
Abstract
Objectives:
Isolated internal iliac artery aneurysm (IIIAA) is a rare condition, accounting for approximately 0.3% to 0.5% of all intra-abdominal aneurysms. This study aimed to evaluate the outcomes of endovascular treatment for IIIAA using a relatively large cohort.
Methods:
A retrospective analysis was conducted on 45 patients diagnosed with IIIAA who were admitted to our hospital between April 2014 and April 2024. Patient demographics, intervention outcomes, and follow-up results were collected and analyzed.
Results:
A total of 45 patients (only 2 female) with 49 IIIAAs were included, with a mean age of 70.4±9.2 years. The cohort exhibited a high prevalence of cardiovascular and cerebrovascular risk factors, and 31.1% had a history of malignancy. Thirty patients (66.7%) were diagnosed with an incidental IIIAA, while the remaining patients presented with symptoms such as abdominal or lumbar pain, dysuria, or aneurysm rupture. Stent-graft placement alone was performed in 3 patients, coil embolization alone in 5 patients, and the remaining 37 patients underwent a combined approach. The rate of complete distal branch embolization was 69.0% (29/42), and technical success was achieved in 44 patients. The mean follow-up duration was 23.8±21.5 months. During follow-up, 5 patients died from cancer or heart failure. Buttock claudication was observed in 7 patients, with only 1 case remaining unresolved after conservative treatment. Sac dilation was noted in 4 patients who had incomplete distal branch embolization; of these, 3 required re-intervention. The 12-month and 24-month re-intervention-free survival rates were 95.5% and 88.2%, respectively.
Conclusion:
Endovascular treatment, particularly the combination of stent-graft implantation and coil embolization, is both safe and effective for IIIAA, with a mid-term re-intervention-free survival rate of 85.25% and an acceptable risk of pelvic ischemia. Complete embolization of the outflow branches is technically challenging in some cases, and the efficacy of sac embolization as an alternative remains debatable.
Clinical Impact
Isolated internal iliac artery aneurysm (IIIAA) is an exceedingly rare condition. This retrospective study identified and included 45 patients with IIIAA who were treated at our institution to evaluate the safety and therapeutic efficacy of endovascular treatment. The majority of patients underwent stent-graft implantation to seal the internal iliac artery ostium, along with coil embolization of the distal branches. The 2-year reintervention-free survival rate for all patients was 85.25%, demonstrating the favorable efficacy of endovascular treatment. However, postoperative sac dilation was observed in 4 patients who did not receive complete distal branch embolization, emphasizing the need for rigorous follow-up in this subset of patients.
Introduction
Internal iliac artery aneurysm (IIAA) is commonly observed in conjunction with other aneurysms, such as aortic aneurysms and common iliac artery aneurysms.1,2 However, isolated internal iliac artery aneurysm (IIIAA), first described by Archibald MacLaren in 1913, is particularly rare, with an estimated incidence of 0.3% to 0.5% of all intra-abdominal aneurysms.3,4 Despite its low incidence, IIIAA should not be overlooked due to its deep anatomical location within the pelvis, its often subtle clinical presentation, and the associated risk of rupture.5,6 For many years, open surgical repair has been the conventional treatment for IIIAA, but it carries a postoperative mortality rate of 10%.7,8 In recent years, endovascular interventions have become increasingly common for treating IIIAA. However, studies evaluating the clinical outcomes of endovascular treatment for IIIAA remain largely limited to case reports and small case series, owing to the rarity of the condition. Therefore, studies with larger cohorts are essential to better assess the safety and efficacy of endovascular treatment for IIIAA. In this study, we aim to report the anatomical characteristics and mid-term outcomes of endovascular treatment for IIIAA, based on a relatively large cohort treated at our center.
Materials and Methods
Patients
The study was approved by the institutional ethics review board (approval number: B2019-231R) and conducted in accordance with the Declaration of Helsinki. Due to the retrospective nature of the study, informed consent was waived. A total of 48 patients with IIIAA who were admitted to our hospital between April 2014 and April 2024 were retrospectively reviewed. The inclusion criteria were as follows: (a) age greater than 18 years; (b) IIIAA confirmed by computed tomography angiography (CTA), magnetic resonance angiography (MRA), and/or digital subtraction angiography (DSA); and (c) availability of complete clinical and radiological data. The exclusion criteria included (a) severe liver or renal dysfunction; (b) pseudoaneurysm; and (c) incomplete data. Demographic data, including gender, age, comorbidities, aneurysm characteristics, and intervention details, were collected and analyzed. Operative and follow-up outcomes of IIIAA patients were also reviewed and analyzed.
Intervention
The indications for intervention were based on several factors, including an aneurysm diameter of at least 30 mm, aneurysm rupture, and overt clinical symptoms such as abdominal or lumbar pain, or symptoms of compression on adjacent organs such as the colorectum or ureter. In cases of ruptured IIIAA, emergency intervention was required.
All procedures were performed under either local or general anesthesia, following standard protocols. For coil embolization, contralateral femoral access was preferred when the anatomical characteristics were favorable. Coil embolization included inflow branch embolization, sac embolization, and outflow branch embolization. To occlude the inflow, stent-graft implantation or inflow branch embolization was performed. To prevent retrograde refilling, complete outflow branch embolization was the primary approach, with sac embolization as an alternative. For patients with an adequate proximal and distal landing zone (≥ 15 mm) and vessel diameter (≥ 5 mm), stent-graft implantation from the proximal to distal internal iliac artery (IIA) was performed. Alternatively, an iliac branch graft (IBD) was used if the proximal landing zone was inadequate but anatomically suitable (Figure 1).
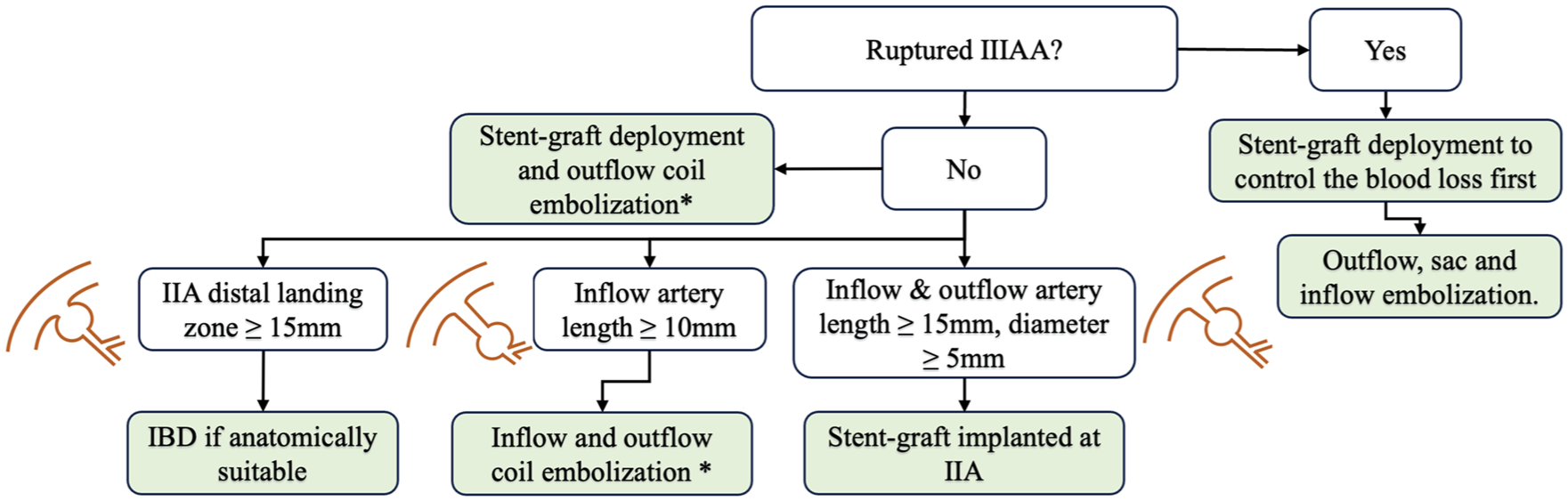
Flow diagram of IIIAA treatment. IIIAA, isolated internal iliac artery aneurysm; IBD, iliac branch-graft device; IIA, internal iliac artery.
Two types of coils were used: detachable coils (Interlock, Boston Scientific, Marlborough, Massachusetts) and undetachable coils (Nester, COOK, Bloomington, Indiana; Tornado, COOK). Stent-graft placement was generally performed after coil embolization (if applicable) via ipsilateral femoral access. However, in cases of ruptured IIIAA, stent-graft deployment was performed prior to coil embolization to control blood loss. The stent-grafts used included Excluder (Gore, Flagstaff, Arizona), Endurant (Medtronic Vascular, Santa Rosa, California), and Viabahn (Gore). The number of stent-grafts used was determined based on the vessel diameters of the common and external iliac arteries. Technical success was defined as the successful deployment of stent-grafts and/or coils as intended, with angiographic evidence of aneurysmal occlusion or sluggish flow under systemic heparinization.
Follow-up
Patients were instructed to undergo at least 1 CTA within 6 months postoperatively, followed by assessments at 12 months and annually thereafter. Magnetic resonance angiography was used as an alternative for patients with impaired renal function. Duplex ultrasound (DUS) was performed in patients with renal insufficiency or contraindications to MRA. During the follow-up period, changes in aneurysm diameter and the presence of endoleak were evaluated using CTA/MRA reformats perpendicular to the artery. Sac dilation was defined as an increase in the maximum aneurysm diameter of 5 mm or more. Adverse events, including mortality, re-intervention, and symptoms of pelvic ischemia (such as buttock claudication, pelvic pain, and ischemic colitis), were also recorded.
Statistical Analysis
The quantitative data, which were compared using the Student’s t-test, are shown as mean±standard deviation (SD) or as the median with the interquartile range (IQRs), depending on their distribution. Categorical variables, presented as frequencies and percentages, were compared using the χ2 test or the Fisher exact test. The re-intervention-free survival rate was calculated with the Kaplan-Meier Product Limit method. All tests were performed using PASW software, version 19 (IBM Corporation, Armonk, New York).
Results
Baseline Characteristics
After excluding 3 lost patients, a total of 45 IIIAA patients who underwent endovascular treatment at our center between April 2014 and April 2024 were identified. The mean age of the patients was 70.4±9.2 years (range=52–85 years), and only 2 were female (4.3%). Of the patients, 20.0% (9/45) presented with abdominal pain, 4.4% (2/45) with lumbar pain, 6.7% (3/45) with dysuria, 2.2% (1/45) with aneurysm rupture, and the remaining 66.7% (30/45) were incidentally diagnosed with IIIAA. The cohort exhibited a relatively high prevalence of cardiovascular and cerebrovascular risk factors, and 31.1% (14/45) had a history of coronary artery disease. Notably, 14 patients (31.1%) had a history of malignancy. Only 1 patient was admitted with a ruptured IIIAA. Among the 44 patients with unruptured aneurysms, 39 had unilateral IIIAA (15 on the left and 24 on the right), and 5 had bilateral IIIAAs. A total of 49 unruptured IIIAAs were identified, with a mean diameter of 44.2±11.2 mm (range=26.1–84.7 mm). Baseline characteristics are detailed in Table 1 and Figure 2.
Preoperative Demographic Characteristics.
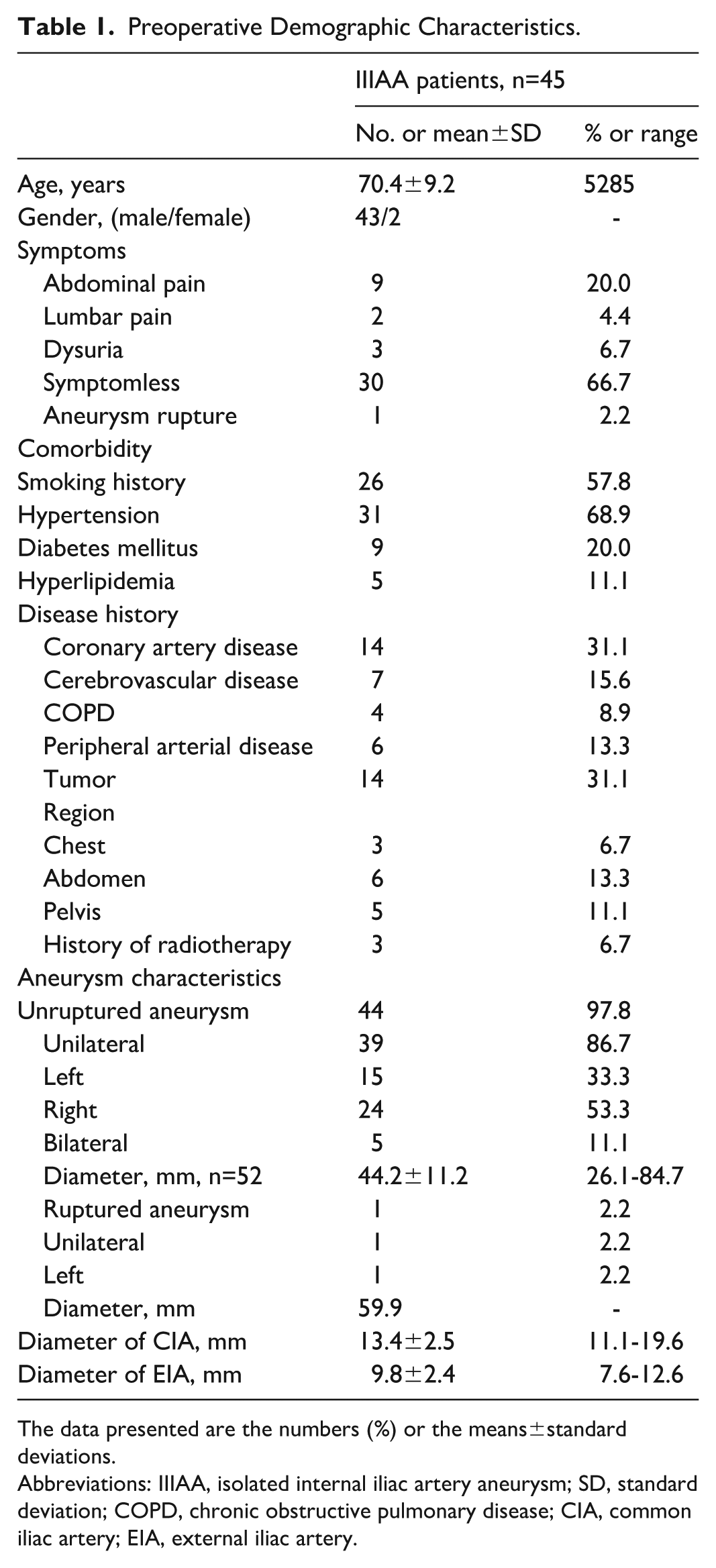
The data presented are the numbers (%) or the means±standard deviations.
Abbreviations: IIIAA, isolated internal iliac artery aneurysm; SD, standard deviation; COPD, chronic obstructive pulmonary disease; CIA, common iliac artery; EIA, external iliac artery.
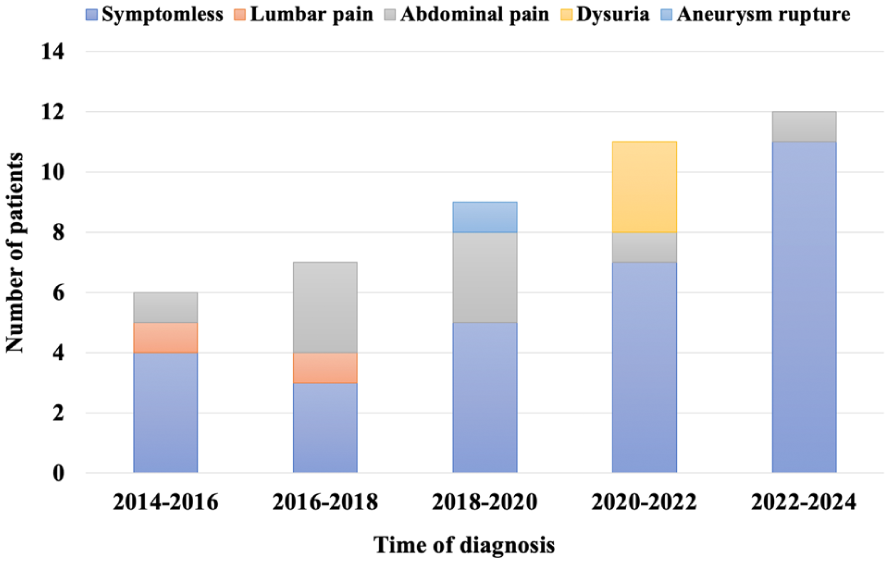
Data and symptoms of IIIAA patients at the time of diagnosis. IIIAA, isolated internal iliac artery aneurysm.
Intervention Outcomes
General anesthesia was used in 32 patients, while 12 patients underwent the procedure under local anesthesia. Bilateral IIIAA intervention was performed in 2 patients: one received stent-graft implantation only, and the other received an iliac branch device (IBD) placement along with contralateral IIA stent-graft implantation (Figure 3). The remaining 43 patients underwent unilateral IIA intervention, including stent-graft implantation alone (n=1), coil embolization alone (n=5), and a combined approach (stent-graft placement and coil embolization, n=37). All stent-grafts were deployed via ipsilateral femoral access, and all coil embolization procedures were performed through a 6F-45 cm sheath (COOK) via contralateral femoral access. The complete distal branch embolization success rate was 69.0% (29/42).
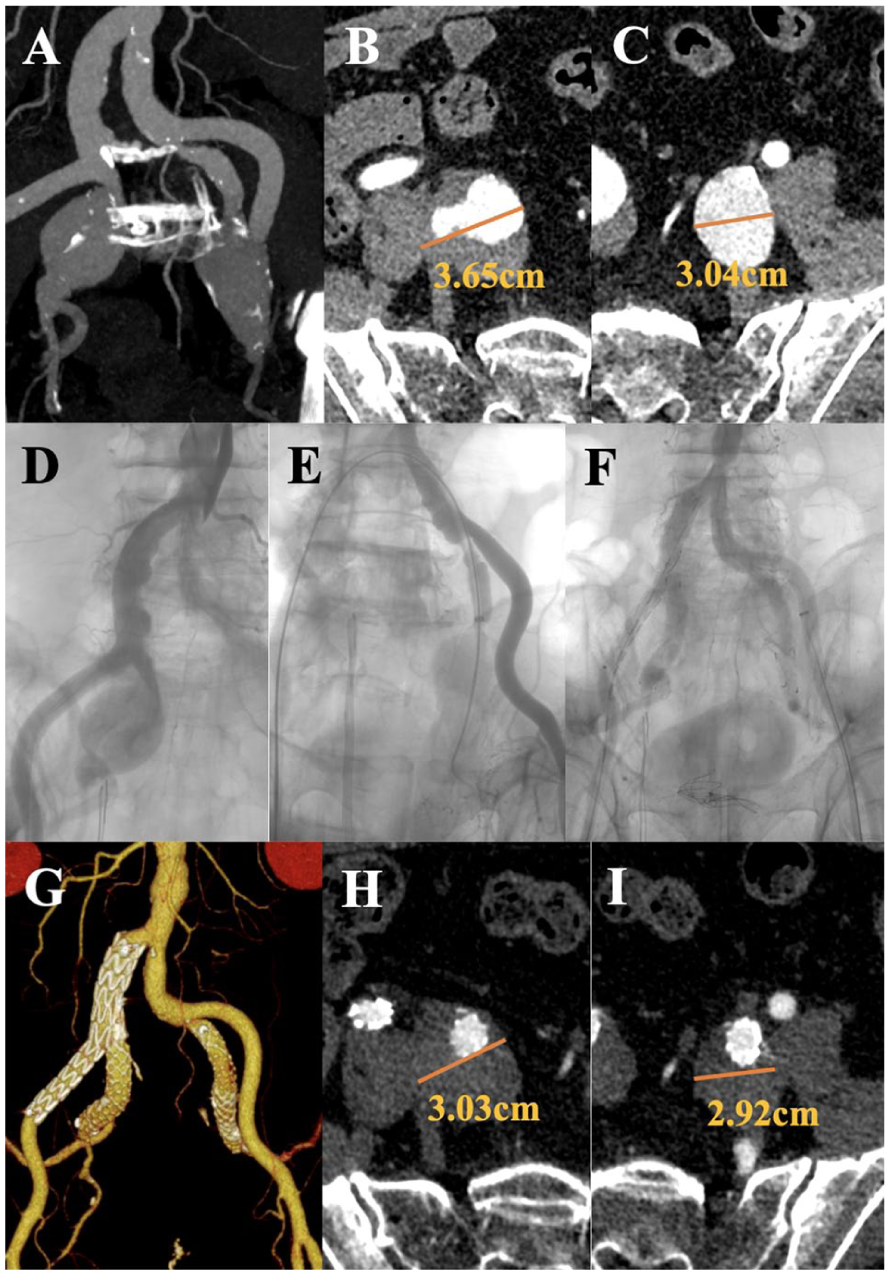
A 67-year-old male patient was admitted following incidental detection of bilateral IIIAAs (A-C). A 12×100 mm SilverFlow stent-graft (LifeTech Scientific, Shenzhen, Guangdong, China) was implanted in the left IIA to exclude the aneurysm. A 16-10×120 mm IBD (LifeTech Scientific, Shenzhen, Guangdong, China) was then placed between the right common and external iliac arteries, followed by a 12×100 mm SilverFlow stent-graft extending into the right IIA (D–F). No symptoms of pelvic ischemia were observed. The 12-month follow-up CTA revealed a reduced sac size and patent outflows (G–I). IIIAA, isolated internal iliac artery aneurysm; IIA, internal iliac artery; IBD, iliac branch-graft device.
The stent-grafts used included Excluder (Gore) iliac limb (n=27), Endurant (Medtronic) iliac limb (n=6), Viabahn (Gore) covered-stent (n=6), and IBD (LifeTech) (n=1). The mean proximal diameter of all stent-grafts was 15.4±2.2 mm (range=8–18 mm), and the mean distal diameter was 12.0±1.3 mm (range=8–14 mm). Except for coil migration in 1 patient (which was captured and removed using a Snare), technical success was achieved in all other patients.
Postoperative immediate endoleak was observed in 13 patients. More detailed information on intervention characteristics is shown in Table 2. During hospitalization, adverse events included protamine-induced anaphylactic shock (1/45), cerebral hemorrhage (1/45), and acute renal failure (1/45, due to ruptured IIIAA). These 3 patients were transferred to the intensive care unit (ICU) for further treatment, and their symptoms were resolved before discharge. The mean length of hospital stay was 5.8±3.8 days.
Intervention Characteristics.
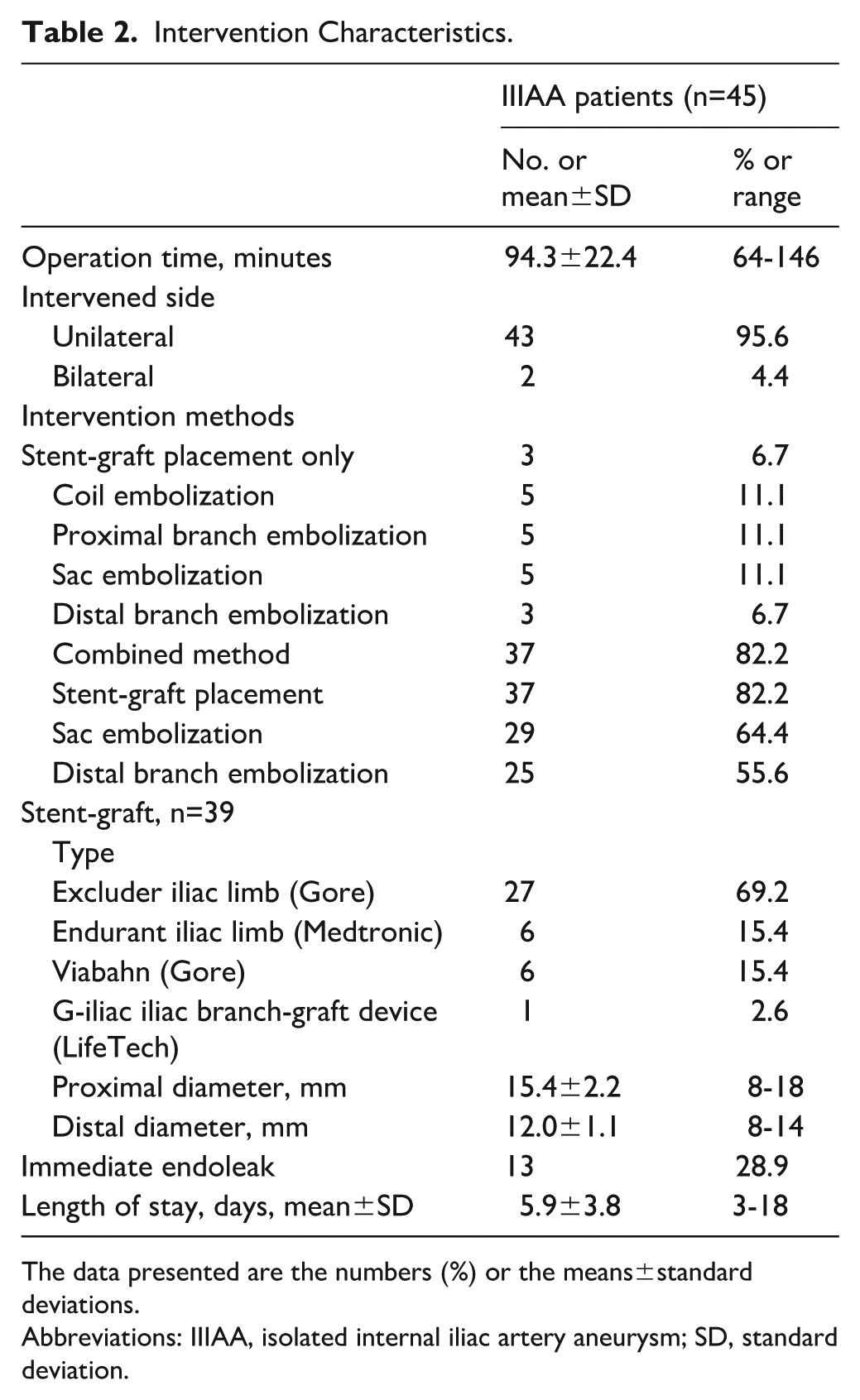
The data presented are the numbers (%) or the means±standard deviations.
Abbreviations: IIIAA, isolated internal iliac artery aneurysm; SD, standard deviation.
Follow-up Outcomes
Within 30 days after intervention, buttock claudication was observed in 7 patients who received the combined method. Symptoms in 6 of these patients were alleviated or eliminated within 6 months after conservative treatment, including drug therapy. The remaining patient’s symptoms did not worsen at the last follow-up. No cases of pelvic pain, ischemic colitis, or spinal cord ischemia were observed.
The mean follow-up time was 23.8±21.5 months (range=3–92 months). During the follow-up period, 4 patients died of cancer-related complications at 3 months, 14 months, 30 months, and 92 months, respectively, and 1 patient died of heart failure at 25 months. Among the 13 patients with immediate endoleak on their completion angiogram, the endoleak disappeared in 8 patients by the last CTA. Of the remaining 5 patients, 4 had IIIAA sac dilation, including 1 with unilateral stent-graft implantation, 1 with a proximal IIA dense sac and incomplete outflow branch embolization, and 2 with stent-grafts covering the ostium of IIA with a dense sac and incomplete branch embolization. Detailed data concerning follow-up outcomes were shown in Table 3.
Perioperative Adverse Events and Follow-up Outcomes.
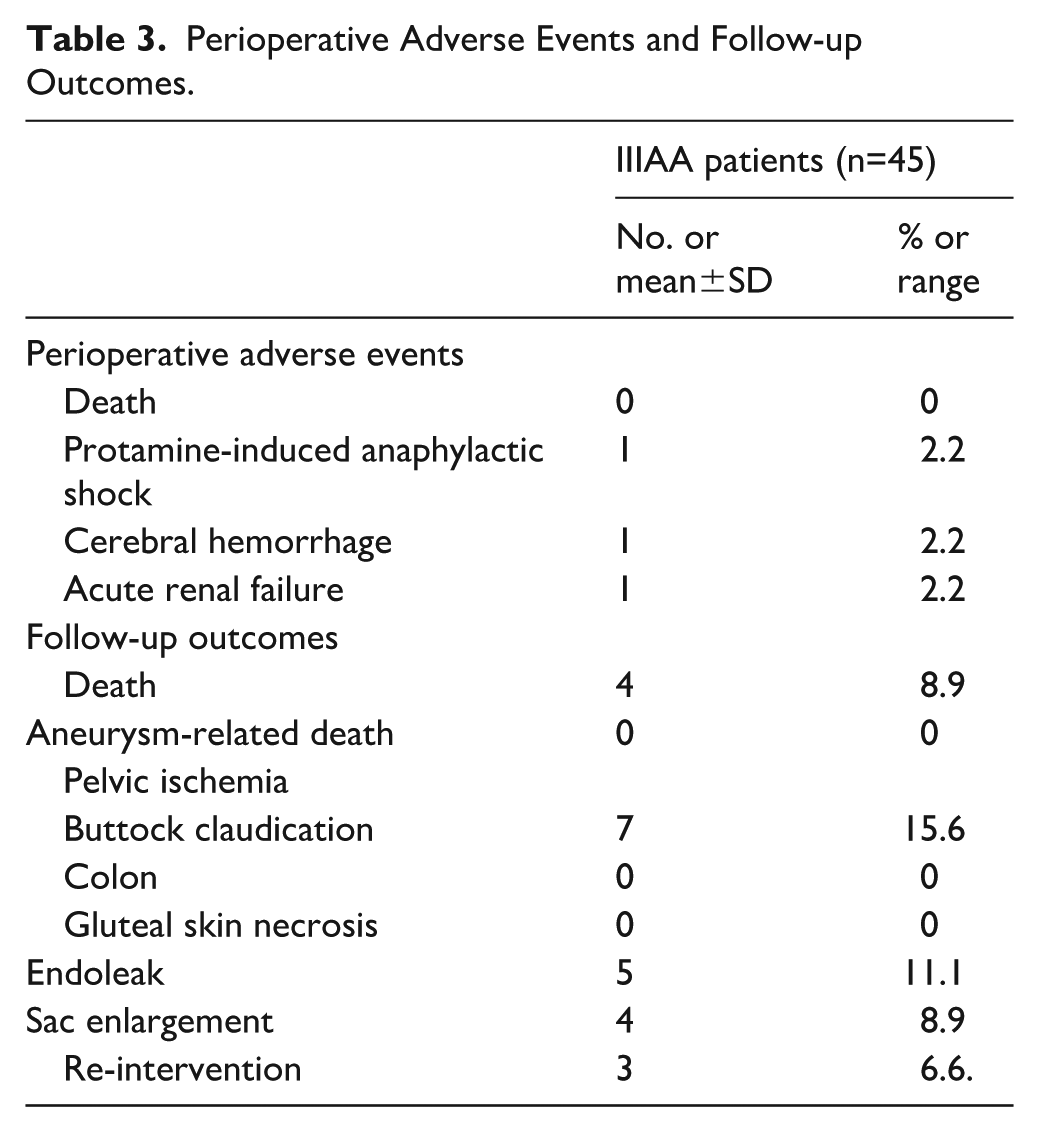
There was no significant difference between the preoperative and postoperative maximum diameter of the 47 treated IIIAAs (46.5±12.6 mm vs 42.3± 11.7 mm, p=0.095). Among the 4 patients with sac dilation, re-intervention was performed in 3 patients: 1 patient with stent-graft implantation only underwent open resection (Figure 4); 2 patients who had received the combined method underwent embolization via contralateral IIA/ipsilateral deep femoral artery; the remaining patient, who had also received the combined method, did not undergo re-intervention due to deteriorating cardiac function and ultimately died of heart failure at 25 months.
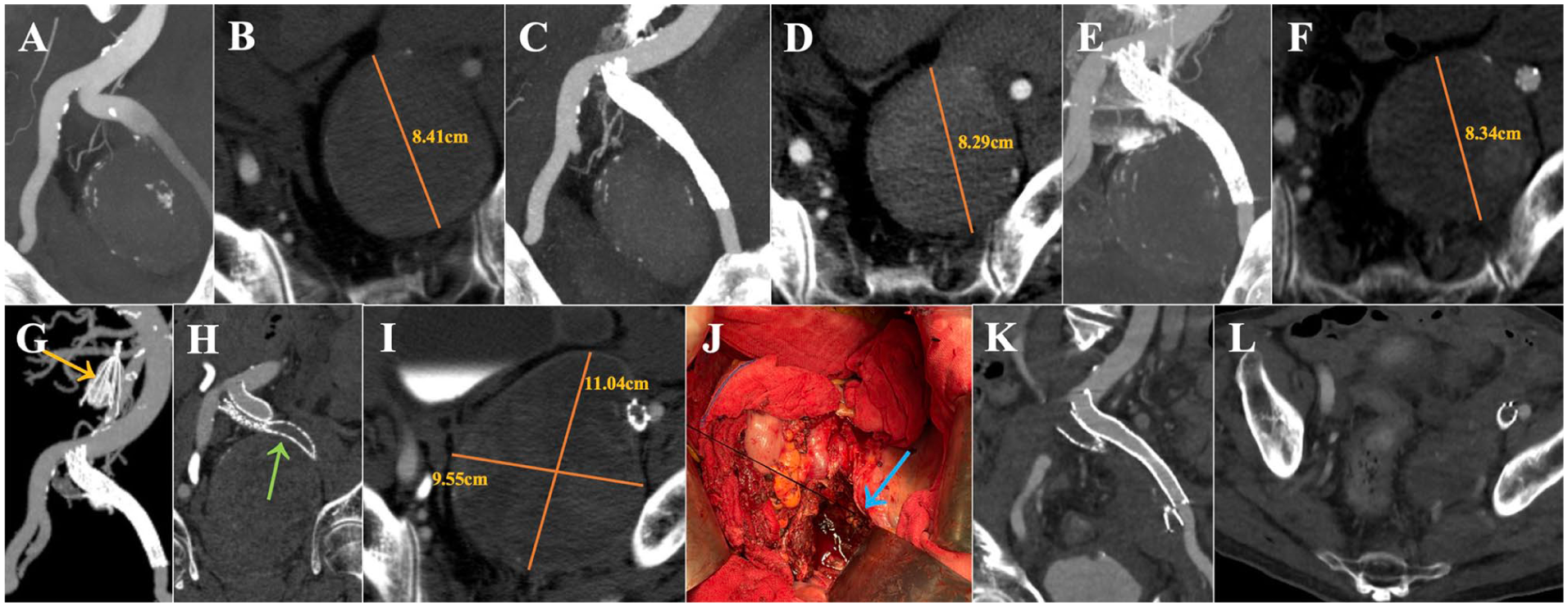
A 54-year-old male with a left giant IIIAA (A and B) underwent stent-graft implantation to cover the ostium of the IIA in 2014. Six-month (C and D) and 12-month (E and F) follow-up CTA showed stable aneurysm maximum diameter. During follow-up, left lower limb deep vein thrombosis (DVT) occurred to the patient and he decided to receive an inferior vena cava filter (G, yellow arrow) and left iliac vein stent implantation at a local hospital (H, green arrow). At 17 months, the patient was sent back to the emergency department of our hospital for abdominal pain, and CTA revealed a ruptured IIIAA (I). The ruptured aneurysm was emergently resected (J, blue arrow: ostium of IIA), and postoperative CTA confirmed the success of the procedure (K and L). IIIAA, isolated internal iliac artery aneurysm; CTA, computed tomographic angiography; DVT, deep vein thrombosis; IIA, internal iliac artery.
The 12-month and 24-month re-intervention-free survival rates for all patients were 95.50% and 88.22%, respectively (Figure 4A). All stent-grafts remained patent during follow-up. For the subgroup that received the combined method (40/48, 83.3%), the 12-month and 24-month re-intervention-free survival rates were 94.52% and 85.25%, respectively (Figure 5B).
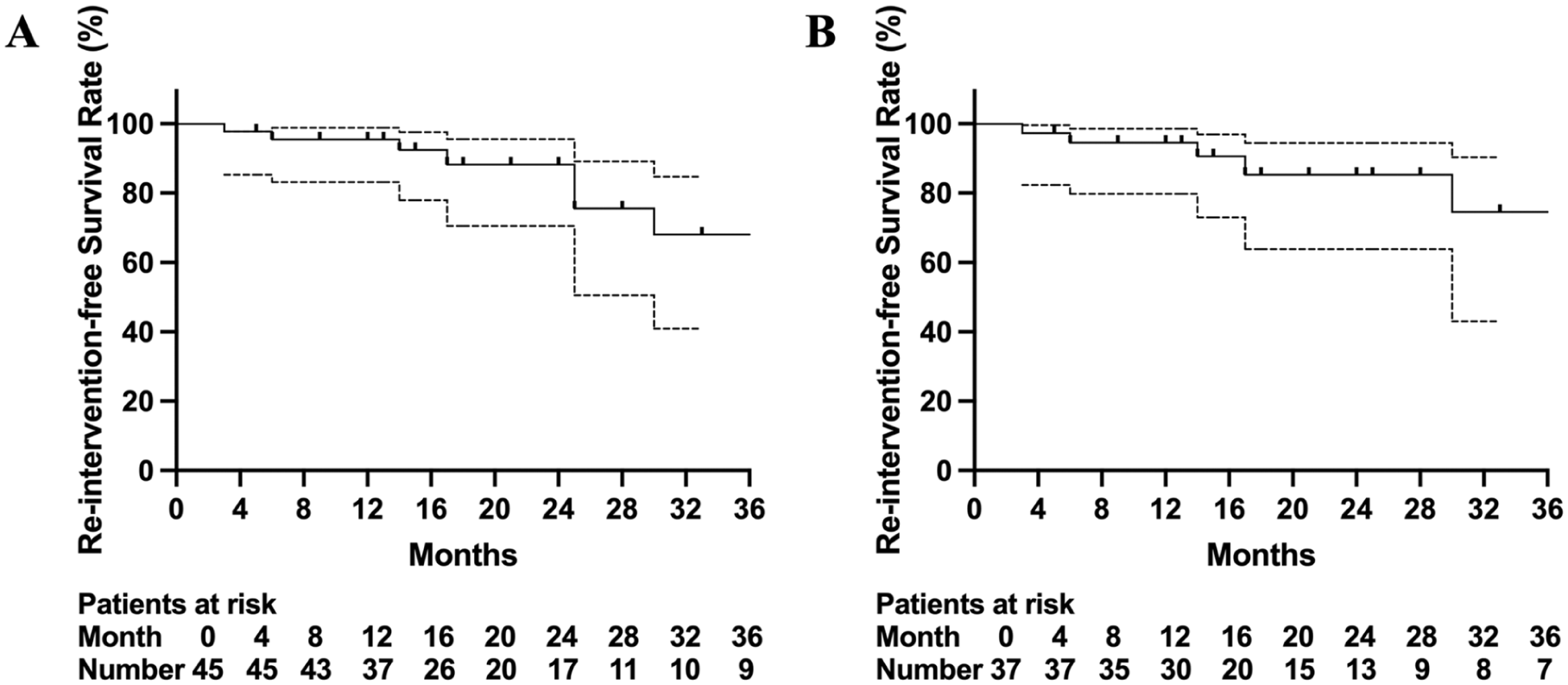
Kaplan-Meier curves showing the re-intervention-free survival rates for all IIIAA patients (A) and for those who received combined methods (B). IIIAA, isolated internal iliac artery aneurysm.
Discussion
Isolated internal iliac artery aneurysm accounts for 2%–7% of all intra-abdominal aneurysms,9–11 but IIIAA is particularly rare in clinical practice, and most of the knowledge regarding its incidence and prevalence is derived from autopsy data and case series.2,12–15 The current study identified and enrolled 45 IIIAA patients who underwent endovascular treatment, aiming to analyze and report their baseline data, anatomical characteristics, and clinical outcomes, demonstrating the safety and feasibility of endovascular intervention.
Previous reviews of IIIAA have highlighted several common patient characteristics, including a male-dominated demographic, a high prevalence of cardiovascular risk factors, admission or diagnosis due to symptoms such as abdominal/lumbar pain, and predominantly unilateral IIIAAs. In line with these findings, our study observed that 43 out of 45 patients (95.6%) were male, with 68.9% having hypertension and 57.8% having a smoking history. Only 5 patients had bilateral IIIAAs. Notably, among the 30 asymptomatic patients, almost half (14/30, 46.7%) had a history of tumors. The proportion of asymptomatic patients has steadily increased over the years (Figure 2). These observations suggest that advances in medical imaging technologies and increased public awareness have led to the earlier detection of asymptomatic IIIAAs, contributing to a reduction in the incidence of ruptured aneurysms. Asymptomatic IIIAAs account for 50% to 70% of all IIIAA cases,8,16 likely due to the deep location of the IIA within the pelvis. Rupture of IIIAA, however, carries a high mortality rate of around 50%, 2 further emphasizing the importance of early detection.
Traditional surgical treatments for IIIAA, such as ligation of the proximal and distal branches, have been commonly employed. Similarly, endovascular treatments also aim to occlude both the inflow and outflow branches to achieve optimal clinical outcomes. In this study, the treatment options for IIIAA included coil embolization and stent-graft placement, with most patients (37/45) receiving a combined approach. The IIIAA patients typically had normal-caliber common and external iliac arteries, allowing for satisfactory sealing of the IIA ostium with appropriate stent-grafts. The choice of stent-graft was primarily based on the diameter of the common and external iliac arteries, with Excluder/Endurant stent-grafts having a minimum distal diameter of 10 mm and Viabahn covered-stents reaching up to 13 mm. Coil embolization plays a crucial role in preventing retrograde refilling, thereby reducing the risk of re-intervention. However, it can be technically challenging and time-consuming, particularly in cases of large aneurysms or multiple branches. In our study, complete distal branch embolization was successfully achieved in 69.0% (29/42) of patients, which is consistent with previous reports.17–19 Muradi et al 20 found that incomplete embolization of outflow branches was associated with sac enlargement and the need for secondary intervention, although it was linked to a lower incidence of buttock claudication during follow-up. Consequently, dense sac embolization was performed as an alternative when complete distal branch embolization was not possible. However, sac enlargement was still observed in 3 out of 14 patients who received sac embolization, indicating that its effectiveness remains uncertain and underscores the need for rigorous follow-up. The 24-month re-intervention-free survival rates for all patients and those who underwent the combined method were 88.22% and 85.25%, respectively, suggesting that endovascular treatment can achieve satisfactory outcomes for IIIAA patients. It is undeniable that open surgery remains the last line of defense in the management of IIIAA. One patient received open resection owing to consistent enlargement and final rupture of aneurysmal sac (Figure 4). Generally, concurrent vascular reconstruction with a prosthetic graft might be ideal. However, there are technical difficulties of reconstruction including the deep anatomical location within the pelvis and atherosclerotic distal IIA.
Pelvic ischemia is a significant concern when embolizing the IIA. Seven patients in our study developed buttock claudication, but none required surgical reconstruction. Studies on endovascular repair of aortoiliac aneurysms report a pelvic ischemia incidence ranging from 10% to 55% after sacrificing the IIA.21–23 Bratby et al 23 observed that embolization limited to the main trunk of the IIA resulted in a significantly reduced ischemic complication rate compared with more distal embolization. Accordingly, in our study, we aimed to perform embolization as proximally as possible, starting from the sac origin, to minimize the risk of pelvic ischemia. For most IIIAA patients, branch embolization seemed to be the only viable endovascular approach to prevent retrograde refilling. In very few cases with ideal proximal and distal landing zones (≥15 mm) and a diameter ≥ 5 mm, stent-graft exclusion of IIIAA was feasible without concerns of ischemia. 24
One patient in our study received a unilateral IBD and contralateral stent-graft exclusion, and no pelvic ischemia or endoleak was observed during follow-up (Figure 3). Since 2022, IBD has become available in China, offering an alternative to traditional approaches by bypassing the need for a proximal landing zone. Noel-Lamy et al 1 reported that even the distal landing zone might not be necessary when the internal iliac component of the IBD extends into the superior gluteal artery, with no pelvic ischemia or endoleak observed. However, IBD is primarily designed to preserve IIA flow in the endovascular treatment of common iliac artery (CIA) aneurysms, with anatomical constraints such as a CIA diameter ≥ 18 mm. In our study, IIIAA patients had relatively small CIA diameters, with a mean stent-graft proximal diameter of 15.4 ± 2.2 mm, limiting the usability of IBD. In addition, the 2 most commonly used IBDs at our center (Gore IBE and LifeTech IBD) require a CIA length ≥ 5 cm, a condition rarely observed in the Chinese population. Even in anatomically suitable cases, IBD may not be the optimal choice for IIIAA. Aneurysms in the main trunk of the IIA increase the difficulty of IBD deployment and are associated with a higher risk of postoperative endoleak.25,26 Furthermore, Parlani et al 27 identified IIA aneurysms as a predictor of re-intervention after IBD deployment.
There are several limitations to this study. First, it was a retrospective study with a small cohort of IIIAA patients. However, given the rarity of IIIAA cases, the cohort in this study is relatively larger than others in the literature. Second, the study spanned a long period during which treatment techniques and devices evolved. Long-term outcomes with larger cohorts of IIIAA patients are needed to confirm these findings.
Conclusion
Endovascular treatment, particularly the combination of stent-graft implantation and coil embolization, is a safe and effective approach for treating IIAA, with a mid-term re-intervention-free survival rate of 85.25%. The risk of pelvic ischemia is manageable, and the procedure demonstrates an acceptable safety profile. However, complete embolization of outflow branches remains technically challenging, and the effectiveness of sac embolization as an alternative requires further evaluation.
Footnotes
Authors’ Note
The manuscript has been read and approved by all the authors, that the requirements for authorship as stated earlier in this document have been met, and that each author believes that the manuscript represents honest work.
Ethics Approval and Consent to Participate
The study design was approved by the Ethics Committee of Zhongshan Hospital, Fudan University, Shanghai, China. All included patients were informed about the nature of the study and gave their written informed consent.
Consent for Publication
All patients signed a consent form for their data to be used for research or publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The China National Natural Science Funds (Grant Nos 82400568 and 82270507) and the Outstanding Resident Clinical Postdoctoral Program of Zhongshan Hospital Affiliated to Fudan University (2024).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.