
Abstract
Objective:
Electrocautery septotomy has been proposed as an adjunctive technique during endovascular repair of aortic dissection with the aim of overcoming technical challenges associated with the presence of dual lumen.
Methods:
We retrospectively analyzed the outcomes of patients treated with electrocautery septotomy, at a single institution, between July 2023 and November 2024. Early outcomes included septotomy technical success, procedural technical success, 30-day mortality, and 30-day major adverse events. Late outcomes included overall survival, positive aortic remodeling, freedom from aortic-related reintervention, and freedom from target vessel instability.
Results:
Between July 2023 and November 2024, 15 consecutive patients were treated with electrocautery septotomy at a single center. The underlying disease was chronic dissection in 13 patients (86.6%), subacute residual aortic dissection in 1 patient (6.7%), and acute type B dissection in 1 patient (6.7%). The primary indication for treatment was a maximum aortic diameter ≥5.5 cm in 8 patients (53.3%) and urgent repair in 7 patients (46.7%) due to pain in 4 patients (26.6%), malperfusion in 2 patients (13.3%), and aortic rupture in 1 patient (6.7%). Septotomy technical success was obtained in all the patients (100%), with full expansion of the true lumen. No aortic lesions, target vessels occlusion, or distal embolization were reported. Procedural technical success was 86.7%. Peri-operative major adverse events occurred in 3 patients (20%), with 1 death (6.7%). During follow-up, 1 additional non-aorta-related death was registered, and 2 reinterventions were performed. Positive aortic remodeling was observed in 78.6% of patients.
Conclusions:
Electrocautery septotomy results in being valuable technique to address technical challenges in the endovascular treatment of postdissection thoracoabdominal aneurysms. Careful patient selection and tailored technical adjustments can further enhance the procedure success.
Clinical Impact
This study contributes to the growing body of evidence supporting electrocautery septotomy as a effective adjuntive technique during endovascular repair of post-dissection thoraco-abdominal aneurysm. However, it also underscores the limitations related to patient selection, highlighting the importance of careful pre-procedural evaluation to identify appropriate candidates and optimize clinical outcomes.
Keywords
Introduction
The aim of the endovascular treatment of aortic dissection is to cover the primary entry tear to promote the thrombosis of the false lumen, leaving the remaining aorta dissected. The natural history of the disease is the progressive dilatation of the aorta, with the occurrence of a postdissection thoracoabdominal aneurysm (PD-TAAA). 1
The most recent international guidelines suggested to treat PD-TAAA with a maximum diameter ≥5.5 cm, and the endovascular treatment should be considered not only in patients unfit for open surgery, but also in patients with low-to-moderate perioperative risk.2,3 Endovascular treatment of PD-TAAA presents 2 main differences compared with the treatment of degenerative aneurysm: peculiar technical challenges and the need to treat the false lumen to promote the complete thrombosis. The technical challenges are represented by narrow true lumen (TL), target vessels originating from both lumens, previous open/endovascular aortic repair and adequate proximal and distal landing zone. To promote the false lumen thrombosis various techniques have been proposed, such as the use of false lumen occluder or false lumen embolization. However, approximately a 30% reintervention rate has been reported, mainly associated with false lumen perfusion and aneurysm sac growth.4,5
Eletrocautery septotomy has been recently proposed to overcome all the technical challenges and to successfully treat the false lumen. 6
The aim of the study is to outline patient selection criteria and technical improvements based on the early outcomes of our experience.
Materials and Methods
Study Design and Patient Population
This was a retrospective study on consecutive patients treated, between July 2023 and November 2024, with electrocautery septotomy at a single-center institution. Follow-up data collection was completed in May 2025. Indications for treatment were aortic dissection with a diameter ≥5.5 cm, rupture, or symptoms. Preoperative anatomical evaluation included: maximal aortic diameter, maximal false lumen diameter, minimum TL diameter, extension of the dissection, false lumen thrombosis, target vessels patency, and target vessels origin from the true or false lumen. Formal consent for the procedure and for publication was obtained from each patient.
The STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) statement was followed. 7 The study complied with the declaration of Helsinki.
Preoperative Planning
Preoperative planning was performed with a dedicated 3D workstation (TeraRecon San Mateo, California). Both the arterial and venous phases of the computed tomography angiography (CTA) scan were evaluated.
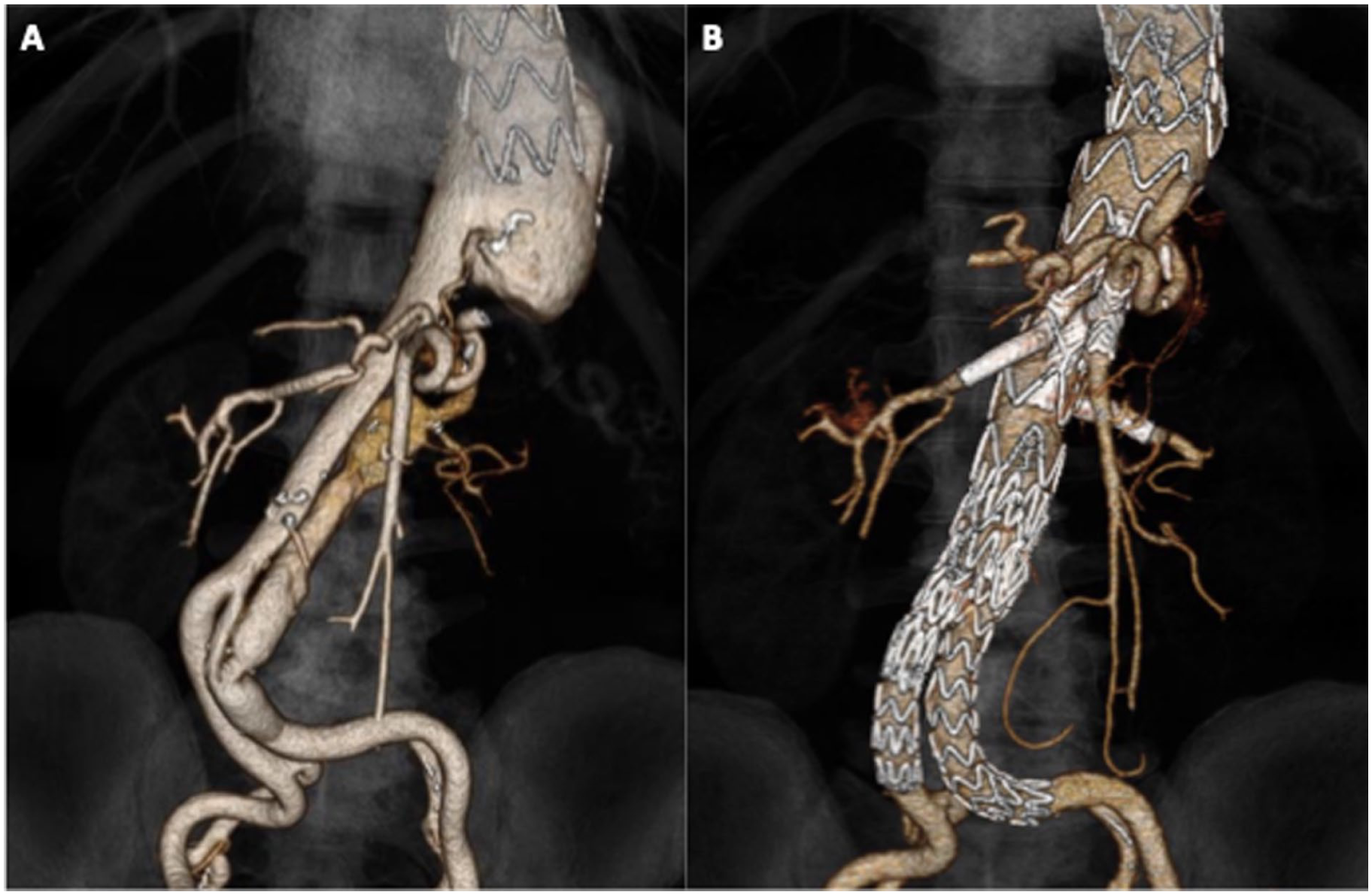
Extension of the septotomy was planned according to the extension of the dissection and the intended endovascular repair. The aim of the septotomy was optimization of the distal landing zone above the celiac trunk (CT), expansion of the TL to allow endograft deployment, and restoration of the origin of target vessel from the TL. In the first case, in patients with a descending thoracic aneurysm, the septotomy was associated with a thoracic endovascular aneurysm repair (TEVAR). The extension of the septotomy always included the visceral aorta to allow the remodeling and to prevent future expansion of the remaining dissected aorta (Figure 1). In the other cases, in patient with a dilatation of the visceral aorta, the septotomy was associated with a branched endovascular aneurysm repair (BEVAR) with or without proximal and/or distal components.
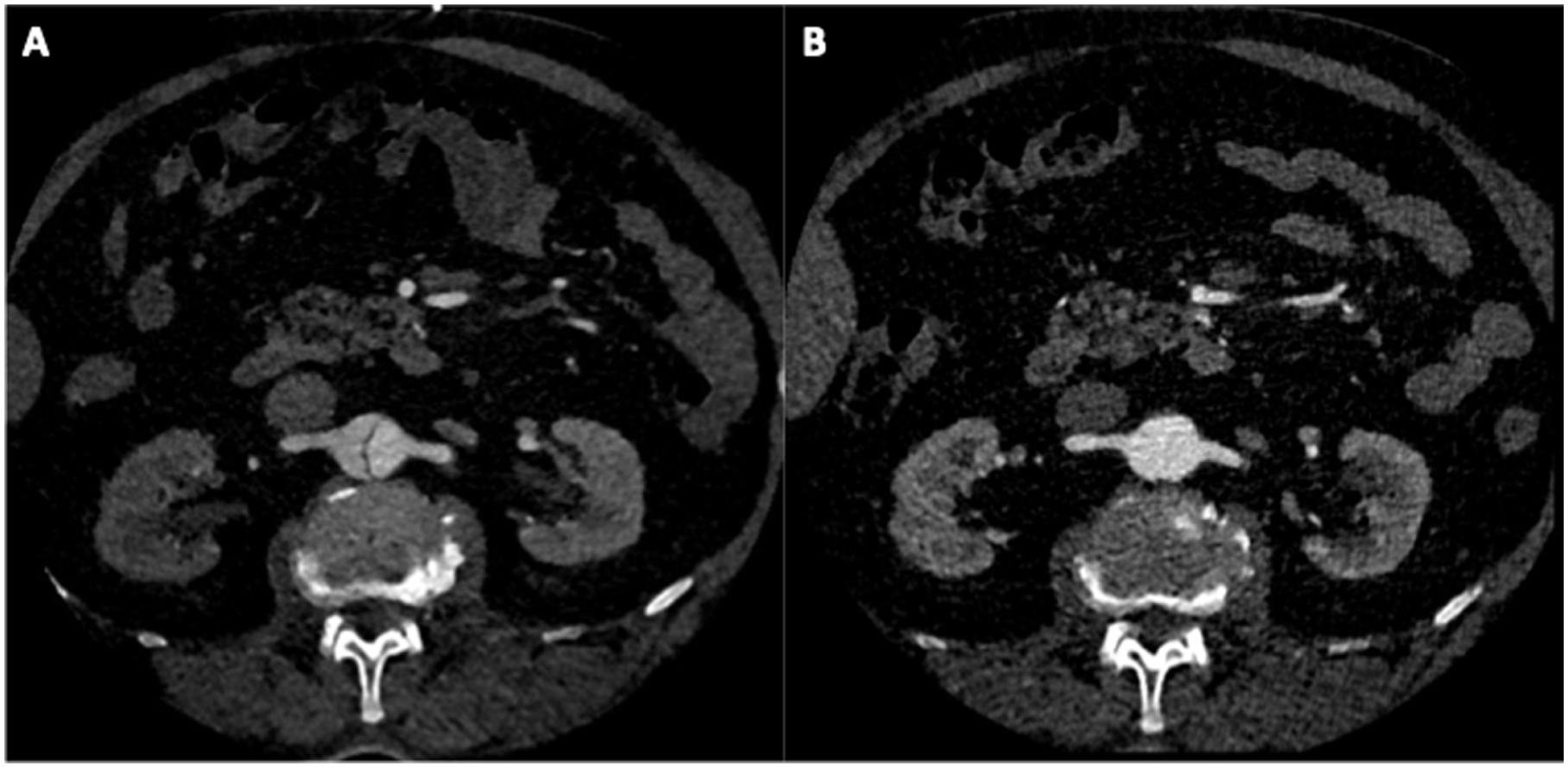
Electrocautery septotomy for optimization of the distal landing zone during thoracic endovascular aneurysm repair (TEVAR). (A) Preoperative computed tomography angiography (CTA) scan showing the presence of 2 lumens at the level of the renal arteries. (B) Computed tomography angiography (CTA) scan at 1 year after electrocautery septotomy shows the presence of a single lumen with complete aortic remodeling and both renal arteries arising from the true lumen.
Technique
Electrocautery septotomy technique consists of the cannulation of the TL and false lumen. According to planned extension of the septotomy, cannulation of both lumens can be performed from the 2 different access if it is planned to treat only the aorta or from the same femoral access for septotomy involving the iliac artery. The guidewire is then snared across the septum using a natural tear or by fenestrating the lamella with the electrocautery guidewire. For lamella fenestration, the use of steerable sheath is recommended, as well as to fenestrate from the narrow lumen to the larger. Intravascular ultrasound (IVUS) in used to confirm the correct location of the through-and-through wire. A 125 cm catheter is advanced over the through-and-through guidewire, which is then removed. A modified Astato XS 20 0.014-inch 300 cm wire (Asahi Intecc USA, Santa Ana, California) is used to perform the septotomy. The modification consists of kinking the guidewire in its middle part and removing the coating from the inner curvature with a scalpel. On both sides of the guidewire, a 5F sheath, flushed with 5% dextrose to reduce the blood coagulation, is advanced.
The cautery is then connected to the uncoated distal extremity of the wire, and the cut button is pressed. Electrocautery power should be between 40 and 80 Watt, according to the device. The wire is pulled down gently to perform the septotomy (Figure 2). Before performing the septotomy, the full isolation of the wire should be checked, all wet surfaces should be removed, and gloves should be changed.
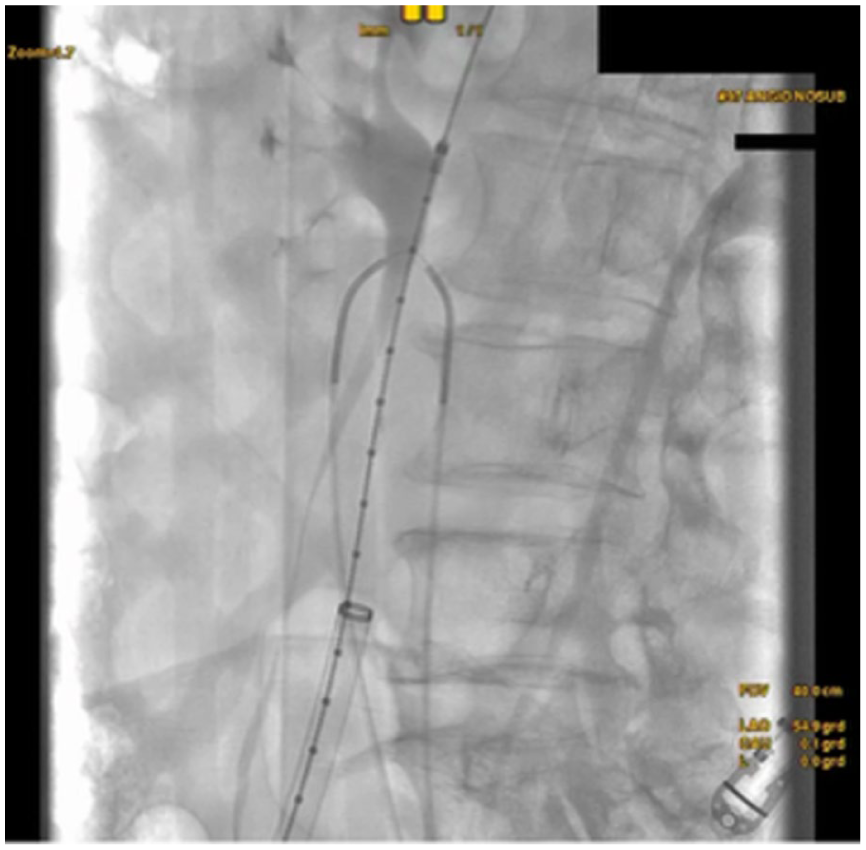
Intraoperative details. Modified Astato guidewire (Asahi Intecc USA, Santa Ana, California) in place across the septum.
Outcomes
Early outcomes that have been evaluated include septotomy technical success, procedural technical success, 30-day mortality, and 30-day major adverse events.
Septotomy technical success was defined as a successful septotomy without evidence of vascular injury, loss of patency in target vessels, and embolization (including lamella fenestration if required). Procedural technical success was defined as a composite of successful septotomy and the successful introduction and deployment of all intended devices, including proximal and distal sealing, full expansion of the devices, and target vessel preservation. Thirty-day outcomes are reported as defined by the Society for Vascular Surgery (SVS) reporting standards for endovascular aortic repair of aneurysms involving the renal-mesenteric arteries. 8
Late outcomes consist of overall survival, positive aortic remodeling, freedom from aortic-related reintervention, and freedom from target vessels instability. Positive aortic remodeling was reported as defined by the SVS reporting standards for type B aortic dissection in the presence of at least one of the following: false lumen reduction in maximal diameter or volume and no growth in total aortic diameter or volume; TL expansion in maximal diameter or volume and no growth in total aortic diameter or volume; and total aortic maximal diameter reduction with variable changes in TL and false lumen diameters. 9
Cone-beam computed tomography (CBCT) scan was performed at the end of the procedure. During follow-up, computed tomography (CT) scan was performed at 1 month, 6 months, 1 year, and yearly thereafter.
Statistical Analysis
All statistical analyses were conducted utilizing R (version 4.0.2, R Foundation for Statistical Computing, Vienna, Austria). The presentation of data was tailored to the nature of the variables. For normally-distributed data, the mean and standard deviation (SD) were provided, while non-normally distributed data were presented through their median (IQR) (interquartile range). The Kaplan-Meier method was used to assess survival and freedom from reintervention. A significance level of p<0.05 was employed to determine the statistical significance.
Results
Patient’s Cohort
Between July 2023 and November 2024, 15 consecutive patients were treated with electrocautery septotomy at a single center. The underlying disease was chronic dissection in 13 patients (86.6%), subacute residual aortic dissection in 1 patient (6.7%), and acute type B dissection in 1 patient (6.7%). Dissection characteristics are reported in Table 1.
Dissection Characteristics.
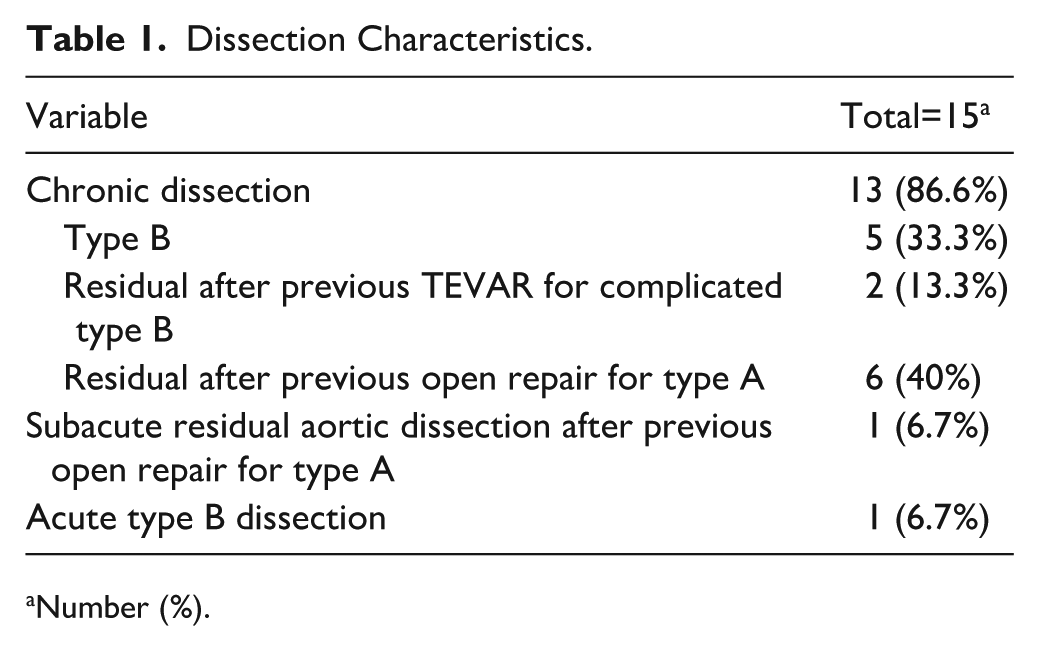
Number (%).
The primary indication for treatment was a maximum aortic diameter ≥5.5 cm in 8 patients (53.3%) and urgent repair in 7 patients (46.7%) due to pain in 4 patients (26.6%), malperfusion in 2 patients (13.3%), and aortic rupture in 1 patient (6.7%).
In the same time period, a total of 45 patients were treated endovascularly for aortic dissection: 16 in the chronic phase and 29 in the acute/subacute phase.
Male patients were 86.7% of the considered sample, and the mean age was 63±9 years.
Demographic characteristics and comorbidities are listed in Table 2.
Demographic Characteristics and Comorbidities.
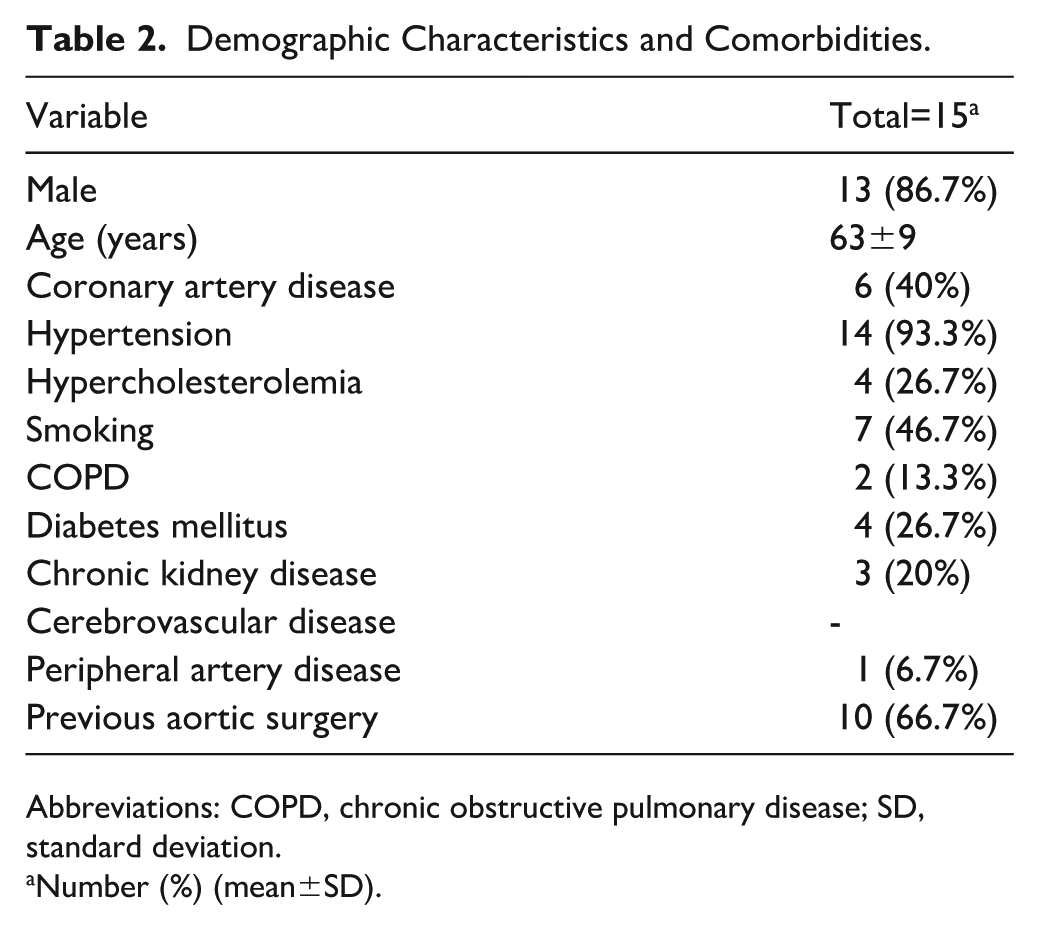
Abbreviations: COPD, chronic obstructive pulmonary disease; SD, standard deviation.
Number (%) (mean±SD).
Previous open or endovascular treatments were reported in 10 patients (66.7%). Mean time between the first procedure and reintervention was 89.3±78.8 months. Previous surgeries are reported in Table 3.
Previous Surgeries.
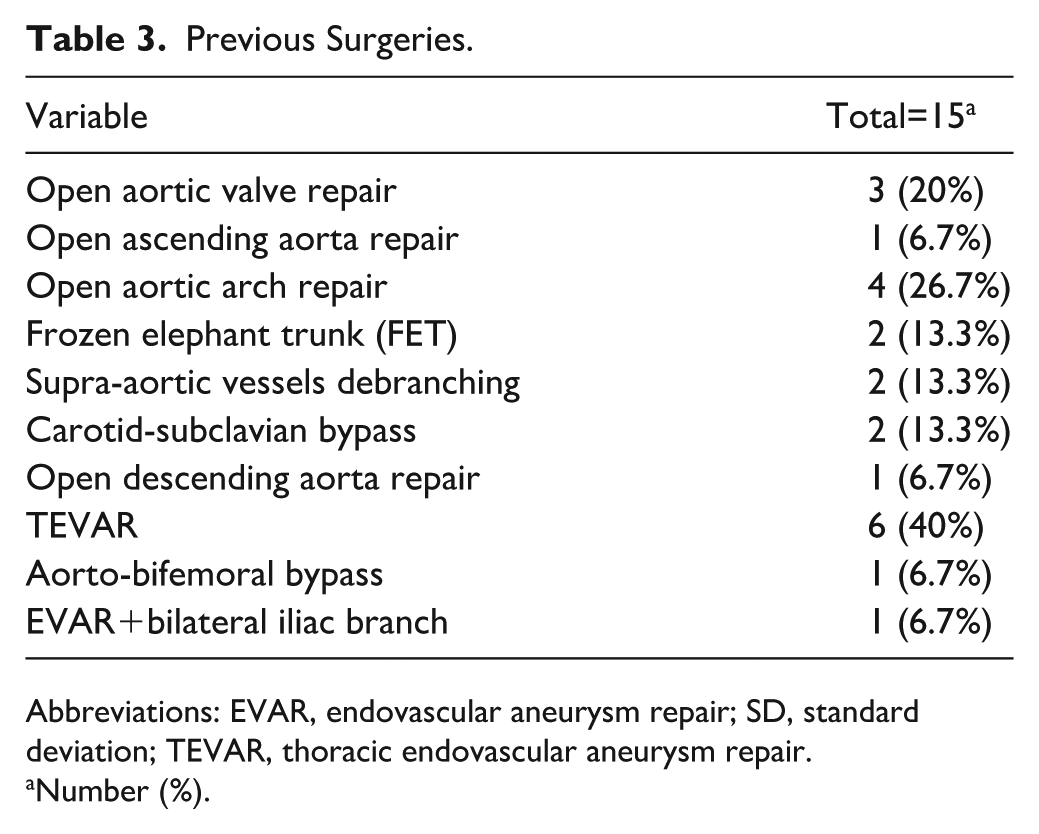
Abbreviations: EVAR, endovascular aneurysm repair; SD, standard deviation; TEVAR, thoracic endovascular aneurysm repair.
Number (%).
The mean aortic diameter was 59.0±12.3 mm, with a maximum false lumen diameter of 37.2±9.3 mm and a minimum TL diameter of 9.0 mm (8.0, 10.0). The minimum TL diameter was at the level of the visceral aorta in all the patients. Extension of the dissections is summarized in Table 4. Both the brachiocephalic trunk (BCT) and the left common carotid artery (LCCA) were patent and not dissected; 5 were involved in previous open arch repair.
Anatomical Characteristics and Procedure Details.
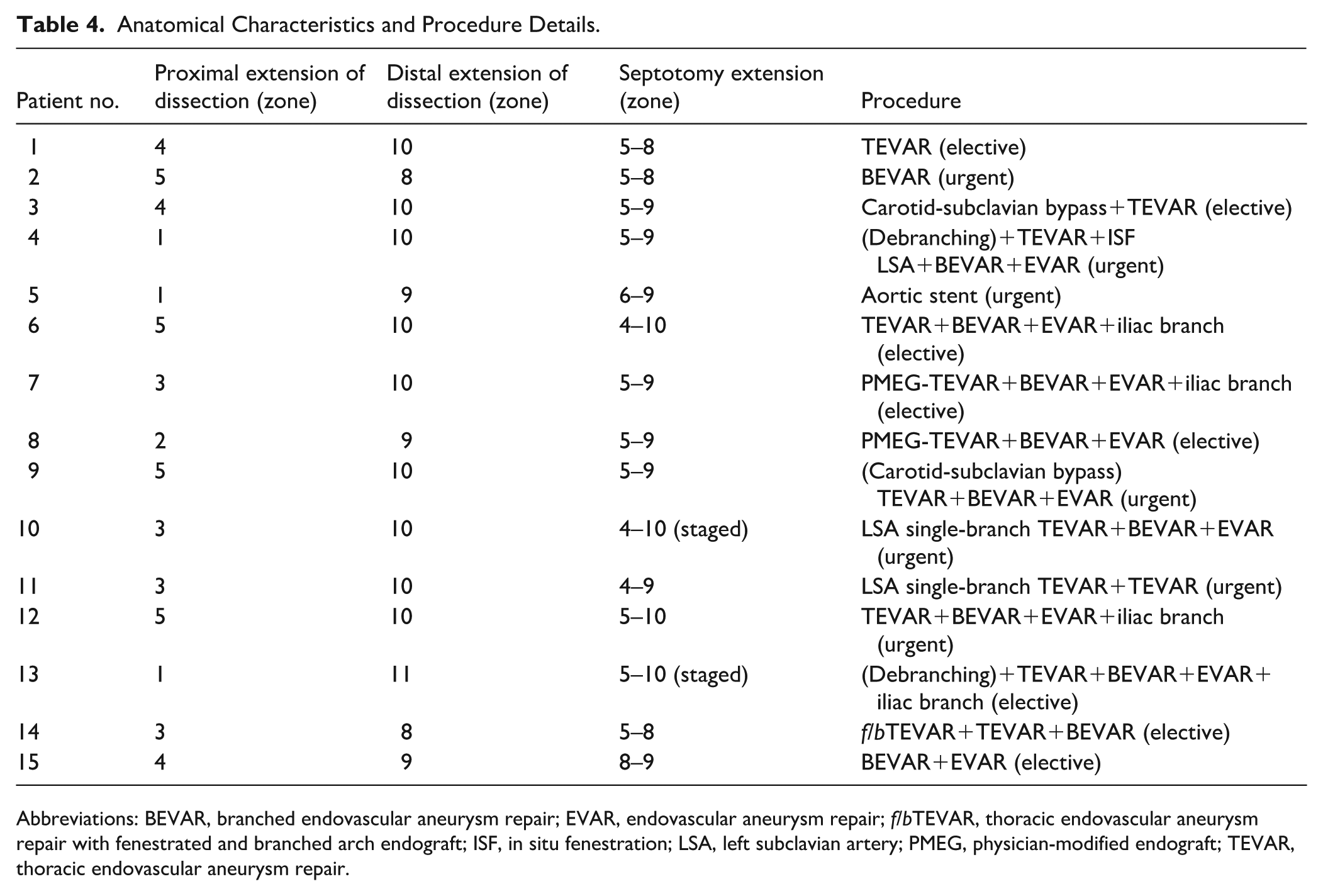
Abbreviations: BEVAR, branched endovascular aneurysm repair; EVAR, endovascular aneurysm repair; f/bTEVAR, thoracic endovascular aneurysm repair with fenestrated and branched arch endograft; ISF, in situ fenestration; LSA, left subclavian artery; PMEG, physician-modified endograft; TEVAR, thoracic endovascular aneurysm repair.
All the left subclavian arteries (LSAs) were patent and not dissected; 4 were involved in previous open arch repair and 2 were revascularized through a left carotid-subclavian bypass.
The CTs were patent and not dissected in 13 patients; 7 originated from the TL, 3 from the false lumen, and 3 from both. All the superior mesenteric arteries (SMAs) were patent, not dissected and originated from the TL, except for 2 (1 from the false lumen and 1 from both lumens). One patient had a common origin of the CT and SMA arising from the TL.
All the renal arteries were patent and not dissected: 10 right renal arteries (RRAs) originated from the TL and 5 from the false lumen; 6 left renal arteries (LRAs) originated from the TL, 8 from the false lumen, and 1 from both.
A native tear of the lamella at the intended proximal beginning of the septotomy was present in 7 patients. In all the other cases, fenestration was obtained using an electrified guidewire. Extension of the septotomies is summarized in Table 4. In all the cases, the septotomy included the visceral aorta. Septotomy was intended for distal landing zone optimization in 3 patients (1, 3, and 11). Also in these patients, the septotomy was extended to the visceral and infrarenal aorta to promote the aorta remodeling and preventing future enlargement. In 1 patient, treated in the subacute phase for malperfusion, an aortic stent was placed.
In all the other patients, a BEVAR with distal bifurcated endograft was performed. Four patients received an additional iliac branch. In 2 cases, a staged septotomy was created according to the extension of the repair planned in each stage.
A total of 50 target vessels were included in the repairs: 7 LSAs, 10 CTs, 11 SMAs, 11 RRAs, and 11 LRAs. Endovascular aortic repairs are summarized in Table 4.
Intraoperative Details
Septotomy technical success was obtained in all the patients (100%), with full expansion of the TL. No aortic lesion, target vessel occlusion, or distal embolization was reported. The procedural technical success was 86.7%; this was due to the occlusion of one LRA after the deployment of the branched endograft and the partial occlusion of both renal arteries after aortic stent-graft placement, resulting from dislodgment of the residual lamella in a patient treated in the subacute phase. In the first case, the intended branch was plugged, and the artery was successfully revascularized with endograft and lamella electrosurgical in situ fenestration. 10 In the second case, a bilateral renal artery stenting was performed. All the intended target vessels were successfully stented and remained patent at the end of the procedure. No type I/III endoleak was observed on completion angiography, except for staged interventions. As additional procedure, one inferior mesenteric artery was plugged. Intravascular ultrasound was used in all patients at the beginning of the procedure to confirm the correct positioning of the guidewires in the TL and false lumen, and again after the septotomy to confirm the technical success. Changes in TL area and diameter measured with IVUS at the level of the TL maximum compression are summarized in Table 5 (Figure 3).
Changes in True Lumen Diameter and Area Measured With IVUS and on CT Scan.

Mean±SD, median (IQR).
Abbreviations: CT, computed tomography; IVUS, intravascular ultrasound; TL, true lumen.
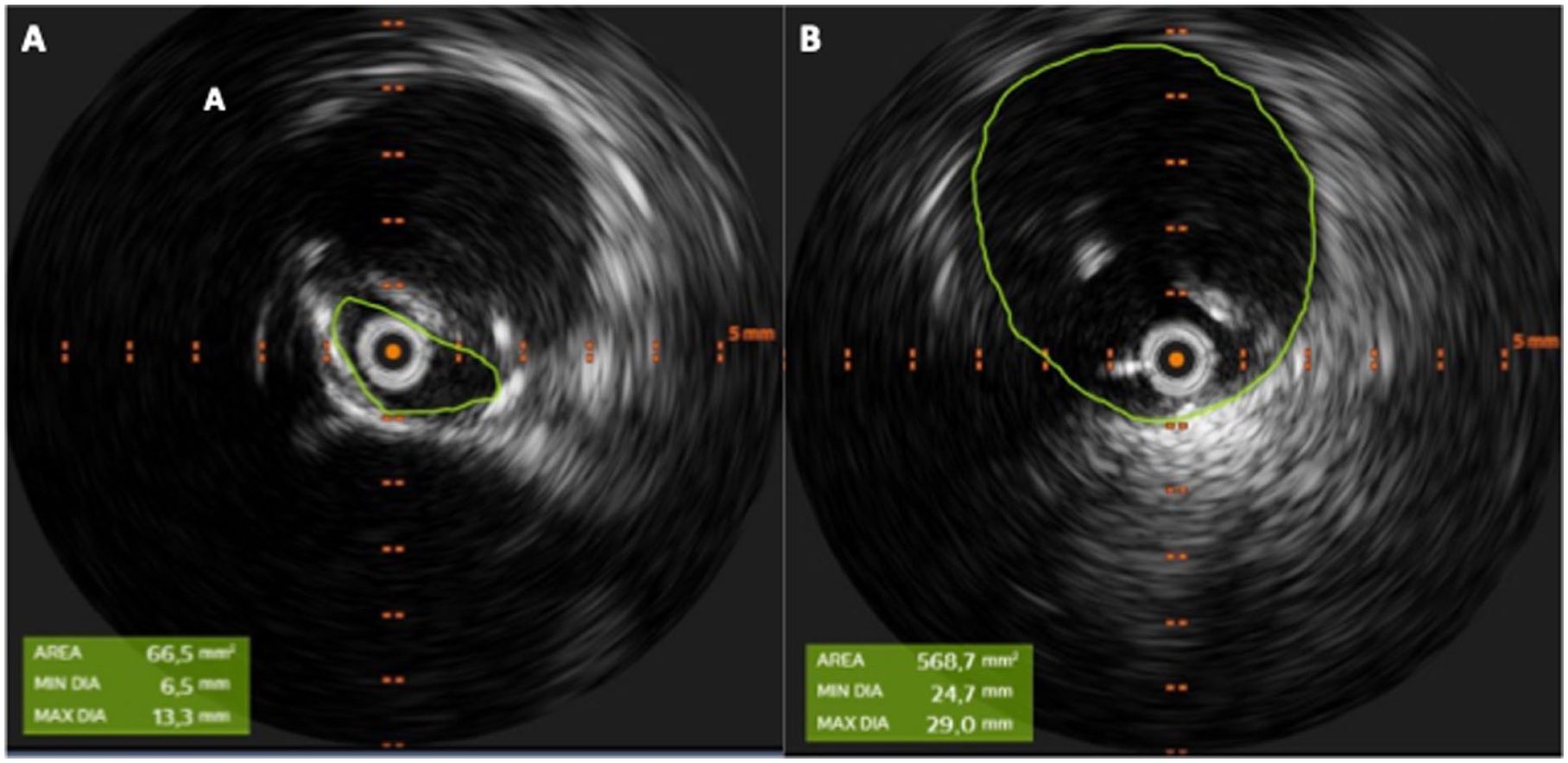
Changes in true lumen (TL) area and diameter measured with intravascular ultrasound (IVUS) at the level of the TL maximum compression.
Cone-beam scan without contrast was obtained in all patients with supra-aortic or visceral vessel stents, and confirmed full endograft expansion in the absence of bridging stent kinking.
The mean operative time for the main procedure was 351.08±146.29 minutes, and the mean fluoroscopy time was 138.1±57.71 minutes, with a mean contrast volume of 275±152.34 ml.
To reduce spinal cord ischemia risk, 2 patients received prophylactic cerebrospinal fluid (CSF) drainage, and 8 repairs were staged.
Thirty-Day Outcomes
During postoperative course, 3 acute kidney injury occurred, in patients with severe chronic kidney disease, 2 of which required dialysis. Two pulmonary failures were reported, leading to the death of 1 patient. This patient also experienced grade 3 spinal cord ischemia, with no improvement after CSF positioning. The same patient, treated in urgent setting, was at high risk for spinal cord ischemia, but due to anticoagulant therapy, CSF was not placed prophylactically.
At the 30-day CT scan, no complications were reported; there were no type Ia/III endoleaks, and only 1 type II endoleak was observed. At 30 days, 2 reinterventions were performed: an iliac limb extension due to a type Ib endoleak and mechanical thromboaspiration of a renal artery stent due to partial thrombosis in the patient treated with the aortic stent graft. Full expansion of the TL was observed in all patients.
Follow-Up Outcomes
Mean follow-up was 8.83 ±5.12 months. One additional death occurred at 3 months due to pulmonary insufficiency. During follow-up, 2 reinterventions were performed to address type II endoleaks, which were observed in 40% of patients. No target vessel instability was reported. Positive aortic remodeling was observed in 78.6% of the patients. The survival probability rate was 86% at 12 months (standard error [SE]=0.1). Freedom from reintervention rate was 77% at 12 months (SE=0.14). Kaplan-Maier analysis for the survival probability and freedom from reintervention are reported in Figure 4.
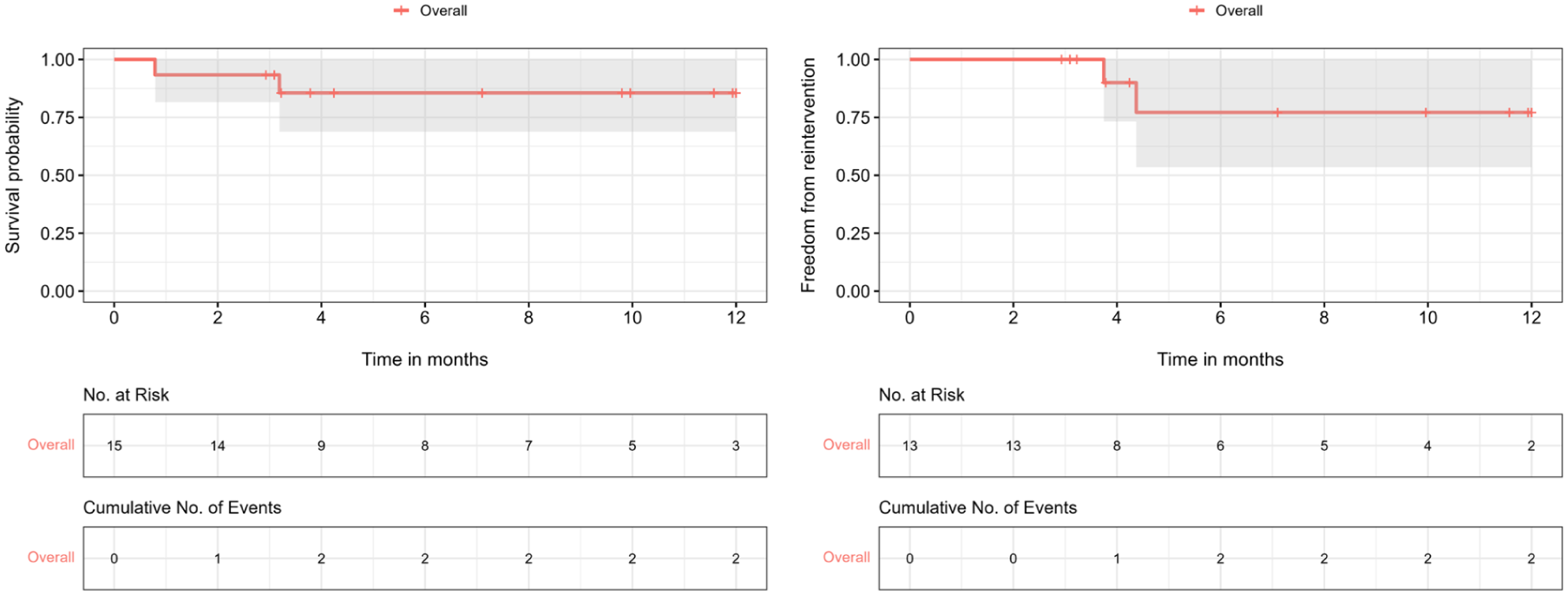
Follow-up outcomes: Kaplan-Maier analysis for survival probability and Kaplan-Maier analysis for freedom from reintervention.
Discussion
Endovascular treatment of PD-TAAA has been demonstrated to be safe and effective, with similar outcomes compare to degenerative aneurysm.11–13 The technical success rate is reported to be around 94.3%, and the main reasons for not achieving technical success are target vessel catheterization failure and type I to III endoleaks. 14 Specific technical challenges remain, increasing the complexity of these repairs: a narrow TL, target vessels originating from both lumens, previous open/endovascular aortic repairs, and the need for adequate proximal and distal landing zones, which often lead to extensive aortic coverage. In addition, in this group of patients, freedom from secondary intervention rate is reported 55% at 2 years and 44% at 5 years.15,16
To overcome both technical challenges and improve outcomes during follow-up, electrocautery septotomy has been proposed. The technique has been described to create a proximal or distal landing zone in a dissected segment and in association with BEVAR, even in cases of aortic rupture.17,18
The largest published experience consists of 36 patients, with a 92% technical success rate, a significant increase in the aortic lumen diameter, and a 36% secondary intervention rate. 19
In our study, we obtain comparable outcomes with septotomy technical success in all the patients and 86.7% of procedural technical success. No case of aortic injury and distal embolization occurred. Positive aortic remodeling was observed in all the patients.
To improve the outcomes of this technique, patient selection is crucial. We discourage the application of septotomy in the following cases: false lumen thrombosis due to the risk of embolization; acute and subacute dissection due to the crumbly consistency of the lamella; and a calcified septum, which may lead to cut failure. Accurate evaluation of the preoperative CT scan, including the venous phase, is mandatory to determine the technical feasibility.
In the majority of patients who underwent previous TEVAR, there is a need to obtain a fenestration of the lamella. To reduce the risk of aortic injury, lamella’s fenestration should be performed from the smaller to the larger lumen, regardless of whether it is the true or false lumen. In this scenario, the use of the 3D fusion model and the preoperative CT scan helps in understanding the relation between the 2 lumens. Another tool to safely perform electrocautery fenestration is the steerable catheter.
A point of debate is the management of dissected vessels. Bail-out strategies may include the position of a guidewire inside the vessels, or prestenting.
An interesting application of this technique is the optimization of the dissected landing zone. In this perspective, septotomy allows to reduce the extension of the endovascular repair. In our approach, we extend the septotomy into the visceral aorta to prevent further enlargement and improve the aortic remodeling.
On the contrary, we discourage, in case of staged procedure, to perform septotomy in an enlarged aorta without concomitant endovascular repair. In case of extensive aortic coverage and staged repair, we proceed with septotomy staging according to the planned endovascular repair.
When the endovascular repair includes the visceral aorta, our preference is the implantation of an off-the-shelf outer-branch endograft. In cases of short-length septotomy with persistent TL compression, a viable alternative is the use of a custom-made, inner-branch endograft20,21 (Figure 5). For the design of a custom-made endograft, attention should be paid to the changes that occur in aortic diameter; preoperative planning should be performed along the real center-lumen line, without considering the TL and false lumen.
Preoperative and postoperative computed tomography angiography (CTA) of a patient treated with electrocautery septotomy extending from zone 8 to 9 and custom-made endograft with inner branches.
The last potential critical part is the extension of the septotomy into the iliac arteries due to the reduction of the diameter, and the increased risk of arterial injury. In this situation, adopting a V-shaped modified Astato guidewire, rather than a trapezoidal shape, reduces the risk of contact with the arterial wall and subsequent rupture. As a bail-out strategy, it is useful to place a stiff guidewire in parallel to maintain a safe pathway to the TL in case of aortic wall rupture. In addition, in the case of septotomy extending into the iliac access, the use of a short 11 Fr sheath is preferred over a longer 33-cm sheath. In this case, the modified Astato guidewire can be insulated using 65 cm 4 Fr catheters.
Our study, despite confirming the feasibility of this technique and expanding the applicability, presents some limitations, mainly represented by the small number of patients and the short follow-up.
Conclusions
Electrocautery septotomy is an effective technique to overcome technical challenges associated with endovascular treatment of PD-TAAA. Specific technical adjustment and patient selection may increase technical success. Our preliminary results should be confirmed in future larger studies and longer follow-up.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.