
Abstract
Purpose:
The aim of this study was to evaluate the feasibility and mid-term results of combining polytetrafluoroethylene (PTFE)-based iliac limbs, having a short dilator tip, with a polyester (Dacron)-based bifurcated component during a fenestrated endovascular aortic repair (FEVAR).
Materials and Methods:
All patients who underwent a FEVAR procedure in a single tertiary center were screened for inclusion in the study. Data were collected retrospectively and all imaging was reviewed for the study. The criterion for inclusion in the study was the implantation of a PTFE-based iliac limb endoprosthesis at the contralateral side of the polyester-based bifurcated component during a FEVAR procedure landing in a native common iliac artery. The primary study endpoints were technical success, adverse events, and reinterventions related to limbs, migration between contralateral iliac limbs and bifurcated components, type Ib and IIIa endoleaks, and iliac limb patency.
Results:
A total of 30 patients with a median age of 77 (70, 79) years, who underwent FEVAR procedures from June 2020 to July 2023, were included in the study. The total number of target vessels was 116, and the majority (N = 24) of patients received 4 fenestrations. Technical success was achieved for the iliac limb in all patients, and for the FEVAR, it was obtained in 29 cases (97%). Median follow-up was 24 (12, 30) months. There were no clinical limb-related adverse events or reinterventions. At the end of the follow-up period, all limbs remained patent. The median absolute and percentual change in overlap between the limb and the cuff of the bifurcated endograft was of −0.1 mm (−0.8, 1.1) and −0.4% (−2.7, 4), respectively. The estimated primary, secondary clinical success of the FEVAR, and survival rates (± standard error) at 2 years were 86 ±7%, 90±6, and 83±7%, respectively.
Conclusions:
The present study demonstrated promising mid-term outcomes, with the absence of limb-related adverse events, reinterventions, and any significant change in the overlap of PTFE iliac limbs combined with polyester bifurcated device during FEVAR. Further validation in a larger cohort as well as comparative analysis between different component combinations are needed to confirm the findings of the present study.
Clinical Impact
This study underscores the feasibility and excellent mid-term clinical outcomes of combining PTFE-based iliac limbs with a short dilator tip and a polyester-based bifurcated component during fenestrated endovascular aortic repair. The absence of significant migration and adverse effects related to the iliac limbs, along with the lack of target vessel occlusions, suggests a potential advantage of using a delivery system that avoids crossing the fenestrations, thereby enhancing technical success and ensuring stable and durable results over time.
Keywords
Introduction
With the progression of endovascular technology, fenestrated endovascular aortic aneurysm repair (FEVAR) has become the standard of care for high-risk patients with complex abdominal and thoraco-abdominal aortic aneurysms (TAAAs) with suitable anatomy.1,2 The most commonly used fenestrated endograft (Cook Medical, Bloomington, IN, USA) consists of full-thickness polyester-based components with a modular design: a proximal tubular part with fenestrations for the visceral arteries, and a distal bifurcated part, which is then extended contralaterally or bilaterally to the iliac limbs. During insertion and deployment of the bifurcated graft and limbs, the tip of the long delivery systems can potentially come in conflict with the bridging stent-grafts of the target vessels, leading to compression or even complete occlusion. A novel, “no-cross” technique was recently described to overcome this issue.3,4 In summary, distal bifurcated devices with short-tipped delivery systems were combined with Polytetrafluoroethylene (PTFE)-based iliac limbs (W.L. Gore & Associates Inc, Newark, DE, USA). However, the combination of the Zenith bifurcated FEVAR component (Cook Medical, Bloomington, IN, USA) with PTFE-based iliac limbs has not been widely studied. The aim of this study is to evaluate their efficacy during follow-up and if there are any determinants of the outcome.
Materials and Methods
Study Design
All patients who underwent a FEVAR procedure in a single tertiary center were screened for inclusion in the study. Clinical data were collected and analyzed retrospectively from medical records. The study was approved by the ethical committee and written informed consent was waived given the retrospective design of the study. The criterion for inclusion in the study was the implantation of a Gore iliac limb endoprosthesis (W.L. Gore & Associates Inc, Newark, DE, USA) at the contralateral side of a polyester-based bifurcated component during the FEVAR procedure, landing in the native common iliac artery. Exclusion criteria were the use of a bifurcated component other than the planned, from the FEVAR manufacturer (Cook Medical, Bloomington, IN, USA), history of previous EVAR as well as the use of an iliac branch device at the contralateral side. All cases were elective and treated according to current international guidelines. 5 Lastly, the study was conducted in accordance with the Declaration of Helsinki and complied with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cohort studies. 6
Outcomes and Definitions
The main focus of the study was the outcomes related to the contralateral limbs. Hence, the primary endpoints were technical success of the procedure as well as any adverse events and reinterventions related to limbs (kink, stenosis, occlusion), migration between contralateral limb and bifurcated component, type Ib and IIIa endoleaks, and limb patency. The secondary endpoints were related to the FEVAR procedure: clinical success, bridging stent compression, target vessel patency, overall mortality (both early and late deaths), aneurysm-related mortality, perioperative major adverse events, other types of early and late endoleaks, and secondary interventions. Severe vascular access complications were defined as access-site events causing death, major bleeding, ischemia, neurological impairment, or requiring surgical/endovascular repair; minor hematomas were excluded. The outcomes were defined as early or late if they occurred ≤ 30 or > 30 days after the FEVAR procedure, respectively. Definitions were assumed according to the reporting standards for endovascular aortic repair. 7
Imaging
All patients were assessed pre-operatively with multi-slice detector computed tomography angiography (CTA). Patient CT follow-up consisted of CTAs with an additional late phase (standard protocol with noncontrast and arterial and delayed series) at 1 month and yearly thereafter. Contrast-enhanced duplex ultrasound was undertaken to determine the origin of any unclear endoleak in the CTA. For this study, CTAs at 3 time points were included: preoperative, first, and most recent postoperative CTA.
Pre-Operative Measurements
The measurements were undertaken in a 3D workstation (Aquarius, iNtuition Version 4.4.13.P5, TeraRecon Inc, Foster City, CA, USA) by the same operator. The pre-operative anatomic characteristics were measured using a semi-automatic center lumen line, where manual adjustments were made to the centerline whenever needed. The landing zone was defined as the maximum diameter of the distal 2 cm of the common iliac artery. The iliac tortuosity index was measured on the dedicated software’s function (Figure 1) as the ratio of the distance between the iliac bifurcation and the common femoral artery along the centerline and the straight path on 3D (shortest distance), as previously defined. 8
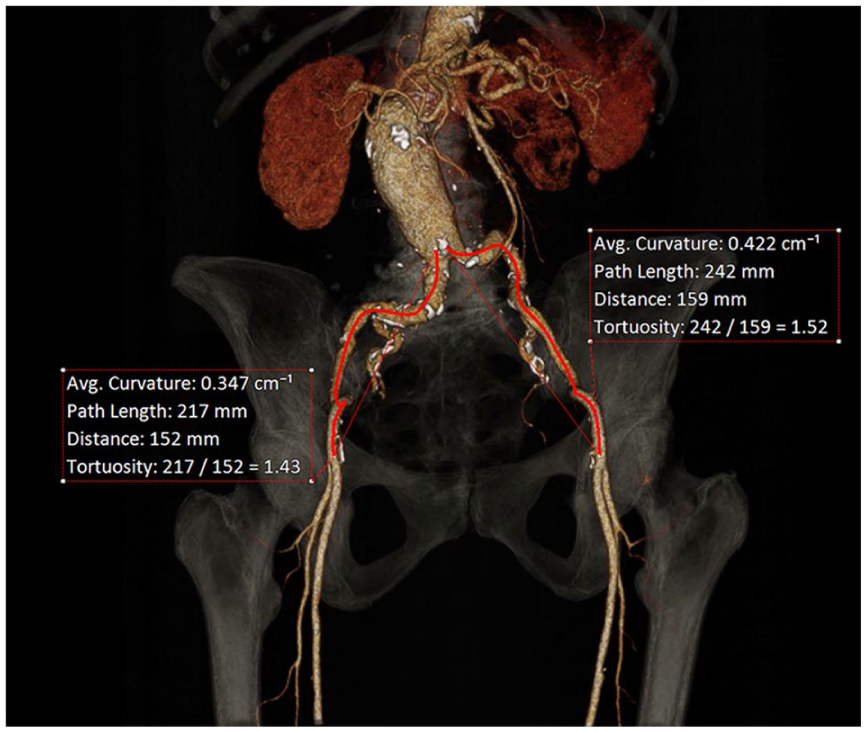
Calculation of iliac tortuosity indexes. The ratio is calculated by dividing the artery length along the centerline of flow by the straight length (shortest distance) between the iliac bifurcation and the common femoral artery. 8
Postoperative Follow-Up Imaging
The first and most recent postoperative CTAs were evaluated in the same 3D workstation with the main focus on the Gore iliac limb. The study involved assessment for the presence of limb kinks, stenosis (defined as more than 50% reduction of lumen, as seen in multiplanar reconstruction perpendicular to the long axis of the vessel) as well as any difference in the angulation of the limb (more than 30°) when comparing the first and last CTAs. Additionally, the overlap between the iliac limb and the bifurcated complement was also assessed on all CTAs to determine any migration between the components including impending, or tendency for, separation. The overlap difference was calculated by subtracting the overlap in the first postoperative CTA from that of the last CTA (Figure 2). Similarly, the percentual change was calculated as follows: Overlap difference/Overlap in first CTA × 100. Migration was defined as cranial or caudal change in the overlap of components of more than 10 mm, according to the reporting standards. 7
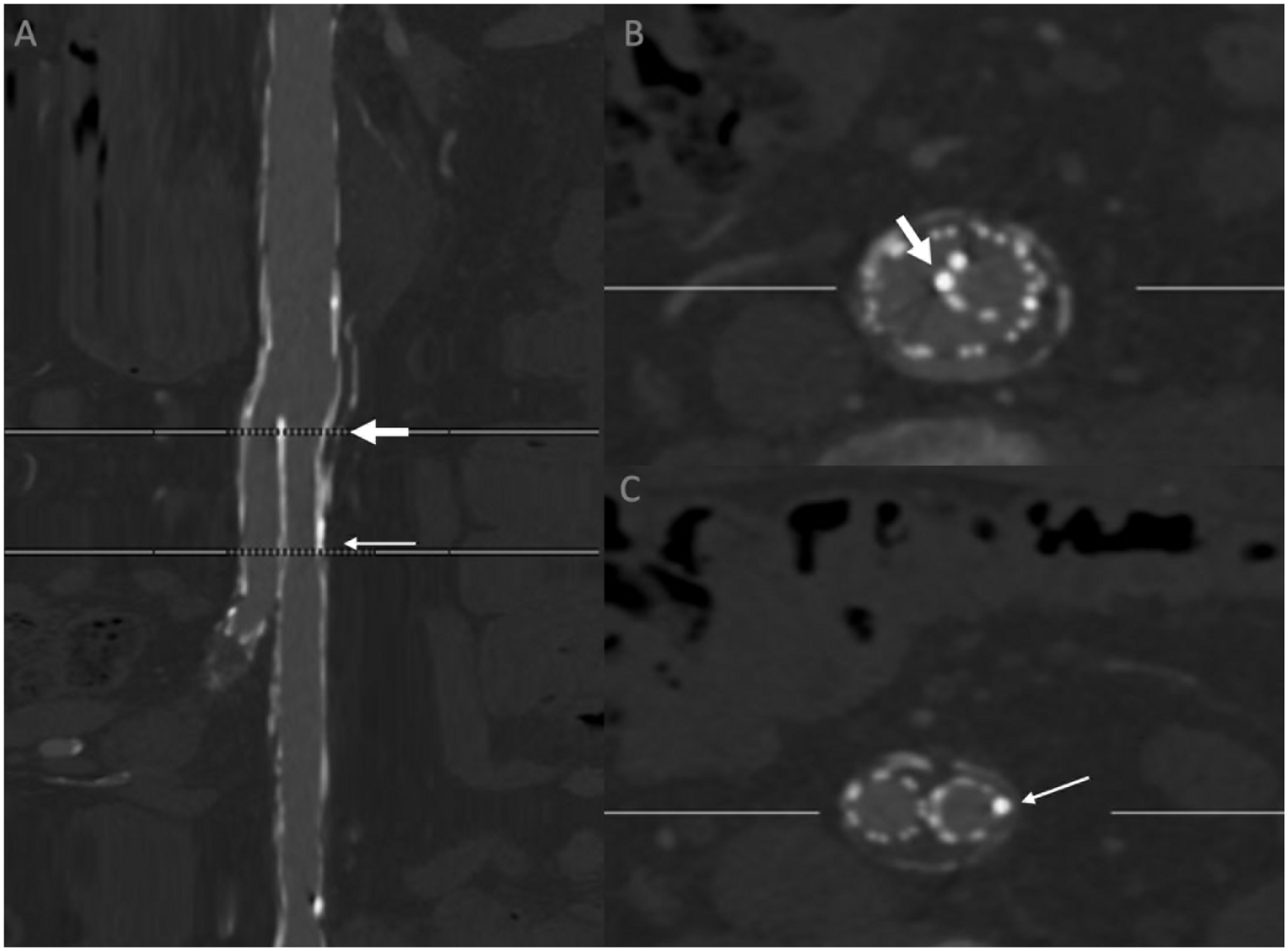
Illustration of how the length of the overlap between the contralateral cuff of the bifurcated graft and the contralateral Gore limb was calculated. The markers on the grafts were measured. (A) Stretched view of the aorta (on a center lumen line). The thick white arrow: leading marker of the contralateral Gore limb. Thin white arrow: distal marker of the contralateral cuff of the bifurcated graft. (B) Orthogonal reconstruction at the level of the leading marker of the Gore limb (thick white arrow), where the flow divider marker of the bifurcated graft is also visible. (B) Orthogonal reconstruction at the level of the distal marker of the contralateral cuff of the bifurcated graft (thin white arrow).
Endografts and Procedure
Fenestrated custom-made devices were designed by the graft manufacturer (Cook Medical, Bloomington, IN, USA) along with the vascular surgeon on a dedicated 3D workstation using the pre-operative CTA. The proximal tubular component included fenestrations for the renovisceral arteries; renal arteries were preloaded. The bifurcated component was customized with or without an inverted limb (Cook Medical, Bloomington, IN, USA) and loaded into a delivery system with a shortened dilator tip (40 mm) as previously described to avoid crossing of the renal fenestrations.3,4 Barbs were freely included in the bifurcated components including all with an inverted limb configuration. The diameter of the gate of the contralateral limb was 11 or 12 mm. The choice of Gore contralateral iliac limb endoprostheses was based on the length and diameter of the common iliac artery, according to the manufacturer’s recommendations for this device regarding the distal sealing zone. During deployment, the proximal marker at the leading end of the Gore limb was aligned with the flow divider of the Cook bifurcated device (Figure 3).
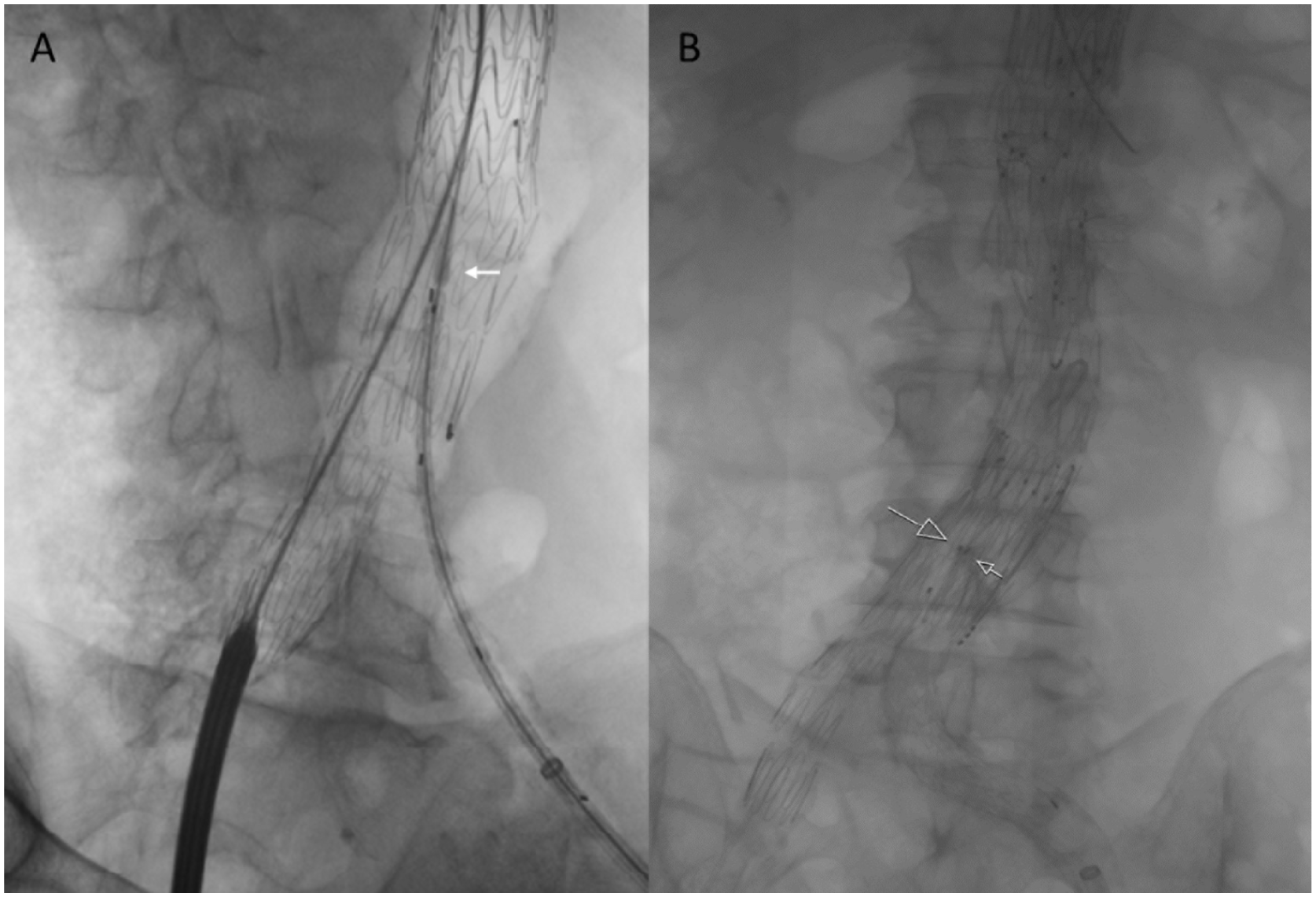
Intraoperative fluoroscopy image of patients who received Zenith FEVAR tubular and bifurcated components on the right side and a Gore limb as the contralateral iliac extension on the left side. (A) Before the deployment of the contralateral Gore limb. The leading marker of the limb is just proximal to the flow divider marker of the bifurcated graft, allowing the tip of the dilator to be well away from the fenestrations (white arrow). (B) After deployment of the contralateral Gore limb. This patient received a bifurcated graft with an inverted limb configuration with barbs proximally. The leading marker of the Gore limb (big arrow) was aligned with the flow divider marker on the bifurcated device (small arrow).
All procedures were performed by the same experienced team of aortic vascular surgeons in a hybrid operating room under general anesthesia using intraoperative fusion guidance, carbon dioxide, as well as iodine angiography. Overlap areas between components were always balloon dilated with semi-compliant balloons. Moreover, evaluation for compression of the limbs and bridging stents was performed with cone-beam computed tomography (CBCT) after the completion of angiography for all procedures. If any significant stenoses were observed after kissing semi-compliant ballooning, they were corrected with kissing balloon expandable stents.
Statistical Analysis
Continuous variables are expressed as median with interquartile range. Categorical variables are presented as absolute numbers and percentages. Mann–Whitney U test was used for group comparisons. Time-dependent outcomes were estimated using lifetables according to Kaplan–Meier and are reported with standard errors. The analysis was performed using IBM® SPSS® statistics software (version 29.0.2.0; IBM Corporation, Armonk, NY, USA).
Results
A total of 30 out of 72 patients with a median age of 77 (70, 79) years, who underwent FEVAR procedures from June 2020 to July 2023, were included in the study (Figure 4). Gore limbs were utilized on the contralateral side in 56 patients in the above-mentioned time interval. However, 16 patients had received a Gore bifurcated device and were excluded. Similarly, 4 patients had a previous EVAR and 6 had an IBD as the landing zone of the contralateral iliac limb, so they were also excluded. Patient characteristics and risk factors can be found in Table 1. All included patients were treated for a juxta-renal aneurysm with a median diameter of 59 (56, 62) mm, and all hypogastric arteries were patent bilaterally. The iliac artery anatomic characteristics were similar on both sides and are summarized in Table 2. Iliac tortuosity indices were 1.28 (1.19, 1.36) and 1.27 (1.21, 1.34), on the right and left side, respectively, whereas the median sealing zone diameters were 14 mm (12, 17) on both sides.
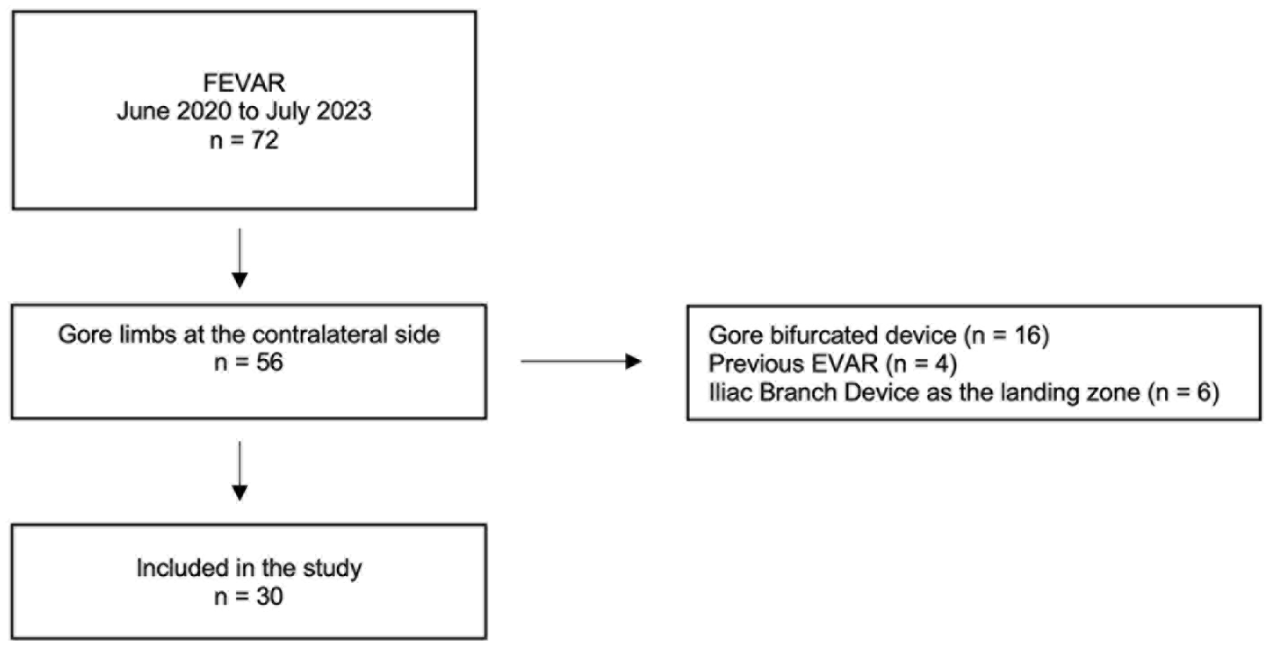
Flowchart of patient inclusion in the study.
Baseline Characteristics of Included Patients.1
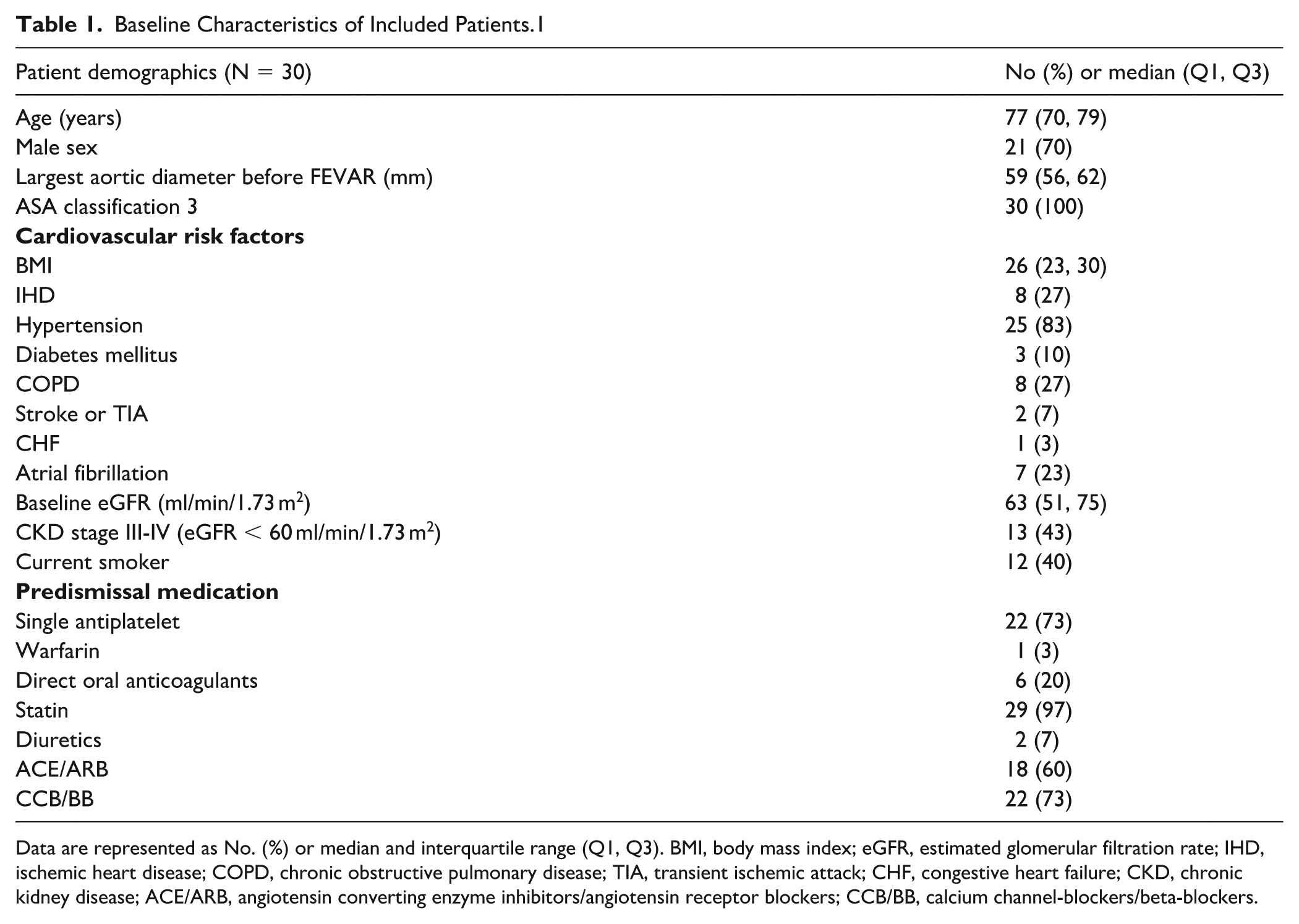
Data are represented as No. (%) or median and interquartile range (Q1, Q3). BMI, body mass index; eGFR, estimated glomerular filtration rate; IHD, ischemic heart disease; COPD, chronic obstructive pulmonary disease; TIA, transient ischemic attack; CHF, congestive heart failure; CKD, chronic kidney disease; ACE/ARB, angiotensin converting enzyme inhibitors/angiotensin receptor blockers; CCB/BB, calcium channel-blockers/beta-blockers.
Preoperative Anatomic Characteristics of Included Patients (N = 30).
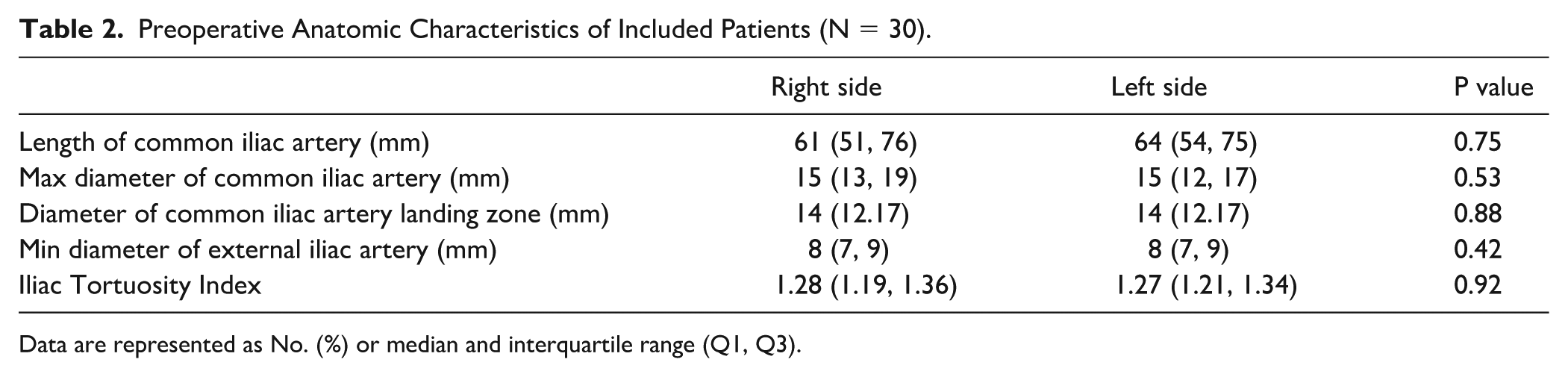
Data are represented as No. (%) or median and interquartile range (Q1, Q3).
Procedure Details
The total number of target vessels was 116 and most (N = 24) patients received 4 fenestrations (Supplementary Table 1). In the majority of procedures (N = 27), the contralateral limb was inserted on the left side (Figure 5) and had a median distal diameter of 16 (15, 19) mm, which was not different from the ipsilateral (16 [16, 20] mm, p = 0.14). Oversizing was discreetly lower on the contralateral compared to the ipsilateral iliac limb (16 [12, 29] % vs 18 [9, 27] %, p = 0.64). The median distance between the lowest stent (which was in the lowest renal artery in all included cases) to the flow divider was 84.3 (73.2-101.8) mm. In 9 cases, there was extension of the iliac limb, but only 2 of these were on the contralateral side, and in both, another Gore limb was used. The first patient received an extension, as one iliac limb was not sufficient to land in the common iliac artery. In the other case, the limb ended up too proximal due to a very tortuous iliac artery (preoperative tortuosity index of 1.76). Regarding extensions at the ipsilateral iliac limb, 8 were Gore limbs and 1 was Endurant (Medtronic, Minneapolis, and Minnesota). Kissing stenting at the aortic bifurcation was undertaken primarily in 3 (10%) patients as an adjunct procedure and in another case after the CBCT revealed compression of the ipsilateral limb, which had not received any extension. No infoldings of the contralateral Gore limbs could be seen in the overlap segment in the CBCT. Technical success was achieved for the iliac limb in all patients, whereas for the FEVAR, it was obtained in 29 cases (97%). The reason for the technical failure of the FEVAR was a persistent small endoleak that was later diagnosed as type Ic from the left renal stent. Two patients with ultimately successful FEVAR required intraoperative adjunctive renal artery bridging stent re-dilatation after the CBCT revealed inadequate flaring, most likely following compression by one of the distal components. Both cases were corrected successfully with balloon angioplasty, with no target-vessel occlusions at follow-up.
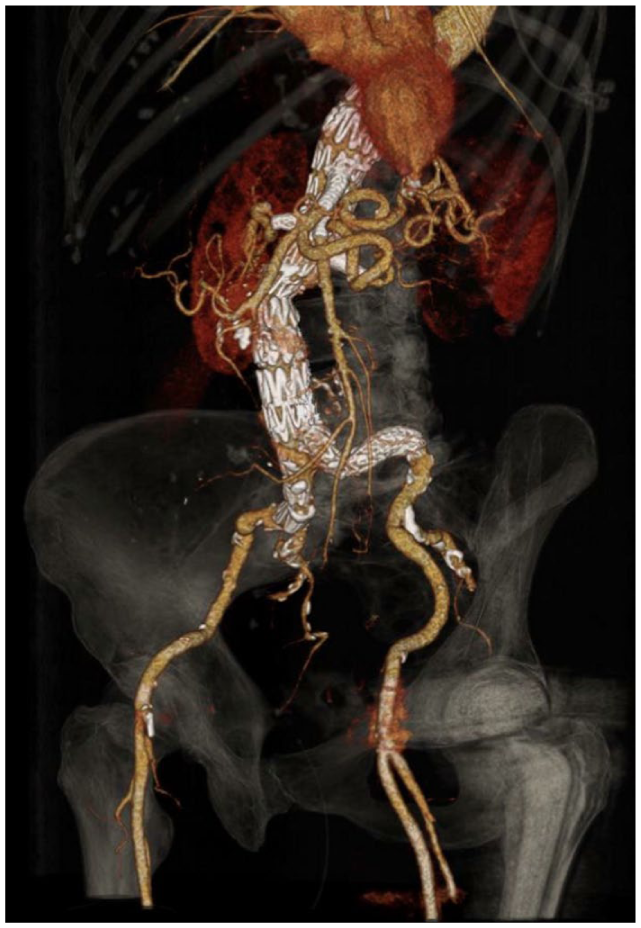
Three-dimensional reconstruction of a postoperative computed tomography angiography (same patient in Figure 1) after FEVAR, demonstrating the configuration and patency of the iliac limbs (Gore iliac limb on the left side) and target renovisceral vessels.
Early Postoperative Results
Three patients died in the early postoperative period. One case was due to bowel ischemia following a superior mesenteric artery dissection. The remaining 2 patients had undergone long procedures with lower limb fasciotomies. One of these developed multiorgan failure and died 2 days postoperatively, while the other suffered extensive bowel ischemia. The iliac limbs were patent on the early postoperative CTA examinations. All iliac limbs remained patent and required no early reinterventions. Early reinterventions were nevertheless needed for other reasons in 6 patients. In one case, a distal extension of a renal stent was performed for residual dissection with rising creatinine levels. Four cases needed reintervention due to vascular access issues, one of which also necessitated a laparotomy for bowel ischemia. Lastly, another patient also underwent laparotomy for bowel ischemia. Both bowel ischemia patients had patent fenestrations. Early results are summarized in Table 3.
Early Results.
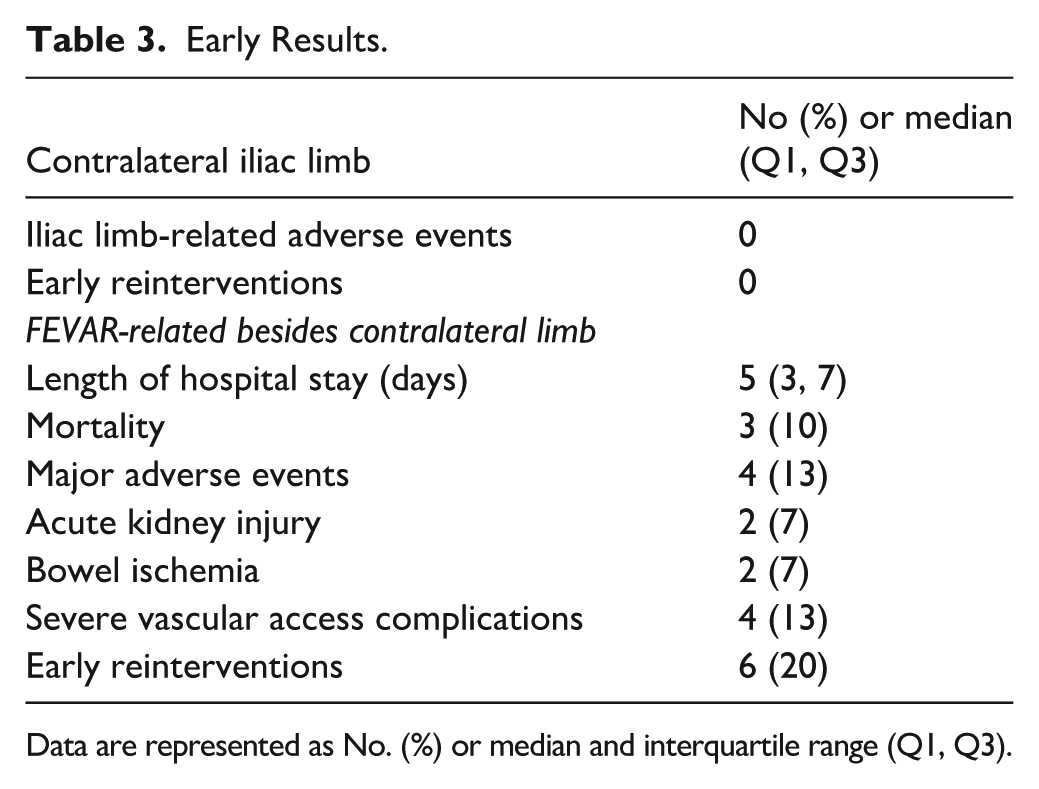
Data are represented as No. (%) or median and interquartile range (Q1, Q3).
Follow-Up Results
At a median follow-up of 24 (12, 30) months, all limbs remained patent, with no adverse configurational changes such as kinks or stenoses. The initial overlap between the bifurcated and contralateral Gore limb on the first postoperative CTA was 27.8 (25.7, 31.3) mm. The median absolute and percentual change in the overlap between the limb and the cuff of the bifurcated graft was −0.1 mm (−0.8, 1.1) and −0.4% (−2.7, 4), respectively. No type Ib or III endoleaks were observed and no patients presented with lower limb symptoms attributable to the iliac limbs or required iliac limb reinterventions. The early results, in regard to iliac limbs, are summarized in Table 3.
All fenestrations remained patent throughout the follow-up period. The estimated primary clinical success rate at 2 years was 86 ± 7%, which was improved to a secondary rate of 90 ± 6% with the help of 4 late reinterventions, all unrelated to the contralateral limb. Estimated survival at 2 years was 83 ± 7% with 2 deaths beyond 30 days, both nonaortic related (Supplementary Figures 5 and 6).
Discussion
The present study confirms the clinical feasibility of the combination of a PTFE-nitinol-based iliac limb with a polyester-stainless steel endograft during FEVAR. More importantly, it shows the mid-term stability of this combination, both clinically and in CTA image assessment.
The reason motivating the use of this combination was the short dilator tip of this specific iliac limb delivery system. This can theoretically preclude the crossing of the fenestrations and thereby potentially reduce the number of intraoperative target vessel-related adverse events. However, to really reach a complete no-cross design, a short dilator introducer tip needs to be used also on the distal bifurcated aortic endograft. This design has been previously demonstrated to considerably reduce the occurrence of adverse events related to the fenestration bridging stents.3,4,9 This study reinforces those results since renal stent compression was detected with CBCT in 2 cases and corrected successfully intraoperatively with balloon angioplasty. Although the short dilator tip reduces the likelihood of bridging stent compression, it does not abolish the risk entirely. The most likely mechanism for this adverse event is the protrusion of the balloon into the aortic lumen during flaring. This can at times come in close proximity of the other renal artery, which may cause a compression. The recently introduced stent where the balloon does the flaring during the same inflation can potentially avoid this issue. 10
The use of an iliac limb manufactured to be used with another graft may condition the stability of the overlap segment, particularly regarding the overlap segment, during follow-up. An experimental assessment in a model showed that the pullout forces of an Excluder limb from a Zenith infrarenal endograft were lower than those for standard Zenith limbs that had a proximal diameter of 12 mm. 11 On the contrary, the clinical outcomes for these hybrid endografts (combination of different manufacturers) have only been studied in infrarenal EVAR. Even if the results were promising, 12 the follow-up was only 19.4 months, which may be too short for clinical events to occur. Our results reinforce the good clinical outcome of the PTFE-based iliac limbs with a median follow-up of 2 years. More importantly, and assuming that an eventual migration or separation would be preceded by a progressive decrease in the overlap, our results are also reassuring since they show that overlap assessed by CTA barely changes during the follow-up. After deployment, the contralateral iliac limb might sometimes protrude above the flow divider, or even be placed a few millimeters distally. During the evaluation for possible migration, the absolute overlap in mm was measured using the graft and limb markers. A tendency toward the separation of the components would lead to only negative values. Theoretically, even an upward movement overtime could happen. Our results could not confirm this, and the median change of much less than 1 mm is well within the expected measurement variation. Importantly, the change does not seem to have any clinical consequence with an absence of endoleaks and reinterventions in the iliac limbs during follow-up. Another theoretical concern of the combination of the grafts would be the excessive oversizing in the overlap segment. The diameters of 11 or 12 mm of the contralateral cuff of the bifurcated graft are smaller than the minimum of 13.5 mm suggested by the PTFE-based limb manufacturer. This could potentially have led to the infolding or development of crimps in the overlapping segment with a consequent risk of type III endoleak. None of these could be seen in the repeated intra- and postoperative 3D radiological assessment. Furthermore, the clinical success in the exclusion of the aneurysm in the vast majority of the patients suggests the absence of any of the above-mentioned concerns.
As discussed in detail previously,3,4 the afore-mentioned “no-cross” concept may require the customization of the distal bifurcated graft with the use of an inverted limb besides the shortening of the tip of the dilator of the delivery system. The use of these inverted limbs has been shown to be associated with good clinical results,13,14 but has not been tested in combination with the PTFE-based limbs. Our results show that the design of the bifurcated component, with the inversion of the limb, does not seem to impact the outcome of using PTFE-based iliac limbs. An alternative strategy to reduce the risk of bridging stent compression by the interaction of the distal components delivery system is the use of integrated/unibody constructs. In these circumstances, the fenestrations are incorporated in a bifurcated device that only needs to be extended with iliac limbs, thereby minimizing the number and duration of large delivery systems traversing the fenestrated segment. There are no reasons to expect that the combination of different graft materials would behave differently when the FEVAR consists of a unimodular device. Preliminary reports suggest satisfying results of the unimodular repair, when compared with the more traditional modular design.15,16 Dorenberg et al compared a standard modular FEVAR setup (fenestrated tube and separate bifurcated body) with an integrated fenestrated bifurcated design in a single-center retrospective series (12 vs 13 patients). Technical success was 100% in both groups, but target vessel stent deformation occurred only in the modular group (4 cases), and none occurred with the combined design. 17 These results need to be confirmed in the long-term since the integration of the fenestration on the same device where the flow divider is, will lead to any migrations caused by forces acting at the flow divider will be directly transmitted to the fenestrations, which may compromise their patency.
One issue that still needs further study is the potential impact of the use of different iliac limbs on the 2 sides. This may potentially affect the columnar support provided to the bifurcated device, which can also be influenced by the different lengths available of the iliac limbs. The PTFE-based iliac limb is longer than the original polyester-based limb since it was originally designed to be used with an endograft with a higher bifurcation, which in turn could affect the long-term stability of the repair. Our study is not designed to answer this question.
One surprising finding was the high perioperative mortality. This does not seem to have been directly related to the use of the limb, but an indirect consequence of the selection of patients who received a PTFE iliac limb cannot be excluded.
There are some limitations to this study that need to be acknowledged. The retrospective cohort design reporting the first results of a technique limit the number of patients and consequently the statistical power of the analysis, and has the potential of introducing some selection bias. Moreover, it is also unclear if some inclusion bias was introduced by the anatomical suitability of this particular combination of grafts. Our study focused on the contralateral limb, as this is a mandatory component of the FEVAR procedure and the site at which the stability of the hybrid combination is most relevant to assess. Ipsilateral limb extensions were not routinely required and, when used, were placed distally rather than at the level of the flow divider. For this reason, overlap measurements on the ipsilateral side were not applicable in our cohort. Finally, it is uncertain if the definition of the intra- and postoperative imaging 3D methods used (cone-beam CT and CTA) have sufficient resolution or freedom from metal artifacts from the graft markers for the identification of the issues such as small folds or minimal migration in the overlap segment.
Conclusion
This study shows the feasibility and mid-term sustainability of the clinical and radiological results of combining PTFE-based iliac limbs with short dilator tips with a polyester-based bifurcated device during FEVAR. Further studies are needed to assess the long-term outcomes in larger cohorts.
Supplemental Material
sj-docx-3-jet-10.1177_15266028251409061 – Supplemental material for Mid-Term Outcomes of PTFE-Based Contralateral Iliac Limbs in Polyester-Based Fenestrated Bifurcated Endografts
Supplemental material, sj-docx-3-jet-10.1177_15266028251409061 for Mid-Term Outcomes of PTFE-Based Contralateral Iliac Limbs in Polyester-Based Fenestrated Bifurcated Endografts by Kalliopi-Maria Tasopoulou, Angelos Karelis, Wendela Jirström, Yasir Mohammed, Márton Berczeli, Umar Sadat, Björn Sonesson and Nuno V. Dias in Journal of Endovascular Therapy
Supplemental Material
sj-tif-1-jet-10.1177_15266028251409061 – Supplemental material for Mid-Term Outcomes of PTFE-Based Contralateral Iliac Limbs in Polyester-Based Fenestrated Bifurcated Endografts
Supplemental material, sj-tif-1-jet-10.1177_15266028251409061 for Mid-Term Outcomes of PTFE-Based Contralateral Iliac Limbs in Polyester-Based Fenestrated Bifurcated Endografts by Kalliopi-Maria Tasopoulou, Angelos Karelis, Wendela Jirström, Yasir Mohammed, Márton Berczeli, Umar Sadat, Björn Sonesson and Nuno V. Dias in Journal of Endovascular Therapy
Supplemental Material
sj-tif-2-jet-10.1177_15266028251409061 – Supplemental material for Mid-Term Outcomes of PTFE-Based Contralateral Iliac Limbs in Polyester-Based Fenestrated Bifurcated Endografts
Supplemental material, sj-tif-2-jet-10.1177_15266028251409061 for Mid-Term Outcomes of PTFE-Based Contralateral Iliac Limbs in Polyester-Based Fenestrated Bifurcated Endografts by Kalliopi-Maria Tasopoulou, Angelos Karelis, Wendela Jirström, Yasir Mohammed, Márton Berczeli, Umar Sadat, Björn Sonesson and Nuno V. Dias in Journal of Endovascular Therapy
Footnotes
ORCID iDs
Ethical Considerations
The study was approved by the ethical committee, and written informed consent was waivered given the retrospective design of the study.
Consent to Participate
Not applicable
Consent for Publication
Not applicable
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Skåne University Hospital (SUS) Research Grants, the Governmental funding of clinical research within the National Health Services (ALF), Hulda Almroth Foundation, and the Bor Maritza Foundation.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Nuno V. Dias is a consultant, holds IP, and has received research support from COOK Medical Inc and has been a speaker and received research support from Gore Medical. Other authors declare no conflict of interest.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.