
Abstract
Aim:
To present a case in which low-dose 4-dimensional computed tomographic angiography (4D-CTA) enabled precise classification of a type II endoleak following hybrid arch repair for chronic type B aortic dissection, in the setting of inconclusive findings on conventional CTA.
Case:
A 74-year-old woman underwent hybrid arch repair with left common carotid-subclavian bypass and thoracic endovascular aortic repair for chronic type B aortic dissection. Six years postoperatively, aneurysm sac enlargement was noted. Conventional CTA with a 2-phase protocol (early arterial and delayed venous phases) could not distinguish between type Ia and type II endoleaks. Low-dose 4D-CTA (dose-length product: 302.6 mGy·cm) revealed delayed contrast enhancement within the sac during the late arterial phase, consistent with a type II endoleak originating from the left subclavian artery (LSCA). Targeted coil embolization was successfully performed to resolve the endoleak, and contrast inflow from a branch of the LSCA was confirmed by intraprocedural angiography.
Conclusion:
Low-dose 4D-CTA allowed for precise classification of the endoleak and guided appropriate reintervention. This modality represents a useful and practical tool for endoleak evaluation, especially when standard imaging is inconclusive.
Clinical Impact
This case highlights the diagnostic value of 4-dimensional computed tomographic angiography (4D-CTA) in classifying endoleaks after thoracic endovascular aortic repair (TEVAR), particularly when standard CTA is inconclusive. The 4D-CTA identified a type II endoleak from the left subclavian artery, enabling definitive diagnosis and targeted coil embolization. Notably, the scan was performed using a low-dose protocol (dose-length product: 302.6 mGy·cm), substantially lower than the >1000 mGy·cm reported in prior studies while preserving diagnostic quality. Standardized low-dose 4D-CTA protocols may support broader clinical adoption for endoleak evaluation.
Introduction
Aneurysm sac enlargement after thoracic endovascular aortic repair (TEVAR) is frequently linked to endoleaks, and accurate classification is essential to guide appropriate secondary intervention. However, conventional contrast-enhanced computed tomographic angiography (CTA) with a 2-phase protocol (early arterial and delayed venous phases) for post-endovascular follow-up can be inconclusive due to subtle or overlapping findings. Four-dimensional computed tomographic angiography (4D-CTA), which provides time-resolved visualization of contrast dynamics, has emerged as a valuable adjunct in these settings.1,2 Despite its diagnostic advantages, increased radiation exposure has been reported as a limitation of 4D-CTA.3,4 The primary reason for the higher radiation dose in 4D-CTA is the requirement to ensure temporal resolution through multiple acquisitions and repeated scanning.3,4 Although no adverse effects have been reported from a single high-dose 4D-CTA, dose reduction remains an important issue to be addressed. We present the case of a 74-year-old individual with chronic type B aortic dissection and distal arch enlargement 6 years after hybrid arch repair, where low-dose 4D-CTA enabled precise endoleak classification and facilitated targeted reintervention.
Case Report
According to institutional policy, ethical approval was waived for single-case reports. Written informed consent for publication of this case and the accompanying images was obtained from the patient. A 74-year-old woman with a history of hypertension and chronic kidney disease initially presented with acute type B aortic dissection 10 years earlier. Over time, the distal aortic arch gradually expanded from 35 mm to 55 mm. Six years prior, she underwent hybrid arch repair for a 55 mm dissecting arch aneurysm due to false lumen expansion, consisting of a left common carotid-subclavian artery bypass and coil embolization of the left subclavian artery (LSCA), followed by TEVAR with a zone 2 landing to exclude the primary entry tear along the greater curvature. Postoperative CTA showed complete thrombosis extending to the distal end of the stent graft with no evidence of endoleak. After the hybrid arch repair, the patient was monitored clinically, with contrast-enhanced CT at 6 months and 1 year postoperatively, and annual non-contrast CT thereafter. The aneurysm sac remained stable at ~50 mm for 5 years, at the 6-year follow-up, sac enlargement to 58 mm prompted re-evaluation.
Conventional CTA, performed with a routine 2-phase protocol (early arterial and delayed venous phases), revealed a “moyamoya-like” endoleak in the false lumen (Figure 1). As described by Iwakoshi et al, 5 a “moyamoya-like” endoleak is defined as a heterogeneous contrast opacity with an indistinct border on CT; however, in this case, the finding could not differentiate between type Ia and type II endoleaks. To clarify the diagnosis, 4D-CTA was performed using a low-dose protocol before diagnostic angiography. The 4D-CTA was performed using an 80 row multidetector CT scanner (Aquilion Prime SP; Canon Medical Systems, Tochigi, Japan) with the following general parameters: 100 kVp tube voltage, 24 second scan duration, and 4.45 cm coverage. The scan was successfully completed with a dose-length product (DLP) of 302.6 mGy·cm. The 4D-CTA revealed sac enhancement during the late arterial phase, consistent with a type II endoleak from the LSCA (Figure 2). Based on these findings, additional coil embolization of the LSCA was performed. Intraprocedural angiography confirmed contrast inflow from an LSCA branch (Figure 3). One-year follow-up CTA showed no residual endoleak and no further sac enlargement.
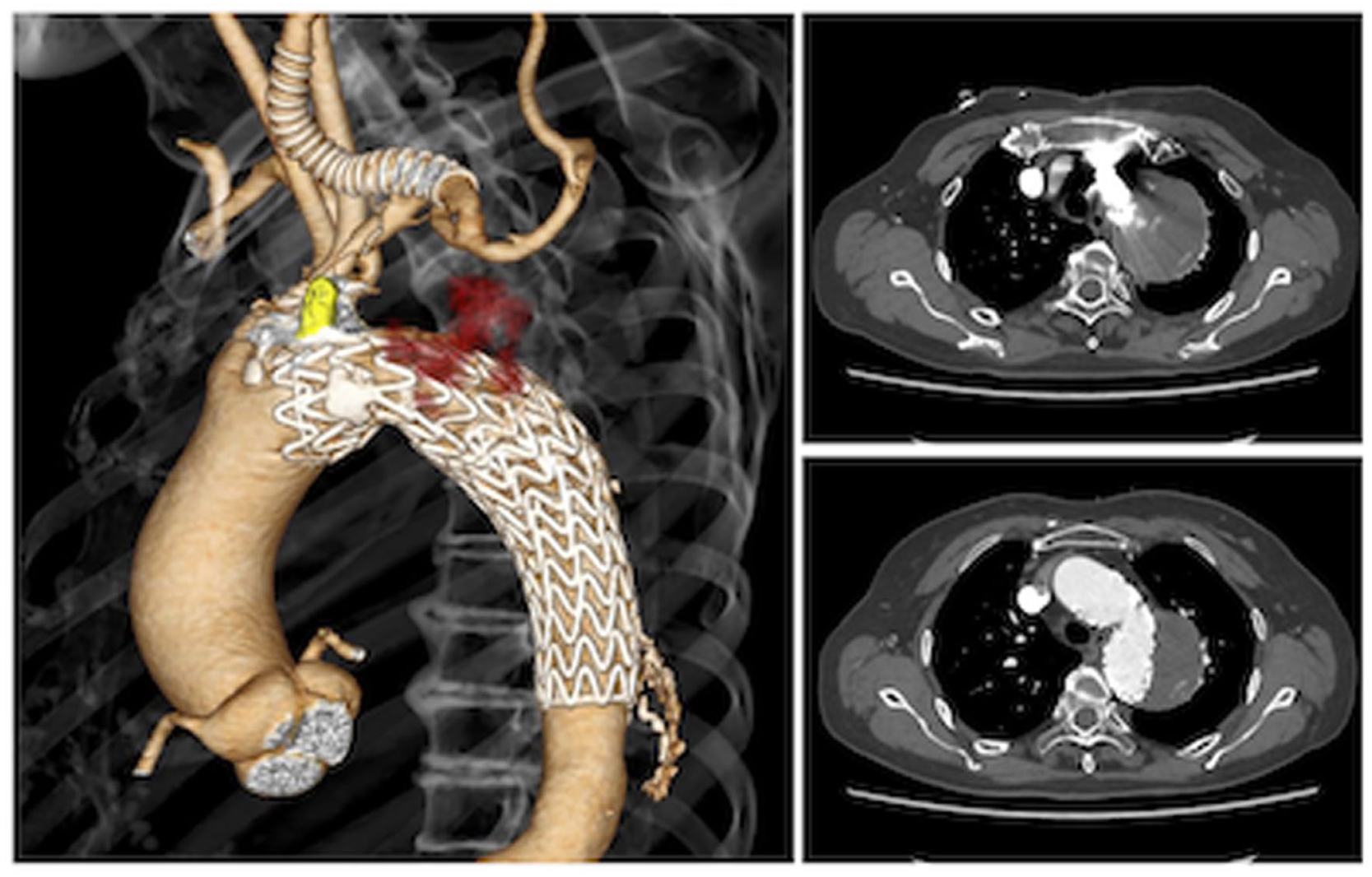
Four-dimensional computed tomographic angiography (CTA). 4D-CTA revealed a “moyamoya-like” endoleak within the false lumen of the distal aortic arch; that is, 4D-CTA revealed delayed contrast enhancement within the aneurysm sac during the late arterial phase, consistent with a type II endoleak originating from the left subclavian artery in a patient previously treated with hybrid arch repair. However, it was inconclusive in distinguishing between type Ia and a type II endoleaks.

Four-dimensional computed tomographic angiography (4D-CTA). 4D-CTA revealed delayed contrast enhancement within the aneurysm sac during the late arterial phase, consistent with a type II endoleak originating from the left subclavian artery.
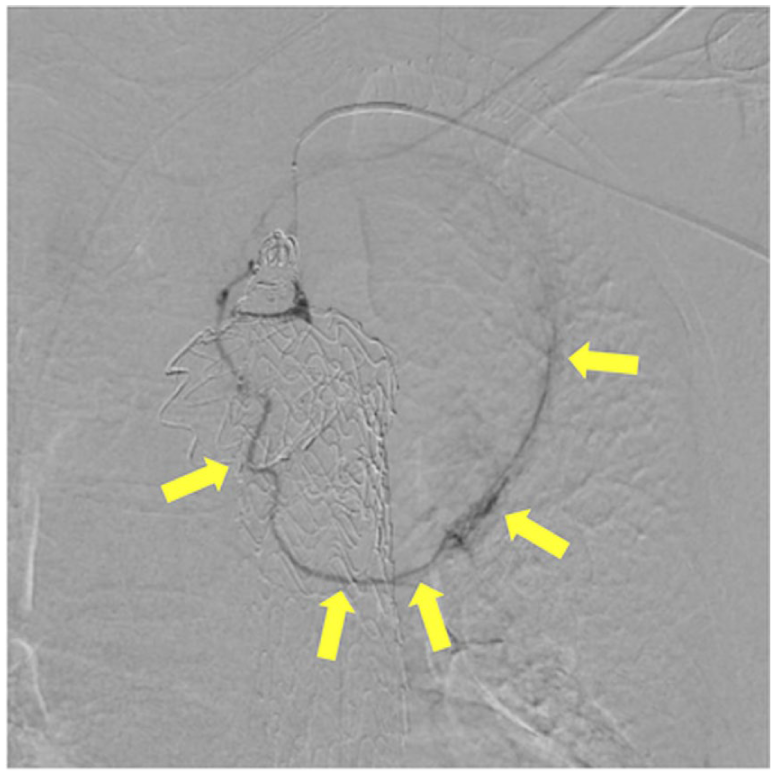
Intraprocedural angiography. Intraprocedural angiography confirmed persistent contrast inflow into the aneurysm sac from a branch near the origin of the left subclavian artery.
Discussion
The 4D-CTA has been shown to improve both endoleak detection and classification, particularly when conventional imaging yields equivocal results.1,3,4,6 Waldeck et al 2 reported significantly higher sensitivity of 4D-CTA compared with standard CTA, underscoring its diagnostic value. However, a major limitation of 4D-CTA remains its high radiation dose. In previous studies, the DLP has exceeded 1000 mGy·cm, primarily due to the requirement to ensure temporal resolution through multiple acquisitions and repeated scanning.3,4 Although no adverse effects have been reported from a single high-dose 4D-CTA, dose reduction remains an important issue to be addressed.
In this case, the most critical factor contributing to radiation dose reduction was the use of an 80 row multidetector CT scanner. Whereas most previous reports have employed 320 row scanners,3,4 the use of an 80 row scanner theoretically allows for imaging at approximately one quarter of the radiation dose under the same scanning conditions. In the present case, this was reflected in the DLP of 302.6 mGy·cm, which was substantially lower than previously reported values while maintaining diagnostic image quality for accurate endoleak classification. Conversely, the drawback is that while the radiation dose with an 80 row scanner can be reduced to one quarter, the scan coverage is also only one quarter compared with a 320 row scanner. In the present case, conventional CTA had already suggested either a type Ia endoleak or a type II endoleak from the LSCA, allowing us to focus the 4D-CTA acquisition on the region just distal to the LSCA (Figure 2). This targeted approach enabled accurate endoleak characterization despite the restricted coverage. This result highlights the feasibility of low-dose 4D-CTA protocols and their potential to reduce radiation exposure without compromising accuracy. Broader adoption of optimized scanning strategies may support more routine use of 4D-CTA in evaluating individuals with suspected endoleaks after endovascular aortic repair.
Conclusion
This case demonstrates that low-dose 4D-CTA can achieve accurate classification of endoleaks after hybrid arch repair, even when conventional CTA is inconclusive. Importantly, diagnostic image quality was maintained despite the reduced radiation dose, highlighting the feasibility of radiation-sparing approaches. Optimized low-dose 4D-CTA may therefore represent a reliable and practical imaging tool for evaluating individuals after endovascular aortic repair.
Footnotes
Acknowledgements
The authors thank Akiteru Toda for excellent technical assistance.
Ethical Considerations
Not applicable. This is a single-patient case report with no experimental intervention beyond standard care.
Consent to Participate
Written informed consent was obtained from the patient for clinical evaluation and follow-up.
Consent for Publication
Written informed consent for publication of clinical data and images was obtained from the patient.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statements
Not applicable. No data sets were generated or analyzed for this case report.