
Abstract
Purpose:
To evaluate the midterm outcomes of the Endurant limb fenestration with internal iliac artery repair and enhanced preservation (ELFIRE) procedure, a physician-modified endograft technique developed to preserve internal iliac artery (IIA) perfusion during endovascular aneurysm repair (EVAR) for complex iliac artery aneurysms.
Materials and Methods:
This single-center observational study retrospectively analyzed a prospectively maintained cohort of 95 patients with common or IIA aneurysms with or without abdominal aortic aneurysm, who underwent EVAR using the ELFIRE procedure between August 2019 and May 2023. The technique utilized a physician-modified fenestrated Endurant contralateral limb incorporating a preloaded wire system to facilitate reliable internal iliac branch cannulation, representing the “enhanced preservation” concept of the ELFIRE procedure, combined with Viabahn VBX bridging stent grafts for IIA preservation. The primary outcome was the incidence of pelvic ischemic complications, including buttock claudication and rectal ischemia. Secondary outcomes included technical success, bridging stent graft occlusion, endoleak occurrence, reintervention, aneurysm sac morphology changes during follow-up, and other postoperative complications. Midterm outcomes were analyzed using the Kaplan-Meier method.
Results:
The mean age was 78 ± 6 years, and 83 patients (87.4%) were men. A total of 126 branches were preserved, including bilateral preservation in 31 patients. Technical success was achieved in 98.9%. The median follow-up duration was 36 months (interquartile range, 26-48 months). Kaplan-Meier-estimated freedom from bridging stent graft occlusion was 97.6% at 5 years (95% CI: 91.5-99.4), and freedom from reintervention was 96.6% at 5 years (95% CI: 90.2-98.9). Pelvic ischemic events consisted solely of buttock claudication (4.2%), and no cases of rectal ischemia were observed. The ELFIRE procedure was successfully applied in anatomically challenging cases, including 68 patients (72.6%) outside the instructions for use (IFU) of commercially available iliac branch devices.
Conclusion:
The ELFIRE procedure demonstrated favorable technical success, durable branch patency, and low complication rates at midterm follow-up. This simple and reproducible technique expands treatment options for patients with complex iliac aneurysms. Continued long-term follow-up is warranted to confirm durability and safety.
Clinical Impact
This study provides the first midterm outcomes of the ELFIRE procedure, previously introduced as a physician-modified endograft technique for internal iliac artery preservation. The results confirm durable branch patency and the absence of complications related to device modification, demonstrating the safety and reliability of this approach. ELFIRE expands the treatment options for patients with anatomies unsuitable for commercial iliac branch devices and offers a practical, reproducible alternative for maintaining pelvic perfusion in complex aortoiliac aneurysms.
This is a visual representation of the abstract.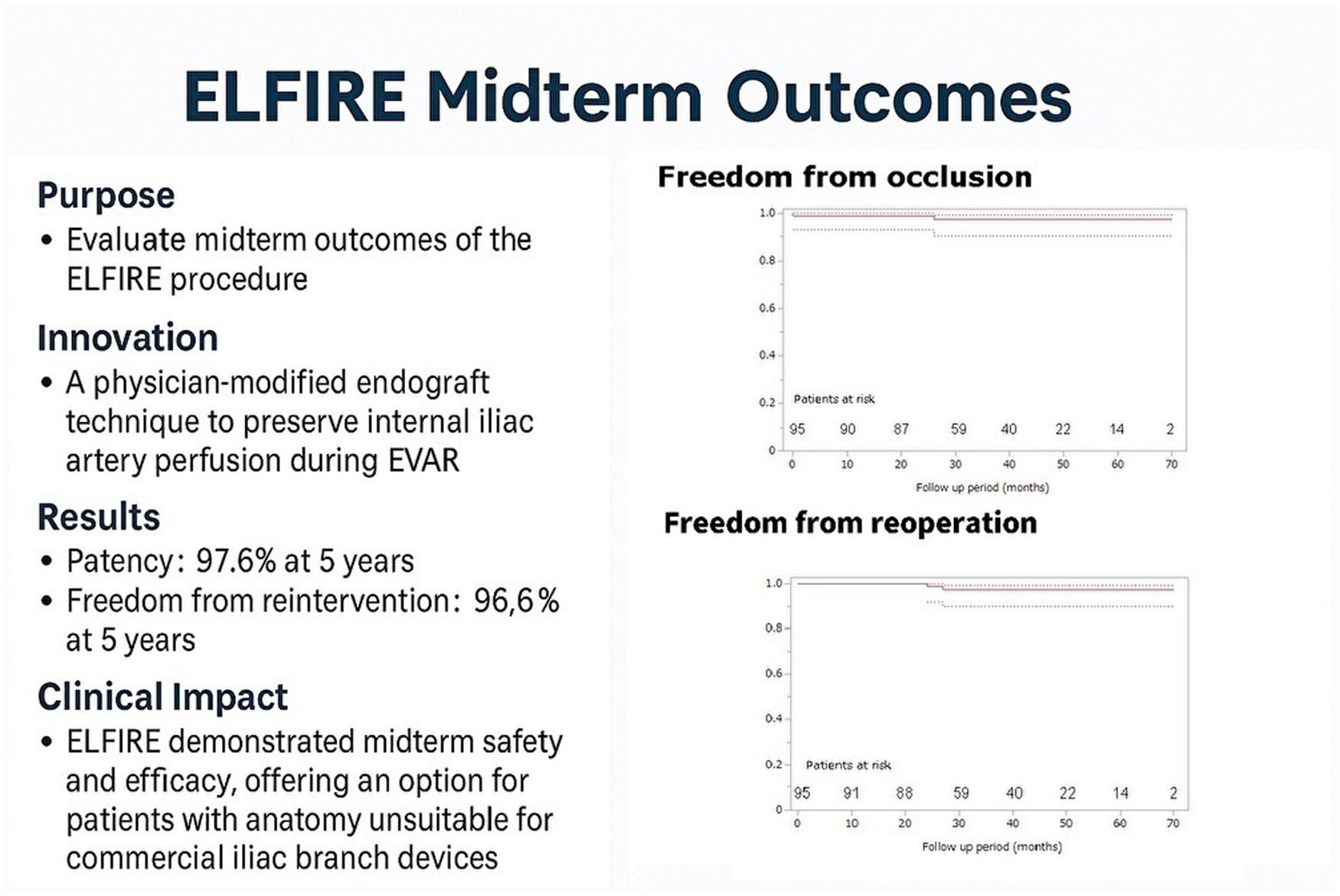
Keywords
Introduction
Endovascular aneurysm repair (EVAR) for abdominal aortic aneurysms (AAAs) with associated common iliac artery (CIA) aneurysms (CIAAs) and/or internal iliac artery (IIA) aneurysms (IIAAs) often requires consideration of IIA preservation. Bilateral IIA preservation is preferred when anatomically feasible, and if this cannot be achieved, maintaining perfusion to at least 1 IIA is recommended to minimize the risk of pelvic ischemic complications. Reported consequences of IIA interruption include buttock claudication, sexual dysfunction, and in rare cases, severe complications such as colonic or spinal cord ischemia.1,2 Previous studies have reported buttock claudication in approximately 20%-40% of patients after IIA coverage, underscoring the importance of preserving pelvic circulation whenever feasible.
Several commercial iliac branch devices (IBDs), including the Gore Excluder Iliac Branch Endoprosthesis (Gore IBE), Zenith Branch Endovascular Iliac Bifurcation Graft, and the more recently released E-liac Stent Graft System, are available to support IIA preservation.3 -5 However, strict anatomical instructions for use (IFU) limit their applicability. In particular, short CIAs, unfavorable iliac bifurcation anatomy, or small iliac diameters frequently preclude the use of these devices, and such anatomical constraints appear to be especially common in Japanese patients.6,7 To address these anatomical limitations, physician-modified endograft (PMEG) strategies have been proposed as alternative solutions when commercial devices cannot be used. Several reports have demonstrated the technical feasibility and encouraging midterm results of PMEGs for preserving IIA perfusion during EVAR.8 -10 However, reproducibility and procedural standardization remain important concerns for wider adoption.
We developed the Endurant limb fenestration with IIA repair and enhanced preservation (ELFIRE) procedure, a standardized PMEG technique that incorporates a fenestrated Endurant contralateral limb and a preloaded wire system designed to facilitate reliable cannulation of the internal iliac branch. This preloaded wire configuration represents the key technical innovation of the ELFIRE technique, allowing controlled contralateral access to the fenestration and improving procedural reproducibility compared with previously reported PMEG approaches. The technical feasibility of this method has been previously described. 11 The objective of this study was to evaluate the midterm clinical outcomes of the ELFIRE procedure in a consecutive cohort of patients undergoing EVAR for complex aortoiliac aneurysms.
Materials/Patients and Methods
Data Source
This was a single-arm observational study approved by the institutional review board of our hospital (No. HS2020-100). The cohort was prospectively maintained but retrospectively analyzed. Written informed consent for both the procedure and study participation was obtained from all patients.
Patient Population
We analyzed 95 consecutive patients with CIAA and/or IIAA with or without AAA who underwent EVAR using the ELFIRE procedure between August 2019 and May 2023 in our institution. All eligible patients treated with the ELFIRE technique during the study period were included without case selection. During the study period, ELFIRE was our standard physician-modified strategy for IIA preservation in anatomically challenging cases unsuitable for commercially available IBDs. Patients with aortic infection or ruptured aneurysms were excluded.
Device Modification and Branch Preservation Strategy
The ELFIRE technique typically used an 82-mm-long Endurant contralateral limb, an AZUR® Detachable 18 HydroCoil (6 mm/20 cm; Terumo Corp.), as both a radiopaque marker and reinforcement for the fenestration, and a Radifocus Guidewire (0.025 inch and 260 cm; Terumo Corp.). A key feature of this procedure is the preloaded wire system, which allows a sheath introduced from the contralateral access to be guided to the fenestration, thereby facilitating contralateral cannulation of the IIA branch. The resheathing maneuver represented the most technically demanding step. During this step, the modified limb reinforced with a hydrocoil is compressed using a silk thread or soft surgical tape and carefully reintroduced into the delivery sheath from the distal end while preventing rotation of the stent structure. Gentle traction sutures placed on the proximal bare stent facilitate the final resheathing. Detailed procedural modifications have been described previously. 11 Device modification was initially performed with 2 operators during the early phase of technique development (approximately the first 10 cases) to facilitate suturing, coil reinforcement, and resheathing of the graft. As experience increased and the workflow became standardized, the modification process became reproducible and was subsequently performed by a single primary operator in the majority of cases. Preparation time decreased from >30 minutes during early adoption to approximately 20 minutes as workflow standardization progressed.
Because the ELFIRE configuration involves physician modification of a commercially available endograft, the procedure represents an off-label use.
Bilateral IIA preservation was the default strategy. Unilateral preservation was performed only when bilateral preservation was anatomically infeasible based on preoperative computed tomography (CT) evaluation (e.g., inability to distinguish IIA bifurcation, pre-existing IIA occlusion, or presence of only small remaining branches (<4 mm)).
Selective Embolization Policy
Although current ESVS guidelines do not recommend routine embolization of the inferior mesenteric artery or lumbar arteries, our strategy evolved based on institutional experience and emerging evidence rather than guideline directives. In line with Japanese practice trends, embolization was performed proactively to reduce the risk of persistent type II endoleak and subsequent aneurysm sac enlargement. This approach was influenced by recent Japanese registry data and reports, including Seike et al, 12 demonstrating an association between persistent type II endoleak and unfavorable sac behavior after EVAR. All embolizations were performed using detachable or pushable coils.
Bridging Stent Selection and Landing Strategy
The landing site selection followed a stepwise strategy based on anatomy rather than a single standardized target. The IIA main trunk was used as the primary landing zone when suitable, whereas the superior or inferior gluteal artery was selected only when trunk landing was not feasible due to aneurysmal degeneration or unfavorable morphology. The choice between the superior and inferior gluteal artery depended on branch caliber and tortuosity.
The Viabahn VBX endoprosthesis (VBX and DrySeal sheath are manufactured by W.L. Gore & Associates (Flagstaff, AZ, USA)) was used as a bridging stent. The diameter of the Viabahn VBX stent was matched to the native IIA or oversized by 1 mm. Oversizing beyond 1 mm was intentionally avoided because the VBX is balloon-expandable, and excessive oversizing may increase the risk of arterial dissection or perforation. The maximum stent diameter used was 8 mm to avoid excessive protrusion into the Endurant limb, manufactured by Medtronic (Minneapolis, MN, USA), which could compromise the lumen at the fenestration level or reduce external iliac artery (EIA) flow.
Stent length selection depended on the distal landing target. When the IIA trunk was used, approximately 10 mm of the proximal VBX was intentionally extended into the Endurant limb to ensure fixation without branch coverage. When the superior or inferior gluteal artery served as the landing site, preoperative centerline measurements determined device length. If the required length exceeded the maximum available 79-mm configuration, 2 VBX devices were implanted with sufficient overlap to prevent type III endoleak. Post-dilation was performed selectively when the native vessel diameter exceeded the available device size.
Endograft Selection and Adjuncts
Because the Endurant limb has a Z-stent structure, kinking may occur when landing in a tortuous or stenotic EIA; therefore, supplemental bare stents were selectively deployed when limb kinking, or significant external iliac tortuosity was observed intraoperatively to optimize alignment and maintain patency.
Endograft platform selection was based on proximal neck and aortic anatomy. An Endurant limb served as the connecting platform for fenestration, allowing compatibility with various main-body devices without junction-related complications in this series. When using AFX2, a longer Endurant limb was intentionally selected and custom-shortened to match the position of CIA bifurcation (terminal aorta) before deployment, ensuring sufficient overlap and preventing junction instability. ALTO required no additional modification. For Aorfix and TREO devices, an additional Endurant limb was used to achieve adequate overlap because of the fish-mouth configuration or limited landing length.
During early adoption, a learning-curve effect was evident, particularly in sheath handling and branch cannulation. After 1 case of failed VBX advancement caused by cephalad sheath deflection, the technique was modified by advancing a 16F DrySeal sheath over the preloaded wire to stabilize access and guide the Destination sheath, manufactured by Terumo Interventional Systems (Tokyo, Japan). This adjustment improved reproducibility and procedural efficiency. A supplemental video demonstrating the updated workflow is included to facilitate technical replication (Supplemental file 1).
Postoperative Follow-Up
All patients underwent standardized computed tomography angiography (CTA) follow-up at 1 week, 6 months, 12 months, and every 6 months thereafter. Duplex ultrasound was not used routinely but selectively when evaluating sac enlargement or graft flow abnormalities. For VBX, patients receiving antiplatelet therapy preoperatively continued the same regimen postoperatively, whereas antiplatelet-naïve patients received aspirin monotherapy (100 mg/day).
Study Endpoints
The primary endpoint was the incidence of IIA ischemic events, including buttock claudication, and rectal ischemia. Secondary endpoints included (1) technical success of the ELFIRE procedure; (2) graft-related outcomes (bridging stent patency, graft occlusion, and endoleaks associated with the ELFIRE technique); and (3) anatomical and clinical outcomes, including aneurysm sac size change, secondary interventions, and other postoperative complications.
Technical success was defined as successful deployment of all grafts with secure proximal and distal fixation, absence of type I or III endoleak, patent grafts without kinking or obstruction on intraoperative imaging, and preserved branch patency.
Buttock claudication was defined as new-onset gluteal pain or fatigue occurring during ambulation and relieved by rest. Pelvic ischemic complications were assessed using clinical symptoms and CT findings. Rectal ischemia was evaluated based on symptoms such as abdominal pain, diarrhea, or hematochezia, with supportive radiologic evidence of reduced mural enhancement or bowel-wall edema. Colonoscopy was performed when clinically indicated.
Statistical Analysis
Descriptive statistics were used to summarize the data. Continuous variables were expressed as mean ± standard deviation or median (interquartile range), and categorical variables were expressed as counts and percentages. The Kaplan-Meier method was used to estimate overall survival and freedom from bridging stent graft occlusion and reintervention, with 95% CIs. Time-to-event was measured from the date of surgery to the date of the last follow-up or an event (e.g., death or graft occlusion). All analyses were performed using JMP Pro 17 (SAS Institute Inc.).
Results
Table 1 summarizes the patient and aneurysm characteristics. The mean age was 78 ± 6 years, 83 (87.4%) were men, and the median follow-up was 36 months (interquartile range: 26-48 months). The distribution of aneurysm type was as follows: AAA+CIAA (n = 42), AAA+CIAA+IIAA (n = 20), CIAA+IIAA (n = 18), isolated CIAA (n = 11), and AAA+IIAA (n = 4).
Clinical Characteristics of the Patients and Characteristics of Aneurysms.
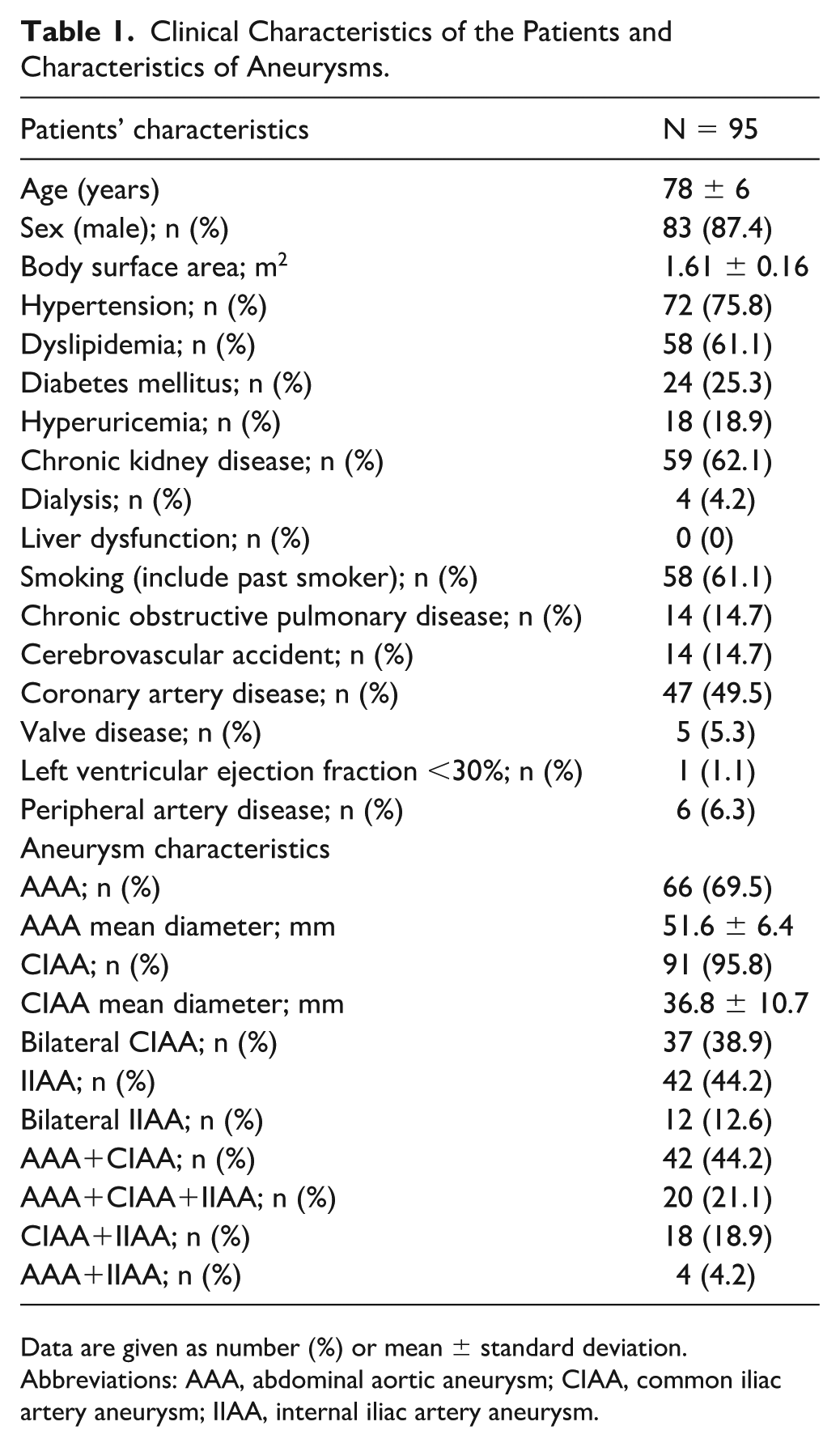
Data are given as number (%) or mean ± standard deviation.
Abbreviations: AAA, abdominal aortic aneurysm; CIAA, common iliac artery aneurysm; IIAA, internal iliac artery aneurysm.
As shown in Table 2, a total of 126 bridging stent grafts were implanted (bilateral IIA preservation in 31 patients). Sixty-eight patients (72.6%) had anatomies outside the IFU for Gore IBE. Most IFU exclusions were related to short CIAs, unfavorable iliac bifurcation anatomy, or small iliac diameters. In IFU-eligible cases, ELFIRE was selected instead of Gore IBE when the EVAR main-body device was not the Excluder platform because junction compatibility and branch alignment were considered suboptimal with AFX2, Endurant, or other platforms. Preservation of the IIA main trunk using a bridging stent graft was achieved in 45 right and 41 left arteries, and preservation of the superior or inferior gluteal branch in 21 right and 19 left arteries. Concomitant procedures included inferior mesenteric artery embolization (22 cases, 23.2%), lumbar artery embolization (46 cases, 48.4%), accessory renal artery embolization (8 cases, 8.4%), percutaneous transluminal angioplasty (7 cases, 7.4%), and thoracic endovascular aortic repair (1 case, 1.1%).
Surgical Procedure Characteristics.
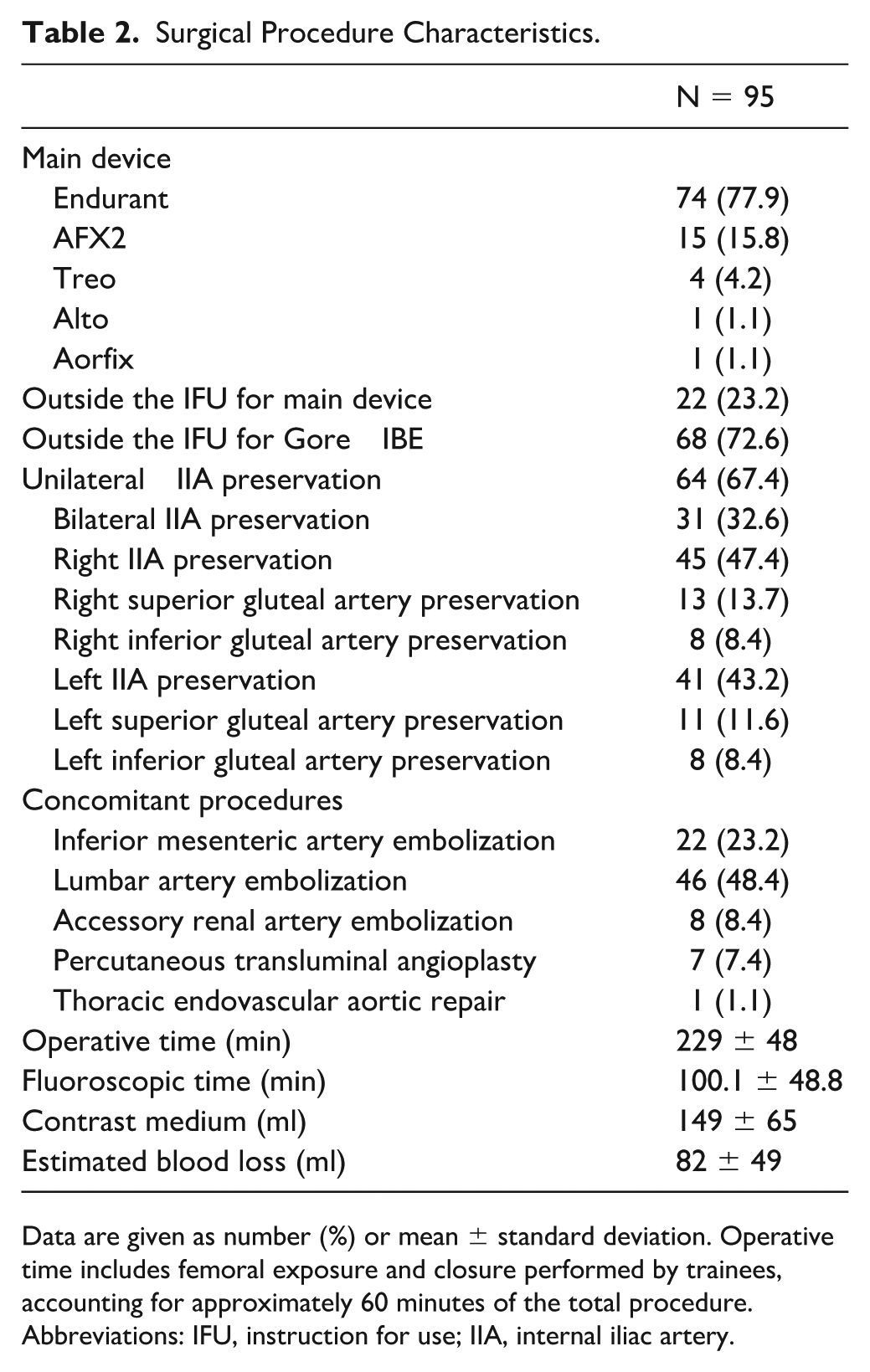
Data are given as number (%) or mean ± standard deviation. Operative time includes femoral exposure and closure performed by trainees, accounting for approximately 60 minutes of the total procedure.
Abbreviations: IFU, instruction for use; IIA, internal iliac artery.
Table 3 summarizes the procedural and follow-up outcomes. The primary endpoint, IIA ischemic events, occurred in 4 patients (4.2%), all presenting with buttock claudication. One case occurred with concurrent bridging stent and EIA occlusion, 2 events occurred on the non-preserved side, and 1 case developed inferior buttock claudication despite superior gluteal preservation. All 4 patients developed buttock claudication that persisted during follow-up, although the symptoms were mild and did not require additional intervention. No rectal ischemia or sexual dysfunction was observed.
The Details of Postoperative Outcomes.
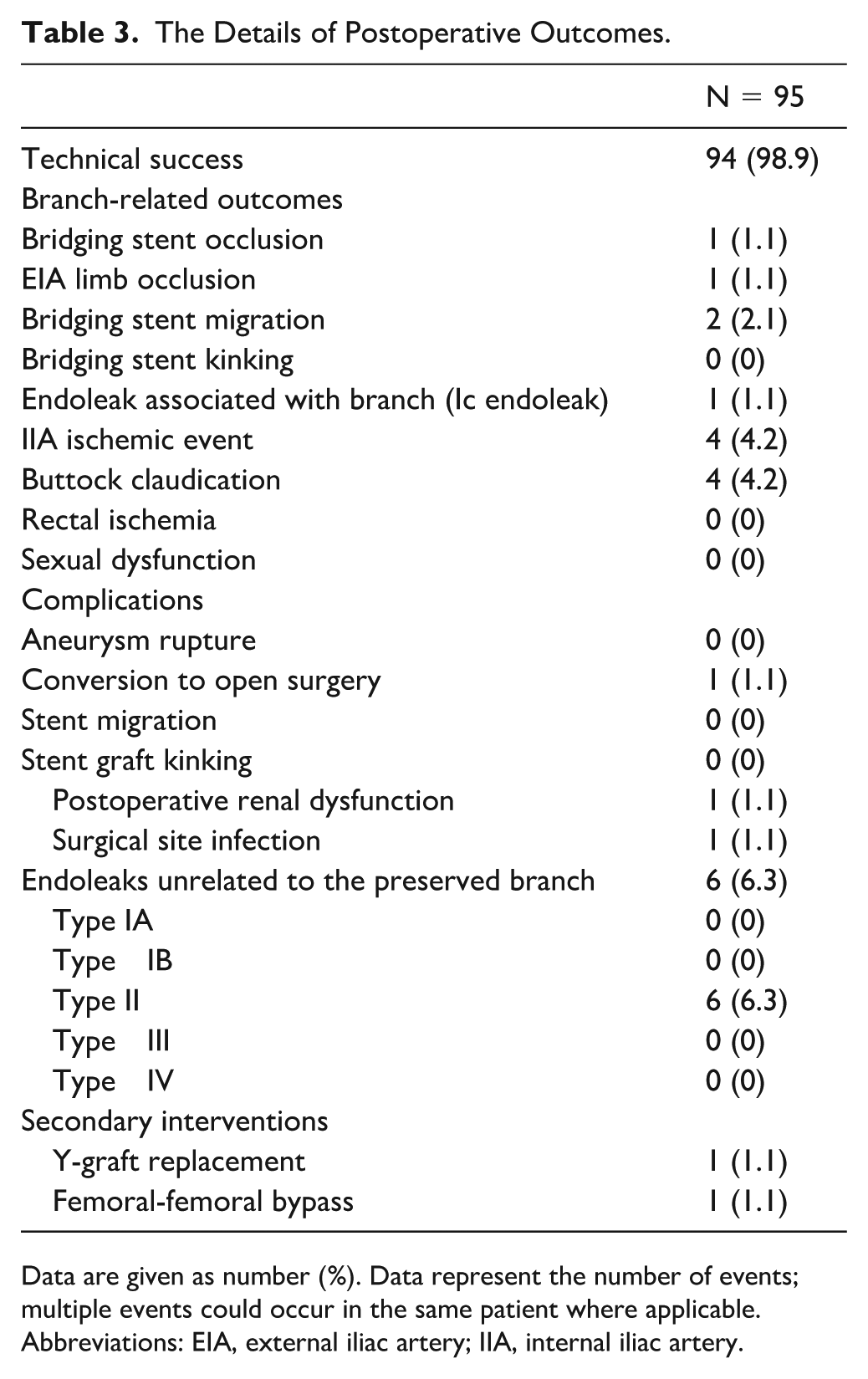
Data are given as number (%). Data represent the number of events; multiple events could occur in the same patient where applicable.
Abbreviations: EIA, external iliac artery; IIA, internal iliac artery.
The technical success rate was 98.9% (94/95). One technical failure occurred due to delivery difficulty of the Viabahn VBX in a patient with an acutely angulated aortic bifurcation and a short ipsilateral CIA of approximately 20 mm length. Bilateral preservation was attempted, and ipsilateral preservation was successful. However, because of the steep bifurcation angle, the tip of the modified limb protruded slightly into the aneurysm sac, and although cannulation of the contralateral IIA was achieved, the sheath was deflected cephalad, and the VBX could not be delivered. Following this event, the technique was modified to introduce the 16F DrySeal sheath along the preloaded wire to the Endurant limb entrance, and then the Destination sheath was advanced inside the DrySeal sheath to avoid cephalad deflection. This modification improved sheath stability.
Figure 1 shows the Kaplan-Meier curves for freedom from bridging stent graft occlusion, reintervention, and overall survival. Freedom from bridging stent graft occlusion was 97.6% at 5 years (95% CI: 91.5-99.4).
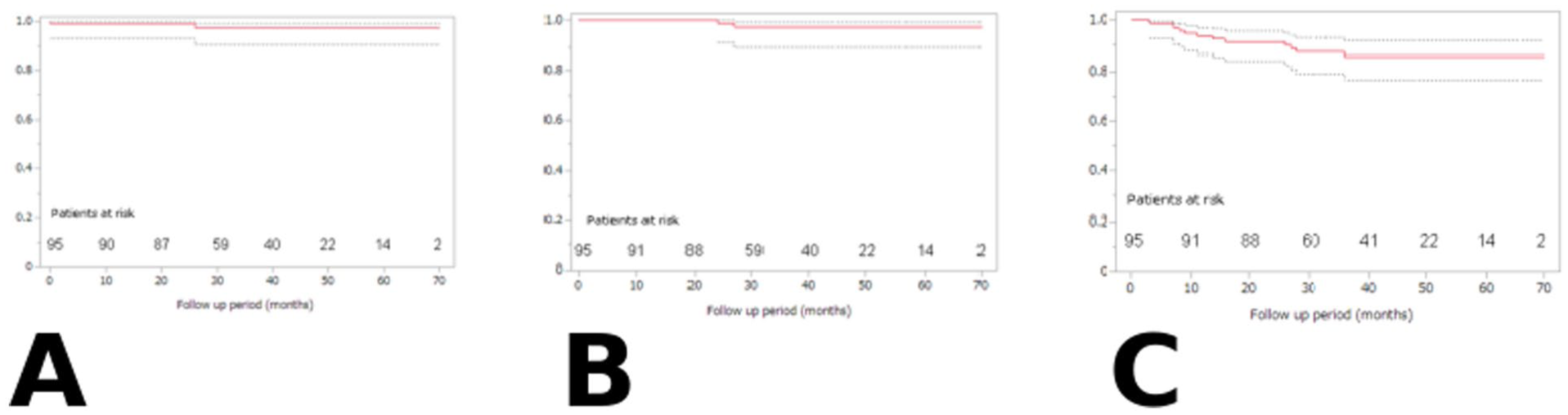
Kaplan-Meier curves showing (A) freedom from bridging-stent graft occlusion, (B) freedom from reintervention, and (C) overall survival after the ELFIRE procedure.
Occlusion of both the bridging stent graft and EIA occurred in 1 patient at 8 months postoperatively after discontinuation of antiplatelet therapy. This was the only bridging stent graft occlusion observed in the present series. Bridging branch migration occurred in 1 case in which the VBX was deployed in the IIA main trunk, resulting in a type Ic endoleak that required open conversion. The likely cause of migration was the presence of an aneurysmal proximal IIA and insufficient distal landing length on the IIA main trunk.
Kaplan-Meier–estimated freedom from reintervention was 100% at 1 year and 96.6% at 5 years (95% CI: 90.2-98.9).
Figure 2 shows aneurysm sac behavior during follow-up. Four patients demonstrated sac enlargement. Two cases were associated with persistent type II endoleak. The remaining 2 patients showed progressive enlargement without visible sac enhancement on CTA and were considered to have suspected endotension or occult endoleak. No limb migration, graft disconnection, or failure of branch components was observed in these cases.
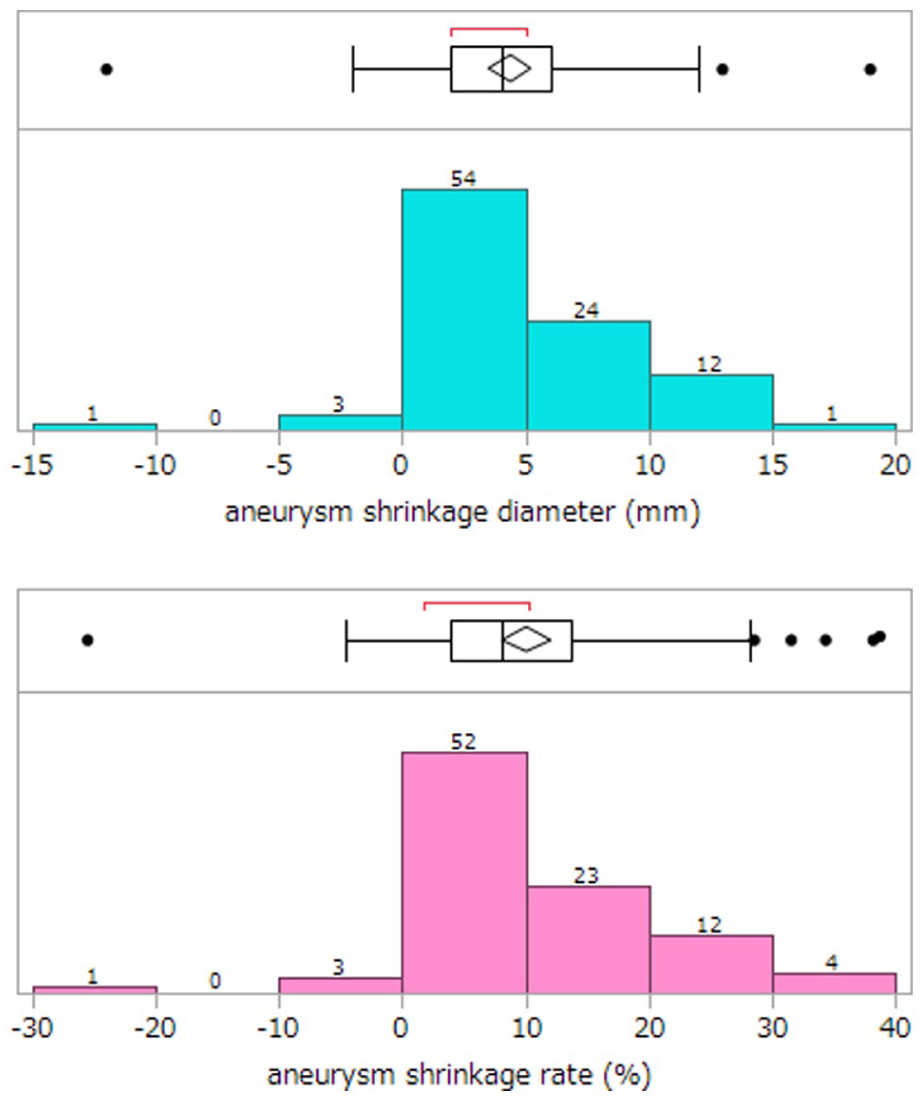
Change in aneurysm sac diameter during follow-up after the ELFIRE procedure. Positive values indicate sac shrinkage, whereas negative values indicate sac enlargement. Four patients demonstrated sac enlargement (2 type II endoleaks and 2 suspected endotension/occult endoleaks). No device-related structural failure was observed in these patients.
Discussion
This study demonstrated favorable midterm outcomes of the ELFIRE procedure, a PMEG technique designed to preserve IIA perfusion during EVAR for complex aortoiliac aneurysms. Although numerous PMEGs have been reported,8,13 procedural reproducibility and technical simplicity remain essential to achieving consistent results. ELFIRE is a versatile, reproducible method that can be readily performed by surgeons familiar with IBD techniques.
Commercial IBDs have demonstrated excellent long-term outcomes in the treatment of aortoiliac aneurysms.6,7,14 Previous reports have shown 5-year reintervention and branch occlusion rates of approximately 20% and 15%, respectively, 3 and a recent meta-analysis confirmed high technical success with low pelvic ischemic event rates and a 30-day mortality of only 0.4%. 4 In addition to established devices such as Gore Excluder IBE and Zenith branch platforms, the E-liac Stent Graft System has emerged as a newer alternative. In the prospective PLIANT trial, 5 E-liac achieved >90% technical success and approximately 98% internal iliac branch patency at 1 year, with continued patency maintained at midterm follow-up. 14
In comparison, the ELFIRE procedure demonstrated a technical success rate of 98.9%, with Kaplan-Meier–estimated 5-year bridging-stent graft patency of 97.6% and freedom from reintervention of 96.6%. Because this study represents a single-arm observational analysis, these outcomes should not be interpreted as a direct comparison with commercially available IBDs. Pelvic ischemic events consisted solely of buttock claudication (4.2%) and no cases of rectal ischemia or sexual dysfunction were observed. Notably, 72.6% of treated patients were outside the IFU criteria for commercial IBDs, yet outcomes remained comparable to published IBD results. These findings indicate that ELFIRE serves as a durable and reproducible alternative when commercial IBDs cannot be applied because of anatomical constraints.
The principal strength of ELFIRE lies in its anatomical adaptability. Unlike commercial systems requiring strict IFU compliance, ELFIRE can accommodate short or ectatic CIAs and variable IIA branching morphology. In our experience, the ELFIRE technique has been successfully applied across a wide range of CIA anatomies, including very short CIA segments, without a strict dimensional threshold. The recently adopted DrySeal sheath technique further improves cannulation stability and allows treatment even in cases with limited CIA length. However, extremely short or severely angulated anatomies may still present technical challenges, and therefore, the anatomical limits of the technique cannot be completely defined. The relatively predictable pelvic anatomy facilitates fenestration alignment, making the modification process considerably simpler than PMEG applications in thoracoabdominal repair. Selective targeting of either the IIA trunk or a suitable gluteal branch provides further flexibility and allows tailored pelvic perfusion.
Despite these advantages, several limitations of the present study should be acknowledged. ELFIRE requires physician modification and therefore is associated with a learning curve, especially during early adoption when sheath stability and catheter alignment are unfamiliar. In our experience, device preparation time and technical handling improved progressively during the early cases as the workflow became standardized. However, procedural metrics were not prospectively recorded in a manner allowing formal statistical learning-curve analysis. Moreover, evaluation of the learning curve was not a primary objective of the present study and was mentioned mainly to provide context regarding the early technical development of the procedure. In addition, although no fenestration-related failures occurred in this cohort, long-term durability remains an unresolved consideration given the suture-reinforced fenestration and partial intraluminal extension of the balloon-expandable bridging stent. These characteristics may become relevant in patients requiring subsequent Thoracic Endovascular aortic repair (TEVAR) or transcatheter aortic valve implantation (TAVI), where stent interaction could theoretically induce migration or material fatigue. Accordingly, unilateral preservation has recently been favored in patients likely to require future aortic interventions. Because a substantial proportion of patients in this cohort were anatomically unsuitable for commercially available IBDs, the study population represents a selected group with complex aortoiliac anatomy. Therefore, the applicability of these results to routine EVAR practice in centers treating standard anatomy should be interpreted with caution.
In this study, the use of multiple main-body platforms did not lead to junctional failures, likely reflecting the standardized overlap strategy and selective reinforcement with additional Endurant components as needed. Cross-manufacturer coupling of endograft components has been reported as a potential risk factor for type III endoleaks in EVAR, emphasizing the importance of a careful overlap strategy and long-term surveillance. 15 Furthermore, by landing distally in the EIA, ELFIRE may reduce the risk of late type Ib endoleak, particularly in short or ectatic CIA anatomy—an established risk factor in prior reports.16 -18 Preservation of the gluteal arteries demonstrated excellent durability—superior to previously reported outcomes3,4,19—however, preservation of very small branches requiring 5-mm VBX stents resulted in early occlusion; therefore, preservation is now limited to branches measuring ≥6 mm. In our previous experience outside the present cohort, a 5-mm VBX deployed in a superior gluteal artery occluded early after the procedure. This event was attributed to the small caliber of the distal branch and limited physiologic flow demand rather than failure of the fenestrated graft construct. Based on this observation, preservation of very small branches requiring 5-mm VBX is currently avoided in our practice.
Overall, ELFIRE provides a practical, reproducible, and durable option when commercial IBDs cannot be applied, while its limitations highlight the importance of continued surveillance and technique refinement.
Conclusions
The ELFIRE procedure demonstrated favorable midterm outcomes with effective aneurysm exclusion and low complication rates. These findings suggest that ELFIRE provides a reliable and reproducible alternative for patients with anatomically challenging aortoiliac aneurysms who are unsuitable for commercial IBDs. Further long-term follow-up is warranted to confirm durability and safety.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.