
Abstract

Introduction
Endovascular aortic repair (EVAR) is nowadays an ordinary procedure for the treatment of abdominal aortic aneurysms.1,2 However, more than 1 in 4 patients diagnosed with abdominal aortic aneurysm (AAA) is not suitable to be treated with standard infrarenal endografts because of complex anatomy, including short infrarenal neck length (<15 mm), severe angulation (>60 degrees), or aneurysms that involve renal and visceral branches. 3
In these complex pathologies, fenestrated endovascular aortic repair (FEVAR) is indicated to repair the aneurysm with adequate sealing and to ensure the patency of the aortic branches.4,5 Many custom-made and off-the-shelf (OTS) endografts for FEVAR are currently available in the market. One of these is the low-profile custom-made Fenestrated TREO endograft (19Fr OD; TERUMO Aortic, Bolton Medical Inc, Sunrise, Florida). This device is designed to provide easier iliac access and navigation, which would result in a more controlled deployment for accurate placement. The early experience is promising.6,7
In this study, we present the midterm follow-up of patients receiving the low-profile custom-made Fenestrated TREO endograft (19Fr OD; TERUMO Aortic, Bolton Medical Inc) of 4 high-volume European academic medical centers.
Materials and Methods
The Fenestrated TREO endograft was implanted in 4 European high-volume academic medical centers that either had experience with the TREO endograft or were participating in the TIGER registry, a prospective registry for aortic endografts from TERUMO Aortic (ClinicalTrials.gov Identifier: NCT04246463; Bolton Medical Inc). The definition of a high-volume center is stated herein, those centers that are treating at least 50 complex aortic surgeries a year. Custom-made devices, other than the Fenestrated TREO endograft, were also used in these centers, such as the Cook custom-made FEVAR platform and branched endovascular aortic repair (BEVAR) inner branches, both for AAA juxtarenal and pararenal cases. The Fenestrated TREO endograft was either chosen because of TIGER registry inclusion or in access complexities (such as elongation and small diameter). Other selection criteria were in case of previous aortic surgery and the choice of percutaneous access and lastly based on surgeon preference.
A cohort of 42 consecutive patients, diagnosed with juxtarenal or pararenal AAA, was followed to assess the midterm outcomes of the custom-made Fenestrated TREO Stent-Graft in an observational, retrospective study. The patient cohort described herein includes patients treated from June 2021 to September 2023 with the fenestrated TREO endograft (Amsterdam: 17/42; Italy: 9/42; Utrecht: 8/42; and Barcelona: 8/42). The study was conducted following the local guidelines of the ethical commission of the specific site.
These 42 patients were followed systematically with computed tomography angiography (CTA) at 1 month and 1 year and duplex ultrasound every 6 months or at different stages according to sac regression and renal function. Additional CTAs have been performed in case of sac growth at duplex ultrasound or concomitant comorbidities and in longer follow-up.
Collected data included patient demographics, aneurysm characteristics, and procedural details. Clinical examination and imaging were analyzed at periodical intervals. Midterm outcomes in terms of overall mortality and aortic-related mortality were reported at 6 months, 1 year and 2 years; sac regression was expressed in mm; and any reinterventions were reported. Target vessel instability was reported as any branch-related complication leading to aneurysm rupture, death, occlusion, component separation, or reintervention to maintain branch patency or to treat a branch-related component separation or endoleaks.
Statistical analysis was performed using descriptive methods to summarize patient characteristics and clinical outcomes. The Wilcoxon test was performed to compare sac diameter before and after FEVAR at midterm. The Kaplan-Meier curves were performed to report the estimated survival of patients at 6 months, 1 year, and 2 years. Microsoft Excel was used to perform statistical analysis; a p<0.05 and 0.01 were considered significant.
Results
A total of 42 consecutive patients undergoing FEVAR were included in this study (Table 1). Across these cases, 149 fenestrations were incorporated to accommodate target vessels. The majority of the devices were constructed with 2 (N=4; 10%), 3 (N=9; 21%), or 4 (N=27; 64%) fenestrations. In 1 case, the device was constructed with a single fenestration (2%) and 1 device contained 5 fenestrations (2%). Seven patients (17%) had undergone previous thoracic/endovascular aortic repair (T/EVAR) for aortic dissections or abdominal aortic aneurysms.
Baseline Characteristics of Study Participants.
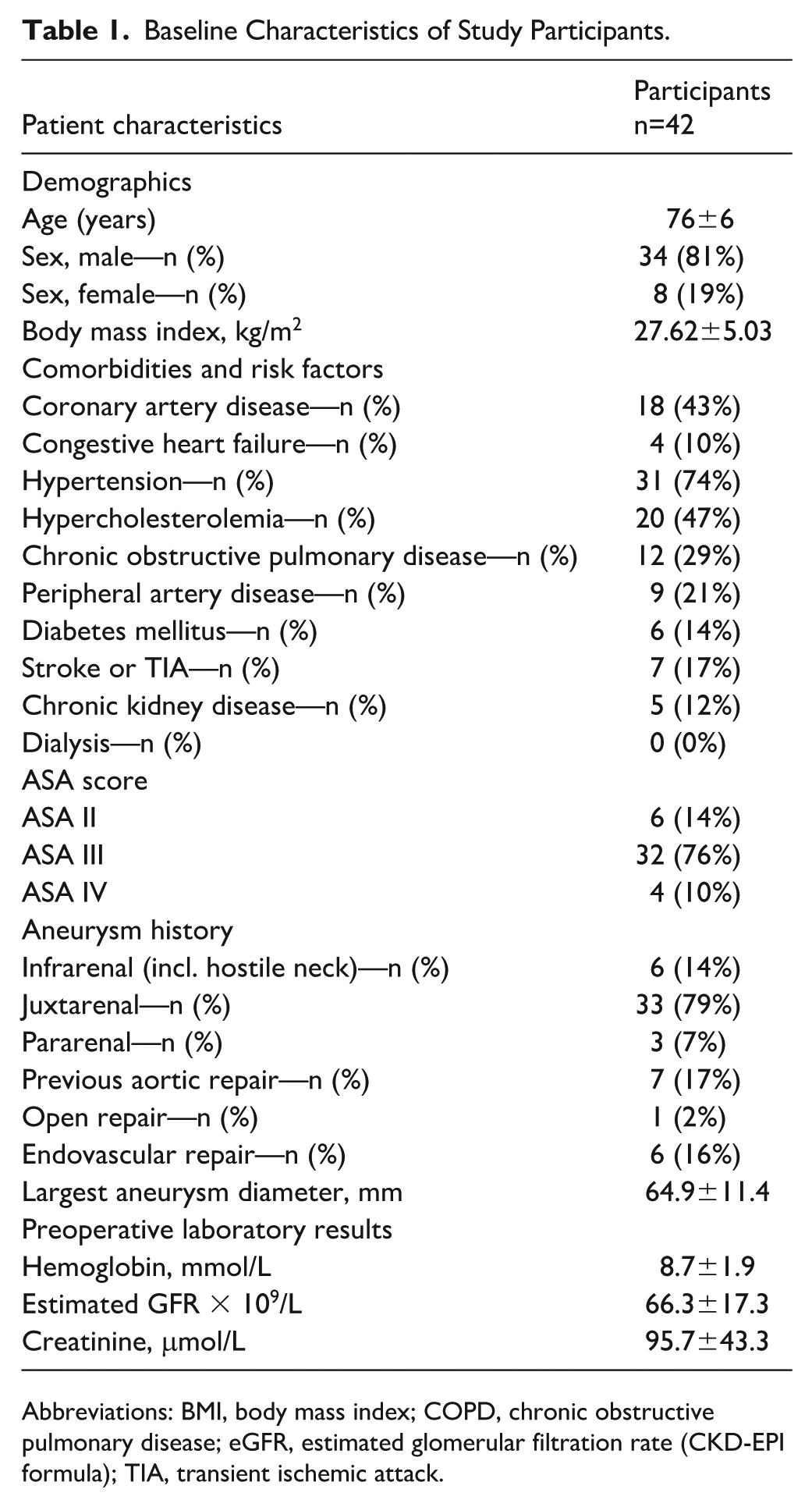
Abbreviations: BMI, body mass index; COPD, chronic obstructive pulmonary disease; eGFR, estimated glomerular filtration rate (CKD-EPI formula); TIA, transient ischemic attack.
Technical success was defined as successful endovascular implantation of the stent-graft with preservation of antegrade flow to the target vessels and absence of type 1 endoleak at the first postoperative CTA. Target vessel cannulation followed by placement of bridging stents was achieved in all but 1 vessel, yielding a technical success rate of 99.3%.
The Kaplan-Meier curve (Figure 1) estimates survival at 6 months, 1 year, and 2 years were 88.0%, 85.7%, and 81.2%, respectively. Importantly, no aortic-related mortality was observed during the follow-up period.
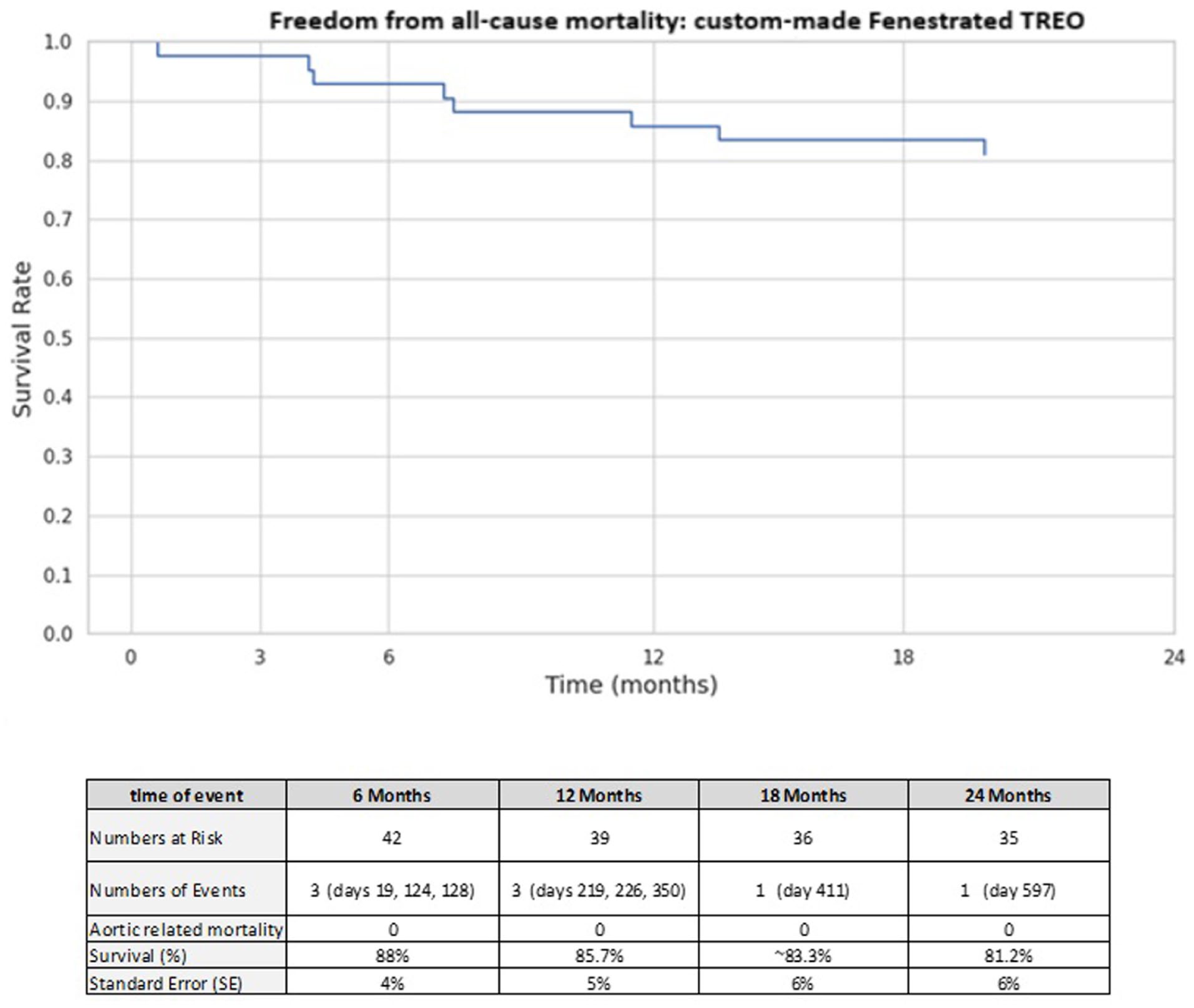
Estimated survival of patients managed with custom-made Fenestrated TREO endograft for juxtarenal and pararenal abdominal aortic aneurysms (AAAs). The estimated survival was 81.2% at 24 months (standard error [SE], 6%). No aortic-related mortality was reported among the 42 patients at 24 months.
The median follow-up duration was 12.9 months (0-29 months). The average preoperative AAA maximum diameter was 65±11 mm (N=42); however, 8 patients were excluded from the sac regression analysis, as 6 died within 1-year postprocedure due to non–aortic-related comorbidities. The other 2 patients died at 13.7 and 19.9 months, respectively. They both were found to have malignancies and had other clinical priorities (Figure 1).
The adjusted average preoperative AAA maximum diameter for these patients was 64±10 mm (n=34). At a median follow-up of 16.1 months (range=0-29 months), the average postoperative AAA maximum diameter had reduced to 60±15 mm (p=0.23) in this mortality-adjusted cohort (n=34).
To evaluate the effect of FEVAR on aneurysm diameter, we performed a Wilcoxon signed-rank test comparing preoperative and postoperative measurements for each patient (p=0.0172). During follow-up, sac regression was observed in 20/34 (59%) of patients. The average reduction in aneurysm sac diameter was 3.68 mm compared to the preoperative AAA maximum diameter, with 47% (16/34) of patients demonstrating sac shrinkage greater than 5 mm. Sac expansion ≥5 mm was found in 4/34 patients (12%) (Figure 2).
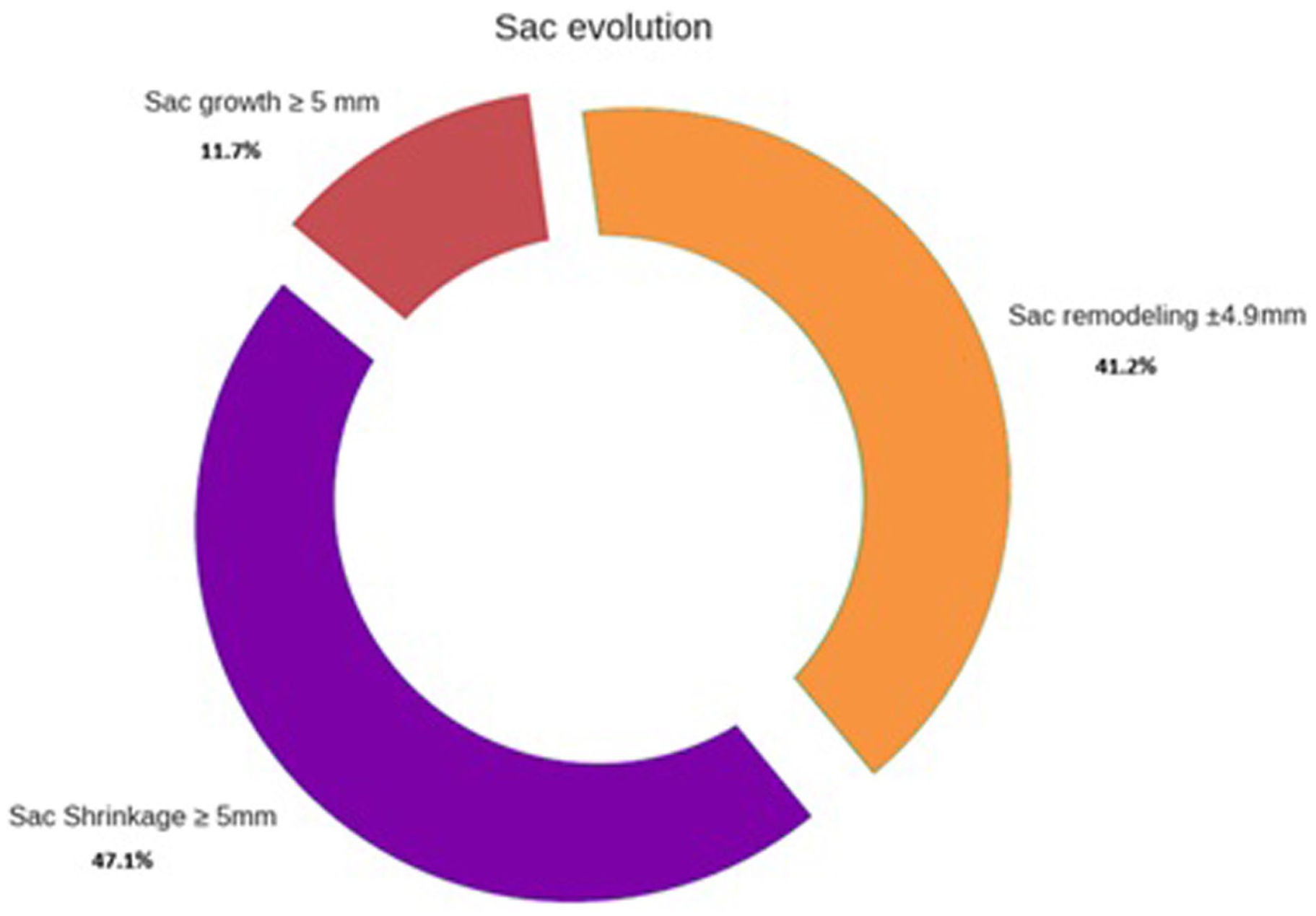
Analysis of AAA sac evolution at follow-up (median=12.9 months). Sac regression (shrinkage) ≥5 mm was found in 47% (16/34). Among the 53% (18/34) of patients that showed no sac regression or regression <5 mm, sac growth ≥5 mm was found in 4/34 patients (12%).
A total of 11 endoleaks have been reported at midterm follow-up (12.9 months [0-29 months]) (Table 2).
Midterm Outcomes of Patients Treated With the Fenestrated TREO Stent-Graft.
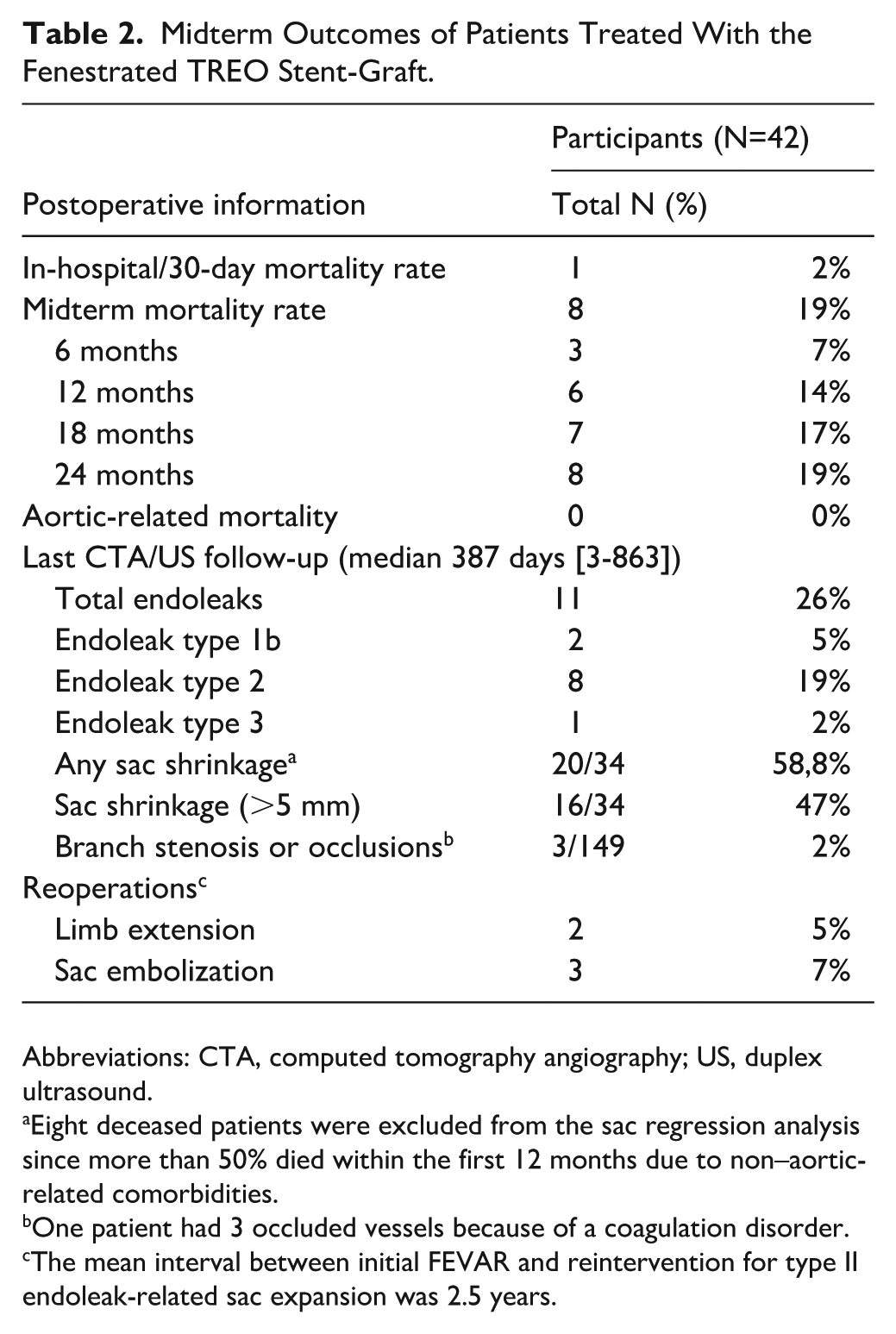
Abbreviations: CTA, computed tomography angiography; US, duplex ultrasound.
Eight deceased patients were excluded from the sac regression analysis since more than 50% died within the first 12 months due to non–aortic-related comorbidities.
One patient had 3 occluded vessels because of a coagulation disorder.
The mean interval between initial FEVAR and reintervention for type II endoleak-related sac expansion was 2.5 years.
Type Ib endoleak was identified in 2 patients (4.7%), both of whom were successfully treated with iliac limb extensions, including one with a custom-made fenestrated TREO limb with a fenestration for the internal iliac artery. In 1 case, type Ib endoleak was a consequence of the evolution of a high-pressure type II endoleak and subsequent sac expansion, with loss of distal sealing detected at 2-year control CTA.
One type IIIc endoleak was associated with the single perioperative failed cannulation case. However, due to technical difficulty related to the presence of a previous EVAR graft, advanced age and significant comorbidities, this patient was not considered a candidate for reintervention and is currently being monitored through serial ultrasound imaging.
Type II endoleaks originating from lumbar or inferior mesenteric arteries were present in 8 patients at midterm follow-up. Among these, 3 patients (7.1%) required secondary interventions with sac percutaneous embolization, due to progressive aneurysm sac enlargement. The mean interval between initial FEVAR and reintervention for type II endoleak-related sac expansion was 2.5 years.
Target vessel instability was found in 1 patient with a coagulation disorder, which was not diagnosed or known before the procedure. In this case, 3 out of 4 occluded target vessels were found, and the patient received successful thrombolysis without signs of a technical failure of the initial FEVAR.
Discussion
A larger number of patients have now been treated worldwide, since the TREO platform has emerged as a promising tool for AAA challenging cases.8,9 Our study supports these overall results, showing the midterm follow-up of the custom-made Fenestrated TREO Abdominal Stent-Graft System.
While OTS solutions represent a valuable option in urgent situations or in regions where custom-made grafts are not widely available, 10 custom-made fenestrated grafts offer a more anatomically precise reconstruction of each patients’ aortic anatomy.
In fact, custom-made devices are specifically designed based on individual patient measurements to achieve optimal implantation and minimize misalignment with target vessels. This precise fit is a key factor in their success and durability in elective cases. 11
On the contrary, OTS devices can be anatomically limited, as they are designed for common anatomies, not individual variations. Evidence shows that even with available designs, a significant number of patients may still require a custom-made device for proper fit. 12
Moreover, when implanted in last-generation hybrid rooms, the precision of custom-made grafts is designed to lead to reduced procedural time, radiation exposure, and contrast material volume compared to potentially more complex intraoperative manipulations required for OTS or PMEGs in challenging anatomies. 13
This study presents the updated midterm outcomes of FEVAR in a cohort of 42 consecutive patients operated in 4 high-volume centers across Europe. The incorporation of 149 fenestrations across devices—most commonly 3 or 4 per graft—reflects the complexity and customization required to accommodate visceral anatomy. Notably, 17% of patients had undergone prior T/EVAR, underscoring the challenging nature of this population.
Overall Mortality and Aortic-Related Mortality
Favorable survival rates were shown in Figure 1, showing the estimated survival of patients managed with custom-made Fenestrated TREO endograft for juxtarenal and pararenal AAAs in this cohort. The Kaplan-Meier survival estimates at 6 months (88.0%), 1 year (85.7%), and 2 years (81.2%) are consistent with previously reported outcomes in similar cohorts.14,15
No aortic-related mortality was reported among the 42 patients through 24 months. This is a strong indicator of the safety and durability of the FEVAR endograft.
Endoleaks, Sac Regression, Target Vessel Instability, and Reinterventions
Sac regression was defined as any decrease in sac diameter, expressed in millimeters (mm), compared to the AAA preoperative diameter. Sac regression analysis, adjusted for early non–aortic-related mortality (34 patients), revealed a statistically significant reduction in aneurysm diameter (Wilcoxon p=0.0172), with an average decrease of 3.68 mm. Sac shrinkage was observed in 58.8% of patients, and nearly half (47%) experienced a reduction greater than 5 mm—an encouraging indicator of aneurysm stabilization.
As previously stated, 17% of patients had undergone prior T/EVAR, underscoring the challenging nature of this population. Some literature now defines FEVAR for primary aortic repair and FEVAR for rescue of prior EVAR with loss of proximal seal as 2 distinct entities. A study by Sulzer et al found that there were high rates of sac expansion and a need for more secondary procedures in FEVAR after EVAR than in primary FEVAR patients, although this did not affect midterm survival.16–18
Larger investigations should be conducted to better assess the underlying process that drives aneurysm sac growth following successful FEVAR after EVAR.
Endoleaks were reported in 11/42 patients (26%), with a predominance of type II endoleaks (72.7%). Most type II endoleaks were managed conservatively; however, 3 patients required percutaneous embolization due to sac expansion, with a mean time to reintervention of 2.5 years. Type Ib endoleaks were identified in 2 patients (4.7%) and successfully treated with iliac limb extensions; one of those was consequent to a high-pressure type II endoleak, causing a distal seal loss detected at follow-up. This highlights the importance of long-term surveillance, as delayed sac enlargement may occur despite initial technical success.
In fact, type II endoleaks may probably not be as benign, as they were initially thought.19,20 A pre- or intra-operative embolization of lumbar arteries may increase sac regression and enhance longer reintervention-free FEVAR outcomes.
A single type IIIc endoleak was associated with the lone failed cannulation case. In this case, the patient had undergone FEVAR for type Ia endoleak following previous EVAR, and the impeachment to cannulation was caused by the presence of the previous free-flow stent at the level of the celiac trunk. The patient is now older, their general condition deteriorated during follow-up, and he informatively decided for conservative treatment, through strict follow-up. Informed consent is crucial in cases like this to plan the best risk-related customized solution.
One patient with a previously unknown coagulation disorder, presented target vessel instability with 3 out of 4 occluded target vessels, that were successfully treated with thrombolysis.
Overall, these findings affirm the effectiveness of FEVAR in achieving high technical success and favorable midterm outcomes, with sac regression occurring in a majority of patients. However, the persistence of endoleaks—particularly type II—remains a significant factor influencing long-term sac behavior and warrants continued monitoring. Future studies with longer follow-up and larger cohorts will be essential to further elucidate the durability of FEVAR and refine strategies for managing endoleak-related complications.
Limitations
The study is limited by its retrospective nature, resulting in a selecting bias and lacking enough numbers to perform solid sac regression and branch analysis in the follow-up. Furthermore, sac measurements were performed using both CTA and duplex ultrasonography, which might introduce small discrepancies in sac diameter assessment, although this is common in studies dealing with sac measurements, as it reflects routine clinical practice. Nevertheless, the midterm experiences and outcomes are promising.
Conclusion
The FEVAR with custom-made Fenestrated TREO Abdominal Stent-Graft demonstrates high technical success and favorable midterm survival rates in patients with complex aortic anatomy, including those with prior AAA repairs. The procedure is associated with meaningful sac regression in a substantial proportion of patients and low rates of aneurysm-related morbidity and mortality. While endoleaks, particularly type II, remain a concern, most could be manageable with secondary less-invasive interventions.
Longer follow-up and larger prospective studies are necessary to fully evaluate the long-term efficacy and durability of this approach.
Footnotes
ORCID iDs
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: TiGER (Terumo Aortic Global Endovascular Registry) ID NCT04246463.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KK Yeung, V Riambau, AWJ Hoksbergen, JA van Herwaarden, CEVB Hazenberg and G Pratesi are performing consultancy work for Terumo Aortic.