
Abstract
Background:
Transradial arterial access (TRA) using 5 French (5F) devices is a new option to manage percutaneous aorto-iliac interventions, potentially reducing the rate of vascular complications and the length of hospital stay. However, evidence is limited on the efficacy and safety of this approach. The aim of our study was to assess the feasibility, efficacy and safety of TRA 5F approach, using Micro device portfolio by Qualimed, for the treatment of aorto-iliac artery lesions up to 12-month follow-up.
Methods:
This is a single-center, all-comers, observational registry in which 60 consecutive patients undergoing transradial angioplasty due to aorto-iliac steno-occlusive disease were prospectively enrolled from April 2022 to September 2024. We assessed: procedural success of angioplasty using at least 1 TRA (primary efficacy outcome); primary patency at 12 months; length of hospital stay (secondary efficacy outcomes); freedom from major adverse events (MAEs) (primary safety outcome); and freedom from access-related vascular complications (secondary safety outcome).
Results:
Procedural success of aorto-iliac angioplasty using at least one 5F transradial access was achieved in 58 of 60 patients (96.7%). In 66.7% of the cases, an additional transfemoral approach was required, whereas in 2 of 60 patients an unplanned switch from radial to femoral access occurred. Primary patency was 95.0%, since 3 patients underwent target vessel revascularization due to restenosis/thrombosis. Mean hospital stay was 2 days. As for safety, no MAEs were reported. Freedom from (radial) access-related vascular complications was 100% during index hospital stay and 88.3% after12-month follow-up, since 7 radial occlusions occurred.
Conclusions:
These 12-month findings suggest mid-term efficacy and safety of transradial aorto-iliac artery interventions using 5F Micro devices by Qualimed, even in the setting of complex lesions (ie, TASC II classification ≥ C). Larger cohorts and randomized controlled trials will be needed to confirm these results.
Clinical Impact
The study suggests that 5F transradial access for aorto-iliac interventions is a feasible and safe alternative to the traditional femoral approach. The high procedural success, absence of major adverse events, and short hospital stay support its integration into routine practice. For clinicians, this technique may reduce access-site complications and facilitate faster patient mobilization without compromising technical outcomes. The main innovation lies in the availability of a complete 5F device platform, enabling treatment of complex lesions previously unsuitable for radial access. If confirmed in larger studies, this approach may shift practice toward safer, minimally invasive endovascular strategies.
Keywords
Introduction
Peripheral arterial disease (PAD) is prevalent worldwide and affects more than 100 million people aged 40 and older. 1 Its global prevalence is almost 2%, increases with age and significantly impacts on quality of life and prognosis. 1 Aorto-iliac steno-occlusive disease is an advanced PAD manifestation which may lead to incapacitating claudication and limb-threatening ischemia, as well as vasculogenic impotence. According to the most recent guidelines, treatment of aorto-iliac lesions, aimed at re-establishing inflow to the lower extremities, may be effectively managed through either a surgical or endovascular approach, depending on lesion morphology and individual patient risk profile. 2 Based on anatomical considerations, these lesions are classified by the TASC II (Inter-Society Consensus for the Management of Peripheral Arterial Disease) into 4 categories. Traditionally, TASC II A and B lesions have been treated with endovascular techniques, while C and D lesions were considered more suitable for open surgery. 3 However, recent evidence supports the expanding role of endovascular therapy even in complex TASC II C and D lesions.
In particular, a recent meta-analysis comparing open surgery and endovascular treatment in aorto-iliac disease, including TASC II C-D lesions, showed no significant differences in secondary patency or limb salvage, while endovascular therapy was associated with lower short-term mortality, morbidity, and shorter hospital stay. Primary patency remained superior in the surgical group, although this may reflect patient selection bias, with surgical candidates being younger and generally healthier. 4
In the percutaneous setting, primary stenting has become the cornerstone in the treatment of aorto-iliac lesions, especially in more complex cases, as it has demonstrated higher clinical success rates compared with balloon angioplasty alone.5,6
Transfemoral arterial access (TFA) has traditionally been the gold standard for peripheral artery intervention. Nevertheless, its pivotal limit is the rate of vascular complications, potentially life-threatening, as well as impacting on the length of hospital stay and long-term prognosis. 7 This consideration has prompted the transition to transradial arterial access (TRA) in the field of coronary intervention, with the achievement of reducing major adverse cardiovascular events (MACE), major bleeding and vascular complications. 8
Transfemoral arterial access for aorto-iliac interventions is gaining popularity with the aim of increasing safety by reducing vascular complications and newer studies demonstrated technical and clinical success of this approach.9,10 However, transradial aorto-iliac interventions have been, up to now, affected by the small number of compatible devices both for shaft length and diameter, as well as being limited to 6 French (6F) devices. The new Micro platform by Qualimed offers an entire portfolio of 5 French (5F) compatible devices: introducers-guiding catheters, balloons and balloon-expandable stents with diameter up to 10 mm and length up to 180 cm, allowing to treat also long diseases involving external iliac artery or femoral artery.
Hence, the aim of our study was to assess the efficacy and safety of these 5F devices in the TRA-treatment of aorto-iliac lesions in a single center, all-comers, observational registry.
Methods
Study Design
This is a single-center, all-comers, observational registry in which 60 consecutive patients undergoing transradial aorto-iliac angioplasty using the new 5F Micro devices, due to steno-occlusive disease, were prospectively enrolled from April 2022 to September 2024.
All patients were previously evaluated with aorto-iliac and femoral computed tomography angiography (CTA) to exclude both complex aorto-iliac disease requiring treatment with Covered Endovascular Reconstruction of the Aortic Bifurcation (CERAB) and aortic aneurysm requiring intervention, and to confirm steno-occlusive disease justifying patient’s symptoms.
Inclusion criteria were as follows:
Age > 18 years old;
Ability to sign the informed consent;
Intermittent claudication (Rutherford category 3) or chronic limb threatening ischemia (CLTI) (Rutherford categories 4–5);
Significant iliac artery stenosis ≥ 70% or occlusion assessed with CTA.
To note. The hemodynamic significance of the aorto-iliac artery stenosis was also confirmed during the index procedure by an invasive trans-stenotic gradient ≥ 20 mm Hg.
Exclusion criteria were as follows:
Refusal to sign the informed consent;
Asymptomatic patients;
Complex aorto-iliac disease requiring CERAB;
Aortic aneurysm requiring intervention.
Written informed consent was obtained from all participants according to the protocol approved by the institution ethics committee.
All patients underwent follow-up clinical visit at 30 days, 6 months, and 12 months. The follow-up assessments included: symptoms or signs of limb ischemia; primary patency (initially assessed by duplex ultrasound); repeated revascularization of the target vessel (by angioplasty or artery bypass graft procedure) or amputation; clinical and/or duplex ultrasonographic assessment of the arterial access sites. The need for a re-evaluation with CTA or invasive angiography was chosen by the clinician, based on the persistence of ischemic symptoms or signs, to unmask target lesion restenosis (TLR).
Endpoints Definition
The primary efficacy outcome was procedural success of aorto-iliac lesions percutaneous transluminal angioplasty (PTA) with 5F Micro Platform and at least 1 radial access: procedural success was defined as PTA resulting in <30% residual stenosis with sufficient anterograde flow, without conversion to TFA.
Secondary efficacy outcomes were as follows:
- Primary patency, defined as a composite of freedom from TLR or thrombosis and persistent patency without any reintervention (PTA, surgical procedures, or amputation) in the target lesion at 12 months; - Length of hospital stay (days).
The safety outcomes were as follows: - Freedom from major adverse events (MAEs), defined as a composite of death, major amputation, and repeated revascularization of the target vessel (by angioplasty or artery bypass graft operation) during the index hospital stay (primary safety outcome); - Freedom from access-related vascular complications (ie, compartment syndrome, radial artery occlusion, hematomas, pseudoaneurysm, nerve damage, abscess, and hand ischemia) (secondary safety outcome).
Index Procedure Description and Medical Therapy
In case of bilateral iliac artery lesions involving the aortic bifurcation, to treat both lesions at the same procedure, we used both radial and femoral contralateral access. In this setting, TRA was used to treat the worst lesion with the aim of increasing anterograde support and minimizing risk of dissections or perforations, while 5F TFA was used for the simpler lesion. In case of bilateral lesions far from the aortic bifurcation, we used a single TRA to treat both lesions consecutively (the most complex first). The choice to treat the second one is left to the operator’s discretion based on clinical aspects (ie, asymptomatic patient and hemodynamic stability) and procedural aspects (ie, procedural time, contrast medium dose, X-ray exposure). In case of monolateral iliac lesion, a single TRA was used.
All procedures were performed with the patient under local anesthesia. After vascular access was achieved, a 0.035” wire was used to cross the stenosis and then was replaced by a 0.018″ 300-cm wire through a multipurpose (MP) catheter. At operator’s discretion, the vessel occlusion was crossed by a hydrophilic guidewire supported by the MP catheter. Subsequently, a 130-cm 5F long introducer guiding catheter (GSQ, Guiding Sheath System, Micro Qualimed, Winsen, Germany) was loaded on the 0.018″ 300-cm wire and advanced near to the target lesion to achieve adequate support. Lesion predilation was performed per protocol with a catheter balloon (PVQ, PTA Balloon Catheter, Micro Qualimed, Winsen, Germany), undersized (ie, balloon diameter 4–5 mm) compared with the reference vessel diameter (RVD) for 60 seconds. After predilation, a QBX stent (QBX, Balloon Expandable Stent System, Micro Qualimed, Winsen, Germany), sized in a 1:1 ratio with the RVD and slightly longer than the lesion length, was delivered to the target side. It is a balloon expandable bare-metal (non‑drug-eluting) cobalt‑chromium stent, compatible with a 5F introducer sheath and guided over a 0.018″ over‑the‑wire system and available in a wide range of diameters (5–10 mm) and lengths (17‑57 mm). The stent balloon was inflated across the lesion at nominal pressure for at least 20 seconds. In case of flow-limiting edge dissections or residual stenosis, an overlapping QBX stent was deployed. Closure of radial vascular access was achieved with “TR-band” (Terumo Medical Corporation, Somerset, NJ, USA). Closure of femoral vascular access was achieved with “AngioSeal” (Terumo Medical Corporation, Somerset, NJ, USA) or “FemoSeal” (Terumo Medical Corporation, Somerset, NJ, USA).
Medical therapy with dual antiplatelet regimen was mandatory: 75 mg of clopidogrel was given daily for at least 5 days prior to the index procedure or a 300-mg bolus of clopidogrel was administered within 24 hours prior to the procedure; a 250-mg loading dose of aspirin was given prior to the procedure if not already on a 100 mg a day regimen. Heparin was administered during the procedure to maintain an activated clotting time (ACT) ≥250 seconds. At discharge, long-term antiplatelet therapy, pharmacological management of cardiovascular risk factors (ie, lipid-lowering medications to achieve an low-density lipoprotein [LDL] cholesterol < 55 mg/dL), together with lifestyle modifications, were recommended according to the most recent “ESC guidelines.” 3
Statistical Analysis
Statistical analysis was performed using SPSS software (version 24.0 for Windows; IBM Corporation, Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation (SD) of absolute numbers; categorical variables were expressed as frequencies and percentages.
Results
From April 2022 to September 2024, 60 consecutive patients undergoing transradial PTA with 5F Micro devices due to aorto-iliac steno-occlusive disease were enrolled in this registry.
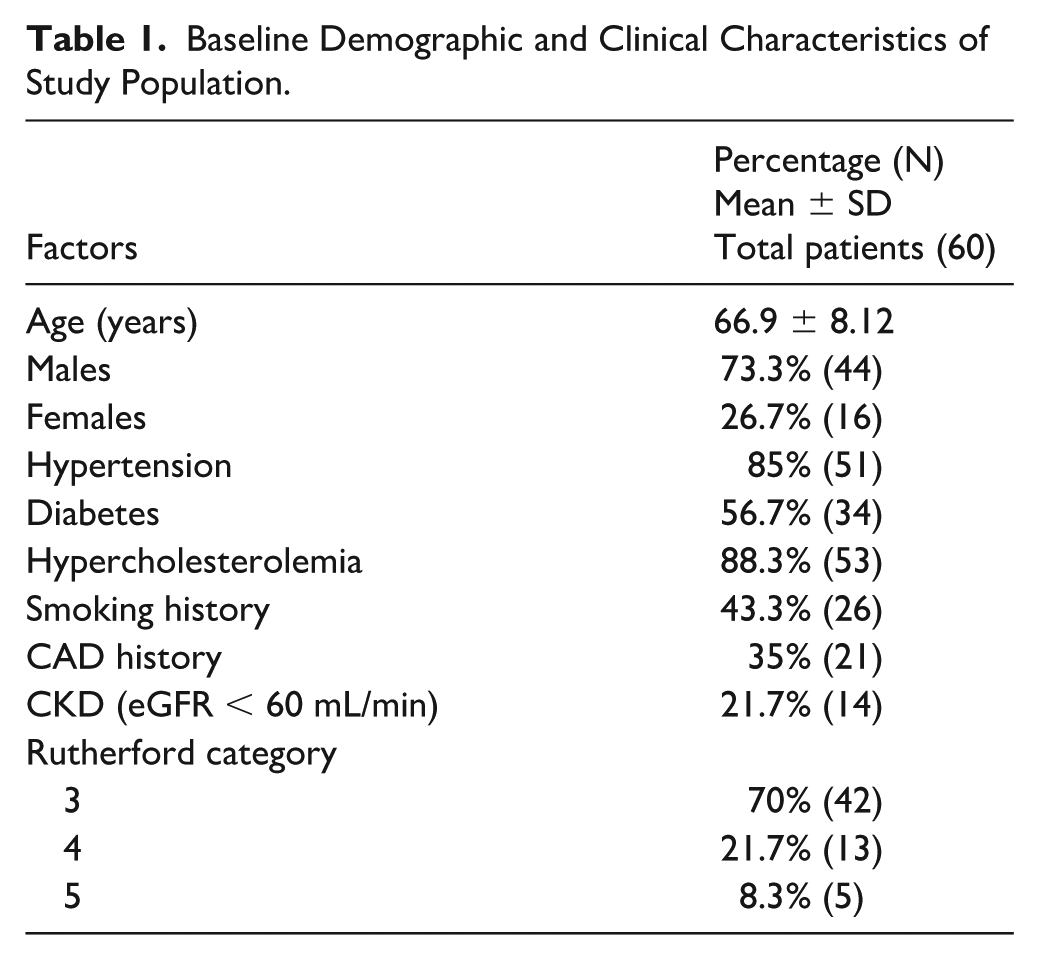
Baseline clinical characteristics of the study patients are shown in Table 1. Most patients were male (73.3%), with an average age of almost 70 years. The burden of the cardiovascular risk factors was high in the entire study population, with a prevalence of hypertension and dyslipidemia. Forty-two patients (70%) were admitted for intermittent claudication (Rutherford category 3), 18 patients for chronic limb-threatening ischemia (CTLI) (Rutherford category 4–5), while 18 patients (30%) had “Leriche Syndrome,” with associated symptoms of vasculogenic impotence (ie, erectile dysfunction).
Baseline Demographic and Clinical Characteristics of Study Population.
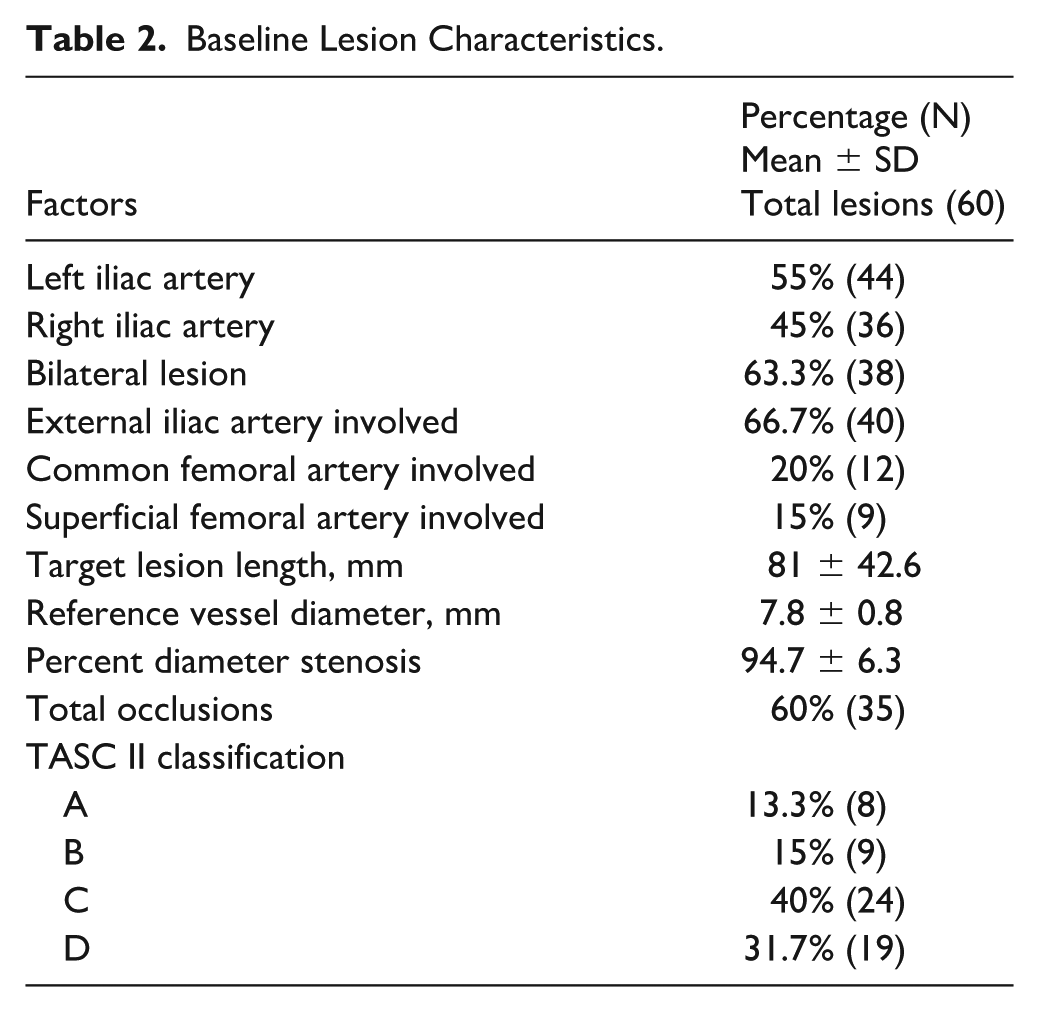
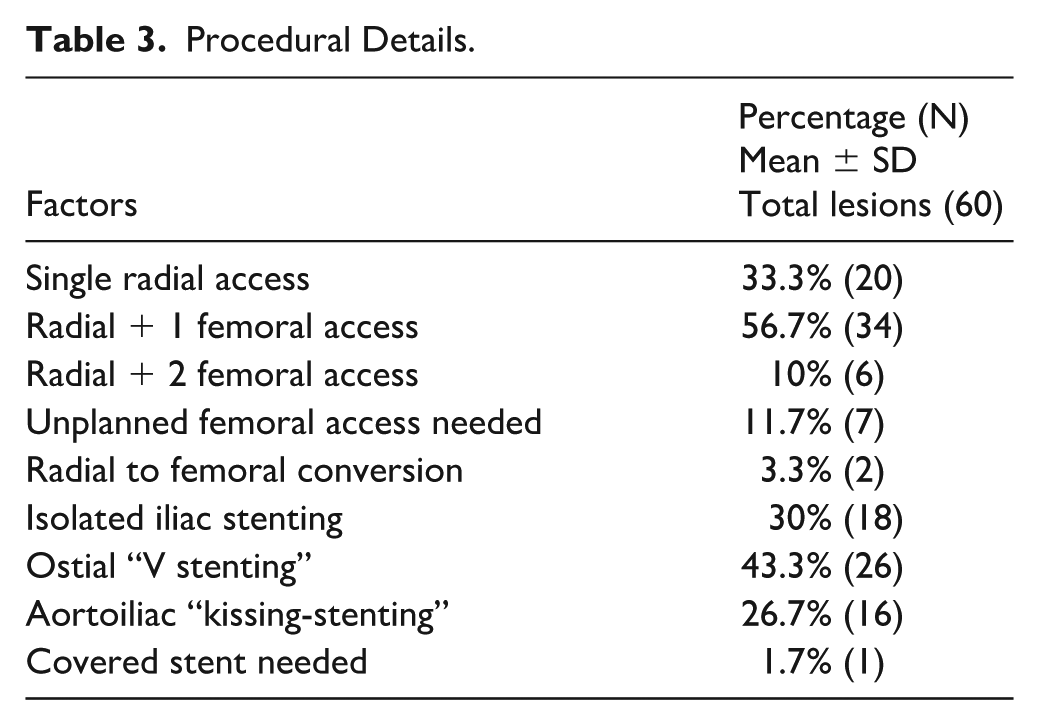
Baseline lesion characteristics and procedural details are shown in Tables 2 and 3, respectively. Most of the lesions (43; 71.7%) were ≥C according to TASC II classification and total occlusions were 35 (60%). Since more than 60% of the lesions involved both iliac arteries (38; 63.3%), a single radial access was used only in 20 procedures, while in the remaining procedures a femoral access was also used (34 with radial + 1 femoral access; 6 with radial + 2 femoral accesses). Indeed, in these cases ostial “V stenting” (26; 43.3%) and aorto-iliac “kissing-stenting” (16; 26.7%) were needed. To note, the disease was often long (mean lesion length 81 ± 42.6 mm) and diffuse, also involving the external iliac artery (40; 66.7%), common femoral artery (12; 20%) and superficial femoral artery (9; 15%).
Baseline Lesion Characteristics.
Procedural Details.
Primary efficacy outcome, secondary efficacy outcomes and safety outcomes are shown in Table 4.
Efficacy and Safety Outcomes.
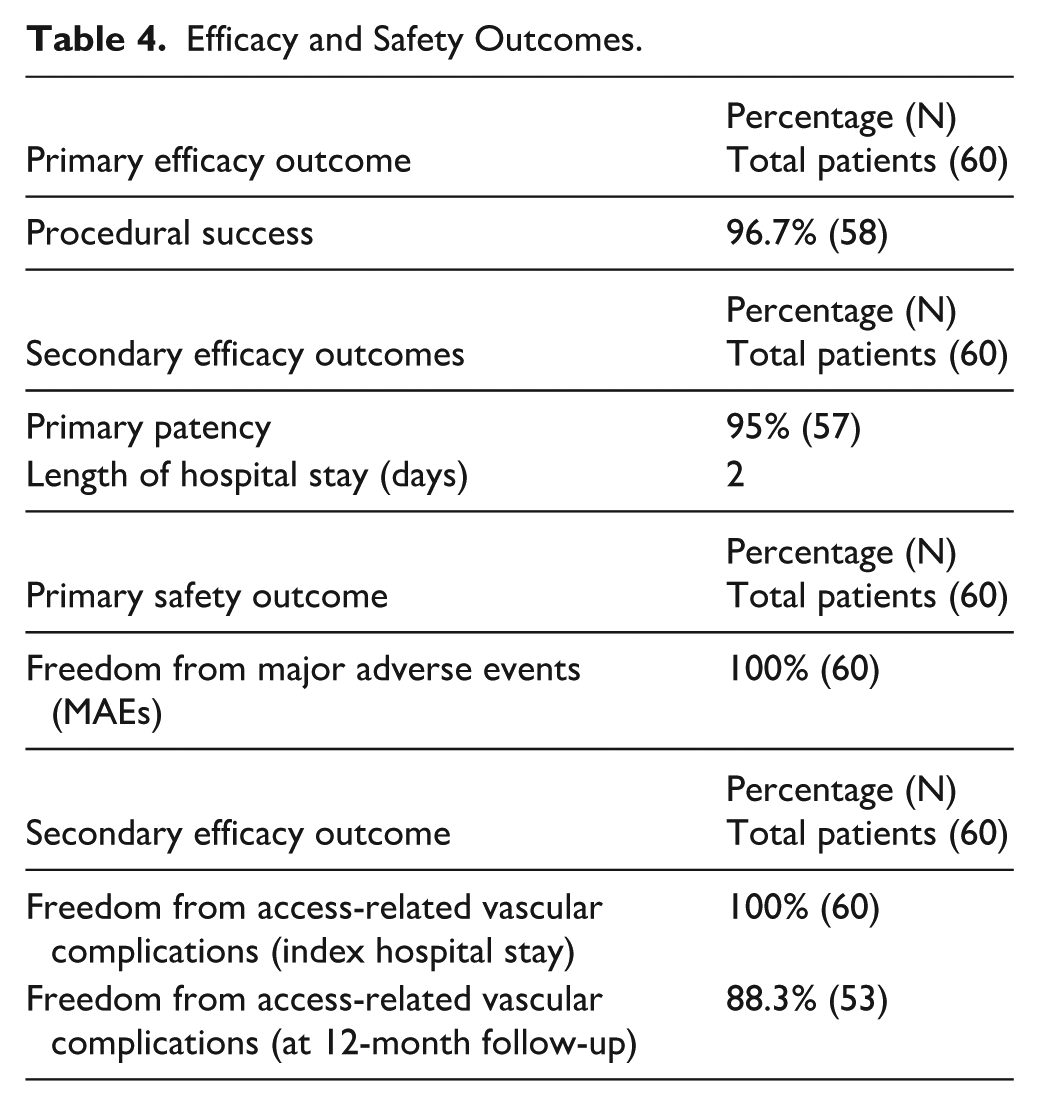
The procedural success (primary efficacy outcome) was 96.7% (58 procedures). In 2 cases, a conversion from TRA to TFA was needed: in 1 case, occluded iliac recanalization was achieved by transfemoral retrograde approach; in another, plaque prolapse into an implanted stent was treated with transfemoral covered stent implantation. After 12-month follow-up, the secondary efficacy outcome of primary patency was 95%, since 3 patients underwent target vessel revascularization due to 1 in-stent thrombosis (at 7 days from the index procedure) and 2 TLR (at 4 and 8 months, respectively). The mean hospital stay was 2 days.
As for safety, there were no major adverse events (MAEs) reported. During hospital stay, no radial access-related vascular complications occurred. While 2 femoral access-related vascular complications occurred, both due to contralateral femoral pseudoaneurysm (one of them inducing hemoglobin loss >3 g/dL). Clinical and ultrasonographic assessment of the radial access at 12-month follow-up revealed 7 occlusions (11.7%), all of which were asymptomatic and not clinically significant.
Discussion
Our study is the first describing the feasibility of 5F transradial approach to guide aorto-iliac PTA with the new Micro Platform, showing high procedural success and favorable safety profile. TFA is the traditionally used approach for percutaneous iliac artery interventions because the puncture is effortless, provides good backup support for the intervention, and allows the use of large femoral sheaths. Its main disadvantages might be bleeding complications and prolonged immobilization. TRA may have advantages over TFA as suggested by extensive literature around its use in the coronary field. 11 Furthermore, transradial approach seems to be better in terms of lower rate of bleeding and access-related complications, fast mobilization and short hospital stay also in the setting of lower limb PTA, without any trade-off in terms of technical success. 12 Meertens et al 13 confirmed these findings with a systematic review and meta-analysis highlighting that TRA for aorto-iliac and femoro-popliteal endovascular interventions can be performed with comparable technical success and lower overall complication profile compared with the traditional TFA. However, TRA had not yet gained wide recognition in the setting of aorto-iliac PTA due to technical limitations (large diameter, inflexible, and short delivery shafts of the first-generation devices). Moreover, the radial artery is more prone to spasm when using 6F and larger bore devices, and sometimes the passage of the sheath in the tortuous and calcified subclavian artery and aortic type II–III descending aorta can prove to be difficult. Therefore, advances in technology in terms of small French sheath compatible stents, long shafts and hydrophilic, flexible, kink-resistant long sheaths had been necessary to make transradial aorto-iliac complex endovascular interventions possible. In our experience, the use of the GSQ guiding sheath system and QBX stents represented a technically advantageous combination for transradial aorto-iliac interventions. The GSQ system, fully 5F-compatible, provided excellent torque control, enhanced support, and high flexibility without compromising stability during device delivery, even in complex anatomies. Its wide range of lengths (15–180 cm) and robust yet low-profile construction proved ideal for minimizing invasiveness while maintaining optimal control. Similarly, the QBX balloon-expandable stents offered high radial strength, excellent trackability, and precise positioning thanks to their radiopaque design and compatibility with 0.018″ guidewires. These features likely contributed to the high procedural success observed in our cohort. In fact, the procedural success was 96.7% and only in 2 of the 60 study procedures, a conversion from TRA to TFA was needed. This is relevant since radial to femoral access-site crossover may be associated with higher mortality and bleeding complications. 14 Furthermore, the primary patency at 12 months was 95%, since 1 in-stent thrombosis and 2 TLR occurred.
No safety concerns were raised: no MAEs or radial access-related vascular complications were reported during index hospital stay, while 2 femoral access complications were noted, both involving contralateral femoral pseudoaneurysms. Moreover, no peri-procedural or follow-up stroke events were observed up to 12 months. The absence of this complication may be partly explained by the small profile and great flexibility of the guiding catheter system used which may have contributed to a gentler navigation through the subclavian-aortic pathway, thus reducing the risk of embolic events during transradial aorto-iliac interventions.
After 12-month follow-up, only 7 radial occlusions occurred. This rate of radial artery occlusion (11.7%) is somewhat higher than the rates typically reported in coronary interventions, such as those in the RIVAL trial, 15 where the rate ranges between 2% and 5%. This difference may be related to the use of long introducers in our transradial iliac angioplasty procedures, which might cause more extensive vascular trauma and contribute to a higher rate of long-term radial occlusion. Importantly, in our series, none of the radial occlusions were clinically significant or symptomatic, and no patient experienced ischemic complications in the limb.
Two studies have also demonstrated that TFA may be safely employed in ambulatory settings, allowing early mobilization and same-day discharge. In particular, the FREEDOM study showed that early walking after femoral manual compression is feasible in patients undergoing 5F interventions, 16 while the BIO4AMB study confirmed the safety of ambulatory endovascular treatment using both 4F and 6F femoral access strategies. 17 However, these studies were conducted in highly selected populations and experimental outpatient contexts that may not reflect broader clinical practice. In our study, all procedures were performed under standard inpatient care, in accordance with the current Italian national health reimbursement system, which requires a minimum hospital stay of 2 days for these interventions. In fact, our length of stay was kept to the absolute minimum: patients were admitted the day before the procedure and discharged the morning after, with only 1 night of post-procedural observation.
With this approach gaining widespread popularity, there will be further development and miniaturization of specific equipment such as debulking, atherectomy devices and covered stents, bringing transradial interventions arsenal at the same level of the transfemoral, as well as allowing the treatment of bilateral iliac lesion involving the aortic bifurcation with double radial accesses. While our study did not include a formal cost‑analysis, transradial access using 5F systems may offer economic advantages: published evidence in coronary procedures indicates that although dedicated radial sheaths may be more expensive, overall procedural and hospital costs tend to be lower with TRA, largely due to reduced use of vascular closure devices and shorter lengths of stay. 18
Limitations
Our study has some limitations: first, the observational nature of the study gives an inferior level of evidence; second, since the lack of a control group, the findings cannot be compared with other endovascular treatments (ie, femoral approach); third, there is not a big-size population; finally, a heterogeneous study population was included in the present registry, ranging from patients with intermittent claudication to those with CTLI, as well as a heterogeneous group of lesions, ranging from simple lesions (ie, short and noncalcified) to complex ones (ie, long, heavy-calcified and chronic occlusion). However, this is an all-comers registry, aiming to represent a real-world cohort consistent with the ordinary clinical practice.
A methodological limitation of our study is the absence of a preprocedural ultrasound assessment of the radial arteries. This assessment was performed only during follow-up to detect complications. Preprocedural imaging might have helped reduce some complications or the need to switch to alternative accesses.
Regarding technical-procedural limitations, this TRA approach cannot be applied to treat complex aorto-iliac diseases requiring covered kissing stenting or CERAB, as well as bailout implantation of covered stents for perforations, due to large sheaths needed.
Conclusions
The above discussed findings suggest feasibility, efficacy and safety of transradial aorto-iliac PTA using 5F Micro devices by Qualimed, showing high procedural success, short hospital stay, and promising results sustained to 12 months in terms of primary patency and freedom from access-related vascular complications. These results will need to be strengthened in further randomized controlled studies with longer follow-up and larger cohorts.
Footnotes
Acknowledgements
Dr Giuseppe Ciliberti has been supported by a research grant provided by the Cardiopath PhD program.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.