
Abstract
Aim:
To evaluate how the guideline-defined target anticipated sealing zone (TASZ) translates into the real achieved sealing zone (RASZ), and whether this relationship is stent-graft-dependent.
Methods:
In a retrospective single-center study, 365 consecutive endovascular abdominal aortic aneurysm repairs (Endurant, n=267; AFX, n=98; 2011–2022) were reviewed. Preoperative and first postoperative computed tomography angiography (CTA) scans were evaluated with a previously reported centerline-driven approach. Target anticipated sealing zone and RASZ were systematically evaluated. After exclusion of patients with a TASZ shorter than 15 mm, propensity-score matching produced 75 device pairs. The primary study outcome was to evaluate the relationship between TASZ and RASZ and its dependence on stent-graft design. The neck/apposition ratio (RASZ/TASZ) was calculated to quantify the proportion of the available preoperative neck length effectively used for circumferential sealing. Linear regression assessed the independent effects of oversizing and device type on the neck-to-seal ratio.
Results:
After matching, AFX achieved longer RASZ than Endurant (median 34 vs 25 mm; p<0.001) and larger sealing surface (2355 vs 1862 mm2, p<0.001). Compared to TASZ length, Endurant showed a median shortfall of −8 mm (IQR=−20.5 to +1 mm), whereas AFX exhibited a median surplus of +2 mm (IQR=−4.5 to +11 mm; p<0.001). Regression analysis confirmed that device type, neck slope, and oversizing are independent predictors of seal utilization. Type Ia endoleak incidence was <5% without inter-device difference.
Conclusions:
In this retrospective analysis, despite no difference in type Ia endoleak rate, achieved proximal sealing differed between devices, with AFX more often extending beyond the traditional neck and Endurant more often not covering the entire projected neck length.
Clinical Impact
This study highlights that guideline-defined neck length does not uniformly translate into achieved proximal sealing across different stent-graft technologies. Quantifying the achieved sealing zone on early postoperative CTA provides additional anatomical information beyond instructions for use-based neck metrics and may help to better characterize device-specific sealing behavior.
Introduction
Endovascular abdominal aortic aneurysm repair (EVAR) has become the standard treatment for abdominal aortic aneurysm (AAA), 1 although up to one third of patients still require reintervention within 10 years.2,3 Type Ia endoleak remains one of the most fearsome late complications of EVAR, and it is correlated with a significant reduction in survival of affected patients. 4 Therefore, durable aneurysm exclusion post-EVAR depends, among other factors, on achieving 5 and maintaining 6 a secure proximal seal in the infrarenal aortic neck. Despite standard instructions for use (IFU)-based planning, hostile neck features—particularly short or angulated segments—remain key predictors of proximal failure and are common in real-world EVAR practice.7,8 Infrarenal neck length is considered as the distance from the lowest renal artery to the point where the increase in diameter reaches 10%. Neck length alone is not a reliable indicator of seal quality, as other anatomical and procedural factors also influence the effectiveness of achieving seal over the target anticipated sealing zone (TASZ).9-11 The real achieved sealing zone (RASZ), even with precise infrarenal graft positioning, might be lower than the TASZ.12,13 As RASZ may significantly differ from the TASZ even when staying in the IFU in a non-hostile anatomy, the concept of the “proximal sealing zone” (PSZ) has emerged.7,14 The RASZ is defined as the length (and area) of circumferential contact between the stent-graft fabric and aortic wall on the post-EVAR computed tomography angiography (CTA) scan. 9 Importantly, the RASZ is not purely a patient anatomy metric – it also depends on device choice and design. Aggressive graft oversizing can cause the graft to seal distal to the infrarenal neck, while incomplete expansion or lower placement can result in a shorter seal. Early research indicates that RASZ might be a better indicator of EVAR durability than neck length alone. 9 Available stent-grafts have distinct intrinsic structural features that interact differently with a given anatomy. The 2 grafts we are comparing in this study are based on radically different approaches to achieving proximal sealing. The Endurant stent-graft (Medtronic Vascular, Santa Rosa, CA, USA) relies on an external asymmetric series of m-shaped nitinol stents that support the internal fabric. 14 Conversely, the AFX stent-graft (Endologix LLC, Irvine, CA, USA) has an internal cobalt-chromium endoskeleton and an external ePTFE graft lining that is free to move and intended to mold to the aortic wall and seal along the entire covered segment.15-17 The active seal behavior of AFX has been described in single-arm reports,17,18 but without comparison to modular grafts. Our study provides the first propensity-matched, head-to-head quantification of sealing zone behavior between AFX and Endurant, comparing the neck/apposition ratio and RASZ to isolate device-specific sealing performance. We specifically examine whether standard IFU-based neck measurements (eg, length) correlate with the RASZ achieved, and whether AFX’s design confers a measurable benefit in sealing zone length/area.
Methods
Study Design
This is a retrospective, single-center study that includes all consecutive AAA patients undergoing EVAR using an Endurant stent-graft (Medtronic Vascular, Santa Rosa, CA, USA), or the AFX stent-graft (Endologix LLC, Irvine, CA, USA) in a tertiary Italian vascular center with a case load of >100 EVAR procedures per year from November 2011 to November 2022.
Inclusion criteria included the presence of AAA with an indication for EVAR according to the most recent guidelines, 19 using the Endurant stent-graft or the AFX stent-graft system. The choice of stent-graft was operator- and graft availability-dependent. Another factor contributing to the choice between the AFX and Endurant systems was the different IFUs for each device, with AFX requiring a longer neck (15 vs 10 mm, respectively).
Exclusion criteria included EVAR procedures performed for different reasons than AAA (penetrating aortic ulcers, dissections, and occlusive disease), performing adjunctive proximal neck procedures such as EndoAnchors positioning or Chimney stent-grafts, unavailability of preoperative and postoperative (<90 days) CTA scans, insufficient quality CTA (less than 512 × 512-pixel resolution and more than 1.5 mm thickness), and the patient’s refusal to be included in the register.
Demographics, clinical, anatomical, periprocedural, and in-hospital course data were systematically collected for each patient.
Patients were divided into 2 groups based on whether they were treated with the AFX or the Endurant stent-graft. All deployments were performed according to the manufacturer’s IFU without the use of off-label techniques (eg, reverse-slider maneuvers).
All patients gave written consent for the anonymous collection of clinical data on the standard consent form provided by the institute. This study was approved by the local ethical committee (no. 2024/21860)
Surgical Planning and Procedure
Before the procedure, all patients underwent a CTA to evaluate the aortoiliac anatomy. Computed tomography angiography images were analyzed using the software OsiriX (Pixmeo SARL, Bernex, SW) version 13. The vascular surgery team discussed the indication and feasibility of the procedure. Device specialists were occasionally consulted for technical advice regarding device sizing or IFU confirmation, without involvement in clinical decision-making. Each procedure was performed in a dedicated operating theater under locoregional or general anesthesia with surgical exposure of both common femoral arteries for Endurant patients and one percutaneous access for the AFX patients.
Technical success was defined as the successful implantation of the stent-graft in the planned position and by the absence of type I or III endoleak at the final angiogram.
Clinical Outcomes and Follow-Up
After discharge, patients underwent clinical and CTA follow-ups at 30 days, 6 and 12 months, and yearly thereafter. This study focuses on early postoperative RASZ and early postoperative outcomes.
In case of chronic kidney disease (eg, estimated glomerular filtration rate <60 mL/min), a Duplex scan was preferred over a CTA during follow-up unless required by specific clinical or imaging suspicion.
The primary outcome was the relationship between TASZ and RASZ, and whether this relationship depended on stent-graft design. Secondary outcomes included quantitative descriptors of seal utilization, the influence of device type, oversizing and neck morphology on sealing metrics, and early postoperative clinical outcomes (type Ia endoleak and reintervention).
Proximal Sealing Zone Assessment
All measurements were performed by the same physician, who did not operate on the patients, and who specialized highly in using OsiriX (Pixmeo SARL, Bernex, SW) version 13. The evaluator followed a standardized and predefined protocol for assessing CTAs based on precisely defined criteria and was unaware of the study-specific assumptions during the evaluation process. The measurement protocol, already described previously,12,13 was performed on all patients on the preoperative and the first postoperative CTA. An overview of the measurement protocol is provided in Figure 1.
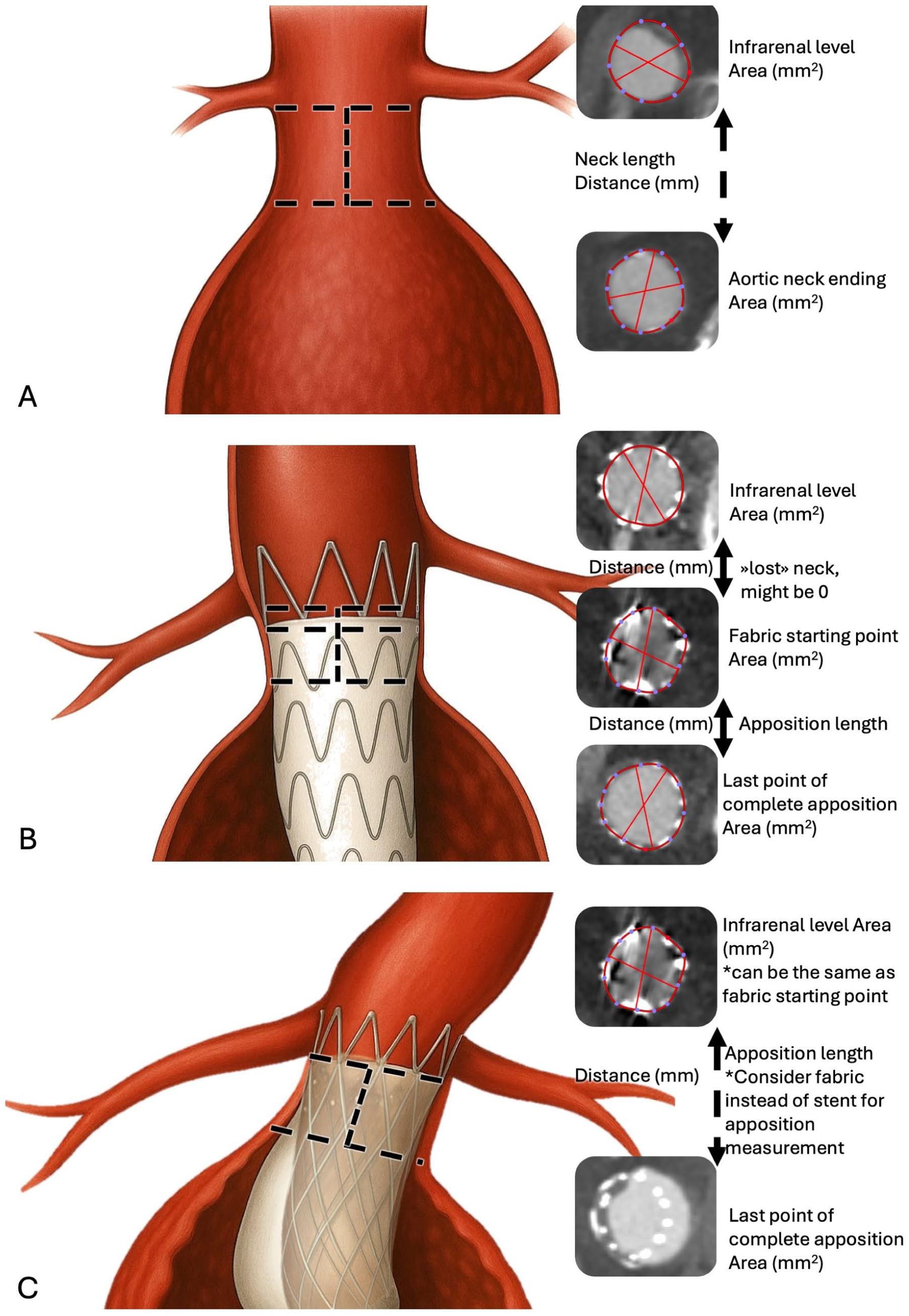
Measurement technique overview. Preoperative measurements (A), Endurant postoperative measurements with graft placed distally to the lowest renal artery (B), and AFX postoperative measurements (C).
Inter-observer reliability was evaluated using a subset of randomly selected CTAs, 20 preoperative, 30 postoperative from the Endurant group, and 30 postoperative from the AFX group. The subset was analyzed by a second independent evaluator (a diagnostic radiologist experienced in vascular imaging) who was not involved in the procedures or in the primary measurements, and the repeated measures were tested with the intraclass coefficient (ICC) method. The ICC showed excellent reproducibility among measures (ICC (2,1) 0.97–1.00 Endurant; 0.96–0.99 AFX); ICCs are reported in Supplemental Table S1. Bias was <2 mm.
The TASZ was defined on the preoperative CTA as the segment of the aorta from just below the lowest renal artery down to the end of the infrarenal neck using axial image slices perpendicular to the aortic centerline. We operationally delineated the distal end of the neck using the conventional criterion: the point at which the aortic diameter increased by >10% of the diameter at the lowest renal artery. Along this TASZ segment, we recorded neck length (in mm) and the cross-sectional areas at the limiting levels using the built-in closed polygon function. We also noted the presence of circumferential thrombus or calcification in the neck (graded qualitatively).
On the first post-EVAR CTA (at ~1 month), we measured the RASZ. Using axial image slices perpendicular to the aortic centerline, we identified the proximal extent of the stent-graft’s fabric in the neck and the most distal point along the graft where there was still continuous apposition between the graft and the aortic wall. The RASZ length (mm) was defined as the length over which the stent-graft fabric had 360° circumferential contact with the aortic wall. We noted the area at the infrarenal level, the area at the fabric starting point, and at the most distal point of complete graft apposition. We then noted the centerline distance between these 3 perpendicular planes. For AFX patients, given the absence of radiopaque fabric markers, direct identification of the graft-fabric interface was not possible. Apposition was defined as circumferential contact between contrast-opacified lumen and aortic wall, in the absence of endoleak. In segments with mural thrombus, the distal limit of apposition was considered where the inner stent struts visibly contacted the aortic wall. Despite the use of contrast mapping and color filters, fabric boundaries could not be reliably visualized; therefore, real fabric-to-wall contact may have been conservatively underestimated.
The difference between TASZ and RASZ was calculated in both length (mm) and area (mm2). A positive value (RASZ>TASZ) indicates the achieved seal extended beyond the anatomic neck, whereas a negative value indicates the achieved seal was shorter or smaller than expected from neck measurements. For each case, we also computed the neck/apposition length ratio, ie, RASZ length divided by neck length (ratio>1 means the graft achieved a seal longer than the neck). Neck morphology was summarized using a continuous neck slope metric, a study-specific continuous descriptor derived from the established concept of neck conicity,20,21 calculated as the difference between the preoperative cross-sectional area at the distal TASZ endpoint and the infrarenal level, divided by TASZ length (mm2/mm). This variable was used in a sensitivity multivariable analysis to account for neck shape.
Statistical Analysis
The normal distribution of continuous parameters was tested with the Kolmogorov-Smirnov test. Normally distributed variables were expressed as mean±standard deviation and compared using the Student t test; variables with a skewed distribution were reported as median and interquartile range and were compared with the Mann-Whitney U test. When appropriate, categorical variables were reported as numbers and percentages and compared using the χ2 test, or the Fisher exact test if the number of observations in any row was lower than 5.
Kaplan-Meier analysis was used to estimate freedom from endoleak and reintervention over time, with log-rank tests to compare groups.
Given the non-randomized comparison between 2 devices, we performed propensity-score matching to minimize confounding from baseline differences. A logistic regression model was built to predict the probability of receiving AFX (vs Endurant) based on preoperative variables. Candidate covariates included AAA diameter, infrarenal neck length, neck diameter/area, and neck angulation. Using the propensity scores, we matched AFX patients to Endurant patients at a 1:1 ratio without replacement, employing a nearest-neighbor algorithm with a caliper of 0.2 standard deviations of the logit. Balance between groups was confirmed by standardized mean differences (SMDs) and independent sample tests. The matching strategy was specifically designed to harmonize proximal sealing-related anatomy, including TASZ and neck morphology, thereby minimizing anatomical or geometrical bias.
A two-sided p<0.05 was considered statistically significant for all tests. Statistical analysis was performed using JASP software version 0.19.3 (JASP Team, the Netherlands) and SPSS version 30 (IBM Corp, NY, USA).
Results
A total of 365 EVAR patients (267 Endurant, 98 AFX) were analyzed. Supplemental Table S2 summarizes the preoperative characteristics of the unmatched cohort. The AFX cohort was on average significantly younger (70.4±7.9 vs 72.9±7.0 years for Endurant; p=0.007) and had a significant lower prevalence of hypertension, and prior myocardial infarction.
Anatomical and TASZ features of the unmatched cohort are reported in Supplemental Table S3.
Periprocedural and follow-up data are summarized in Table 1. Technical success was achieved in all cases.
Perioperative Details and Outcomes.
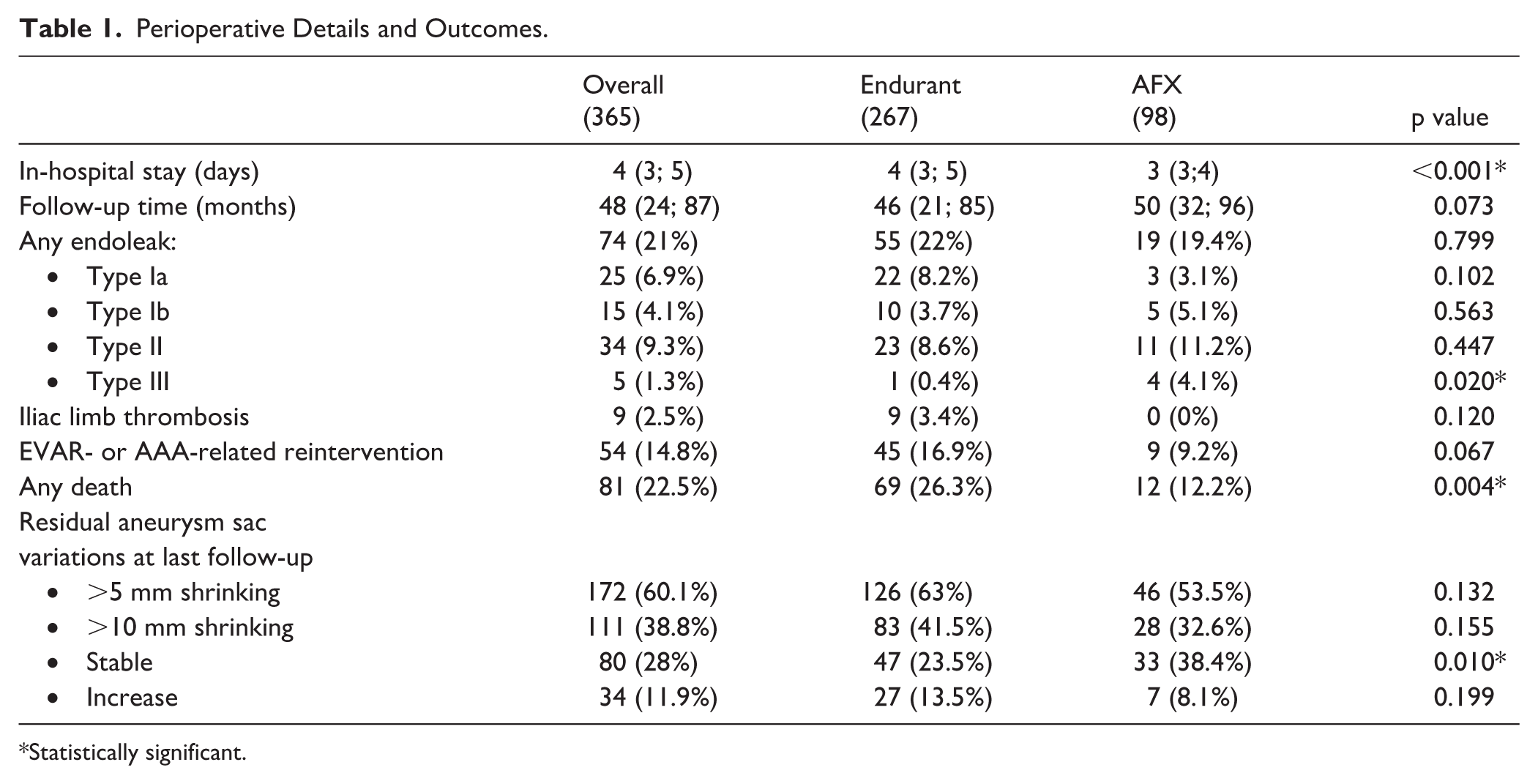
Statistically significant.
Median follow-up was 48 months (IQR=24–87). At 108 months, freedom from type Ia endoleak was 85.2% in the Endurant group and 88.2% in the AFX group; freedom from any endoleak was 69.4% and 72.5%, respectively; and freedom from EVAR-related reintervention was 71.2% and 81.7% (Figure 2).
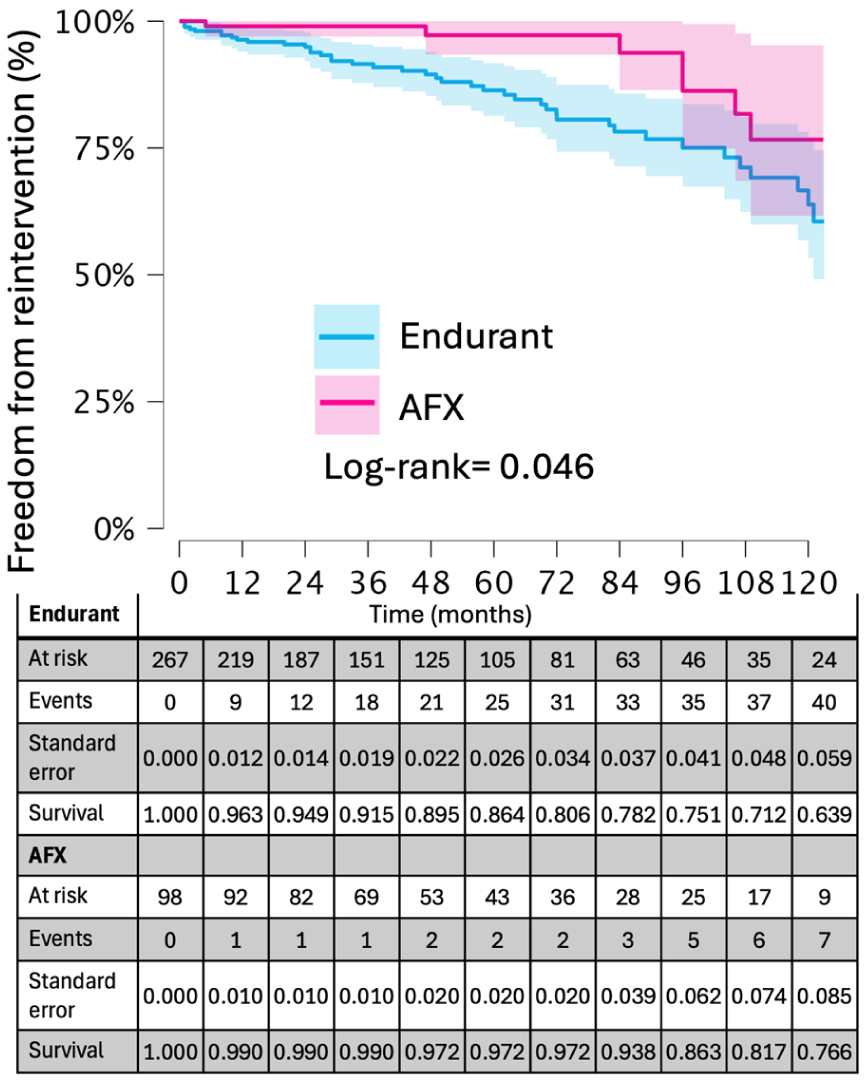
Kaplan-Meier survival plot of freedom from procedure-related reintervention (unmatched cohort).
Unmatched postoperative sealing features are reported in Supplemental Table S4, and TASZ-RASZ comparisons are summarized in Table 2. Real achieved sealing zone length was longer in AFX than in Endurant patients (32 [23–42] vs 13 [4–24] mm), and RASZ exceeded TASZ more frequently in AFX (65% vs 31%, p<0.001).
TASZ and RASZ Comparison in the Unmatched Cohort.
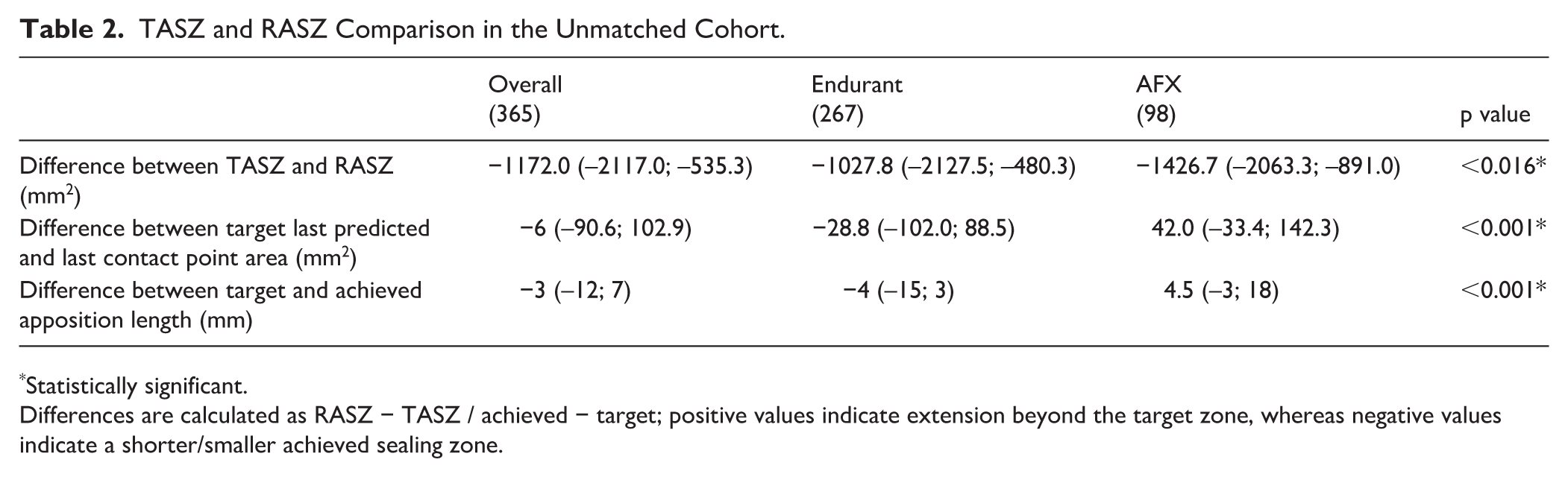
Statistically significant.
Differences are calculated as RASZ − TASZ / achieved − target; positive values indicate extension beyond the target zone, whereas negative values indicate a shorter/smaller achieved sealing zone.
After restricting to neck length ≥15 mm for both devices, the matching algorithm retained 75 well-matched pairs (n=150). All post-match absolute SMDs were ≤0.10 (Figure 3). Overall neck slope was 2.76 (1.36; 4.86) mm2/mm; 2.47 (1.05; 4.86) in the Endurant group and 2.83 (1.75; 4.94) mm2/mm in the AFX group, p=0.550. Post-matching neck length distribution is reported in Figure 4.
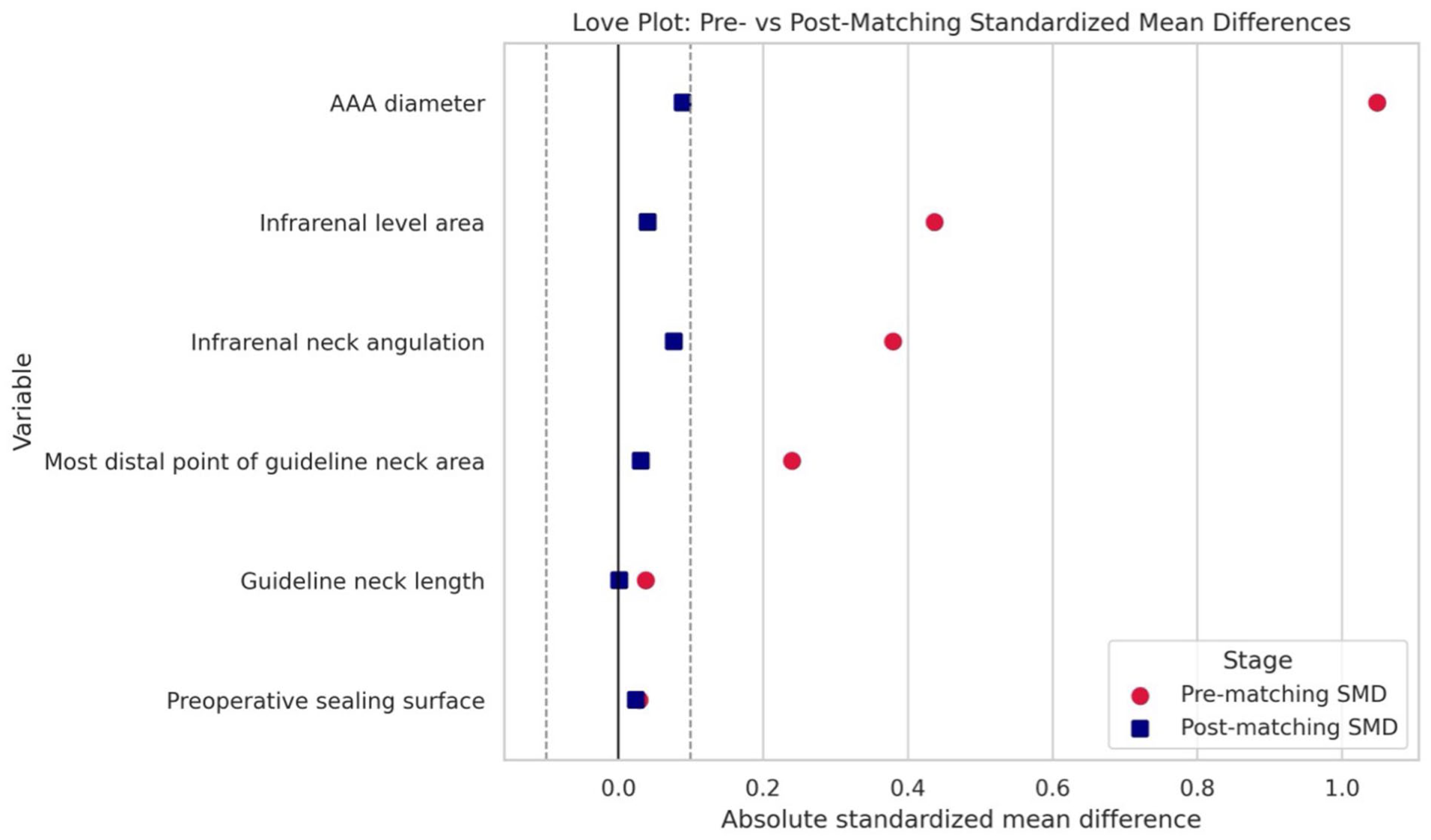
Love plot showing standardized mean difference (SMD) before and after matching.
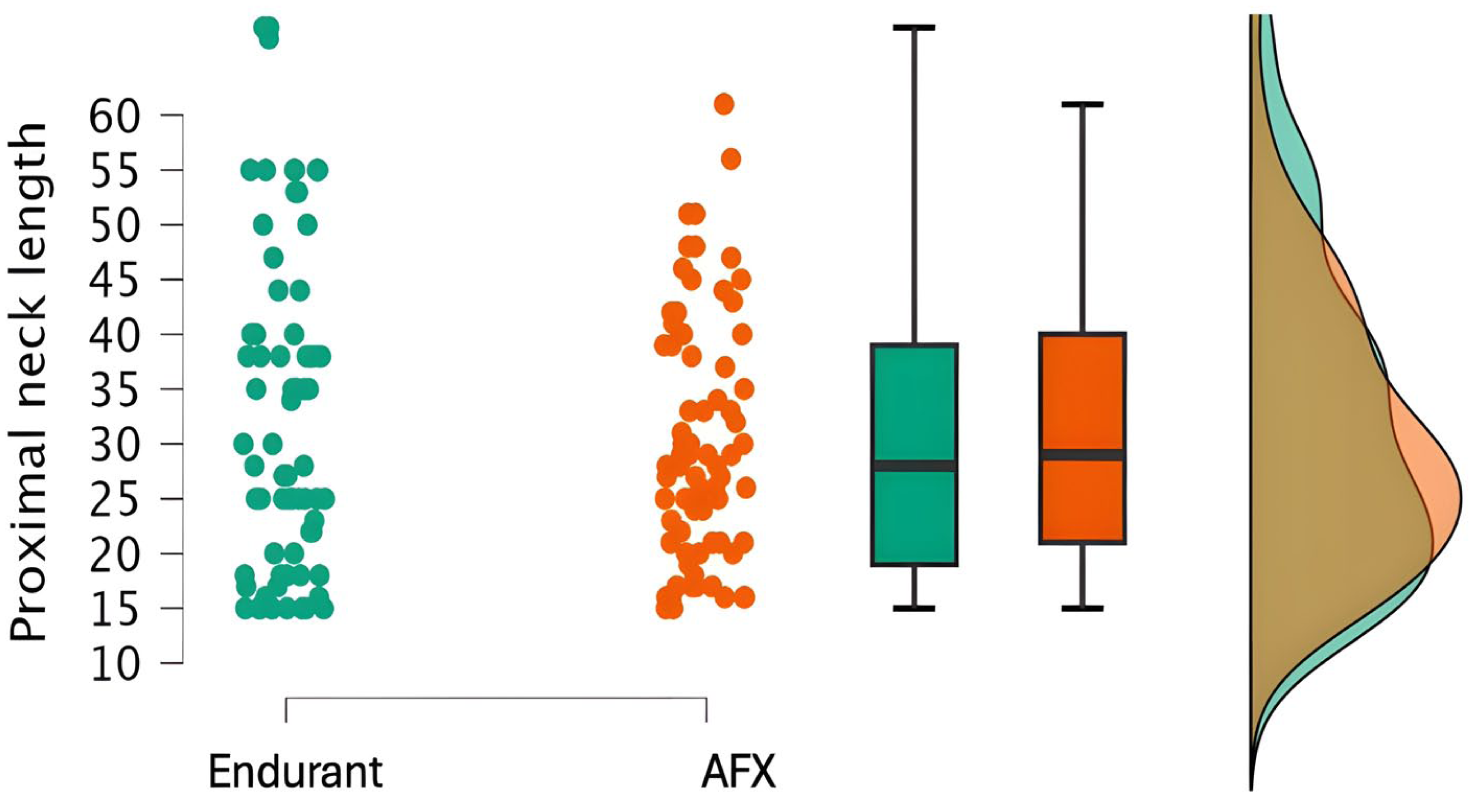
Post-matching proximal aortic neck comparison.
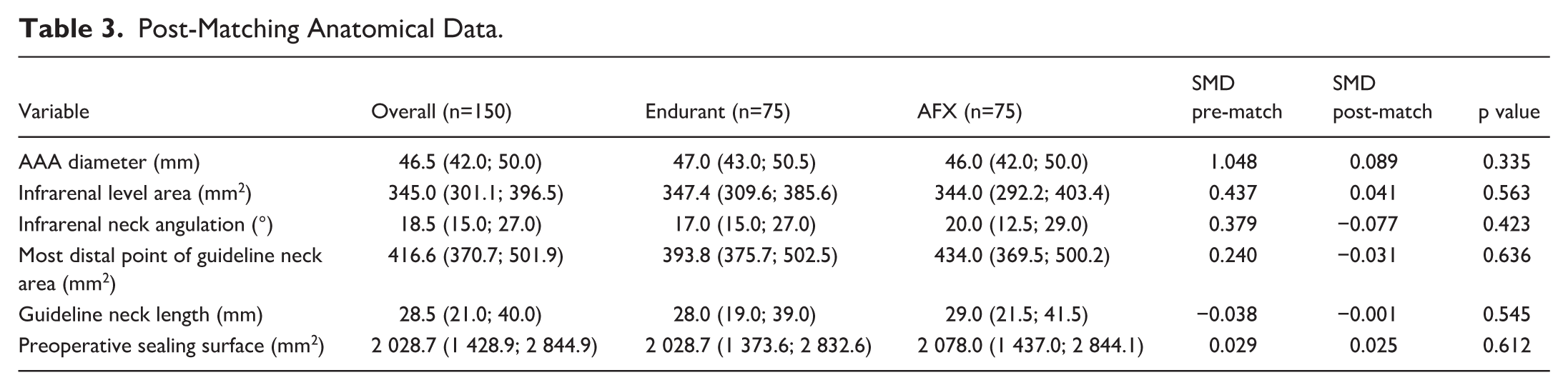
Post-matching anatomical data are reported in Table 3.
Post-Matching Anatomical Data.
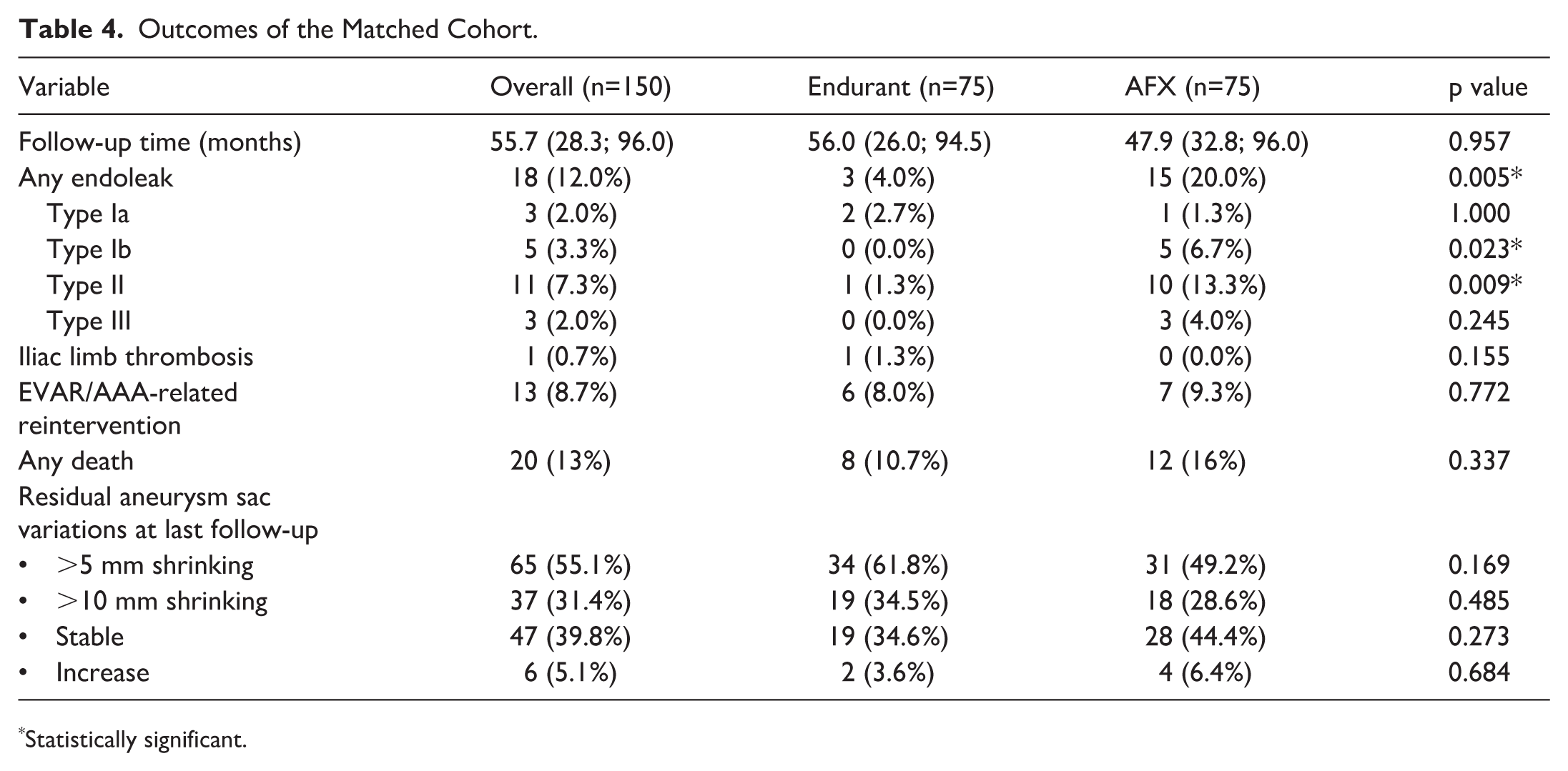
Mid-term outcomes of the matched cohort are reported in Table 4.
Outcomes of the Matched Cohort.
Statistically significant.
After matching, 43 (57.3%) AFX patients showed a RASZ longer than the neck, opposed to 20 (26.6%) Endurant patients (p<0.001). Twenty-nine (38.7%) patients from the AFX cohort had RASZ shorter than the predicted neck, opposed to 55 (73.3%) in the Endurant group (p<0.001). Exact correspondence between anatomical neck length and RASZ length occurred in 3 patients (3 AFX and 0 Endurant). Detailed RASZ and TASZ-RASZ differences in the matched cohort are reported in Table 5. Compared RASZ/TASZ length difference graphs are reported in Figure 5.
Post-Matching RASZ Details and TASZ/RASZ Comparison.
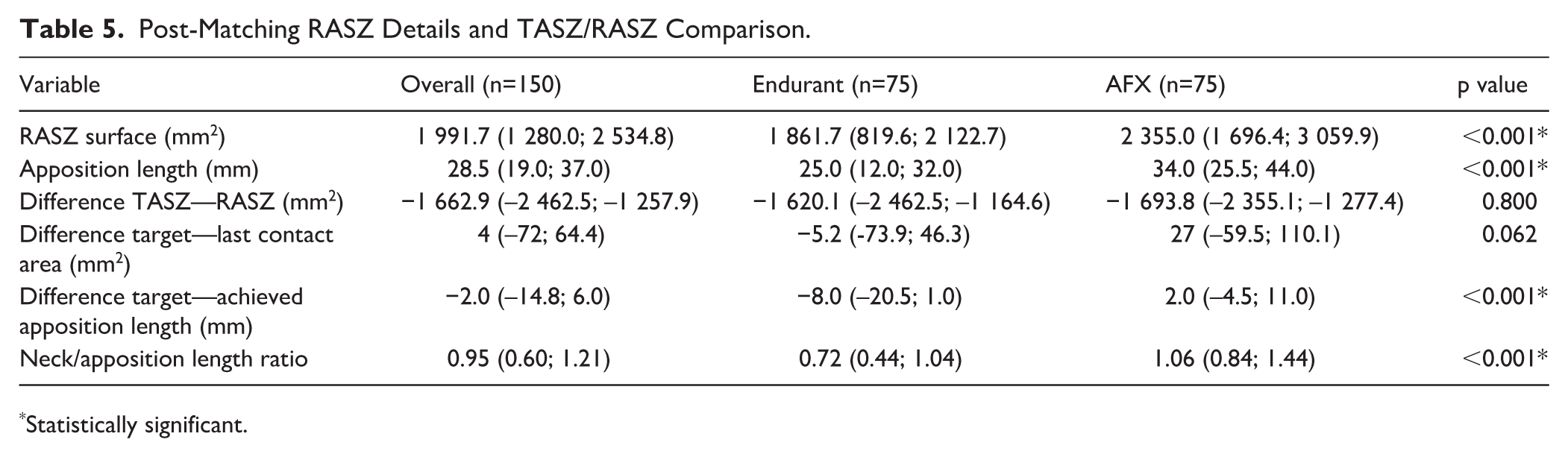
Statistically significant.
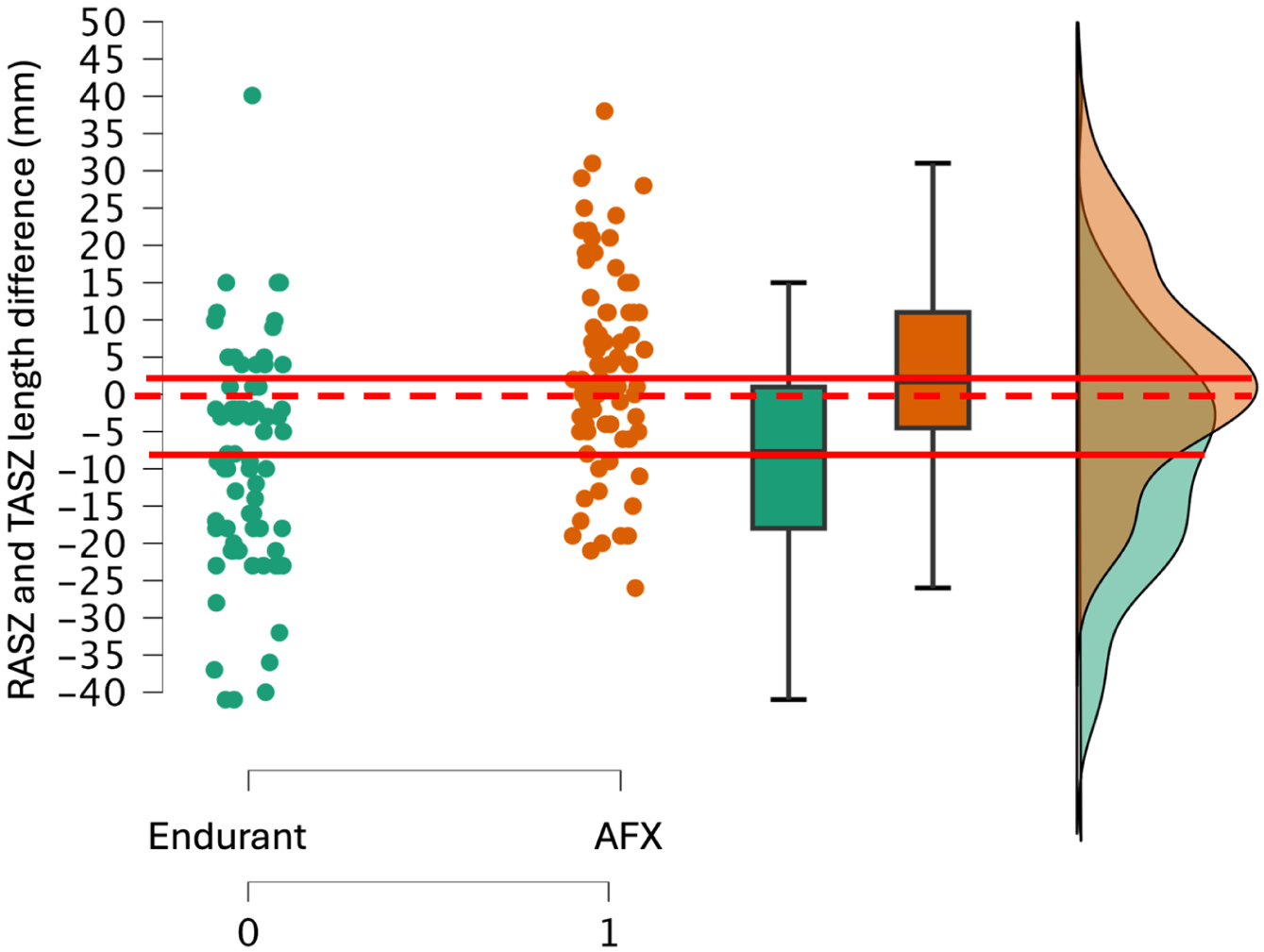
Post matching TASZ/RASZ length comparison in the study groups.
The median neck/apposition ratio was consistently higher in the AFX group (p<0.001). Endurant showed a median shortfall of −8 mm (IQR=−20.5 to +1 mm), whereas AFX exhibited a median surplus of +2 mm (IQR=−4.5 to +11 mm; p<0.001). In a multivariable linear regression model including device type, oversizing, and neck slope (entered simultaneously as covariates), all 3 variables independently predicted the neck/apposition ratio, with device type (β=0.521, p<0.001), neck slope (β=0.039, p=0.004), and oversizing (β=0.365, p=0.003); the overall model was statistically significant (adjusted R2=0.28, p<0.001).
AFX grafts were associated with an average +0.34 increase in the neck/apposition length ratio compared with Endurant (p<0.001), while oversizing also contributed positively (β=0.22, p=0.005). The same pattern was observed in the whole cohort (β=1.3±0.3, p<0.001).
Discussion
Our study shows the PSZ achieved after EVAR is device-dependent rather than purely anatomy-driven. In anatomically-matched patients, AFX achieved a significantly longer and larger RASZ than Endurant. Although neck morphology influenced sealing behavior, inclusion of neck slope as an added index to capture conicity did not attenuate the device-dependent effect.
RASZ is therefore influenced by each device’s fixation strategy, oversizing, and conformational design. Endurant relies on radial force and suprarenal fixation to achieve proximal sealing, 14 whereas AFX employs an anatomical fixation strategy with a conformable external fabric. 22
Our patients had markedly different anatomies, which is most likely a consequence of different IFUs for the 2 stent-graft systems (10mm neck length for Endurant and 15 mm for AFX, among others). Data on oversizing confirm that the different sealing behaviors of AFX is not solely attributable to more aggressive oversizing but reflects inherent design differences. Importantly, while oversizing contributes to sealing behavior, excessive oversizing beyond device-specific IFU recommendations is known to increase the risk of adverse mechanical phenomena such as graft infolding; therefore, the present findings should be interpreted within the context of guideline- and IFU-compliant sizing.
Our results also question the traditional “neck length” paradigm in EVAR planning. Historically, an infrarenal neck of ≥10 or 15 mm has been the cornerstone for graft selection and IFU compliance. Current stent-grafts, like AFX (and Endurant with additional endoanchors 13 ), show that circumferential apposition may extend beyond the formal neck. A fixed neck length criterion may be outdated for contemporary EVAR—a more nuanced, device-specific appraisal of the proximal sealing might be helpful.
Future preoperative planning and post-EVAR evaluation might incorporate device-tailored sealing zone analysis, not just neck length, to assess complete circumferential apposition. RASZ length thresholds are likely device-specific, underscoring the need for larger studies to define optimal sealing requirements for each stent-graft system. Our findings also highlight a critical issue: the infrarenal segment just below the lowest renal artery, traditionally considered a reliable landing zone, may in some patients already represent the early aneurysmal transition, with structural weakness despite a normal appearance on imaging. This warrants caution when evaluating the proximal seal and supports longitudinal studies assessing RASZ evolution over time. This study focuses primarily on early RASZ rather than its evolution and long-term outcomes. Postoperative RASZ may provide complementary information to the preoperative TASZ, as it reflects the achieved circumferential seal at the start of follow-up. 5
In the matched cohort, proximal Type Ia endoleaks were rare (<5%) and evenly distributed between devices. While encouraging, this low event rate limits statistical power to correlate RASZ parameters with clinical failure, and the findings should therefore be interpreted as hypothesis-generating. We also report a lower overall reintervention rate for the AFX group. Notably, the type IIIb endoleaks of the previous “Strata” fabric overshadow AFX’s otherwise excellent safety profile. In the matched cohort, the AFX exhibited a higher endoleak rate, which is primarily due to type II and type III endoleaks. Since the introduction of the “Duraply” fabric in 2016, the incidence of type III endoleaks has reduced, although sporadic cases of Type III endoleak have still been reported, 23 highlighting the need for continued surveillance.
Study Limitations
This study has several limitations. Its retrospective, single-center design and the modest matched sample size limit the generalizability of the findings and statistical power for rare events such as type Ia endoleak. Despite strict propensity-score matching (all SMD≤0.10), unmeasured confounders and technical variability may persist. The assessment of apposition in AFX cases was constrained by the absence of radiopaque fabric markers, possibly leading to conservative RASZ estimates. The present analysis focused on the guideline-defined PSZ; morphometric characterization of the aortic segment distal to TASZ was beyond the scope of this study and warrants dedicated investigation. The smaller median AAA diameter in the matched cohort reflects historical device selection and the constraints of anatomical matching. Finally, the analysis focused on early postoperative sealing; longer follow-up and multicenter validation are needed to determine whether the observed device-specific sealing patterns translate into improved long-term durability.
Conclusion
In anatomically matched patients, the AFX unibody graft achieved a significantly longer and larger PSZ compared with the modular Endurant graft, suggesting that the seal achieved after EVAR is strongly influenced by device design and oversizing strategy rather than by neck length alone. These observations highlight that the PSZ is not a fixed anatomic entity but a dynamic, device-dependent outcome.
Supplemental Material
sj-docx-1-jet-10.1177_15266028261452810 – Supplemental material for Beyond the Neck: Device-Dependent Proximal Sealing After EVAR—A Propensity-Matched Comparison of AFX and Endurant
Supplemental material, sj-docx-1-jet-10.1177_15266028261452810 for Beyond the Neck: Device-Dependent Proximal Sealing After EVAR—A Propensity-Matched Comparison of AFX and Endurant by Giulio Accarino, Mattia Sica, Giancarlo Accarino, Enrico Cappello, Umberto Marcello Bracale and Jean-Paul P. M. de Vries in Journal of Endovascular Therapy
Footnotes
Author Contributions
All authors contributed to substantial contributions to the conception and design, or acquisition of data, or analysis and interpretation of data; drafting the article or revising it critically for important intellectual content; and final approval of the version to be published.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.