
Abstract
Introduction:
Prevertebral left subclavian artery (LSA) occlusion was traditionally performed using conventional coil embolization or vascular plugs. The Penumbra Occlusion Device (POD) is a hybrid coil specifically designed for embolizing high-flow vessels. This study aims to report the technical and clinical success of the POD for LSA embolization during Zone 2 Thoracic Endovascular Aortic Repair (TEVAR).
Materials & methods:
All consecutive patients who underwent LSA embolization using the POD in Zone 2 TEVAR in 2 high-volume aortic centers were retrospectively collected and analyzed. Procedural data and clinical outcomes were collected. The primary endpoint was the technical success rate of LSA embolization using the POD. Secondary endpoints included short-term outcomes and freedom from reintervention. Follow-up was performed with Computed Tomography Angiography (CTA) to confirm successful LSA prevertebral embolization without type Ic endoleak and to assess patency of surgical revascularization of the distal LSA.
Results:
Between January 2020 and April 2024, 37 patients (68% men, median age: 70 years) with degenerative chronic thoracic aortic disease or acute aortic syndromes were included. A single POD was deployed in 49% of cases, primarily via brachial access (81%) using a 4F introducer sheath (68%). In the remaining cases, 1 additional coil was deployed to obtain angiographic occlusion. Technical success of LSA embolization was achieved in 97% of cases, with no evidence of type Ic endoleak on final angiography. At 30-day CTA, 9 patients (24%) had type Ic endoleak: 2 required reintervention with coiling, 4 resolved spontaneously, and 3 were managed conservatively without progression of aortic pathology. Clinical success of LSA embolization at follow-up was 92%, with no reported strokes or transient ischemic attacks. All extra-anatomical bypasses, left vertebral arteries, and distal LSAs remained patent.
Conclusion:
The POD is an effective tool for LSA embolization during TEVAR. This occlusion system offers a promising alternative to traditional methods by overcoming anatomical limitations, potentially eliminating the need for large introducers in upper extremity access and reducing the number of coils required for permanent occlusion of a high-flow vessel.
Clinical Impact
The Penumbra Occlusion Device (POD) represents a practical alternative to conventional coil or plug embolization for large, high-flow vessels. Its design allows controlled deployment through small-caliber access, potentially simplifying the procedure and reducing the number of devices required. This study demonstrates high technical success and acceptable short-term outcomes, suggesting that the POD can achieve reliable left subclavian artery occlusion during Zone 2 TEVAR. These results may guide procedural planning and support wider adoption of the POD as a feasible option in this setting.
Introduction
Endovascular treatment of Ishimaru Zone 2 aortic arch pathologies poses challenges related to left subclavian artery (LSA) revascularization, which is recommended in elective cases according to various clinical guidelines.1–3 Strategies include preserving the LSA using new branched endoprostheses,4,5 Thoracic endovascular aortic repair (TEVAR) with in situ fenestration6–8.or physician-modified TEVAR with LSA fenestration.9,10 In selected cases, intentional LSA coverage, with or without surgical debranching, may also be considered. 11 Surgical revascularization techniques typically involve LSA transposition or left carotid-subclavian bypass; in the latter approach, occlusion of the prevertebral LSA is necessary to prevent retrograde type Ic endoleak.
Among the endovascular options for prevertebral LSA occlusion, traditional methods include coil embolization or vascular plugs. 12 More recently, the Penumbra Occlusion Device (POD, Penumbra Inc, Alameda, California) has emerged as a promising alternative for large and high-flow aortic side branch embolization.
Originally developed for neurovascular vessel occlusions, 13 the POD has since demonstrated safety and efficacy in the proximal embolization of medium-sized vessels across various vascular territories, including splenic, renal, mesenteric, and iliac arteries.14,15 However, to the best of our knowledge, the use of the POD for LSA embolization has not yet been reported in the literature.
This article presents the feasibility and preliminary outcomes of LSA embolization using the POD in aortic arch pathologies requiring Zone 2 TEVAR, based on the experience of 2 high-volume aortic centers.
Materials and Methods
Study Design
All consecutive patients who underwent subclavian artery embolization using the POD at the Vascular Surgery Department of ASST Spedali Civili Hospital (Brescia) and Santa Maria della Misericordia University Hospital (Perugia) between January 2020 and April 2024 were included in this study. The inclusion criterion was the presence of an aortic arch pathology requiring TEVAR with coverage of the LSA and embolization of the prevertebral LSA with POD. No specific exclusion criteria were applied. Baseline patient characteristics, procedural details, and clinical outcomes were retrospectively collected from a shared institutional database.
The primary endpoint was to evaluate the technical success of LSA embolization using the POD system. Secondary endpoints included the assessment of short-term clinical outcomes and freedom from reintervention. The study complied with the Declaration of Helsinki and subsequent amendments. 16 The article adhered to the STROBE reporting guidelines for cross-sectional studies. Due to the retrospective nature of the research and these cases being part of locally approved institutional databases, ethical committee approval was requested and considered unnecessary.
Operative technique and device description
The POD System consists of a 0.020 inch coil implant attached to a detachment pusher and detachment handle, specifically designed according to instructions for use for arterial and venous embolization, especially in large and high-flow arteries. This hybrid coil comes in sizes from 3 to 14 mm wide and lengths from 15 to 60 cm, and it has a double nitinol-coated anchoring part that smoothly connects to a softer packing part. After deployment of the anchoring loops, the soft segment conforms tightly within the vessel to form a dense plug. The POD is fully retrievable before detachment, allowing for repositioning if necessary (Figure 1). Device sizing is based on preoperative contrast-enhanced computed tomography (CT) analyzed on TeraRecon Aquarius iNtuition (TeraRecon Inc, Foster City, California), with inner diameter measurements of the LSA at 3 points: at the origin of the LSA from the aortic arch (D1), at the midpoint between the origin and the first branch (D2) and just proximal to the left vertebral artery or first branch (D3). A 1:1 sizing strategy is used, with preference for matching the LSA diameter at D1 or D2, enabling treatment of vessels up to 14 mm in diameter. The POD is delivered via a microcatheter inserted through a minimum 4F sheath, typically introduced through upper extremity access (ie, radial). Digital subtraction angiography is performed to identify the LSA collaterals and the vertebral artery. The microcatheter is advanced to the LSA origin, and the POD is deployed under fluoroscopic guidance. Final angiography confirms proper POD placement and successful embolization of the subclavian artery (Figure 2). If retrograde flow into the aortic arch persists, additional coiling with a POD or packing coil (Penumbra Inc) may be performed. No additional technical considerations are necessary in the presence of an aberrant right subclavian artery.
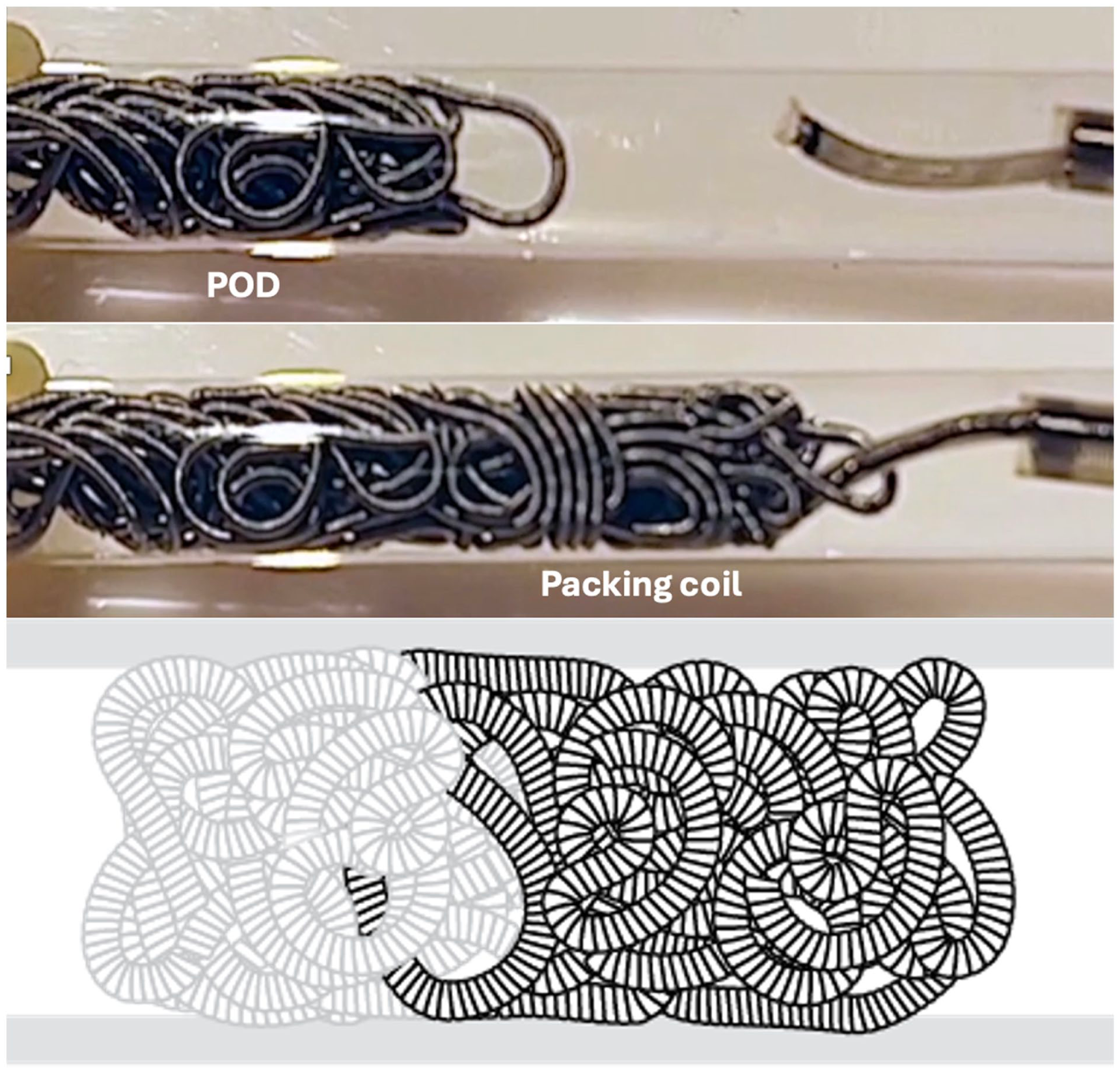
Deployed Penumbra Occlusion Device (POD) with anchor and packing segments in place, supported by a packing coil backstop to enhance vessel occlusion.
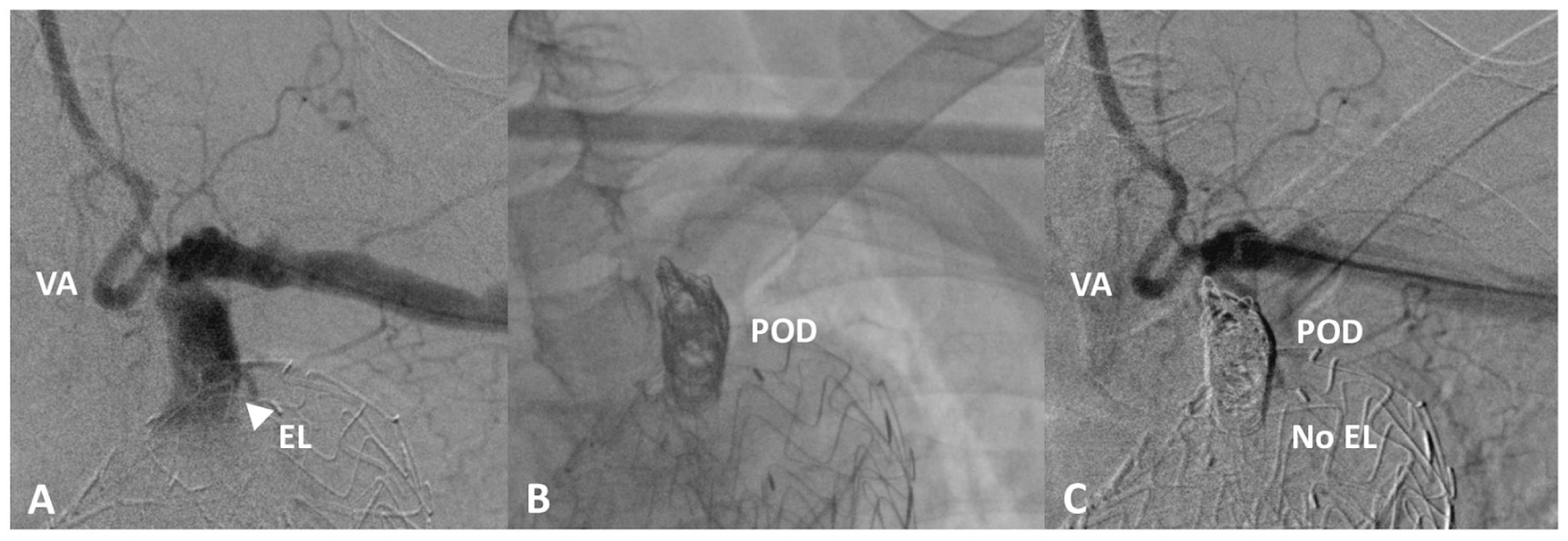
A. Zone 2 TEVAR with type Ic endoleak from covered LSA; B. Prevertebral LSA occlusion with POD; C. LSA occlusion without type Ic endoleak.
Endovascular aortic repair, aimed at exclusion of the thoracic aortic pathology, is performed either before or after LSA embolization according to the operator’s preference. Notably, the anchoring segment allows for POD deployment even in the absence of a stent graft in situ (Figure 1).
Evaluation of Treatment and Patient Follow-up
Technical success was assessed separately for both LSA embolization and the TEVAR procedure, based on predischarge and postoperative CT angiography. Definitions followed Reporting Standards for Endovascular Aortic Aneurysm Repair. 17
Primary technical success was defined as meeting all of the following criteria within the first 24 hours postprocedure:
- Complete embolization of the prevertebral LSA without evidence of retrograde type Ic endoleak. In this study, the term type Ic endoleak, though traditionally associated with iliac artery interventions, refers to persistent retrograde flow into the excluded aortic segment from the LSA following its intentional coverage during TEVAR, consistent with prior literature advocating for its broader application beyond the iliac territory;
- Patency of the vertebral artery and proximal LSA collaterals;
- Patency of the surgical LSA revascularization.
Clinical success was defined as sustained LSA occlusion at follow-up imaging, including cases requiring additional embolization to achieve complete occlusion (assisted primary closure).
Short-term outcomes included 30-day clinical results in accordance with Society for Vascular Surgery (SVS) TEVAR outcome reporting standards, as well as procedure-related upper extremity access complications.
Results
The study included a total of 37 patients. Twelve patients (32%) were women, with a median age of 70 (range=66-79) years. Demographics and cardiovascular risk factors are summarized in Table 1. Thirty patients (81%) underwent elective TEVAR. The primary indication was degenerative thoracic aortic aneurysm in 22 cases (60%). The remaining indications included aortic dissection (5 patients, 14%), aortic trauma (3 patients, 8%), penetrating aortic ulcer (2 patients, 5%) and pseudoaneurysm (2 patients, 5%). The mean diameter of the subclavian artery at D1 was 12 mm (range=12-14.5 mm). Aberrant subclavian anatomy was present in 2 patients (5%). Anatomical data from preoperative CT angiography are summarized in Table 2. Proximal sealing was achieved predominantly in Zone 1 or 2 (24 patients; 65%). In 28 cases (76%), LSA embolization was performed after TEVAR.
Demographics and Cardiovascular Risk Factors.
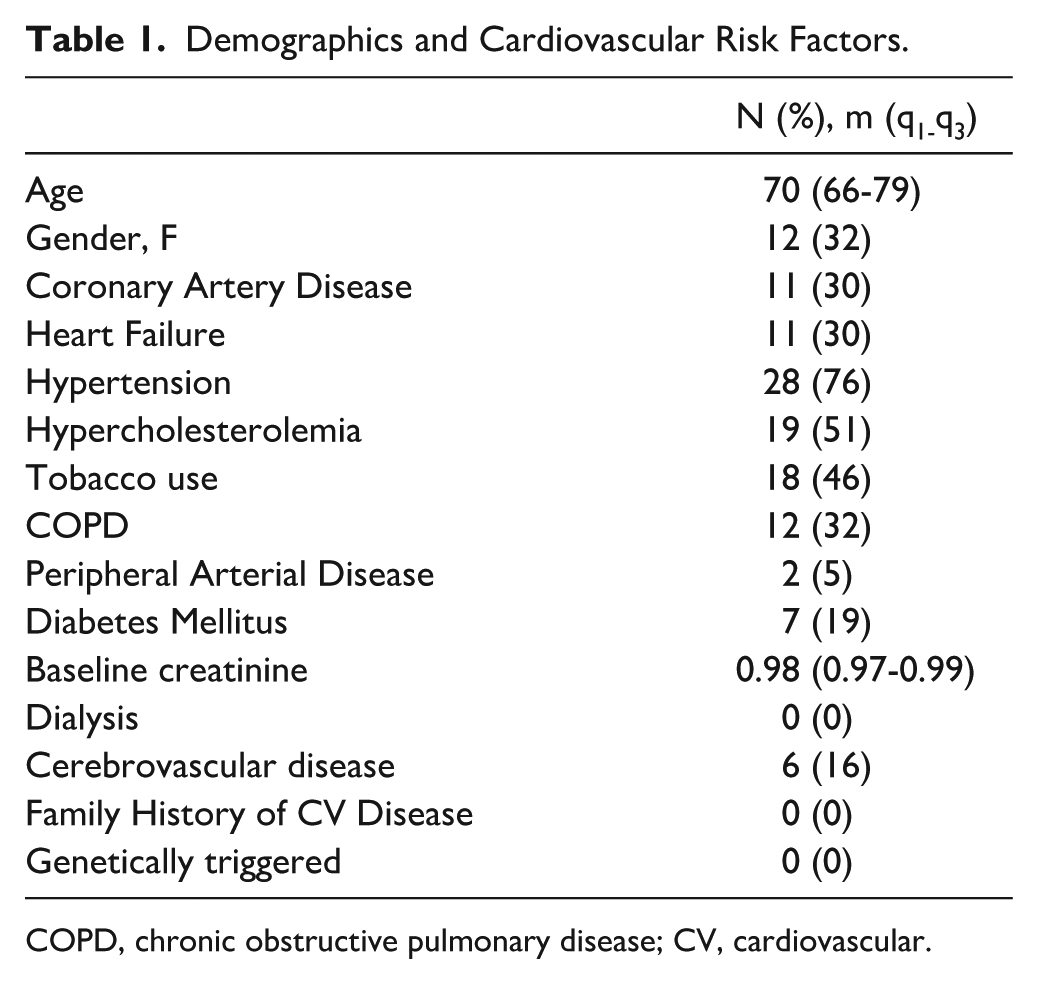
COPD, chronic obstructive pulmonary disease; CV, cardiovascular.
Preoperative LSA Anatomy and Aortic Pathology Characteristics.
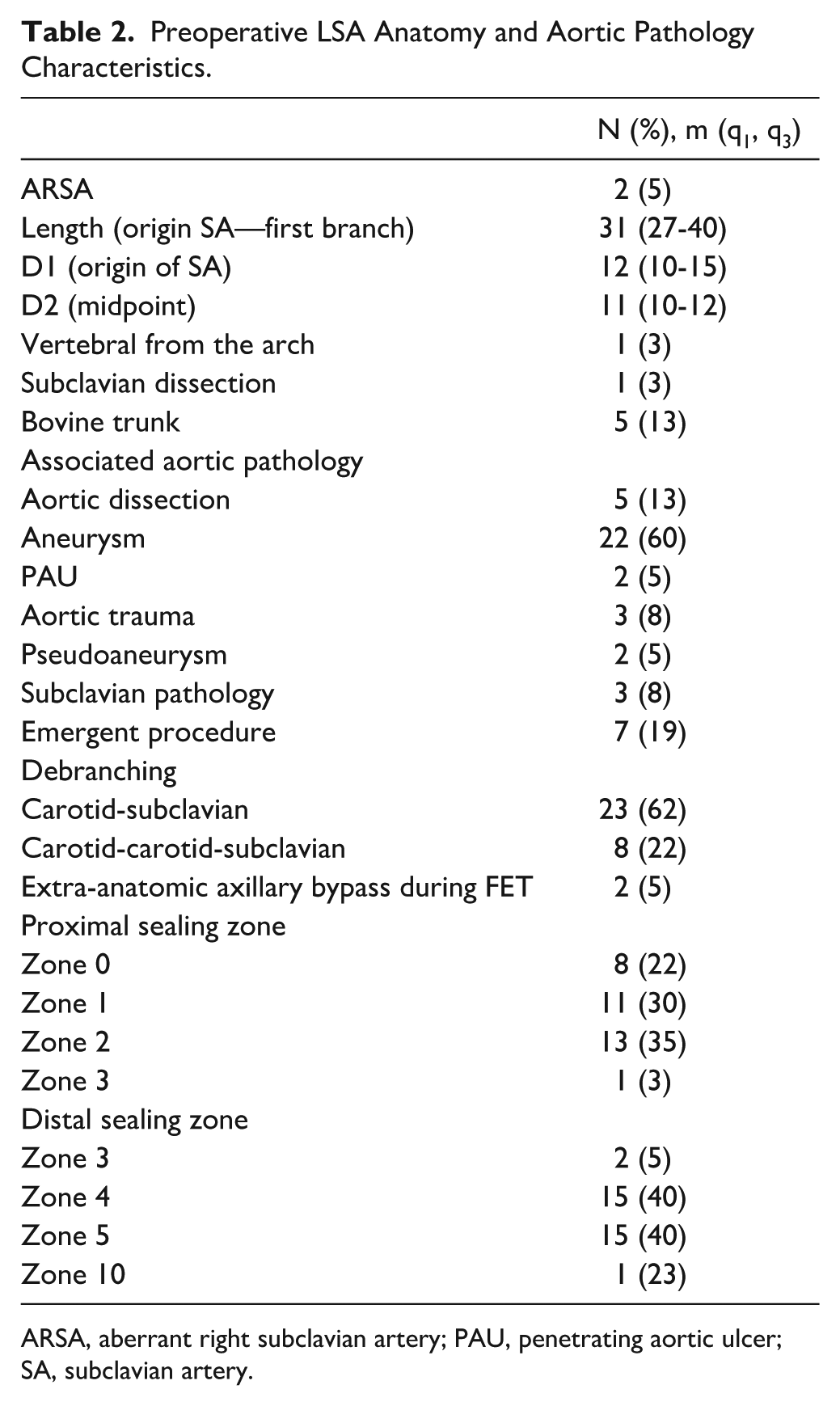
ARSA, aberrant right subclavian artery; PAU, penetrating aortic ulcer; SA, subclavian artery.
Primary technical success of the TEVAR procedure was achieved in 34 patients (92%). Two patients experienced partial coverage of the left common carotid artery (LCCA), and 1 case of inadvertent coverage of the innominate artery required bailout chimney stenting. Three patients (8.1%) experienced access-related complications involving iliofemoral arteries.
The POD delivery was primarily achieved through percutaneous upper extremity access (31 patients, 83%), with overall upper extremity used in 35 patients (95%). The brachial artery was the most commonly used access site (30 patients, 81%), typically using a 4F introducer sheath (23 patients, 68%). A single POD was sufficient to achieve LSA occlusion in 18 patients (49%). Among the remaining 19 patients: one required 2 PODs for complete embolization; 18 required additional coils in conjunction with the POD: in 17 cases, a single additional Penumbra packing coil was used, of 30 cm in 7 patients and 60 cm in 10; 1 patient required 2 additional Penumbra packing coils (30 cm and 60 cm). Intraprocedural details are summarized in Table 3. Two patients (5%) reported paresthesia in the median nerve distribution related to brachial access. No strokes or transient ischemic attacks were observed within 30 days postprocedure.
Intraprocedural Data.
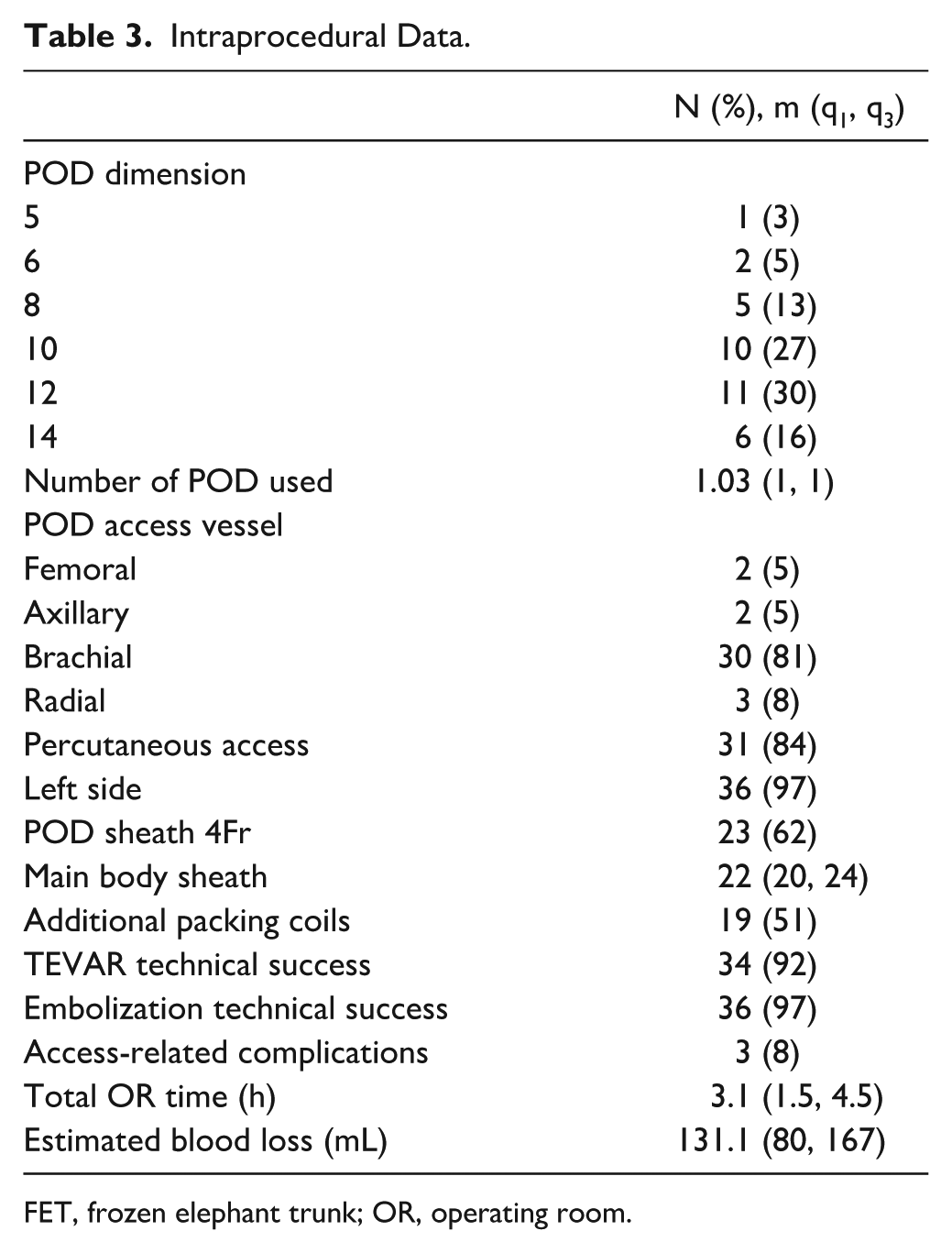
FET, frozen elephant trunk; OR, operating room.
Final intraoperative angiography confirmed the primary technical success of LSA embolization in 36 out of 37 (97%) cases. Nine patients (24%) presented type Ic endoleak at predischarge computed tomography angiography (CTA). Among these, 4 (11%) resolved spontaneously by the first follow-up CTA. Two patients required reintervention with an additional embolization at 3 and 49 days after the index procedure. Both had initially received a single POD, and reintervention was successfully completed with packing coils. This resulted in a clinical success rate of 92% with assisted primary closure at 6-month follow-up.
All extra-anatomical bypasses remained patent at both 30-day and 6-month evaluations. The mean follow-up duration was 13 ± 11 months. In-hospital, short-term, and >30 days outcomes are summarized in Table 4.
In-hospital, Short-term and >30 Days Outcomes.
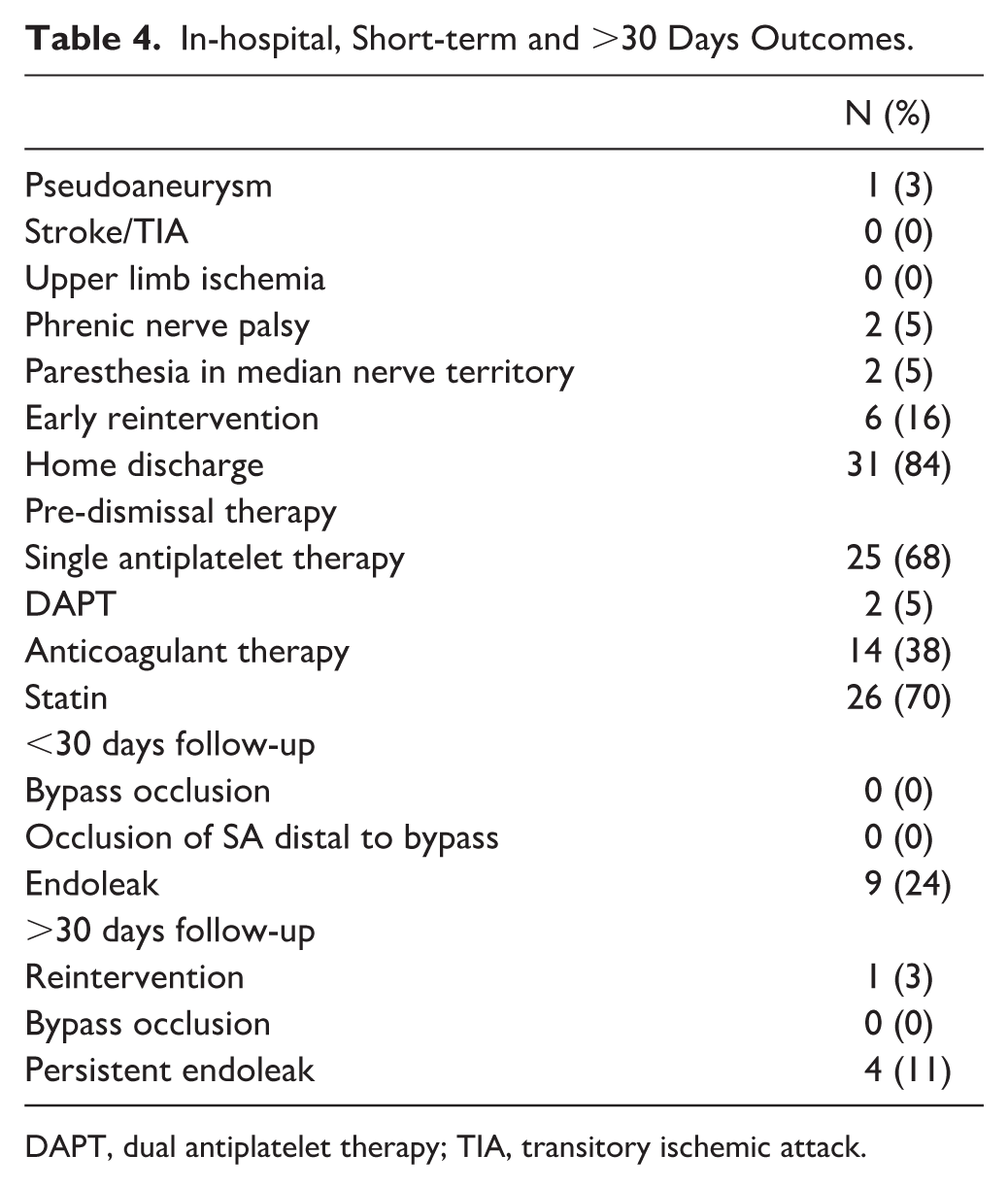
DAPT, dual antiplatelet therapy; TIA, transitory ischemic attack.
Discussion
This study reports on 37 cases of POD device use for LSA embolization during TEVAR procedures for various acute and chronic aortic pathologies. Primary LSA embolization technical success was achieved in 36 patients (97%), with no strokes or transient ischemic attacks recorded at 30 days. Lower TEVAR technical success (92%) may reflect the greater complexity of TEVAR procedures, which require precise graft deployment in challenging aortic arch anatomy. These maneuvers carry a higher risk of complications such as inadvertent coverage of branch vessels or access-related issues, as observed in our series.
The LSA embolization was predominantly performed via percutaneous brachial artery access using a small sheath (4F). A single POD was sufficient to achieve occlusion in approximately half of the cases, while the remainder required an additional coil, resulting in an assisted primary clinical success rate of 92%. Notably, both patients who required reintervention during follow-up had initially received a single POD.
The LSA embolization was initially performed using conventional coil embolization (CCE), 18 which often required deployment of multiple coils or a combination with other occlusion devices. 19 However, distal coil migration in high-flow vessels was a frequently reported complication, making prior TEVAR deployment preferable. 20 To address these limitations, Amplatzer Vascular Plugs (AVPs; St. Jude Medical, St. Paul, Minnesota) began to be used to treat type Ic endoleaks from the LSA after TEVAR 21 demonstrating results comparable with coil embolization. 22 The main advantage of AVPs lies in their capacity to achieve occlusion with a single device 22 ; however, this comes at the cost of requiring larger delivery systems and longer prevertebral LSA segments for deployment. 23
Recently, the POD (Penumbra Inc, Alameda, California) has emerged as a promising alternative for vessel embolization, particularly in large, high-flow arteries where conventional coils are prone to migration. The POD consists of a 0.020 inch system with a stiff distal anchoring segment and a double nitinol loop designed to engage the vessel wall.
Selection of the optimal embolization device depends on several factors.
First, high-flow environments increase the risk of inadvertent embolic device migration. Amplatzer Vascular Plugs, with their self-expanding nature and high radial force, are rarely displaced even in high-flow settings. 24 Coils, by contrast, are more vulnerable to migration and are generally favored for use in low-flow arteries. 25 PODs offer a hybrid solution: their anchoring segment provides reliable fixation, reducing the likelihood of distal migration even in dynamic flow conditions.
Second, the size of the required delivery system influences access trauma and associated complications. Amplatzer Vascular Plugs necessitate 6F and 7F sheaths depending on plug size, resulting in thrombosis of percutaneous radial access in 54% of 7F cases and 32% of 6F cases. 26 For patients requiring a 6-7F sheath via a brachial artery approach, percutaneous brachial access carries a 10% complication rate; 27 open surgical exposure with primary brachial repair may be preferred to reduce the incidence of postprocedural access complications requiring reintervention. 28 In contrast, POD’s compatibility with a 4F platform minimizes, similarly to coils, arterial trauma and lowers the rate of access-related complications.
Third, the optimal embolization method depends on the size and length of the prevertebral LSA, which shows a significant variability. 29 One study found that LSA length was <40 mm in 28% of cases. 26 AVPs require relatively straight vessel segments of approximately 46 ± 5 mm in length, 21 which may limit their feasibility in shorter vessels. Coils and PODs are more anatomically adaptable and better suited for tortuous or short LSA segments.
Last, the number of devices needed to achieve complete occlusion varies widely across different embolization options. Amplatzer Vascular Plugs generally achieve occlusion with a single device, while coil-based strategies can be resource-intensive. For example, internal iliac artery embolization has been shown to require an average of 1.4 AVPs versus 7.5 coils. 24 LSA embolization with coils may require approximately 10 ± 3 coils per case, translating to an 80% increase in procedural cost compared with AVPs. 22 PODs, by contrast, have demonstrated reduced device usage, with an average of 2 PODs and a median of 4 (range=0-13) additional standard coils reported in neurovascular applications. 13
The rationale for selecting the POD over traditional embolization devices lies primarily in its ability to address anatomical and procedural limitations commonly encountered during zone 2 TEVAR. 19 However, few studies to date have evaluated POD use in medium-sized vessels,13–15 and to our knowledge, no prior series have reported on their application in the LSA. Our multicenter study demonstrated the feasibility and effectiveness of POD use for LSA embolization during TEVAR, with a competitively low incidence of short-term and >30 days complications and reinterventions. Limitations include its retrospective design and the relatively small sample size, which limit the generalizability of the findings; additionally, the short follow-up period restricts assessment of long-term outcomes, including late complications or device durability. Lastly, the absence of a comparator group prevents direct comparison with other embolization techniques such as coils or AVPs.
Conclusions
The POD represents a valuable addition to the endovascular armamentarium for embolizing large, high-flow vessels. Its ability to achieve effective occlusion without migration, coupled with minimal anatomical limitations related to access vessel size or target vessel dimensions, makes it a viable alternative to currently available embolization devices. The results from this preliminary cohort demonstrate that POD can be used effectively for embolization of the prevertebral LSA, serving as a preventive strategy against type Ic endoleak following endovascular exclusion of distal aortic arch pathologies requiring a zone 2 landing zone.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.