
Abstract
Purpose:
To investigate the safety and performance of multilayer stents in patients with type B aortic dissection (TBAD) and high-risk features.
Materials and Methods:
Prospective, multicenter, single-arm clinical trial. All patients were identified, treated, and managed according to each site’s standard procedures for thoracic endovascular aortic repair (TEVAR). Clinical and radiographic evaluations were performed to assess the device safety and its technical and clinical performance. All computed tomography (CT) scans were analyzed by an independent imaging core laboratory. Statistical analyses were performed by an independent statistician based on predefined analysis plans. The intention-to-treat cohort was used to analyze device safety and technical success, and the per-protocol cohort for technical and clinical performance.
Results:
Twenty-seven participants (21 males, 6 females; mean [SD] age: 51.4 [13.2] years) were enrolled. The dissection extended distally into the abdominal aorta in all evaluable participants. Mean (SD) follow-up was 54.9 (10.2) months for the intention-to-treat cohort and 54.1 (13.6) months for the per-protocol. A total of 63 aortic multilayer stents were implanted (mean [SD] of 2.3 (0.7) per participant). In 94.7% of the participants, the aorta was treated distally up to zone 9. Technical success was achieved in all but 1 participant (96.3%). No ischemic events (paraplegia/paraparesis or stroke) were observed, neither within 30 days nor during the follow-up period. Seven participants (25.9%) had 1 serious adverse event more than 30 days postoperatively; of these, 4 were possibly or probably device-related. Estimated 5-year survival was 90%. No device deficiencies (eg, stent kinking, collapse, fracture, migration, or separation) were reported. No dissection extension occurred. Stable or decreasing maximum transverse aortic diameter at last follow-up was observed in 78.6% of participants. Distal flow was preserved in 98.3% of major side branches. All participants were free from aortic rupture, reintervention, and open conversion during the long-term follow-up.
Conclusion:
Treatment of high-risk TBAD patients with multilayer stents is feasible, has an acceptable safety profile, and stabilizes the dissection. Further research is warranted to confirm these findings in other populations of patients.
Clinical Impact
New therapeutic options are needed to meet the ACC/AHA primary goals for thoracic endovascular aortic repair (TEVAR) in patients with type B aortic dissection (TBAD) extending into the abdominal aorta, namely, to prevent aortic rupture, retrograde extension, and antegrade propagation and alleviate malperfusion. The findings of this study indicate that these goals can be met in patients with high-risk TBAD by using multilayer stents, as these devices allow to treat extensively the dissected aorta with adequate survival, a low risk of ischemic complications, and stabilization of the transaortic diameter over long-term follow-up. Interestingly, multilayer stents can meet these clinical goals without sealing the primary tear or inducing complete false lumen thrombosis. The unique design characteristics and mechanism of action offer a new approach to TEVAR treatment for patients with TBAD.
Keywords
Introduction
Aortic dissection is a rare but life-threatening disease. It arises from an entry tear that causes blood to enter the aortic wall behind the intimal layer and consequently creating a false lumen (FL) through which blood flows. Over time, the FL expands, compressing the true lumen (TL).1,2
In type B aortic dissections (TBAD), the entry tear is located distal to the left subclavian artery (LSA) and can progress as the FL propagates in the retrograde (proximally) or antegrade (distally) direction. As a result, TBAD can evolve to affect most of the aorta down to its abdominal segment. The acute management of patients with TBAD is driven by the presence or absence of complications (aortic rupture or malperfusion syndrome). Over the last years, the use of Thoracic EndoVascular Aortic Repair (TEVAR) has become more widespread than traditional open surgery thanks to TEVAR lower complication and mortality rates. Today, TEVAR is the recommended treatment in patients with complicated TBAD and suitable anatomy.1,3
In the absence of complications (ie, uncomplicated TBAD), medical treatment remains the gold standard. In patients with uncomplicated TBAD who have features indicative of a high risk to develop complications, the latest guidelines indicate that TEVAR may be considered in the subacute phase (15-90 days after symptoms onset).1,3
Current options for TEVAR rely on the use of impermeable stent grafts to seal the primary entry tear. However, when the dissection extends into the abdominal aorta, the absence of treatment in the dissected abdominal segment will frequently lead to disease progression (eg, aneurysmal growth) and necessitate reinterventions. Attempts have therefore been made to complement the use of stent grafts with bare metal stents in the dissected abdominal segment (ie, Provisional ExTenTion to Induce COmplete ATtachment—PETTICOAT approach). Unfortunately, long-term results with this approach have frequently shown continued progressive dilatation of the abdominal aorta.4,5
New therapeutic options are therefore still needed to help meet the primary goals of TEVAR as stated in the 2022 ACC/AHA guidelines: “to prevent (or treat) aortic rupture, prevent retrograde extension of the dissection into the aortic root, prevent antegrade propagation of the dissection into distal yet undissected segments, and alleviate malperfusion syndromes.” 1
The multilayer stent (MFM; Cardiatis, now Intressa Vascular; Gembloux, Belgium) is a self-expanding, multilayer, cobalt alloy stent consisting of a 3-dimensional (3D) braided wire mesh. Early users hypothesized that the stent’s unique mechanical properties were well suited for the treatment of aortic dissection. 6 Indeed, its properties allow the multilayer stent to reapproximate the dissection flap to the aortic wall and provide mechanical support to the aortic wall, which reopens the TL and recentralizes blood flow to the TL. The open mesh and 3D porosity of the stent enable extensive coverage of the dissected aorta, including where side branches originate while ensuring their patency. Early user experience with the stent in patients with aortic dissection 7 led the device manufacturer to initiate a prospective multicenter study to investigate the safety and performance (technical and clinical) of the multilayer stent in patients with TBAD and high-risk features. The objective of this article is to report the long-term outcomes of this study.
Materials and Methods
Trial Design
The study is a prospective, multicenter, single-arm clinical trial conducted at 3 tertiary centers in Europe. Patients with TBAD referred to the above-mentioned clinical sites for treatment were considered for enrollment in the study, and if eligible, approached to participate in this trial. Scheduled evaluations were performed pre-implantation (baseline visit), at hospital discharge, and during follow-up visits at 6 months, 12 months, and yearly thereafter up to 5 years post-implantation. Computed tomography (CT) scans were performed as per site practices. Patients were enrolled between January 2016 and September 2019. Due to restrictions placed by the COVID-19 pandemic, follow-up visits were only performed until February 2020. In 2022, ethics committee approval was obtained for a protocol amendment to resume patient follow-up. Patients were contacted and asked to reconsent. Those who reconsented were evaluated during an onsite follow-up visit in 2022. Results from all patients enrolled and followed up in 2022 are presented in this article.
Ethics
The study was conducted in compliance with the principles of the Declaration of Helsinki, Good Clinical Practice, the study’s clinical investigational plan, and requirements of the approving ECs and regulatory authorities. Written informed consent was obtained from each participant before any study-specific procedures or assessments were conducted and, specifically, before the participant was treated with MFM stents. All collected and analyzed data were pseudonymized.
Study Participants
Eligibility was based on predefined inclusion and exclusion criteria. Key inclusion criteria were age >18 years; TBAD; dissection symptom onset more than 30 days (which was considered chronic at the time of study design); 8 at least one of the following high-risk factors: poorly controlled hypertension, refractory back or chest pain, expansion of the FL diameter (False Lumen diameter >20 mm) and total diameter of the aorta (ie, maximal aortic diameter >40 mm), or partial thrombosis of the FL; healthy (ie, undissected) proximal and distal landing zones; and adequate arterial anatomy to perform TEVAR with the multilayer stent (MFM) (ie, allowing vascular access, navigation of the delivery system, and deployment of the device). Key exclusion criteria were stage 4 or 5 renal insufficiency; aorta rupture; aortic root aneurysm; untreated pleural effusion at the time of the scheduled procedure; presence/suspicion of connective tissue disorders; or previously implanted stent grafts.
Device Description
The MFM multilayer stent, now known as the Allay Aortic Stent (Intressa Vascular, formerly Cardiatis, Belgium), is a radiopaque, tubular, bare stent composed of interlaced layers of braided cobalt-chromium alloy wires (Phynox) with flared anchoring ends and 3D porosity (Figure 1). Stents of different lengths and diameters are available and are delivered through an 18/20Fr delivery system.
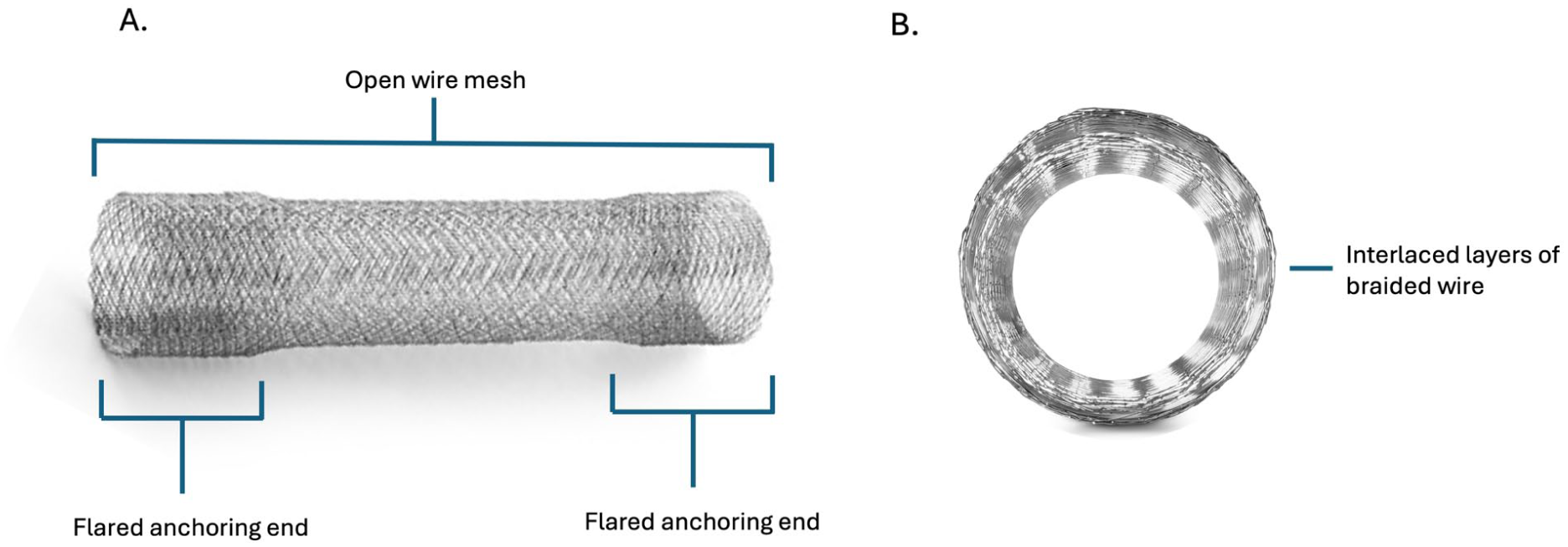
Design of the multilayer stent (MFM, now Allay Aortic Stent): (A) longitudinal view showing the flared anchoring ends and open wire mesh that translates into 3D porosity; and (B) cross-sectional view of the multilayer stent. The self-expanding technology provides mechanical support to the aortic wall.
Two key design features of the stent are (1) its mechanical properties that allow the stent to provide mechanical support to the aortic wall and (2) the open multilayer mesh that translates into 3D porosity. Upon placement in the aorta, the stent reopens the compressed TL, reducing the FL and recentralizing blood flow in the TL. The 3D porosity of the stent allows branch perfusion to be preserved in both single and overlapped configurations. In combination, these 2 features allow extensive treatment of the aortic dissection to provide columnar support to the aorta, aiming at reducing reintervention for dissection extension and aneurysm degeneration with a low risk of ischemic events.
Implantation Procedure
All patients were treated according to each site’s standard procedures for TEVAR (including prescription of anticoagulant and antithrombotic therapies). Baseline CT scans were sent to the sponsor for procedure planning recommendation (number, model, and appropriate oversizing of stents based on patient-specific dissection length and recommended sizing table in Instructions for Use [IFU]). Implantation of the multilayer stents was performed as described in the device IFU (compliant balloon was used as per investigator’s discretion to further dilate the stent). Postoperative anticoagulant and antithrombotic therapies were prescribed as per site standard of care after TEVAR.
Outcome Parameters
Device safety was evaluated over time based on the following outcome parameters: (1) incidence of ischemic events (including renal failure requiring dialysis, visceral ischemia requiring surgical intervention, stroke, limb ischemia, and paraplegia); (2) incidence of serious device- or procedure-related adverse events (AEs); (3) change in distal flow in major branches covered with the device between baseline and follow-up (based on the presence or absence of blood flow in the peripheral branches of the artery); (4) incidence of new entry tears; and (5) incidence of retrograde type A aortic dissection (RTAD).
Device technical performance was assessed over time by the following: (1) technical success defined as the successful introduction and deployment of the device at the intended aortic segment with successful coverage of the primary tear site; (2) extent of treatment coverage; (3) change in the diameter of the TL at the plane of maximum compression (PMC); and (4) incidence of device deficiencies defined as loss of stent patency, or stent kinking, collapse, fracture, or migration, or loss of stent overlap.
Clinical performance, and benefit, of the device during the follow-up period were evaluated by the following parameters: (1) overall survival; (2) freedom from aortic rupture; (3) freedom from aortic reintervention; (4) freedom from open conversion; (5) freedom from aortic growth since hospital discharge, where aortic growth was defined as an increase in the maximum transverse aortic diameter of 5 mm or more; and (6) incidence of dissection extension beyond treated aortic segment.
Data Analysis
All CT scans were analyzed by an independent imaging core laboratory (Astute Imaging, USA) based on predefined imaging endpoints. AEs were assessed as to their relation to a pre-existing or unrelated condition or related to the procedure and/or device. In addition, AEs were analyzed according to their occurrence over time, for example, perioperatively, within the first 30 days postoperatively, or later follow-up timepoints. Study data were source-verified during site monitoring visits.
All statistical analyses were performed by an independent statistician (ECSOR, Belgium) using IBM SPSS Statistics (Version 27.0 or higher) based on predefined plans. Missing values were not replaced or extrapolated. Patient-related baseline variables and surgical procedures were analyzed using data from both the intention-to-treat (ITT) and per-protocol (PP) cohorts. The ITT cohort was used to analyze safety data and technical success and the PP cohort for the remaining technical and clinical performance parameters. The primary analyses were based on descriptive techniques (using mean, median, standard deviation, minimum, and maximum values for continuous variables and using N, n, and % for discrete variables). Changes vs baseline were assessed using Friedman’s tests; when results of continuous and discrete ordinal variables were significant, post-hoc Wilcoxon’s tests were performed, and in the case of discrete nominal variables, McNemar’s tests were performed. Cumulative probabilities of success were estimated in accordance with the Kaplan-Meier method to account for stops due to the different numbers of follow-up visits per participant and censored data. Variability around the mean and median survival time was calculated using corresponding formulas.
Results
Participant Flow
A total of 27 participants were enrolled and treated (ITT cohort). Of these, 3 were withdrawn shortly after the procedure due to suspicion of connective tissue disorder (n=1) and treatment with devices other than multilayer stents (n=2). An additional 4 participants were also withdrawn over the course of the follow-up period: another participant for suspicion of a connective tissue disorder and 3 others for being identified by the Imaging Core Laboratory as having a perforating aortic ulcer (PAU). Thus, 20 participants fulfilled the eligibility criteria and formed the PP cohort for performance analysis.
Attrition over the course of the study was due to participant death (n=3; 2 in PP cohort), being lost to follow-up (n=2), or being unable to attend the 2022 follow-up visit (n=2). In the ITT cohort, mean (SD) follow-up duration after the procedure was 1671 (309) days (54.9 [10.2] months) and in the PP cohort, it was 1645 (415) days (54.1 [13.6] months). Participant flows for the ITT cohort and for the PP cohort are presented in Figure 2A and Figure 2B, respectively.
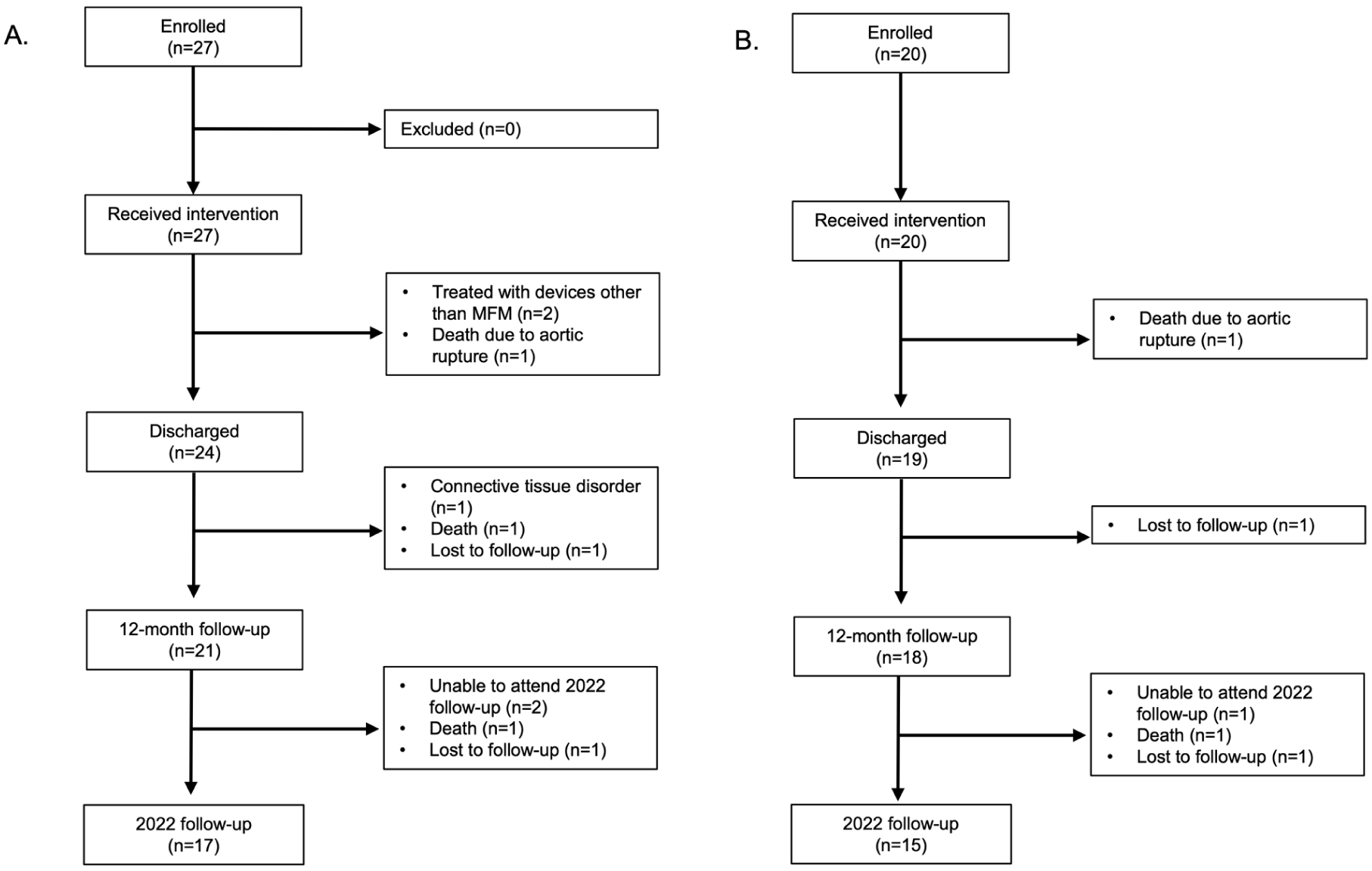
Participant flow in the study up to the resumed follow-up in 2022 for the (A) intention-to-treat cohort and (B) per-protocol cohort.
Participant Characteristics
Baseline demographics and past medical history of the ITT and PP cohorts are presented in Table 1. Based on the ITT cohort, a majority (77.8%) of the study population was male and the mean (SD) age was 51.4 (13.2) years. Mean (SD) body mass index (BMI) indicated participants were slightly overweight (30.4 [5.7] kg/m2). The 3 most common comorbidities were hypertension (85.2%), hyperlipidemia (37.0%), and congestive heart failure (25.9%). Six participants (22.2%) had a history of previous heart valve replacement or aortic treatment. All patients were on beta-blockers and a majority on angiotensin-converting enzyme (ACE) inhibitors (64.0%) and calcium channel blockers (60.0%). Nearly all (96.3%) were classified as having TBAD with high-risk features and 74.1% were asymptomatic. Based on current definitions of disease chronicity,2,9 63.0% were categorized as having subacute TBAD, 25.9% as chronic, and 7.4% as acute.
Baseline Demographics, Past Medical History, and Clinical Characteristics of the Intention-to-Treat and Per-Protocol Cohorts.
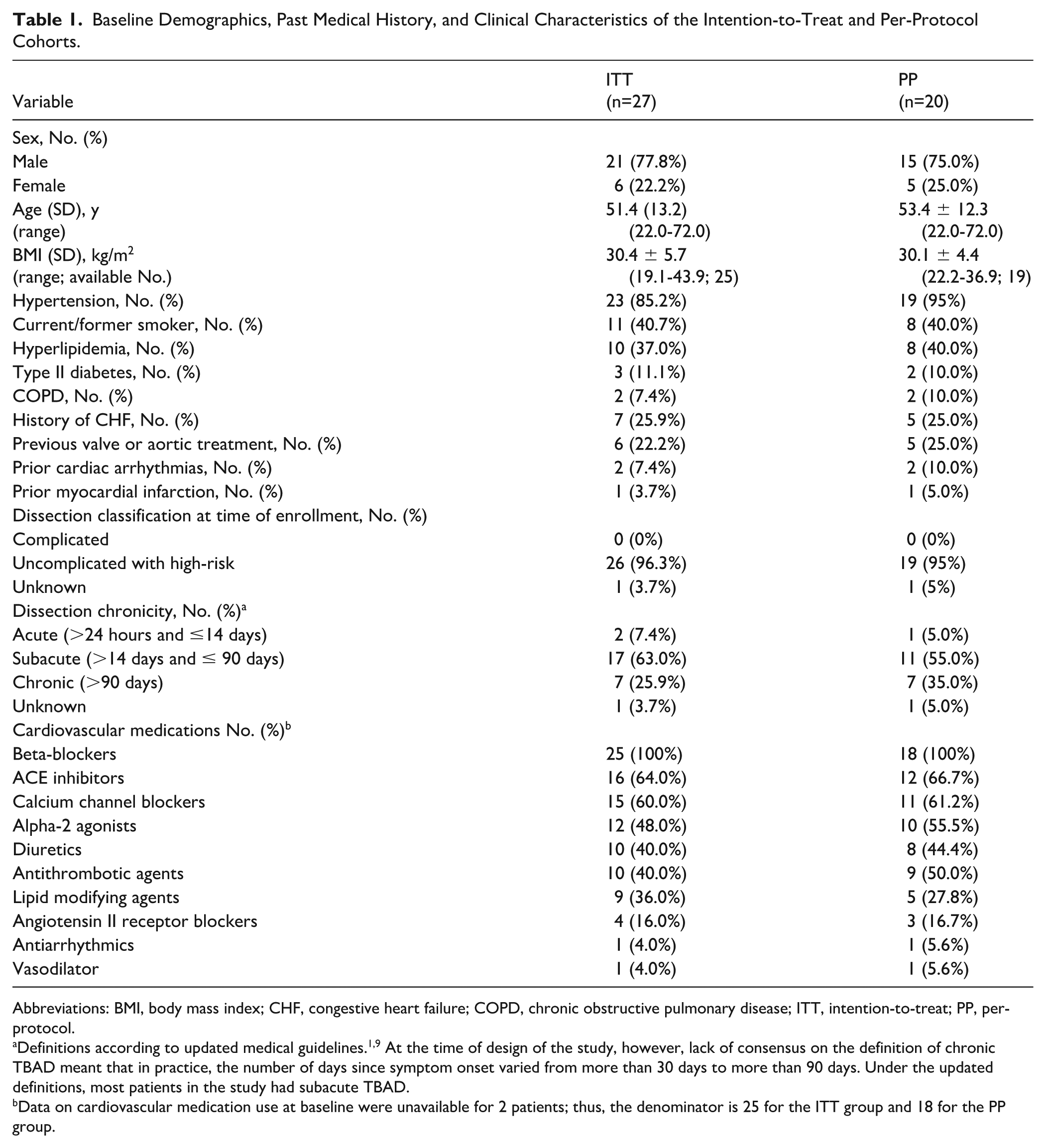
Abbreviations: BMI, body mass index; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; ITT, intention-to-treat; PP, per-protocol.
Definitions according to updated medical guidelines.1,9 At the time of design of the study, however, lack of consensus on the definition of chronic TBAD meant that in practice, the number of days since symptom onset varied from more than 30 days to more than 90 days. Under the updated definitions, most patients in the study had subacute TBAD.
Data on cardiovascular medication use at baseline were unavailable for 2 patients; thus, the denominator is 25 for the ITT group and 18 for the PP group.
Clinical Presentation of the Per-protocol Cohort
With regard to the 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease categories of high-risk factors, 1 maximal aortic diameter was wider than 40 mm in 50%. Primary entry tears were greater than 10 mm in 78.6% who had visible tears and greater than 20 mm in 28.6%.
At baseline, mean diameters of the aortic arch and iliac and femoral arteries were within normal range. Mean (SD) length of the dissections was 364.9 (52.9) mm with the proximal end of the dissection located in the ascending aorta in 20.0% of participants and in zone 3 in 50.0%. The dissection extended distally to zone 6 or further (abdominal aorta) in 100.0% of participants and into the iliac arteries in 60.0%. The FL was significantly compressing the TL: the mean (SD) diameter of the TL at the PMC was 8.0 (4.9) mm, while that of the FL was 21.7 (8.6) mm. Maximum transverse aortic diameter was greater than or equal to 50 mm in 26.3% and greater or equal to 55 mm in 10.5% of participants, and the FL was (fully) patent in all participants. Among the 14 participants with visible primary entry tears, all tears were located in the descending thoracic aorta. Five participants did not have a primary tear, as they presented with a residual dissection (ie, dissection after graft repair of the ascending aorta for type A aortic dissection extending in the descending aorta).
With respect to the perfusion and patency of side branches, 21.7% of major aortic sides branches (brachiocephalic artery [BCA], left common carotid artery [LCCA], LSA, celiac trunk [CT], superior mesenteric artery [SMA], inferior mesenteric artery [IMA], left renal artery [LRA], right renal artery [RRA]) were fed from the FL either partially or completely. Perfusion of the LRA was solely from the FL or both TL and FL in 26.3% of participants each. Perfusion into the RRA was solely from the FL in 5.3% and from both lumens in 21.0%. Perfusion into the IMA was from the FL in 26.3% of participants and from both lumens in 5.3%. The CT was occluded in 1 participant.
At baseline, 19 of 152 (12.5%) major aortic branches were dissected; the most commonly dissected branches were the LRA and LSA (occurring in 21.1% of participants each). In addition, stenosis was observed at 7 (4.6%) major aortic branch ostia. Complete stenosis of the IMA was found in 15.8% of participants and the CT in 5.3%. Partial stenosis of the SMA was observed in 10.6% of participants and the CT in 5.3%. Finally, 2 (1.3%) major aortic branches (1 IMA and 1 LRA in 1 [5.3%] participant each) had no distal flow at baseline.
Procedure
A total of 63 aortic multilayer devices were implanted in the 27 participants. The mean (SD) number of aortic devices was 2.3 (0.7). In 63.2% of participants, the landing of the most proximal stent was in the ascending aorta, and in 36.8%, it was in the aortic arch (all in Ishimaru zone 2). The aorta was treated distally up to zone 9 in 94.7% of participants (Figure 3).
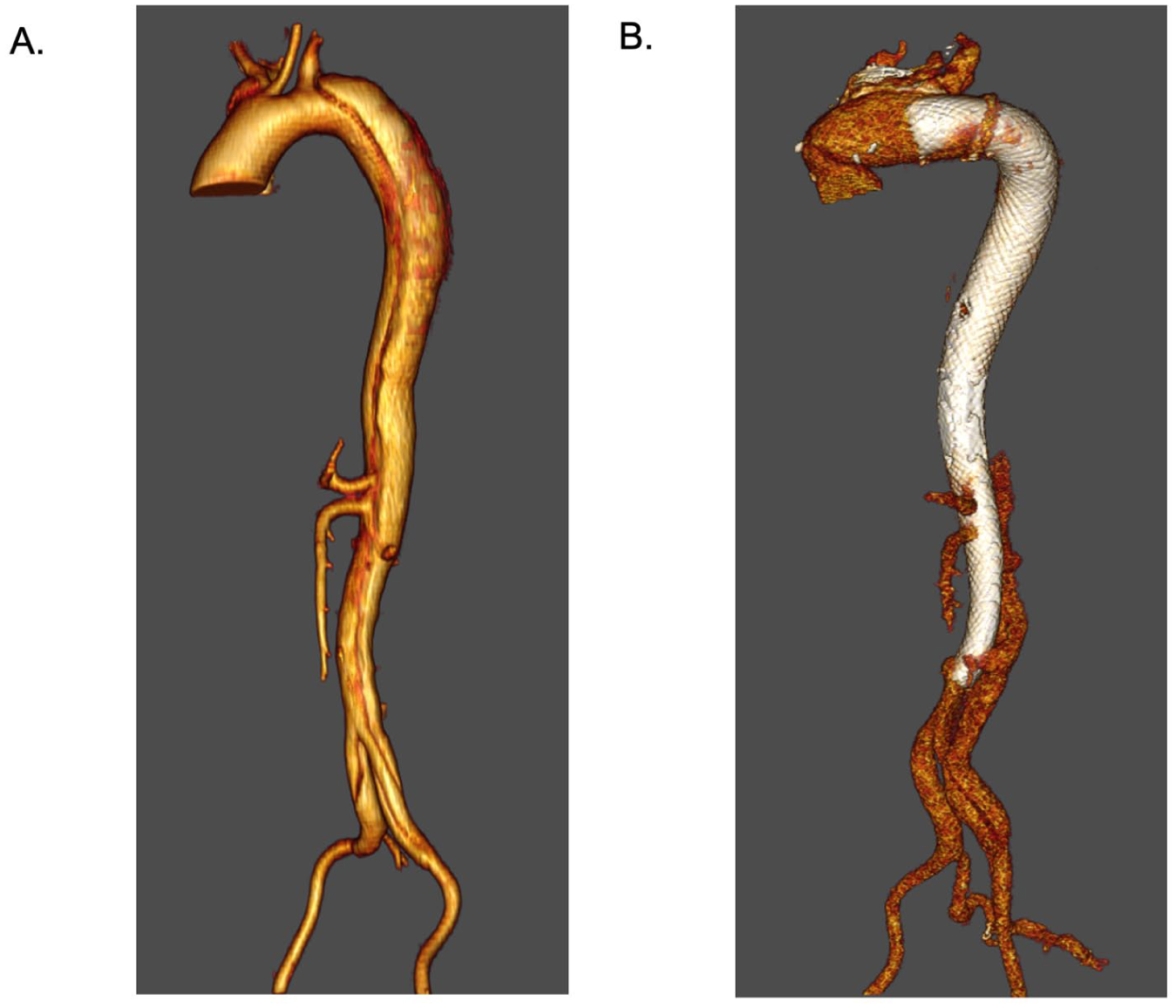
3D CT scan reconstruction of the aorta in a typical participant (A) before treatment with multilayer stents and (B) after treatment.
All CTs, SMAs, LRAs, and RRAs and 89.5% of IMAs were covered by stents, meaning that 88.8% of the major aortic branches were covered and a mean (SD) of 7.1 (1.0) branches were covered per participant. Of the aortic arch branches, 63.2% of the BCAs and LCCAs and 94.7% of the LSAs were covered by stents. Flow to these covered branches was not compromised, and no bypass/transposition was required. The perfusion of some side branches improved following treatment: 1 LRA fed pre-op by the FL was fed by both lumens post-op; 1 BCA and 2 RRA fed by both lumens pre-op were fed by the TL post-op. In 78.9% of participants, at least one or more lumbar arteries originating from the FL segment were covered by a multilayer stent. In 84.2% of participants, one or more intercostal arteries were covered. Perfusion of the lumbar and intercostal arteries was maintained in 100% of subjects during the follow-up period.
The technical success rate of the surgical procedure was 96.3%, as the proximal part of 1 stent did not open completely in the proximal healthy landing zone in 1 participant. Nevertheless, stent deployment and treatment of the dissection could still be performed, and there were no negative consequences nor AEs over the long-term follow-up period.
Mean (SD) fluoroscopy time was 29.3 (2.4) minutes, and mean (SD) contrast used was 209.0 (114.3) mL. None of the patients required blood transfusions, and no adjunctive procedures were performed. Mean (SD) total anesthesia duration was 194.9 (43.2) minutes and mean (SD) total implantation time 59.1 (30.4) minutes.
Mortality and Morbidity
Thirty-day mortality occurred in 1 of 27 participants (3.7%; from PP cohort), who died perioperatively from an aortic rupture during the implantation, an event assessed as related to the procedure by the investigator (Immediately after the procedure, subject suffered pericardial effusion and cardiac tamponade due to ascending aorta rupture.). Two additional participants died from unknown causes during the follow-up period (1 in PP; 1 in ITT). These 2 deaths were documented upon resumption of the follow-up visits in 2022, post-COVID pandemic. Mean (SD) survival time was 68 (6) months, and the estimated 5-year survival was 89% in the ITT population (Figure 3) and 69 (5) months and 90% in the PP population.
Table 2 summarizes the AEs documented during the follow-up period. There were no reports of neurological complications (stroke, paraparesis, paraplegia) or signs or symptoms of ischemic events (spinal cord ischemia, myocardial infarction, bowel ischemia, kidney failure requiring dialysis, limb ischemia), within the first 30 days of the procedure. All participants (100%) remained free from neurological or ischemic events during the follow-up period.
Frequency of Serious and Non-serious Adverse Events in the Safety (ITT) Population (n=27).
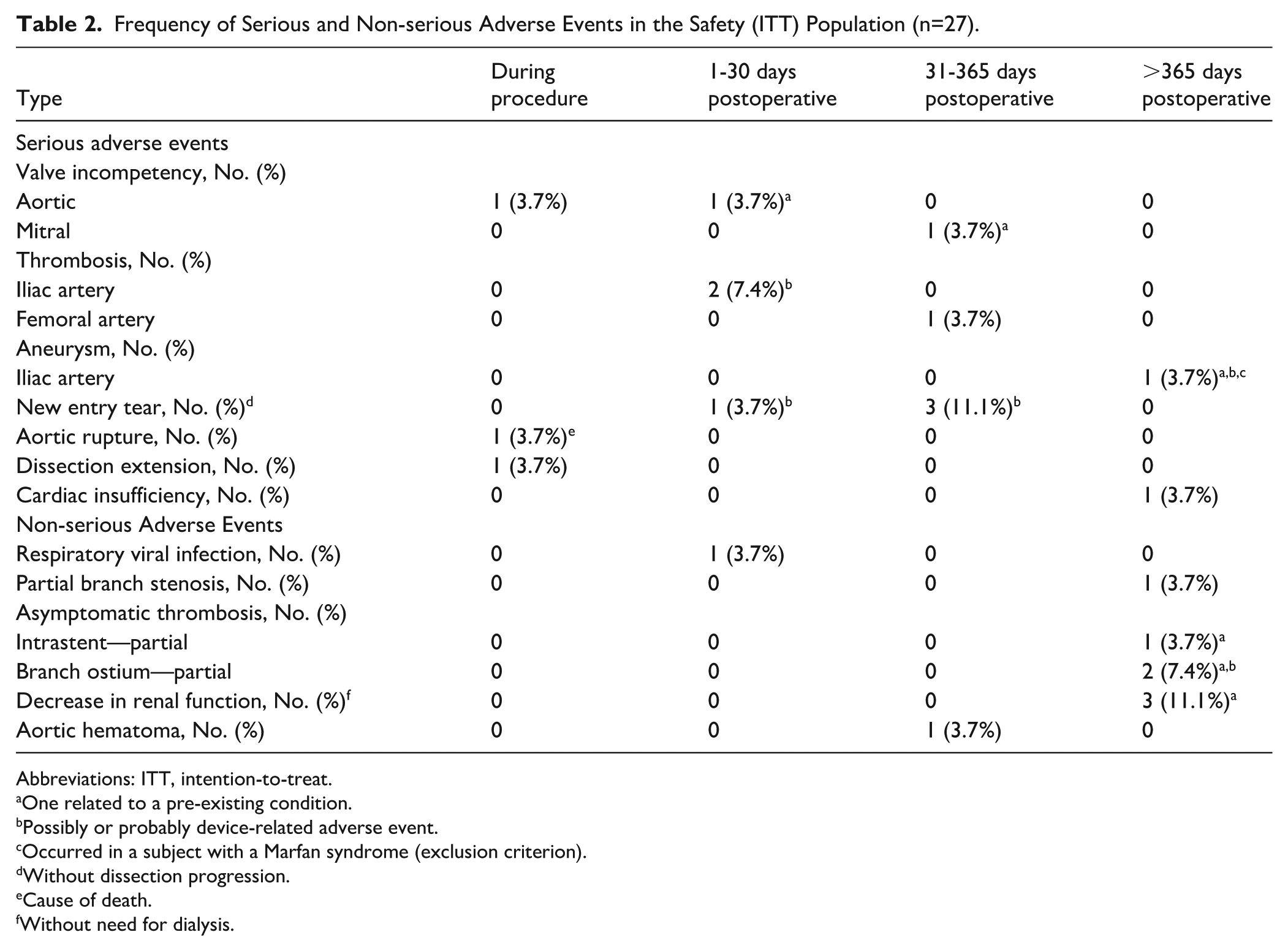
Abbreviations: ITT, intention-to-treat.
One related to a pre-existing condition.
Possibly or probably device-related adverse event.
Occurred in a subject with a Marfan syndrome (exclusion criterion).
Without dissection progression.
Cause of death.
Without need for dialysis.
Fourteen serious adverse events (SAEs) were documented, including 7 device-related ones in 6 participants. The most common SADEs were 4 proximal new tears (14.8%), which occurred in participants in whom the multilayer stent had been deployed in the native ascending aorta and arch. The proximal new tears were observed on CT scans performed between 8 and 198 days after the implantation procedure and assessed as probably procedure- and device-related (tears were located either proximal or adjacent to the stent proximal edge). The proximal new tears were identified as stable and participants were asymptomatic; no intervention was deemed necessary by the investigator during the follow-up period. In addition, no RTADs were observed during the follow-up period. Seven SAEs occurred more than 30 days postoperatively in 7 participants (25.9%); 4 of these SAEs were assessed as possibly or probably device-related.
Nine non-SAEs were reported (Table 2); of these, 7 (77.8%) occurred more than a year after the procedure. The most common non-SAE was a decrease of renal function in 3 participants (33.3%), which was unrelated to the device; none of them required dialysis. Independent third-party review of the CT scans indicated a low incidence of new-onset complete stenosis (<1%) and of new-onset loss of aortic branch distal flow (<2%) in the major aortic branches. There were no clinical consequences associated with the new-onset complete stenosis or loss of distal flow.
True Lumen Reopening, Device Integrity, and Migration
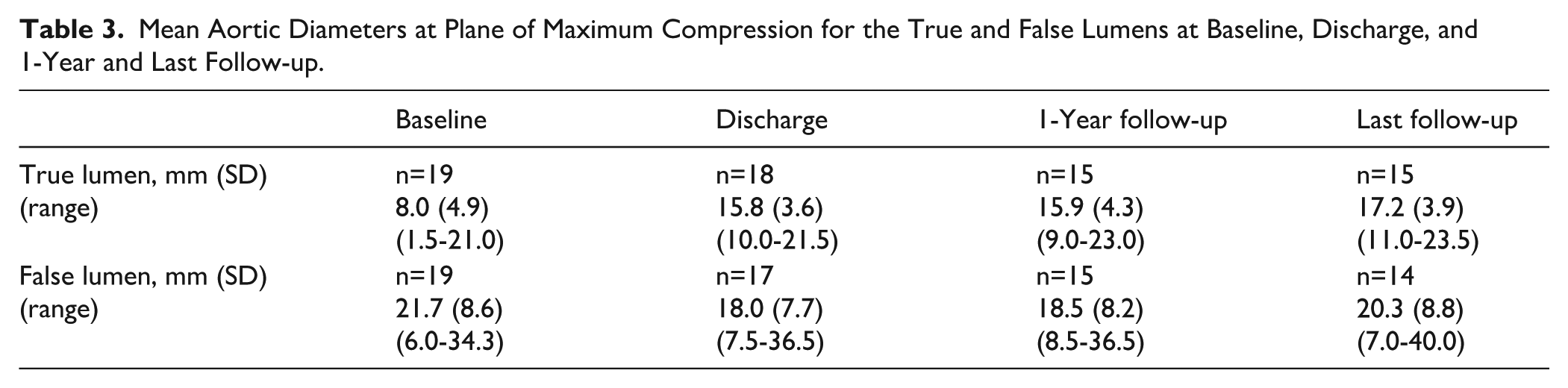
The device performed as expected, specifically by increasing the TL diameter and decreasing the FL diameter along the entire length of the treated aorta. The diameter measurements at the PMC are presented in Table 3. In summary, the diameter of the TL increased between baseline and discharge and remained stable during follow-up. Conversely, the diameter of the FL decreased between baseline and discharge, with little variation over the long-term follow-up period. Of note, in this population of subacute and chronic patients, the flap was reapproximated to the aortic wall but was not opposed to it, preserving the perfusion of the branches fed by the FL.
Mean Aortic Diameters at Plane of Maximum Compression for the True and False Lumens at Baseline, Discharge, and 1-Year and Last Follow-up.
No implanted stent malfunctions (ie, stent kinking, collapse fracture, or migration) occurred during the follow-up period, as confirmed by independent imaging review. All aortic devices remained patent; in cases where 2 stents overlapped, there was no indication of change in overlap length.
False Lumen status and transaortic diameter change
Over the course of the follow-up period, all participants except for 1 had patent FLs (partially or completely); only 1 participant (6.6%) had a fully thrombosed FL at the last follow-up.
With regard to aortic growth, mean maximum transverse aortic diameter is presented in Table 4. The mean maximum TA diameter appears to remain stable over the follow-up period. Maximum TA diameter remained stable (change since discharge less than 5 mm) or decreased (by 5 mm or more since discharge) in 78.6% of participants. No extension of the dissection beyond the treated segment, either retrograde or anterograde, occurred.
Mean Maximum Transverse Aortic Diameter at Baseline, Discharge, and 1-Year and Last Follow-up.

Side Branches Perfusion
Distal flow was preserved in 98.3% of major branches (Figure 4). New loss of distal flow 30 days or more after the procedure was documented in only 1.7% branches (ie, 1 RRA and 1 IMA; see Table 5), in the same participant who had complete CT and IMA occlusion at baseline and developed complete RRA occlusion during the study. Furthermore, perfusion of the lumbar and intercostal arteries flow was maintained in all participants throughout the follow-up period. No neurological complications or end-organ ischemia were reported during the follow-up.
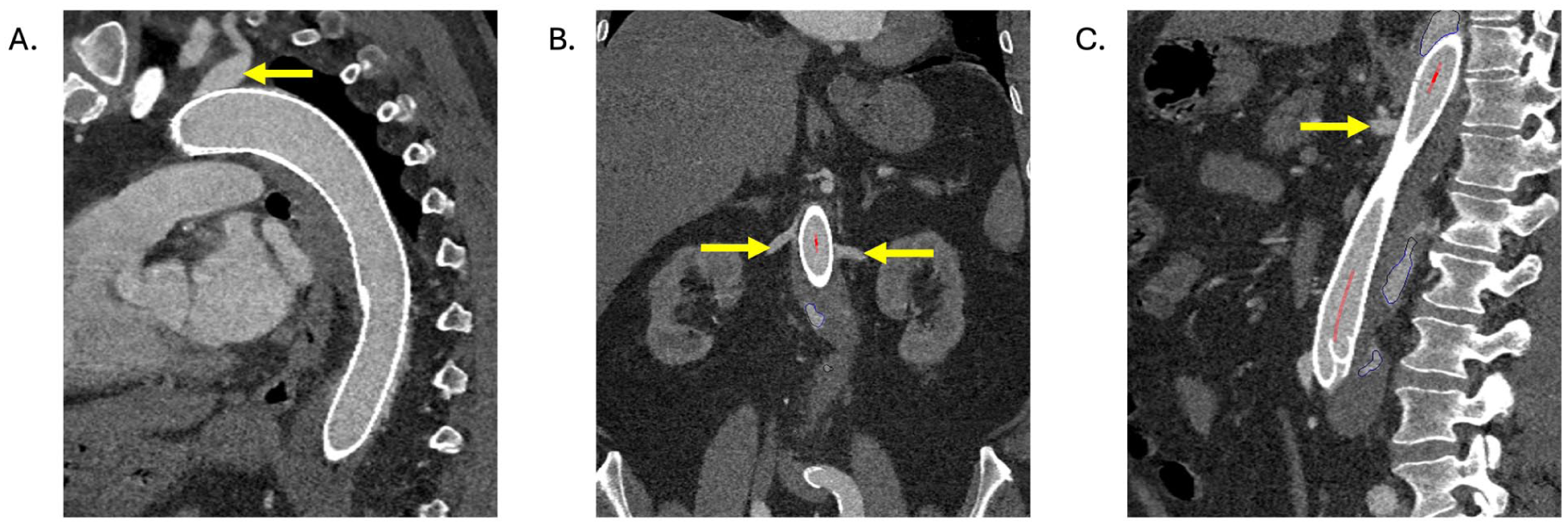
CT scans taken at 59 months after multilayer stent implantation in the same participant as in Figure 3, showing preserved perfusion through the (A) left subclavian artery, (B) right and left renal arteries, and (C) celiac trunk (see yellow arrows).
Overview of the Presence or Absence of Distal Flow in Major Aortic Branch Arteries at Baseline and During Follow-up.

Reinterventions
No reinterventions were required to prevent aortic growth beyond a postoperative period of 30 days. Furthermore, no aortic ruptures, open conversions, or dissection-related deaths were documented.
Discussion
The study is a prospective multicenter study designed to investigate the safety and performance of the multilayer stent device (MFM, now Allay Aortic Stent) in patients with high-risk TBAD. In this study, the multilayer stent was successfully implanted in 96% of participants.
During the 54-month average follow-up of the PP cohort, there was no device deficiency: all devices remained patent, there was no stent migration, kinking, collapse, or fracture, and there was no separation of overlapped aortic stents as assessed by the independent imaging Core Laboratory. In the PP cohort, the estimated 5-year survival was 90% (Figure 5). This result is in line with a reported 89.9% 5-year survival reported for stent grafts in patients with uncomplicated TBAD, which in turn was significantly higher than the 5-year survival (81.7%) among patients treated with the standard optimal medical treatment. 10
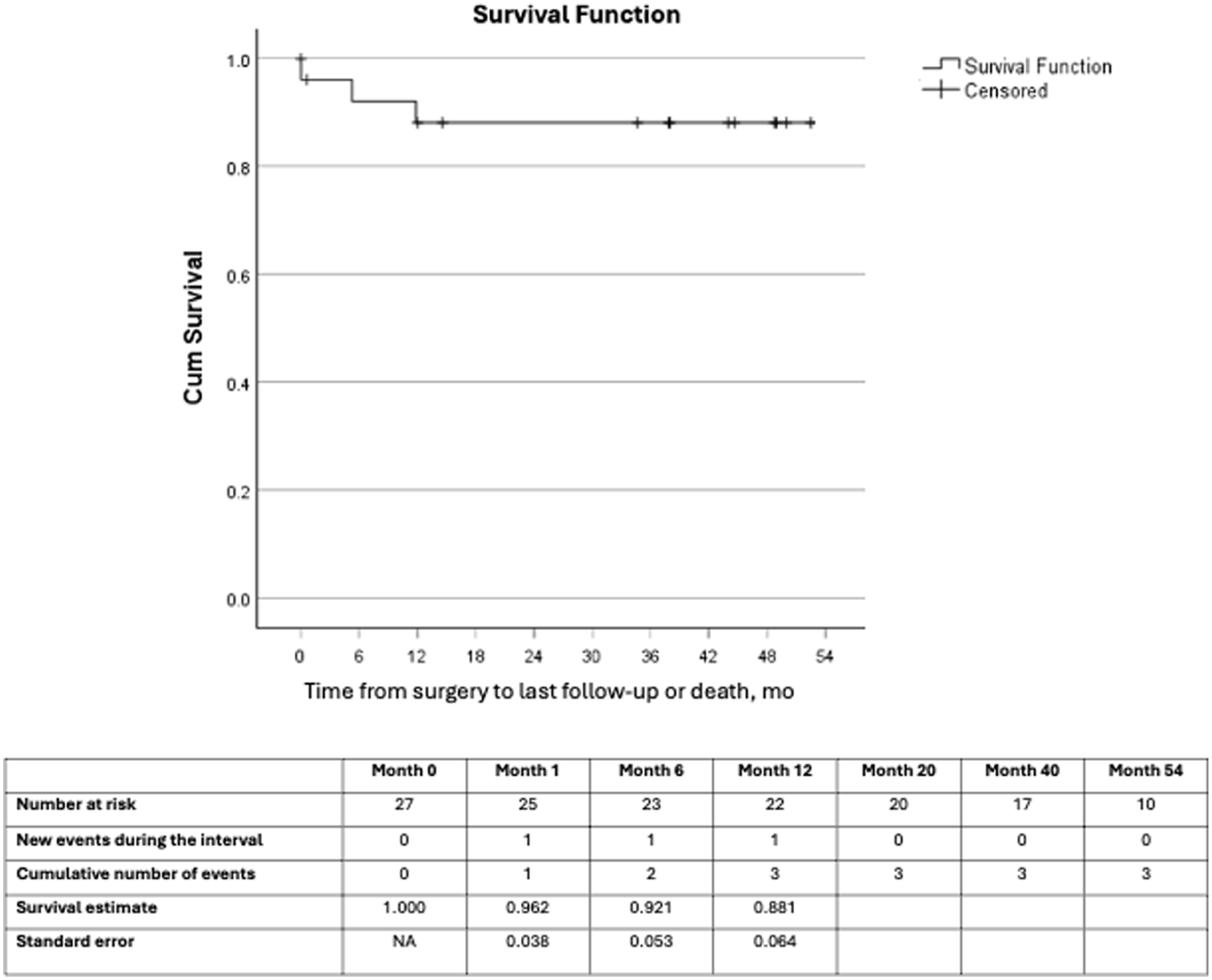
Survival curve and estimates from the Kaplan-Meier survival analysis for the ITT cohort from surgery to last follow-up or death.
The device performed functionally and clinically as expected reopening the TL, reducing the FL diameter, and stabilizing the dissection along the treated aorta. There was no progression of the aortic dissection, no aortic ruptures, or no reinterventions or open conversion during the 54-month follow-up period. In addition, there were no signs or symptoms of ischemic or neurological events such as stroke, bowel infarction, paraplegia, limb ischemia, or renal failure leading to dialysis. Furthermore, the independent imaging Core Laboratory confirmed that patency of the side branches was maintained. The incidence of new-onset loss of flow in aortic side branches was less than 2% (ie 2 new losses in 1 participant) and none of these cases were associated with any clinical consequences, the participants remaining asymptomatic.
The results of this prospective, multicenter, single-arm clinical trial are consistent with the results reported by Costache et al 11 regarding the feasibility and safety of treating TBAD patients with multilayer stents and confirm that the clinical outcomes observed at 12 months by the authors can be maintained in the longer term, over 54 months on average.
Moreover, these results compare favorably with the results of TEVAR performed with stent grafts in cases of TBAD. A meta-analysis by Li et al 12 indicated that aorta-related mortality after TEVAR was 5.2% and procedure-related mortality 7.0%, with the most common cause being aortic rupture (25.6%). They also found that although complications after TEVAR with stent graft can be significantly lower in high-volume centers, major perioperative complications are not uncommon with acute renal failure requiring hemodialysis occurring in 5.1% of patients, type I endoleak in 4.9%, stroke in 4.2%, spinal cord ischemia (SCI) in 3.3%, RTAD in 3.2%, and visceral ischemia in 3.1%.
The finding that no reinterventions were necessary during the 54-month follow-up period is also noteworthy. In contrast, when patients with TBAD are treated with stent grafts, the coverage with stent grafts is usually limited to 200 mm to reduce the risk of SCI, 13 which increases as the length of the stent graft increases. 14 Such limited coverage leads to progression of TBAD due to uncovered secondary entry tears necessitating surveillance 15 and reintervention in a significant number of cases.16,17
Furthermore, the frequency of progressive growth and aneurysmal degeneration of the unstented abdominal aorta at 5-year follow-up is about 40%, 18 and reintervention rates after TEVAR with stent grafts may range between 15 and 35%.16,17 Data from the STABLE II study, which evaluated the PETTICOAT procedure using a commercially available stent graft-bare stent combination device system, showed that the maximum transaortic diameter in the stented region distal to stent graft increased more than 5 mm in 45% of patients by the 2-year follow-up moment and in 62% of patients by the 5-year follow-up. 19 In comparison, after a mean of 54-month follow-up, only 21% of participants in our study had an increase in maximum transaortic diameter that was greater than 5 mm post-implantation; this considerably lower aortic growth rate may partially explain why no reinterventions were observed. Overall, the device prevented an increase in maximum transaortic diameter in 79% of the participants, with no aortic ruptures reported over the follow-up duration. However, although some patients enrolled in this study with a maximum transaortic diameter greater than or equal 55 mm fared well, they remain at a high risk of aortic rupture. Considering the residual risk of rupture in this subgroup of patients, they should be considered for first-line open surgical aortic replacement as per current medical guidelines following proper assessment of their surgical risk.1,3
The most common SAE observed in this study was proximal entry tears, which occurred in participants in whom the MFM had been deployed in the native ascending aorta and arch. As these new tears were stable (ie, no evidence of dissection extension) and the participants were asymptomatic, no further interventions were deemed necessary by the investigators during the follow-up period. Such new entry tears therefore seem different from the retrograde type A dissection due to proximal SINE. This finding nevertheless provides valuable insights that in TBAD patients, the proximal stent is preferably deployed in the descending aorta or in a surgical graft in the ascending aorta and that caution should be exercised when deploying the proximal stent in the native ascending aorta. 20 As opposed to TEVAR with stent graft for which this is a frequent complication, there were no distal new tears observed in this study. 21
Overall, the multilayer stent safely met the primary goals of TEVAR treatment as defined in the ACC/AHA guidelines, ie, preventing aortic rupture, retrograde extension, and antegrade propagation of the dissection. 1 Multilayer stents achieve these goals through a mechanism of action that differs from that of stent grafts. Whereas the mechanism of action of stent grafts relies on sealing the primary entry tear to induce the thrombosis of the FL, blood flow in the FL was observed in all but 1 patient treated with the multilayer stent. It is hypothesized that such blood flow is necessary to preserve the perfusion of aortic side branches fed by the FL and thereby contribute to the device’s favorable safety profile. Remarkably, such residual blood flow in the FL does not appear to lead to aneurysmal degeneration over the 54-month follow-up period.
The mechanism of action of the multilayer stent is thus based on reopening the compressed TL and recentralizing blood flow into the TL. In addition, multilayer stents can be overlapped to provide extensive treatment of the entire length of dissected aorta and prevent the dissection from progressing beyond the treated segments. The extensive treatment can include the abdominal aorta and coverage of the side branches thanks to the multilayer stent’s open mesh design with high 3D porosity. The 3D porosity preserves patency of side branches fed from the TL or FL, and this preserved patency mitigates the risk of ischemia to downstream tissues and organs.
The main limitations of this study are that it was a study with a small number of enrolled patients and no control group. However, the long-term follow-up period of 54 months, the high retention rate (the status of 92% of subjects was known at the time of analysis), and standardized imaging analysis by an independent imaging Core Laboratory ensure reliable study results. Also, the study design resembled clinical practice, which facilitates the generalizability of the findings. Taken together, the results of this study support the safer use of the multilayer stent in high-risk TBAD patients.
Conclusion
In patients with high-risk TBAD, extensive treatment of the dissected aorta with multilayer stent devices is feasible and has an acceptable safety profile. Other than an intraoperative aortic rupture death, there were no aortic ruptures, dissection-related deaths, neurological complications, or end-organ ischemia reported over a long-term follow-up (54.9 months in the ITT cohort; 54.1 months in the PP cohort). Interestingly, treatment with multilayer stents met the primary goals of TEVAR treatment in aortic dissection without the need to seal the primary entry tear nor induce complete FL thrombosis. The unique characteristics and mechanism of action of the multilayer stent offer a new approach to TEVAR treatment. Further research is warranted to confirm the findings of this study.
Footnotes
Acknowledgements
Assistance with preparing the manuscript and submission was provided by LS Academy. Special thanks to Ms Ana Maria Coman for her administrative support.
Ethical Considerations
This study was approved by the Romanian National Competent Authority (approval no. 37) on 29 October 2015 and the Bulgarian National Competent Authority (approval no. 0001) on 19 January 2017. The study received ethical approval from the local Romanian Ethics Committee (Polisano European Hospital - Approval no. 2) on 24 July 2015, local Bulgarian Ethics Committee (UMHAT City Clinic - Approval no. 15) on 20 October 2016, and national Bulgarian Ethics Committee (Ministry of Health, Ethics Committee for Multicenter Trials - Approval no. 151) on 28 November 2016. All patients provided written informed consent before enrollment in the study. The study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice.
Consent to Participate
All patients provided written informed consent before enrollment in the study.
Consent for Publication
Not applicable.
Author Contributions
All authors made significant contributions to the conceptualization or design; acquisition of patients and their data; critically reviewed and edited the manuscript; and approved the final version of the article for publication. All authors agreed to be accountable for this work and resolved any issues related to its integrity or accuracy. VSC and IP provided supervision as the principal investigators.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This clinical trial was sponsored by Cardiatis (Gembloux, Belgium), now Intressa Vascular. The sponsor was involved in the design of the study, collection of the data, interpretation of the results, and drafting of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data sets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.