
Abstract
Purpose:
Baseline lesion characteristics have been reported to be associated with vessel patency after drug-coated balloon (DCB) treatment for femoropopliteal artery lesions. Intravascular ultrasound (IVUS) evaluation was also associated with vessel patency. The present study aimed to investigate whether the IVUS endpoints could predict the incidence of restenosis after DCB treatment, independent of classical risk factors.
Methods:
We retrospectively reviewed 111 patients with 147 consecutive femoropopliteal (FP) lesions treated with IVUS-guided endovascular therapy (EVT) using DCB between 2021 and 2023. We assessed the association between 1-year restenosis and sufficient postprocedural lumen area measured by IVUS, in addition to the classical risk score, including no below-the-knee runoff, a history of EVT, distal reference vessel diameter of <5 mm, Peripheral Arterial Calcium Scoring System grade 4, chronic total occlusion (CTO), popliteal segments, low-dose DCB, and residual stenosis. The sufficient lumen area was defined as that ≥12.7 mm2.
Results:
The chronic limb-threatening ischemia, CTO, and hemodialysis rates were 23%, 48%, and 16%, respectively. Restenosis was found in 38 lesions (26%) at 1 year. The Cox multivariate analysis showed that the classical risk score was an independent predictor of restenosis (hazard ratio [HR] = 1.45, per 1.0, P = .018), whereas sufficient lumen area was protective against restenosis (HR = 0.40, P = .015).
Conclusion:
The IVUS evaluation might be associated with restenosis onset after DCB treatment, independent of the classical risk factors.
Clinical Impact
In femoropopliteal endovascular therapy, we demonstrate that intravascular ultrasound (IVUS)-derived minimum lumen area (MLA) is an independent predictor of restenosis beyond the established predictors of patency after coated balloon angioplasty (POPCORN) risk factors. Incorporating MLA into periprocedural assessment may help with risk stratification, device selection, and planning of postprocedural surveillance.
Keywords
Introduction
The current guidelines have stated that drug-coated balloons (DCBs) are the first-line devices of endovascular therapy (EVT) for femoropopliteal artery (FPA) disease. 1 A previous large-scale prospective registry demonstrated an acceptable primary patency rate of 84.5%. 2 This registry identified the predictors for restenosis after DCB treatment, which included no below-the-knee (BTK) runoff, a history of EVT, small vessels, calcification, chronic total occlusion (CTO), popliteal lesions, types of DCB, and residual stenosis.
Intravascular ultrasound (IVUS), a catheter-based imaging modality, provides more detailed insights into vessel dimensions and plaque characteristics as compared to angiography.3,4 Additionally, IVUS reveals procedural findings such as the wire-crossing route in CTO lesions, the lumen area after balloon dilatation and stent implantation, and modification of the calcification and plaque following the use of atherectomy devices. Recently, randomized controlled trials have shown that IVUS guidance improved the outcomes at 12 months following EVT using DCB in FPA lesions in terms of primary patency and freedom from clinically driven target lesion revascularization, as compared with standard angiography-guided angioplasty. 5 Although IVUS is the established modality for assessing lesion morphology in limb arteries, only a few studies have validated the conventional risk factors and IVUS parameters in DCB treatment. Hence, the present study aimed to investigate whether the IVUS endpoints could predict the incidence of restenosis after DCB treatment, independent of the conventional risk factors.
Materials and Methods
Study Participants
This single-center retrospective observational study enrolled patients with symptomatic lower limb artery disease (Rutherford categories 2-5) who underwent IVUS-guided EVT using DCB for FPA lesions between 2021 and 2023. Patients with (1) non-atherosclerotic disease, (2) life expectancy of <1 year, (3) acute limb ischemia, and (4) aneurysmal lesions were excluded. We reviewed 111 consecutive patients with 147 FPA lesions who underwent EVT using both DCB and IVUS.
The study protocol was approved by the local ethics committee of the participating institution, and the study was conducted in accordance with the guidelines stipulated in the Declaration of Helsinki. The requirement for obtaining informed consent from the patients was waived due to the retrospective study design, in which the existing medical records were used. Alternatively, patients can opt out of the study. Relevant information regarding the study is available to the public in accordance with the Ethical Guidelines for Medical and Health Research Involving Human Subjects.
Procedures
Following local anesthesia, a 4.5 to 7.0F guiding sheath was inserted into the ipsilateral or contralateral common femoral artery. In the CTO lesions, intraplaque crossing was first attempted using a 0.018- or 0.014-inch guidewire and a microcatheter. If unsuccessful, a subintimal approach was implemented by forming a loop at the tip of the hydrophilic guidewire. The bidirectional approach was performed as needed. Vessel preparation was performed using standard balloon angioplasty. Semi-compliant, non-compliant, scoring, or high-pressure balloons were selected at the operator’s discretion depending on lesion characteristics and expansion resistance. Balloon diameter was generally selected according to the distal reference vessel diameter (RVD) assessed by IVUS, and additional post-dilatation was performed when necessary to achieve adequate luminal expansion. After successful balloon dilatation, 3 DCBs—IN.PACT Admiral (Medtronic Invatec, Frauenfeld, Switzerland) with 3.5 μg/mm2 of paclitaxel, Lutonix (BD/Bard, Tempe, Arizona) with 2.0 μg/mm2 of paclitaxel, or Ranger (Boston Scientific, Marlborough, Massachusetts) with 2.0 μg/mm2 of paclitaxel—were used at the operator’s discretion. Lutonix was defined as a first-generation low-dose DCB. 2 When necessary, bailout stenting was performed to treat vessel dissection and recoil at the operator’s discretion. Information regarding vessel preparation, including balloon type, balloon diameter, maximum inflation pressure, and inflation duration, was retrospectively collected from procedural records. Given that atherectomy devices and intravascular lithotripsy were not commercially available in our country during the study period, these devices were not used in the present study.
Analysis, Measurement, and Definition of Intravascular Ultrasound
Baseline and postprocedural IVUS examinations were performed using a Vision/Eagle Eye Platinum catheter (Philips Volcano, Rancho Cordova, California) or AnteOwl WR/Navifocus WR/AltaView (TERUMO, Tokyo, Japan), which was pulled back through the lesion for image capture. The DCB size was adjusted to the distal vessel diameter by a balloon-to-vessel ratio of 1:1. The reference segments were defined as the most normal-looking cross-sections within the same arterial segment (typically <20 mm distal to the target lesion) but proximal to any large side branch. 4 The cross-sectional area (CSA) of the external elastic membrane (EEM) was measured at the distal reference segment. 4 After DCB treatment, IVUS images were analyzed to determine the minimum lumen area (MLA), defined as the luminal area obtained by tracing the vessel lumen at the site with the smallest lumen identified on IVUS within the treated segment according to the expert consensus document. 6 When vessel dissection was present, the area continuous with the true lumen was included in the MLA measurement, whereas the dissection cavity itself was excluded. Subintimal wire passage was also assessed using IVUS according to the same consensus criteria, based on the guidewire position relative to the medial and adventitial layers on cross-sectional imaging. All IVUS measurements were performed by a single experienced observer who was blinded to procedural details and clinical outcomes. Residual stenosis after the procedure was assessed on the final angiographic images using quantitative vessel analysis and defined as >50% diameter stenosis relative to the RVD. Intra-observer reproducibility of MLA measurements was evaluated in a randomly selected subset of lesions, and the results are reported in the Supplemental Table S1. A sufficient lumen area was defined as an MLA ≥12.7 mm2. 6
Study Definitions
Primary patency was defined as the absence of both restenosis and revascularization in the treated lesion. Restenosis was defined as a peak systolic velocity ratio of >2.4 on duplex ultrasonography or >50% diameter stenosis or occlusion on follow-up angiography. 7 Color Doppler ultrasonography was performed routinely at 6 and 12 months after EVT to evaluate vascular patency, as recommended by the reports from the Society for Vascular Surgery. 8 Peripheral Arterial Calcium Scoring System (PACSS) classification was recorded using granular categories (grades 0-4) based on fluoroscopic assessment, and severe calcification was defined as grade 4. 9 The present study adopted the typical predictors for restenosis following DCB treatment according to the previous large-scale registry, including no BTK runoff, a history of EVTs, distal RVD of <5 mm, PACSS grade 4, CTO, popliteal lesion, low-dose DCB, and residual stenosis. The BTK runoff was categorized according to the number of patent tibial vessels (0-1 or 2-3 vessels) as assessed by angiography. The distal RVD was measured by angiography. 2 The predictors of patency after coated balloon angioplasty (POPCORN) registry risk score (range = 0-6) were calculated according to the previously reported criteria. Receiver operating characteristic (ROC) analysis was performed to determine the optimal cut-off value of the POPCORN risk score for predicting 1-year restenosis.
Statistical Analysis
Categorical variables were reported as percentages and were compared using the chi-square test or Fisher’s exact test. Continuous variables were expressed as mean ± standard deviation and were assessed using the t-test. All baseline values and procedural characteristics were prescreened using univariate logistic regression analysis to identify the independent predictors of restenosis. The predictors of restenosis after DCB treatment were evaluated using the Cox proportional hazards regression model. The simple risk score from the POPCORN study (ie, the number of accumulated independent risk scores) was used to evaluate the multivariate model. The ROC curve analysis was performed to determine the optimal cut-off value of the POPCORN risk score for predicting 1-year restenosis. The time-to-event outcomes were analyzed using the Kaplan-Meier method and subsequently compared using the log-rank test. A probability value of P < .05 was considered statistically significant. JMP statistical software (version 14.2.0; SAS Institute, Cary, North Carolina) was used to conduct all statistical analyses.
Results
Baseline Clinical and Lesion Characteristics
The baseline patient and lesion characteristics are summarized in Table 1. The mean age was 74.9 ± 8.4 years, and 77.4% (n = 86) of the study participants were male. The prevalence values of diabetes mellitus and chronic kidney disease on dialysis were 60.4% and 16.2%, respectively. Approximately one-fourth of the patients presented with chronic limb-threatening ischemia (CLTI; 22.5%, n = 25). The mean RVD and lesion length were 5.4 ± 0.77 mm and 23.2 ± 9.8 cm, respectively. The proportions of CTO and severe calcification were 47.6% and 12.9%, respectively.
Baseline Characteristics.
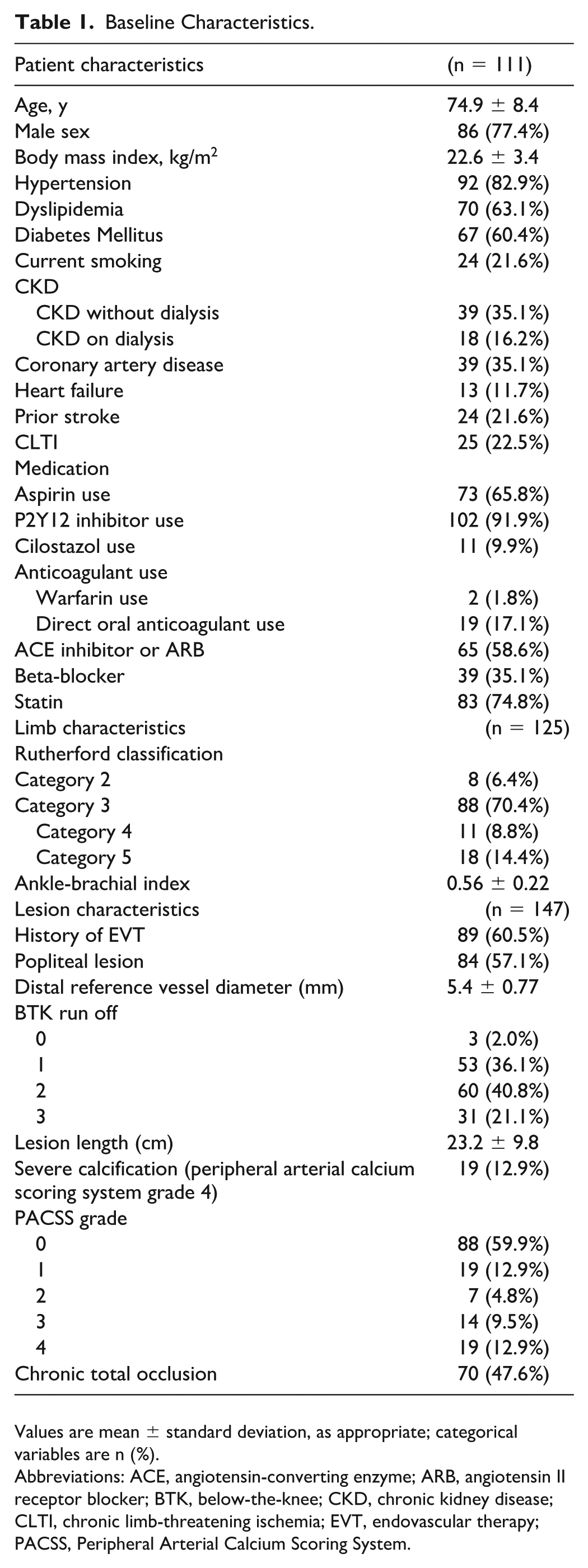
Values are mean ± standard deviation, as appropriate; categorical variables are n (%).
Abbreviations: ACE, angiotensin-converting enzyme; ARB, angiotensin II receptor blocker; BTK, below-the-knee; CKD, chronic kidney disease; CLTI, chronic limb-threatening ischemia; EVT, endovascular therapy; PACSS, Peripheral Arterial Calcium Scoring System.
Procedural Characteristics
Table 2 summarizes the procedural findings. The EVT was technically successful in all patients without arterial perforation or distal embolization after DCB treatment. The comparison of baseline characteristics and procedural findings between lesions treated with each DCB was presented in Supplemental Table S2. Significant differences among the 3 DCB groups were observed for male sex, chronic kidney disease status, aspirin use, popliteal lesion involvement, distal RVD, and lesion length.
Procedural Findings.
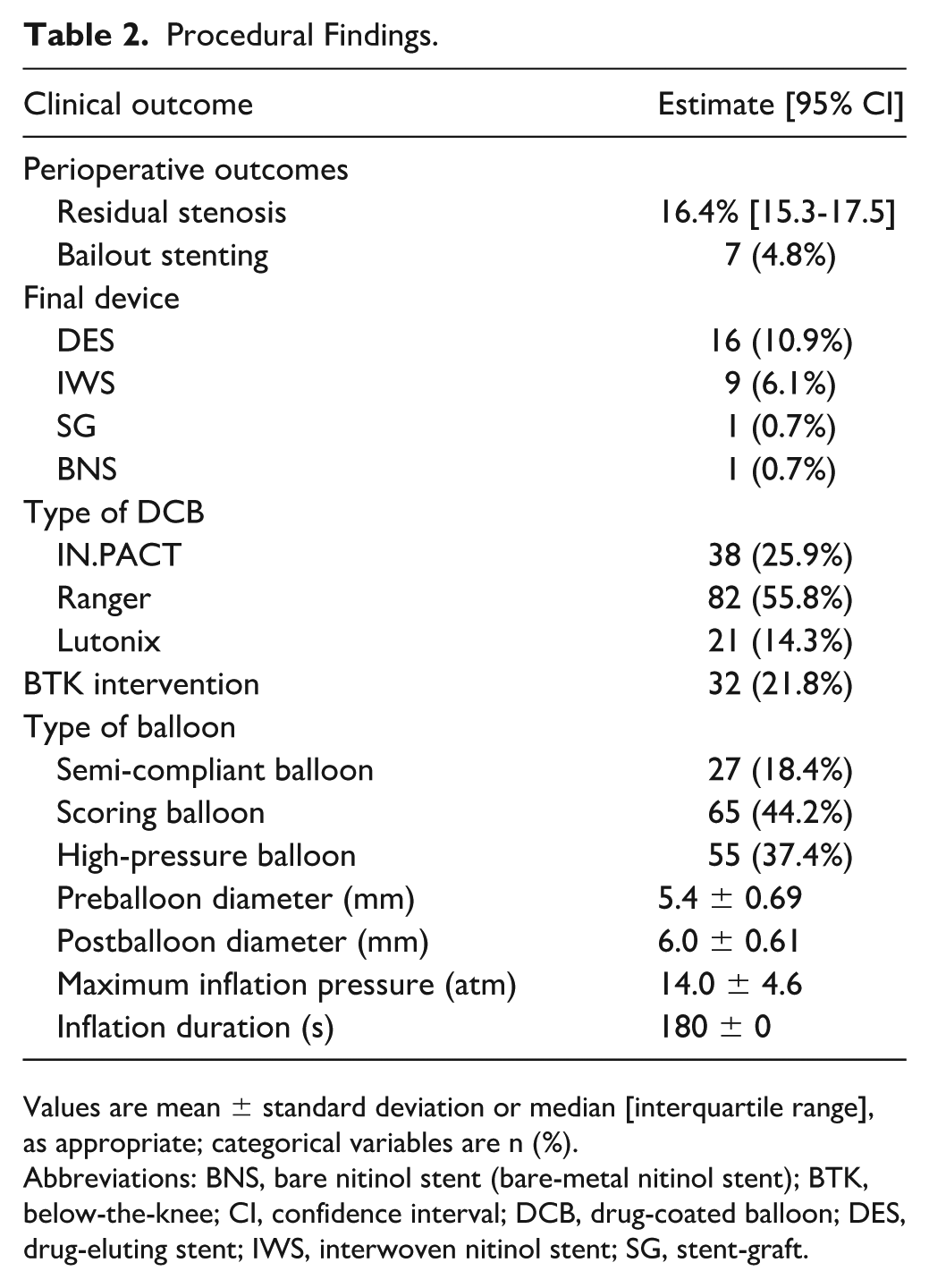
Values are mean ± standard deviation or median [interquartile range], as appropriate; categorical variables are n (%).
Abbreviations: BNS, bare nitinol stent (bare-metal nitinol stent); BTK, below-the-knee; CI, confidence interval; DCB, drug-coated balloon; DES, drug-eluting stent; IWS, interwoven nitinol stent; SG, stent-graft.
Postprocedural Intravascular Ultrasound Findings
The pre- and postprocedural IVUS findings are summarized in Table 3. The mean values of distal and proximal EEM CSA were 28.5 ± 9.2 and 35.0 ± 11.3 mm2, respectively. The distributions of the calcification angle assessed by IVUS were as follows: no calcification in 52 lesions (35.4%), 0° to 90° in 36 lesions (24.5%), 91° to 180° in 25 lesions (17.0%), 181° to 270° in 14 lesions (9.5%), and 271° to 360° in 20 lesions (13.6%). The mean MLA after DCB dilatation was 17.8 ± 5.4 mm2. Sufficient lumen area, defined as a postprocedural MLA >12.7 mm2 measured by IVUS, was achieved in 83.0% of lesions. Variables associated with achieving sufficient MLA in univariate analysis are summarized in Supplemental Table S3. Sufficient MLA was associated with male sex, chronic kidney disease, coronary artery disease, heart failure, CLTI, the Rutherford classification, baseline ankle-brachial index, a history of EVT, popliteal lesion involvement, and distal RVD. In contrast, procedural variables related to vessel preparation, including balloon type and inflation duration, were not significantly different between lesions with and without sufficient MLA.
Pre- and Postprocedural IVUS Findings.
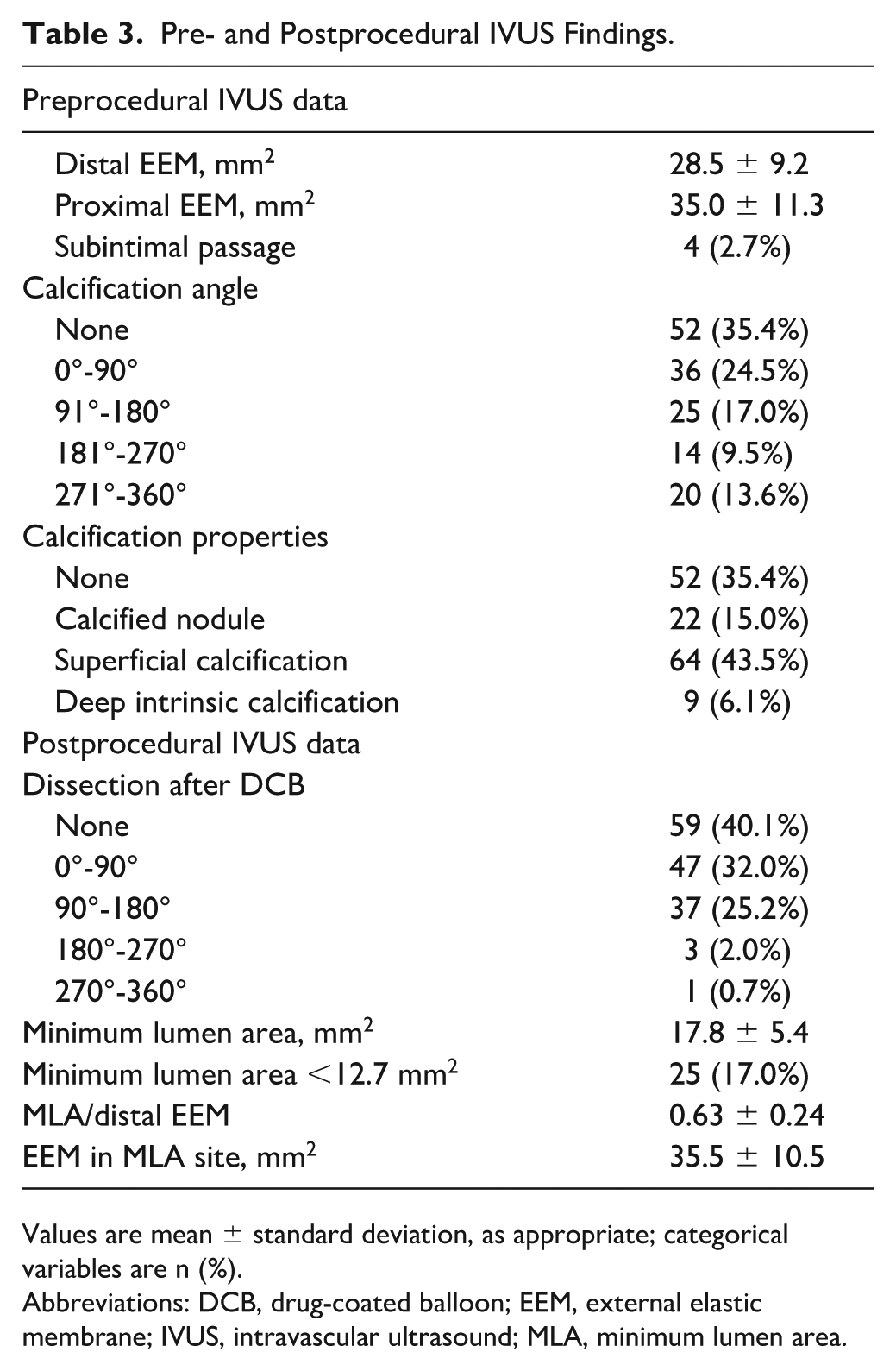
Values are mean ± standard deviation, as appropriate; categorical variables are n (%).
Abbreviations: DCB, drug-coated balloon; EEM, external elastic membrane; IVUS, intravascular ultrasound; MLA, minimum lumen area.
Clinical Outcomes
Restenosis at 1 year/12 months was detected in 38 cases (25.9%). The Kaplan-Meier estimate of 1-year primary patency, ie, freedom from restenosis, was 74.2% (95% confidence interval [CI] = 66.5%-80.5%) (Figure 1).
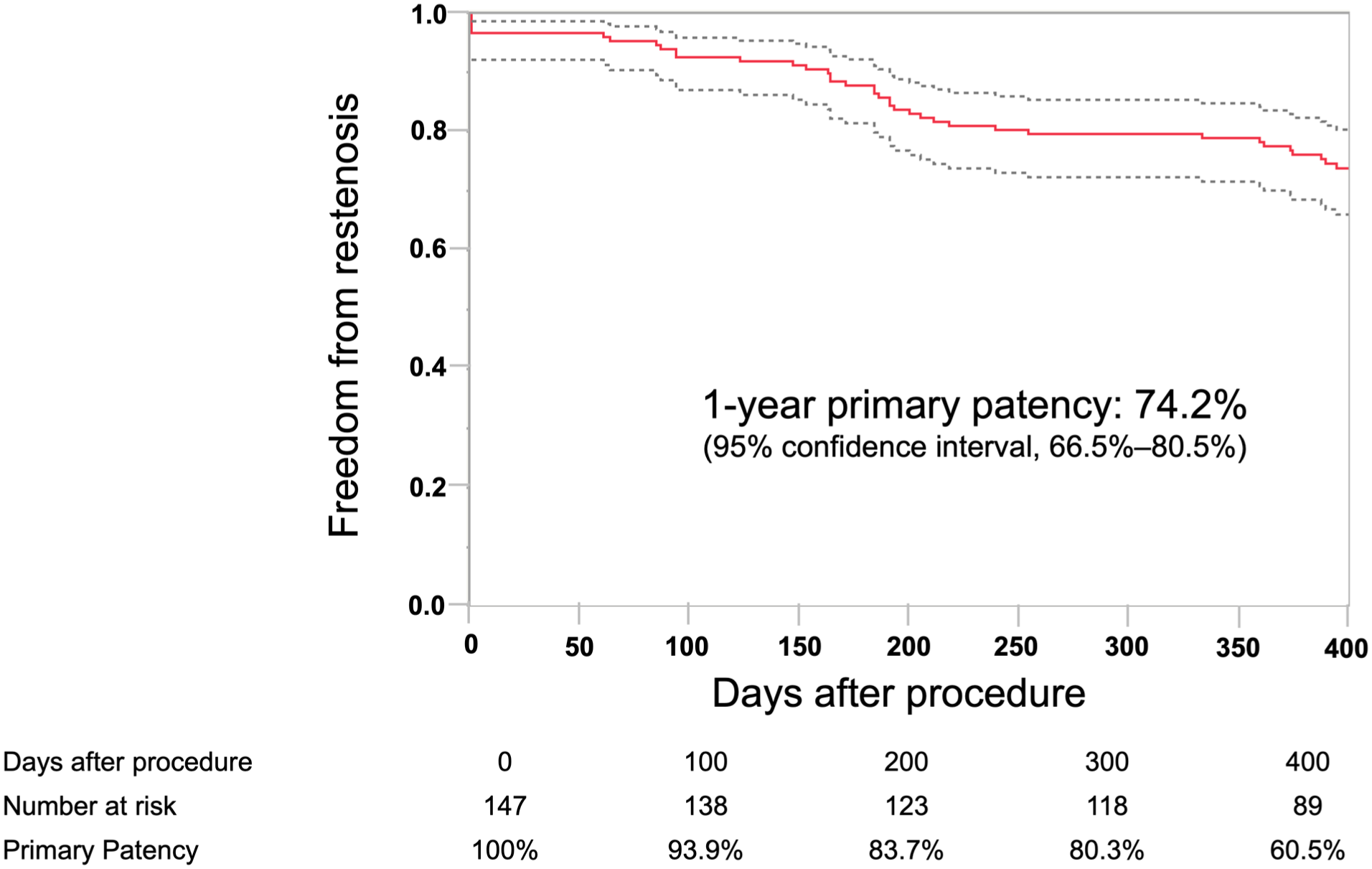
Primary patency after femoropopliteal EVT. Dotted lines indicate 95% confidence intervals. CI, confidence interval; EVT, endovascular therapy; MLA, minimum lumen area.
Predictors of Restenosis
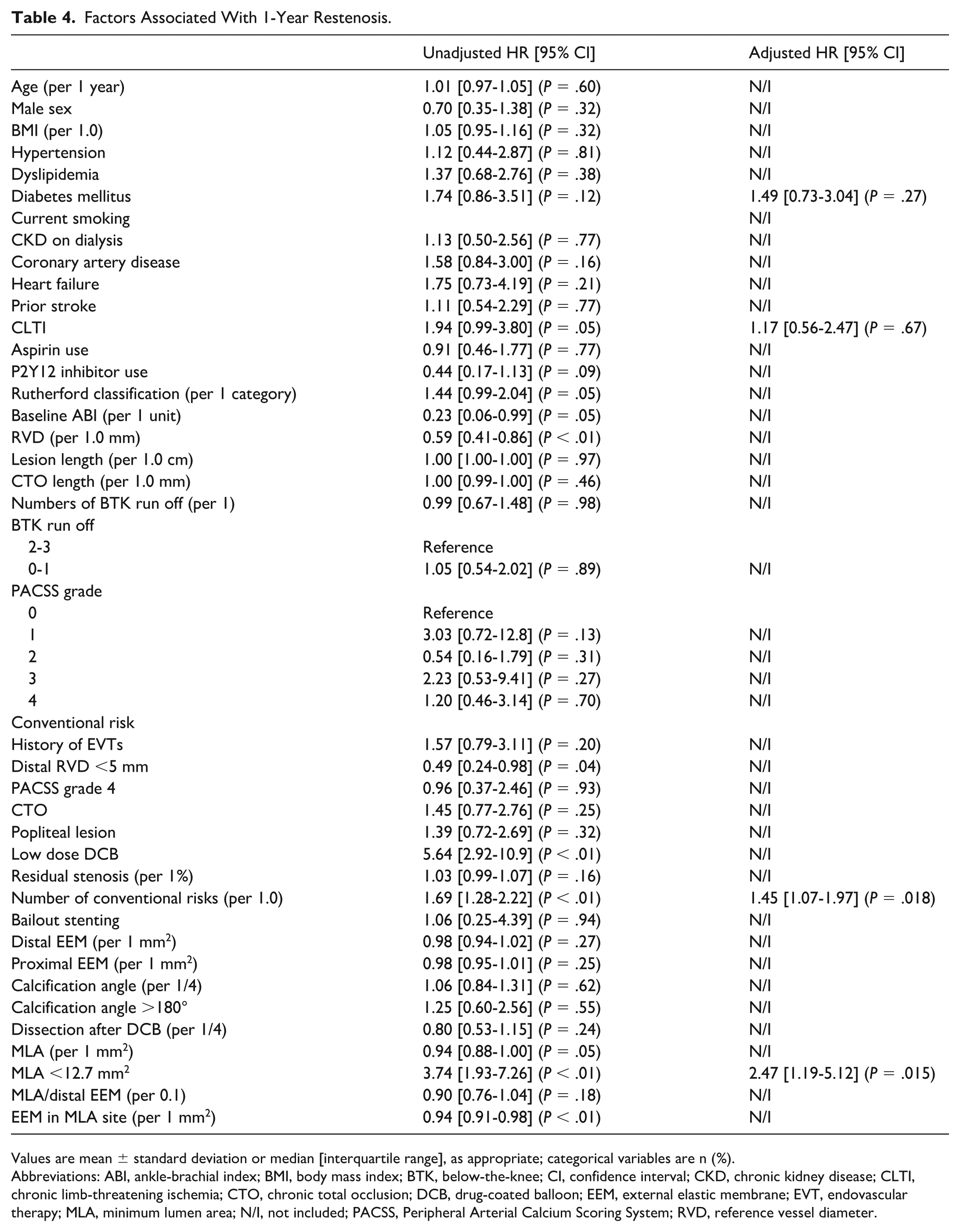
The ROC analysis identified a POPCORN risk score of 3 as the optimal cut-off value for predicting 1-year restenosis (area under the curve [AUC] = 0.65, P = .0007). Accordingly, a score ≥3 was defined as high risk for the subsequent analyses. As shown in Table 4, restenosis after DCB treatment was independently associated with a higher POPCORN risk score (adjusted hazard ratio [HR] = 1.45 per 1-point increase; 95% CI = 1.06-1.97; P = .018). Furthermore, sufficient postprocedural MLA measured by IVUS was a protective factor against restenosis (HR = 0.40, 95% CI = 0.19-0.84; P = .015). In contrast, the relative expansion parameter defined as MLA divided by the distal reference EEM area was not significantly associated with primary patency (P = .18). Similarly, IVUS-derived calcification angle ≥180° was not significantly associated with restenosis (P = .55).
Factors Associated With 1-Year Restenosis.
Values are mean ± standard deviation or median [interquartile range], as appropriate; categorical variables are n (%).
Abbreviations: ABI, ankle-brachial index; BMI, body mass index; BTK, below-the-knee; CI, confidence interval; CKD, chronic kidney disease; CLTI, chronic limb-threatening ischemia; CTO, chronic total occlusion; DCB, drug-coated balloon; EEM, external elastic membrane; EVT, endovascular therapy; MLA, minimum lumen area; N/I, not included; PACSS, Peripheral Arterial Calcium Scoring System; RVD, reference vessel diameter.
Combined Impact of Predictors of Patency After Coated Balloon Angioplasty Risk and Postprocedural Minimum Lumen Area
To further explore the combined impact of baseline risk and procedural lumen optimization, patients were stratified according to POPCORN risk status (≥3 vs 0-2) and postprocedural MLA. The Kaplan-Meier analysis demonstrated significant differences in 1-year primary patency among the 4 groups (log-rank P < .0001; Figure 2), showing a stepwise gradient in patency across the groups. The Kaplan-Meier estimates of 1-year primary patency were 86.4% in the low POPCORN risk with sufficient MLA group (n = 88), 75.8% in the high POPCORN risk with sufficient MLA group (n = 33), 66.7% in the low POPCORN risk with insufficient MLA group (n = 12), and 35.7% in the high POPCORN risk with insufficient MLA group (n = 14), respectively.
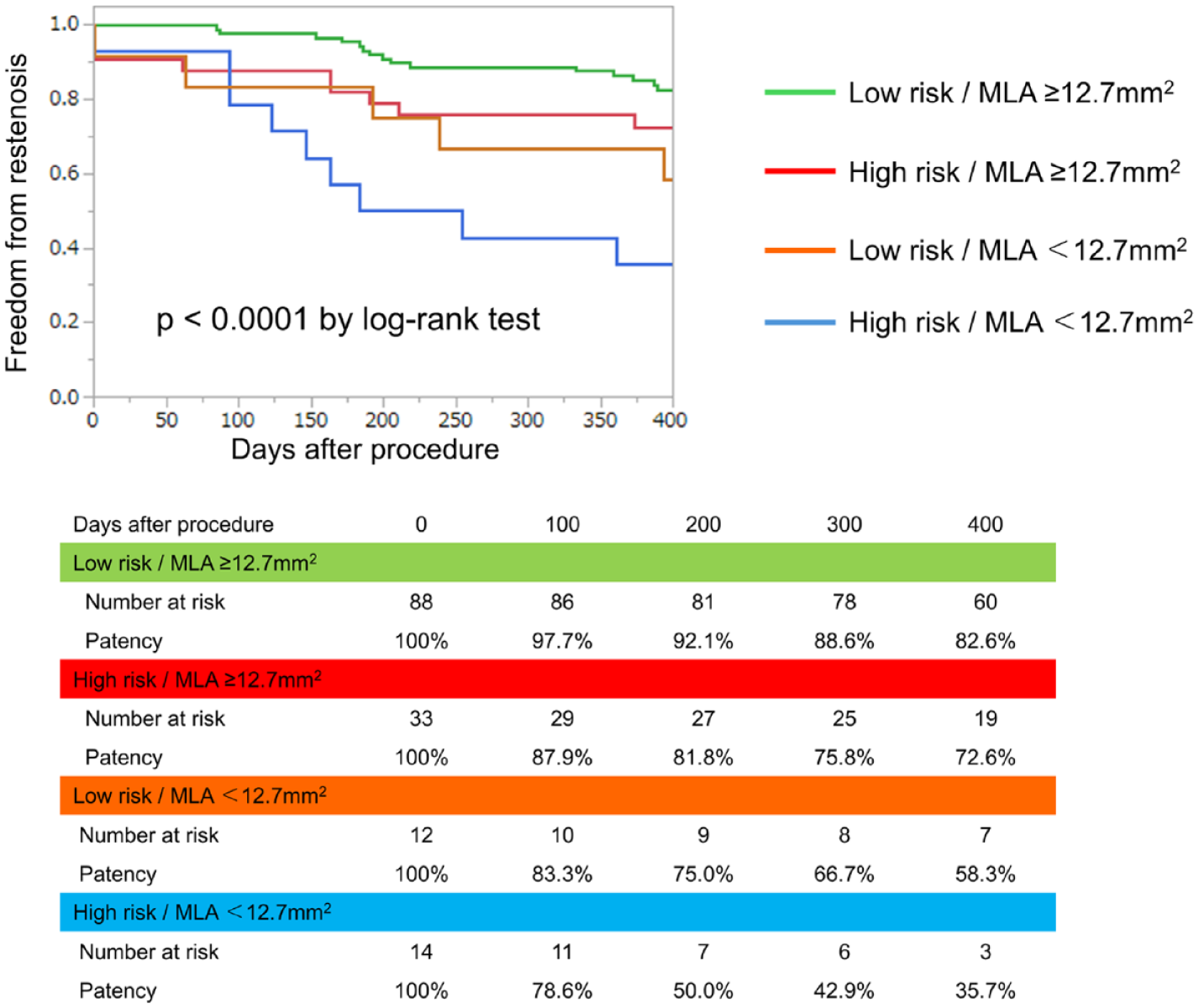
Kaplan-Meier curves for 1-year primary patency according to combined POPCORN risk status and postprocedural MLA. Patients were stratified into 4 groups based on POPCORN risk (≥3 vs 0-2) and postprocedural MLA (≥12.7 mm2 vs <12.7 mm2). The Kaplan-Meier estimates of 1-year primary patency were 86.4%, 75.8%, 66.7%, and 35.7% in the 4 groups, respectively (log-rank P < .0001). MLA, minimum lumen area; POPCORN, predictors of patency after coated balloon angioplasty (color print requested).
Discussion
The present study demonstrated that both the conventional risk score and sufficient postprocedural lumen area measured by IVUS were significant predictors of restenosis after EVT with DCB. Although the POPCORN risk score has been previously established as a predictor of restenosis, our findings suggest that incorporating IVUS-derived MLA measurements may provide additional prognostic value. Furthermore, stratified analysis combining baseline POPCORN risk and postprocedural MLA demonstrated a clear stepwise difference in primary patency across the 4 groups. Notably, patients with high baseline risk but sufficient MLA exhibited better outcomes than those with low baseline risk but insufficient MLA. These findings suggest that procedural lumen optimization may modify the impact of baseline risk factors, highlighting the clinical relevance of achieving adequate expansion irrespective of inherent patient risk.
The POPCORN study identified the risk factors for restenosis following DCB treatment, including the anatomical findings according to the baseline characteristics, procedural findings, and angiographic evaluation. However, for measuring the lumen area, angiography is often susceptible to several factors. Iida et al 10 demonstrated that angiography-assessed RVD was significantly smaller than IVUS-assessed RVD. This discrepancy was likely to occur in lesions with bilateral calcification, a history of stent implantation, and small RVD. These anatomical characteristics are often observed in FP lesions that are treated in the current DCB era, potentially leading to an inaccurate assessment of baseline lesion findings and postprocedural endpoints. The IVUS has been more reliable for evaluating the lesion morphology, as compared to angiography, especially the cross-sectional measurement of the lumen and vessel area. 4 Therefore, the integration of IVUS-derived parameters, including MLA and EEM measurements, may provide a more comprehensive assessment during the EVT procedure. Although a relative expansion parameter (MLA/distal reference EEM ratio) was explored to account for vessel size variation, it did not demonstrate superior predictive performance compared with absolute MLA in this cohort. These findings suggest that absolute postprocedural lumen area may represent a more practical procedural target in FPA lesions. 6 This concept is analogous to coronary stent implantation, where intravascular imaging–derived minimal stent area is a well-established determinant of long-term outcomes. 11 These observations support the importance of adequate luminal expansion as a procedural target in EVT. Notably, although the POPCORN study reported an IVUS usage rate of 73.4%, detailed evaluation of IVUS might improve DCB treatment.
Importantly, the present study focused on MLA measured by IVUS after the procedure rather than IVUS use itself. Our findings suggest that achieving adequate lumen expansion assessed by IVUS may be important for long-term patency, even after accounting for baseline restenosis risk represented by the POPCORN risk score. Achieving sufficient luminal expansion is essential for long-term vessel patency, and IVUS guidance may facilitate optimal balloon sizing and detect incomplete dilatation, which should be treated with scaffold implantation. In our cohort, a larger postprocedural MLA measured by IVUS was associated with a lower restenosis risk, suggesting that the IVUS-derived MLA can serve as a practical indicator of procedural success. Future studies should prospectively validate whether the specific MLA thresholds can guide the treatment strategies and improve the clinical outcomes of DCB-based EVT.
The present study has several limitations. First, the retrospective nature of the analysis may introduce selection bias, and the sample size was relatively small. Second, angiographic and IVUS assessments were not performed by an independent core laboratory, and different IVUS systems were used across cases; moreover, MLA measurements were performed by a single observer. Third, the present study included only Asian patients, which may limit the generalizability of the findings. Finally, vessel preparation (including balloon types, balloon size, inflation pressure, and inflation duration) and the selection of DCB types were not standardized by a predefined protocol and were left to the operator’s discretion.
Conclusion
Our study data suggest that IVUS-derived MLA assessment may complement the existing risk models, such as the POPCORN risk score, by providing more accurate vascular measurements in DCB treatment for FPA lesions.
Supplemental Material
sj-docx-1-jet-10.1177_15266028261453007 – Supplemental material for The Utility of Intravascular Ultrasound Evaluation in Addition to the Conventional Risk Factors for Predicting Restenosis After Endovascular Therapy Using Drug-Coated Balloon in Femoropopliteal Artery Lesions
Supplemental material, sj-docx-1-jet-10.1177_15266028261453007 for The Utility of Intravascular Ultrasound Evaluation in Addition to the Conventional Risk Factors for Predicting Restenosis After Endovascular Therapy Using Drug-Coated Balloon in Femoropopliteal Artery Lesions by Hiroaki Akai, Kazunori Horie, Akiko Tanaka, Naho Itou and Norio Tada in Journal of Endovascular Therapy
Footnotes
Acknowledgements
The authors gratefully acknowledge the clinical and administrative staff of the Department of Cardiovascular Medicine at Sendai Kousei Hospital for their dedicated support of patient care and data collection.
Ethical Considerations
This study was approved by the local ethics committee. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Consent to participate
The requirement for informed consent was waived owing to the retrospective study design utilizing preexisting medical records. Alternatively, patients could opt out of the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Supplemental Material
Supplemental material for this article is available online.
Transparency Statement
Hiroaki Akai affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned have been explained.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.