
Abstract
Background & objectives:
Chronic limb-threatening ischaemia (CLTI) not amenable to conventional revascularization options (no-option CLTI) is associated with high rates of major amputation and mortality. Promising results were reported following percutaneous deep venous arterialization (pDVA) using the LimFlow system. This study reports mid-to-long-term clinical and patency outcomes of pDVA in real-life single-centre settings.
Design:
Retrospective, single-arm cohort study.
Methods:
The study included patients with no-option CLTI (Rutherford classes 5 and 6) who underwent pDVA using the LimFlow between January 2020 and June 2024. Patients were designated “no-option” by a multidisciplinary team after exhausting conventional revascularization options. Primary outcome was amputation-free survival (AFS). Secondary outcomes included technical success, limb salvage (LS), primary and secondary patency (PP/SP), freedom from reintervention (FFR) and wound healing rates.
Results:
Thirty-four patients (median age of 67 years; 79.4% diabetic) were included, with a median follow-up of 21 months (4–62 months). Technical success was 100%. At 24 months, AFS was 72% and LS was 88.6%. Full wound healing was achieved in 66% of patients, with a median time of 262 days from the index procedure. Kaplan-Meier analysis showed 24-month PP and SP rates of 46.3% and 76%, respectively. Freedom from reintervention was 58% at 24 months. Four major amputations (11.7%) were required.
Conclusion:
Percutaneous deep venous arterialization using the LimFlow system provides acceptable mid-term outcomes. Satisfactory AFS, LS, PP, SP and wound healing rates were achieved in these no-option CLTI options. Strict post-procedure surveillance and reintervention protocols are essential to maintain satisfactory outcomes.
Clinical Impact
The LimFlow system introduces a novel option for patients with no revascularization alternatives. It enables limb salvage in severe CLTI cases previously destined for amputation. By creating arterial flow through the venous system, it redefines vascular intervention strategies. Clinicians gain a new tool for “no-option” patients, expanding treatment eligibility. This may reduce major amputation rates and improve quality of life. The approach requires new technical skills and multidisciplinary collaboration. It shifts practice toward advanced endovascular innovation rather than palliative care. Patient selection and procedural expertise become critical for success. The study highlights the feasibility and safety of transcatheter arterialization. Overall, it represents a paradigm shift in managing advanced peripheral artery disease.
Keywords
Introduction
Chronic limb-threatening ischaemia (CLTI) is associated with increased burden on health and social care services. Best medical therapy with risk factors control is frequently insufficient, and revascularization is often required. 1 Without revascularization, patients with CLTI are likely to end up with major amputation, which is associated with overall mortality of 50% within 2 years. 2
Although revascularization techniques, both open and endovascular, have evolved significantly in recent years, around 20% of patients with CLTI may still be considered as “no-option CLTI.” These are patients who are deemed unsuitable or not candidates for available revascularization options, either by surgical or endovascular techniques, such as those with no distal target vessel or no available vein conduit. 3 This group of “no-option” patients are reportedly associated with very poor outcomes, including up to 40% major amputation rates and 20% mortality rates at 6 months. 4
Percutaneous deep venous arterialization (pDVA) was introduced, initially with off-the-shelf devices, to allow arterialization of the deep veins of the foot in an attempt to save the limbs in patients with no-option CLTI. 5 It has been suggested that the complete flow reversal in veno-capillary circulation not only provides nutritive oxygen delivery, but also triggers angiogenesis. 6
The LimFlow system, which obtained European Conformity (CE) marking in October 2016, is a purpose-built system, which was developed in an attempt to standardize the procedural steps during pDVA. The PROMISE I early feasibility study was initiated in the United States in 2017. 7 This was later supported by the results from PROMISE II and PROMISE UK. However, outcomes beyond 12 months have not yet been widely reported in real-life settings. In this study, we present the clinical outcomes of pDVA in patients with no-option CLTI using the LimFlow system in real-life setting in a tertiary vascular centre.
Methods
This is a single-arm, retrospective cohort study designed to evaluate the outcome of using the LimFlow system in treatment of patients with no-option CLTI. Consecutive patients who underwent pDVA using the LimFlow system in our centre were included in this study. Patients were classified as “no-option CLTI patients” after a thorough assessment and agreement by the multidisciplinary team (MDT) having been satisfied that the available conventional revascularization options (open and/or endovascular) have all been exhausted.
Percutaneous deep venous arterialization was only considered in patients presenting with Rutherford classes 5 and 6 (with tissue loss including unhealed ulcer and/or tissue necrosis) with or without rest pain. All patients had previous failed conventional endovascular revascularization attempts. Patients with no distal target pedal artery for bypass or those who did not have any suitable veins were also included in the study. While patients were classified using the Ferraresi SAD-MAC computed score into 12 patients with moderate scoring and 15 patients with severe scoring, the scoring system was not a part of surgical decision.
The primary outcome was amputation-free survival (AFS) rate. The secondary outcomes; included technical success, patency of the pDVA (both primary and secondary – PP/SP), freedom from reintervention (FFR), limb salvage (LS) rate and wound healing. These were defined as per the Society of Vascular Surgery guidelines. 8
Patients who had a valid conventional revascularization option, those with foot sepsis not controllable with antibiotics, those who presented with acute limb ischaemia and patients with life expectancy less than 1 year were not considered suitable candidates for pDVA.
Procedural Protocol
Pre-procedure assessment
Eligibility criteria
I. Imaging Criteria:
–Patients were considered for pDVA when angiogram showed evidence of “desert foot”, defined as absence of patent named artery crossing the ankle into the foot. The arterial inflow down to the popliteal trifurcation should be optimized as needed. One of the tibial arteries, usually the posterior tibial artery (PTA), is selected as the inflow for the pDVA. Ideally, this inflow artery should not be the sole supply of collaterals to the foot, to avoid worsening foot ischaemia after the creation of the pDVA due to arterial steal phenomenon. Collateral supply to the foot should be preserved to maintain foot perfusion during the pDVA maturation phase.
–Foot and leg deep venous mapping: All patients underwent duplex ultrasound assessment (DUS) of their foot and leg venous system, to confirm patency and diameter of the lateral planter vein (LPV), and the remaining deep and superficial veins, including the posterior tibial vein (PTV). Lateral planter vein diameters below 2.5 mm were considered unfavourable for pDVA, Vein diameters were obtained as part of the detailed preoperative venous mapping duplex scan under resting condition. In borderline diameters, a conventional venogram while using tourniquet was performed to assess the suitability of the foot deep venous system for pDVA. This was performed in 2 cases. Of note, intraoperative foot vein cannulation was performed after inflation of mid-leg tourniquet to a pressure of 100 mm Hg.
All patients underwent a focused foot vein mapping the day before pDVA to ensure patency of the deep foot veins and to mark the LPV on the plantar skin surface of the forefoot and midfoot to facilitate venous access during the index pDVA procedure.
Clinical
Patients with Rutherford classes 5 and 6 were included in this study. Patients with extensive foot necrosis and/or infection beyond salvage were not deemed suitable for pDVA. Those with heel necrosis with or without calcaneal osteomyelitis were also not considered for pDVA, in our experience, we noticed marked improvement of the vascularity and development of arterialized venous flow in the forefoot and midfoot following successful pDVA procedures. We have therefore not considered heel necrosis, with or without calcaneal osteomyelitis, for pDVA as we are still uncertain if it will result in meaningful improvement in the perfusion to this area. We, however, continue to monitor the literature for the reported experiences of other centres who might consider using pDVA in patients with heel necrosis.
Procedure
Procedural steps using the LimFlow system were previously described in detail in the published PROMISE I trial. 7
Post-procedure
A popliteal nerve sheath catheter was routinely placed in all patients during the pDVA procedure. This serves 2 functions: The first is to help with the foot pain, which might occur secondary to potential ischemic steal phenomenon. In addition, adequate pain control allows limb elevation to reduce postoperative foot oedema secondary to the venous hypertension caused by the arterialization of the deep veins.
Following the procedure, a strict anticoagulation protocol was followed. All patients were kept on weight-adjusted therapeutic dose of low-molecular-weight heparin, as well as an antiplatelet. For the first 24 hours, neurovascular status of the limb was checked every 2 hours. Strict leg elevation was adhered to for the first 48 hours to reduce leg oedema.
In view of the current lack of guidance on the best anti-thrombotic regimen following pDVA, our MDT (with the inclusion of our haematology/thrombosis and pharmacy teams) had several discussions/meetings to agree a standardized postoperative protocol. It was decided to manage these patients as per deep venous stenting protocols, keeping them on anticoagulation until the wounds are healed, or the stent occludes, to improve stent patency. Patients were also commenced on lifelong aspirin 75 mg once daily as the antiplatelet regimen.
A check angiogram was routinely performed, typically 72 hours after the index procedure, to optimize the flow into the foot deep veins by embolization of any stealing tributaries as needed.
Patients were discharged on Rivaroxaban 20 mg once daily in addition to an antiplatelet. All patients were enrolled into a strict Doppler ultrasound (DUS) surveillance programme, involving a scan pre-discharge, then at 1, 3, 6, 9 and 12 months. Threatened pDVAs detected during DUS surveillance, or those who presented acutely with threatened or thrombosed stent-grafts, were scheduled for urgent angiograms within 72 hours, with the aim to optimize or salvage the pDVA circuit.
Threatened pDVAs detected during DUS surveillance, 70% stenosis or more, significant reduction the blood flow velocity compared with the first post-procedure duplex scan, or those who presented acutely with threatened or thrombosed stent-grafts. We took the characteristics described by Schreve et al regarding the volume flow (VF) rates and peak systolic velocities (PSVs) into consideration, as a PSV of ≤55 cm/s and a VF value of ≤195 mL/min were found predictive for failure. If any of the above features was identified in duplex scan, the patient was offered an angiogram to validate and treat any stenosis as needed. 9
Routine postoperative clinical evaluation included assessment of wound healing, and foot infection status using WIfI (wound, ischaemia and foot infection) scoring system. 10 Partial wound healing was defined as tissue granulation with wound edge epithelization. Complete wound healing was defined as complete epithelization of the entire wound area. 7 Wound assessment was performed during regular podiatry outpatient clinics, with wound photos being uploaded onto the hospital’s electronic patient record. These were used retrospectively to assess wound healing progression. Foot surgery, such as debridement or amputation of the toes, were preferably delayed for 4 to 6 weeks if clinically safe to do so, to allow maturation of the pDVA and improve the chances of wound healing.
As this study is a retrospective review, a separate ethics approval was not obtained. This study was registered as a service evaluation project in our institution. Eleven of the patients of this cohort were recruited in PROMISE UK study. 11
Statistical analysis was performed using SPSS version 26, categorical variables were expressed as median and continuous variables were expressed as mean. Kaplan-Meier analysis was used to report the PP and SP rates, AFS and FFR.
Results
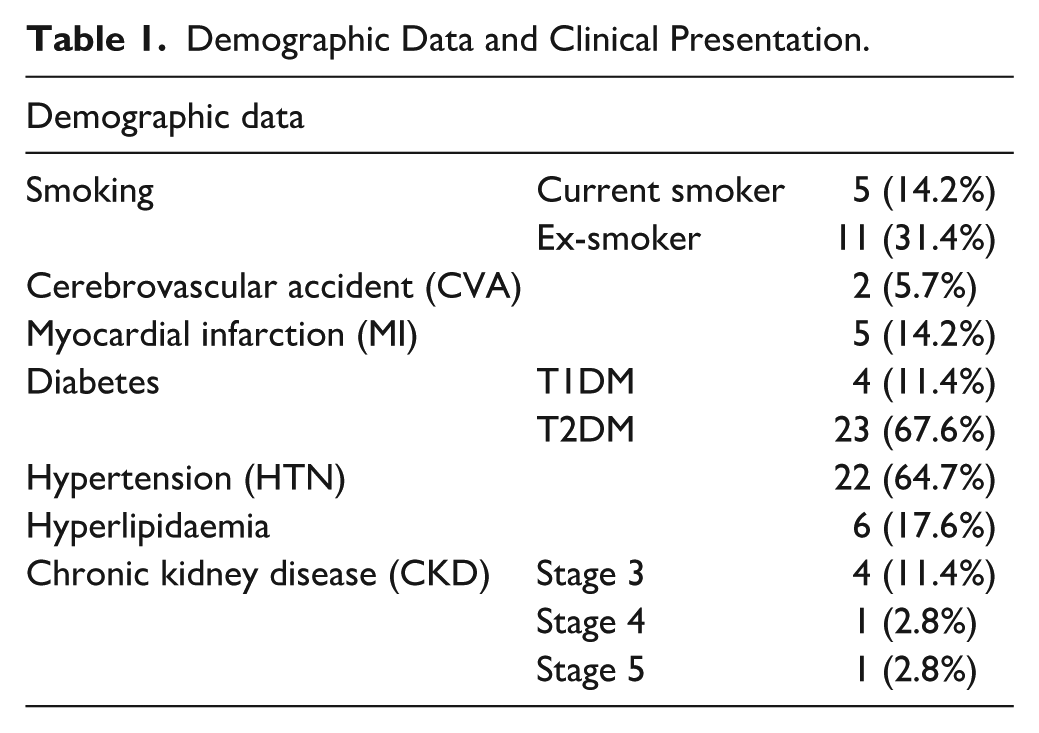
A total of 34 patients (8 women) were included in the study. The median age was 67 years (range: 41–83 years). Median follow-up time was 21 months (ranging from 4 to 62 months). Four patients had previously contralateral major lower limb amputations (3 below-the-knee amputations and one above-the-knee amputation). Twenty-seven patients (79.4%) were diabetic (4 had type 1 diabetes mellitus), while only 5 patients (14.2%) were current smokers. Six patients (17.6%) had chronic kidney disease (CKD), with only 1 patient with end-stage renal disease (ESRD) and on dialysis. Table 1 shows the risk factors among the study cohort.
Demographic Data and Clinical Presentation.
Thirty-two patients from our cohort presented with minor tissue loss, classified as Rutherford stage 5; while only 2 patients had major tissue loss, classified as Rutherford stage 6. 8
Anatomical Criteria and Procedure Details
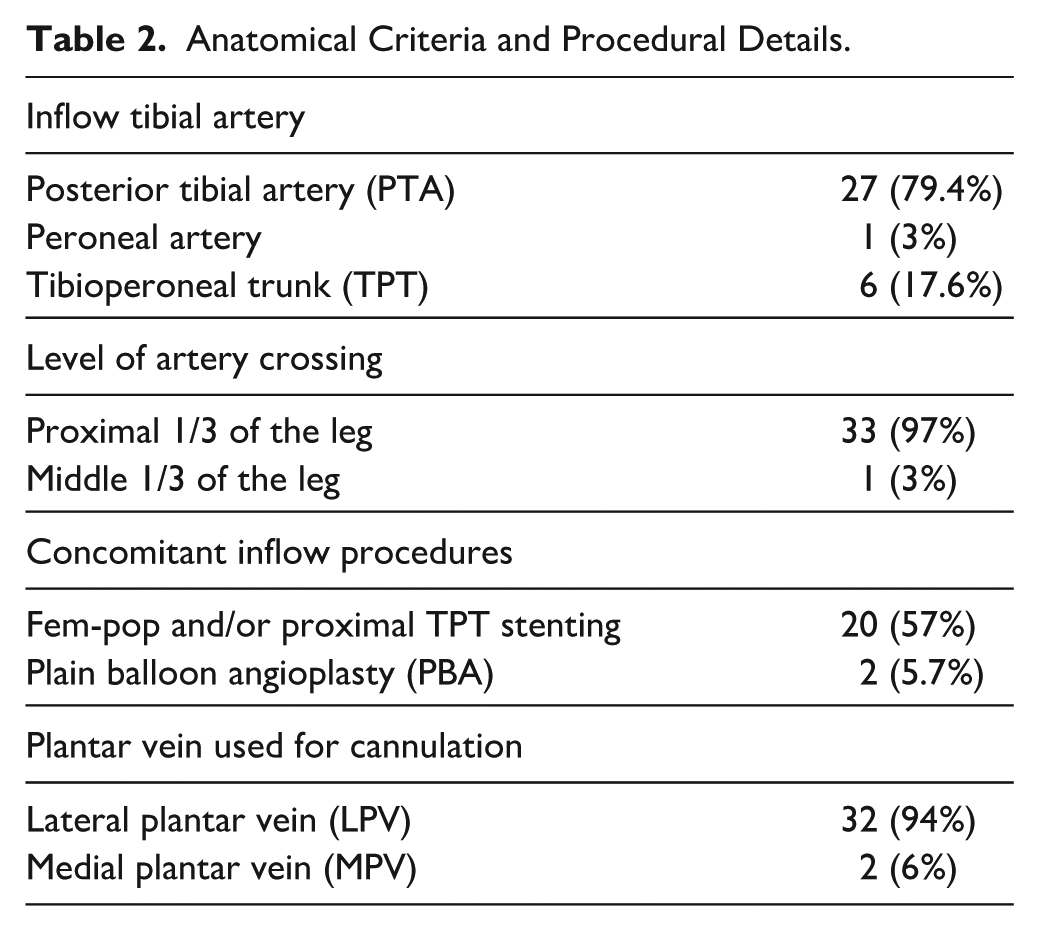
Anatomically, LPV was the outflow target in 33 patients. The medial plantar vein was used in 1 patient, who did not maintain graft patency, where the LPV was of inadequate diameter. The mean diameter of the outflow target vein was 3.9 mm. Twenty-four venous embolizations were performed in total, 19 embolizations were performed in the planned first angiogram check during the first 10 days, and 5 more embolizations were done later between the first admission and first 3 months. Total of 18 patients needed venous embolization in this cohort.
The inflow artery for the pDVA was mainly the PTA in 27 patients, while the tibio-peroneal trunk (TPT) was used in in 6 patients. The peroneal artery was used as an inflow artery in 1 patient.
Proximal third of the leg was used as the anatomical site for arteriovenous crossing in 33 patients, while in 1 patient, the crossing was performed at the level of the middle third of the leg. Although this patient needed 2 thrombectomy attempts to maintain graft patency, it was not possible to show any statistically or clinically significant difference between proximal or mid leg for anatomical crossing due to the very small sample size in the latter approach.
Twenty-two patients had concomitant inflow endovascular procedures, 20 of them had inflow arterial stenting (femoropopliteal segment or proximal TPT), while 2 patients had plain balloon angioplasty (PBA). Table 2 shows the anatomical criteria and procedural details. We had a very low threshold to treat inflow arterial disease, as securing a reliable inflow is essential to maintain graft patency, this was maintained without affecting the outcome of pDVA patency. This is shown in Figure 1.
Anatomical Criteria and Procedural Details.
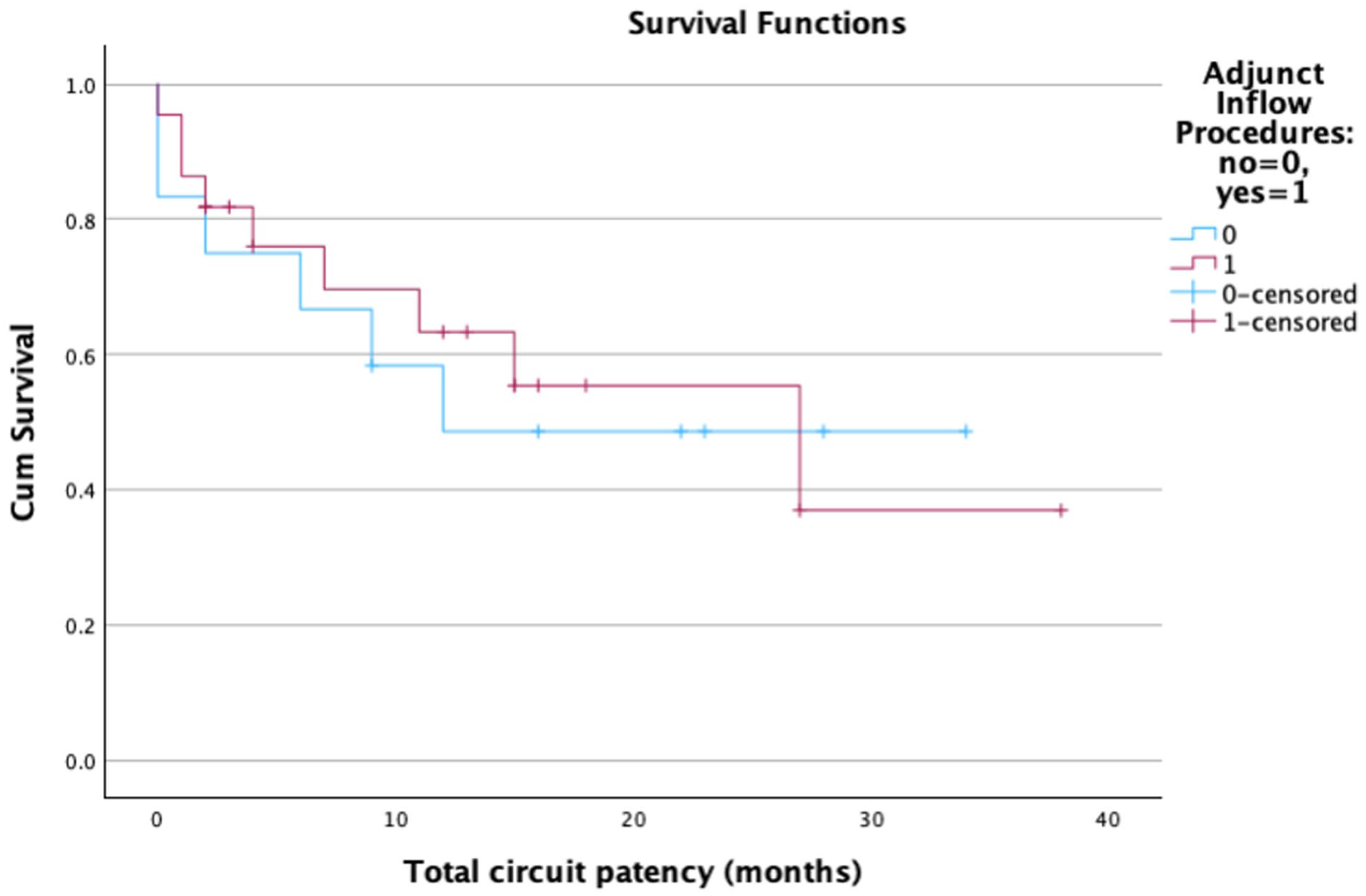
Kaplan-Meier curve of the concomitant inflow procedures with p value 0.806.
Median total procedure time was 157 minutes (ranging from 82 to 251 minutes). The foot veins were treated with PBA only in 15 patients, while the LimFlow antegrade valvulotome was used in the LPV in 18 patients. We elected to using the antegrade valvulotome in relatively larger LPVs, or in the case of resistant valves post-PTA. We have not used the antegrade valvulotome in small or borderline LPV due to the fear of causing perforation as well as spasm, which might consequently compromise the outflow of the stents. We have not noticed any difference between the 2 techniques. This is shown in Figure 2.
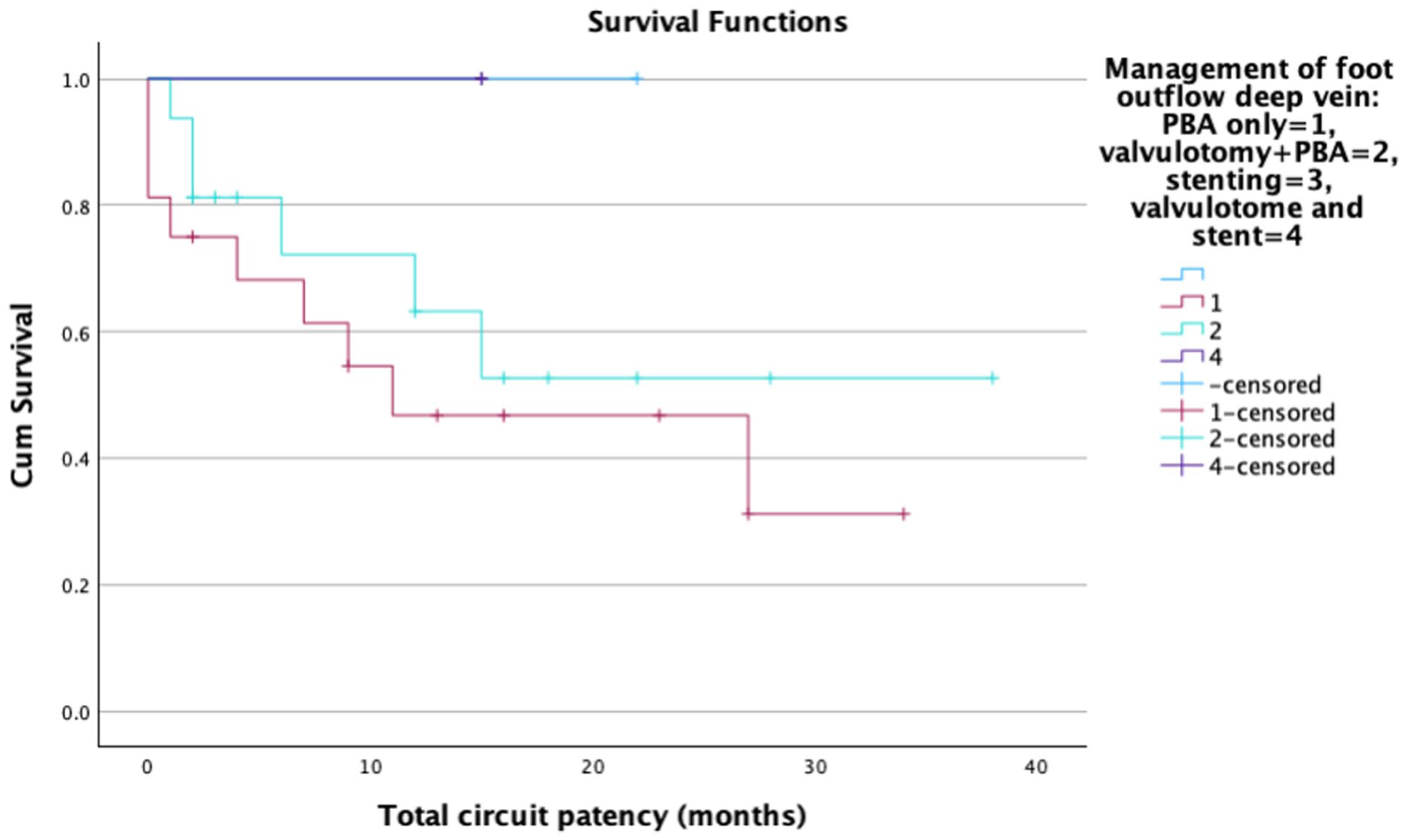
Kaplan-Meier curve of deep vein outflow management with p value of 0.804.
We noted that some published literatures have highlighted the efficacy of using drug-eluting stent (DES) extending into the LPV with excellent results in terms of patency and reduction of target vessel reintervention in the LPV. In our series, we did not perform this routinely, as we relied on close postoperative duplex monitoring, with a strategy of low threshold for intervention if restenosis was detected. However, in 2 of our patients, restenosis was detected in the LPV, which was indeed treated with DES.
In view of the current lack of guidance on the best anti-thrombotic regimen following pDVA, our MDT (with the inclusion of our haematology/thrombosis and pharmacy teams) had several discussions/meetings to agree a standardized postoperative protocol. It was decided to manage these patients as per deep venous stenting protocols, keeping them anticoagulation until the wounds are healed, or the stent occludes, to improve stent patency. Patients were also commenced on lifelong aspirin 75 mg once daily as the antiplatelet regimen.
Post-Procedure Follow-up
The median hospital stay was 22 days (range: 6–140 days), with a median time from the index procedure to complete wound healing of 262 days, while those who needed completion trans metatarsal amputation (TMA) had a median time of complete wound healing of 277 days. This explains the long hospital stay. Twelve patients required additional foot surgical treatment, in the form of debridement or toe amputation to treat sepsis, prior to discharge. However, minor amputations (digital or trans metatarsal) in the absence of infection, were delayed 4 to 6 weeks after the index procedure if feasible to allow for the maturation of the arteriovenous circuit. Major (below-the-knee) amputations were required in 4 limbs (11.7%). Table 3 shows the details of minor amputations performed in this series.
Minor Amputation Numbers.
During the follow-up period, full wound healing occurred in 23 patients (66%) with a median time from the index procedure to complete wound healing of 262 days. Those who had completion TMA had a median time to complete wound healing of 277 days. Three patients who had TMA received split skin graft.
The AFS was 79.4% at 6 and 12 months and 72% at 24 months of follow-up, while the LS rate remained at 88.6% at 6, 12 and 24 months of follow-up; this was demonstrated in Figure 3. Figure 4 shows the PP and SP achieved in this group, as we had PP and SP rates of 46.3% and 76%, respectively, at 24 months.
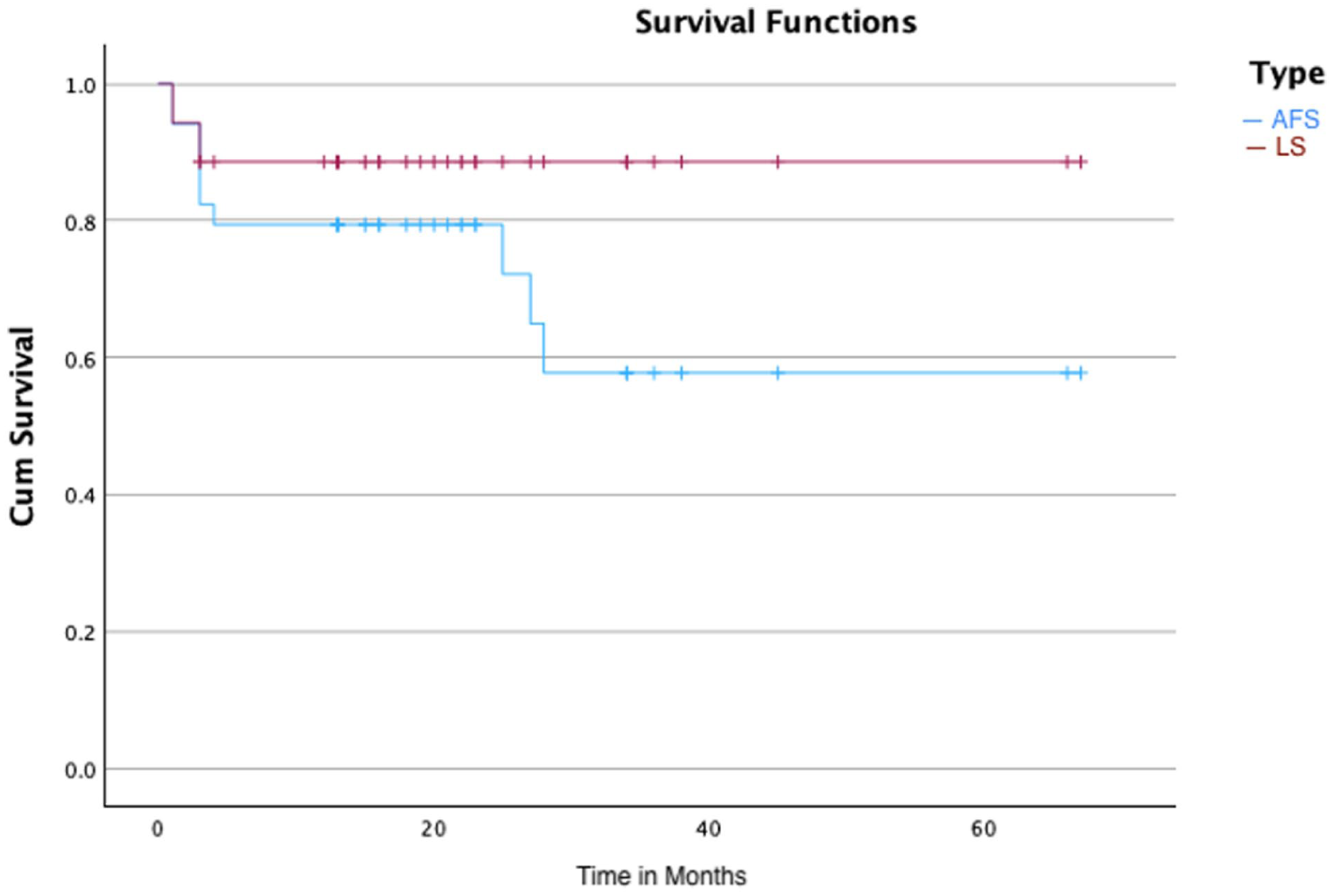
Kaplan-Meier curve of amputation-free survival (AFS) and limb salvage (LS).
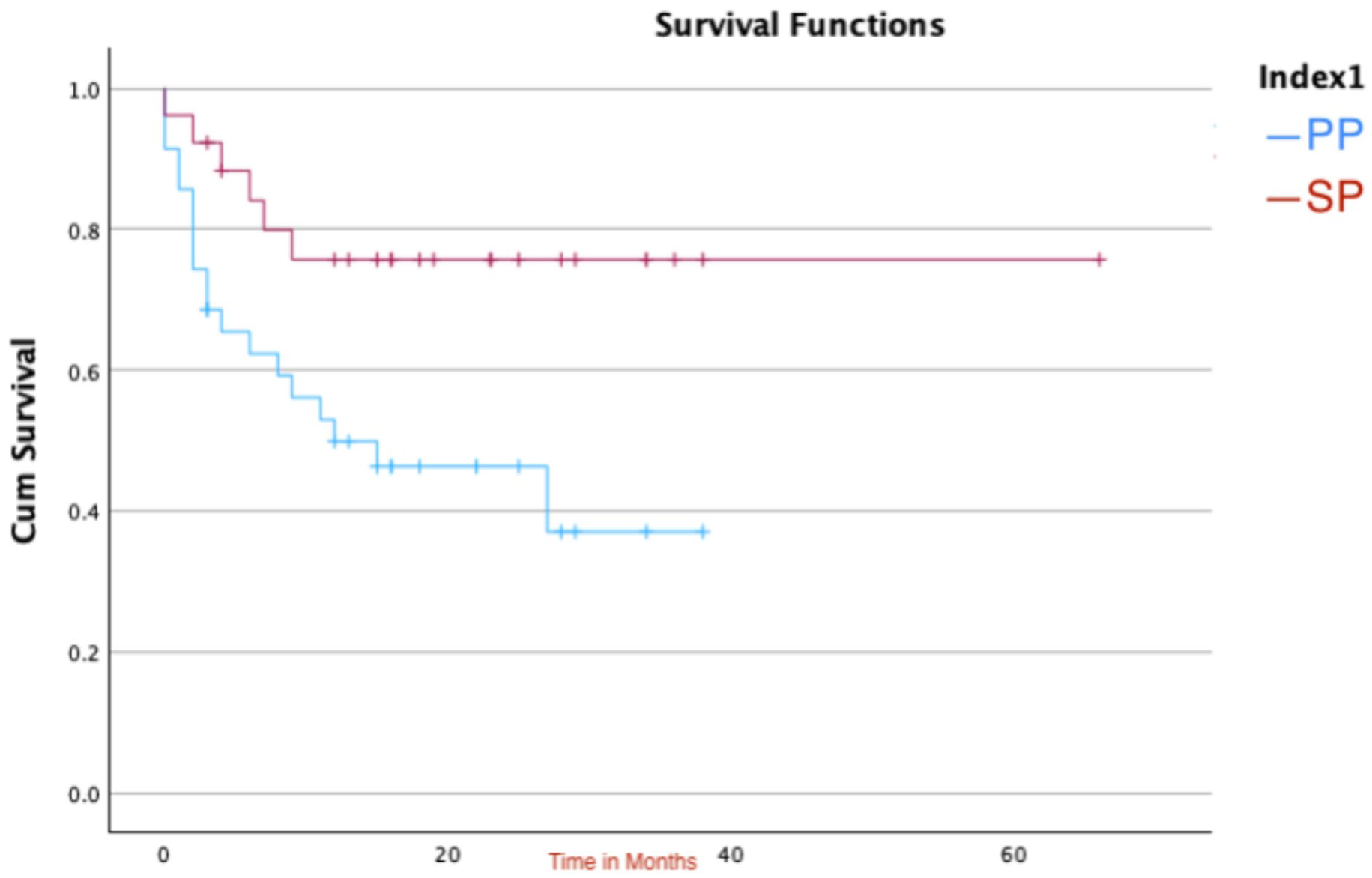
Kaplan-Meier curve showing primary patency (PP) and secondary patency (SP).
In our study, in total; we had fourteen circuit thrombectomies done to eleven patients included in our study. According to Rundback’s classification, one patient was type 1b (proximal stent edge), four were type 3a (distal stent edge), six were type 5 (culprit lesion not defined) and three patients had both type 1b and type 3a lesions.
One patient had proximal TPT and Anterior tibial arteries angioplasty to maintain assisted PP with a total FFR of 67%, 67% and 58% at 6, 12 and 24 months of follow-up, respectively, as shown in Figure 5.
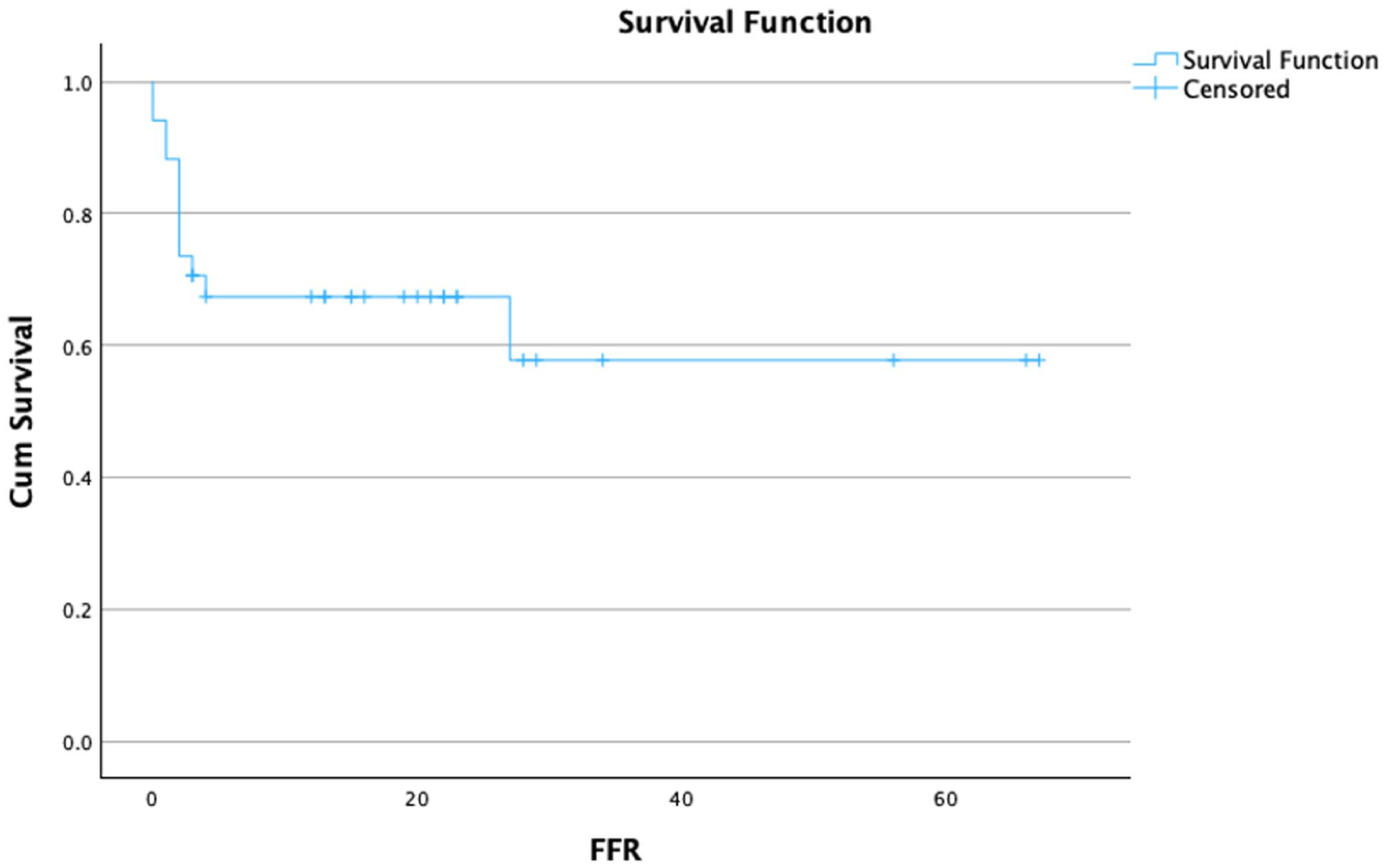
Kaplan-Meier curve showing freedom from reintervention (FFR).
Discussion
This study reports the mid-term outcomes of pDVA using the LimFlow system in no-option patients with Rutherford 5 and 6 CLTI in real-life settings. At 2 years, the LS was 88.5%, with an AFS of 72%. Complete wound healing was achieved in two-thirds of patients, with a median time of 262 from the index procedure. The PP and SP rates were 46.3% and 76%, respectively, at 24 months. This satisfactory outcome is mainly achieved by multiple factors including careful patient selection; the timing of the procedure is also crucial; by avoiding delays until the tissue loss becomes extensive and the foot is beyond salvage. We would also like to emphasize the importance of strict clinical and radiological follow-ups. This involved weekly or fortnightly clinical review in a multidisciplinary foot clinic. In addition, a strict surveillance programme, and early interventions to focalize/re-direct the flow to the forefoot towards the area of tissue loss. Close wound monitoring by dedicated podiatry team with vast wound management experience is invaluable.
Open surgical arterialization of lower limb veins was first introduced by Lengua F. It was associated with multiple surgical complications including infection, wound complications and steal phenomenon. 12 In an attempt to overcome these limitations, pDVA was proposed to deliver more oxygenated blood to the foot through the venous system. 13 Medical treatment post-intervention has not been standardized yet; however, single antiplatelet agent (aspirin or clopidogrel) added to anticoagulation has shown better patency outcomes and reduced reintervention rates. 14
In a retrospective study including 70 patients reporting the outcomes of pDVA in patients with no-option CLTI; technical success was achieved in 96% of patients, with AFS of 51.4%, 40% and 30% at 6 months, 1 and 2 years, respectively, confirming feasibility and safety of this procedure. 15
In 32 patients included in PROMISE I trial, technical success was achieved in 96% (31 patients). Amputation-free survival was 91%, 74% and 70% at 30 days, 6 and 12 months, respectively. After 6 months of follow-up, 6 major amputations and 2 deaths were reported in this cohort. Full wound healing was observed in 67% of patients at 6 months and 75% at 12 months. Twelve minor amputations were recorded at 12 months of follow-up. 7 On the contrary, in PROMISE II study including 105 patients, AFS was 54.2% with an LS of 68.7% at 1 year, with 99% technical success. 16
In this study, we had 100% technical success in 34 patients treated with pDVA using LimFlow system, with AFS of 80% and 72% at 6 and 24 months, respectively. Four patients underwent below-the-knee amputation, and full wound healing occurred in 66% of patients at 24 months of follow-up, with a median time of 262 days from the index pDVA procedure.
The nerve sheath catheter was used in our study for the early postoperative period, 5 to 7 days maximum, mainly for pain control and oedema reduction. Although using popliteal nerve sheath catheters might increase the vasodilator effect of peripheral circulation, which can facilitate wound healing, this was not analysed in detail in our study.
In a meta-analysis published in 2017, the LS rate was 75% at 12 months in patients treated with venous arterialization. 13 In our study, LS was 88.5% at 6 and 24 months. This could be a reflection of the intense clinical and imaging monitoring and surveillance programme employed in these patients, which could facilitate the early intervention on threatened arterialized venous systems to improve the patency and LS.
In another series of pDVA published 2022 included 42 patients, the PP rate in only 8 patients was 19% and the SP rate was 7% in 3 patients at 6 months. This was associated with 19% partial wound healing and 4.8% complete wound healing. Interestingly, the authors described the ultrasonographic criteria of end-stage plantar disease, named as the white stop signs. This reflects a totally occluded calcified vessel, which can be different from hibernating lumen. Also, angiographic criteria of patent proximal tibial arteries with complete occluded distal plantar segments are indicators for pDVA treatment. 14
In a multicentre retrospective study in Japan (DEPARTURE JAPAN), the results of pDVA using the off-the-shelf technique were reported. The technical success rate was 88.9%, with freedom from major amputation rates of 55.6% and 49.4%; and wound healing of 23.0% and 53.2%, at 6 and 12 months, respectively. 17
In this study, which included 34 patients, the PP was 85.7%, 68.6% and 46.3% at 6, 12 and 24 months, respectively. Of note, the SP was 84% at 6 months and remained 76% at 12 and 24 months of follow-up. This compared relatively favourably with the reported outcomes from the pooled analysis of PROMISE studies, in which the SP was 64.2% and 44% at 6 and 12 months of follow-up, respectively. 16 This might again be due to the intensive postoperative radiological and clinical surveillance programme we recruit these patients to. Also, a check angiogram was routinely performed, typically 72 hours after the index procedure, to confirm stent patency and treat early stent stenosis or compression. In addition, we carefully examined the foot arterialized venous system and, if needed, embolize major stealing tributaries to focalize/direct the flow towards the forefoot where tissue loss is located. We believe this might have played a role in improving the early patency of the pDVA until full maturation of the arterialized foot venous system is achieved.
It is important to note that patients who maintains LS in the early postoperative period, are more likely to achieve full wound healing and maintain long-term LS and AFS. This highlights the importance of close monitoring and early interventions to maintain pDVA patency in the early postoperative period. If this is successfully achieved, it will likely lead to LS at 2 years.
In the PROMISE I trial, the reintervention rate was 52%; 75% of these were performed to improve the arterial inflow, 7 whereas in the PROMISE II trial, the reintervention rate was 36.5%. 16 This reflects the improvement in the technical aspect with the development of better understanding of the need for and the timing of interventions if needed. In our study, we observed an FFR rate of 67% and 58% at 6 and 24 months, respectively. Notably, each of the 4 patients who ended up with below-the-knee amputation had received unplanned interventions to treat thrombosed stent-grafts.
The full wound healing was obtained in 28% and the partial healing was obtained in 51% of patients in the PROMISE II study. 13 In the PROMISE I study, the full and partial wound healing rates were 67% at 6 months, and with the remaining alive and amputation-free patients; wound healing rates were 75%. 7 The wound healing outcomes documented in our study are consistent with these published results. We had a full wound healing of 66% with a median time from the index procedure to complete wound healing of 262 days. In addition to the close clinical/ radiological monitoring and the low threshold for intervention strategy detailed above, the multidisciplinary input in the care of these patients is paramount. These patients are monitored in a multidisciplinary clinic with access to advanced foot wound care team, infectious diseases/microbiology team as well as orthotics/offloading team. We believe that this comprehensive postoperative care has played an important part in achieving this satisfactory wound healing rates.
Subgroup analysis in the PROMISE II study has demonstrated the importance of defining the risk factors of atherosclerotic arterial disease, as patients with CKD were associated with higher mortality. Also, the associated physical and psychological burden of CLTI on patients, together with the increased cost of hospital admissions and social care services, must be taken into consideration when defining patients with no-option CLTI. 13 Seventeen (17%) of our patients had CKD, 1 of being on haemodialysis, with no significant difference in outcome. As demonstrated in PROMISE II; patients with ESRD on dialysis did not show favourable outcomes following pDVA. However, being on dialysis was not an exclusion criterion for pDVA in our study, which might affect the long-term patency outcomes.
It should be noted that this is a retrospective, single-arm and single-centre study. We did not routinely collect data regarding the quality of life in these patients, which would have been helpful in providing a comprehensive view of this procedure. However, despite these limitations. Our experience with the use of LimFlow system in patients with “no-option” CLTI has been encouraging. The reported AFS, LS and wound healing rates seem reasonable in the context of the no-option status of these patients. We would therefore recommend considering pDVA in appropriately-selected patients who are deemed unsuitable for the conventional revascularization options.
Conclusion
Percutaneous deep venous arterialization using the LimFlow system seems to provide acceptable mid-term outcomes, with reasonable AFS, LS and wound healing rates in suitable no-option patients. Strict monitoring, both clinical and radiological, seems essential to maintain these satisfactory outcomes.
Footnotes
Acknowledgements
Dr Diamantopoulos has been supported by the National Institute for Health and Care Research (NIHR) (Senior Clinical and Practitioner Research Award, NIHR306224). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Professor Hany Zayed is a consultant to Inari.
Data Availability Statement
All data generated or analysed during this study are included in this published article.