
Abstract
Background:
Fenestrated endovascular aortic repair (FEVAR) is an established and effective treatment for thoracoabdominal aortic aneurysms (TAAAs). Although secondary endovascular interventions are not uncommon during follow-up, device-related failures causing type III endoleaks are rare but potentially life-threatening. When these defects occur within the visceral segment, standard relining techniques may be unfeasible, requiring alternative endovascular strategies to avoid open conversion.
Case Presentation:
A 73-year-old man, previously treated with a custom-made FEVAR, presented 3 years after the index procedure with severe back pain. Urgent computed tomography angiography revealed a large endoleak in the visceral segment, associated with aneurysm sac expansion and contained rupture. After relining of the superior mesenteric artery and the left renal artery, a type III endoleak originating from a small fabric defect between these vessels was identified and selectively catheterized. The defect was successfully treated by deploying an Amplatzer Vascular Plug IV across the graft tear.
Results:
Completion angiography demonstrated near-complete exclusion of the endoleak. Follow-up imaging confirmed progressive aneurysm sac shrinkage and full endoleak resolution at 1 year, with preserved visceral and renal perfusion.
Conclusion:
In selective settings, plug embolization represents a practical and durable bailout option for type III endoleaks caused by small fabric disruptions after FEVAR, especially when conventional relining is not feasible. This approach enables rapid hemodynamic stabilization and offers favorable mid-term outcomes in high-risk patients.
Clinical Impact
Type IIIb endoleaks caused by fabric disruption after FEVAR are rare but potentially catastrophic complications that may lead to aneurysm rupture and require urgent treatment. When the defect is located within the fenestrated visceral segment, conventional relining techniques may be technically unfeasible or risk compromising target vessel perfusion. This report describes a novel bailout strategy based on selective catheterization of the graft defect and deployment of an Amplatzer Vascular Plug IV directly across the fabric tear. The technique allowed exclusion of the endoleak and preservation of visceral branch patency, expanding the endovascular armamentarium.
Introduction
Fenestrated and branched endovascular aortic repair has revolutionized the management of thoracoabdominal aortic aneurysms (TAAAs), offering reduced perioperative morbidity and mortality compared to open repair. 1 However, late complications associated with device material failure may arise, and while the majority of these events can be treated with endovascular techniques, there are circumstances in which a standard endovascular solution may not be feasible or effective. In these cases, alternative approaches should be considered to prevent the need for open surgical conversion.2-5
We report a case of a ruptured TAAA in a patient previously treated with fenestrated endovascular aortic repair (FEVAR), successfully managed with an emergency endovascular exclusion of a fabric hole using a vascular plug.
Case Report
A 73-year-old man with a history of hypertension, chronic obstructive pulmonary disease, and ischemic heart disease had undergone a custom-made FEVAR for a TAAA in 2021. The postoperative course and the follow-up were uneventful with no aneurysm sac enlargement. Three years after the FEVAR procedure, the patient presented to the emergency department, hemodynamically stable but with severe back pain. An emergent contrast-enhanced computed tomography (CT) scan showed a massive endoleak at the level of visceral vessels, between the superior mesenteric artery (SMA) and the left renal artery (LRA), associated with sac expansion (from 72 mm to 93 mm) and contained rupture with periaortic hematoma (Figure 1). In an emergency setting, under general anesthesia, the procedure was performed through a percutaneous transfemoral approach. Although local anesthesia is generally preferred for endovascular management of contained ruptured aneurysms at our institution, general anesthesia was required due to severe patient agitation. Initial angiography confirmed the presence of a large endoleak on the left side of the aorta, at the level of the visceral arteries, likely originating from the LRA or the SMA. Thus, selective catheterization of the LRA-stent was performed, followed by relining of the previously implanted 6 × 38-mm BeGraft balloon-expandable covered stent (Bentley InnoMed GmbH, Hechingen, Germany) using a 6 × 38-mm BeGraft, over a Rosen guidewire. Due to persistent endoleak, the SMA-stent was subsequently selectively cannulated, and the previously implanted 8 × 38-mm Advanta-V12 balloon-expandable covered stent (Getinge Group, Hudson, New Hampshire) was relined with an 8 × 37-mm BeGraft, also advanced over a Rosen guidewire. However, angiographic control revealed a persistent endoleak. Right renal artery stent and the celiac trunk were checked as well but revealed no endoleak; however, aortography demonstrated a discontinuity in the main body of the FEVAR graft between the SMA and the LRA, consistent with a type III endoleak due to fabric disruption. Therefore, a 12F × 33-mm introducer was placed, and a steerable 9F catheter with a 6F × 90-mm sheath was advanced coaxially into the abdominal aorta, and a selective catheterization of the graft defect was achieved with a .035 hydrophilic guidewire. Given the difficulty in advancing the introducer sheath across the graft defect, a diagnostic 4F catheter was used to cross the hole and access the aneurysm sac. Crossing proved technically challenging, even after predilatation with a 3 × 20-mm Armada 35 balloon (Abbott Vascular, Santa Clara, California). The defect could ultimately be crossed only with a 4F catheter, suggesting a relatively small defect size. In light of these technical findings, the largest device available in the institutional stock that was compatible with a 4F catheter and suitable for occluding a defect of this size was selected. Accordingly, an 8-mm Amplatzer Vascular Plug IV (Abbott, Abbott Park, Illinois) was deployed through the diagnostic 4F catheter to seal the fabric defect. The distal disk was opened within the sac and subsequently retracted toward the stent graft, allowing deployment of the proximal disk inside the stent graft and securing the plug across the defect (Figure 2). Final angiography showed a marked reduction of the endoleak, with minimal residual flow at the completion angiogram and duplex ultrasound (Figure 3).
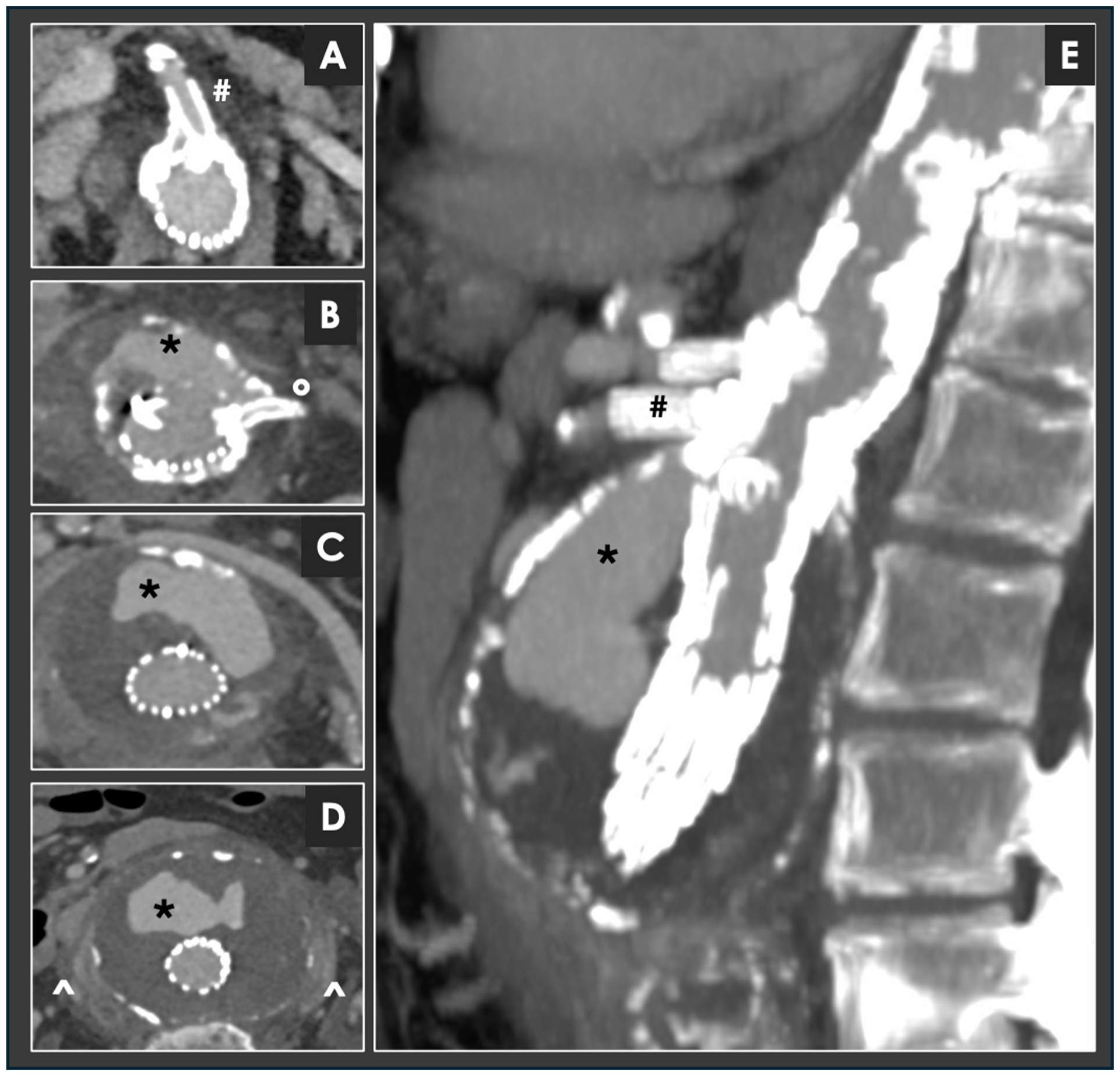
Computed tomography (CT) angiography performed in emergency in a patient treated with a custom-made fenestrated endovascular aortic repair (FEVAR) for a thoracoabdominal aortic aneurysm (TAAA) 3 years earlier. Axial images (A-D) and multiplanar reconstruction (E) demonstrate a massive endoleak originating at the level of the visceral vessels, between the superior mesenteric artery (SMA, #) and the left renal artery (LRA, °). The endoleak (* in panels B, C, D, and E) is associated with marked aneurysm sac enlargement compared with the previous CT (from 72 mm to 93 mm) and signs of contained rupture with periaortic hematoma (^ in panel D).
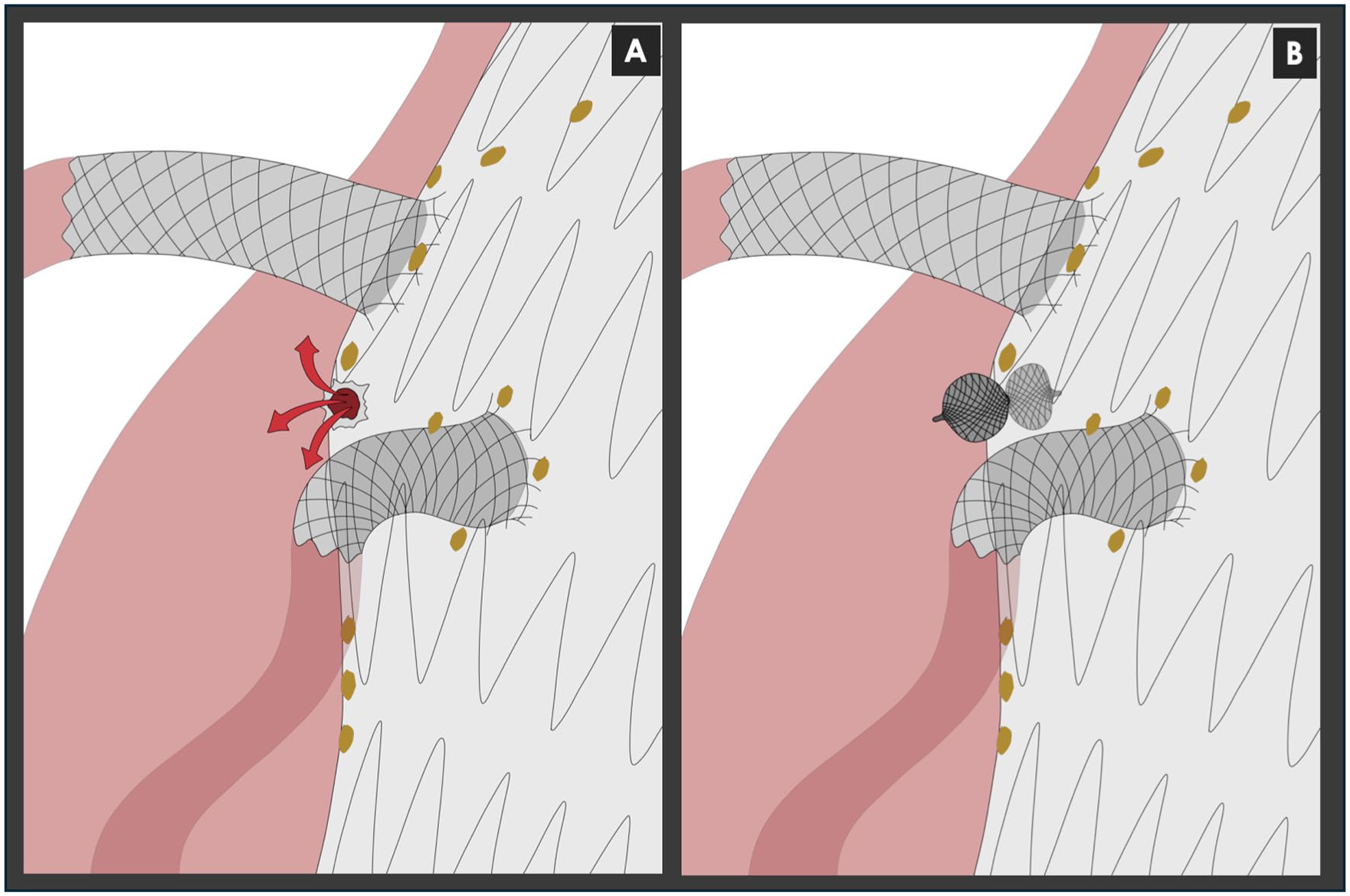
Representative imaging of the lesion and endovascular repair. (A) This image shows a discontinuity in the main body of the fenestrated graft, between the SMA and left LRA, consistent with a type III endoleak secondary to fabric disruption. (B) An endovascular repair was performed using an Amplatzer Vascular Plug IV deployed across the graft defect. The distal disk was positioned within the aneurysm sac, and the proximal disk was expanded within the stent graft lumen, securing the device across the fabric defect and achieving exclusion of the endoleak.
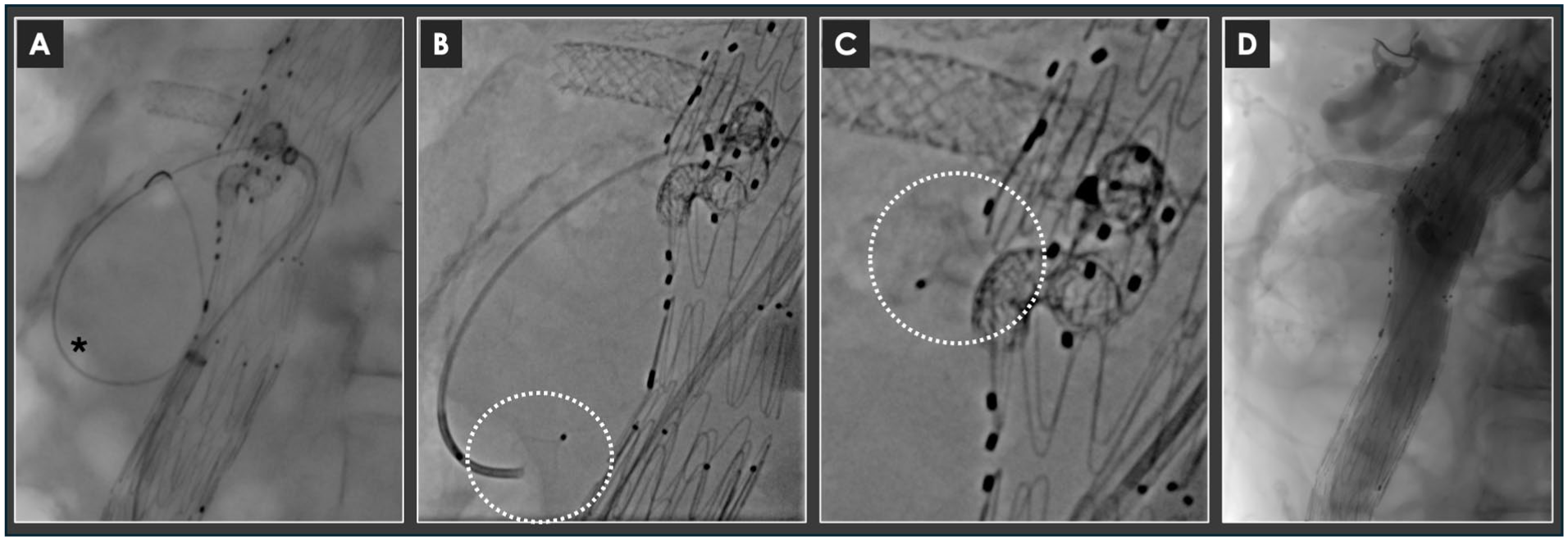
Intraoperative angiographic images of the procedure performed in an emergent setting. After relining with covered stents of the SMA and of the LRA, a persistent endoleak was documented. A discontinuity in the main body of the FEVAR graft between the SMA and the LRA, consistent with a type III endoleak due to fabric disruption, was detected. (A) A steerable 9F sheath and a 6F × 90-mm sheath were advanced coaxially into the abdominal aorta, and a selective catheterization of the graft defect was achieved using a .035 hydrophilic guidewire. (B) Due to the difficulty of advancing the materials over the narrow defect in the fabric, after a predilatation with a 3 × 20-mm balloon, a diagnostic 4F catheter was used to overpass the hole and enter the sac. An Amplatzer Vascular Plug IV (8 mm) was used to seal the hole in the fabric; the distal disk was opened inside the sac (dotted circle). (C) Then, the device was retracted until the proximal disk opened within the stent graft, securing the plug across the fabric defect (dotted circle). (D) Final angiography showed a marked reduction of the endoleak; a minimal residual flow at the completion angiogram was detected.
The procedure was well tolerated. The postoperative course was uneventful, and the patient was discharged home on postoperative day 6. Serial ultrasound and CT follow-up demonstrated progressive reduction of the endoleak, of the aneurysm sac, and complete regression of the periaortic effusion. The CT angiography performed 1 year after the procedure showed complete resolution of the endoleak and a significant shrinkage of the aneurysm sac (from 93 mm to 70 mm), with preserved visceral and renal perfusion (Figure 4).
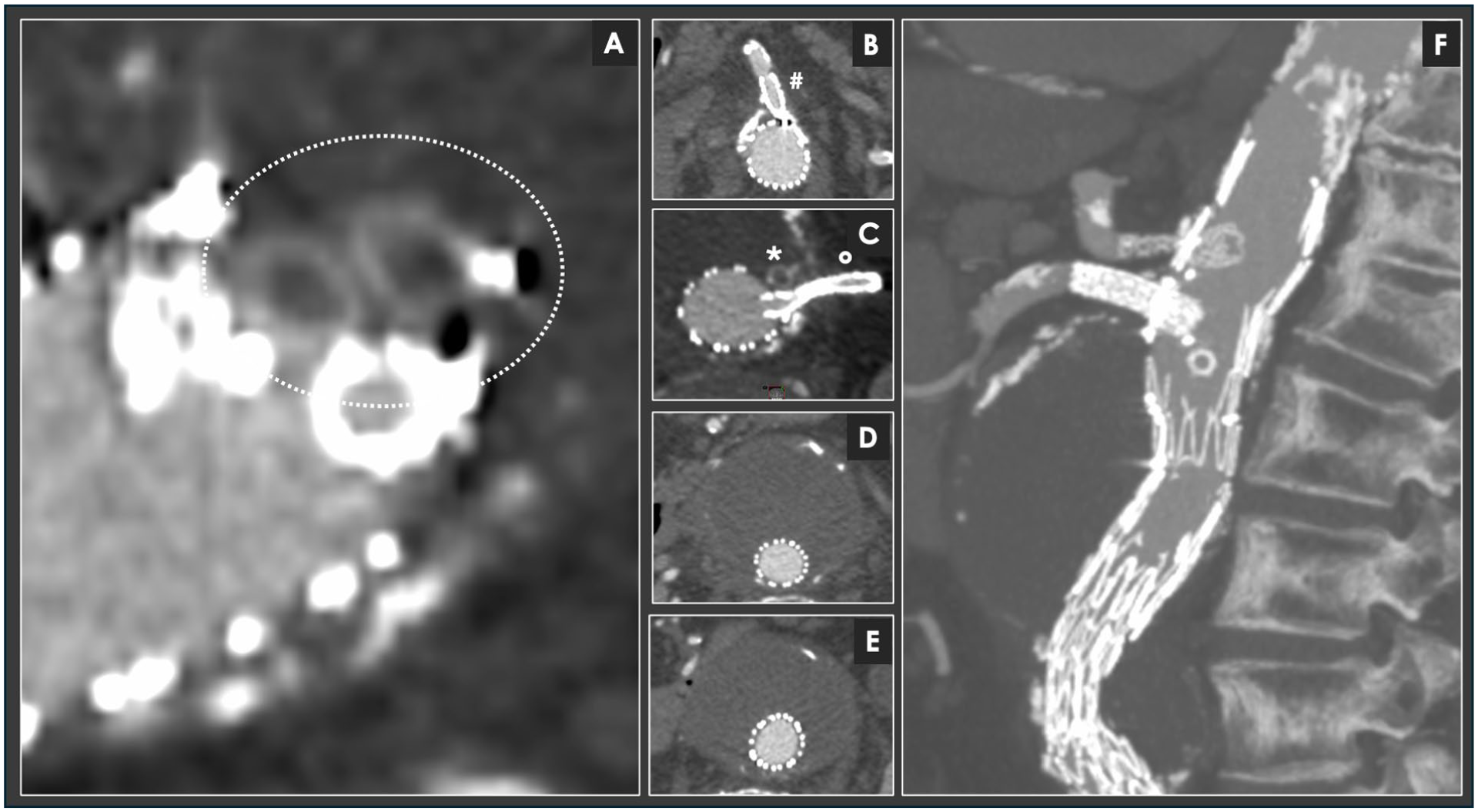
One-year follow-up CT scan. Serial imaging within the first postoperative year showed progressive reduction of the endoleak and initial sac shrinkage. At 1 year, CT confirmed complete exclusion of the endoleak and significant aneurysm sac regression (from 93 mm to 70 mm). (A) Multiplanar reconstruction showing the thrombosed Amplatzer Vascular Plug IV (dotted circle) with no residual endoleak. (B-E) Axial images and (F) multiplanar reconstruction (with the same projection of image 1E) confirm complete exclusion of the aneurysm sac and absence of further endoleak. The thrombosed plug is positioned between the SMA (#) and the LRA (°).
Discussion
This case highlights a rare but serious complication following FEVAR: a type III endoleak due to graft body disruption in the visceral segment. Such structural failures are uncommon but can lead to rapid sac expansion and rupture due to high-pressure endoleak; notably, the occurrence of a fabric defect only 3 years after the index implantation, as observed in the present case, raises concerns regarding device durability.2,5 Type III endoleaks are classified into type IIIa (component separation) and type IIIb (fabric disruption), the latter being less frequent but particularly concerning because of the direct systemic pressurization of the aneurysm sac.2,5,6
Previous reports have shown that fabric defects most commonly occur at areas of increased mechanical stress, including overlap zones between components, near fenestrations, or in proximity to bridging stents within the visceral segment. In fenestrated and branched configurations, the interaction between the main body graft and balloon-expandable bridging stents may generate focal stress concentrations, potentially predisposing to late fabric fatigue or suture-line failure. Proposed mechanisms include chronic pulsatile mechanical fatigue, micromotion at junctional zones, material degeneration, and continuous radial forces exerted by bridging stents. Although the overall incidence of type IIIb endoleaks after FEVAR remains low, their clinical impact is significant, often requiring urgent reintervention. 6
When such defects occur in aortic segments without adjacent visceral branches or critical collaterals, relining with an aortic cuff is generally a straightforward and effective solution. However, in the present case, the defect was located within the fenestrated visceral segment, between target vessels, precluding the use of a standard cuff without compromising branch perfusion. An alternative strategy could have been the implantation of a custom-made fenestrated-in-fenestrated device; nevertheless, this approach is technically more complex and not feasible in an urgent setting.7,8
Therefore, cases such as the one described may be particularly challenging to manage. In this scenario, selective catheterization and plug deployment provided an effective bailout solution, allowing exclusion of the defect while preserving visceral branch patency.7-10 Strict postoperative surveillance remains essential for early identification of late complications.
Conclusion
This emergent endovascular reintervention with plug embolization in a patient previously treated with FEVAR, presenting with a hole in the fabric in the visceral segment, provided an effective solution for treating a minor fabric defect. In this high-risk patient, prompt diagnosis and the described peculiar endovascular management resulted in complete exclusion of the ruptured aneurysm and sustained sac regression at 1-year follow-up. However, a 1-year follow-up period may be insufficient to draw definitive conclusions regarding long-term durability, and extended follow-up is warranted to further assess the sustained safety and effectiveness of this technique.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.