
Abstract
Thoracic endovascular aortic repair (TEVAR) is a minimally invasive technique for the treatment of thoracic aortic aneurysms (TAA). We hypothesized that alteration of blood hemodynamics in the thoracic aorta caused by stent implantation can possibly lead to hypertension and reduced coronary flow leading to the induction of heart failure (HF). The search in PubMed, Web of Science, Scopus, and the Cochrane library for studies containing data about the occurrence of HF after TEVAR resulted in 1231 articles of which 11 fulfilled the inclusion criteria. A meta-analysis was undertaken with the raw incidence of HF post-implantation as the primary endpoint. This occurred, in the first 30 days, to 684 out of 30,680 total patients (2.23%), and the raw incidence rate of HF was 0.03 [0.02–0.04], p<0.001. The random effects model was used because the examined studies had significant heterogeneity (I2=99.999%, τ2=3.905×10−4, p<0.001. In addition, significant publication bias was observed (Egger’s test z=2.156, p=0.031). HF may develop in 30 days post-TEVAR possibly because of the increased aortic stiffness and the subsequent heamodynamic alterations which reduce the coronary blood supply. Thus, it may be necessary to initiate early pharmacological intervention while further research with randomized controlled trials with longer follow-up is warranted for the evaluation of the incidence of HF in the long term after TEVAR.
Clinical Impact
Our meta-analysis shows that heart failure (HF) can occur in approximately 3% of patients within 30 days after TEVAR, indicating that HF is a clinically relevant but often under-recognized complication. Increased aortic stiffness and subsequent heamodynamic alterations which reduce the coronary blood supply may contribute to the development of HF. Our findings highlight the need for careful peri- and post-operative cardiac monitoring, particularly in patients with pre-existing cardiovascular risk and the need for hemodynamic optimization after stent-graft implantation.
Keywords
Introduction
Thoracic aortic aneurysms (TAA) may be confined to aortic root, ascending aorta, aortic arch, and descending aorta and are defined as an increase in diameter by 50% compared to proximal healthy segment. Aneurysms located above the ligamentum arteriosum are usually caused due to degenerative processes of the tunica media. Below this point, atherosclerosis is the main cause. TAA usually go unnoticed as they do not cause warning symptoms causing devastating consequences with the case fatality ratio reaching 80% to 90% in the case of rupture.1 –3
Therefore, effective treatment for TAA is a must to prevent these consequences. One treatment modality for TAA is thoracic endovascular aortic repair (TEVAR). It involves the implantation of an endovascular stent-graft that is introduced endovascularly with the use of a catheter.4,5 TEVAR is less invasive than open surgery, leading to lower return to hospital stay and improved recovery times.
Despite its advantages, the use of TEVAR has its own unique pitfalls and complications with the most common ones being spinal cord ischemia, stroke, and endoleaks. 6
Some authors have suggested that TEVAR may significantly alter hemodynamics due to the increased stiffness of the graft compared to native tissues potentially leading to increased left ventricular strain, higher pulse pressure, and eventually congestive heart failure (CHF). 7 Heart failure (HF) was defined by the international HF societies as “a clinical syndrome with symptoms and/or signs caused by a structural and/or functional cardiac abnormality and corroborated by elevated natriuretic peptide levels and/or objective evidence of pulmonary or systemic congestion.” 8 Furthermore, HF has been reported to be a risk factor for 1-year mortality after thoracic endovascular aortic repair. 9
We hypothesized that alteration of blood hemodynamics in the thoracic aorta caused by stent implantation can possibly lead to hypertension and reduced coronary flow, leading to the induction of HF. The aim of the present meta-analysis was to investigate possible relationship between TEVAR and HF and explore the consequences of TEVAR on the cardiac function.
Materials and Methods
Search Strategy
We used the Cochrane Handbook and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) principles for the structure and implementation of the literature search.10,11 The aim of the search was to find articles that reported HF as an outcome, in patients that had undergone TEVAR.
An unrestricted search was performed in the following databases: PubMed, Web of Science, Scopus, and the Cochrane Library. The last search was conducted in March 2024.
The principal search terms for all databases were HF and endovascular aneurysm repair. The references for the selected articles were also evaluated. The specific search queries were as follows:
PubMed: (“Heart Failure”[Mesh] OR “heart failure” OR “cardiac failure”) AND (“Endovascular Aneurysm Repair”[Mesh] OR “Endovascular Aneurysm Repair” OR TEVAR), Web of science: (“heart failure” OR “cardiac failure”) (All Fields) AND (“endovascular aneurysm repair” OR TEVAR) (All Fields), Cochrane: “heart failure” AND aneurysm AND (endovascular OR TEVAR OR EVAR) in abstract, title, keywords, Scopus: (TITLE-ABS-KEY(“heart failure” OR “cardiac failure”) AND TITLE-ABS-KEY((“Endovascular Aneurysm Repair” OR TEVAR))).
Two of the authors (AIM and KS) designed and conducted the literature search and the search was reviewed by a third author (GK).
Selection Process
For the selection process, specific inclusion and exclusion criteria were used. The following inclusion criteria were applied:
(1) Human studies. (2) Full research articles that included quantitative data on the frequency of HF after endovascular aneurysm repair.
The following exclusion criteria were applied:
(1) Non-human studies, (2) case reports and reviews, (3) previous meta-analyses, (4) editorials, (5) studies in languages other than English.
Risk of Bias Assessment
Two independent reviewers (ΑΙΜ and GG) assessed the risk of bias. Each observational non-randomized study was assessed using a modified version of the Risk of Bias in Non-randomized Studies-of Interventions (ROB-INS-I) tool. 12 The evaluation of the risk of bias in randomized controlled trials (RCTs) was assessed with the Cochrane Checklist. 13
Quality Assessment
The quality of the studies included in the analysis was assessed using an 18-item version of a rating scale based on the Downs and Black checklist for measuring. 14 Each item was ranked with a binary score (0 or 1). As an exception, one item was ranked with a scale from 0 to 2.
Two researchers (AIM and AX) independently assessed the ratings and a third reviewer (KS) reviewed and quantified the ratings using Cohen’s kappa. 15
Statistical Analysis
The meta-analysis was conducted using the statistical software R v. 3.6.1 (R Foundation for Statistical Computing, Vienna, Austria). Based on the existing data, we chose to analyze the raw incidence rate of AF after TEVAR in the short term (up to 30 days after the procedure). As heterogeneity among studies was anticipated, we used the random effects model. Heterogeneity was evaluated with the statistical inconsistency Higgin’s I2 test. 16 Low heterogeneity was considered when I2 values were <40%, and high heterogeneity when I2 values were >75%. Heterogeneity was visualized with a forest plot. The Egger’s test of the intercept was used for assessment of publication bias and visualized with a funnel plot. A meta-regression analysis was performed to explore the impact of the potential interaction factors for which adequate numerical data were available for the analysis, particularly age and hypertension. Probability values <0.05 were considered as statistically significant.
A few of the selected studies included data and information divided into groups. The separate sets of data from the above-mentioned articles were analyzed separately as independent data sets.
Endpoints
The primary endpoint of this study was the occurrence of post-TEVAR HF. Secondary endpoints were the possible effects as coefficients of the demographic characteristics and comorbidities of the patients, particularly age and hypertension.
Results
Search Results and Characteristics of the Studies
The search resulted in 318 results from PubMed, 793 from Scopus, 24 from Cochrane, and 121 results from the Web of Science, a total of 122 articles. After the elimination of duplicates, the exclusion and inclusion criteria were applied, and 10 articles were selected, and their full text was examined. One additional article was found from the references of the selected articles. Finally, 11 articles were included in the analysis (Figure 1).17–27
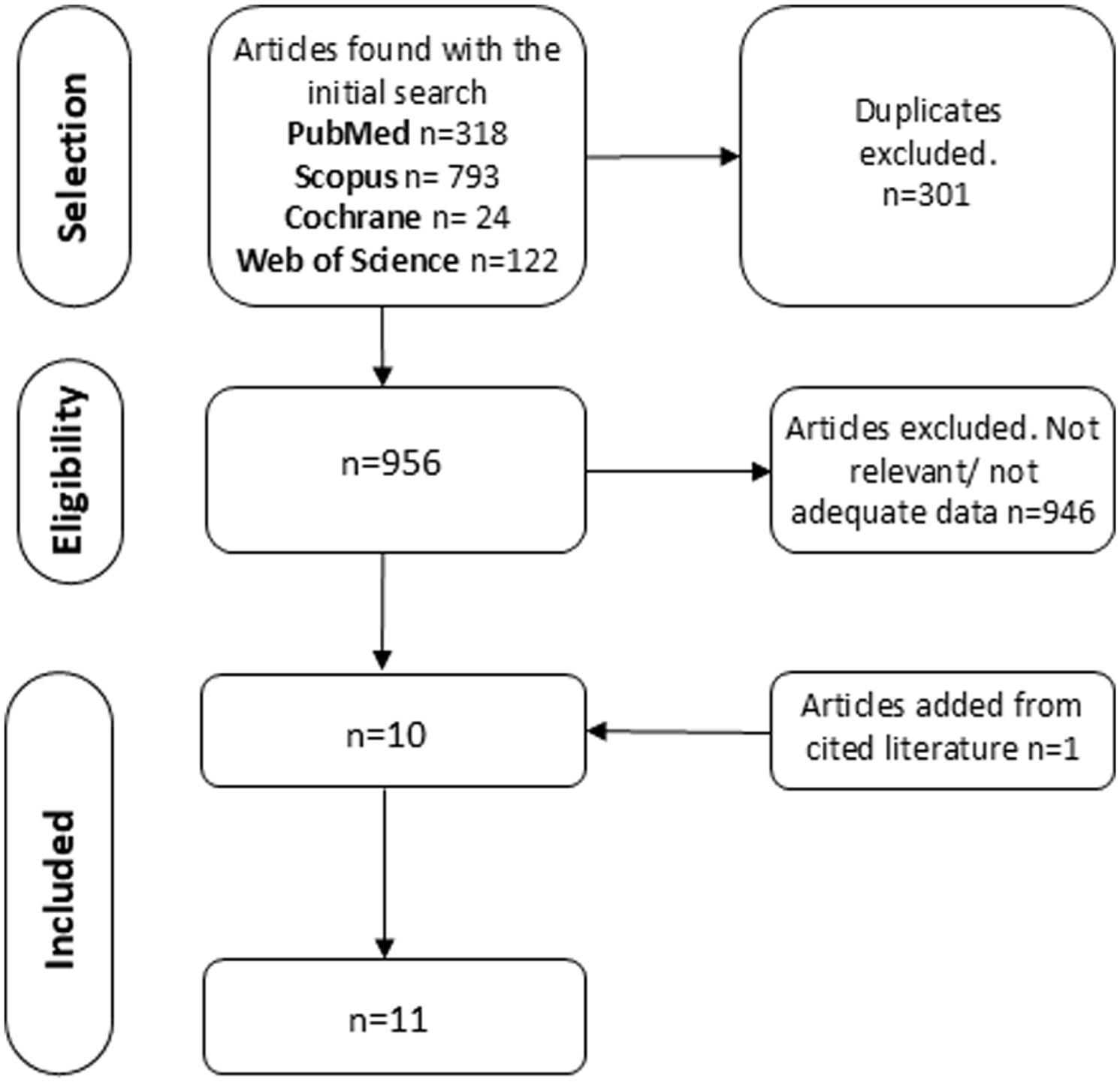
Search strategy.
The selected studies included 1 randomized controlled trial and 10 retrospective studies (Table 1).
Studies Included in the Meta-Analysis, Demographic Characteristics of Patients and Pre-Operative Comorbidities.
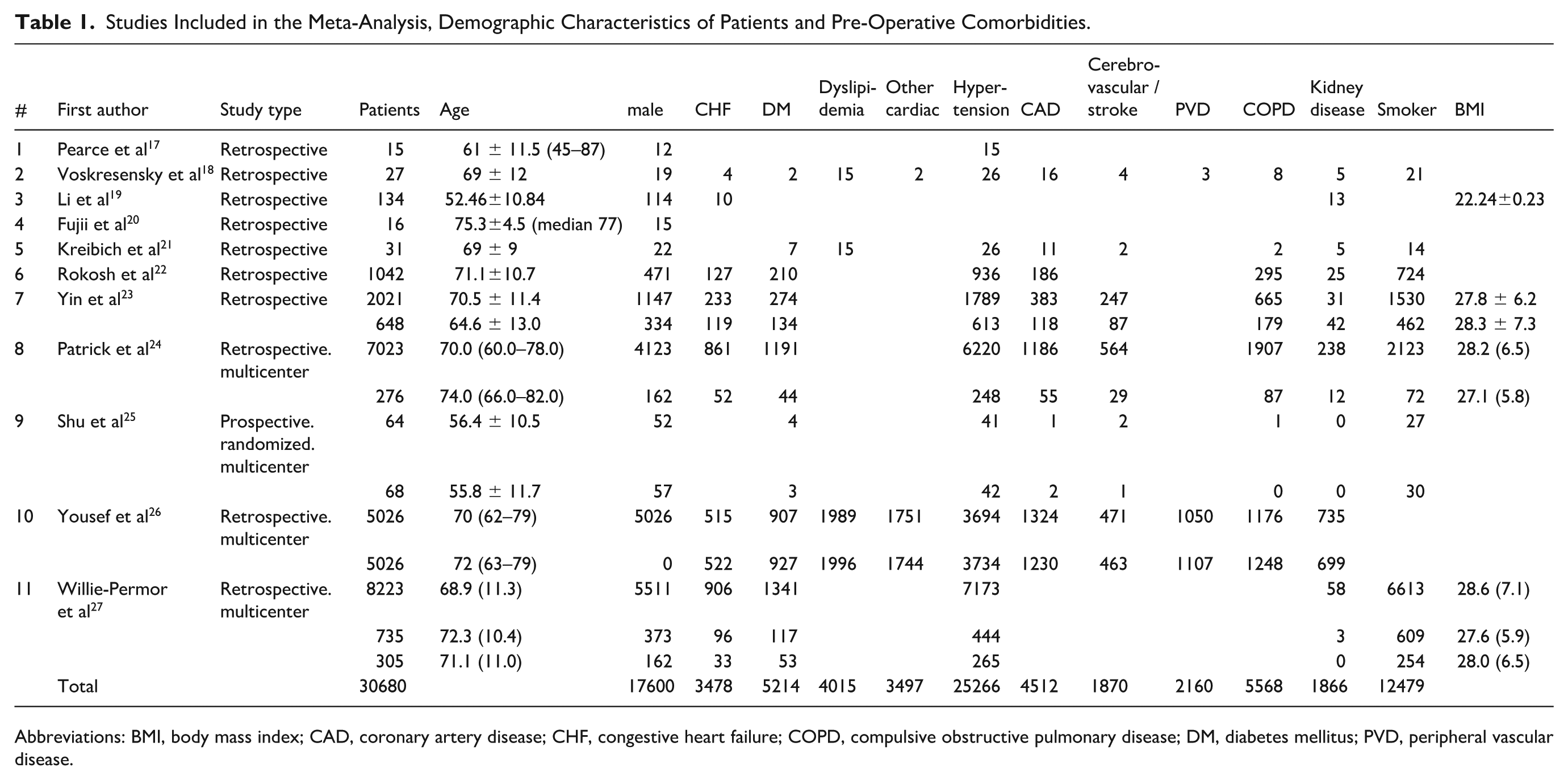
Abbreviations: BMI, body mass index; CAD, coronary artery disease; CHF, congestive heart failure; COPD, compulsive obstructive pulmonary disease; DM, diabetes mellitus; PVD, peripheral vascular disease.
The included articles included 19,315 patients, of which 11,072 (57.3%) were male. The age range was 52 to 82 years. The pre-operative characteristics of the patients, including their comorbidities, are shown in Table 1. There was no data in the selected articles about the methods used to estimate of myocardial changes leading to HF (magnetic resonance imaging or ultrasound) mainly because the design of these studies was not initially to estimate the rate of HF after TEVAR.
Some of the selected articles contained two or more separate sets of data for different patient groups without providing data for all the patients. Yin et al, 23 contained separate data for Caucasian and black patients. Patrick et al 24 contained separate data for patients treated with local and general anesthesia. Shu et al 25 contained two separate sets of data depending on the device used for TEVAR. Yousef et al, 26 contained separate data for male and female patients. Willie-Permor et al 27 separated the patients undergoing TEVAR in three groups, depending on the volume of transfused blood. As mentioned in the methods section, different groups of patients from the same article were treated as separate data sets.
Quality of the Studies
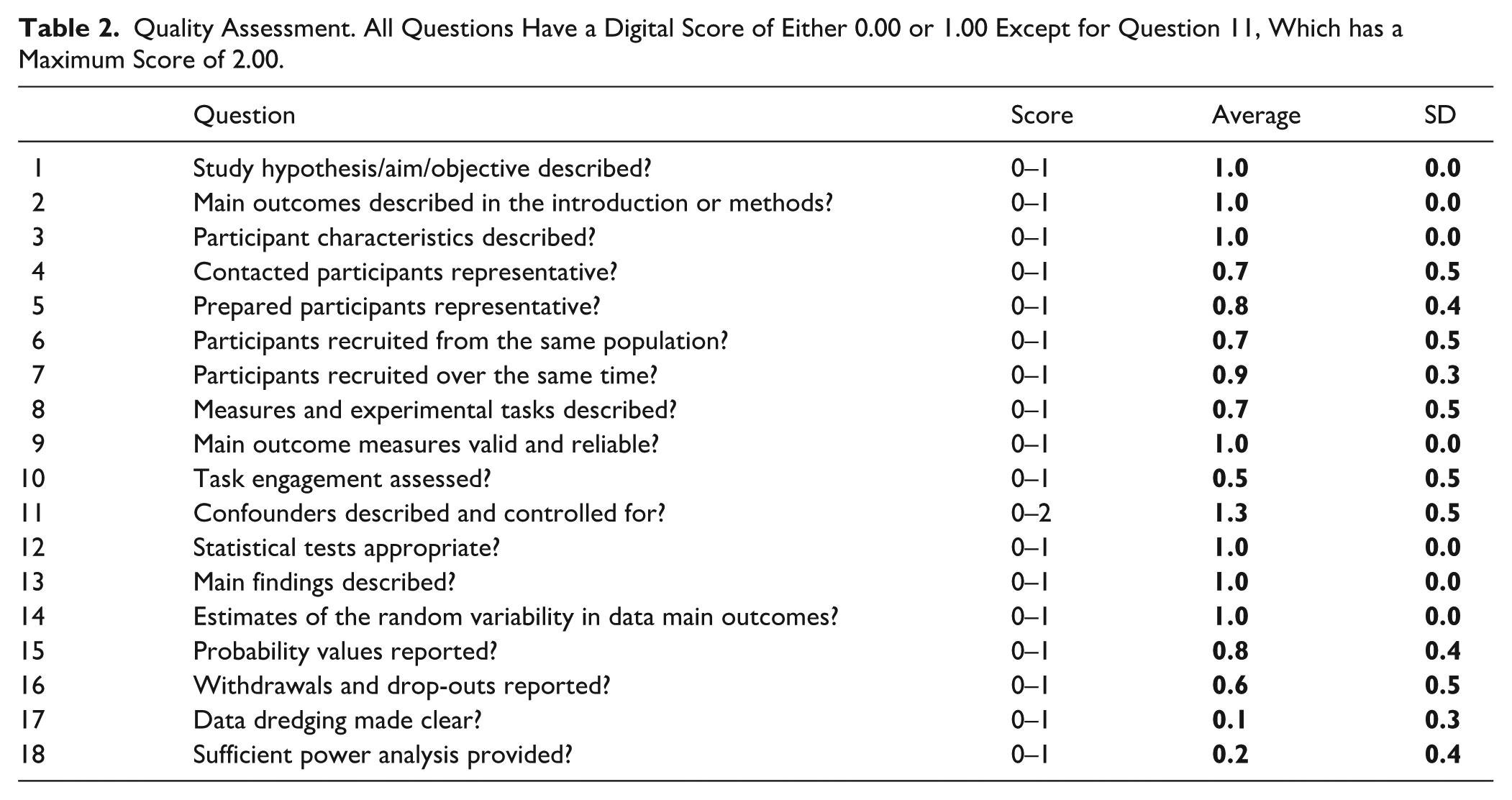
The quality assessment is shown in Table 2. The studies had a median rating of 0.80 [IQR 0.36–0.84], and a range from 0.5 to 1.3.
Quality Assessment. All Questions Have a Digital Score of Either 0.00 or 1.00 Except for Question 11, Which has a Maximum Score of 2.00.
Meta-Analysis Results
HF occurred to 684 out of the 30,680 total patients of the meta-analysis (2.23%). The overall raw incidence rate of short-term (post-operative up to 30 days) HF was 0.03 [0.02–0.04], p<0.001.
The examined studies had significant heterogeneity (I2=99.999%, τ2=3.905×10−4, p<0.001) and thus we used the random effects model. A forest plot of the raw incidence rate of HF is shown in Figure 2.
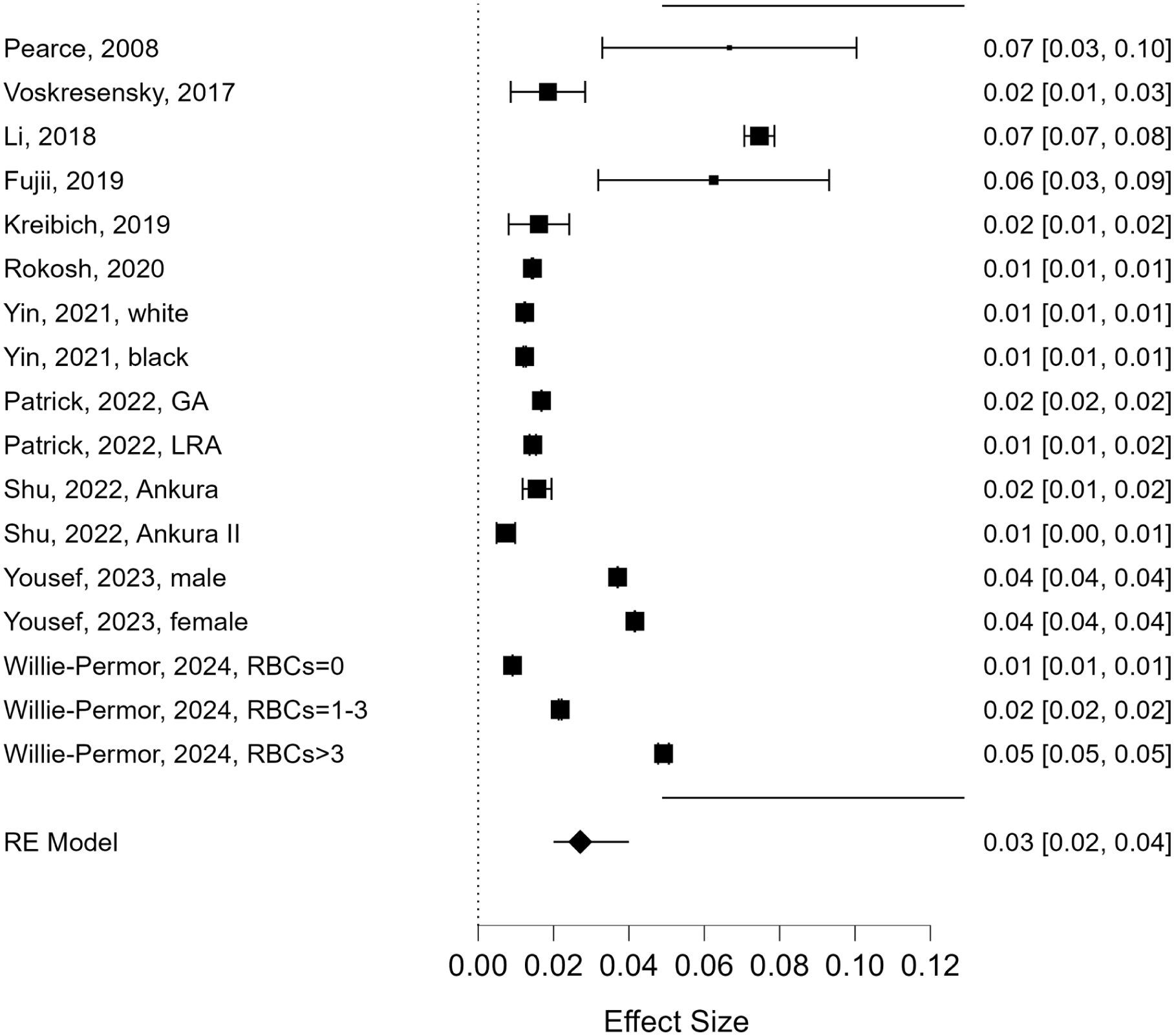
Forest plot: raw incidence rate of short-term heart failure (HF) after thoracic endovascular aortic repair (TEVAR).
Significant publication bias was observed (Egger’s test z=2.156, p=0.031) as it is displayed in the funnel plot (Figure 3).
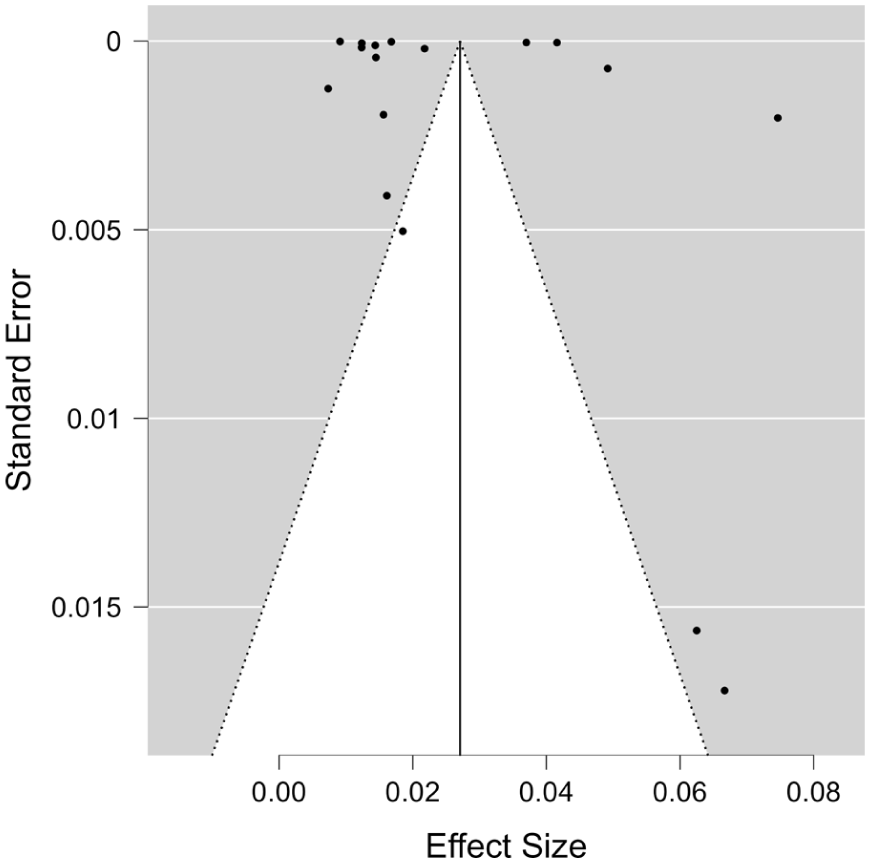
Funnel plot: raw incidence rate of short-term heart failure (HF) after thoracic endovascular aortic repair (TEVAR).
A meta-regression was conducted to investigate the possible effect of covariates for which adequate numerical data were available. The meta-analysis with covariates age and previously existing hypertension resulted that hypertension and age were not statistically significant coefficients.
Discussion
Our meta-analysis showed that HF after TEVAR may develop early post-operatively, though not frequently, with the occurrence rate being 0.03 [0.02–0.04].
Beck et al, 28 found significantly increased possibility for post-operative HF in patients with acute type b aortic dissection when TEVAR was conducted in the acute phase (1–14 days after onset) compared to TEVAR conducted in the subacute phase (15–90 days after onset).
Patrick et al 24 found a lower rate of HF after TEVAR in patients that were given local anesthesia in comparison with patients that were given general anesthesia (OR, 0.19; 95% CI, 0.01–0.89; p=0.01). Willie-Permor et al 27 found a 2-fold increased risk of HF (adjusted relative risk 2.04, 95% confidence interval 1.09, 3.83, p=0.03) in patients that received 1 to 3 blood units during operation compared to those ones who did not receive any transfusion. Yin et al 23 found similar rates of post-operative HF in black and white patients. Yousef et al 26 found no statistically significant differences in the rate of HF between men and women (3.70% vs 4.16%, p=0.238). In a recent study with 22 patients, Hauguel et al 29 found a non-statistically significant increase in the Heart Failure Association’s HF with preserved ejection fraction (HFA-PEFF) score after TEVAR.
A possible explanation of the correlation of TEVAR with HF could be that the increased aortic stiffness due to the stent implantation through induction of hypertension, reduced coronary blood flow that can contribute to the development of HF. 21 TEVAR was found to be associated with increased left ventricular stroke work and mass 7 and aortic stiffness has been reported to contribute to the development of HF. 30 Interestingly, patients with HF (but not controls) were reported to exhibit a significant reduction in aortic distensibility after acute exercise, indicating higher aortic stiffness. 31
The implants used in such operations are made of materials with different properties than the native tissues of the aorta. This in turn leads to altered hemodynamics and to different responses in the hemodynamic changes increasing the strain to the left ventricle and thus resulting potentially in the development of HF.
The disturbance of blood flow to the coronary arteries due to the placement of the prosthesis is also a cause of increased strain and a lower ability of optimal left ventricular function also leading to an increased likelihood of developing HF.
It should be acknowledged that the studies included in our meta-analysis contained only data for the evaluation of the incidence of HF in the short term, i.e. up to 30 days after the operation. It cannot be excluded that HF can occur in the mid- or long- term. Arguably, in the long-rank higher rates of HF may be expected as the strain of the changes caused by the placement of the prosthesis may accumulate overtime but, this remains to be confirmed by further research of good quality.
Limitations
Our study is inherent to potential limitations. First, the included studies were of retrospective nature and only one was a randomized controlled trial. Secondly there were differences in the demographics of the populations included in the studies. There was relatively high heterogeneity and high publication bias in these studies. Finally, the articles included in this meta-analysis did not have as a primary outcome the research question of this study, i.e. if TEVAR contributes to the development of HF.
Conclusion
Short-term post-TEVAR HF occurs at a relatively low rate (~3%). Nevertheless, HF should be promptly recognized and treated. Further research with randomized controlled trials including longer follow-up, are warranted to define the incidence of HF after TEVAR in the long-term.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.