
Abstract
Background:
Carotid blowout syndrome (CBS) is a rare but potentially fatal complication of head and neck cancer (HNC), with radiotherapy being a major risk factor. Because of its high mortality, urgent treatment is essential. Endovascular therapy has become the standard approach, although complications such as stent extrusion may occur.
Method:
This study reports a single case with a brief review of the relevant literature.
Case Presentation:
A 67-year-old woman underwent neck dissection and chemoradiotherapy for metastatic cervical carcinoma. Radiation dermatitis developed during treatment and persisted thereafter. Four months later, she developed a carotid artery pseudoaneurysm that resulted in CBS. Emergency endovascular repair was performed using a covered stent from the left common to internal carotid artery. Two months later, the stent spontaneously extruded through the cervical skin. Remarkably, there was no active bleeding or neurological deficit. The stent detached naturally, and the patient remained clinically stable.
Conclusion:
This case highlights an extremely rare occurrence of carotid stent extrusion. Although endovascular therapy is effective for CBS, serious complications such as hemorrhage and neurological damage may occur. Careful long-term follow-up is essential to detect delayed adverse outcomes.
Clinical Impact
This case highlights a rare but clinically important phenomenon of spontaneous carotid stent extrusion following endovascular treatment for carotid blowout syndrome (CBS). While endovascular therapy is widely accepted as the first-line treatment due to its minimally invasive nature, this report emphasizes the potential for delayed and unexpected complications, particularly in irradiated and infected fields. The absence of hemorrhagic or neurological sequelae despite stent extrusion suggests that complete thrombosis and collateral circulation may mitigate catastrophic outcomes. Clinicians should recognize this risk and implement close multidisciplinary follow-up, early wound management, and consider preventive strategies such as flap reconstruction or timely stent removal to improve patient safety.
Introduction
Carotid blowout syndrome (CBS) is a rare complication of head and neck cancer (HNC). It has been reported in 3% to 4.5% of patients with HNC, despite any treatment, and can result in pseudoaneurysm, hematoma, airway obstruction, or cerebral infarction. Moreover, its mortality rate has been reported to exceed 40%. 1 Therapeutic options for CBS include surgical ligation and endovascular approaches such as coil embolization or stent placement. The latter has gained acceptance as the standard treatment owing to its less invasive nature; however, severe complications, including recurrent bleeding and stent extrusion, have also been documented. Herein, we report a case in which carotid stent extrusion occurred 2 months after endovascular treatment for CBS, without associated complications, as the stent spontaneously exited through the cervical skin. This was our first experience with spontaneous extrusion of an endovascularly placed stent. In this case, we were able to avoid mortality from both CBS and stent extrusion; however, it is important to recognize that if adequate intravascular thrombosis has not yet formed and the stent protrudes externally due to damage to the surrounding vascular wall or skin, the patient may be at high risk of fatal hemorrhage.
Case Report
A 67-year-old woman presented to the otolaryngology department of our hospital with a palpable mass in the left cervical region. A lymph node biopsy from the lesion revealed metastatic disease. Special staining revealed positivity for CD5 and c-kit, suggesting a high likelihood of thymic carcinoma; however, as this was a metastasis of a poorly differentiated carcinoma, determining the histological type or the primary tumor was difficult. Three months later, the patient underwent a left neck dissection and left tonsillectomy. Subsequently, she received concurrent chemoradiotherapy over a 3-month period. Two cycles of chemotherapy with CBDCA and 5-FU were administered. Radiation therapy was initially delivered at 8 Gy to the nasopharynx, hypopharynx, larynx, cervical esophagus (3 cm), the mucosa, and bilateral cervical lymph node levels II, III, IV, V, VI, VIIa, and VIIb, as well as the left level Ib. This was followed by a localized boost of 66 Gy to the left cervical tumor bed only. About 1 month after the initiation of radiation therapy, radiation-induced dermatitis developed at the irradiated site. Treatment was continued with cleansing, topical application of Antebate ointment, and Melolin gauze dressing. A follow-up computed tomography (CT) scan, obtained 2 months after completion of chemoradiotherapy, demonstrated no evidence of local recurrence in the neck.
Four months later, an exacerbation of radiation-induced dermatitis on the neck was observed, during hospitalization at another hospital for loss of appetite. The affected area showed poor epithelialization and became secondarily infected, leading to the formation of a pseudoaneurysm. Several days after infection, the patient presented to our emergency department in shock due to acute hemorrhage originating from the pseudoaneurysm. The patient’s hemoglobin level was preserved, and no evident abnormalities in other coagulation parameters were observed. Temporary hemostasis was obtained through manual compression, after which the patient stabilized from shock vital signs. Contrast-enhanced CT revealed protrusion of the left common carotid artery into the subcutaneous tissue near the bifurcation of the internal and external carotid arteries (ECAs). On the same day, urgent endovascular intervention was performed, and a stent was deployed extending from the left common carotid artery to the left internal carotid artery (ICA) (Figure 1). A catheter was advanced from a sheath inserted into the right femoral artery to the left common carotid artery (Figure 1A (←a)). Branches arising from the common carotid artery were selectively catheterized, followed by coil embolization using AZUR Soft 3D coils (Figure 1B (←b)). The guiding catheter was then advanced into the left ECA, and an Amplatzer Vascular Plug was deployed at the origin of the ECA after introducing a microcatheter through the device. Multiple AZUR CX18 and AZUR Soft 3D coils (Figure 1C (←c)) were delivered through the microcatheter positioned distal to the plug within the main trunk of the ECA. The microcatheter was subsequently pulled back into the plug, and 3 additional AZUR Soft 3D coils were packed within the plug to achieve complete occlusion of ECA flow (Figure 1D). A Gladius MG18 guidewire was advanced into the left ICA, and a VIABAHN stent-graft (8 mm/10 mm) was deployed from the ICA to the common carotid artery. After post-deployment balloon angioplasty using a SENRI balloon, satisfactory stent expansion and the absence of procedure-related complications were confirmed, completing the procedure.
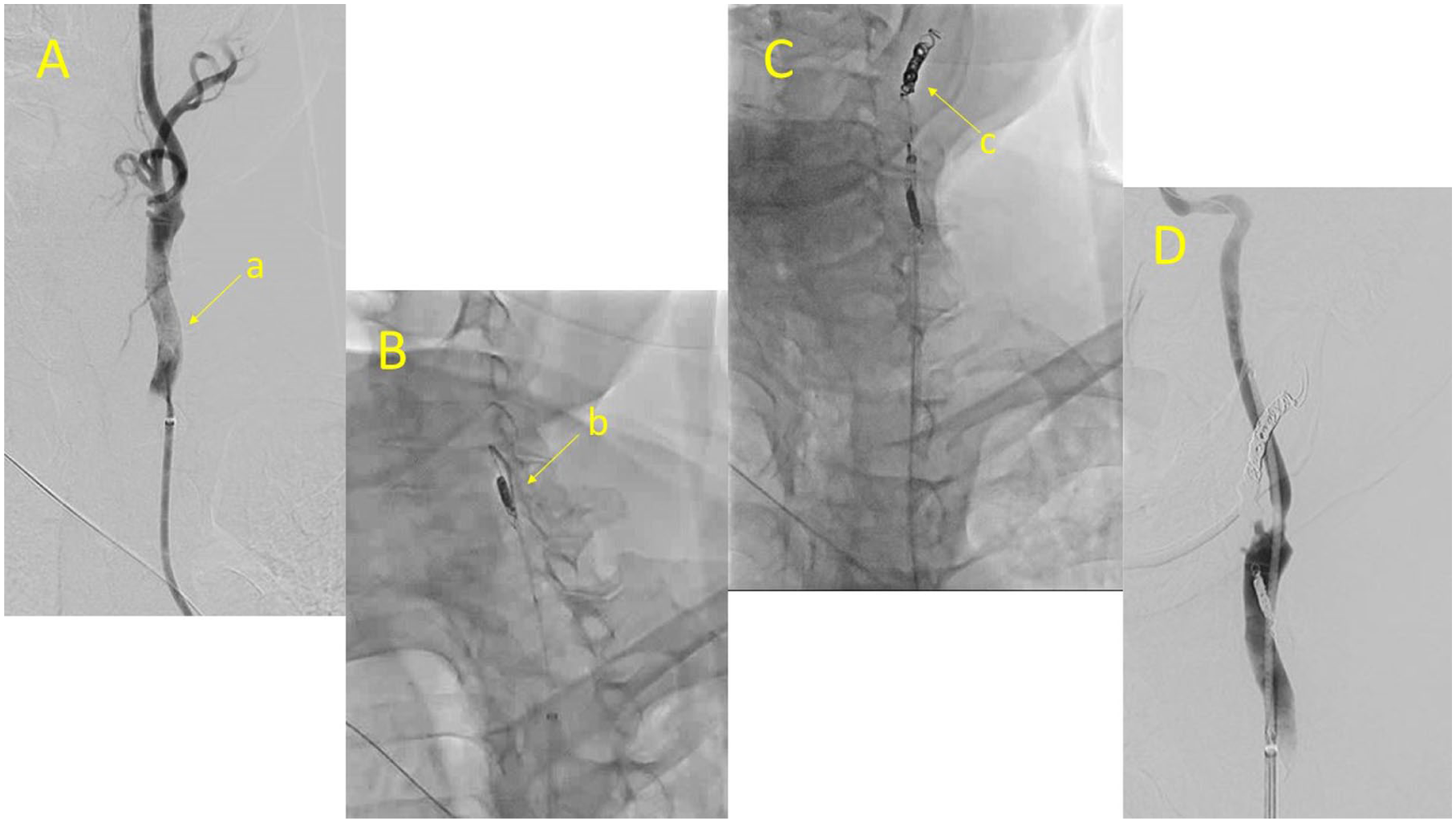
(A, B, C, D) This series of angiographic images documents the emergent endovascular treatment for a ruptured pseudoaneurysm of the left carotid artery. A catheter was advanced from a sheath inserted into the right femoral artery to the left common carotid artery (←a) (A). Branches arising from the common carotid artery were selectively catheterized, followed by coil embolization using AZUR Soft 3D coils (←b) (B). The guiding catheter was then advanced into the left external carotid artery (ECA), and an Amplatzer Vascular Plug was deployed at the origin of the ECA after introducing a microcatheter through the device. Multiple AZUR CX18 and AZUR Soft 3D coils (←c) were delivered through the microcatheter positioned distal to the plug within the main trunk of the ECA (C). The microcatheter was subsequently pulled back into the plug, and three additional AZUR Soft 3D coils were packed within the plug to achieve complete occlusion of ECA flow (D). A Gladius MG18 guidewire was advanced into the left internal carotid artery (ICA), and a VIABAHN stent-graft (8 mm/10 mm) was deployed from the ICA to the common carotid artery. After post-deployment balloon angioplasty using a SENRI balloon, satisfactory stent expansion and the absence of procedure-related complications were confirmed, completing the procedure.
And this patient had a history of lower extremity arterial disease and had been receiving dual antiplatelet therapy with cilostazol and clopidogrel, therefore, these antiplatelet agents were continued after the stent placement. Simultaneously, regarding the treatment of the infected wound, Pseudomonas aeruginosa was detected from the wound culture, and sulbactam/ampicillin (3 g every 8 hours) was initiated and continued for 2 weeks. The wound was cleaned daily, and treatment with prostaglandin ointment was continued. Coverage with a pectoralis major muscle flap was planned 2 weeks after stent placement; however, as inflammatory markers remained unstable, the procedure was postponed, and the patient was discharged without it.
Approximately 1 month following stent placement, the patient developed an ulcer in the left cervical region. Progressive exposure of the stent was noted at the ulcer base. Over time, the proximal portion of the stent became completely detached (Figure 2A), prompting admission to the otolaryngology department. At the time of admission, angiographic evaluation demonstrated absence of flow through the stent. Purulent discharge was observed from the tissue surrounding the distal portion of the stent, which was embedded in the ulcer base. Computed tomography imaging confirmed thrombotic occlusion of the left common carotid artery from its origin, with additional occlusion of the intracranial ICA at the C3–4 cavernous segment. The proximal end of the cervical stent was externally exposed and filled with air (Figure 3A and B).
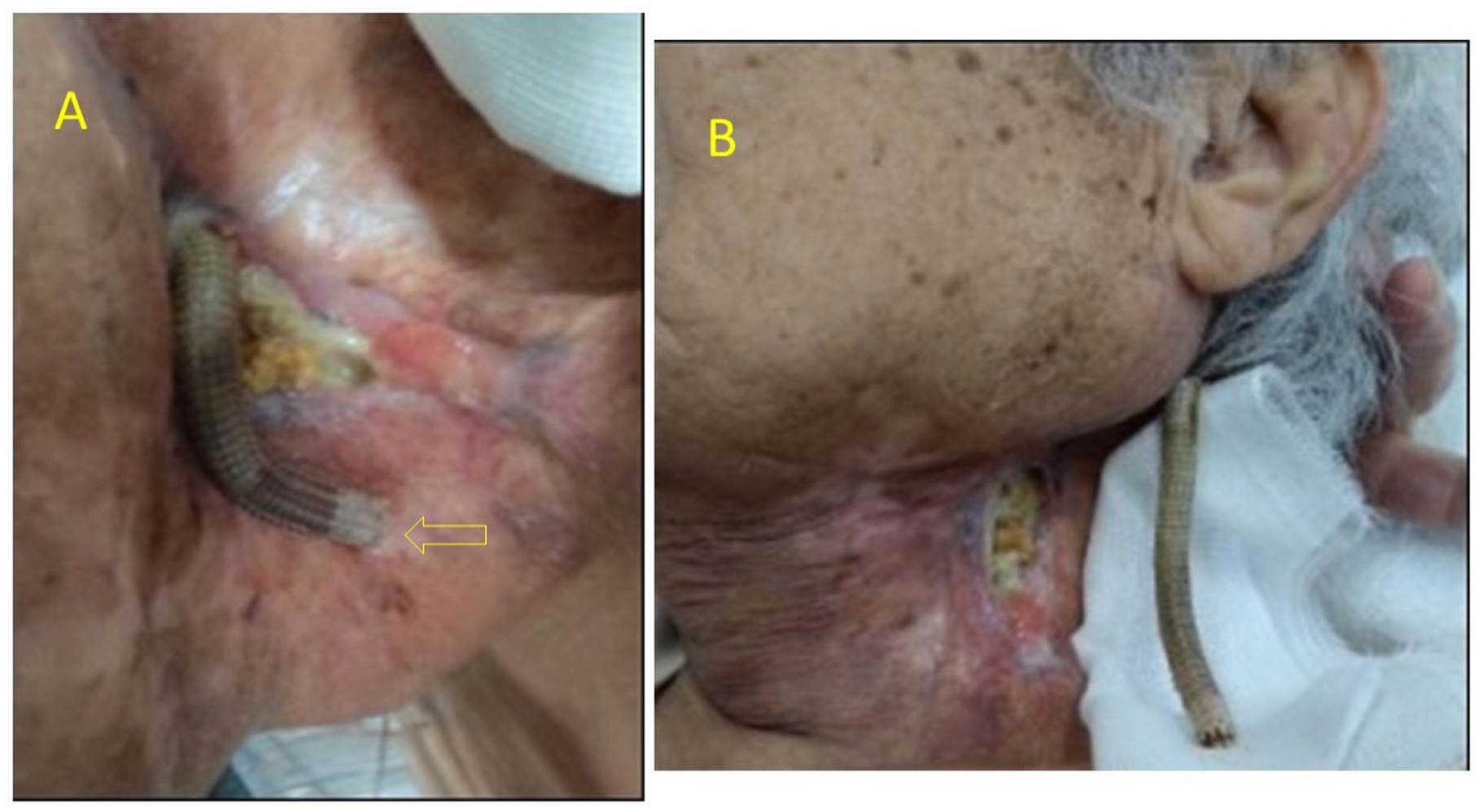
(A, B): (A) Photograph obtained approximately 1 month after stent-graft placement, showing distal stent extrusion through the skin surface. The arrow (⇦) points to the exposed distal end of the stent. In this image, the left side corresponds to the mandible, the lower side to the ventral aspect of the neck, and the upper side to the dorsal aspect of the neck. (B) Photograph taken after the stent had been completely expelled from the body; in this image, the upper side corresponds to the cranial direction and the lower side to the caudal direction. The completely detached stent was placed on a gauze pad and photographed in the same orientation as it had been positioned in the vessel.
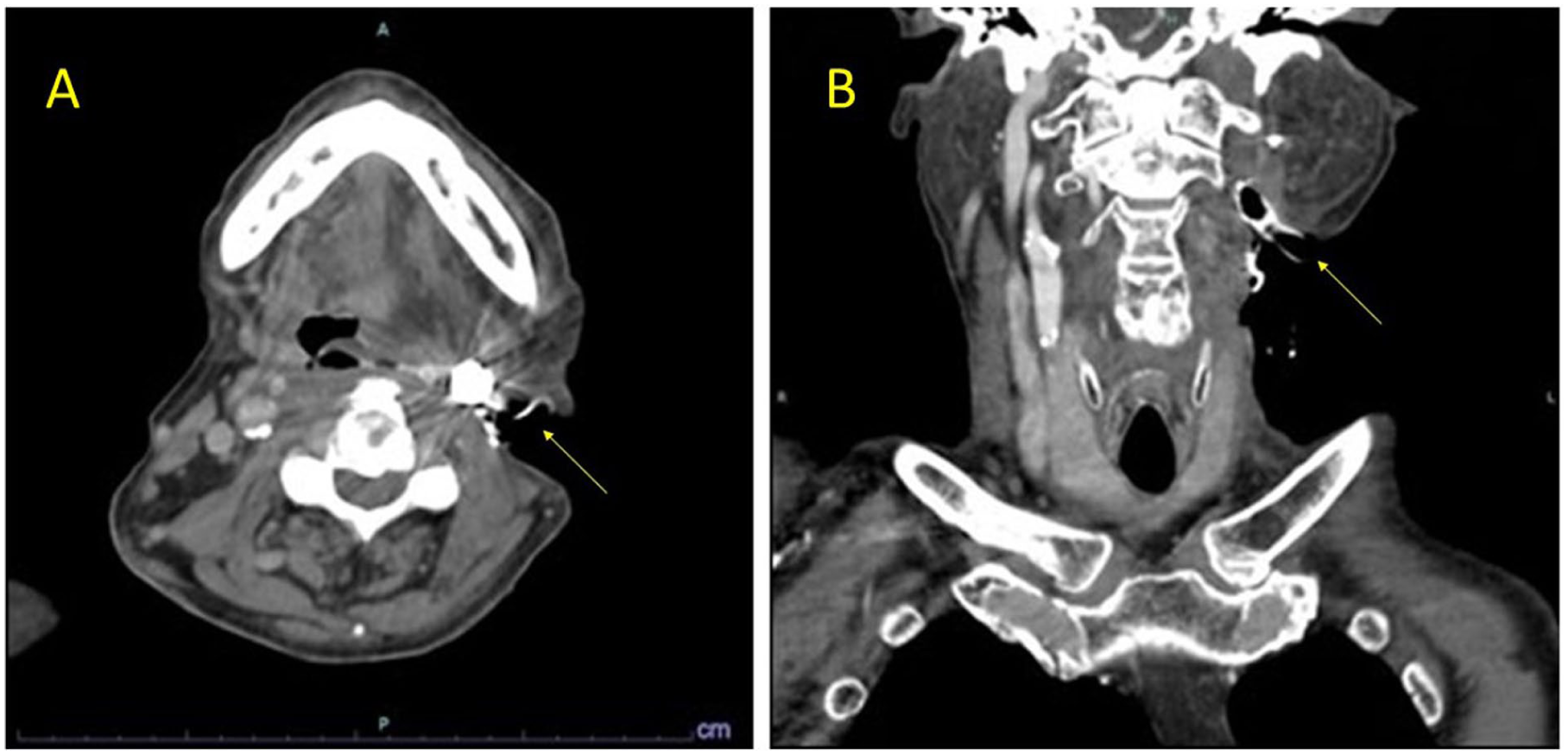
(A, B): Axial (A) and coronal (B) CT images of the neck obtained approximately 1 month after stent-graft placement, demonstrating exposure of the stent through the overlying skin at the treated site. The left common carotid artery was found to be occluded by thrombus from its origin, and the proximal portion of the cervical stent (→) was exposed outside the body.
Despite these findings, the patient remained hemodynamically stable and did not exhibit any signs of rebleeding or neurological deficits. She was managed conservatively. On the fourth day of hospitalization, the proximal portion of the stent spontaneously detached and was naturally expelled (Figure 2B). Following this event, her general condition remained stable, and no hemorrhagic or neurological complications were observed during follow-up. She was transferred to another hospital, 2 weeks after the stent extrusion, without undergoing additional imaging studies. Seven months have passed since the transfer, and no new symptoms have developed; the patient’s overall condition remains stable.
Discussion
Carotid blowout syndrome is a rare complication in patients with HNC, but it is an extremely serious condition, as the mortality rate is so high. 1 It is characterized by rupture of the carotid artery, resulting in massive cervical hemorrhage. Reported risk factors include a history of neck dissection, direct tumor invasion of the carotid artery, wound infection, fistula formation, radiotherapy, and chemotherapy. While radiotherapy is a used and indispensable modality in the management of HNC, the mortality of CBS occurring in previously irradiated patients has been reported to increase to as high as 76%. 1 This is because radiation therapy promotes the formation of free radicals, which can induce thrombosis, occlusion of the vasa vasorum in the adventitia, and vascular fibrosis. These changes subsequently lead to atherosclerosis and marked fragility of the vessel wall, ultimately resulting in CBS.2,3 Considering the effects of radiation, the patient had received a high dose of 66 Gy to the neck in this case, and therefore, the risk of developing CBS was considered to be high. In addition, chronic inflammation may cause thrombosis of the arterial vasa vasorum and increase the sensitivity to inflammatory mediators, further weakening the arterial wall. These mechanisms also contribute to the development of CBS. 2 In this patient, dermatitis developed during radiotherapy and persisted without complete healing, leading to chronic inflammation, which was thought to be a factor contributing to the elevated risk of CBS.
Carotid blowout syndrome is commonly classified into 3 categories according to its clinical presentation.
Type I involves exposure of the carotid artery due to soft tissue breakdown, requiring intervention to prevent rupture. Type II involves hemorrhage that can be controlled temporarily with compression or wound closure. Type III represents catastrophic carotid rupture associated with massive hemorrhage. While type I cases may be managed electively, types II and III require urgent intervention. In this case, although the pseudoaneurysm had already ruptured and required emergency treatment, temporary hemostasis was achieved by compression; therefore, it was classified as type II, emergency treatment was undertaken.
Therapeutic options for CBS include surgical ligation and endovascular procedures. Surgical ligation is considered a definitive treatment with relatively low rates of rebleeding and neurologic complications. However, it is highly invasive and is generally reserved for patients who can tolerate surgery, are expected to have a longer survival, or have lesions involving the common or ICA. Conversely, endovascular therapy has become the preferred modality because it can be performed rapidly and less invasively, making it suitable even for patients with poor general condition, and it has been associated with lower postoperative morbidity and mortality compared with surgical ligation. 1 Nevertheless, endovascular treatment carries important risks, including distal embolism leading to cerebral ischemia, foreign-body reaction, and infection due to intravascular prostheses. Serious complications such as stent exposure and rerupture of the carotid artery have been documented. 4 When our patient was transferred to the emergency department with hemorrhage from the left common carotid artery, she presented in shock. Although temporary hemostasis was achieved by manual compression, the situation was critical and required immediate intervention. After consultation with the departments of neurosurgery and cardiovascular surgery, endovascular treatment performed by the radiation oncology team was selected. This decision was based on the fact that, given the institutional circumstances at that time, endovascular management could be initiated most rapidly and was relatively less invasive for the patient.
Rebleeding and neurological complications are the most common adverse events after treatment for CBS, with rates of 35.6% and 10.8% to 14%, respectively. 1 In our case, carotid stent extrusion occurred approximately 2 months after placement. Remarkably, this occurred without rebleeding or neurological complications. Reports of carotid stent extrusion in the literature are exceedingly rare. Aaronson et al 5 reported a case of a stent extruding into the upper airway 9 months after placement, precipitated by coughing and presenting with acute stridor and dysphagia. Similarly, O’Connor et al 6 described a patient who coughed out his carotid stent 6 months after placement; the patient remained asymptomatic, and CT angiography demonstrated occlusion of the common carotid artery. On the contrary, Jia-Zheng Huang et al reported a case in which wide excision and neck lymph node dissection were performed for tongue cancer, followed by chemoradiotherapy for a locally-recurrent tumor 2 years later. Eight years thereafter, massive bleeding from the ulcerated tumor site necessitated coil embolization of both the CCA and ICA. They further noted that progressive skin defects over the tumor led to exposure of the implanted coils, and, after confirming complete intravascular thrombosis, conservative management was selected. According to their report, necrosis and cavitation around the tumor are likely to occur in the long-term course of HNCs. 7 Compared with these reports, our case was unique in several respects: extrusion occurred relatively early at 2 months, the patient remained entirely asymptomatic, the stent was spontaneously expelled without intervention, and extrusion occurred externally through the skin rather than into the airway. The patient had undergone high-dose radiotherapy, which markedly increased the risk of CBS, and had experienced repeated dermatitis during the course of treatment. Even after the stent was placed in the vessel due to CBS, the surgical site remained infected. Coverage with a flap was considered but could not be performed, and the wound did not fully epithelialize. As a result, the stented vessel remained close to the surface, and it is likely that the fragile vessel wall could easily protrude. Furthermore, despite the generally high mortality associated with CBS after radiotherapy, and the substantial risk of rebleeding and neurological deficits, our patient experienced none of these adverse outcomes and maintained a favorable clinical course. When a stent extrudes from the intravascular space to the body surface, it must penetrate the vascular wall, and under normal circumstances, massive hemorrhage from the site and neurological deficits in the supplied territory would be expected. In our case, however, complete thrombosis within the stented vessel was observed, and neurological symptoms did not develop, likely because collateral circulation had sufficiently developed to maintain cerebral perfusion. Such cases have not been encountered in our institution, and only a few have been reported in the literature; therefore, we considered this presentation to be clinically exceptional.
Nevertheless, CBS remains a life-threatening condition with a high fatality rate. Even after initial treatment, recurrent hemorrhage may occur and can be fatal. Therefore, when endovascular therapy is performed for CBS, regular and careful follow-up is essential and should include regular clinical and imaging assessments. Clinical evaluation should focus on early signs of infection, wound deterioration, skin breakdown, or sentinel bleeding, particularly in patients with prior irradiation or impaired wound healing. Imaging surveillance using contrast-enhanced CT angiography or duplex ultrasonography is recommended to evaluate stent patency, vascular wall integrity, thrombosis progression, and possible stent exposure or migration. Close monitoring at short intervals during the early post-treatment period is particularly important because complications may develop rapidly. Furthermore, multidisciplinary collaboration among vascular surgeons, head and neck surgeons, plastic surgeons, and interventional specialists may facilitate early detection of complications and timely intervention. Preventive strategies should also be considered to reduce the risk of subsequent complications. Examples of such measures include reconstruction of the weakened skin using a flap—preferably a pectoralis major flap, which is suitable even for irradiated areas and is technically feasible for this region—and early removal of the stent. There are no established clinical guidelines regarding the timing of stent or coil removal following treatment for CBS. Nevertheless, our experience and previous case reports suggest that a comprehensive evaluation is required, taking into account the condition of the wound and vessel wall, tumor control status, adequacy of collateral circulation, degree of thrombosis, and the patient’s overall prognosis. These findings highlight the importance of individualized management and meticulous follow-up after endovascular treatment for CBS, particularly in patients with prior irradiation or compromised wound healing, to prevent life-threatening complications while preserving neurological function.
Conclusions
In the present case, CBS developed following neck dissection and chemoradiotherapy for cervical malignancy. Two months after emergency endovascular treatment, an exacerbation of radiation-induced dermatitis on the neck was observed, which was followed by extrusion of the carotid stent. Compared with previous reports, the clinical course was relatively short, and the stent was spontaneously expelled through the skin surface without hemorrhage or neurological complications, making this case unique. Although CBS is a rare complication of HNC, it is potentially fatal and requires prompt therapeutic intervention. Endovascular therapy is currently the treatment of choice because of its minimally-invasive nature; however, it carries substantial risks of rejection and infection. In patients with a history of radiotherapy and concomitant skin ulceration at the treatment site, the risk of stent extrusion may be increased. While no hemorrhagic or neurological complications occurred after stent exposure in this case, such events can result in massive bleeding or airway obstruction. Therefore, regular and careful follow-up is essential in the management of these patients. And also preventive strategies—including reinforcement of the vulnerable carotid wall with flap reconstruction and, in selected cases, early stent removal—should be considered to reduce the risk of subsequent complications.
Footnotes
Acknowledgements
The authors would like to thank the medical and nursing staff involved in the care of this patient for their dedicated support. They also acknowledge the contributions of the radiology and pathology departments in the diagnostic evaluation.
Ethical Consideration and Consent to Participate
The operation technique described in this case report was performed under a protocol approved by the Institutional Review Board (IRB) of Saiseikai Utsunomiya Hospital (No. 2020-49, September 24, 2020). Consistent with the retrospective reporting of this case and reliance on de-identified patient data, the IRB waived the requirement for individual informed consent (Helsinki Declaration).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data underlying this article will be shared on reasonable request to the corresponding author.