Christos P. Dimitroukas, Stavros K. Kakkos, George S. Panayiotakis and Konstantinos G. Moulakakis in Journal of Endovascular Therapy
Footnotes
ORCID iDs
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.