
Abstract
Objectives:
The objective of this systematic review was to provide evidence-based data regarding the incidence and outcome of retrograde type A dissection (RTAD) in patients treated with thoracic endovascular aortic repair (TEVAR) for type B aortic dissection (TBAD).
Methods:
A systematic literature review was conducted through November 2025 in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses guidelines. Primary outcomes included the overall incidence of retrograde dissection, as well as incidence stratified by to the phase (acute, subacute, and chronic) of TBAD at the time of TEVAR and by the proximal sealing zone of endograft. Secondary outcomes were 30-day and late mortality after open or conservative management of RTAD.
Results:
From 538 identified records, 22 studies met inclusion criteria, comprising 5088 patients (71% male) with a median follow-up of 28 months (range, 12–70 months). The pooled 30-day and late incidence of RTAD was 1.8% (95% confidence interval [CI], 1.2–2.7; I2=58%) and 2.2% (95% CI 1.6–3.0; I2=44%), respectively. The incidence of RTAD was highest after TEVAR performed for acute TBAD at 3.2% (95% CI 2.3–4.3), compared with 1.6% (95% CI 0.9–3.1) for subacute and 2.0% (95% CI 1.2–3.4) for chronic TBAD. Pooled 30-day mortality after open surgical repair was 43.7% (95% CI 27.6–61.2; I2=0%) and increased to 51.5% (95% CI 37.5–65.3; I2=10%) during late follow-up. Retrograde type A dissection occurred more frequently in complicated cases (2.6%; 95% CI 1.6–4.1) than in uncomplicated cases (1.5%; 95% CI 0.5–4.4). The highest RTAD incidence was observed with proximal sealing zone 1 (15.4%; 95% CI 8.2–27.2), compared with zone 2 (6.9%; 95% CI 4.8–9.9).
Conclusions:
Retrograde type A dissection remains a rare but highly lethal complication following TEVAR for TBAD. Immediate or delayed open surgical repair carries substantial mortality. Primarily uncomplicated clinical presentation, delayed TEVAR, and more distal sealing zones bear lower risk for RTAD.
Clinical Impact
Retrograde type A aortic dissection (RTAD) is a rare but catastrophic complication following thoracic endovascular aortic repair (TEVAR) for type B aortic dissection. Previous research has highlighted this risk emphasizing the lethal potential of RTAD suggesting etiological factors such as procedural manipulation and stent deployment techniques while demonstrated that RTAD after TEVAR for acute type B dissection may be successfully managed with staged hybrid surgical techniques and underscoring its clinical severity. Despite these important contributions, the literature remains fragmented with varying incidence estimates and outcomes. The aggregated evidence confirms that although uncommon, RTAD carries a high mortality risk and necessitates meticulous procedural planning, vigilant post-TEVAR surveillance, and well-defined management strategies. These findings help inform practice guidelines, risk stratification, and future device innovations to minimize this devastating complication.
Keywords
Introduction
Type B aortic dissection (TBAD) is a life-threatening vascular condition, associated with poor prognosis if left untreated. 1 Its main morphological characteristics include the presence of an intimal tear and the development of a false lumen (FL), which disrupts the blood flow within the true lumen (TL), leading to malperfusion of the visceral arteries and, in some cases, to the lower limbs. The principal objective of treatment is to exclude the primary intimal tear, promoting thrombosis of the FL, and re-expansion of the TL, thereby re-establishing normal haemodynamics.2,3 With ongoing advances in endovascular therapy, thoracic endovascular aortic repair (TEVAR) has been established as the standard of care for TBAD, supported by consistent evidence demonstrating favorable short-term outcomes. 2
However, TEVAR is associated with several complications including stroke, spinal cord ischemia, access-related injuries, stent graft migration, endoleaks, device collapse, false aneurysm formation at the proximal or distal end of the stent graft erosion, and stent frame fracture. 2 Retrograde type A dissection (RTAD) has also been reported following TEVAR, however, its true incidence and associated mortality rate remain unanswered. A recent systematic review and meta-analysis attempted to shed more lights on this issue. 4 Nevertheless, this analysis had several limitations, including the inclusion of studies with small TEVAR cohorts (<50 patients), short (<12 months) or absent follow-up periods, and overlapping data, thus lacking some clarity on the available data included in the analysis.
The aim of this systematic review was to determine the true incidence of RTAD following TEVAR, as well as the associated reintervention and mortality rates related to this serious complication.
Methods
Design and Registration
The systematic review was designed and reported in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement (Figure 1). 5 The study protocol was registered in PROSPERO (CRD420251145712).
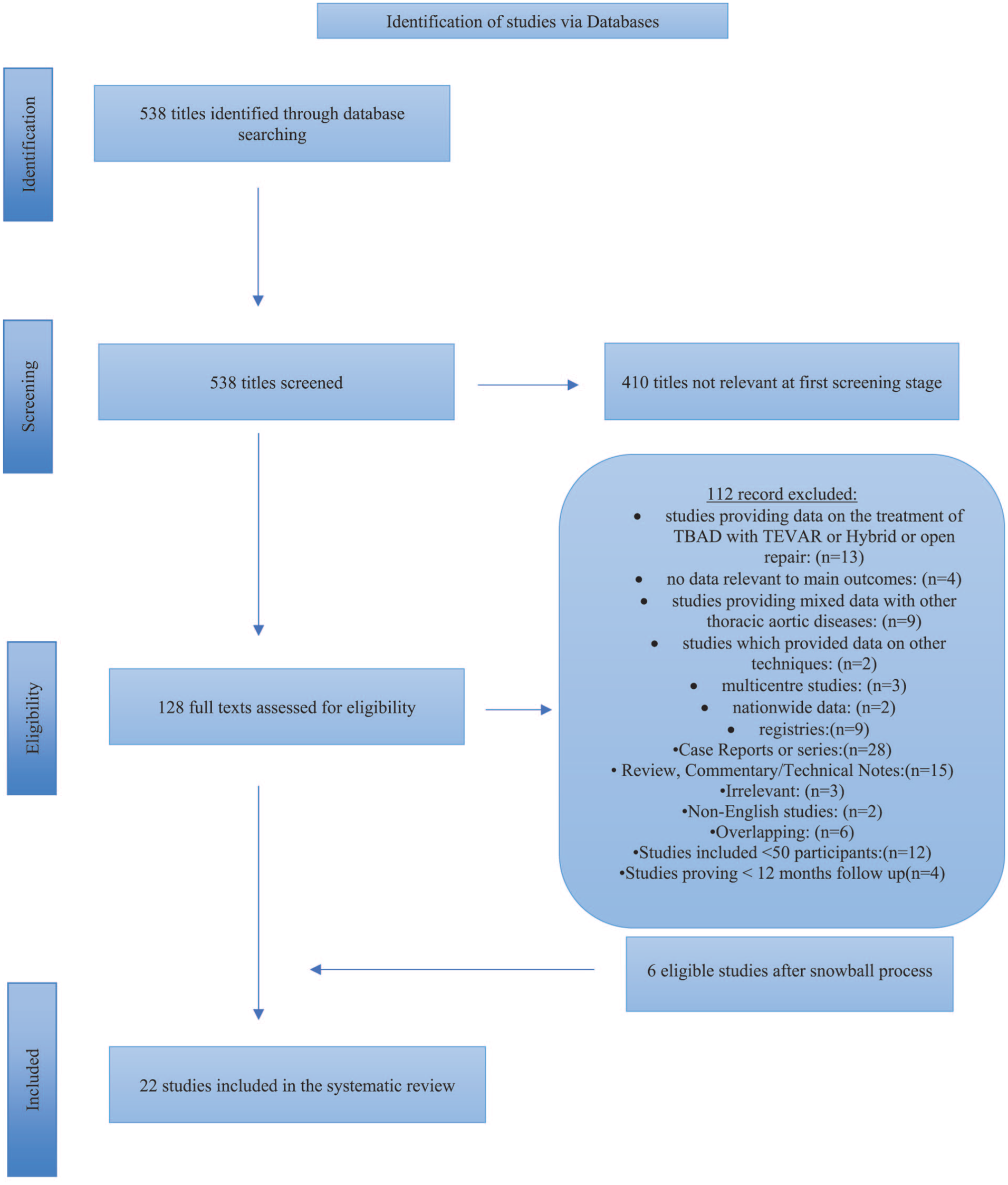
Study flow chart (“Preferred Reporting Items for Systematic Reviews and Meta-Analysis” diagram).
Eligibility Criteria
Observational cohort studies (prospective or retrospective), case-control studies, cross-sectional studies, and randomized clinical trials enrolling more than 50 patients who underwent TEVAR, with a follow-up period exceeding 12 months, published in English, and reporting data on RTAD following TEVAR, were considered eligible. Studies that provided data on hybrid procedures (frozen elephant trunk+TEVAR), or those where use TEVAR as treatment option for RTAD were excluded. The following were also excluded: studies that provided mixed outcomes with other aortic diseases or had not provided data regarding the main outcomes, review articles, commentary and technical notes, editorials, and letters. Multicenter studies (>2 centers) that included vascular centers reporting their experiences separately were also excluded to avoid overlap and overestimation of the data. Duplicate studies were excluded and in case of metachronous publications from the same surgical group, only the latest report or the one with the largest number of patients was included. Four studies from 2 distinct vascular centers were considered eligible, as the patients were recruited during different time periods.6 –9
Ethical Considerations and Approval
Ethics committee approval or patient consent was waived due to the nature of the study.
Outcome Measures
The primary outcomes were the early (≤30 days) and late (>30 days) incidence of RTAD after TEVAR, as well as the pooled 30-day and late mortality of patients managed with open surgical repair or with conservative treatment. Secondary outcomes included the early and late proportions of patients treated with open surgical repair or conservative treatment, the incidence of RTAD according to the phase of TBAD (acute, subacute, or chronic) at the time of TEVAR, the incidence of RTAD according to patients’ clinical presentation at the admission, and the incidence of RTAD according to the proximal sealing zone of TEVAR endograft.
Search Strategy
The PICO (Population, Intervention, Comparison, Outcome) model (Supplemental Table 1) was followed to perform a systematic search to MEDLINE (database provider PubMed; from 1966 to November 2025), EMBASE (database provider Ovid; from 1980 to November 2025), and Google Scholar and Cochrane Central Register of Controlled Trials (November 2025). A snowball process of the reference lists from the eligible studies was following the retrieval of relevant reports from the databases searches. The following search items, including expanded medical subject headings terms were used in various combination: ((retrograde) AND (type a) AND (aortic dissection)) AND ((endovascular repair) OR (thoracic stent graft) OR (endograft) OR (graft)) AND (type b dissection). All English-language scientific studies related to RTAD following TEVAR, reported up to November 2025 were potentially eligible. Scrutiny was accomplished after full-text assessment by 2 authors, including the snowball process, to identify potential additional eligible studies. Disagreements were resolved through consensus or by discussion, with a third senior reviewer serving as the final arbitrator.
Data Extraction
Data were extracted by 2 independent authors in a prespecified datasheet Microsoft Excel file (Microsoft Corp., Redmond, WA, USA). Extracted data included study characteristics (authors, journal, year of publication, study design, timespan, country, center, and database) in addition to general clinical information (baseline demographics [age and sex]). The baseline data, including cardiovascular risk factors (ie, smoking history, hypertension, dyslipidemia, and diabetes mellitus) and other comorbidities (ie, chronic obstructive pulmonary disease, history of cerebrovascular event, coronary disease, and chronic renal failure), were also extracted. Moreover, data were collected regarding surgical urgency (ie, elective, emergent, and urgent); types of aortic endograft; the phase of TBAD in which every patient was treated, symptomatology at presentation; the zones of proximal entry tear; the zones of proximal sealing zone, the type of adjunctive procedures for TBAD treatment and the number of type Ia endoleaks (early [<30 days] and late [>30days]).
Study Quality Assessment and Publication Bias
The assessment of methodologic quality of each study was assessed by 2 authors, using the Newcastle-Ottawa scale (NOS). 10 The NOS was developed to assess the quality of the studies using the star system (maximum of 9 stars), in which a study was judged using 3 broad perspectives: (1) selection of the study groups, (2) comparability of the groups, and (3) ascertainment of the outcome of interest (Supplemental Table 2).
Risk of bias was assessed using the ROBINS-I (Risk Of Bias In Non-randomized Studies of Interventions) tool, which evaluates observational studies based on 7 domains of potential risk of bias, providing a score (low, moderate, serious, or critical), to achieve the maximum transparency of the conducted evaluation. 11 The overall quality and summary of evidence was assessed using the Grading of Recommendations Assessment, Development, and Evaluations (GRADE) for each of the main outcomes.12,13 Various factors were incorporated to upgrade or downgrade the overall quality of evidence, including risk of bias, inconsistency, indirectness, imprecision, large effect, dose response, and confounder control. 13 The assessment using the ROBINS-I tool and GRADE was performed by 2 independent investigators and any discrepancy was resolved after discussion with a third author.
Definitions
Retrograde type A dissection was reported as a complication among the eligible studies.6 –9,14 –32 It was defined as a new dissection originating after TEVAR for TBAD, in which the dissection flap progresses retrogradely into the ascending aorta.22,33 All events that occurred intraoperatively or within 30 days postoperatively were defined as early outcomes, whereas RTAD events occurring more than 30 days after surgery were defined as late outcomes.
Aortic dissections are classified based on time from onset of symptoms as hyperacute (<24 hours), acute (1–14 days), subacute (15–90 days), and chronic (>90 days). 34 Type B aortic dissections are further categorized as “complicated,” “with high-risk features,” or “uncomplicated.” Complicated dissection is characterized by the presence of malperfusion syndrome or rupture. High-risk features may include refractory pain, refractory hypertension, bloody pleural effusion, aortic diameter >40 mm, imaging evidence of malperfusion, entry tear on lesser curvature, or FL >22 mm. Uncomplicated TBADs do not have evidence of rupture, malperfusion syndrome, or high-risk features. 34
The proximal entry tear zone and aortic endograft landing zone were reported according to the Ishimaru and Mitchell classification.35,36
Statistical Analysis
Values of the concomitant outcomes were subsequently appropriately calculated, expressed as proportions and 95% confidence intervals (CIs), and thereafter transformed into quantities according to the Freeman-Tukey variant of the arcsine square root transformed proportion. The pooled effect estimates were calculated as the back-transformation of the weighted mean of the transformed proportions, using Der Simonian-Laird weights of random effects model and expressed as percentage proportions.
The interstudy heterogeneity (I2) was estimated using the Higgin’s I2 metric. Approximately, an I2<40% may be considered as low heterogeneity, 30% to 60% as moderate, 50% to 90% as substantial, and 75% to 100% as considerable. 12 The proportion incidence was assessed using the random effects model when I2 was >50% and with the fixed-effects model when I2 was 50%. A continuity correction equal to 0.5 was used for metrics associated with zero events. The results were visualized in forest plots. Publication bias was assessed using the Egger test and visualized by funnel plot. Statistical significance was set at p<0.050. Statistical analyses and plots were performed using the Comprehensive Meta-analysis statistical software, version V4 (Englewood, NJ, USA). 37
Results
Study Selection
A total of 538 study titles were identified by the initial search strategy. The review of the titles and abstracts revealed that 410 studies were irrelevant at the first screening stage. An additional 128 reports were evaluated further. Of the eligible studies 112 were excluded for one or more of the following reasons: studies providing data on the treatment of TBAD with TEVAR or hybrid or open repair (n=13); or no data relevant to main outcomes (n=4); studies providing mixed data with other thoracic aortic diseases (n=9); studies which provided data on other techniques (n=2); multicenter studies (n=3); nationwide data (n=2); registries (n=9); or case reports or series (n=28); review, commentary or technical notes (n=14); irrelevant (n=3); non-English studies (n=2); and studies with duplicate data and/or patients (n=6). Finally, after applying these exclusions, 22 retrospective studies6 –9,14 –32 with a total of 5088 patients, matched the inclusion criteria for the systematic review and meta-analysis after the addition of 6 studies6,7,9,29,31,32 resulting from the snowball process (Figure 1). Four studies from 2 vascular centers were included in the present meta-analysis because they provided data from different patient recruitment periods.6 –9 Following data extraction, 57 patients from 20 studies6 –9,15 –24,26 –30,32 in the early period and 96 patients from 20 studies6 –9,15,16,18 –29,31,32 in the late period presenting with RTAD were included in the present meta-analysis for further analysis. All eligible studies encompassing patients with RTAD are summarized in Tables 1 and 2. The mean follow-up was 28 months (ranged from 12 to 70 months).
Baseline Characteristics of 57 Patients With RTAD in the Early Period.
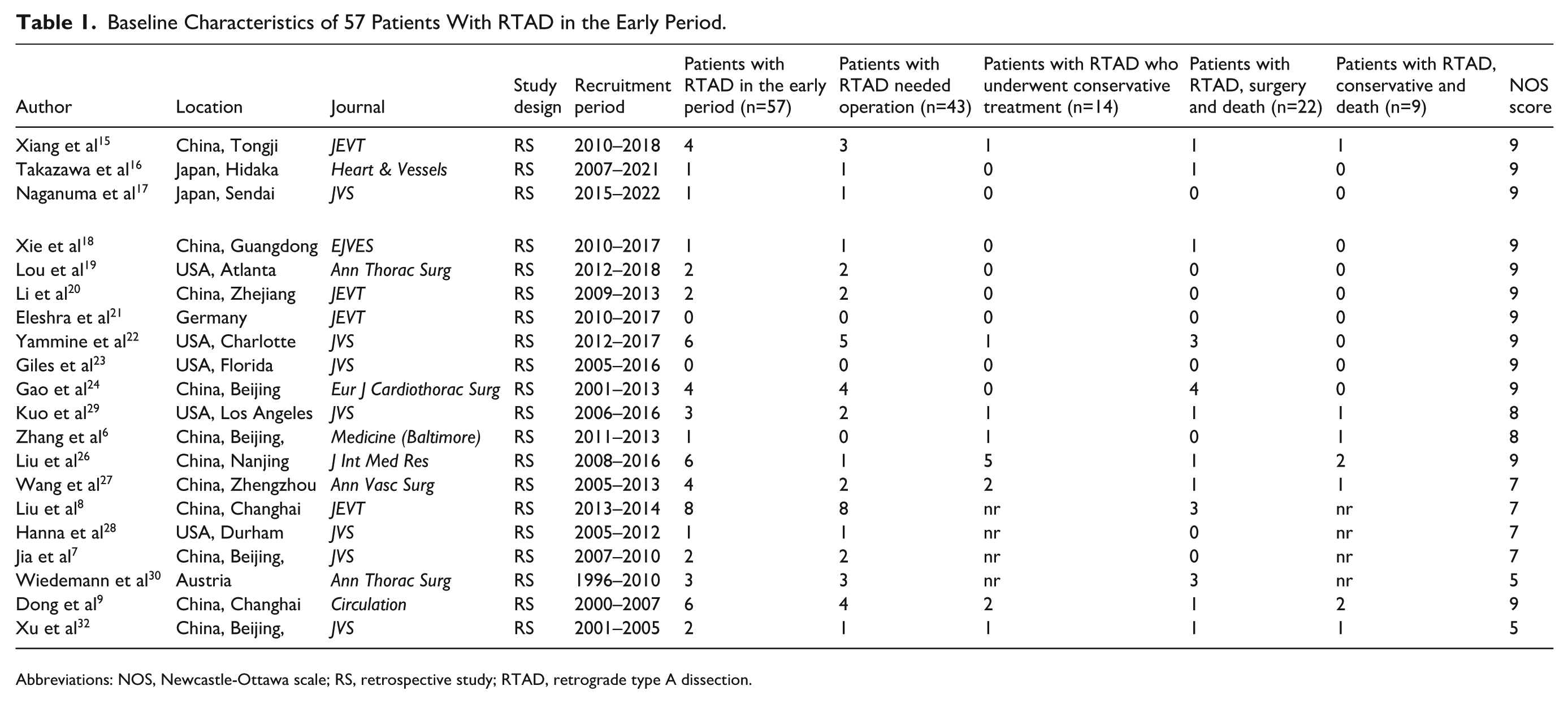
Abbreviations: NOS, Newcastle-Ottawa scale; RS, retrospective study; RTAD, retrograde type A dissection.
Baseline Characteristics of 108 Patients With RTAD in the Late Period.
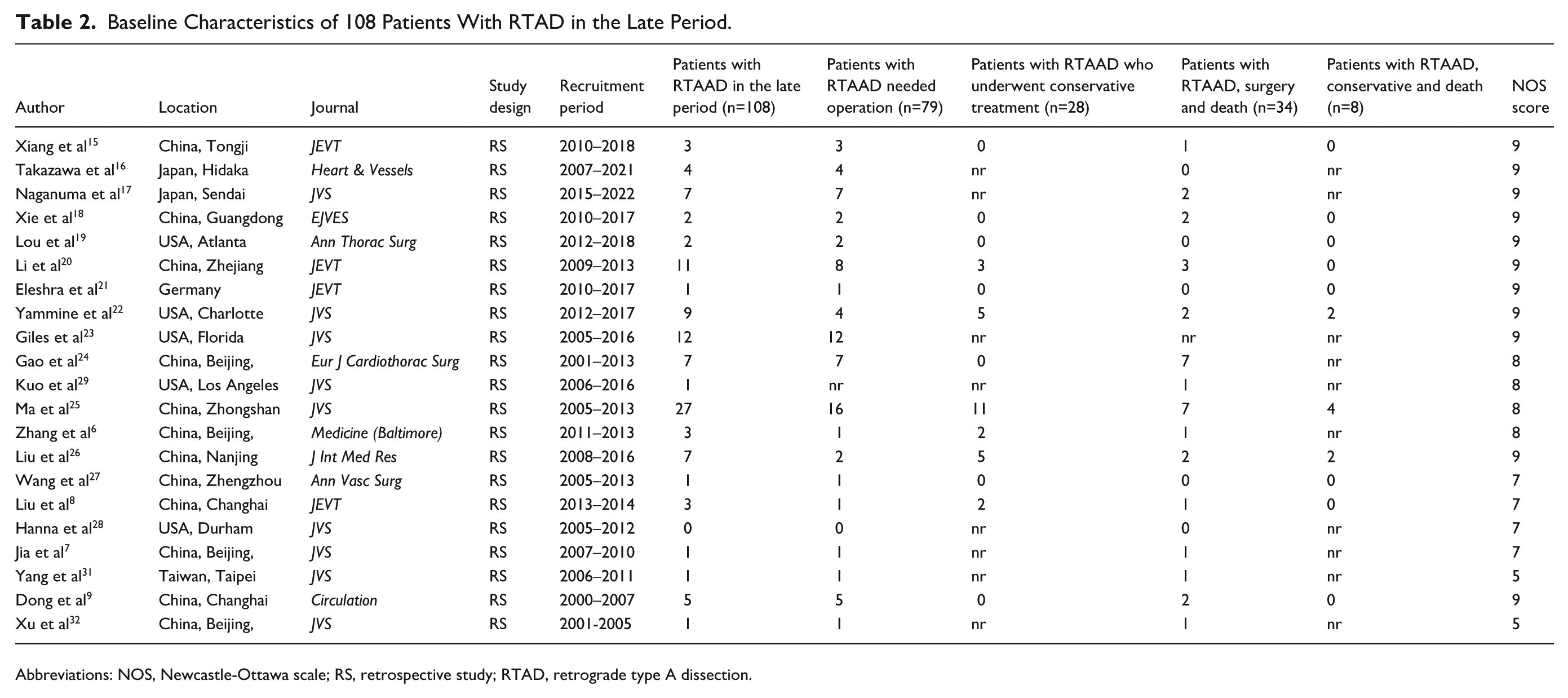
Abbreviations: NOS, Newcastle-Ottawa scale; RS, retrospective study; RTAD, retrograde type A dissection.
Study Characteristics
The baseline study characteristics of the 22 eligible studies published between 2006 and 2024, including the current systematic review, are presented in Tables 1 and 2. Of the 5088 patients included, with mean age of 57 (50–66) years, 3611 (71%) were male. Of them, 67% (3416 of 5088) had hypertension, 8% (429 of 5088) had coronary artery disease, 8% (412 of 5088) dyslipidemia, 6% (308 of 5088) chronic kidney disease, 5.6% (290/5088) chronic obstructive pulmonary disease, 5% diabetes (255 of 5088), 2.3% (120/5088) history of cerebrovascular diseases, and 2.3 % (121/5088) had prior aortic procedure whereas 34% (1707/5088) were active smokers.
Sixty-two percent of all TEVARs were elective, 23% emergent, and 15% urgent. Overall, 51% of patients were treated during the acute phase, 21% during the subacute phase, and 28% during the chronic phase. At presentation, 51% of patients were symptomatic and 49% asymptomatic. The most common presenting symptom was refractory (intractable) pain (27%), followed by malperfusion (19%), impending or contained rupture (5%), and refractory hypertension (4%) as they were extracted from 16 studies.6,9,15 –17,19 –25,28,29,31,32
Various aortic endografts were used for the treatment of TBAD reported in 16 studies.9,15,17 –26,28 –32 The most commonly employed device was the Valiant (Medtronic Inc., Minneapolis, MN, USA) in 24% of cases, followed by the Zenith TX2 (Cook Medical, Bloomington, IN, USA) in 17%, Hercules (MicroPort, Shanghai, China) in 8%, cTAG (W. L. Gore & Associates, Flagstaff, AZ, USA) in 7%, Talent (Medtronic Inc., Minneapolis, MN, USA) in 6%, and Ankura (Lifetech Scientific, Shenzhen, China) in 6%.
Treatment of TBAD was achieved with standard TEVAR in the majority of cases (92%), while adjunctive procedures were required in a small proportion (8%), including chimney+TEVAR in 4% and supra-aortic vessels’ bypass in 4%. According to the Ishimaru and Mitchell classification35,36 the proximal sealing zone for TEVAR was located in zone 0 in 12 patients, zone 1 in 64 patients, zone 2 in 1430 patients, and zone ≥3 in 780 patients as reported across 13 studies.6,7,15 –23,26,28
Risk of Bias in Included Studies
The overall risk of bias was judged to be moderate in 19 studies7 –9,15 –25,28 –32 and high in 3 studies.6,26,27 The 2 most common cause for failing to achieve low risk of bias were confounding factors (Supplemental Figure 1).
Certainty of Evidence
The GRADE evidence quality assessment indicated a very low certainty of evidence for all the primary outcomes (Table 3). Certainty statements were built upon GRADE and follow the odds ratio and 95% CI for all main outcomes, to assist outcome interpretation.
GRADE Summary of Findings.
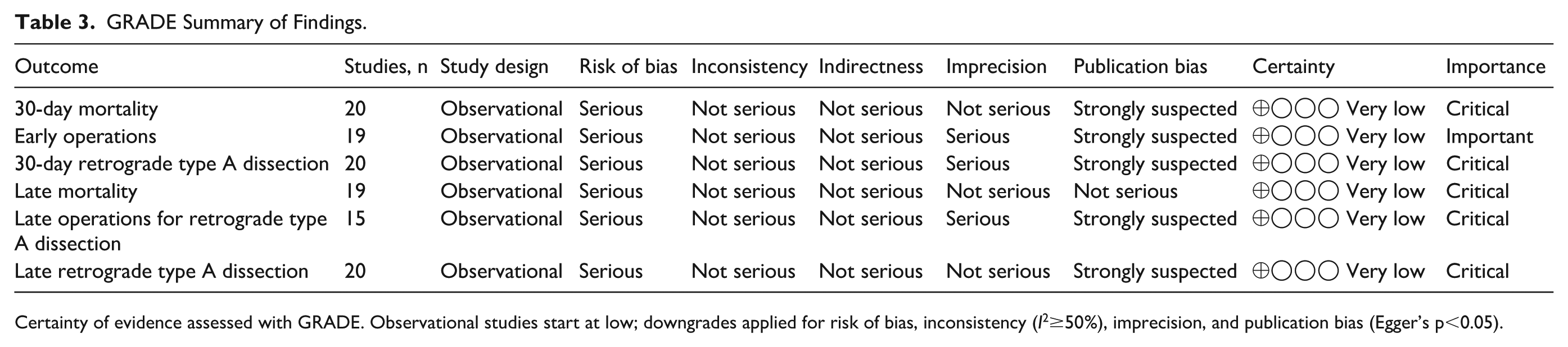
Certainty of evidence assessed with GRADE. Observational studies start at low; downgrades applied for risk of bias, inconsistency (I2≥50%), imprecision, and publication bias (Egger’s p<0.05).
Meta-analysis
Incidence of RTAD
The 30-day pooled incidence of RTAD was 1.8% (95% CI 1.2%–2.7%, heterogeneity, p=0.01, I2=58%; publication bias, p=0.04) among 18 studies6,8,9,15,16,18 –24,26 –30,32 (Figure 2A). The individual study crude rate among the eligible studies ranged from 0.2% to 10.3%. The study by Liu et al 26 reported the highest crude rate of RTAD after TEVAR of 10.3% (95% CI 4.7%–21.2%). Supplemental Figure 2A demonstrates the funnel plots for evaluation of potential publication bias
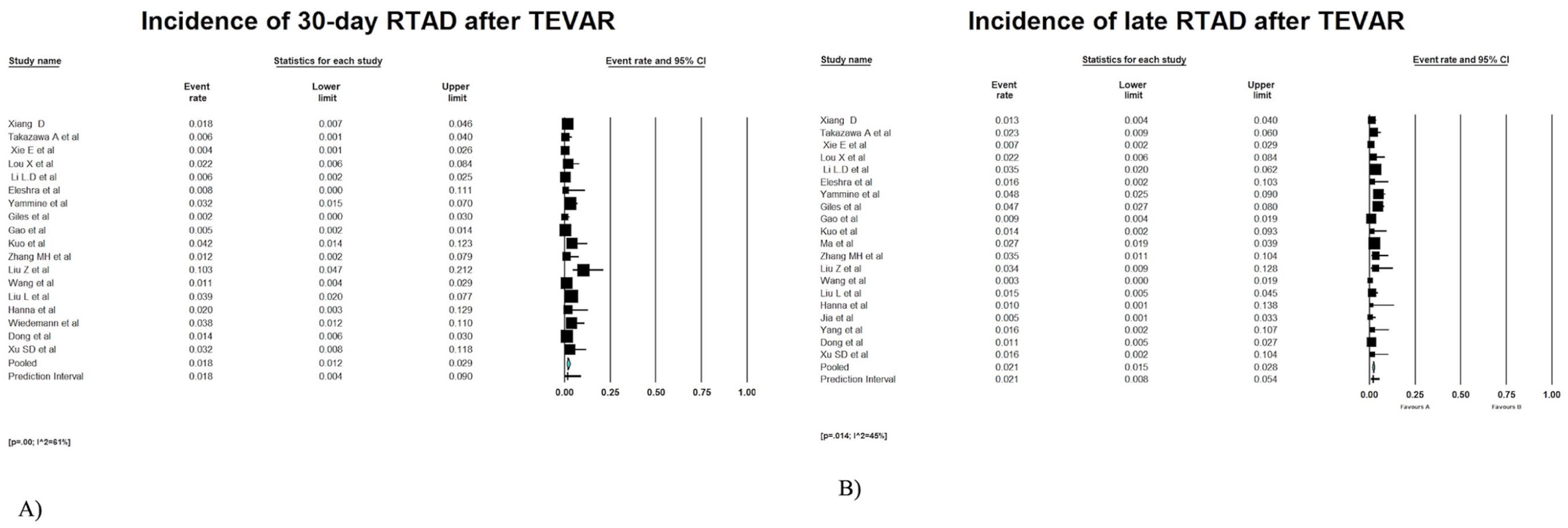
Forest plot presenting the meta-analysis of incidence of retrograde type A dissection after TEVAR. Event rates in the individual studies presented as squares, with 95% confidence interval (CIs) presented as extending lines. The pooled event rate with its 95% CI is depicted as a diamond. ES, effect estimate.
The pooled late incidence of RTAD was 2.2% (95% CI 1.6%–3.0%, heterogeneity, p=0.017, I2=44%; publication bias, p=0.018) among 20 studies6 –9,15,16,18 –29,31,32 (Figure 2B). The individual study crude rate among the eligible studies ranged from 0.3% to 4.8%. Yaminne et al 22 reported the highest crude rate of RTAD after TEVAR of 4.8% (95% CI 2.5%–9.0%). Supplemental Figure 2B demonstrates the funnel plots for evaluation of potential publication bias
Mortality of RTAD After Open Surgery
The pooled 30-day mortality after open surgery was 43.7% (95% CI 27.6%–61.2%; heterogeneity, p=0.58; I2=0%; publication bias, coefficient=0.12; SE=1.09; p=0.90) in 11 eligible studies7 –9,15,19,20,22,24,27,29,30 (Figure 3A). The individual study crude rate for the eleven eligible studies ranged from 16.7% to 90%.
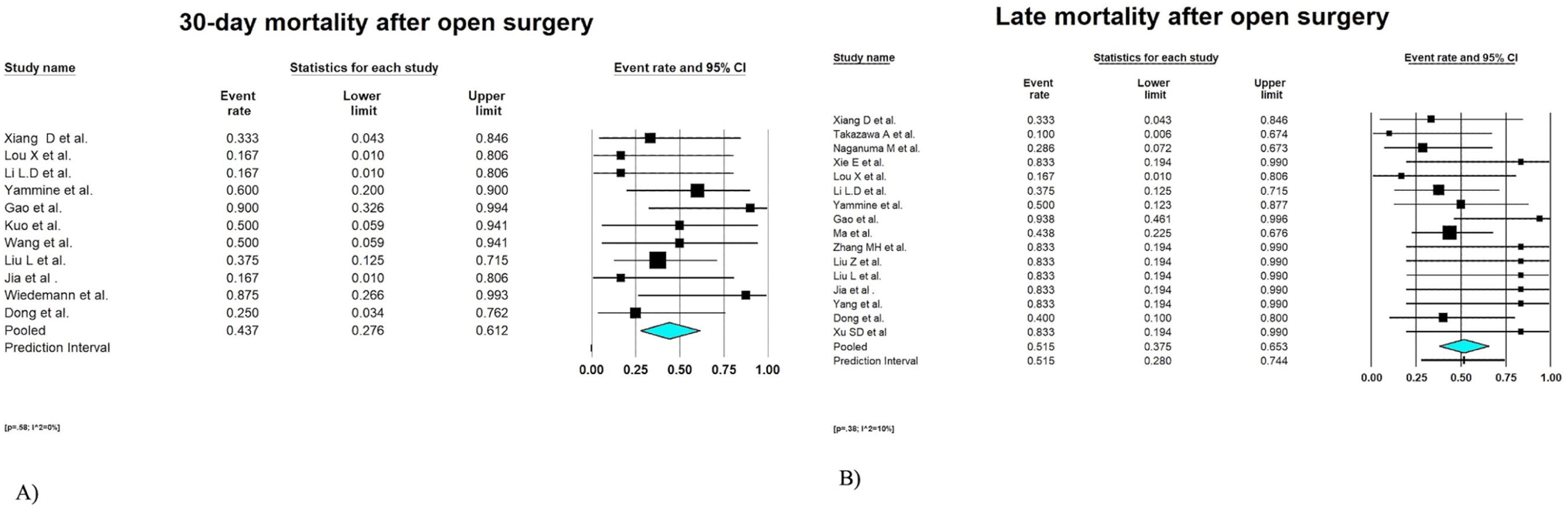
Forest plot presenting the meta-analysis of 30-day and late mortality rate after open surgical repair. Event rates in the individual studies presented as squares, with 95% confidence interval (CIs) presented as extending lines. The pooled event rate with its 95% CI is depicted as a diamond. ES, effect estimate.
The pooled late mortality rate after open surgery was 51.5% (95% CI 37.5%–65.3%; heterogeneity, p=0.38; I2=10%; publication bias, coefficient=2.21; SE=0.60; p=0.04) in 16 studies6 –9,15 –20,22,24 –26,31,32 (Figure 3B). The individual study crude rate for the 16 eligible studies ranged from 16.7% to 93.8%.
Mortality of RTAD After Conservative Treatment
The pooled rate of 30-day mortality in patients who treated conservatively was 68.1% (95% CI 43.8%–85.4%; heterogeneity, p=0.75; I2=0%; publication bias, coefficient=4.85; SE=0.61; p=0.004) in 7 eligible studies6,9,15,26,27,29,32 (Figure 4A). The individual study crude rate for the 7 eligible studies ranged from 40% to 83.3%.
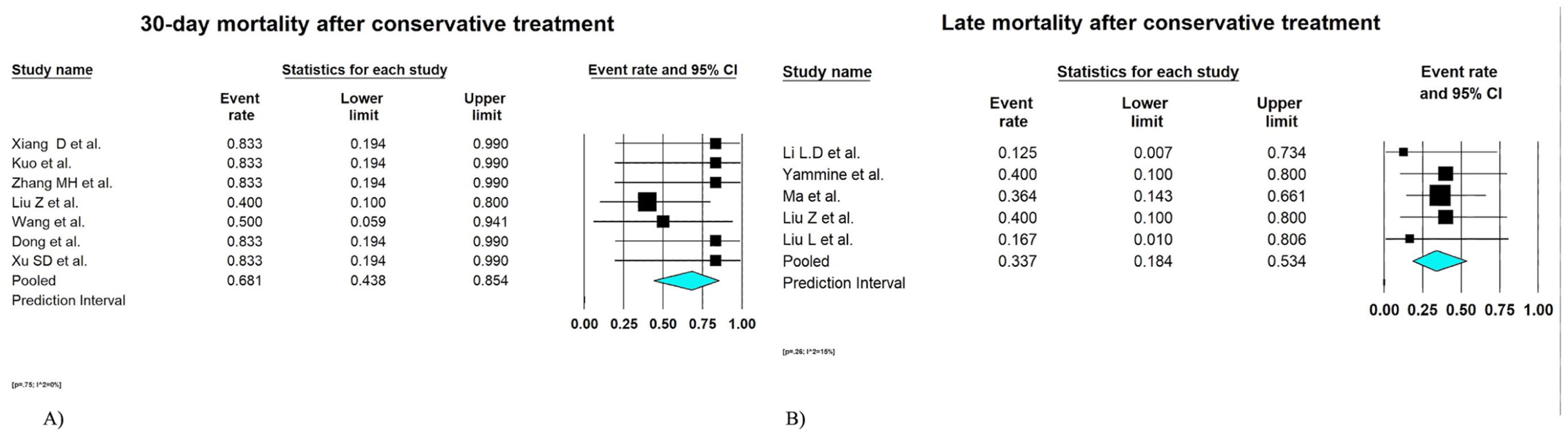
Forest plot presenting the meta-analysis of 30-day and late mortality rate after conservative repair. Event rates in the individual studies presented as squares, with 95% confidence interval (CIs) presented as extending lines. The pooled event rate with its 95% CI is depicted as a diamond. ES, effect estimate.
The pooled late mortality rate of conservatively-treated patients was 33.7% (95% CI 18.4%–53.4%; heterogeneity, p=0.26; I2=15%; publication bias, coefficient=1.16; SE=0.52; p=0.27) in 5 studies8,20,22,25,26 (Figure 4B). The individual study crude rate for the 7 eligible studies ranged from 12.5% to 40%.
Incidence of Patients With RTAD Treated With Open Surgery
The pooled incidence of patients with RTAD treated with open surgery was 72% (95% CI 58.5%–82.4%; heterogeneity, p=0.80; I2=0%; publication bias, coefficient=2.43; SE=0.90; p=0.02) in 18 eligible studies6 –9,15 –20,22,24,26 –30 (Figure 5A). The individual study crude rate for the 7 eligible studies ranged from 16.7% to 94.4%.
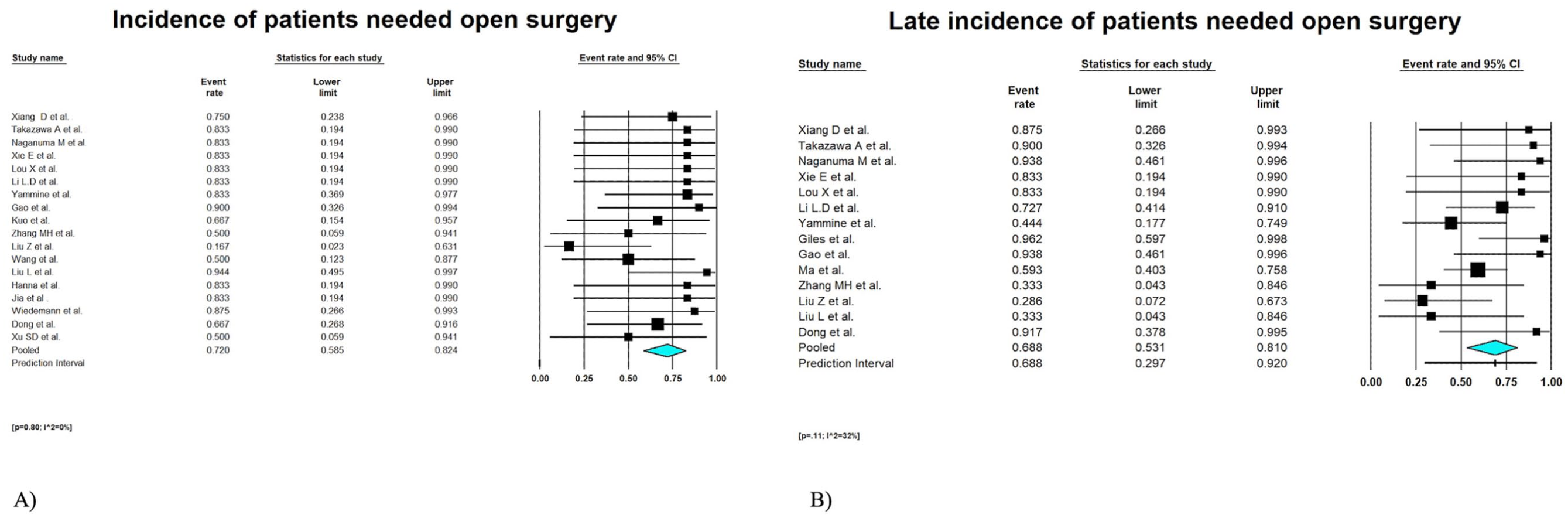
Forest plot presenting the meta-analysis of incidence of patients required open surgery during the early and late periods. Event rates in the individual studies presented as squares, with 95% confidence interval (CIs) presented as extending lines. The pooled event rate with its 95% CI is depicted as a diamond. ES, effect estimate.
The pooled late incidence of patients with RTAD treated with open surgery was 68.8% (95% CI 53.1%–81%; heterogeneity, p=0.11; I2=32%; publication bias, coefficient=2.17; SE=0.60; p=0.05) in 14 eligible studies6,8,9,15 –20,22 –26 (Figure 5B). The individual study crude rate for the 14 eligible studies ranged from 28.6% to 96.2%.
Incidence of Patients With RTAD Treated With Conservative Treatment
The pooled incidence of patients with RTAD treated conservatively was 32.5% (95% CI 20%–48.1%; heterogeneity, p=0.77; I2=0%; publication bias, coefficient=1.66; SE=1.05; p=0.12) in 14 eligible studies6,9,15 –20,22,24,26,27,29,32(Supplemental Figure 3A). The individual study crude rate for the 14 eligible studies ranged from 10% to 83.3%.
The pooled late incidence of patients with RTAD treated conservatively was 39.1% (95% CI 25.9%–54%; heterogeneity, p=0.26; I2=15%; publication bias, coefficient=1.16; SE=0.69; p=0.27) in 11 studies6,8,9,15,18 –20,22,24 –26 (Supplemental Figure 3B). The individual study crude rate for the 14 eligible studies ranged from 6.3% to 66.7%.
Subgroup Analysis
We performed a subgroup analysis based on the TBAD phase (acute, subacute, or chronic) at the time of TEVAR and the occurrence of RTAD as a complication, as well as on patients’ symptomatology at admission.
The pooled incidence of RTAD in acute TBAD treatment was 3.2% (95% CI 2.3%–4.3%; heterogeneity, p=0.11; I2=32%; publication bias, coefficient=1.37; SE=0.90; p=0.19) in 15 eligible studies6,8,15,17 –21,23,26 –30,32 (Supplemental Figure 4A). The individual study crude rate for the 15 eligible studies ranged from 0.7% to 10.3%.
The pooled incidence of RTAD in subacute TBAD treatment was 1.6% (95% CI 0.9%–3.1%; heterogeneity, p=0.037; I2=57%; publication bias, coefficient=0.82; SE=1.71; p=0.45) in 6 eligible studies9,15,18,22,24,32 (Supplemental Figure 4B). The individual study crude rate for the 6 eligible studies ranged from 0.4% to 4.8%.
The pooled incidence of RTAD in chronic TBAD treatment was 2% (95% CI 1.2%–3.4%; heterogeneity, p=0.005; I2=60%; publication bias, coefficient=1.86; SE=1.28; p=0.09) in 11 eligible studies.6 –9,16,22 –24,26,31,32 (Supplemental Figure 4C). The individual study crude rate for the 11 eligible studies ranged from 0.2% to 5.4%.
Regarding the patients’ symptoms at hospital admission, the pooled incidence of RTAD for complicated patients was 2.6% (95% CI 1.6%–4.1%; heterogeneity, p=0.014; I2=60%; publication bias, coefficient=4.7; SE=1.23; p=0.003) in 8 eligible studies7,8,15 –18,23,24 (Supplemental Figure 5A). The individual study crude rate for the 8 eligible studies ranged from 1.1% to 5.4%.
The pooled incidence of RTAD uncomplicated patients was 1.5% (95% CI 0.5%–4.4%; heterogeneity, p=0.012; I2=87%; publication bias, coefficient=2.52; SE=1.09; p=0.04) in 8 eligible studies6,15,19 –21,28,31,32 (Supplemental Figure 5B). The individual study crude rate for the 8 eligible studies ranged from 0.1% to 15.9%.
The pooled incidence of RTAD for TEVAR in sealing zone 1 was 15.4% (95% CI 8.2%–27.2%; heterogeneity, p=0.026; I2=27%; publication bias, coefficient=1.5; SE=0.76; p=0.27) in 4 studies7,25,28,31 (Supplemental Figure 6A).
The pooled incidence of RTAD in sealing zone 2 TEVAR was 6.9% (95% CI 4.8%–9.9%; heterogeneity, p=0.02; I2=71%; publication bias, coefficient=0.03; SE=1.06; p=0.97) in 17 studies6 –8,15 –23,25,26,28,29,31 (Supplemental Figure 6B).
Discussion
In this systematic review and meta-analysis, we report the evidence-based incidence and mortality rate of RTAD after TEVAR in patients with TBAD, as well as the proportion of patients who required open surgery or conservative management. To the best of our knowledge, this is the first study to comprehensively synthesize all available evidence on this uncommon complication following TEVAR.
The pooled incidence of RTAD was 1.8% during the early and 2.2% during the late follow-up period. These findings are consistent with 2 previous meta-analyses that reported similar pooled estimates of early RTAD incidence, although they did not provide additional evidence for the late follow-up period.4,38 Several factors have been reported to contribute to this complication after TEVAR, emphasizing the importance of the phase in which the procedure is performed.4,17,20,27 Our subgroup analysis showed that in the acute phase, the incidence of RTAD was significantly higher than with subacute and chronic phases. This outcome is consistent with the findings of Li et al, 20 who demonstrated that subacute patients exhibited better early and midterm clinical results after 5 years of follow-up. 20 A possible explanation for this observation may relate to the condition of the dissecting membrane; during the acute phase the membrane tends to be more fragile, while in the chronic phase, it becomes less fragile. 39
Another factor contributing to RTAD appears to be the sealing zone in the aortic arch during TEVAR. Previous meta-analysis demonstrated a statistically-significant difference in the incidence of RTAD between the sealing zones 0 to 1 and 2 (p<0.0001). Similar findings were reported in the study by Canaud et al 40 showing that the more proximal sealing zone, the higher the risk of RTAD. This study also observed that deployment of the stent-graft in zone 1 is another significant risk factor of RTAD, with the risk being approximately double compared with zone 2.
In addition to the sealing zone of the endograft, several other factors have been suggested in the literature as potential contributors to the development of RTAD following TEVAR. These include connective tissue disorders (such as Marfan syndrome), excessive stent-graft oversizing, aggressive balloon dilatation, and device-related characteristics.9,25,40 In particular, excessive oversizing of the stent-graft has been associated with increased mechanical stress on the fragile dissected aortic wall, which may facilitate retrograde propagation of the dissection flap. Furthermore, more proximal landing zones in the aortic arch may expose the ascending aorta to higher shear stress at the proximal edge of the endograft.9,25,40 However, these variables were inconsistently reported across the included studies and therefore could not be formally analyzed in the present meta-analysis.
A tear-oriented exclusion strategy remains the standard of care for the treatment of aortic dissection. Open surgery continues to represent the gold standard for RTAD, aiming to resect and exclude the intimal tear, most commonly through total arch replacement or the frozen elephant trunk technique.41,42 However, this approach is associated with substantial mortality and morbidity.41,42 Reported postoperative mortality rates range from 13% up to 46% depending on the extent of open repair.43 –45 Consistent with these findings, our study demonstrated that 72% of patients with RTAD required open surgery with pooled mortality rates of 43.7% in the early period and 51.7% in the late period. The remarkably high mortality rate is largely driven by a non-negligible incidence of severe postoperative complications, including neurological, renal, and respiratory dysfunction. 46
Advances in endovascular technology have enabled the rapid development of endovascular techniques for the treatment of RTAD. Recently, several studies have reported a remarkably low mortality rate compared with open surgery (3.9% for TEVAR and 12.5% for open repair).46,47 Furthermore, the rates of postoperative neurological complications (stroke and spinal cord injury; 4.1% for TEVAR and 11.6% for open repair) and aortic-related complications associated with stent-graft placement (9.8%) such as new intimal tear, progression of ascending aortic dissection, and aortic rupture were also notably low.46,47 These findings highlight the advantages of TEVAR in reducing immediate perioperative risks. However, it is important to note that long-term mortality and other composite morbidities, including postoperative dialysis, ischemic bowel, and postoperative dialysis did not differ significantly between the 2 surgical approaches. 46 The authors suggested that although TEVAR may offer short-term benefits, long-term outcomes were comparable between the 2 surgical arms if the patient survives open aortic repair. 46
An additional concern for TEVAR is the potential for stent-induced new entry (SINE). 47 Several preventive measures have been reported, including careful preoperative planning, limiting graft oversizing ≤10%, avoiding ballooning and maintaining strict blood pressure control to minimize this risk. Close collaboration between physician and anesthesiology team is of paramount importance during endograft deployment. 47
Conservative treatment for patients with RTAD has poor prognosis. The main reasons to follow this strategy was age and/or hemodynamic instability and/or unfitness for surgery. 48 Unfortunately, few studies reported outcomes based on conservative treatment of patients with RTAD, some of them are limited to case reports.48 –50 The mortality rate was 10% in a recently published meta-analysis with a mean follow-up of 33 months. 48 In the present meta-analysis, the mortality rate was higher up to 40%. However, the current evidence is poor and needs to be validated by further and more robust data before such a strategy could be suggested more widely.
Limitations
This study has several limitations, mainly reflecting those of the included studies. First, the retrospective design of all included studies introduced considerable bias. The risk of bias, assessed with the ROBINS-I tool, varied significantly among studies, with 14% of them being characterized as low quality. Second, there was significant heterogeneity regarding the aortic endografts which used for TEVAR in TBAD. This merits special attention as a possible cause for RTAD, however, these data are missing and needs further clarification. Third, there is variation in the learning curve and expertise across the eligible studies. The results between specialized aortic centers with high-volume and greater experience may differ from other centers with low-volume and less expertise. As a result, the reported outcomes should be evaluated with caution, as they may not reflect current outcomes in less experienced and low-volume centers. Fourth, Sensitivity analyses were considered to evaluate the robustness of the pooled estimates. However, given the relatively small number of RTAD events reported across several studies, the statistical reliability of such analyses would have been limited and potentially unstable. Finally, as the RTAD represents an uncommon but with high mortality rate complication, more studies with high-volume centers and longer follow-up are required. A head to head analysis comparing open and endovascular repair performed at expert vascular centers could provide further clarification on this still unresolved topic. In addition, meta-regression analysis could potentially provide further insight into study-level associations between outcomes and potential confounders, such an analysis was not feasible in the present study. Several clinically-relevant variables, including connective tissue disorders, stent-graft oversizing, device characteristics, and detailed anatomical features of the aortic arch, were inconsistently or incompletely reported across the included studies. Consequently, performing a robust meta-regression analysis could have introduced substantial bias and unreliable estimates. Future studies with standardized reporting of procedural and anatomical variables may allow more comprehensive exploration of these associations.
Conclusion
Retrograde type A dissection represents a very rare complication after TEVAR for the treatment of TBAD. Despite its low incidence, a substantial proportion of affected patients require open surgical repair, which is associated with a non-negligible mortality rate. The timing of treatment for TBAD, as well as careful selection of the proximal sealing zone for TEVAR, should be cautiously considered to reduce the risk of RTAD.
Supplemental Material
sj-docx-1-jet-10.1177_15266028261453320 – Supplemental material for Incidence and Outcomes of Retrograde Type A Aortic Dissection After Thoracic Endovascular Aortic Repair for Type B Aortic Dissection: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-1-jet-10.1177_15266028261453320 for Incidence and Outcomes of Retrograde Type A Aortic Dissection After Thoracic Endovascular Aortic Repair for Type B Aortic Dissection: A Systematic Review and Meta-analysis by Georgios I. Karaolanis, Konstantinos Koumarelas, Konstantinos Kotopoulos, Dimitrios Papazoglou, Leszek Kukulski, Daniel Becker, Michel J. Bosiers, Silvan Jungi, Drosos Kotelis and Vladimir Makaloski in Journal of Endovascular Therapy
Supplemental Material
sj-docx-2-jet-10.1177_15266028261453320 – Supplemental material for Incidence and Outcomes of Retrograde Type A Aortic Dissection After Thoracic Endovascular Aortic Repair for Type B Aortic Dissection: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-2-jet-10.1177_15266028261453320 for Incidence and Outcomes of Retrograde Type A Aortic Dissection After Thoracic Endovascular Aortic Repair for Type B Aortic Dissection: A Systematic Review and Meta-analysis by Georgios I. Karaolanis, Konstantinos Koumarelas, Konstantinos Kotopoulos, Dimitrios Papazoglou, Leszek Kukulski, Daniel Becker, Michel J. Bosiers, Silvan Jungi, Drosos Kotelis and Vladimir Makaloski in Journal of Endovascular Therapy
Supplemental Material
sj-jpg-3-jet-10.1177_15266028261453320 – Supplemental material for Incidence and Outcomes of Retrograde Type A Aortic Dissection After Thoracic Endovascular Aortic Repair for Type B Aortic Dissection: A Systematic Review and Meta-analysis
Supplemental material, sj-jpg-3-jet-10.1177_15266028261453320 for Incidence and Outcomes of Retrograde Type A Aortic Dissection After Thoracic Endovascular Aortic Repair for Type B Aortic Dissection: A Systematic Review and Meta-analysis by Georgios I. Karaolanis, Konstantinos Koumarelas, Konstantinos Kotopoulos, Dimitrios Papazoglou, Leszek Kukulski, Daniel Becker, Michel J. Bosiers, Silvan Jungi, Drosos Kotelis and Vladimir Makaloski in Journal of Endovascular Therapy
Supplemental Material
sj-tif-4-jet-10.1177_15266028261453320 – Supplemental material for Incidence and Outcomes of Retrograde Type A Aortic Dissection After Thoracic Endovascular Aortic Repair for Type B Aortic Dissection: A Systematic Review and Meta-analysis
Supplemental material, sj-tif-4-jet-10.1177_15266028261453320 for Incidence and Outcomes of Retrograde Type A Aortic Dissection After Thoracic Endovascular Aortic Repair for Type B Aortic Dissection: A Systematic Review and Meta-analysis by Georgios I. Karaolanis, Konstantinos Koumarelas, Konstantinos Kotopoulos, Dimitrios Papazoglou, Leszek Kukulski, Daniel Becker, Michel J. Bosiers, Silvan Jungi, Drosos Kotelis and Vladimir Makaloski in Journal of Endovascular Therapy
Supplemental Material
sj-tif-5-jet-10.1177_15266028261453320 – Supplemental material for Incidence and Outcomes of Retrograde Type A Aortic Dissection After Thoracic Endovascular Aortic Repair for Type B Aortic Dissection: A Systematic Review and Meta-analysis
Supplemental material, sj-tif-5-jet-10.1177_15266028261453320 for Incidence and Outcomes of Retrograde Type A Aortic Dissection After Thoracic Endovascular Aortic Repair for Type B Aortic Dissection: A Systematic Review and Meta-analysis by Georgios I. Karaolanis, Konstantinos Koumarelas, Konstantinos Kotopoulos, Dimitrios Papazoglou, Leszek Kukulski, Daniel Becker, Michel J. Bosiers, Silvan Jungi, Drosos Kotelis and Vladimir Makaloski in Journal of Endovascular Therapy
Supplemental Material
sj-tif-6-jet-10.1177_15266028261453320 – Supplemental material for Incidence and Outcomes of Retrograde Type A Aortic Dissection After Thoracic Endovascular Aortic Repair for Type B Aortic Dissection: A Systematic Review and Meta-analysis
Supplemental material, sj-tif-6-jet-10.1177_15266028261453320 for Incidence and Outcomes of Retrograde Type A Aortic Dissection After Thoracic Endovascular Aortic Repair for Type B Aortic Dissection: A Systematic Review and Meta-analysis by Georgios I. Karaolanis, Konstantinos Koumarelas, Konstantinos Kotopoulos, Dimitrios Papazoglou, Leszek Kukulski, Daniel Becker, Michel J. Bosiers, Silvan Jungi, Drosos Kotelis and Vladimir Makaloski in Journal of Endovascular Therapy
Supplemental Material
sj-tif-7-jet-10.1177_15266028261453320 – Supplemental material for Incidence and Outcomes of Retrograde Type A Aortic Dissection After Thoracic Endovascular Aortic Repair for Type B Aortic Dissection: A Systematic Review and Meta-analysis
Supplemental material, sj-tif-7-jet-10.1177_15266028261453320 for Incidence and Outcomes of Retrograde Type A Aortic Dissection After Thoracic Endovascular Aortic Repair for Type B Aortic Dissection: A Systematic Review and Meta-analysis by Georgios I. Karaolanis, Konstantinos Koumarelas, Konstantinos Kotopoulos, Dimitrios Papazoglou, Leszek Kukulski, Daniel Becker, Michel J. Bosiers, Silvan Jungi, Drosos Kotelis and Vladimir Makaloski in Journal of Endovascular Therapy
Supplemental Material
sj-tif-8-jet-10.1177_15266028261453320 – Supplemental material for Incidence and Outcomes of Retrograde Type A Aortic Dissection After Thoracic Endovascular Aortic Repair for Type B Aortic Dissection: A Systematic Review and Meta-analysis
Supplemental material, sj-tif-8-jet-10.1177_15266028261453320 for Incidence and Outcomes of Retrograde Type A Aortic Dissection After Thoracic Endovascular Aortic Repair for Type B Aortic Dissection: A Systematic Review and Meta-analysis by Georgios I. Karaolanis, Konstantinos Koumarelas, Konstantinos Kotopoulos, Dimitrios Papazoglou, Leszek Kukulski, Daniel Becker, Michel J. Bosiers, Silvan Jungi, Drosos Kotelis and Vladimir Makaloski in Journal of Endovascular Therapy
Footnotes
Author Contributions
Scrutiny was accomplished after full-text assessment by 2 authors (G.I.K. and K.K.), including the snowball process, to identify potential additional eligible studies. Disagreements were resolved through consensus or by discussion, with a third senior reviewer (V.M.) serving as the final arbitrator. Data were extracted by 2 independent authors (G.I.K. and K.K.) in a prespecified datasheet Microsoft Excel file (Microsoft Corp., Redmond, WA, USA). The assessment of methodologic quality of each study was assessed by 2 authors (G I.K. and K.K.), using the Newcastle-Ottawa scale (NOS). The assessment using the ROBINS-I tool and GRADE was performed by 2 independent investigators (G.I.K. and K.K.) and any discrepancy was resolved after discussion with a third author (V.M.).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.