
Abstract
Purpose:
To report early outcomes of physician-modified Endurant limbs for IIA preservation, highlighting a novel mini-inner branch design.
Materials and Methods:
From January 2023 to April 2025, 12 patients with aortoiliac aneurysms and common iliac artery bifurcation diameters ≤18 mm underwent EVAR using one of 3 Physician-Modified Endograft(PMEG) configurations: (1) single fenestration, (2) outer branch with a 6 × 10-mm PTFE graft, or (3) mini-inner branch with a 6 × 5-mm obliquely cut PTFE graft. The outer branch was chosen when commercial devices were unavailable, offering a slightly smaller profile than most off-the-shelf devices. Outcomes included technical success, IIA patency, and type I/III endoleaks.
Results:
Technical success was achieved in all cases, with no type I or III endoleaks. The mini-inner branch improved sealing and simplified resheathing.
Conclusion:
PMEG configurations are feasible alternatives for IIA preservation in narrow or resource-limited settings. The mini-inner branch offers a promising balance between sealing and procedural simplicity, but long-term evaluation is warranted.
Clinical Impact
This study presents a novel mini-inner branch design for physician-modified Endurant limbs, offering a practical solution for internal iliac artery preservation in patients with narrow iliac anatomy. The design improves sealing and simplifies resheathing without requiring larger sheaths. It expands endovascular options where standard iliac branch devices are not feasible, supporting safer and more adaptable aneurysm repair in challenging anatomies.
Keywords
Introduction
Endovascular aneurysm repair (EVAR) has become the preferred treatment for aortoiliac aneurysms due to its minimally invasive nature and favorable perioperative outcomes. 1 When aneurysms involve the common and internal iliac arteries, preserving internal iliac artery (IIA) perfusion is essential to prevent complications such as buttock claudication, sexual dysfunction, and pelvic organ ischemia.2,3 Commercial iliac branch devices (IBDs) are widely used for IIA preservation and have demonstrated high technical success rates and excellent patency outcomes. 3
However, patients with narrow iliac anatomy often present specific anatomical constraints, including common iliac artery (CIA) diameters less than 18 mm, short CIA length, and tortuous external iliac arteries. These anatomical limitations render patients ineligible for iliac branch devices according to the instructions for use (IFU) criteria and may require more proximal graft deployment to achieve adequate sealing and facilitate IIA branch cannulation.4,5
In such scenarios, physician-modified endografts (PMEGs) provide a flexible and customizable alternative for IIA preservation when commercial devices are unsuitable.6–8 A previous report by Tatsuishi et al 9 described the use of a physician-modified fenestrated Endurant contralateral limb for IIA preservation with promising early results. Building upon this concept, we initially adopted the fenestration only technique in selected cases and subsequently developed additional configurations incorporating outer and inner branch extensions to improve sealing at the bridging stent interface. In this case series, we describe 3 representative patients treated with distinct PMEG configurations: single fenestration, outer branch, and a mini-inner branch constructed with an oblique-cut PTFE graft. We also report early clinical outcomes from a total of 12 patients with narrow CIAs who underwent this technique.
Materials and Methods
This retrospective study included patients with aortoiliac aneurysms who underwent endovascular aortic repair involving the iliac arteries between January 2023 and April 2025. Inclusion criteria were patients with a common iliac artery (CIA) diameter ≤18 mm at the CIA bifurcation who were treated with physician-modified Endurant limbs. Demographic data, aneurysm characteristics, anatomical measurements from preoperative computed tomography angiography (CTA), and procedural outcomes were collected and analyzed.
This retrospective case series received ethics approval from the Research Ethics Committee (Study Code: SUR-2568-0394; Research ID: 0394). The study was certified as exempt from informed consent requirements.
Back Table Modification of Physician-modified Endurant Iliac Limbs
The Endurant contralateral iliac limb (Medtronic) was deployed on a sterile back table. For the single fenestration configuration, a circular opening was created just below the overlap marker and reinforced with a double-loop snare wire to enhance fluoroscopic visibility and facilitate precise branch alignment during deployment. The reinforcement was secured using 5-0 Prolene or CV-5 sutures. The size of the fenestration was limited to approximately 6 to 8 mm due to the proximity of adjacent stent struts. To avoid interference with the strut structure, the fenestration was often fashioned in an elliptical shape. The fenestration diameter was selected based on the internal iliac artery size measured from the preoperative computed tomography angiography (CTA).
In the outer branch configuration, a 6-mm polytetrafluoroethylene (PTFE) graft segment measuring 10 mm in length was anastomosed to the outer surface of the graft fabric. Double-loop snare wires were sewn into both the inlet and outlet of the branch to enhance fluoroscopic guidance and facilitate cannulation. This design resulted in an overall branch diameter smaller than most commercial iliac branch devices, which typically incorporate an 8-mm branch, making it relatively smaller even if the difference is only a few millimeters. In Thailand, commercial iliac branch devices are not universally available, and cost remains a barrier for some patients. The outer branch configuration was particularly useful in such cases, offering IIA preservation with a slightly smaller profile than off-the-shelf devices.
The mini-inner branch design was constructed by attaching a 6-mm PTFE graft segment, cut obliquely to a length of 5 mm, to the inner surface of the graft. The outlet of the graft was sutured at the fenestration site, and one end of the inlet was anchored to the inner graft wall adjacent to the stent struts. This configuration provided a short internal channel for bridging stent placement while minimizing intraluminal protrusion.
After completion of the modification, a 0.018-inch guidewire was preloaded into the branch or fenestration by puncturing through the delivery system and advancing the wire into the prepared channel. The endograft was then carefully resheathed using silk ties and reloaded into the delivery system. For the outer branch configuration, which exceeded the internal diameter of the original delivery system, a 17 to 20 French sheath was occasionally required to contain the proximal portion of the graft, while the distal portion was reloaded into the standard delivery system. The process of back-table modification for physician-modified Endurant limbs is detailed in Figure 1.
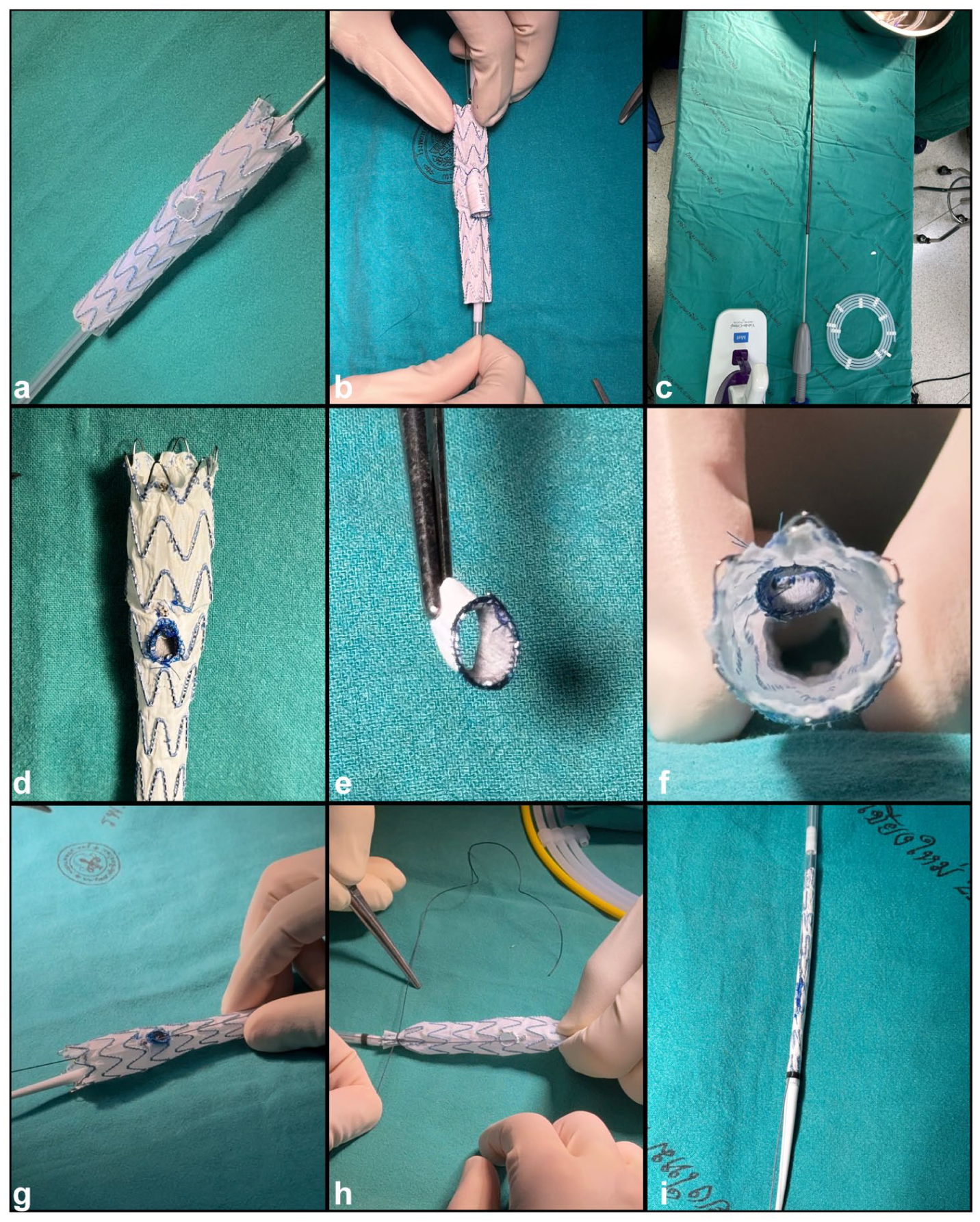
Back table modification of physician-modified Endurant iliac limbs. (A) Single fenestration reinforced with a double-loop snare wire. (B) Outer branch configuration constructed using a 6-mm PTFE graft segment. (C) Large-caliber sheath used to contain the outer branch during reloading. (D–F) Mini-inner branch constructed with an obliquely cut 6-mm PTFE graft segment, sutured at the fenestration and anchored to the inner graft wall. (G) Preloading of a 0.018-inch guidewire through the delivery system into the fenestration or branch. (H) Resheathing of the modified graft using silk ties. (I) Final assembled and reloaded device ready for endovascular deployment.
Procedural Steps
The procedures were performed under either general or locoregional anesthesia. Bilateral femoral artery access was obtained percutaneously using preclosed ProGlide devices. In cases with sufficient common iliac artery (CIA) length, a through-and-through catheter from femoral to contralateral femoral access was used to facilitate insertion of the preloaded 0.018-inch wire. When the CIA was short, a brachial-to-femoral through-and-through catheter was preferred instead. The modified graft was then advanced to the target location under fluoroscopic guidance, with careful attention to rotational alignment of the fenestration or branch with the internal iliac artery (IIA) origin. Bridging stents were deployed between the modified graft and the IIA, followed by balloon flaring to ensure optimal sealing and apposition. After completion of the procedure, completion angiography was performed to confirm aneurysm exclusion, branch patency, and the absence of endoleaks. Figure 2 presents representative intraoperative fluoroscopic images and completion angiography for each configuration, illustrating device positioning, internal structure visualization, and successful exclusion of the aneurysmal sac with preservation of internal iliac artery flow.
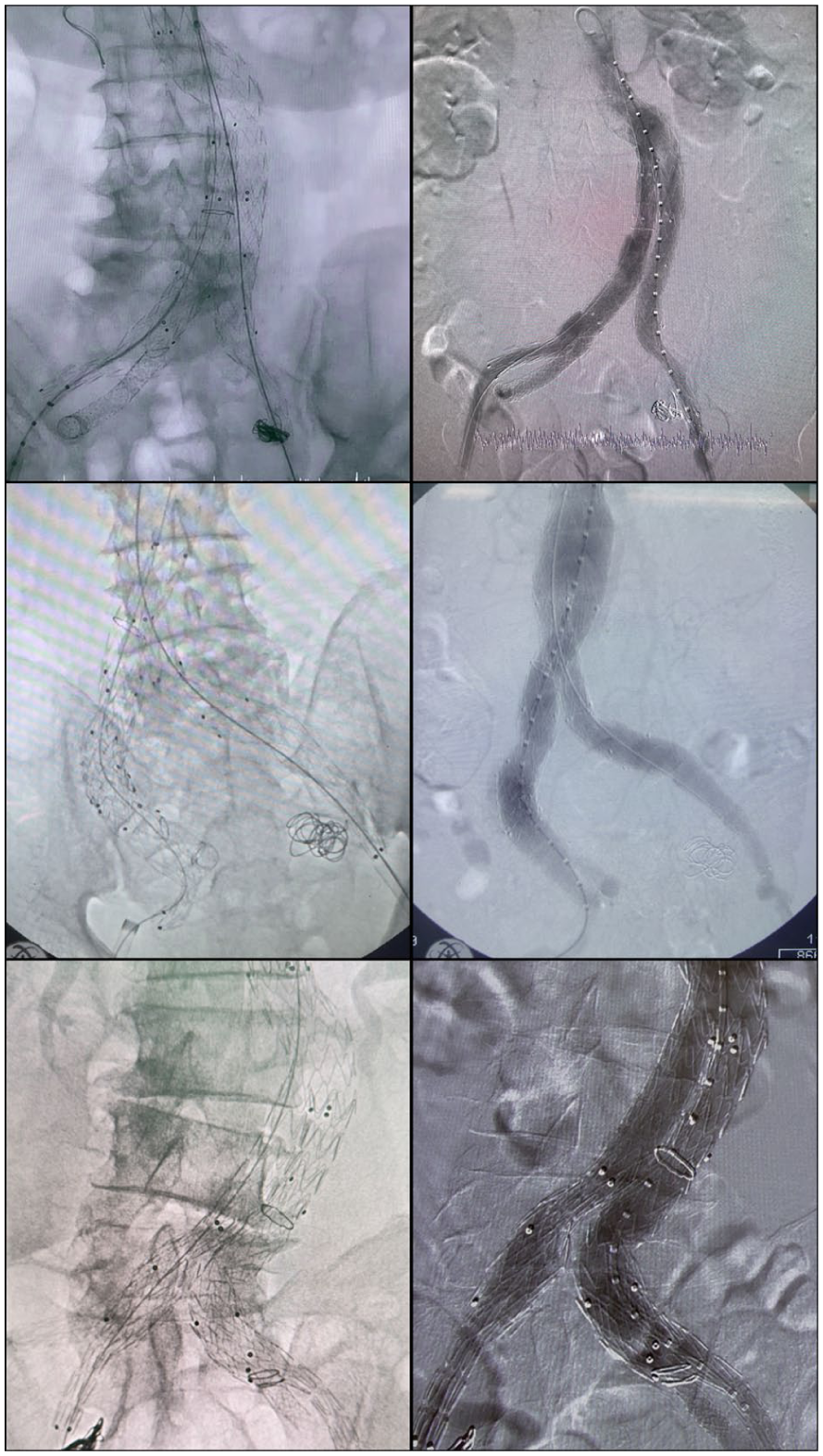
Intraoperative fluoroscopic images demonstrating 3 configurations of physician-modified Endurant iliac limbs. Left column: device positioning and internal structure visualization showing the fenestration site (top), outer branch inlet and outlet (middle), and obliquely cut mini-inner branch with internal fixation (bottom). Right column: completion angiography showing technical success, preservation of internal iliac artery (IIA) flow, and exclusion of the aneurysmal sac in each respective case.
Representative Cases
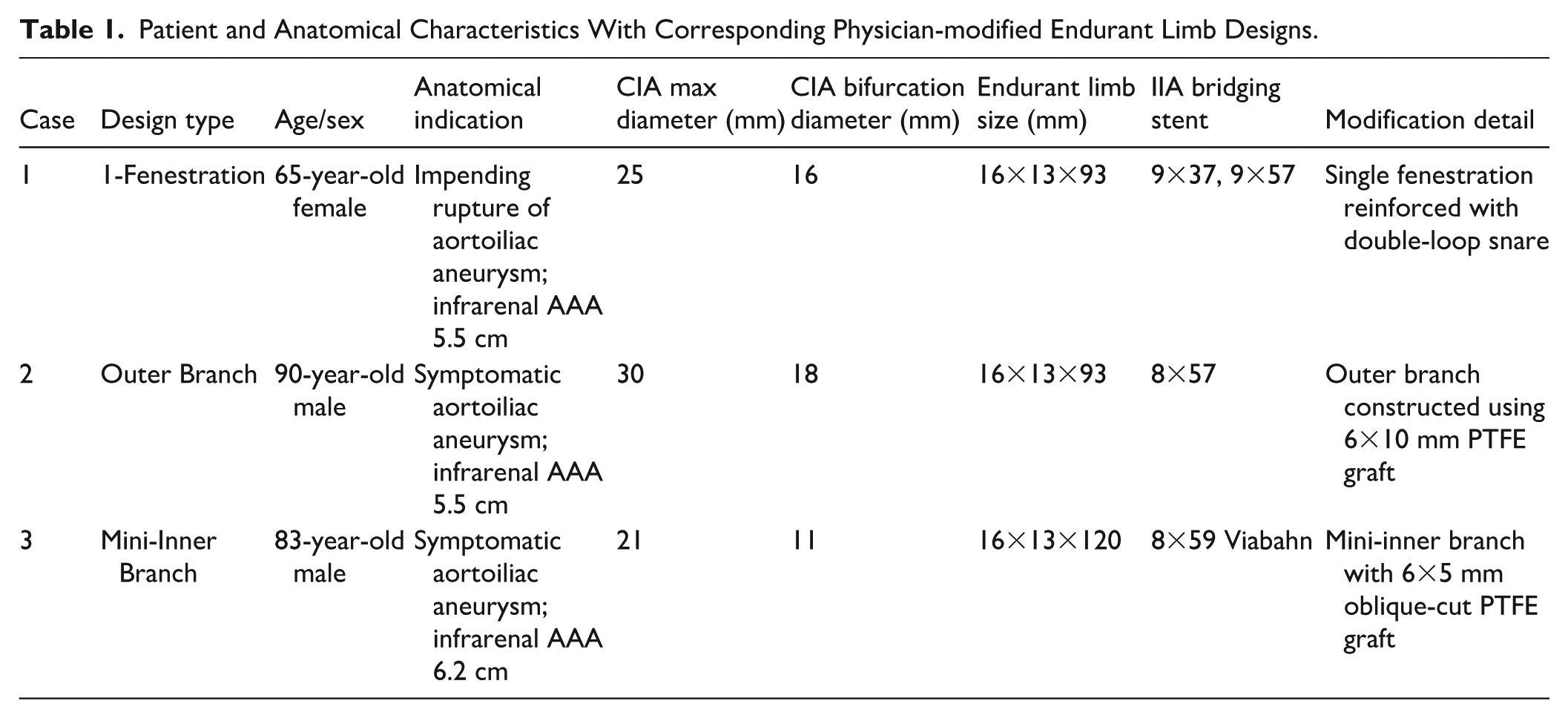
A summary of 3 representative configurations of physician-modified Endurant iliac limbs is provided in Table 1. The designs consisted of single fenestration, outer branch, and mini-inner branch. The initial design utilized a single fenestration, which was considered a suitable configuration for patients with common iliac artery diameters less than 18 mm. While technically straightforward and easily resheathable, concerns were raised regarding the adequacy of sealing between the bridging stent and the limb. To address this limitation, an outer branch configuration was developed to enhance sealing while maintaining a graft profile that remained relatively smaller than off-the-shelf iliac branch devices. However, resheathing the outer branch proved technically challenging and often required the use of a larger sheath to contain the proximal portion of the graft. As a result, the mini-inner branch technique was introduced with the aim of improving sealing while facilitating easier resheathing. This design avoided interference with the external iliac artery lumen and eliminated the need for a larger sheath. Balloon-expandable covered stents were used in all cases for internal iliac artery bridging, with stent sizing determined based on preoperative computed tomography angiography (CTA) measurements.
Patient and Anatomical Characteristics With Corresponding Physician-modified Endurant Limb Designs.
Results
A total of 12 patients underwent physician-modified Endurant iliac limbs procedures during the study period. All patients had aortoiliac aneurysms, with no isolated CIA or IIA aneurysms. The mean CIA bifurcation diameter at the IBD site was 13.9 ± 2.34 mm. Branch patency at 1 month was observed in 11 of 12 patients (91.7%), with one in-hospital death due to stroke. At 3 months, branch patency data were available in 9 patients, all of whom maintained patency. Patency at 12 months was confirmed in 2 patients. The remaining cases are still under follow-up. No type I or type III endoleaks were identified in any of the 12 patients.
Discussion
Previous studies have described the use of single fenestration in physician-modified endografts as a practical technique for internal iliac artery preservation. In principle, this approach offers a smaller graft profile compared to iliac branch devices, making it potentially suitable for narrow iliac anatomy. Based on this concept, we initially adopted the single fenestration configuration, which proved technically feasible. In Thailand, commercial iliac branch devices (IBDs) are not universally available and their cost can limit patient access, making the outer branch configuration particularly valuable when such devices are unavailable. This design provided a more secure sealing interface but required a larger sheath for resheathing and was technically more demanding. Its overall profile was only slightly smaller than that of commercially available IBDs. To overcome these limitations, we introduced the mini-inner branch design as a novel configuration. This approach offered 2 main advantages: improved sealing and simplified resheathing without the need for a larger sheath. Additionally, the design minimized protrusion into the external iliac artery lumen, which may further reduce the risk of limb compromise. Early results demonstrated favorable branch patency without any type I or III endoleaks. Despite these encouraging short-term outcomes, long-term durability and comparative performance against standard off-the-shelf devices remain to be established. Further data from larger cohorts and extended follow-up are required to validate the clinical utility of these configurations, particularly the mini-inner branch design.
Conclusions
Physician-modified Endurant limbs with single fenestration, outer branch, and mini-inner branch configurations are feasible options for internal iliac artery preservation in narrow iliac anatomy. The mini-inner branch, as a novel design, offers a promising balance between sealing efficiency and procedural simplicity. However, further long-term data are needed to confirm its durability and clinical applicability.
Footnotes
Acknowledgements
The authors would like to thank the surgical teams at Maharajnakorn Chiang Mai Hospital and Nakornping Hospital for their technical support and collaboration during the procedures.
Ethics Considerations
This study was reviewed and certified as exempt by the Research Ethics Committee of the Faculty of Medicine, Chiang Mai University, Thailand. Study Code: SUR-2568-0394. Research ID: 0394. The committee operates in accordance with Good Clinical Practice (GCP) guidelines and all relevant national and international regulations and ethical standards.
Consent to Participate
The requirement for informed consent was waived by the Research Ethics Committee of the Faculty of Medicine, Chiang Mai University, as the study was deemed to fall under the exemption category.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The de-identified data supporting the findings of this study are available from the corresponding author upon reasonable request.