
Abstract
Objective:
Drug-eluting resorbable scaffold (DRS) has emerged as a promising adjunctive treatment to traditional percutaneous transluminal angioplasty (PTA) for infrapopliteal arterial disease. This systematic review aims to evaluate the clinical efficacy and safety of DRS in this application.
Methods:
PubMed, ScienceDirect, and Embase databases were systematically searched as of November 2025. Studies concerning infrapopliteal arterial revascularization using DRS were included. The primary endpoints were 12-month primary patency rate and freedom from clinically driven target vessel revascularization (CD-TLR). Secondary endpoints included 12-month limb salvage rate and 30-day all-cause mortality.
Results:
Seven studies, comprising 1 randomized controlled trial, 3 prospective, and 3 retrospective studies, including 497 patients were included in the analysis. Treatment of infrapopliteal arterial lesion with DRS yielded a 12-month primary patency of 88% (95% CI = 0.81-0.93) and a 12-month freedom from CD-TLR of 95% (95% CI = 0.93-0.97). The 12-month limb salvage rate was 99% (95% CI = 0.97-1.00), and freedom from 30-day all-cause mortality rate was 99% (95% CI = 0.97-1.00).
Conclusion:
Drug-eluting resorbable scaffold was associated with high patency and low reintervention rates in this systematic review of predominantly observational studies. Nevertheless, additional large-scale randomized controlled trials are warranted for direct comparison between DRS and PTA and further investigation to establish long-term durability.
Clinical Impact
By summarizing recent data from interventional and observational studies, this systematic review demonstrated favourable efficacy and safety of drug-eluting resorbable scaffolds (DRS) in the treatment of infrapopliteal arterial disease. While superiority of DRS over conventional balloon angioplasty alone could not be established due to limited randomized trials and lack of long-term follow-up. The available data support use of DRS as an adjunctive option in selected patients with chronic limb-threatening ischemia.
Keywords
Introduction
Chronic limb-threatening ischemia (CLTI) represents an important emergency in below-the-knee (BTK) arterial disease. It is characterized by ischemic rest pain, tissue loss, and gangrene, leading to approximately 20% to 25% annual mortality. 1 Increased risk of tissue loss and mortality indicates that the condition requires immediate intervention, where revascularization without delay is recommended by current clinical guidelines to optimize outcomes.2 -4 Despite the advancements in endovascular surgical technique with improved accessibility of arteries, management of infrapopliteal lesions remains technically challenging, considering their small vessel diameter, high incidence of diffuse lesions with calcification or occlusion, and inadequate imaging accuracy.5,6
Percutaneous transluminal angioplasty (PTA) with permanent metallic stenting remains the current standard of care for infrapopliteal arterial lesions when stenting is necessary, such as in cases of flow-limiting dissection and severe recoil after angioplasty.7,8 Nevertheless, leaving the stents in the arteries would predispose to in-stent restenosis, which would potentially impede further re-intervention. In recent years, drug-eluting resorbable scaffold (DRS) gradually emerged as an innovative adjunctive approach to BTK revascularization. Aligning with the “leave nothing behind” strategy, DRS are composed of biodegradable polymers or metals which naturally undergo decomposition by metabolic reactions over time upon implantation. The utilization of DRS offers advantages of restoring native vessel functionality and enabling adaptive remodeling once the scaffold resorbs, thereby eliminating the risk of stent fracture and facilitating future intervention. In addition, the incorporation of antiproliferative drugs in DRS helps preventing neointimal hyperplasia and subsequent restenosis. The latest first FDA approval of DRS for treating BTK arterial disease – Esprit BTK system marks a profound breakthrough in the clinical application of DRS. 9 In view of the significant advancements in the development of DRS, this systematic review aims to evaluate the clinical outcomes of current DRS for treatment of BTK peripheral arterial disease.
Methods
Search Strategy
We systematically searched PubMed, ScienceDirect, and Embase as of November 2025. The search strategy used a combination of terms (“bioresorbable” OR “resorbable” OR “biodegradable”) AND (“scaffolds” OR “scaffold” OR “stents”) AND (“below-the-knee” OR “infrapopliteal” OR “chronic limb-threatening ischemia”) for relevant studies. Reference lists from included articles were cross-checked for other potential studies. All titles and abstracts were subsequently assessed for eligibility by 2 independent reviewers manually. Upon consensus on study selection was reached, the study outcomes were collectively extracted by the investigators.
Study Design, Inclusion and Exclusion Criteria
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines and the Meta-analysis of Observational studies in Epidemiology checklist. 10 The study has been registered in PROSPERO after initiation of the review.
We planned to include randomized controlled trials and retrospective observational studies which focused on evaluating the clinical outcome of BTK revascularization with DRS.
Our inclusion criteria were as follows: (1) studies including patients with symptomatic infrapopliteal arterial stenosis or occlusion, Rutherford Classification 2 or above; (2) studies that evaluated BTK revascularization using DRS; and (3) studies published in English language.
Exclusion criteria were as follows: (1) treatment involving infrapopliteal arterial revascularization with bare-metal stents (mainly derived from coronary stents); (2) treatment with non-drug-eluting bioresorbable scaffolds; (3) studies including patients with non-infrapopliteal arterial disease; and (4) studies with follow-up periods less than 12 months or with insufficient clinical data.
Primary Endpoints and Secondary Endpoints
Angiographic primary patency, which was defined by absence of binary restenosis (>50% stenosis), as well as freedom from clinically driven target lesion revascularization (CD-TLR) at 12 months were recorded as primary endpoints in the studies. Clinically driven target lesion revascularization refers to revascularization of the target lesion upon confirmation of restenosis generally ≥50% by angiography or presentation of ischemic signs, although the threshold for intervention differed between studies. Freedom from amputation at 12 months and 30-day all-cause mortality were recorded as secondary endpoints.
Subgroup Analysis
We further conducted post hoc subgroup analyses of primary patency by stratifying studies according to scaffold material and generation based on the time of their release. Scaffolds were categorized as either polymer-based or magnesium-based. Regarding scaffold generation, the Absorb BVS is generally deemed the first-generation commercially available scaffold for BTK lesion stenting, whereas other scaffolds are classified the new-generation devices based on advanced design and later release.
Statistical Analysis
A random-effects model meta-analysis was performed using R version 4.5.1. The endpoints were reported with 95% confidence interval. I2 statistics was used to assess study heterogeneity, where >75% heterogeneity was rated as substantial variation. Pooled results were presented with Freeman-Tukey transformed proportion. Statistical significance was defined as P ≤ .05.
Quality Assessment
To evaluate the risk of bias for the included studies, appropriate quality assessment tools were applied according to study design. As for single-arm observational studies, each study was examined using the Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I). Studies assessed by ROBINS-I would be rated as low, moderate, serious, or critical risk of bias.
As for randomized controlled trials, the Cochrane Risk of Bias (RoB-2) tool was used. The instrument assesses bias across 5 domains and provides an overall judgment of “low,” “some concerns,” or “high” risk of bias.
Sensitivity Analysis
A pre-specified leave-one-out sensitivity analysis was performed to evaluate the robustness of the pooled primary patency estimates. Each study was sequentially removed and the overall effect size was reformulated with meta-analysis.
Results
The literature search and screening process are shown in Figure 1. The literature search yielded a total of 508 records (53 from PubMed, 357 from ScienceDirect, 98 from Embase). After removing 16 duplicates, 492 studies underwent title and abstract screening. Among the 11 articles which fully met the eligibility criteria, 4 of them were follow-up publications based on previously reported studies with the same participant samples.11 -14 These follow-up publications were treated as additional reports of the same underlying studies and were linked to the earliest publication for data extraction. Consequently, 7 unique studies were included in meta-analysis, 9 ,11 -20 including 1 randomized-controlled trial and 6 single-arm observational studies. The risk of bias of each study was provided in Supplementary Table 1.
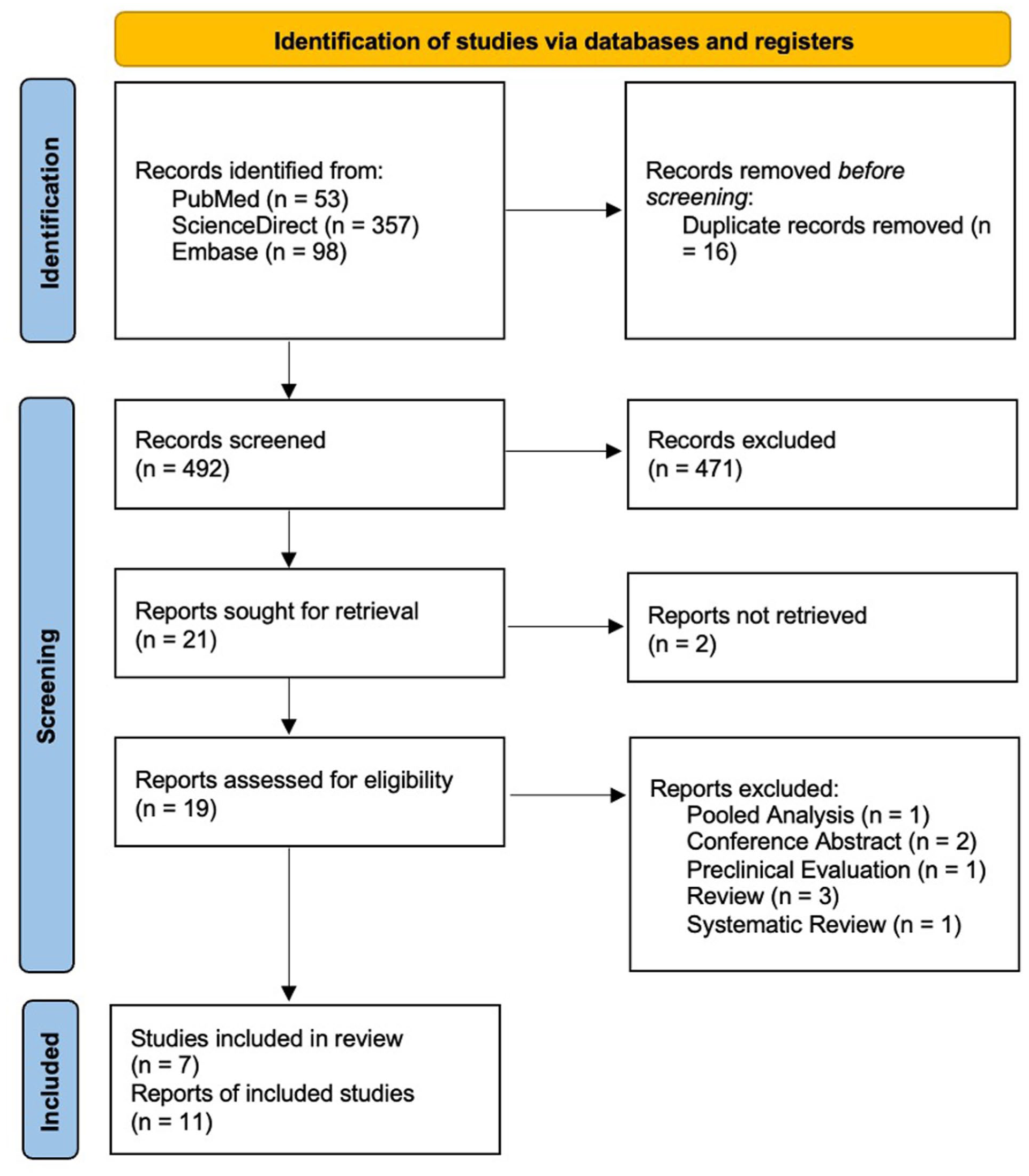
Flowchart of literature search.
Of the 7 selected studies, 497 patients primarily treated with DRS were included. Baseline and clinical characteristics of patients with infrapopliteal arterial disease are summarized in Tables 1 and 2, respectively. The clinical data for primary patency (PP) rate, freedom from CD-TLR rate, limb salvage (LS) rate, and 30-day all-cause mortality were directly extracted from the results in the articles.
Baseline Characteristics of Patients With Infrapopliteal Arterial Diseases in Included Studies Treated by Drug-Eluting Resorbable Scaffolds (DRS).
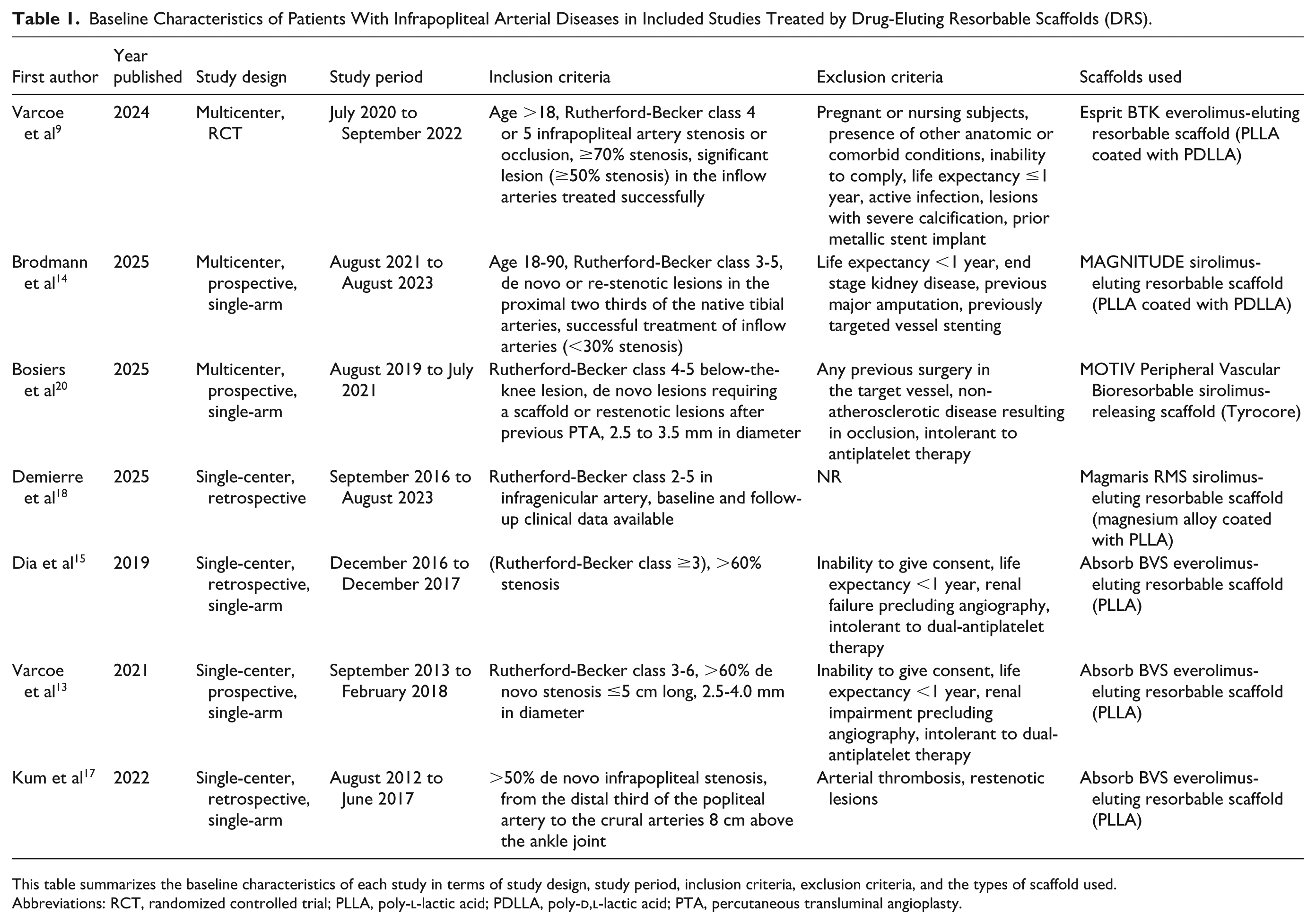
This table summarizes the baseline characteristics of each study in terms of study design, study period, inclusion criteria, exclusion criteria, and the types of scaffold used.
Abbreviations: RCT, randomized controlled trial; PLLA, poly-
Clinical Characteristics of Patients With Infrapopliteal Arterial Diseases in Included Studies Treated by Drug-Eluted Resorbable Scaffolds (DRS).
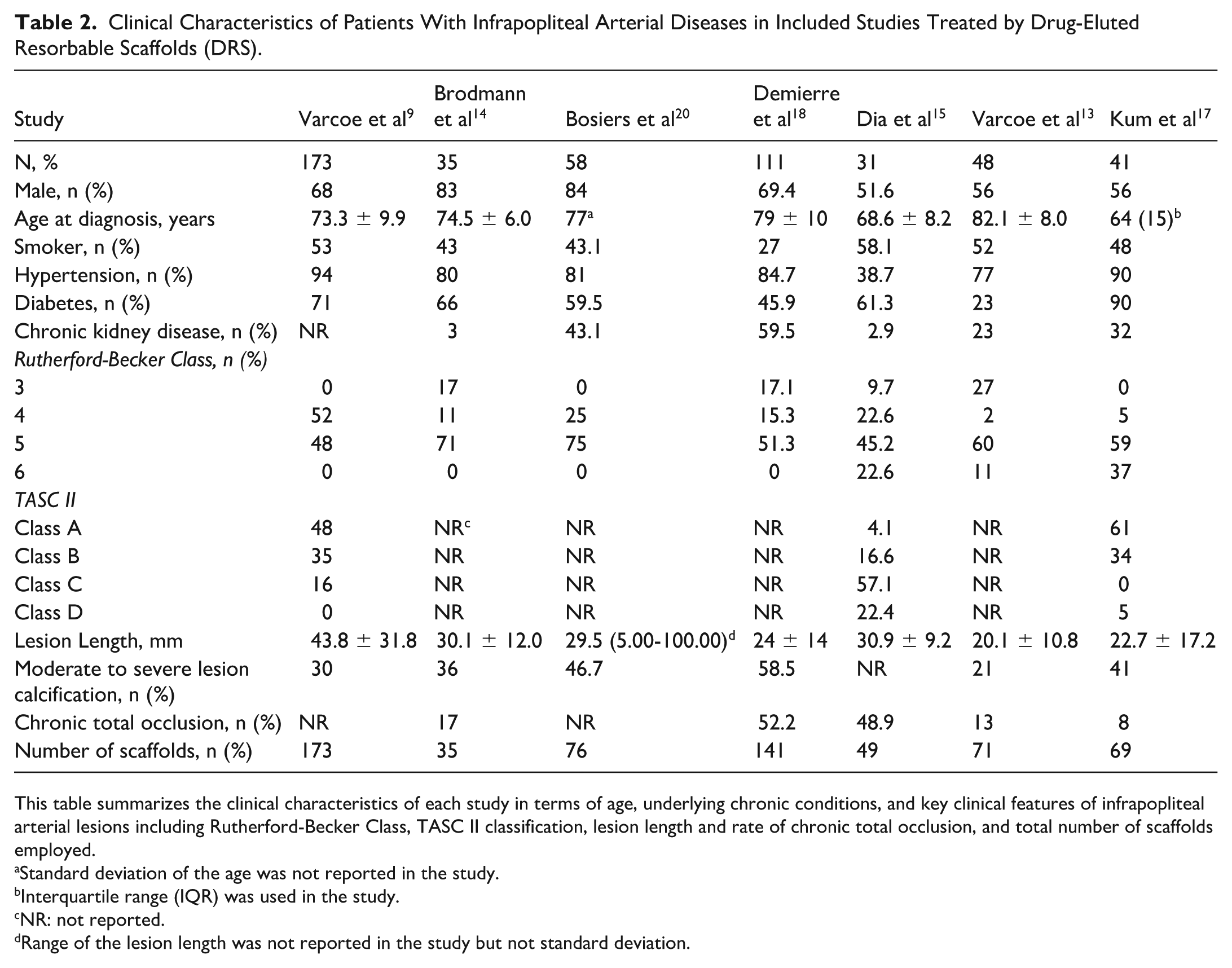
This table summarizes the clinical characteristics of each study in terms of age, underlying chronic conditions, and key clinical features of infrapopliteal arterial lesions including Rutherford-Becker Class, TASC II classification, lesion length and rate of chronic total occlusion, and total number of scaffolds employed.
Standard deviation of the age was not reported in the study.
Interquartile range (IQR) was used in the study.
NR: not reported.
Range of the lesion length was not reported in the study but not standard deviation.
Angiographic PP rate at 12 months and 30-day all-cause mortality rate were assessed based on 6 of the included studies. The PP rate in the study by Brodmann et al 14 was not included because there was no sequential assessment of PP at 12 months. The 30-day all-cause mortality rate was not reported in the study by Bosiers et al. 20 A random effects model meta-analysis of studies showed 88% 12-month angiographic PP rate in 462 patients treated with DRS (Freeman-Tukey transformed proportion: 0.88; 95% CI: 0.81-0.93; I2 = 74.0%; Figure 2). However, there was discrepancy on the definition of primary patency from the studies.
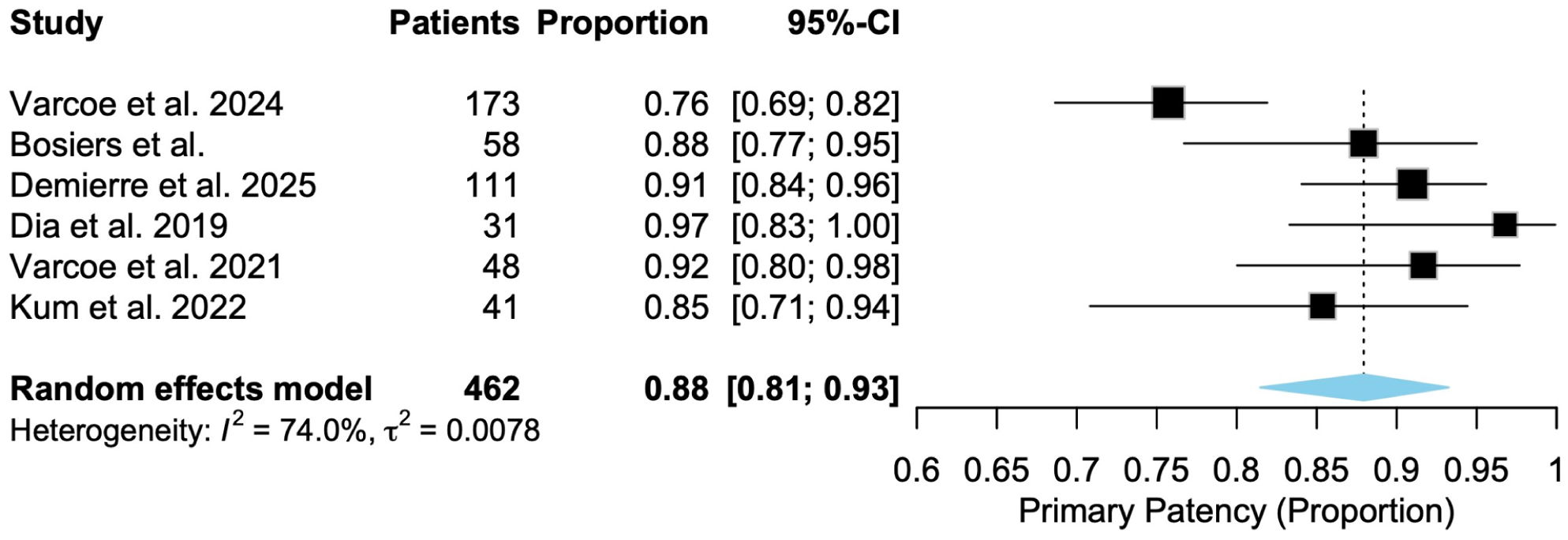
Forest plot of 12-month angiographic primary patency rate. This plot displays the primary patency rate of drug-eluting resorbable stents with 95% confidence interval at 12 months. The pooling was performed using the Freeman-Tukey double arcsine transformation to stabilize variances. The study by Brodmann et al was not included due to lack of documentation of relevant data. I2 and P-value are shown to reflect heterogeneity and statistical significance.
Rate of freedom from CD-TLR and LS rate at 12 months were assessed based on all studies involving 497 patients. Meta-analysis result revealed 12-month freedom from CD-TLR of 95% (Freeman-Tukey transformed proportion = 0.95; 95% CI = 0.93-0.97; I2 = 2.5%; Figure 3) and 12-month LS rate of 99% (Freeman-Tukey transformed proportion = 0.99; 95% CI = 0.97-1.00; I2 = 0.0%; Figure 4).
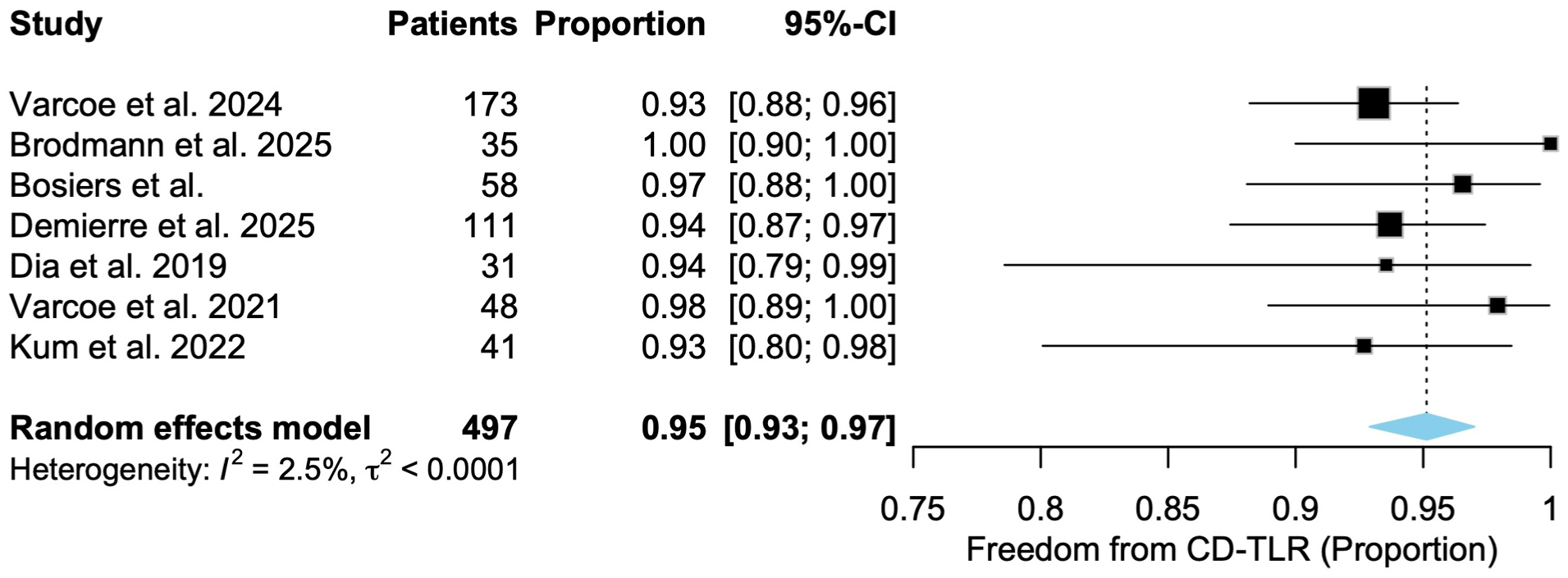
Forest plot of 12-month freedom from clinically driven target lesion revascularization rate. This plot displays the rate of freedom from clinically drive target lesion revascularization (CD-TLR) of drug-eluting resorbable stents with 95% confidence interval at 12 months. The pooling was performed using the Freeman-Tukey double arcsine transformation to stabilize variances. I2 and P-value are shown to reflect heterogeneity and statistical significance.
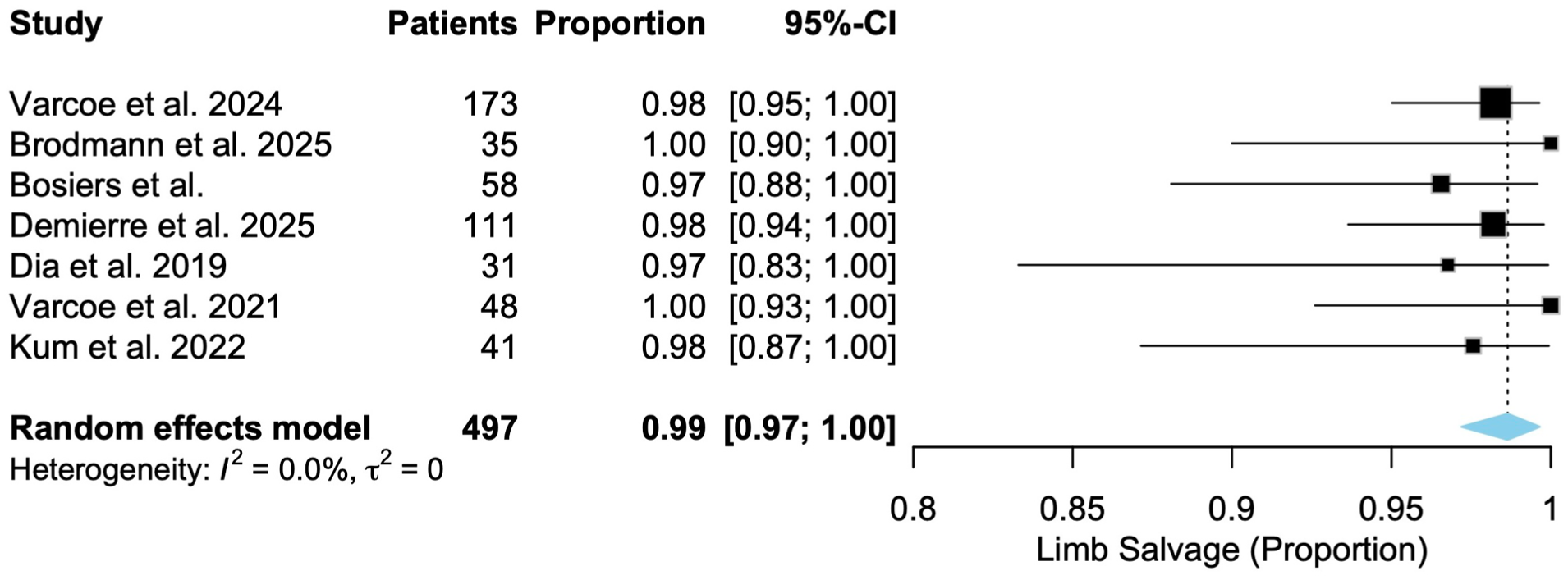
Forest plot of 12-month limb salvage rate. This plot displays the rate of limb salvage of drug-eluting resorbable stents with 95% confidence interval at 12 months. The pooling was performed using the Freeman-Tukey double arcsine transformation to stabilize variances. I2 and P-value are shown to reflect heterogeneity and statistical significance.
Data on freedom from 30-day all-cause mortality rate was available in 6 of the included studies involving 439 patients. Varcoe et al 9 recorded perioperative death of 1 patient within 30 days after treatment with DRS, while other studies reported 0% mortality rate. Meta-analysis resulted in freedom from 30-day all-cause mortality of 99% (Freeman-Tukey transformed proportion = 0.99; 95% CI = 0.97-1.00; I2 = 0.0%; Figure 5).
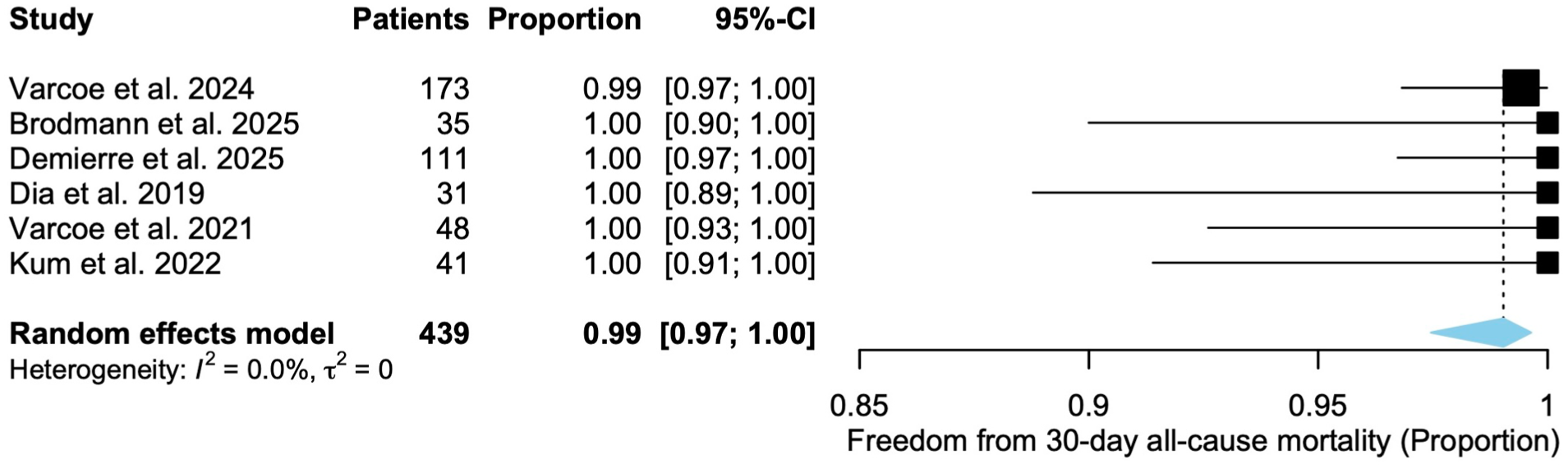
Forest plot of 30-day all-cause mortality. This plot displays the rate of freedom from 30-day all-cause mortality of drug-eluting resorbable stents with 95% confidence interval. The pooling was performed using the Freeman-Tukey double arcsine transformation to stabilize variances. The study by Bosiers et al was not included as the 30-day mortality rate was not documented, although it was mentioned that 3 patients died throughout the study period. I2 and P-value are shown to reflect heterogeneity and statistical significance.
The 12-month angiographic PP showed significant heterogeneity (I2 = 74.0%). Other outcomes showed mild to no heterogeneity.
Subgroup Analysis
Subgroup analyses were performed to explore potential sources of the observed heterogeneity of 12-month PP, specifically evaluating the impact of scaffold material and device generation.
In terms of scaffold material, A random-effect model meta-analysis showed that polymer-based scaffolds (5 studies, n = 351 9 ,13,17,18,20) demonstrated a 12-month PP of 87% (Freeman-Tukey Proportion: 0.88, 95% CI = 0.76-0.95, Figure 6), with significant internal heterogeneity (I2 = 73.4%). In contrast, the magnesium-based scaffold (1 study, n = 111 19 ) reported a 12-month PP of 91%. No significant difference in patency was observed (P = .351).
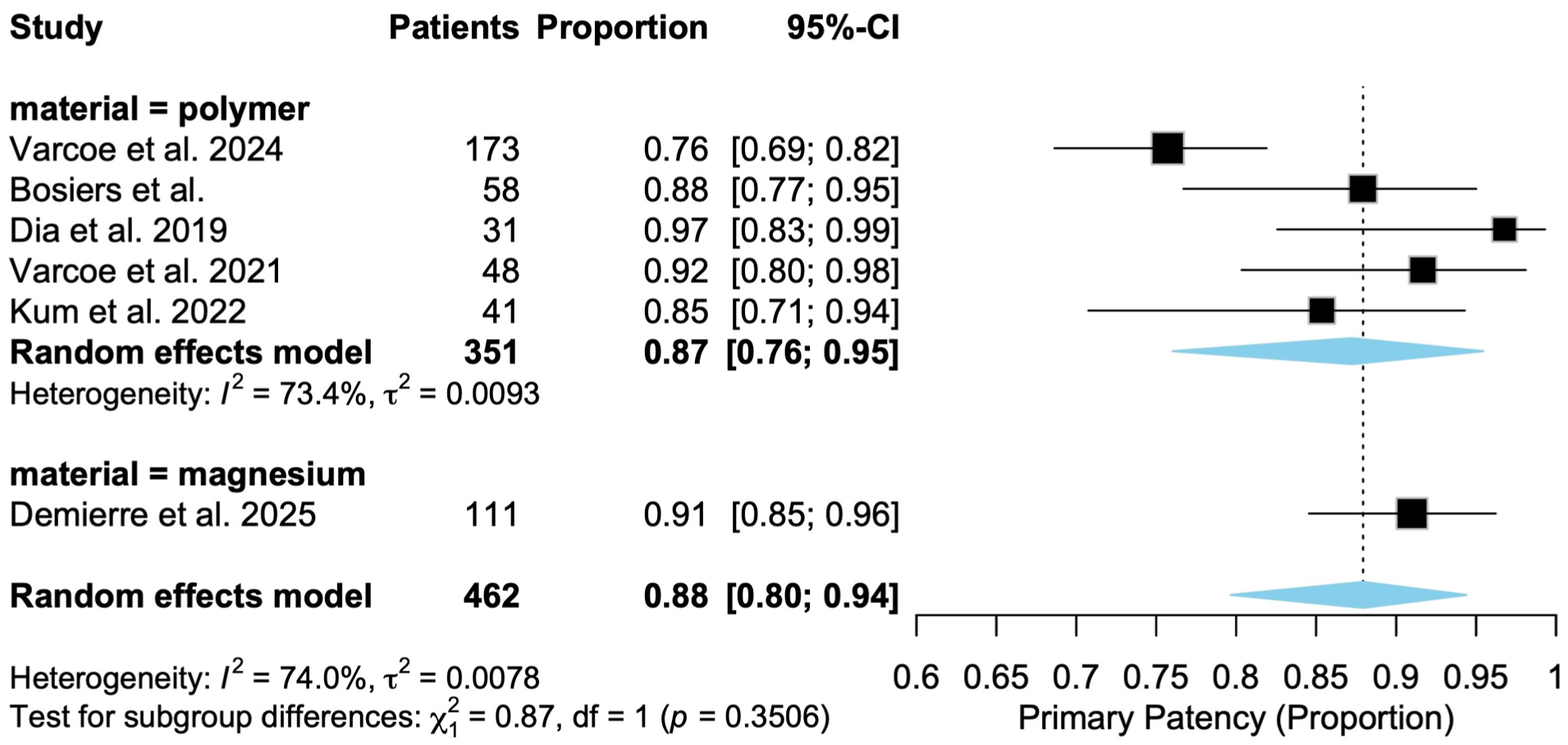
Forest plot of subgroup analysis on 12-month angiographic primary patency rate based on scaffold material. This plot displays the primary patency rate of drug-eluting resorbable stents stratified by scaffold material (polymer vs magnesium) with 95% confidence interval at 12 months. The pooling was performed using the Freeman-Tukey double arcsine transformation to stabilize variances. The study by Brodmann et al was not included due to lack of documentation of relevant data. I2 and P-value are shown to reflect heterogeneity and statistical significance.
Regarding device generation, scaffolds were categorized into first-generation (n = 342) and second-generation (n = 120). First-generation devices showed a 12-month PP of 91% with lower heterogeneity than second-generation devices with 12-month PP of 85% (I2 = 22.5% vs 84%, Figure 7). Despite the marked difference in consistency between generations, no significant difference was observed between the 2 material subgroups (P = .293).
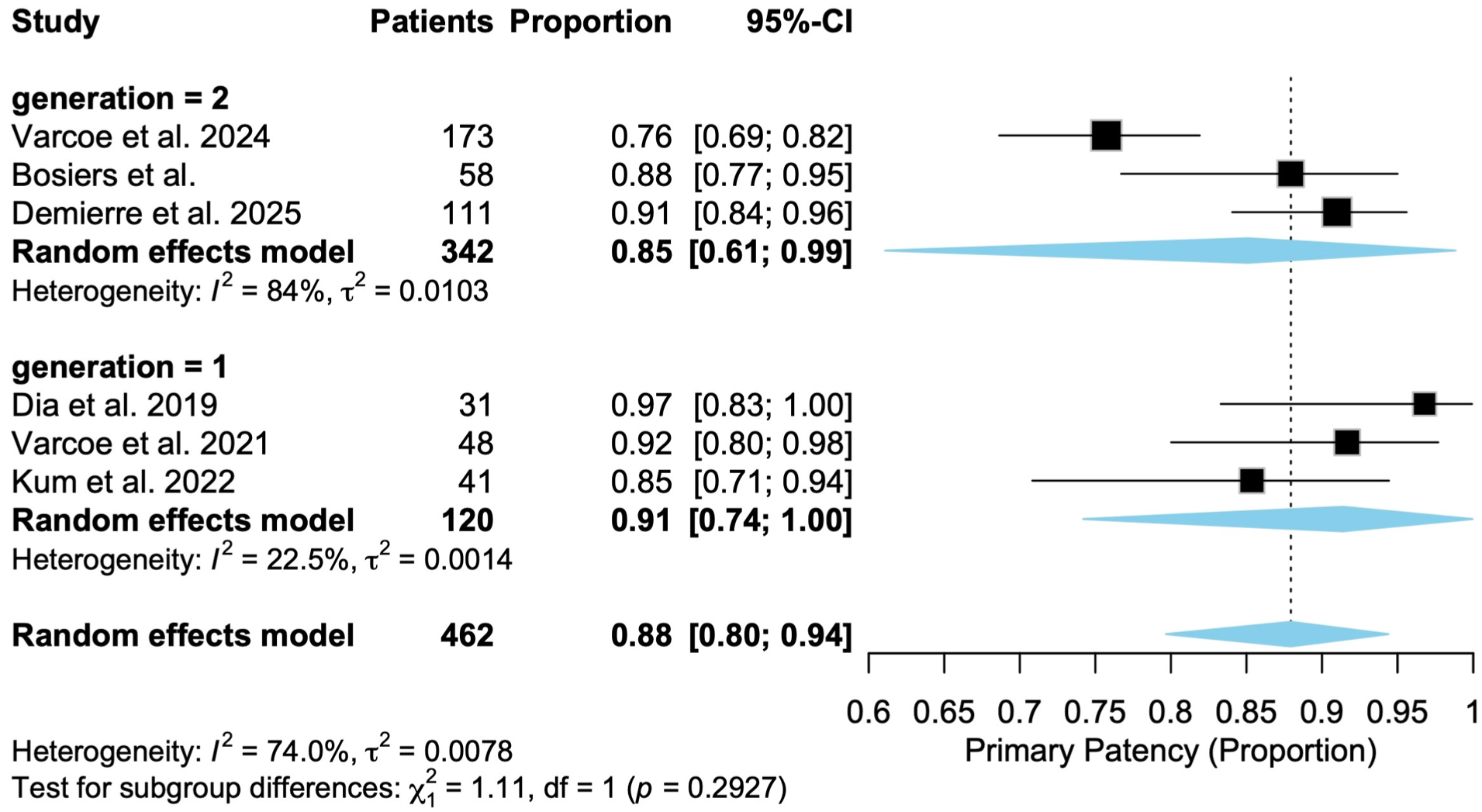
Forest plot of subgroup analysis on 12-month angiographic primary patency rate based on device generation. This plot displays the primary patency rate of drug-eluting resorbable stents stratified by device generation with 95% confidence interval at 12 months. The pooling was performed using the Freeman-Tukey double arcsine transformation to stabilize variances. The study by Brodmann et al was not included due to lack of documentation of relevant data. I2 and P-value are shown to reflect heterogeneity and statistical significance.
Sensitivity analysis
Sensitivity analysis concerning the primary patency was summarized in Supplementary Table 2. LIFE-BTK trial by Varcoe et al 9 was identified as the primary source of heterogeneity, while other studies did not change the findings from the main analysis.
Discussion
The goal of this systematic review was to evaluate the clinical outcomes of DRS as the primary treatment for infrapopliteal arterial disease. In summary, the results revealed good 12-month primary patency, freedom from CD-TLR, limb salvage rate, and minimal 30-day mortality rate with the use of DRS. These results reinforce the idea that DRS is compatible with the “leave nothing behind strategy,” while providing temporary scaffolding and drug elution, this technique is able to achieve durable patency while facilitating future re-intervention.
Percutaneous transluminal angioplasty with elective bare-metal stents (BMS) has long been the standard of care for disease management but struggles to achieve long-term vessel patency, offering 60% to 70% 12-month primary patency rate for its high re-stenosis rate and limited durability.21 -23 The advent of drug-eluting stents (DES) made an attempt to resolve the problem of neointimal hyperplasia using anti-hyperplatic agents. However, its use is limited by issues including persistent inflammation, impaired vessel motion, risks of stent fracture, and difficulty for future surgical re-intervention. Due to its permanent nature, benefits of DES are blunted in the long term. 24 Drug-eluting resorbable scaffold overcome these limitations by combining the antiproliferative effects of DES with the transient presence of a biodegradable scaffold.
Contemporary biodegradable materials are mainly categorized into biopolymers (eg, poly-
Although direct comparison through meta-analysis between these treatments is impossible due to insufficient studies, LIFE-BTK trial by Varcoe et al 9 as the first multicenter, randomized controlled trial has demonstrated superior efficacy of DRS over angioplasty in terms of freedom from binary restenosis at 1 year (76% and 50%, P < .001) as well as freedom from CD-TLR (93% vs 87%, P < .001). Incidence of serious adverse events was similar for both groups (2% for DRS, 3% for PTA), proving the non-inferior safety of DRS in comparison to the traditional approach. Notably, in the 2-year follow-up report of LIFE-BTK trial, the patency rate of DRS remained superior to PTA despite 5.8% decline from 1-year to 2-year time points, with an absolute risk difference of 28%. 14 Coherent with this result, a previous retrospective follow-up study by Dia et al 16 reported a durable 87.1% primary patency and 93.5% freedom from CD-TLR at 2-year using Absorb BVS scaffolds. This result was achieved in a complex cohort with 49% of chronic thrombotic occlusions and near 80% of TASC C or D lesions, reflecting that the therapeutic efficacy of DRS can possibly be generalized to more complex lesions and patients with worse prognosis. 11 While Absorb BVS has been withdrawn from the market, studies with Absorb BVS served as a vital “proof of concept” for the newer, dedicated BTK scaffolds that are the focus of current practice. The durable patency of DRS is likely explained by their gradual biodegradation, which mitigates the risk of mechanical complications, accompanied by the prolonged release of antiproliferative agents.
While the primary patency outcome in our review showed significant heterogeneity (I2 = 74.0%), this result is not unexpected and does not represent conflicting findings. Discrepancies likely stem from differences in device generation and the design used by each study. Subgroup analysis indicated that scaffold material (polymer vs magnesium) was not the primary driver of this variance (P = .351). Nevertheless, given the paucity of data regarding magnesium-based scaffolds, these results should be interpreted with caution, as the performance of a single device may not be generalized to represent the clinical potential of the entire material class.
In contrast, older generation devices (Absorb BVS13,17,18) demonstrated higher consistency in patency (I2 = 22.5%) compared with newer generation devices (Espirit BTK, MOTIV, Magmaris RMS9,19,20) (I2 = 84%). More specifically, sensitivity analysis identified LIFE-BTK trial as the primary source of this heterogeneity. Its lower patency may be attributed by more complex clinical profiles, such as longer lesion lengths and a higher prevalence of chronic comorbidities. While these factors suggest a relationship between lesion complexity and scaffold performance, a formal meta-regression was precluded by the limited number of available studies (k < 10).
Limitations
Considering that the development of DRS is still in a relatively early phase, only one randomized controlled trial on direct comparison between DRS and PTA was available and the remaining studies were single-arm and retrospective in nature, which mostly carried serious risk of bias. Further confirmatory randomized controlled trials justifying the efficacy of DRS are warranted. While our results support the high efficacy of DRS, causality cannot be confirmed from the largely observational study cohort included in the pooled analysis. Longitudinal research with a longer term of follow-up is needed to assess the outcomes after the scaffolds are fully resorbed. In addition, investigation of the biochemical pictures and imaging of vessel remodeling could provide deeper insights on the long-term effects of DRS.
The review process also faced inherent limitations. It is impossible to fully exclude publication bias despite a comprehensive search strategy, as studies with significant results are more likely to be published. Language restrictions may also have led to the omission of relevant studies. Finally, confounders across studies were not consistently reported. Important factors such as lesion length, degree of vessel calcification, and diabetes status were handled differently, making it difficult to determine the independent effect of DRS across all patient subgroups.
Conclusions
In conclusion, this systematic review demonstrates that DRS is associated with high patency and low intervention rates in treating infrapopliteal artery disease. This is supported by excellent pooled 12-month rates for primary patency (88%), freedom from CD-TLR (95%), and limb salvage rate (99%). These results reinforce that the strategy of “leave nothing behind” is a viable and powerful approach in managing BTK lesions.
Supplemental Material
sj-docx-1-jet-10.1177_15266028261453275 – Supplemental material for Systematic Review and Meta-Analysis of Drug-Eluting Resorbable Scaffolds for Infrapopliteal Arterial Disease
Supplemental material, sj-docx-1-jet-10.1177_15266028261453275 for Systematic Review and Meta-Analysis of Drug-Eluting Resorbable Scaffolds for Infrapopliteal Arterial Disease by Jerry T. Y. Lau, Hai-Lei Li, King Sum Tong, Lin Ye and Stephen W. K. Cheng in Journal of Endovascular Therapy
Supplemental Material
sj-docx-2-jet-10.1177_15266028261453275 – Supplemental material for Systematic Review and Meta-Analysis of Drug-Eluting Resorbable Scaffolds for Infrapopliteal Arterial Disease
Supplemental material, sj-docx-2-jet-10.1177_15266028261453275 for Systematic Review and Meta-Analysis of Drug-Eluting Resorbable Scaffolds for Infrapopliteal Arterial Disease by Jerry T. Y. Lau, Hai-Lei Li, King Sum Tong, Lin Ye and Stephen W. K. Cheng in Journal of Endovascular Therapy
Footnotes
Ethical Considerations
An ethical statement is not applicable for this systematic review as it was conducted based on published literature without direct participants involvement.
Author Contributions
Conceptualization: Hai-Lei Li, Jerry T. Y. Lau.
Data curation: Jerry T. Y. Lau, Hai-Lei Li.
Formal analysis: Jerry T. Y. Lau, King Sum Tong.
Investigation: Jerry T. Y. Lau, Hai-Lei Li, King Sum Tong.
Methodology: Hai-Lei Li, Jerry T. Y. Lau, Lin Ye.
Software: Jerry T. Y. Lau, Hai-Lei Li, Lin Ye.
Supervision: Hei-Lei Li, Stephen W. K. Cheng.
Validation: Hei-Lei Li, Stephen W. K. Cheng, Lin Ye.
Visualization: Jerry T. Y. Lau, Lin Ye, King Sum Tong.
Writing – original draft: Jerry T. Y. Lau, King Sum Tong, Hai-Lei Li.
Writing – review & editing: Jerry T. Y. Lau, Hei-Lei Li, Stephen W. K. Cheng, Lin Ye.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by The University of Hong Kong Seed Fund for Basic Research (No. 2401103787) and Beijing Science and Technology Program International (Hong Kong, Macao and Taiwan) Joint Research and Development Project (No. Z251100007125020).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Registration Number for Review
This systematic review was registered in PROSPERO under registration number CRD420251268062 after initiation of the review.
Declaration of Generative AI and AI-Assisted Technologies in the Manuscript Preparation Process
During the preparation of this work, the author(s) used Chat-Gpt version 5.1 in order to improve the clarity and flow of the language. After using this tool/service, the authors reviewed and edited the content as needed and take full responsibility for the content of the published article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.