
Abstract
Objective:
To investigate the operational efficiency, safety, and postoperative recovery differences between the transradial approach (TRA) and the transfemoral approach (TFA) in performing digital subtraction angiography (DSA) in patients with different aortic arch types. Additionally, to compare the applicability of Simmon 1 and Simmon 2 catheters in complex aortic arch configurations.
Methods:
This single-center, prospective, randomized controlled trial included 114 patients with cerebrovascular disease scheduled for DSA. Preoperative aortic arch computed tomography angiography (CTA) was performed on all patients to classify the aortic arch into type I, type II, or type III, with 38 patients in each group. Each arch type was then randomly assigned in a 1:1 ratio to either the TRA (n=57) or TFA (n=57) group. The comparison between the 2 groups included puncture time, fluoroscopy time, contrast agent usage, postoperative hemostasis time, immobilization time, and the incidence of puncture-related complications for each aortic arch type. For patients with type III aortic arch in the TRA group, a further random allocation was made to use either the Simmon 1 or Simmon 2 catheter to assess differences in performance for complex arch types.
Results:
Baseline characteristics between the 2 groups were similar. Compared with the TFA group, the TRA group had a longer puncture time (29.08±1.53 min vs 20.11±1.65 min, p<0.001), but shorter fluoroscopy time (4.52 min vs 5.45 min, p<0.001), and significantly reduced postoperative hemostasis and immobilization times (both p<0.001). The incidence of puncture-related complications was significantly lower in the TRA group (1.75% vs 19.30%, p=0.006). In all aortic arch type subgroups, TRA demonstrated superior postoperative recovery and safety compared to TFA, with the most pronounced advantage observed in patients with type III aortic arch. Furthermore, in type III aortic arch patients within the TRA group, the use of Simmon 2 catheter significantly reduced contrast agent usage (43.73±6.20 mL vs 53.36±5.93 mL, p=0.002), shortened hemostasis and immobilization times (p<0.001), but there were no significant differences in puncture and fluoroscopy times.
Conclusion:
TRA demonstrated excellent safety and postoperative recovery advantages across different aortic arch types, with a particular adaptive benefit in type III aortic arch patients. The Simmon 2 catheter performed better in TRA-treated type III arch patients, supporting individualized approach and catheter selection based on preoperative aortic arch morphology. This strategy may improve procedural efficiency, reduce complications, and optimize patient outcomes. Further validation in larger, multicenter studies is recommended.
Clinical Impact
This study validates the TRA as a safer, more efficient alternative to transfemoral access for cerebral angiography, regardless of aortic arch complexity. It challenges the hesitation to use TRA in Type III arches by demonstrating significantly reduced complications and faster recovery. A key innovation is the stratified evaluation of catheters, identifying the Simmon 2 catheter as superior for Type III arches to optimize contrast usage and hemostasis. For clinicians, this supports shifting toward individualized, anatomy-based strategies, encouraging the use of TRA with specific catheter selection to improve safety and patient outcomes in neurointerventional procedures.
Keywords
Introduction
Cerebrovascular disease is one of the leading causes of mortality and disability worldwide, accounting for approximately 16% of all global deaths. 1 Timely and accurate imaging assessment of cerebrovascular lesions is critical for developing appropriate treatment strategies and predicting patient outcomes. Among various imaging modalities, digital subtraction angiography (DSA) is considered the gold standard for evaluating cerebrovascular abnormalities due to its excellent spatial resolution, dynamic imaging capabilities, and comprehensive visualization of vascular anatomy.2,3
However, as an invasive procedure, DSA places higher demands on the selection of vascular access routes, particularly in patients with complex anatomical variations of the aortic arch. 4 To systematically evaluate the impact of aortic arch variations on endovascular procedures, clinical classification typically divides the aortic arch into 3 types based on the vertical distance from the origin of the brachiocephalic trunk to the apex of the arch. In a type I arch, the brachiocephalic artery originates at or below the apex of the arch, forming a small angle that allows the catheter to easily enter the cervical vasculature. In a type II arch, the origin is slightly above the apex, creating a more curved vascular path. A type III arch is characterized by a markedly higher origin of the brachiocephalic artery, with a steep take-off angle and elongated, tortuous vascular pathways, significantly increasing the difficulty of catheter shaping and access to target vessels. 5 In addition to these anatomical classifications, the aortic arch frequently exhibits varying degrees of atherosclerotic changes, such as thrombotic or calcific deposition, and in some cases, dissection flaps or penetrating aortic ulcers. 6 These pathological alterations may further increase the technical difficulty of catheter passage and shaping, as well as the risk associated with the procedure.7,8
Currently, the 2 most commonly used access routes in clinical practice are the TFA and the TRA. TFA is a mature and well-established technique, but it often requires prolonged postoperative immobilization and is associated with a higher risk of access-site complications.3,9 In recent years, TRA has gained widespread application in the field of neurointervention due to its lower incidence of access-related complications, faster postoperative recovery, and higher patient satisfaction. 10 Nevertheless, in patients with a type III aortic arch, TRA also presents significant technical challenges, such as catheter slippage, failure of catheter shaping, and an increased risk of access conversion. 11 In addition to access selection, the structure and type of catheter are also critical to procedural success. Due to their unique looped configuration and pre-shaped design, Simmon catheters have become one of the most commonly used catheter types for carotid angiography via the TRA, particularly in patients with elongated and steeply angled vascular anatomy.12,13 Among them, the Simmon 2 catheter, compared to the Simmon 1, features a larger secondary curve and a longer supporting segment, theoretically providing greater stability and improved shaping efficiency in type III arches. 14 However, comparative studies evaluating the effectiveness of TRA versus TFA across different aortic arch types are currently lacking, and prospective research comparing Simmon 1 and Simmon 2 catheters in type III arches is also insufficient. As a result, catheter selection in clinical practice is often based on operator experience, limiting the standardization and evidence-based refinement of procedural strategies.
Based on the above background, this study aims to conduct a prospective, randomized controlled trial to: (1) systematically compare the technical efficiency, postoperative recovery, and complication risks of TRA versus TFA in patients with type I, II, and III aortic arches undergoing DSA; and (2) further evaluate the clinical performance of Simmon 1 versus Simmon 2 catheters in TRA-treated patients with a type III arch. Through precise classification of aortic arch types and optimization of catheter selection strategies, this study seeks to provide robust clinical evidence for access route decision-making in cerebral angiography involving complex vascular anatomy.
Materials and Methods
Study Design and Ethics
This single-center, prospective, randomized controlled trial was conducted from June 2024 to April 2025 at hospital, a university-affiliated hospital. The study protocol was approved by the hospital’s Ethics Committee, and written informed consent was obtained from all participants prior to enrollment.
Participants
Inclusion criteria:
Age ≥ 18 years and scheduled for cerebral DSA via either transradial or transfemoral access for the diagnosis or evaluation of cerebrovascular diseases, primarily including carotid artery stenosis, intracranial arterial stenosis, and subclavian artery stenosis, with the purpose of identifying the lesion location, type, and severity; 15
Underwent preoperative CTA of the cervical vessels and aortic arch, with confirmed arch classification; 5
Voluntarily agreed to participate and signed informed consent.
Exclusion criteria:
Known severe allergy to iodine-based contrast agents;
Severe coagulopathy;
Contraindications at the intended access site, such as weak radial pulse, positive Allen’s test, poor femoral artery pulsation, or local infection;
Severe cardiac, pulmonary, or renal dysfunction;
Patients with malignant tumors and an expected survival of less than 6 months.
Group Allocation and Surgical Protocol
A total of 114 eligible patients were enrolled in the study. All patients underwent preoperative aortic arch CTA to determine the arch classification, including 38 cases each of type I, type II, and type III arches. After enrollment, patients scheduled for DSA were randomized in a 1:1 ratio into either the TRA group or the TFA group using a computer-generated randomization sequence. Randomization was performed by an independent investigator after obtaining informed consent, and the group allocation was disclosed to the operator using sealed envelopes. Since randomization was stratified by arch type, the distribution of aortic arch types was balanced between the 2 groups, with each group comprising 19 patients with type I, 19 with type II, and 19 with type III arches.
In terms of catheter selection, a single-curve catheter was used uniformly in the TFA group. For patients in the TRA group who were intraoperatively confirmed to have a type III arch, a second randomization was performed to assign either a Simmon 1 or Simmon 2 catheter in a 1:1 ratio. This included 10 patients assigned to Simmon 1 and 9 to Simmon 2. This randomization was also conducted using a computer-generated sequence, implemented by the study coordinator immediately after the arch type was confirmed. For patients with type I and type II arches, Simmon 1 catheters were used uniformly.
To minimize bias, all procedures were performed by neurologists specialized in interventional neurology, each holding official interventional certification and with experience in more than 100 TRA and TFA cerebral angiography cases. Operators were not blinded to catheter allocation during the procedure.
Surgical Protocol—TFA Group
Patients in the control group were placed in the supine position, and puncture was performed at the site of palpable femoral artery pulsation below the inguinal ligament. Local infiltration anesthesia was achieved using 5 mL of 1% lidocaine (National Drug Code: H20063856; Specification: 10 mL: 0.173 g). The puncture site was selected where the femoral artery path was clearly visible. Puncture was performed using the Seldinger technique. After inserting a short J-tip guidewire, a 5F femoral sheath was advanced into the artery, followed by removal of the guidewire. Intravenous heparin (3000 U) was administered intraoperatively for anticoagulation, and a 6F catheter system was used for aortic angiography. At the end of the procedure, the sheath was removed, and the puncture site was covered with sterile gauze. Manual compression was applied for hemostasis, lasting no less than 15 minutes or until active bleeding ceased. After initial hemostasis, a compression bandage was applied using an elastic wrap and maintained for at least 6 hours. Postoperatively, patients were instructed to immobilize the lower limb on the puncture side, avoiding flexion, extension, and weight-bearing movements. The bandage and immobilization were removed 24 hours after the procedure, as shown in Figure 1.
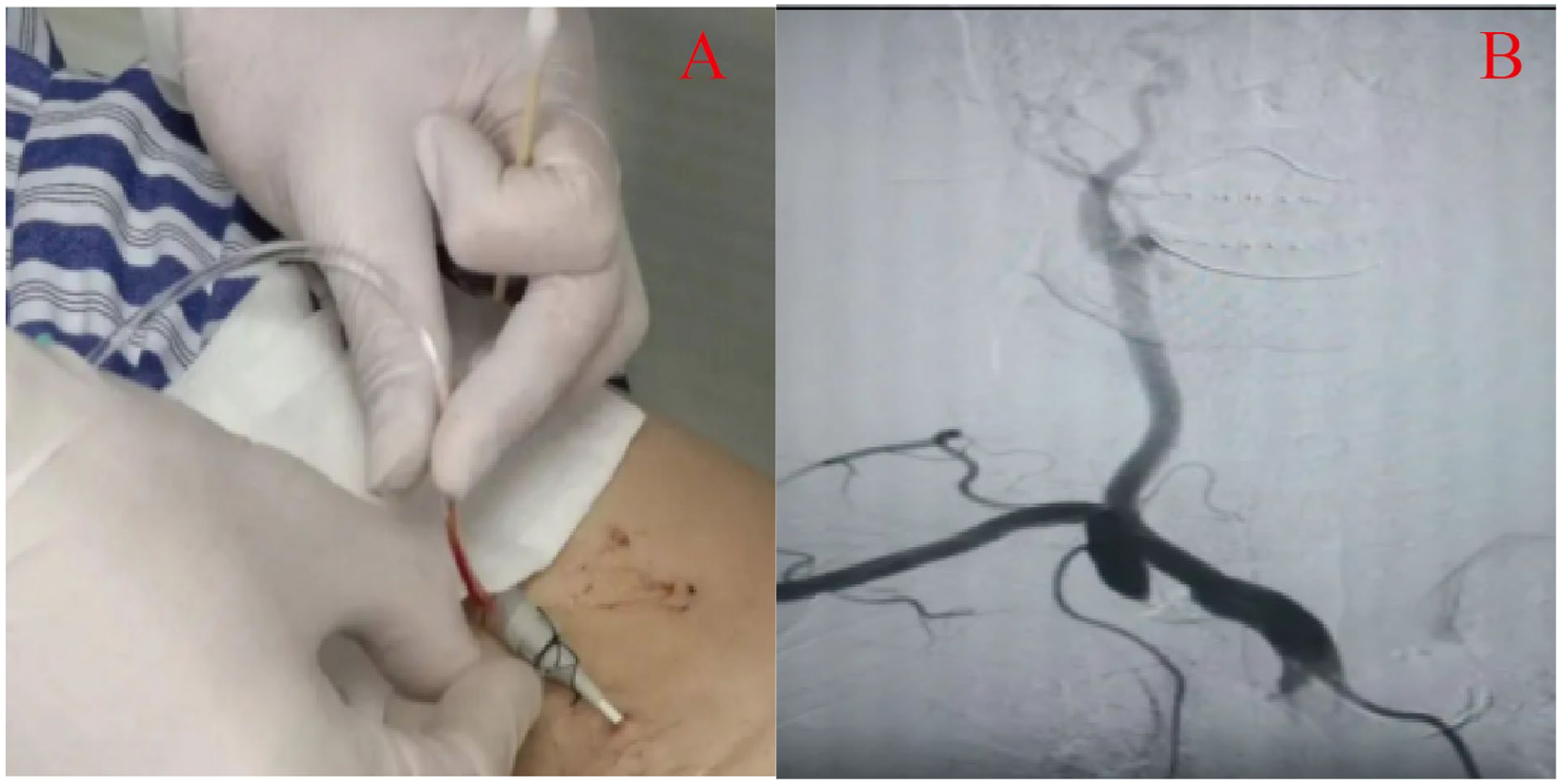
Intraoperative images of the transfemoral approach (TFA). (A) Intraoperative view of the TFA procedure. (B) Cerebral digital subtraction angiography (DSA) image obtained via the TFA.
Surgical Protocol—TRA Group
Patients in the observation group were placed in the supine position. Local infiltration anesthesia was administered with 5 mL of 1% lidocaine. The puncture site was identified at the medial side of the radial styloid process where the radial artery pulsation was prominent. Radial artery puncture was performed using the Seldinger technique. Upon successful arterial blood return, the puncture needle was withdrawn, and an arterial sheath was inserted.
To prevent radial artery spasm, intra-arterial nitroglycerin (National Drug Code: H20057216; Specification: 1 mL: 5 mg ×10 ampoules) was administered intraoperatively at a dose of 200 μg. Additionally, intravenous heparin (Specification: 0.4 mL: 4100 AXaIU) was administered at a dose of 3000 U for systemic anticoagulation. A 6F catheter system was used to complete aortic arch angiography, and both bilateral carotid and vertebral arteries were selectively visualized and evaluated.
After removal of the arterial sheath, a radial artery hemostatic device (such as a radial compression band or elastic dressing) was immediately applied at the puncture site for continuous compression over 6 hours. Pressure was gradually reduced during this period while closely monitoring the puncture site to ensure the absence of active bleeding or hematoma formation.
Postoperatively, patients were allowed to ambulate freely; however, the upper limb on the puncture side was kept relatively immobilized, and strenuous activity was restricted for 24 hours. The TRA access site and cerebral angiography procedure are illustrated in Figure 2.
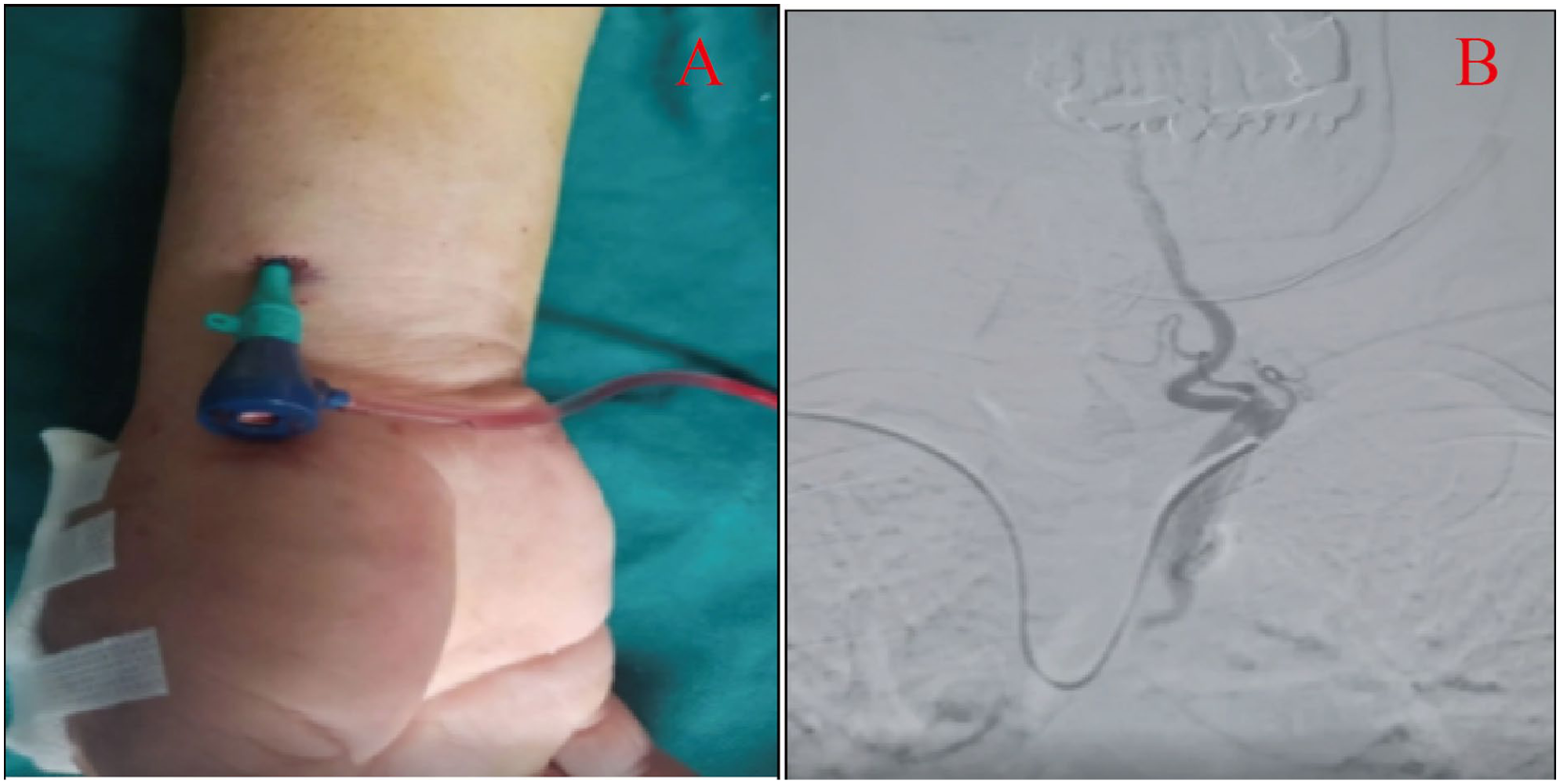
Intraoperative images of the transradial approach (TRA). (A) Intraoperative view of the TRA procedure. (B) Cerebral digital subtraction angiography (DSA) image obtained via the TRA.
Outcome Measures
The following parameters were collected and analyzed:
Puncture time: Defined as the duration from the initiation of local anesthesia to the successful insertion of the arterial sheath, measured in minutes (min).
Fluoroscopy time: Defined as the total X-ray exposure time recorded by the system, including fluoroscopy and DSA, from the successful insertion of the sheath to the end of the procedure, measured in minutes.
Contrast agent volume: Defined as the total amount of iodine-based contrast medium injected into the patient to visualize vessels under X-ray, measured in milliliters.
Hemostasis time: Defined as the time required to achieve complete cessation of bleeding at the puncture site after sheath removal through manual or device-assisted compression, measured in minutes.
Immobilization time: Defined as the postoperative duration during which strict immobilization of the puncture site was required to ensure hemostasis and prevent complications.
Postoperative complication rate: In this study, complications were predefined to include common adverse events observed after cerebral DSA, namely subcutaneous hematoma, ecchymosis, urinary retention, and vasospasm. Although some of these events may not require additional treatment, they were included because they affect patient comfort, recovery, and overall clinical experience. The complication rate was calculated as the proportion of patients who developed any of the above events relative to the total number of procedures performed.
Statistical Analysis
The primary outcome of this study was the incidence of access-site complications. Based on preliminary data, the complication rate in the TFA group was approximately 18.91%, and the expected rate in the TRA group was 4.36%. Using a two-sided test with α=0.05 and power (1–β) of 80%, and assuming a 1:1 allocation ratio, the sample size was calculated using the formula for comparison of 2 independent proportions, yielding a required sample size of 42 patients per group (total n=84). Considering an anticipated dropout rate of approximately 10%, a total of 90 patients were initially planned for inclusion. Ultimately, 114 patients were enrolled in the study.
All statistical analyses were performed using SPSS version 27.0. Continuous variables were tested for normality. Variables with normal distribution were presented as mean ± standard deviation (SD) and compared between groups using independent sample t-tests. Non-normally distributed variables were presented as median (P25, P75) and analyzed using the Mann–Whitney U test. Categorical variables were expressed as number and percentage [n(%)] and compared using the chi-square test. A p-value < 0.05 was considered statistically significant.
Results
Baseline Characteristics of Included Patients
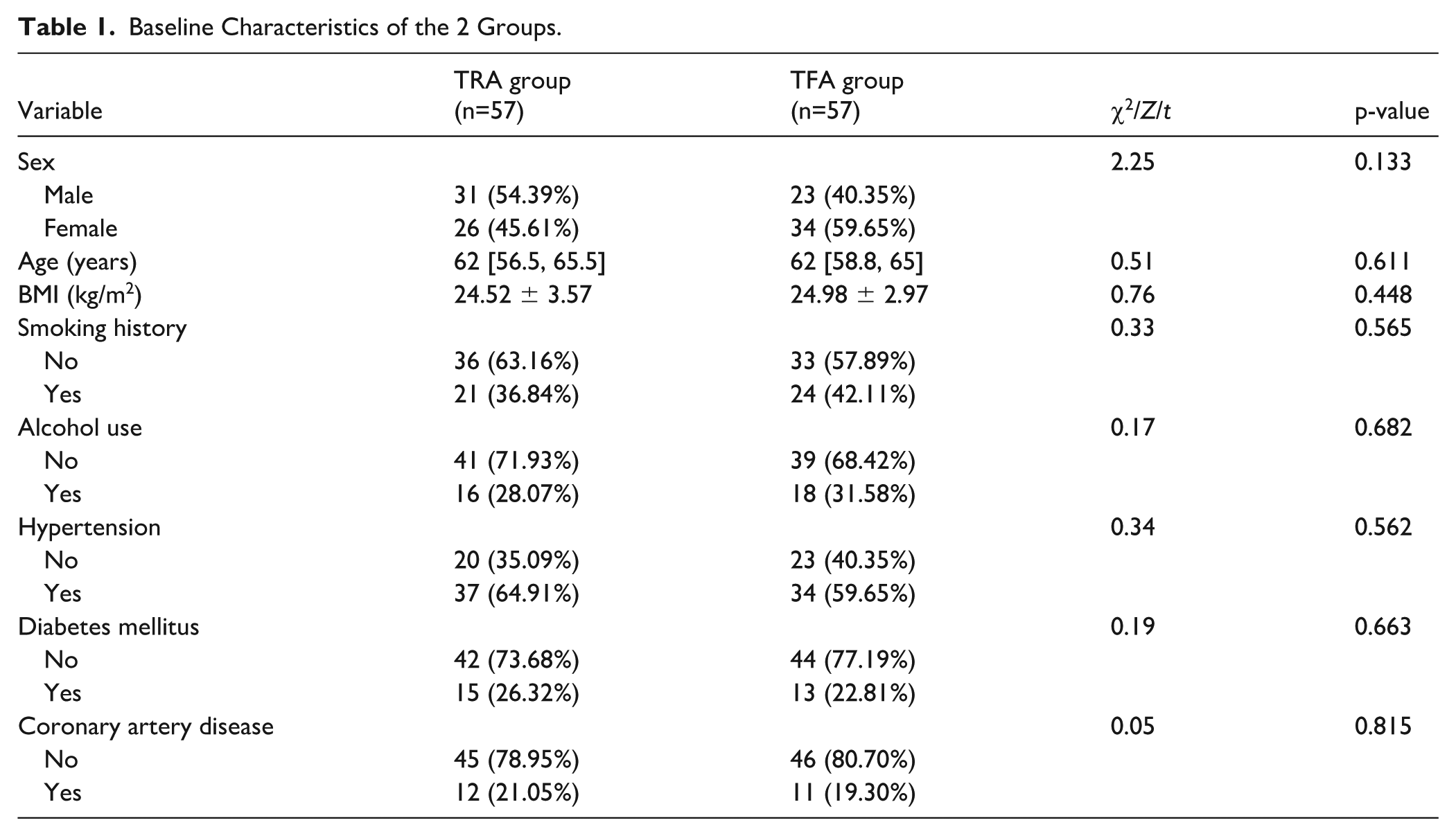
A total of 114 patients were enrolled, including 57 in the TRA group (31 males, 26 females) and 57 in the TFA group (23 males, 34 females). There were no statistically significant differences between the 2 groups in terms of gender, age, or body mass index (BMI) (all p>0.05). The distribution of smoking and alcohol consumption histories was comparable between groups. Likewise, the prevalence of comorbidities, including hypertension, diabetes mellitus, and coronary artery disease, did not differ significantly between the 2 groups (all p>0.05). These findings indicate that the baseline characteristics were balanced and comparable between the groups (Table 1).
Baseline Characteristics of the 2 Groups.
Comparison Between TRA and TFA
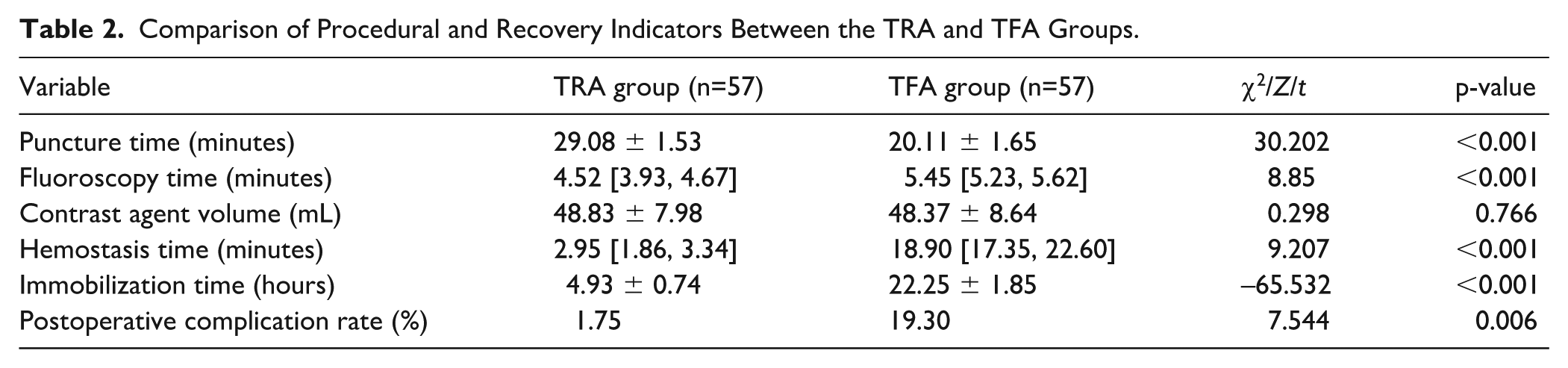
Regarding procedural metrics, the TFA group demonstrated a significantly shorter puncture time compared to the TRA group (p<0.001). However, fluoroscopy time was significantly longer in the TFA group (p<0.001). There was no statistically significant difference in contrast agent volume between the 2 groups (p>0.05).
In terms of postoperative recovery, the TRA group showed clear advantages, with significantly shorter hemostasis time (p<0.001) and immobilization time (p<0.001) compared to the TFA group. The postoperative complication rate was also significantly lower in the TRA group (p=0.002). Only one case of vasospasm occurred in the TRA group, whereas 11 complications were reported in the TFA group, including 4 cases of subcutaneous hematoma, 2 cases of ecchymosis, and 5 cases of urinary retention.
Although the TFA approach was superior in terms of puncture speed, the TRA approach significantly reduced intraoperative radiation exposure and markedly improved postoperative recovery—demonstrated by shorter hemostasis and immobilization times—as well as a lower risk of complications. These findings suggest that TRA offers superior clinical safety (Table 2).
Comparison of Procedural and Recovery Indicators Between the TRA and TFA Groups.
Comparison of TRA and TFA in Patients With Type I, Type II, and Type III Aortic Arches
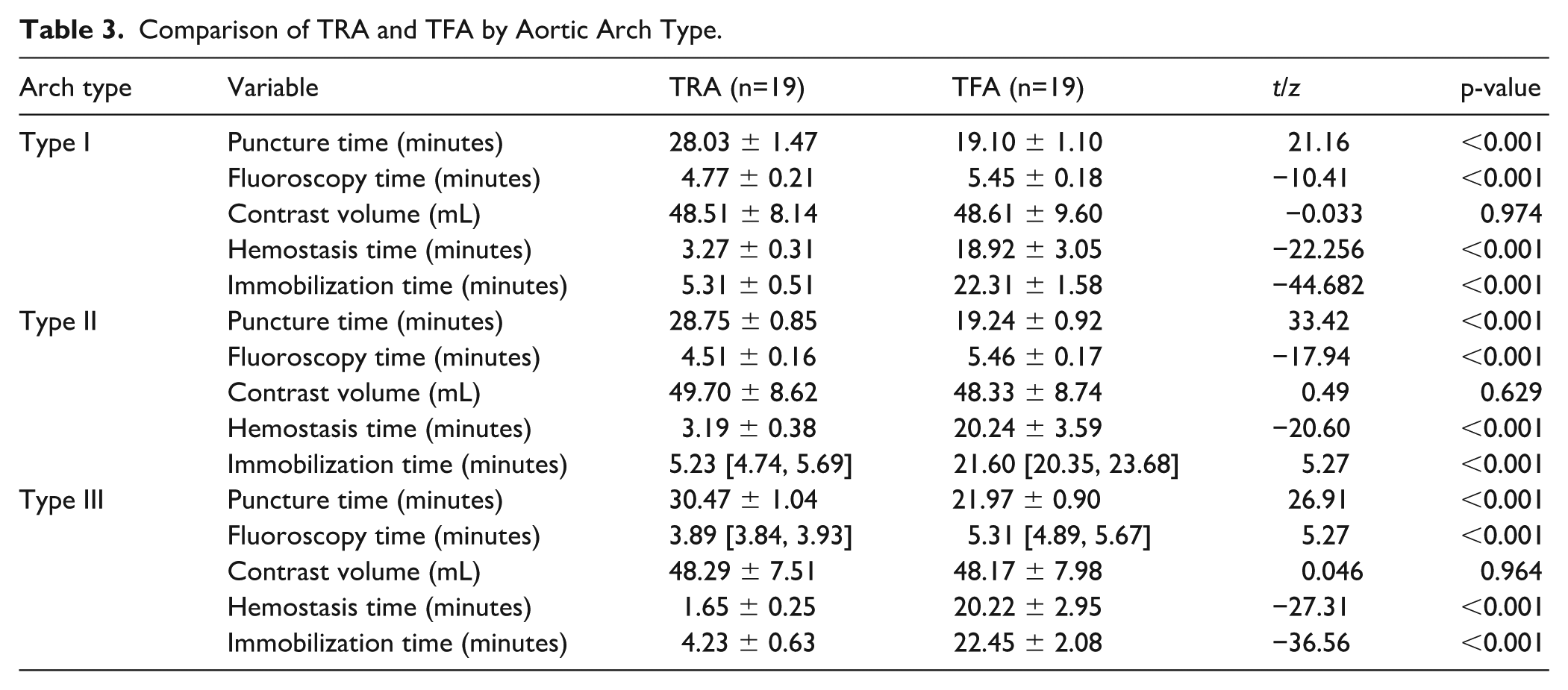
A stratified analysis was performed to compare the clinical outcomes of DSA using TRA and TFA based on different aortic arch types. The results showed that regardless of aortic arch classification, TRA consistently demonstrated superior postoperative recovery and safety profiles compared to TFA (Table 3). In all 3 arch types, the TRA group exhibited significantly shorter fluoroscopy time, hemostasis time, and immobilization time (all p<0.001). Although the TRA group had slightly longer puncture times than the TFA group across all arch types (all p<0.001), no significant differences were found in contrast agent usage between the groups (all p>0.05). Notably, in patients with type III arches, the advantages of TRA were especially pronounced, with greater reductions in fluoroscopy time, hemostasis time, and immobilization time. These findings suggest that TRA may be the preferred access route for patients with complex aortic arch anatomy.
Comparison of TRA and TFA by Aortic Arch Type.
Comparison of Simmon 1 and Simmon 2 Catheters in TRA Patients With Type III Aortic Arches
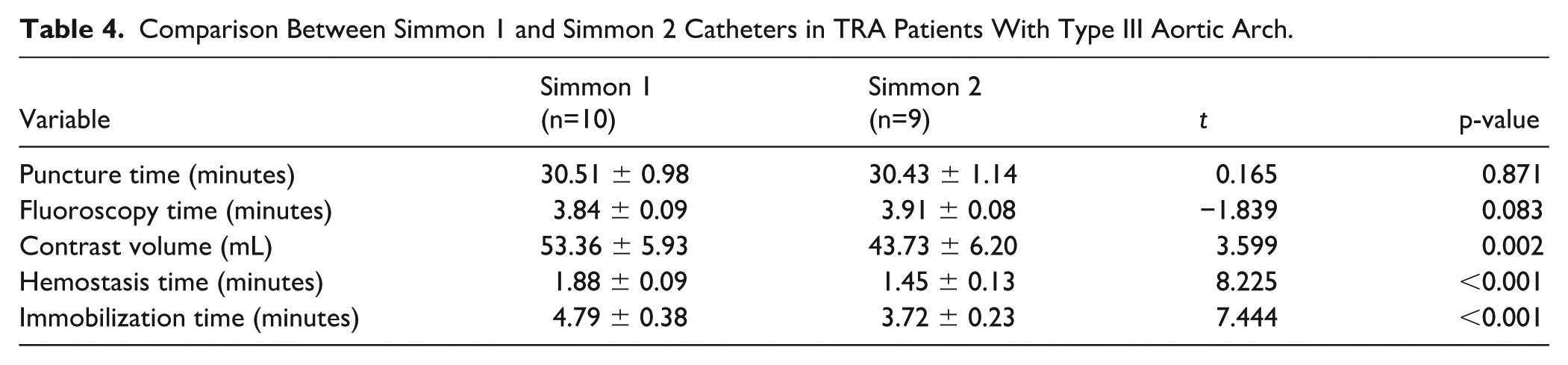
Among patients with type III aortic arches in the TRA group, a comparison was made between the use of Simmon 1 and Simmon 2 catheters. No significant differences were observed in puncture time (p=0.871) or fluoroscopy time (p=0.083) between the 2 catheter types. However, patients who received Simmon 2 catheters required significantly less contrast agent (p=0.002), and experienced markedly shorter hemostasis time (p<0.001) and immobilization time (p<0.001) compared to those who used Simmon 1 catheters (Table 4). These findings indicate that although the 2 catheters performed similarly in procedural duration, Simmon 2 demonstrated a clear clinical advantage in postoperative recovery and contrast efficiency, particularly in minimizing hemostasis and immobilization durations.
Comparison Between Simmon 1 and Simmon 2 Catheters in TRA Patients With Type III Aortic Arch.
Discussion
This prospective randomized controlled trial systematically evaluated the technical performance, safety, and postoperative recovery of TRA versus TFA approaches in patients undergoing digital subtraction DSA with varying aortic arch anatomies. Additionally, we assessed the value of using the Simmon 2 catheter in type III aortic arches within the TRA group. In this study, the enrolled patients primarily presented with stenotic cerebrovascular diseases, including intracranial arterial stenosis, carotid artery stenosis, and subclavian artery stenosis, which constituted the main clinical background for evaluating the procedural performance of TRA and TFA. Our findings showed that although TRA was associated with a slightly longer puncture time, it was linked to shorter hemostasis and immobilization times, lower complication rates, and favorable intraoperative efficiency metrics compared to TFA. In patients with type III arches, the Simmon 2 catheter was associated with reduced contrast usage and shorter recovery indicators compared with the Simmon 1 catheter.
Specifically, the TRA group exhibited significantly shorter postoperative hemostasis and immobilization times, along with a lower incidence of puncture-related complications. These findings may be attributed to the superficial location, compressibility, and relatively fixed anatomical course of the radial artery. 16 This is consistent with the findings of Bhat et al, 10 who reported fewer complications and higher patient satisfaction following TRA. Although TRA was associated with longer puncture duration, it paradoxically resulted in reduced fluoroscopy time, suggesting enhanced catheter manipulation precision and potentially shorter vascular selection and imaging preparation time.
Subgroup analysis by aortic arch type revealed that type III arches indeed posed greater technical challenges due to their anatomical complexity, which may prolong procedural duration. 17 However, TRA still demonstrated unique advantages in this subgroup. Our results showed that, among type III arch patients, TRA reduced fluoroscopy time by 26.7% and lowered complication rates from 21.1% to 5.3%. This benefit may stem from the reduced need for prolonged bed rest and a lower incidence of vascular complications associated with TRA. 3 These findings suggest that, in the hands of experienced operators, TRA is not only feasible in standard anatomies but can also be safely and effectively applied in complex vascular conditions, expanding its scope of indication.
In addition, this study focused on the impact of catheter selection within the TRA group for patients with type III arches. The Simmon 2 catheter outperformed the Simmon 1 catheter by reducing the required contrast volume and significantly shortening both hemostasis and immobilization times. These findings align with previous studies, which reported that the Simmon 2 catheter achieved a 89.8% success rate in accessing the left vertebral artery in type III arches, compared to only 52.2% with Simmon 1. 17 Our prospective design further validates the advantages of the Simmon 2 catheter in complex arch anatomy and provides direct comparative data, supporting the development of individualized catheter selection strategies. The wider curvature and longer supporting segment of the Simmon 2 catheter may provide greater stability and support during rotation and manipulation, particularly in the complex anatomy of type III aortic arches, allowing the catheter to better conform to the vascular pathway.18,19
This study also underscores the clinical value of preoperative aortic arch classification via CTA. Accurate preoperative identification of aortic arch type allows for the development of tailored access and catheter strategies based on individual anatomy, which can enhance procedural efficiency and safety. Particularly for patients with type III arches, TRA combined with the Simmon 2 catheter may offer a more controlled and optimized operative pathway.
Despite the strengths of this prospective trial, several limitations should be noted. First, this was a single-center study with a limited overall sample size and a relatively small subgroup of type III arch patients in the TRA group, which may affect generalizability. Second, although all operators were highly experienced, inter-operator variability may have influenced some procedural metrics. Third, the catheter comparison was limited to existing models, and newer steerable or adjustable catheters were not included. Lastly, this study did not assess long-term clinical outcomes, which warrants future studies incorporating follow-up data and functional recovery assessments.
In conclusion, this study demonstrated that TRA is not only a safe and effective access strategy for routine cerebral angiography but also offers clear procedural and safety advantages in patients with complex aortic anatomy, particularly type III arches. The observed superiority of the Simmon 2 catheter in this context provides operators with a more reliable tool for challenging cases. Future large-scale, multicenter studies with extended follow-up are needed to validate these findings and further standardize the application of TRA in neurovascular interventions.
Conclusions
This study suggests that TRA may be a preferable alternative to TFA for patients undergoing DSA. Although TRA requires more time for arterial puncture, it significantly reduces intraoperative fluoroscopy exposure, shortens postoperative hemostasis and immobilization durations, and markedly lowers the incidence of access site complications. Notably, the advantages of TRA remain consistent even in patients with the most anatomically challenging type III aortic arches. In this subgroup, the combined use of the Simmon 2 catheter further improves operative metrics by reducing contrast agent usage and accelerating postoperative recovery. These findings provide preliminary evidence supporting the use of TRA in complex cerebrovascular anatomy. Future large-scale, multicenter studies with long-term follow-up are warranted to validate and enhance the evidence base for access strategy selection.
Footnotes
Acknowledgements
Not applicable.
Ethical Considerations
The study was approved by the Ethics Committee of Jinhua Hospital of Traditional Chinese Medicine.
Consent to Participate
Written informed consent was obtained from all participants prior to enrollment.
Consent for Publication
Not applicable.
Author Contributions
Bin Xu, Xinli Liu, and Xi Liu contributed to the study design. Xinli Liu conducted the literature search. Xi Liu acquired the data. Bin Xu wrote the article. Bin Xu and Xinli Liu performed data analysis. Bin Xu and Xi Liu revised the article and gave the final approval of the version to be submitted. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Jinhua Municipal Public Welfare Technology Application Research Projects: Prospective controlled study on the application value of transradial approach in complex aortic arch type cerebral angiography (Grant No. 2024-4-130).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Clinical Trial Registration
This study was registered with the Chinese Clinical Trial Registry under the identifier ChiCTR2500100127.
Availability of Data and Materials
The data and materials in the current study are available from the corresponding author on reasonable request.